Embed Size (px)
Citation preview
Clinical case on HEVAntonio Rivero-Juarez
Clinical Virology and Zoonisis Research Group (GC-26)
Instituto Maimonides de Investigación Biomédica de Córdoba (IMIBIC)
Infectious Diseases Unit
Hospital Universitario Reina Sofía de Córdoba
Disclosure• Payment to my Institution:
• Public Funds: Fundación para la investigación en Salud (FIS)
• Private Funds: AbbVie y ViiV Healthcare
• Payment to me:
• Consultancy: Roche Diagnostics, Gilead, and Bristol Mier Squidd
• Payment for lectures including service on speakers bureaus: Bristol Mier Squidd, ViiV Healtcare,
Janssen Cilag, MSD, y Roche Diagnostics, AbbVie, and Gilead.
• Other relationships/conditions/circumstances:
• I have no personal, business, social or acquaintance relationship with food or livestock enterprises.
• I´m not vegetarian

Today agenda
Plan
• One case of hepatitis E virus infection in HIV infected patient
Aims
• Appreciate presentations of Hepatitis E virus in HIV infected patients
• Explore epidemiology and risk groups
• Explore diagnostic aspects
• Explore treatment options
• Explore follow-up measures
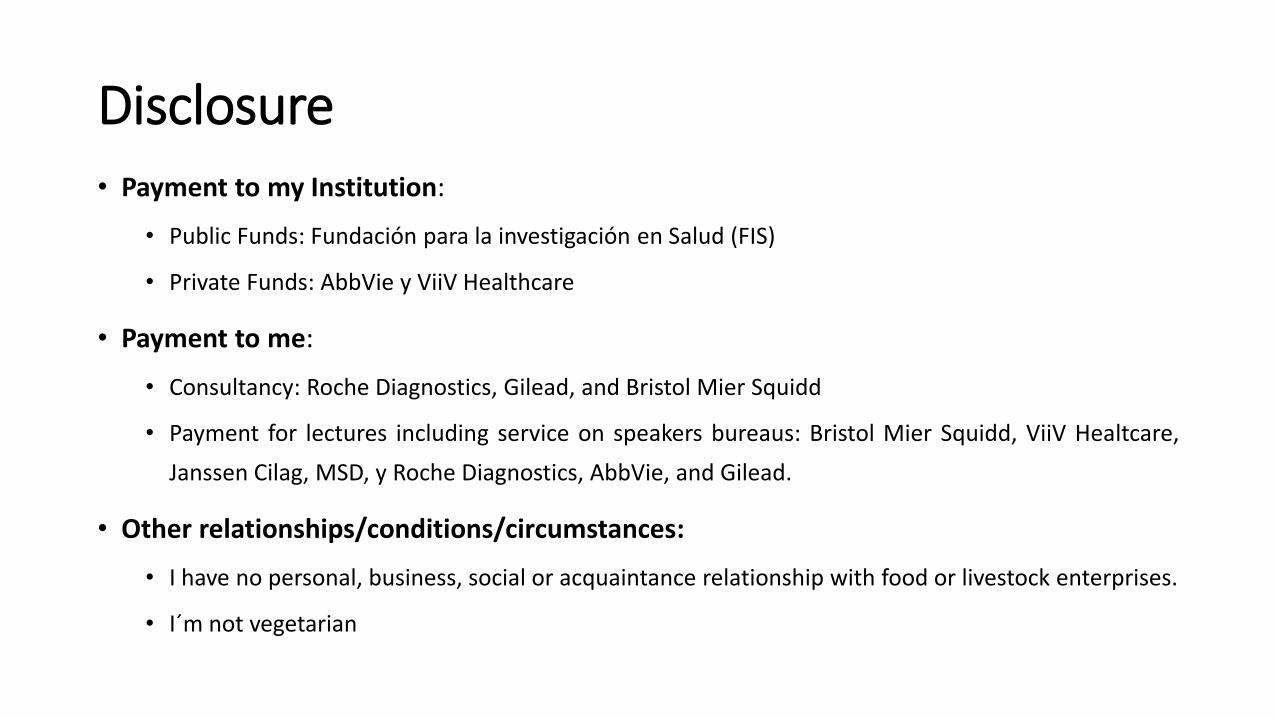
Case presentation• 47-year-old white MSM diagnosed of HIV infection
• Weight: 105 kg ; AP: 125/79
• On-ART with undetectable viral load with a CD4+ count of 97 cells/uL
• Experienced a increase on ALT levels (482 IU/L), without symptoms.
• LS of 4.9 kPa = F0-F1
• Serological evaluation:
• HCV: negative
• HBV: negative
• HAV: negative
• HEV IgM: positive
• HEV IgG: negative
• HEV-RNA: positive
• Genotype: 3
EASL HEV Guidelines 2018
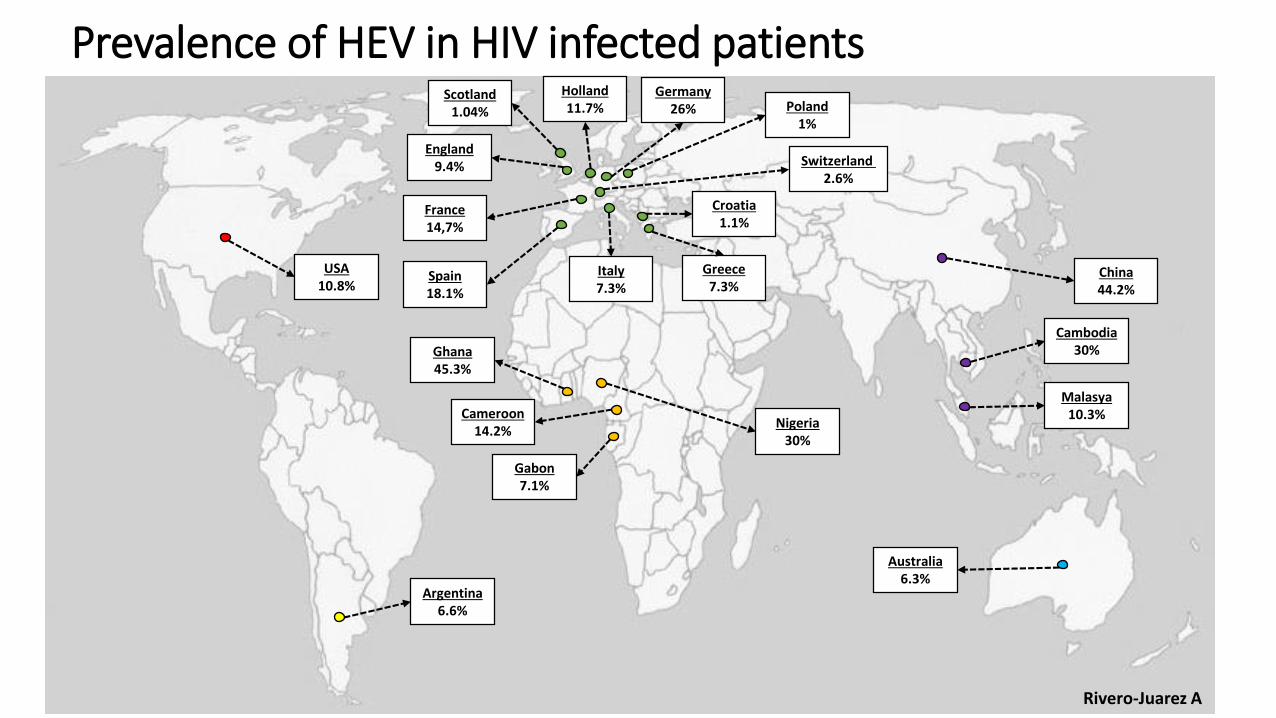
Prevalence of HEV in HIV infected patients
France14,7%
Spain18.1%
Italy7.3%
Greece7.3%
Scotland1.04%
England9.4% Switzerland
2.6%
Holland11.7%
Croatia1.1%
Gabon7.1%
Cameroon14.2%
Nigeria30%
Ghana45.3%
USA10.8%
Argentina6.6%
Australia6.3%
Malasya10.3%
Cambodia30%
China44.2%
Poland1%
Germany26%
Rivero-Juarez A
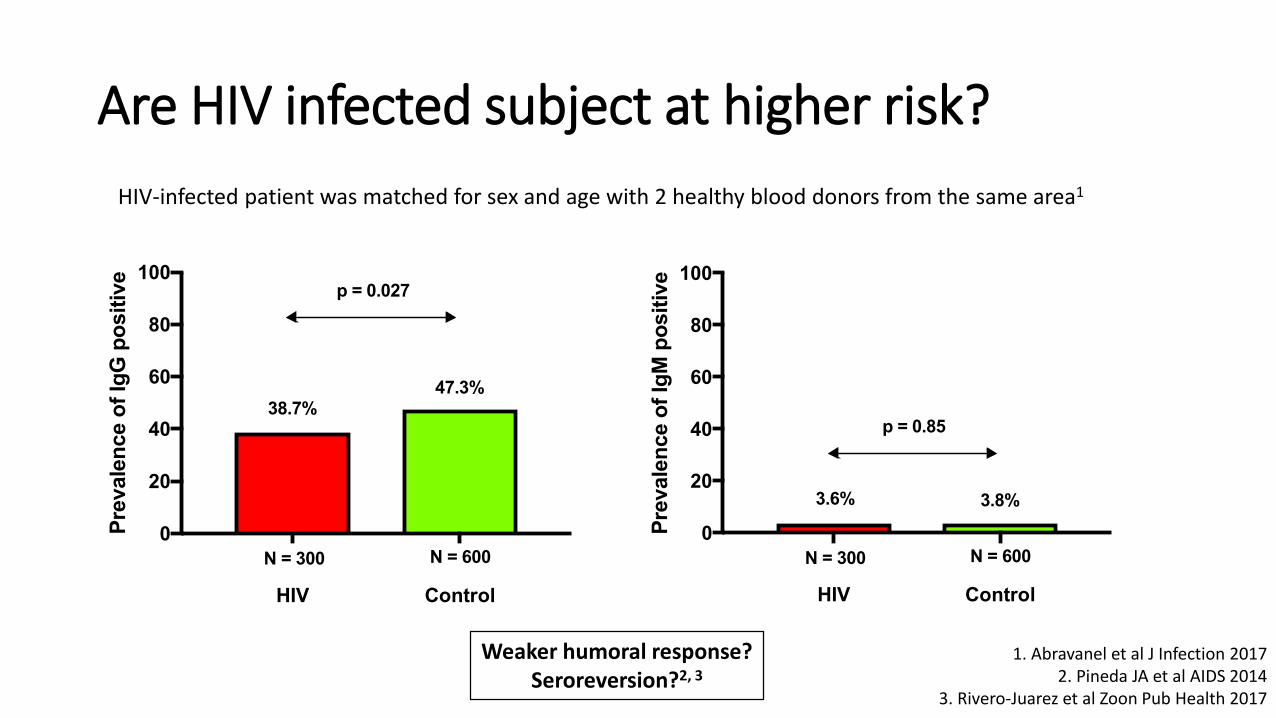
Are HIV infected subject at higher risk?
HIV Control
0
20
40
60
80
100
Pre
vale
nce o
f Ig
G p
osit
ive
N = 300 N = 600
38.7%47.3%
p = 0.027
HIV Control
0
20
40
60
80
100
Pre
vale
nce o
f Ig
M p
osit
ive
N = 300 N = 600
3.6% 3.8%
p = 0.85
HIV-infected patient was matched for sex and age with 2 healthy blood donors from the same area1
1. Abravanel et al J Infection 20172. Pineda JA et al AIDS 2014
3. Rivero-Juarez et al Zoon Pub Health 2017
Weaker humoral response?Seroreversion?2, 3
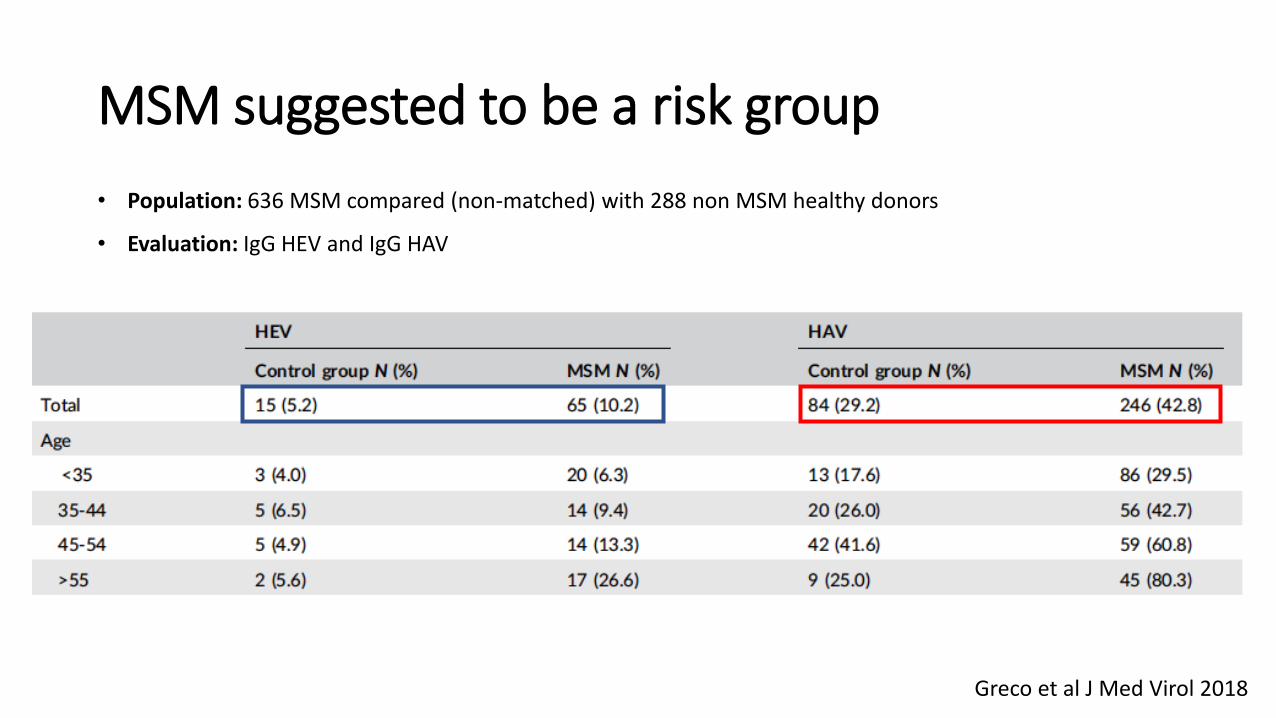
MSM suggested to be a risk group
• Population: 636 MSM compared (non-matched) with 288 non MSM healthy donors
• Evaluation: IgG HEV and IgG HAV
Greco et al J Med Virol 2018
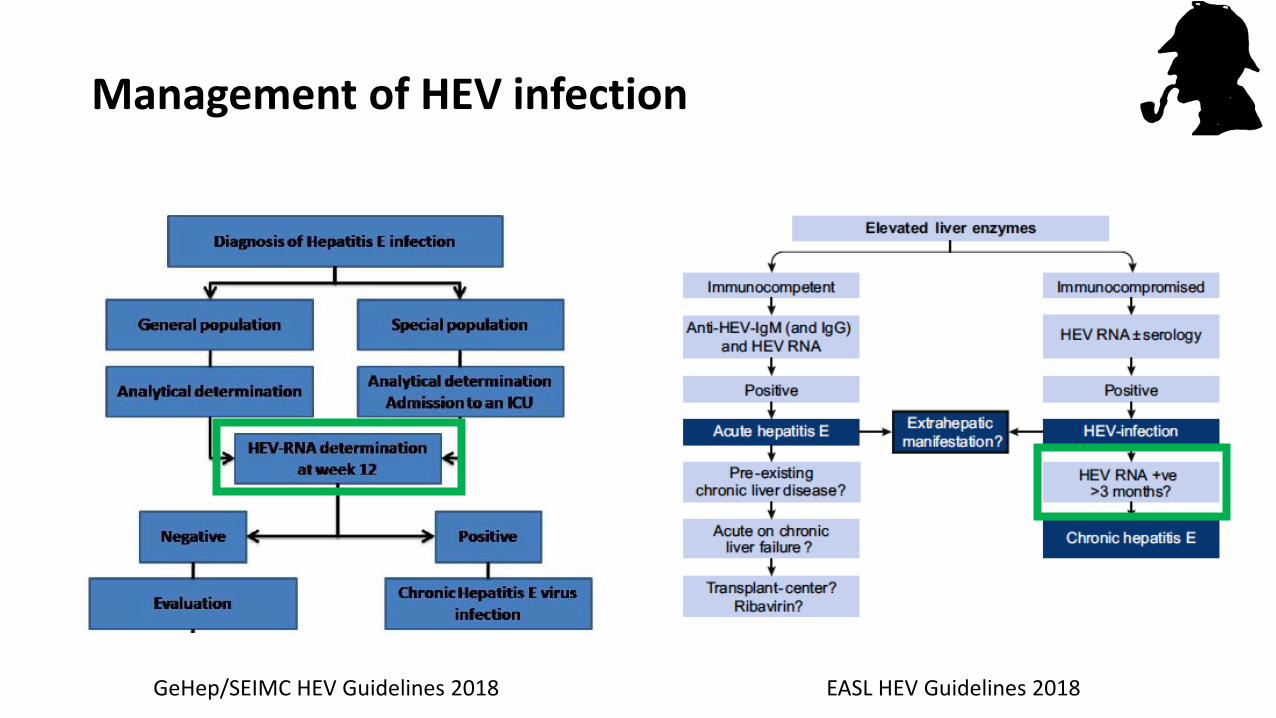
Management of HEV infection
GeHep/SEIMC HEV Guidelines 2018 EASL HEV Guidelines 2018
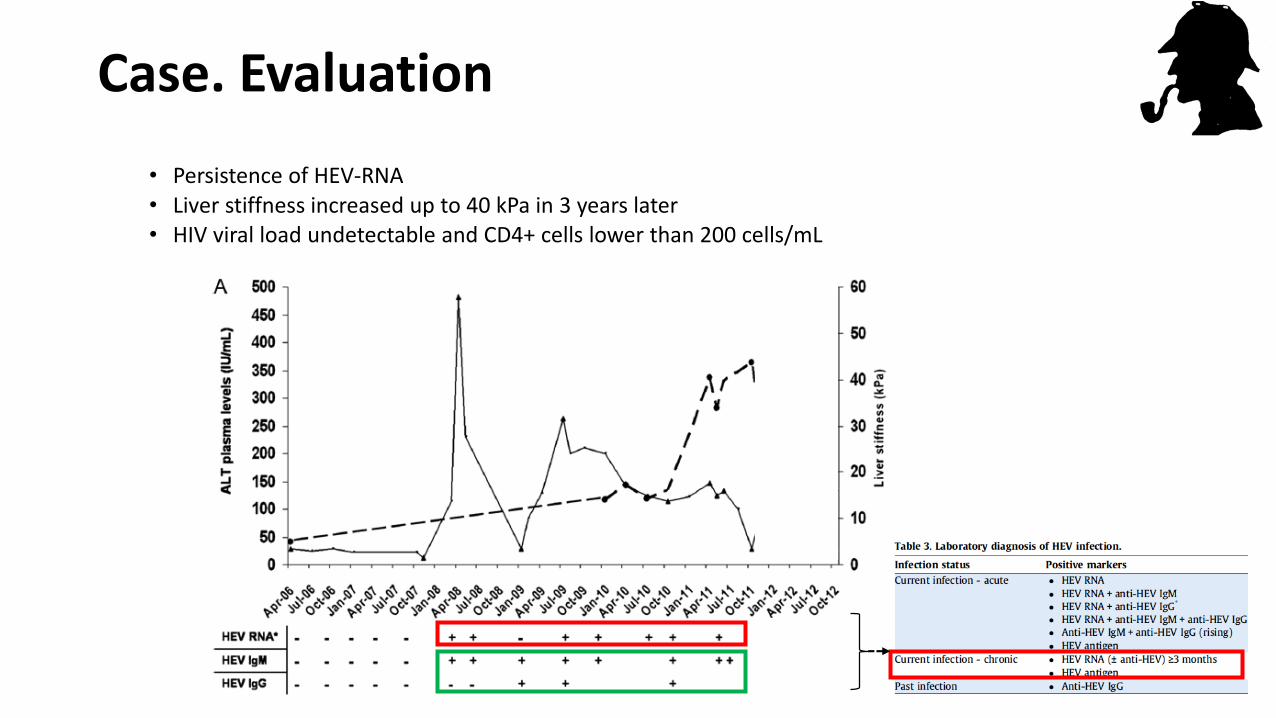
Case. Evaluation
• Persistence of HEV-RNA• Liver stiffness increased up to 40 kPa in 3 years later• HIV viral load undetectable and CD4+ cells lower than 200 cells/mL
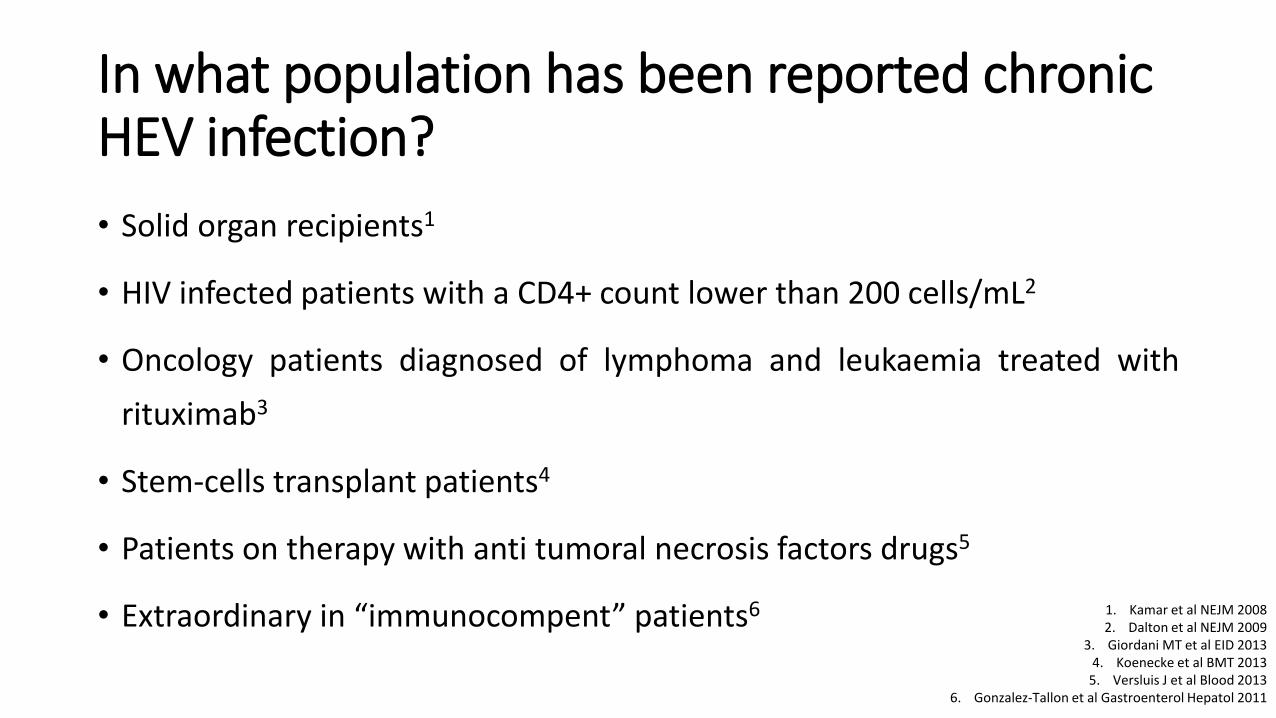
In what population has been reported chronic HEV infection?
• Solid organ recipients1
• HIV infected patients with a CD4+ count lower than 200 cells/mL2
• Oncology patients diagnosed of lymphoma and leukaemia treated with
rituximab3
• Stem-cells transplant patients4
• Patients on therapy with anti tumoral necrosis factors drugs5
• Extraordinary in “immunocompent” patients6 1. Kamar et al NEJM 20082. Dalton et al NEJM 2009
3. Giordani MT et al EID 20134. Koenecke et al BMT 2013
5. Versluis J et al Blood 20136. Gonzalez-Tallon et al Gastroenterol Hepatol 2011
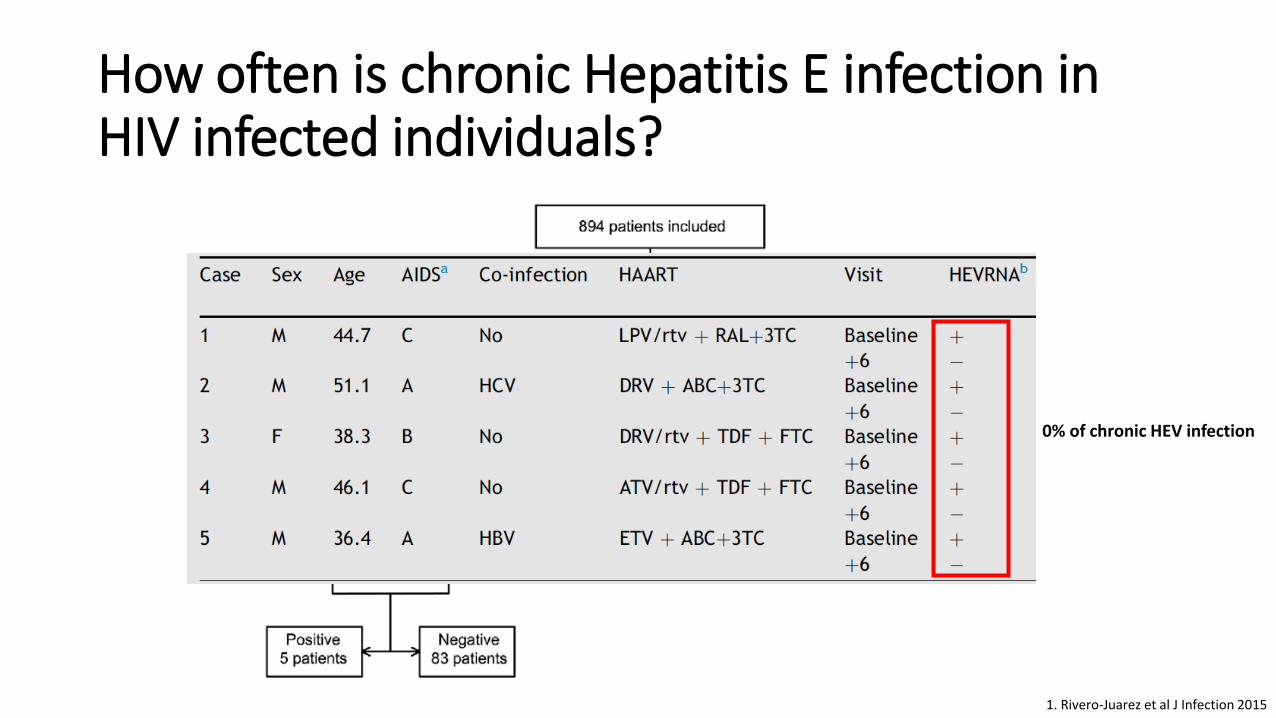
How often is chronic Hepatitis E infection in HIV infected individuals?
1. Rivero-Juarez et al J Infection 2015
0% of chronic HEV infection
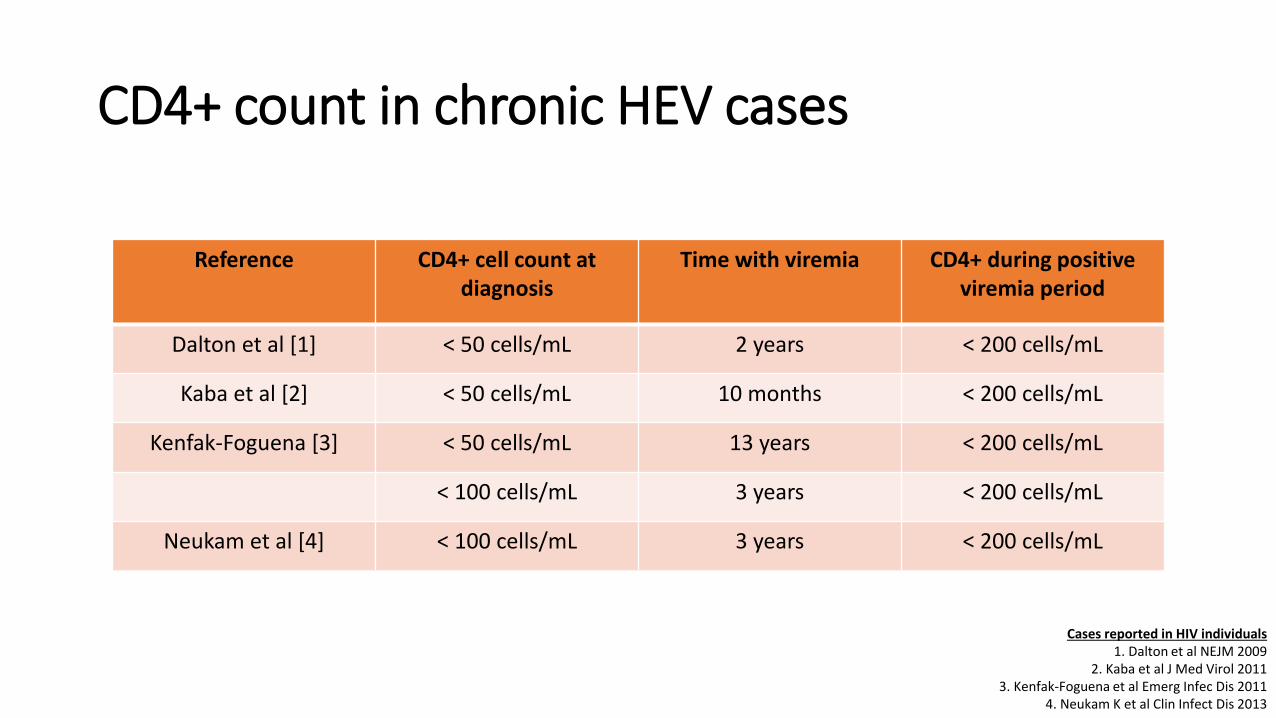
CD4+ count in chronic HEV cases
Reference CD4+ cell count at diagnosis
Time with viremia CD4+ during positive viremia period
Dalton et al [1] < 50 cells/mL 2 years < 200 cells/mL
Kaba et al [2] < 50 cells/mL 10 months < 200 cells/mL
Kenfak-Foguena [3] < 50 cells/mL 13 years < 200 cells/mL
< 100 cells/mL 3 years < 200 cells/mL
Neukam et al [4] < 100 cells/mL 3 years < 200 cells/mL
Cases reported in HIV individuals1. Dalton et al NEJM 2009
2. Kaba et al J Med Virol 20113. Kenfak-Foguena et al Emerg Infec Dis 2011
4. Neukam K et al Clin Infect Dis 2013
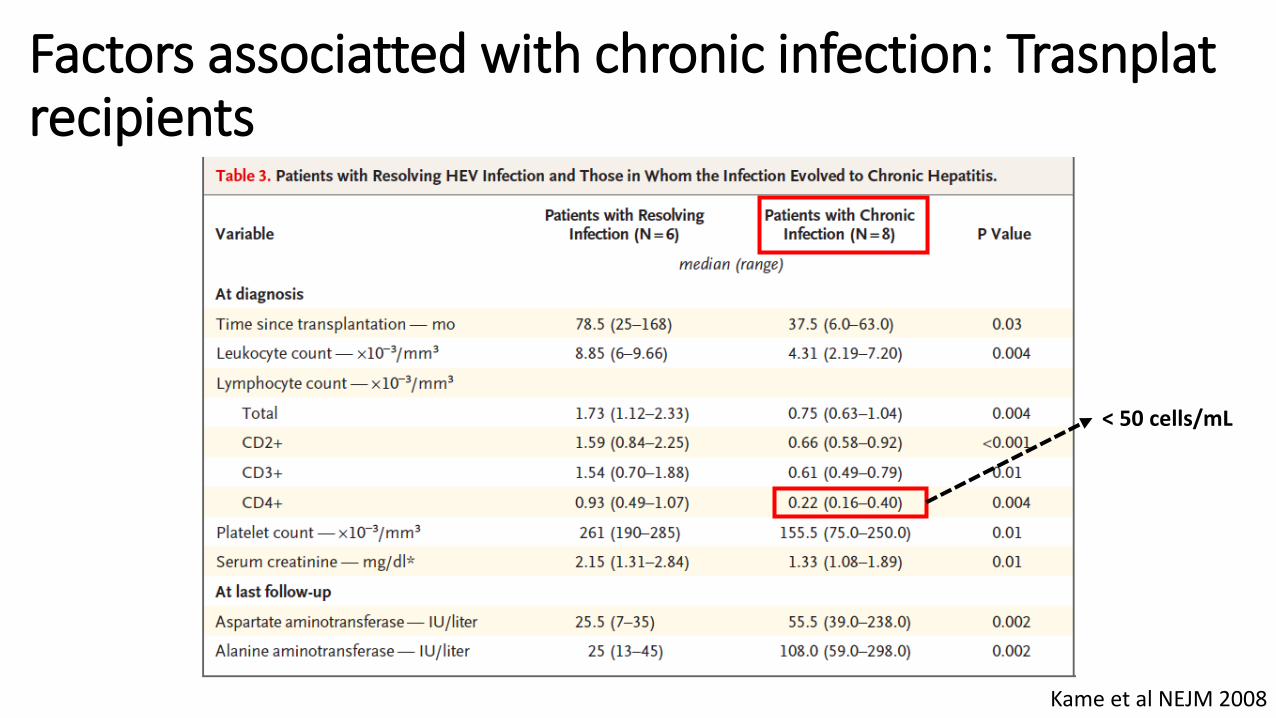
Factors associatted with chronic infection: Trasnplatrecipients
Kame et al NEJM 2008
< 50 cells/mL
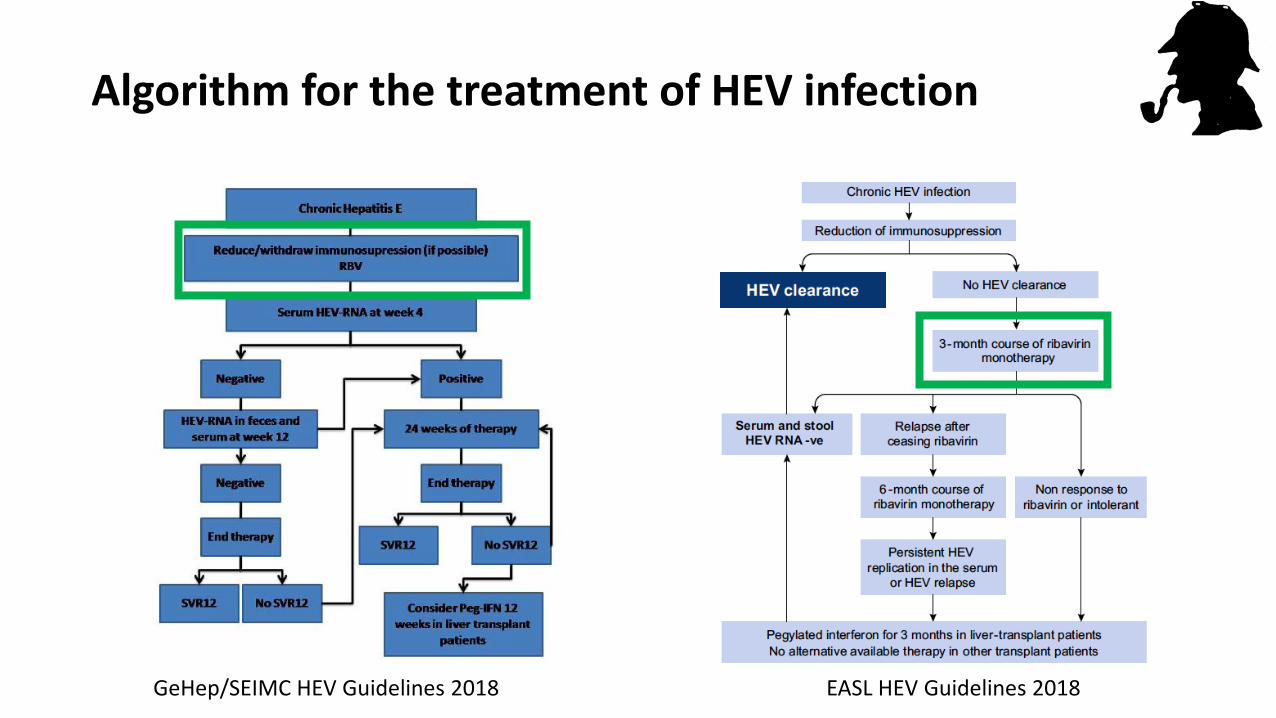
Algorithm for the treatment of HEV infection
GeHep/SEIMC HEV Guidelines 2018 EASL HEV Guidelines 2018
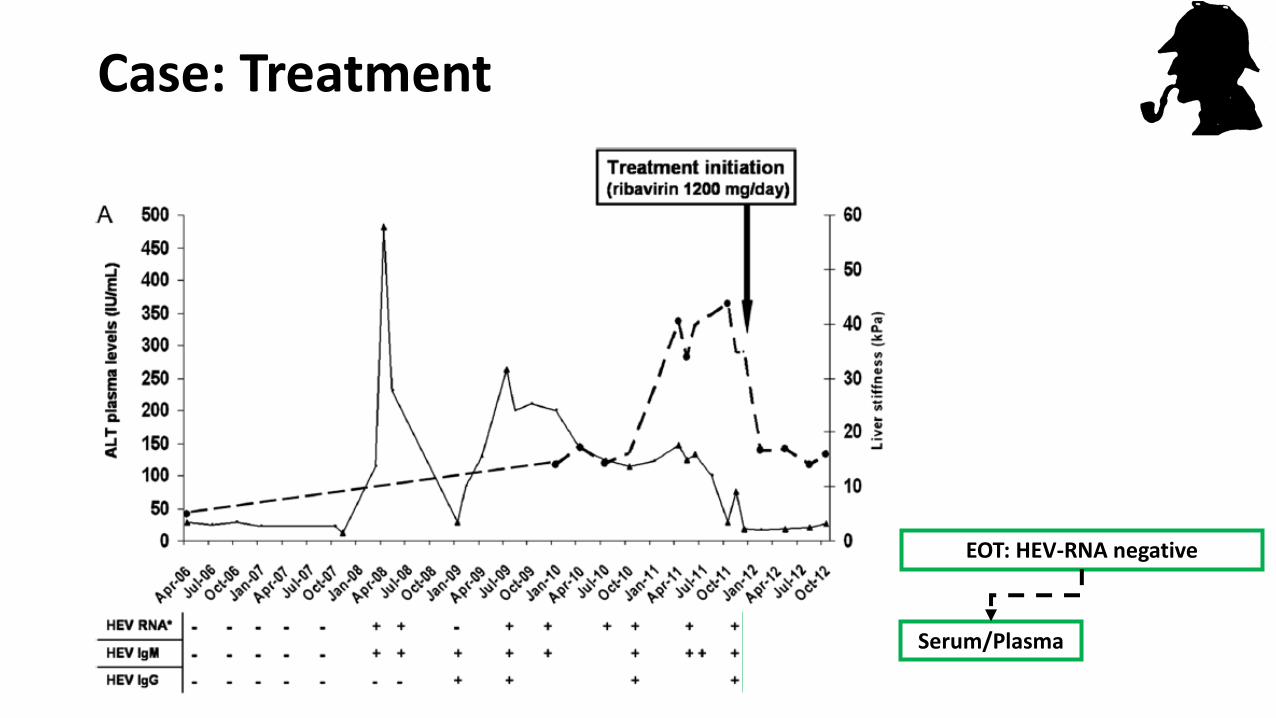
Case: Treatment
EOT: HEV-RNA negative
Serum/Plasma
Evaluation after complention of therapy
• HEV-RNA
• In serum
• In faeces
• If detectable HEV-RNA in faeces, absence of a response to treatment should be
assumed, since the persistence of HEV-RNA in the faeces, even when absent in the
serum, is associated with HEV recurrence following the interruption of the RBV1
1. Abravanel et al Clin Infect Dis 2015
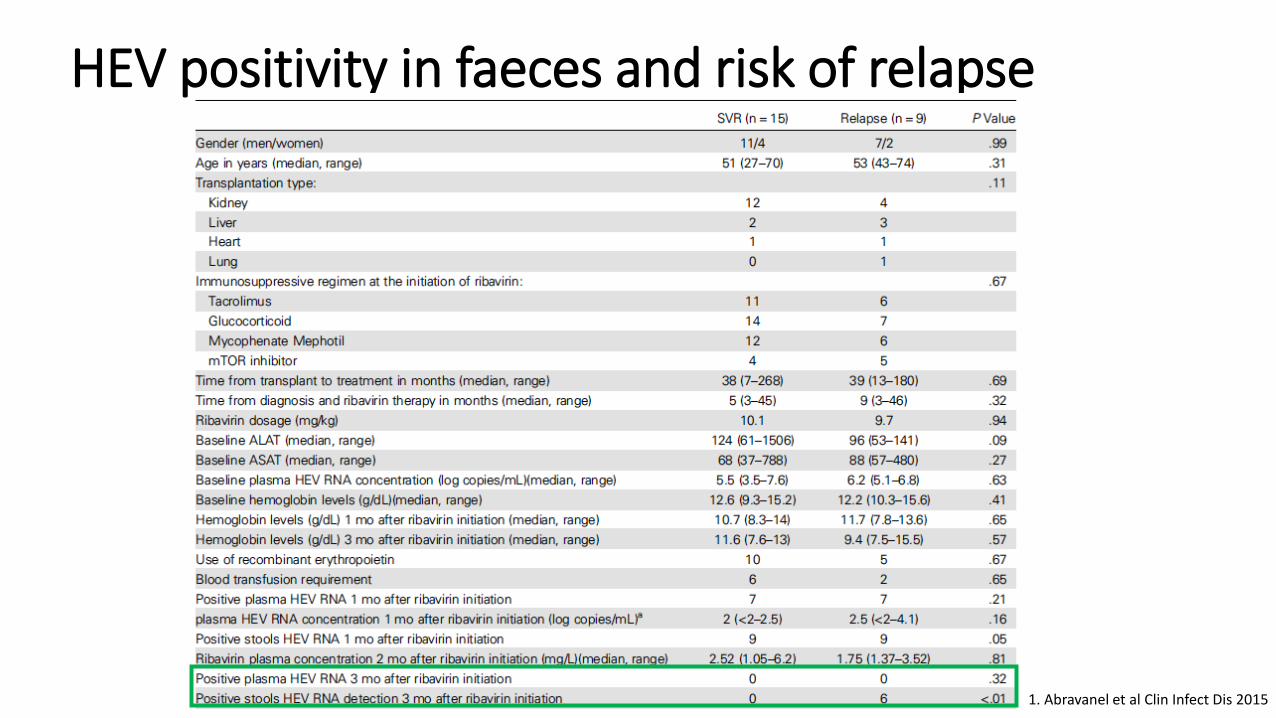
HEV positivity in faeces and risk of relapse
1. Abravanel et al Clin Infect Dis 2015
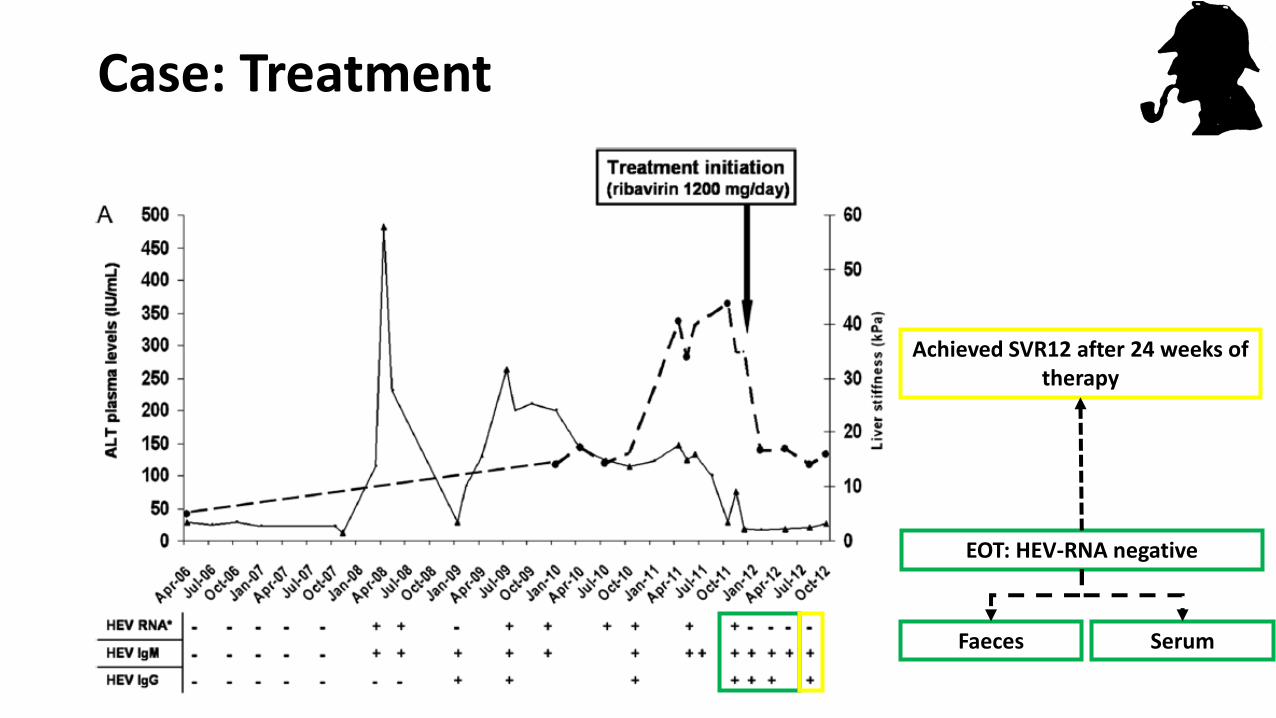
Case: Treatment
Achieved SVR12 after 24 weeks of therapy
EOT: HEV-RNA negative
Faeces Serum
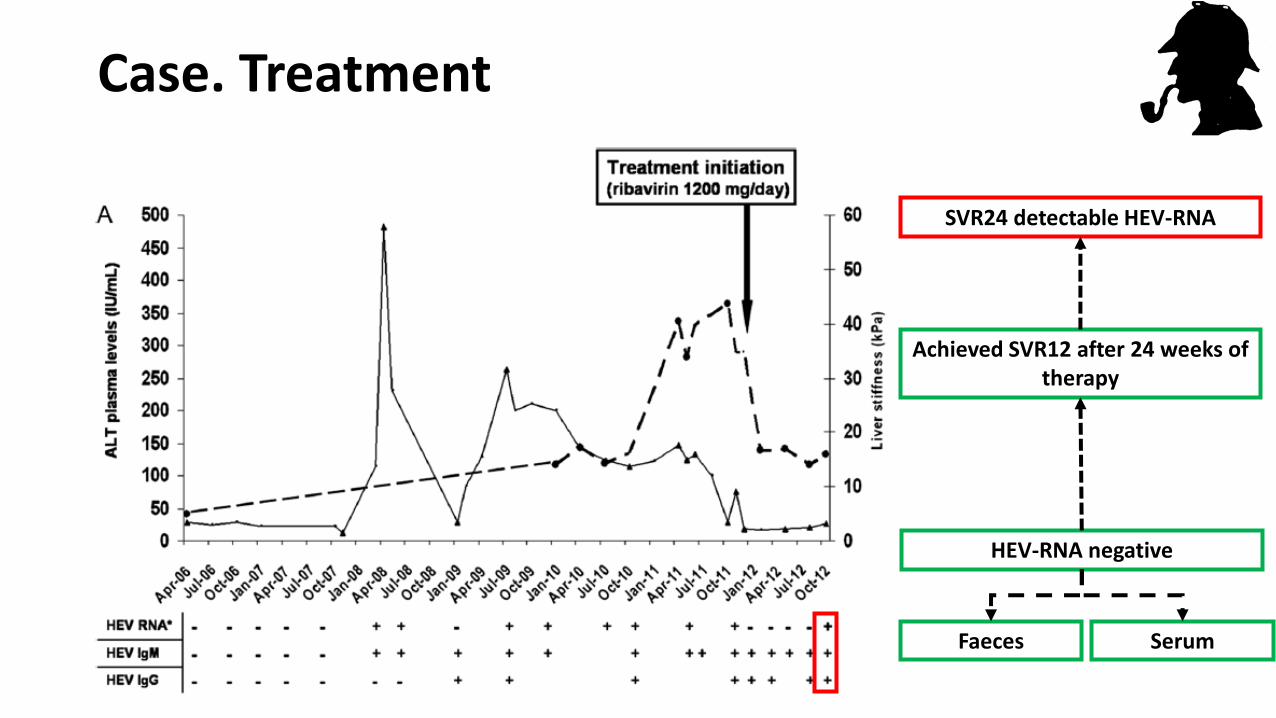
Case. Treatment
Achieved SVR12 after 24 weeks of therapy
HEV-RNA negative
Faeces Serum
SVR24 detectable HEV-RNA

Rates of SVR
Peters van Ton J Viral Hep 2015
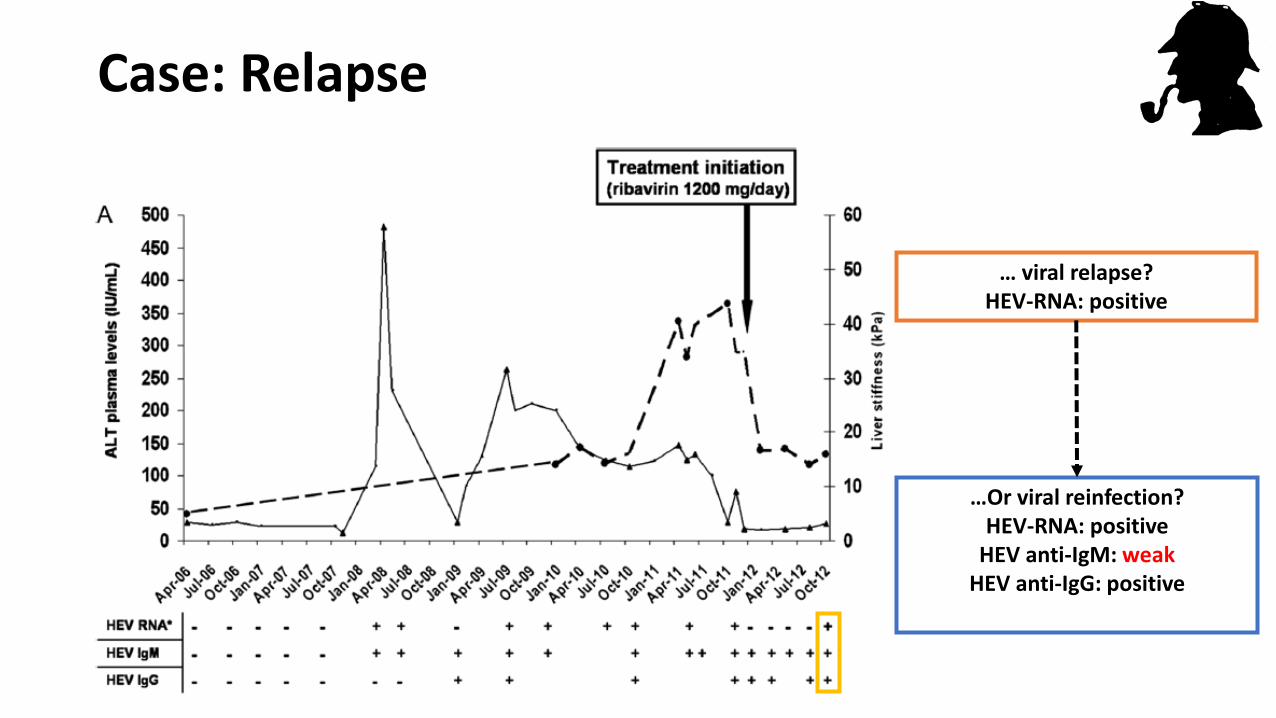
… viral relapse?HEV-RNA: positive
…Or viral reinfection?HEV-RNA: positive
HEV anti-IgM: weakHEV anti-IgG: positive
Case: Relapse

Reinfection: serological and virological patern
GeHep/SEIMC HEV Guidelines 2018 EASL HEV Guidelines 2018

Reinfection in solid organ transplant patients
1. Abravanel JID 2014
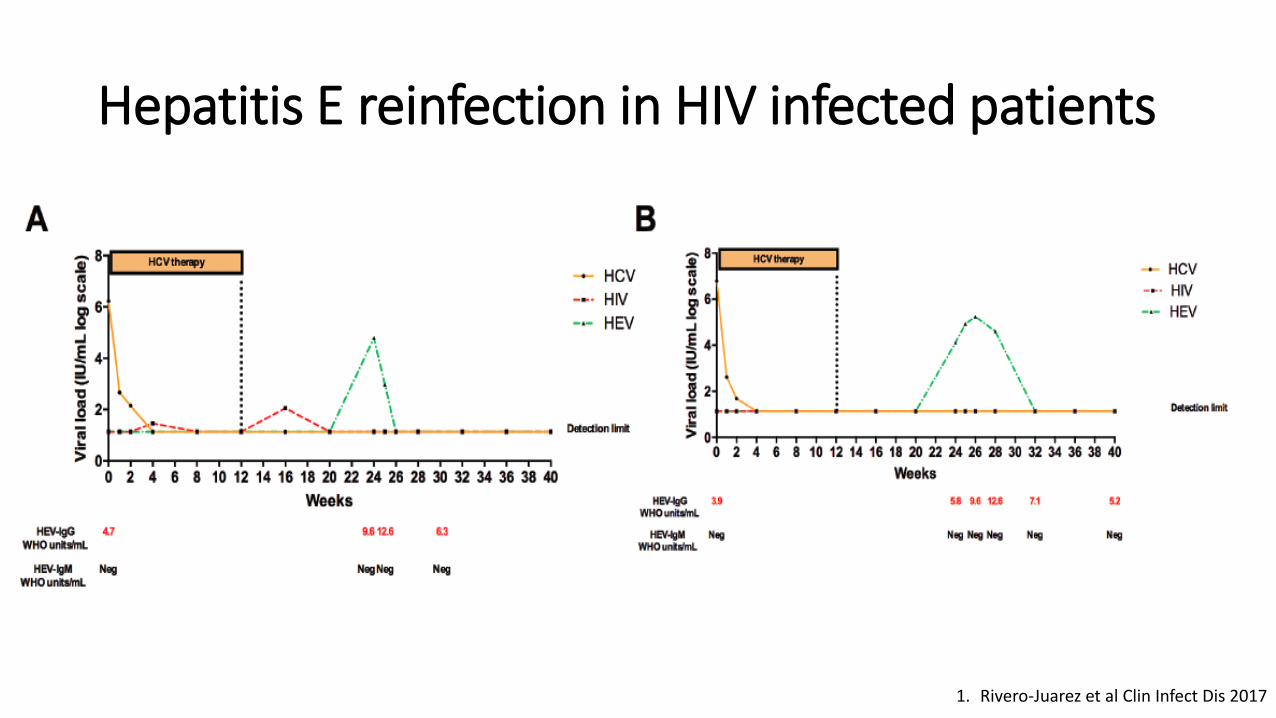
Hepatitis E reinfection in HIV infected patients
1. Rivero-Juarez et al Clin Infect Dis 2017
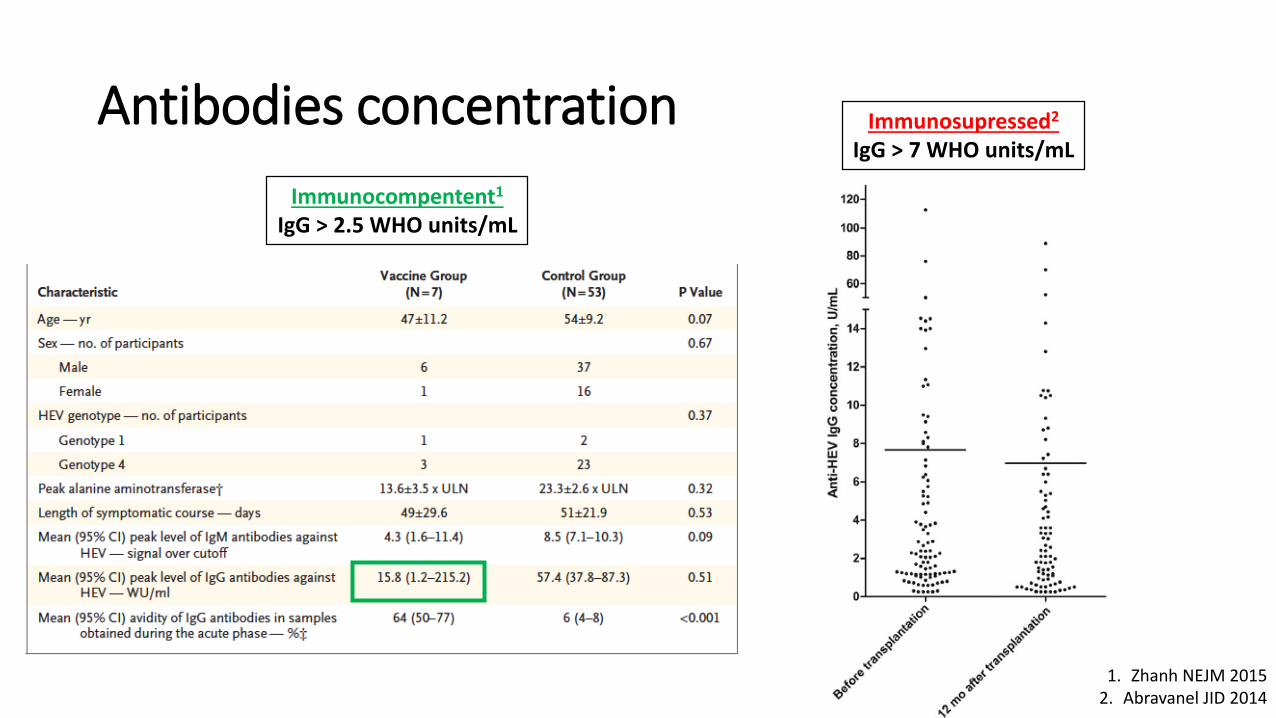
Antibodies concentration Immunosupressed2
IgG > 7 WHO units/mL
1. Zhanh NEJM 20152. Abravanel JID 2014
Immunocompentent1
IgG > 2.5 WHO units/mL
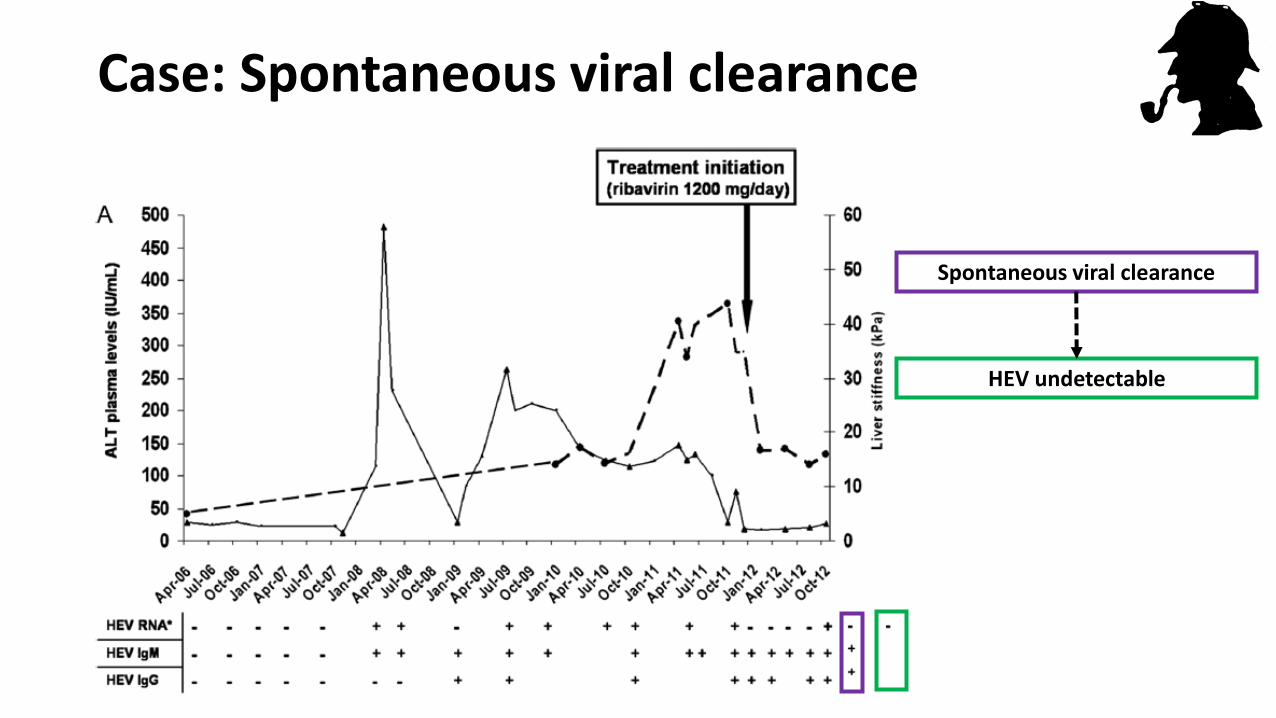
Spontaneous viral clearance
Case: Spontaneous viral clearance
HEV undetectable
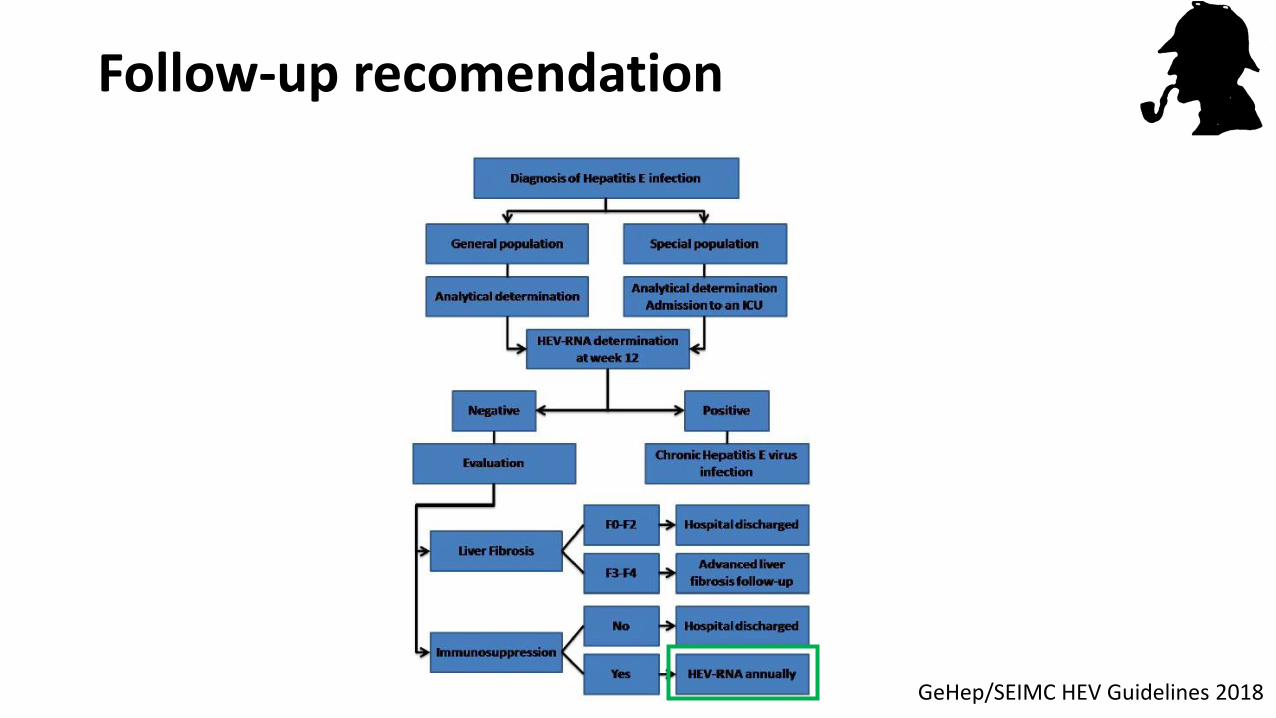
Follow-up recomendation
GeHep/SEIMC HEV Guidelines 2018
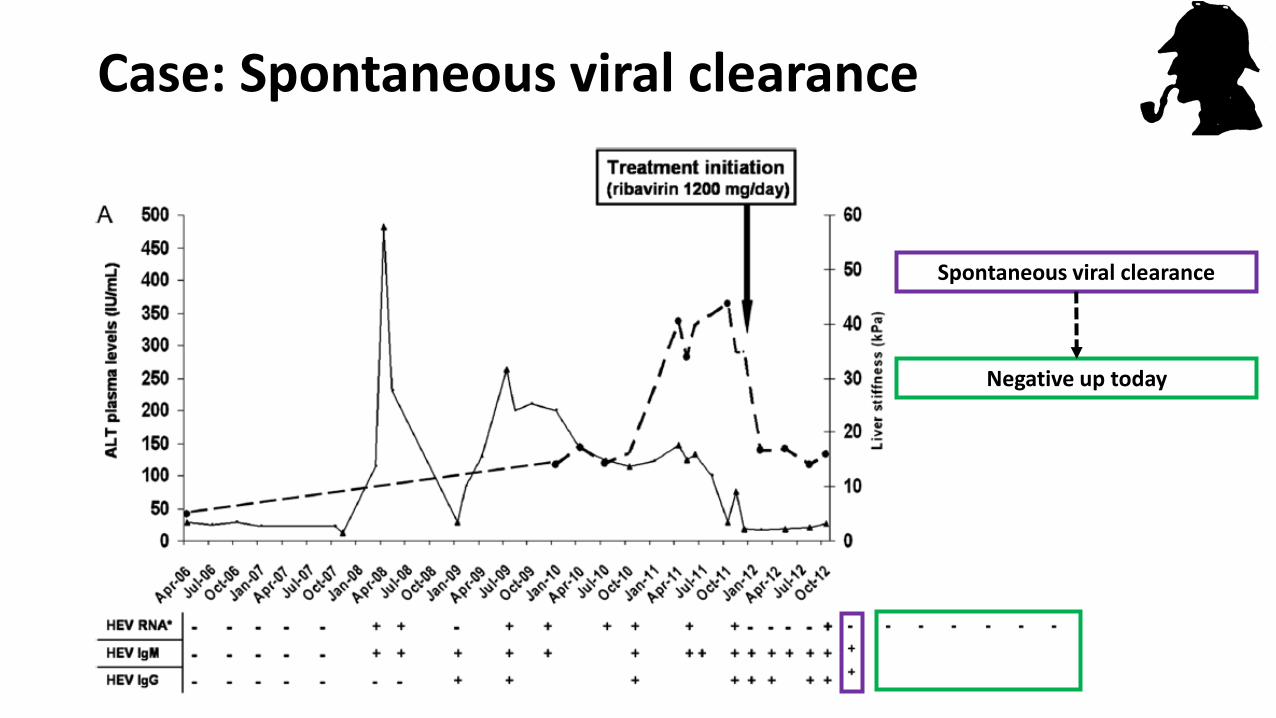
Spontaneous viral clearance
Case: Spontaneous viral clearance
Negative up today
Case. Resolution
• Chronic HEV infection with spontaneous viral clearance after late
relapse to RBV monotherapy during 24 weeks
• Or spontaneous viral clearance after HEV reinfection after achieve
SVR to RBV monotherapy during 24 weeks (phylogenetic analysis is
needed to confirm)
Final remarks
• Hepatitis E virus infection is common and should be take in mind in the screening
of acute hepatitis
• Chronic Hepatitis E virus infection, although is rare, should be considered in HIV
infected patients with chronic liver damage of unknow origin
• First-line chronic HEV infection: RBV w-a during 12 weeks
• SVR should be only considered when both serum and faeces are negative
• Reinfections should be considered in HIV infected patients, so annually HEV-RNA
must be performed in immunosuppressed patients.
Acknowledge:
Mario FríasIsmael ZafraTeresa BrievaDiego Rodríguez CanoLaura RuizÁngela CamachoFrancisca CuencaIsabel MachucaPedro LópezAntonio MartínezAngeles RisaldeAntonio Rivero
Ignacio García BocanegraDavid CanoSaul JimenezFernando Romero José Carlos Villamandos
Vicente FernandezJuan Luis Millan
Pilar AlberdiUrsula HöfleChristian GortázarFrancisco Ruiz Fons
@Arivejua