Embed Size (px)
Citation preview

Clinical Cardiovascular Anatomy & Physiology
Concepts, Definitions, & Principles
Slides developed in collaboration with Dr. John Green, 2003.




Intima
Adventitia
Media
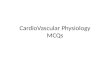
The Normal Heart - Coronary Artery Anatomy
Left Main CA
Circumflex
Left Anterior Descending CA
Right CA
Marginal Branch
Layers of the Arterial Wall

The Heart as a Pump
Reference: Berne and Levy, “Physiology”







Cardiac Muscle Differences
• Fibers organized into functional syncytium– branching, interconnected fibers
• ends separated by intercalated disks fused to adjoining fibers by tight junctions; low resistance
• all-or-none law applies to entire myocardium
• Cannot be tetanized– due to phase 2 (plateau) of action potential

Left Ventricular Volumes - Definitions
End Diastolic Volume (EDV) Volume at the end of diastole (end of ventricular filling)
End Systolic Volume (ESV)Volume at the end of systole(end of ventricular contraction)
Stroke Volume (SV) = EDV - ESV
Ejection Fraction (EF) = SV EDV
Left ventricular norm: 62%
Ejection Fraction is the best indicator of heart performance and disease prognosis



• Cardiac Output (Q) = HR X SV
• Cardiac Index = Q / body surface area
• Preload: diastolic filling volume of the left ventricle (EDV reflects stretch of the cardiac muscle cells)
• Afterload: resistance to ventricular emptying during systole (the amount of pressure the left ventricle must generate to squeeze blood into the aorta
• Frank Starling Law of the Heart - the heart will contract with greater force when preload (EDV) is increased
• Myocardial Contractility - the squeezing contractile force that the heart can develop at a given preload
•regulated by:•sympathetic nerve activity (most influential)•catecholamines (epinephrine norepinephrine)•amount of contractile mass •drugs
Definitions

Starlings Law of the Heart and Contractility
SV
leftventricular
performance
preload (venous return)
↑ contractility
normal contractility
↓ contractility(heart failure)

0
120
dP/dt dP/dt
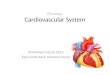
Using Ventricular Pressure Curves as Indices of Contractility & Cardiac Function
Normal
Heart Failure
dP/dt = change in pressure per unit of time
Note elevation in end diastolic pressure

Contractility• - a change in developed tension at a given
resting fiber length OR an increase in Vmax
– increase max dP/dt from LV pressure curve– Positive and negative inotropic effects– Ejection fraction (EF = SV/EDV) used in clinical
practice• increase contractility assumed with increase EF
with Ca, NE, digitalis, exercise; with [K]o, [Na]o

↑ Contractility related to : beta-sympathetic adrenergic nerves
catecholamines: epinephrine norepinephrine
drugs: digitalissympathomimetics
↓ Contractility related to:loss of contractile mass - myocardial Infarction
myocardial muscle disease - cardiomyopathy
drugs: anesthetics, barbiturates
Influences on Myocardial Contractility

• Arteriovenous Oxygen Difference (AVO2D) the difference in oxygen content between arterial and venous blood
• measured in ml% - ml O2 / 100 ml blood
• Oxygen Consumption (VO2) - the rate at which oxygen can be used in energy production and metabolism
• “absolute” measures: L / min , ml / min• “relative measures: ml / kg body wt. / min• Fick equation: VO2 = Q X AVO2D
• Maximum Oxygen Consumption (VO2max) maximum rate at which a person can take in and utilize oxygen to create usable energy
• defined as plateau of consumption rate increase• often estimated with VO2peak
• Myocardial Oxygen Consumption VO2 of the heart muscle (myocardium)• "estimated" by RPP: HR X SBP
• Functional Aerobic Impairment:predicted VO2max - attained VO2max
predicted VO2max
mild 27% - 40%moderate 41% - 54%marked 55% - 68%severe > 69%
Definitions

• Systolic Blood Pressure (SBP) pressure measured in brachial artery during systole (ventricular emptying and ventricular contraction period)
• Diastolic Blood Pressure (DBP) pressure measured in brachial artery during diastole (ventricular filling and ventricular
relaxation)
• Mean Arterial Pressure (MAP) "average" pressure throughout the cardiac cycle against the walls of the proximal systemic
arteries (aorta)• estimated as: .33(SBP - DBP) + DBP
• Total Peripheral Resistance (TPR) - the sum of all forces that oppose blood flow
• length of vasculature (L)
• blood viscosity (V)
• hydrostatic pressure (P)
• vessel radius (r)
Definitions
TPR = ( 8 ) ( V ) ( L )
() ( r 4 )

Cardiovascular Hemodynamic Basics
Flow (Q) Pressure (MAP) P aorta – P vena cava
= = Resistance (TPR) (8) (V) (L)
() (r 4)
Flow (Q) = () (Pa – Pv) (r 4)
(8) (V) (L)
V = viscosity of fluid (blood) flowing through the pipe L = length of pipe (blood vessel) r = radius of the pipe (blood vessel) Pa = aortic pressure Pv = venous pressure
Normally Resting Q is about 5 - 6 liters / minute

Lungs
Brain
Veins (Flexible Compliant “Pipes”)
Arteries (Stiff Inflexible “Pipes”)
Liver
Stomach
Pancreas
Intestines
Kidneys
Skin
Muscle
Arterioles
Precapillary Sphincters
The Systemic Circulation

Smooth Muscle Arteriole
Anastomosis (Shunt)
Precapillary Sphincter
True Capillary With Single
Layer of Endothelium
Metarteriole
Venule
Microcirculatory Anatomy

Left Ventricular Pressure
(mmHg)
Volume (ml)
120
6
40 140
Effects of an Increase in Preload on Left Ventricular Pressure Volume Loop
↑ EDV↑ EDP
↑ Ejection Pressure
↑ SV

Left Ventricular Pressure
(mmHg)
Volume (ml)
120
6
40 140
Effects of an Increase in Afterload on Left Ventricular Pressure Volume Loop
↑ ESV↑ ESP
↓ SV

Mechanism of Control of Cardiovascular and
Respiratory Systems

Sites of Cardiorespiratory
Control



Stroke Volume – regulated by Frank Starling mechanism
• ↑ venous return → ↑ EDV → ↑ stroke volume
Cardiac Output (Q) – main determinant: body O2 needs
• Autoregulated by intrinsic changes in preload, & SV
•↑ afterload → initial ↓ in Q → ↑ EDV → ↑ SV back to normal
•↑ venous return → ↑ preload → ↑ SV
• Autoregulated by extrinsic hormonal influences• Norepinephrine release → ↑ HR and SV
Cardiorespiratory Control

Cardiorespiratory ControlExercise Systemic Blood Flow: Autonomic influences
Sympathetic outflow & circulating catecholamines• activation → vasoconstriction in non - exercising tissue
• Approximate redistribution of blood flow during maximal exercise• NC in brain blood flow 500 ml/min ↑ to heart
• 11,300 ml/min ↑ to muscle 400 ml/min ↑ to skin
• 500 ml/min ↓ to kidneys 800 ml/min ↓ to viscera
• 200 ml/min ↓ to various other parts of the body
Rest Max Exercise

Acute Cardiorespiratory Responses to Endurance
Exercise

Acute Responses to Aerobic Exercise• Heart Rate
• ↑ up to 3 times resting value at peak exercise (↓ time spent in diastole)
• Oxygen Consumption (VO2)
• Expressed in both relative and absolute terms
• Relative: ml O2/kg/min Absolute: ml/min or L/min
• average VO2max for 40 year old male 37 ml/kg/min
• Resting metabolic equivalent = 1 MET = 3.5 ml/kg/min
• Oxygen consumption linked to caloric expenditure (1 liter of O2 consumed = 5 kcal)
180
160
140
100
HeartRate
1.0 2.0 3.0Oxygen Uptake (L / min)
50 150 250
Workloads (Watts)
HR – VO2
relationship is
linear until about
90% VO2max

• Cardiac Output (Q)• ↑ up to 4 times resting value at peak exercise (↑ is rapid at onset, then levels off)• ↑ Q → ↑ venous return
• Venous return mediated by and related to:• sympathetic venoconstriction• muscle pump• ↑ inspiration → ↓ thoracic pressure
• blood flows to an area of reduced pressure• ↑ inspiration → ↑ abdominal pressure
• contraction of abdominal muscles • squeezing of abdominal veins
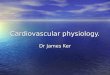
• Stroke Volume• ↑ up to 1.5 resting value at peak exercise
• increase levels off at 40% - 50% VO2 max
• ↑ in venous return → ↑ EDV (Starling mechanism)• ↓ ESV eluding to an ↑ in myocardial contractility• ↑ ejection fraction: rest: 58% max exercise: 83%
StrokeVolume(ml/beat
120
110
70
25% 50% 75%
Percentage of VO2 max
Acute Responses to Aerobic Exercise

• Arteriovenous oxygen difference• Difference in [O2] between arterial and mixed venous blood
• Illustrated by the oxyhemoglobin desaturation curve• ↑ approximately 3 fold from rest to max exercise• at rest, about 25% of arterial O2 is extracted
• at peak exercise 85% of arterial O2 is extracted
• Blood Pressures and Resistance to Flow• SBP: ↑ - failure to ↑ signifies heart failure• DBP: slight ↑ or slight ↓ or NC• MAP: slight ↑ • TPR: ↓ - mainly due to vasodilation in exercising muscle
• Coronary (Myocardial) Blood Flow• 4.5% of Q goes to myocardium at rest and at peak exercise
• this increase is due to ↑ MAP and CA vasodilation
• Blood Flow to the Skin• ↑ as exercise duration ↑ to allow for heat dissipation• ↓ at max exercise to meet exercising muscle demands
• ↑ during exercise recovery, again for heat dissipation
Acute Responses to Aerobic Exercise

• Minute Ventilation• resting average: 6 Liters/min• peak exercise average: 175 Liters/min• respiratory rate: resting 12-18 peak exercise: 45-60• tidal volume: resting .5 liters peak exercise: 2.25 Liters
• Plasma Volume• blood plasma ↑ in the interstitum of exercising muscle• fluid shift results in a 5% ↑ in the hemoconcentration• blood viscosity increases
Acute Responses to Aerobic Exercise

Untrained or people with certain cardiorespiratory diseases will have larger DEBTS and DEFICITS
Oxygen DEBT & Oxygen DEFICIT
Oxygen Debt(EPEOC)
Oxygen Deficit“Steady State”VO2
VO2
Rest
Onset TerminationEXERCISE TIME
Oxygen Debt and Deficit
Oxygen Deficit due to:
• delay in time for aerobic ATP production to supply energy
Oxygen Debt due to:
• resynthesis of high energy phosphates (CP, ATP)
• replace oxygen stores
• lactate conversion to glucose (gluconeogenesis)
• ↑ HR, respiration, catecholamines, body temperature

V O 2
VCO 2VO 2
V E
HCO 3-
pH
m ax
P CO P COA 2 a 2&
P Oa 2
P OA 2
Increasing workload
OBLA Respiratory Compensation(hyperventilation)
No Change inVE
VCO2
Ventilatory and Metabolic Changes During
Exercise

Training Adaptations to Chronic Endurance
Exercise

RestingNC ↓ NC
VO2 = HR x SV x AVO2diff
due to: due to: ↑ time in diastole ↑ preload
↓ afterload↑ ventricle size↑ blood volume
Submax Workload (measured at same pre-training workload)
NC NC VO2 = HR x SV x AVO2diff
note: a ↓ in afterload (mentioned above) accompanied by a ↓ in HR response translates into
a ↓ myocardial VO2 at rest or at any workload
Max Workload (measured at peak exercise) NC
VO2 = HR x SV x AVO2diff
some studies show a slight decrease
Effects of Exercise Training on the Components of the Fick Relationship
↑↑

• Mean Arterial Pressure• NC at rest or during exercise
• Systolic and Diastolic Blood Pressure• usually NC at rest or during exercise• possible ↓ at submaximal workload• may ↓ at rest in borderline hypertensives
• some studies report a mean ↓ of about 9 mmHg
• Total Peripheral Resistance and Afterload• ↑ capillarization (more parallel circuits) → ↓ TPR• ↓ TPR → ↓ Afterload (slight – not of major significance)
• Respiratory Variables• Respiratory Rate
• Rest: NC• Submax exercise: d• Max exercise: slight ↑
• Tidal Volume• Rest: NC• Submax exercise: NC or slight ↑ • Max exercise: slight ↑
• Anaerobic Threshold• Occurs at a higher percentage of VO2 max• Pre-training: 50% VO2max Post-training: 80% VO2max
Training Adaptations

• Mitochondria• ↑ number, size and membrane surface area
• Aerobic Enzymes in Exercising Muscle• ↑ Krebs cycle enzymes (succinate dehydrogenase)• ↑ oxidation enzymes (carnitine acyltransferase)• ↑ electron transport enzymes (cytochrome oxidase)
• Fatty Acid & Glycogen Utilization• ↑ utilization of oxidative pathways to produce ATP• Called the “glycogen sparring” effect• ↓ RER for any given submaximal workload• ↑ muscle glycogen stores (with high carbohydrate diet)
• ↓ Platelet Aggregation
• ↑ Fibrinolytic Activity
• ↓ Circulating Catecholamines• ↑ vagal tone → ↓ risk of arrhythmia
• No Appreciable Change in Resting Metabolic Rate• Exception: training induced ↑ in lean muscle mass
• Resistance to Pathological Events• smaller infarct size and quicker recovery• Less of a ↓ →in ventricular function during ischemia
Training Adaptations

75
185
60
185
0
50
100
150
200
sedentary-rest sedentary-max trained-rest trained-max
"Average" Values for Sedentary and Trained Individuals
Heart Rate( beats / minute )

Stroke Volume( ml / beat )
"Average" Values for Sedentary and Trained Individuals
60
120
80
160
0
50
100
150
sedentary-rest sedentary-max trained-rest trained-max

Cardiac Output( liters / minute)
"Average" Values for Sedentary and Trained Individuals
5
22
5
30
05
10152025303540
sedentary-rest sedentary-max trained-rest trained-max

A-V O2 Difference( ml%)
"Average" Values for Sedentary and Trained Individuals
6
14
6
16
0
5
10
15
20
sedentary-rest sedentary-max trained-rest trained-max

Oxygen Consumption( liters / minute)
"Average" Values for Sedentary and Trained Individuals
0.25
3
0.25
4.5
0
1
2
3
4
5
6
sedentary-rest sedentary-max trained-rest trained-max

"Average" Values for Sedentary and Trained Individuals
3.5
38
3.5
55
0
10
20
30
40
50
60
sedentary-rest sedentary-max trained-rest trained-max
Oxygen Consumption( ml / kg / minute)

"Average" Values for Sedentary and Trained Individuals
134
210
130
206
0
50
100
150
200
sedentary-rest sedentary-max trained-rest trained-max
Systolic Blood Pressure( mm Hg)

"Average" Values for Sedentary and Trained Individuals
8284
80
82
747678808284868890
sedentary-rest sedentary-max trained-rest trained-max
Diastolic Blood Pressure( mm Hg)

"Average" Values for Sedentary and Trained Individuals
6
120
6
150
0
20
40
60
80
100
120
140
160
sedentary-rest sedentary-max trained-rest trained-max
Minute Ventilation( liters / minute)