Embed Size (px)
Citation preview

Clinical Brain Imaging
Stephen Salloway, M.D., M.S.Department of Clinical Neurosciences and
PsychiatryBrown Medical School

Nobel Prize for Medicine 2003
Paul C. Lauterbur Sir Peter Mansfield

Objectives
• Learn about the use of CT, MRI and SPECT scanning in clinical practice
• Recognize key anatomical landmarks and begin to recognize and describe the appearance of common disorders
Please look at the scans on your patients.


Neanderthal Homo Sapiens


CT vs. MRI
Wide doughnutOpening
10-20 minutesLength
Adjust windowTechnique
AxialPlane
$330Cost
Bright Bone
Long, narrow
30-60 min
T1, T2, Pd
3-D
$900
Dark
Magnetic fldX-ray beamObtained
MRICT

Advantages to CT
• Costs less than MRI
• Better access
• Shows up acute bleed
• A good quick screen
• Good visualization of bony structures and calcified lesions

Disadvantages to CT
• Resolution• Beam-hardening artifact• Limited views of the posterior fossa and
poor visualization of white-matter disease



Advantages to MRI• Good resolution—excellent view of brain
structure
• 3 dimensions
• Good gray-white differentiation
• Adjust settings based on characteristics of the lesion
• Good view of the posterior fossa

Advantages to MRI
• No radiation exposure
• Gadolinium contrast is relatively nontoxic
• Capacity for quantitative imaging, 3-D reconstruction, angiography, spectroscopy

Disadvantages of MRI
• Cost
• Some patients ineligible because of pacemakers, other metal
• Claustrophobia
• Long exam
• Access





FLAIR Image

MRI Is the Test of Choice for Evaluating
• Most lesions causing epilepsy—temporal lobe glioma, mesial temporal sclerosis
• White-matter disease—subcortical dementia, HIV, MS
• Lesions in the posterior fossa
• TBI—axonal injury
• Extent of anoxic injury, herpes encephalitis
• Frontal atrophy, NPH
• Other—brain anomalies, SLE, vasculitis, sagittal sinus thrombosis, pituitary lesions, AVM

What Is Bright on CT?• Blood• Contrast• Bone• Calcium• Metal
What Is Dark on CT?
•Air
•CSF/H20

Artifacts
• Beam hardening
• Bone
• Foreign body
• Motion






Uses for SPECT and PET
• Acute stroke
• Identify a seizure focus-increased flow during sz and decreased interictal flow
• Dementia-frontal pattern in FTLD, temporo-parietal pattern in AD
• Ligand imaging in PD, others






Landmarks• Axial views
– Fourth ventricle– Petrous bone and sphenoid ridge– Aqueduct– Third ventricle– Lateral ventricles– Frontal horns– Calcifications in the choroid plexus, pineal,
basal ganglia and falx– Caudate, putamen and globus pallidus

Landmarks (Cont.)
– Internal capsule—anterior and posterior limbs– Thalami– Sylvian fissures
• Sagittal views– Severity of cortical atrophy– Corpus callosum and cingulate gyrus
• Pituitary– Coronal views– Hippocampus and amygdala




• 65 year old man with right carotid occlusion, left hemiparesis, apathy, and depression. What is wrong with his scan?

72 year old woman with gradually progressive memory loss and word finding difficulty. Can you find the Sylvian fissures? What is wrong with this scan?


NormalHippo-campus

Atrophic
Hippo-campusin AD
62 year old woman with rapid progression of memory loss

Mesial Temporal Sclerosis
31 year old woman from Africa with frequent complex partial seizures and mild developmental delay. Can you find the hippocampi? What is wrong with her scan?

Introduction to Scan Interpretation
• Is the scan
– Contrast or noncontrast?
– Good quality?
• Describe the abnormality
– Size—small, punctuate, medium, large
– Shape—round, well circumscribed, ovoid, irregular, patchy

Introduction to Scan Interpretation (Cont.)
• Signal intensity– High signal, hyperdense– Low signal, hypodense– Isointense, isodense– Mixed signal
• Location


Which scan is a normal variant? What is the abnormality on the other scan?

3 year old boy with mild developmental delay.What does this scan show?

65 year old with dizziness, mild hearing loss, and mild tinnitus on the left. Can you detect the subtle abnormality on this scan?


66 year old admitted to the hospital with the abrupt onset of expressive aphasia and mild right hand weakness. Describe the abnormality on the CT on hospital day 2.

55 year old with new onset of seizure discovered to have a small bleed from a communicating artery aneurysm. Describe the abnormality on the CT 2 days post-op aneurysm surgery.

45 year old with left subclavian occlusion developed Wernicke’s aphasia following a revascularization procedure. Describe the abnormality on the MRI 7 days after the surgery.

50 year old with new onset seizure. What does the contrast enhanced CT show?

A 32 year old woman with anticardiolipin antibody syndrome on coumadin for stroke prophylaxis was admitted to the hospital for confusion. What does her admission CT scan show?

30 year old IV drug abuser admitted to the hospital with headache, confusion, and fever. What does the contrast CT scan show? How many different types of abnormal signal do you see?

30 year old woman with right sided numbnessfor 2 weeks. MRI on left is non-contrast, MRI on right is enhanced with gadolinium. Describe the abnormalities. What is the most likely diagnosis?

72 year old man with
short-term memory loss
and trouble recalling
people’s names. He is
driving without difficulty
and works out at the gym 3 times per week. What does the MRI show?

Vascular DementiaThree types of vascular dementia
Multiple large Vessel infarctions
Bilateral strategic thalamic infarcts
Binswanger’s Disease

Normal Pressure Hydrocephalus: NPH
• Cognitive Impairment• Gait Disturbance• Bladder Control• May Have:
Behavior Problems
Parkinsonism

MRI findings
• Ventricular enlargement disproportionate to the amount of atrophy• Bowing of the corpus callosum• Smooth rimming of high signal around the ventricles due to
transependymal flow of CSF

NPH: pre-opNPH: pre-op NPH: post-op-130 NPH: post-op-130 mm H2Omm H2O


Types of fMRI• BOLD-fMRI which measures regional differences in oxygenated blood• Diffusion-weighted fMRI which measures random movement of water molecules. Diffusion
tensor imaging (DTI) measures diffusion of water in different directions and is a good test for studying white matter tracts.
• MRI spectroscopy which can measure certain cerebral metabolites non-invasively


DTI reconstruction of the corpus callosum

3D reconstruction with functional
overlay
fMRI:Visual stimulation

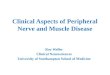
MR Spectroscopy
MR spectroscopy of N acetyl aspartate (NAA) showing decline of NAA over time in patients with Alzheimer’s disease (lower line) compared to age-matched controls.

QuestionsThe best initial test for the following is:
1) Routine screen for dementia2) Rule out multiple sclerosis3) Acute subdural hematoma4) Closed head injury with personality change5) Fever and delirium in an HIV + patient
a. CT without contrast b. MRI without contrastc. CT with and without d. MRI with and without

Questions
6. Which of the following is not bright on CT?a. Bone b. Acute blood c. CSFd. Contrast e. Metal
7. MRI is the best test for evaluating all of the following excepta. Lesions in the posterior fossab. Calcified lesions at the base of the skullc. Small lesions in the temporal lobed. Multiple sclerosis plaquese. Herpes encephalitis

Answers
1. A 2. B 3. A 4. B
5. D 6. C 7. B