-
i${i,t'#/q#rBrit. J. Ophthal. GgZ6) 6o, r35
Clinical assessment of rhodopsin in the eyeUsing a standard
fundus camera and a photographic technique
U. B. SHEOREYFrom the Department of Visual Science, Institute of
Ophthalrnology, London
In recent years, the technique of fundus reflecto-metry (see
Weale, tg74), has been shown to beparticularly helpful in locating
defects in the pri-mary stage of the transduction of light into
vision.It has thus been possible to assess the availabilityof
retinal pigment in cases such as night blindness.When the results
are considered together with thosefrom colnplementary
electrophysiological or psycho-physical tests, a much clearer
diagnosis concerningthe site of the lesion is possible. The basis
of themeasurement is the marked change in the absorp-tion spectrum
of the visual pigment rhodopsinwhen it is bleached by strong
exposure to light.Thus if a defined part of the retina is
bleached-that is, an imprint or an 'optogram' is formed onthe
retina-a comparison of the reflectances of theunexposed and exposed
areas can be used as anindicator of the availability of pigment in
thatregion. The measurement can be carried outonly for a double
transit of light through theretinal layer provided that the
bleaching of theeye has affected only the retinal pigment.
In most previous clinical studies, complexapparatus r,vas used
and the procedure was involved.We have been able to use a simple
procedure and aconventional fundus camera, albeit slightly
modi-fied. The use of a standard fundus camera and aflash bleaching
technique has obvious clinicaladvantages-for example, the
co-operation re-quired of the patient is minimal. These
modifica-tions are described in this paper and the use of
thistechnique in assessing the pigment concentrationin rod rich
parts of the retina is illustrated. Thesemodifications were
designed so that they couldeither be easily removed from the light
path in thecamera or left in place provided they did nothinder the
original application of the camera. Asvery little machining is
required on the main bodyof the apparatus, its absence from the
clinic isshort. An approximate assessment of the densitycontrast of
the optogram can be made immediatelyafter developing and fixing the
latent image on thephotonegative. A value for the density
contrastAddress for reprints: U. B. Sheorey, Department of Visual
Science,Institute of Ophthalmology, Judd Street, London WCIH
qQS
can be obtained later by means of a microdensito-meter. The
modified apparatus thus provides asimple procedure for routine and
rapid clinicalassessment of rhodopsin in the eye.
MethodThe spectral absorption of the visual pigment is
differentfor the bleached and the unbleached states' and
theintensity of the light beam which has traversed throughthe
retinal layer containing the pigment will be modifiedaccordingly.
We may compare the intensities eitherfrom two adjacent areas' one
of which is bleached, orfrom a given area before and after it is
bleached. Ifthisdifference is due orly to a change in the retinal
pigrnent,we can relate the changes in the concentration of
thatpigment to changes in optical densities. The change inoptical
density is a function of the wavelength of lightused for the
measurement; it is largest in bluish-greenlight for the rod
pigment.
The present method uses a photographic techniqueto record this
difference from adjacent areas of theretina after a defined part of
the retina has been bleached.In order to relate the recorded
density differences totrue differences, the photonegative also
carries a cali-bration which is superimposed at the same time asthe
recording. Thus, distortions which may be intro-duced during the
process of the development of thelatent image on the film can be
compensated (Arnold,Rolls, and Stewart, ry7t).
APPARATUS
The basic apparatus consists of a standard Zeiss*fundus camera
and its associated electronic powersupply unit for the xenon flash
tube. The paths ofthe light beams which are used to provide
theretinal illumination for general viewing, flashbleaching, and
photography are unfortunatelylargely common. In order to produce an
optogramby bleaching a defined part of the retina, an aper-ture in
this light path is required, but it has to beremoved for general
viewing of the fundus andduring photography.
These modifications are illustrated schematicallyin Fig. r. The
original tubular holder which sup-ports the objective lens L is
replaced by a modified*C. Zeiss, Oberkochen, Germany
-
L- ...sk,
136 British Journal of Ophthalmology
housing. The axial length of the housing and themechanical
dimensions at both its ends are exactlythe same as for the original
tube so that the twocan be interchanged. The housing accommodatesa
moveable carriage which in turn accommodatesan aperture-plate. The
apertures can be movedalong the optical axis by rotation of the
shaft S, sothat they can be made conjugate with the
patient'sretina. Either aperture may be brought into thelight path
by means of the knob Kr. A shieldedpress-switch, Sw, is mounted at
the end of K, toactivate the xenon flash B, for retinal
bleaching.This switch is wired electrically in parallel withthat on
the mechanical shutter of the 35 mmcamera. This duplication of the
switch is desirableto enable the flash to be activated
independentlyof the camera and to reduce the number of
handmovements by the operator during the procedure.
The aperture-plate P carries two apertures, A,for normal viewing
of the retina and for photo-graphy, and 42 for defining the retinal
area that is tobe bleached (Fig. rc). The plate is mounted
perpen-dicular to the optical axis of the fundus camera andin the
moveable carriage. Both apertures are madefrom thin sheets of brass
and can easily be removedand exchanged for other shapes and
sizes-forexample, as might be required for the investigationof the
density of the retinal pigment along thevertical meridian. The
aperture A, is currentlyz8 mm diameter, equivalent to a retinal
view of35'. Access to these apertures may be obtainedsimply by
removing the lens L. All internal sur-faces of this housing and the
additional componentswhich are mounted in the fundus camera
arepainted matt-black so as to prevent stray reflectionswithin the
camera reaching the patient's eye or therecording camera.
F1 is the deep-red colour filter that is requiredin the path of
the white light from the bulb B, toprovide a safelight for retinal
viewing. It is con-structed from a sheet of coloured gelatine
(Ilford,no. 6o8) which is clamped between two thin platesof glass
and held rvithin a metal plate. A rectangularslot is required in
the side panel of the apparatusfor the insertion or removal of the
filter from thelight path. Note that F, does not need to be
handledsince it does not interfere with either the bleachingor the
recording steps. Two miniature light-emitting diodes* are also
provided within thehousing as additional fixation targets. These
diodesare required because the patient cannot see theinternal
target T once the aperture A1 is changedto A, if his centre of
fixation is outside the areadefined by Ar. Furthermore, since the
paths of theviewing and the bleaching lights are largely com-mon, T
is not illuminated when the bluish-greenfilter is introduced into
the light path before*Motorola, type MLED zo
photography. Few people, however, have anydifficulty in
maintaining fixation during the briefinterval required to introduce
the bluish-greenfilter and photograph the optogram.
The safelight path is combined with the path ofthe xenon flash
light by means of the half-mirrorBS. In order to remove the
infrared content ofthe intense xenon-flash, BS was remade from
apiece of heat-absorbent glass. The bluish-greencolour filter F,
which is required during therecording of the optogram, is placed in
the lightpath after BS. The rest position of this filter isout of
the light path as it is manually pushedinto place immediately
before photography andthen retracted. Within the same mount,
neutral-density filters may also be incorporated so as toadjust the
retinal illumination independently ofthe power supply to the flash
tube. It is therebypossible to achieve a common setting for
bleachingand photography, thus considerably simplifyingthe
procedure and avoiding waiting for the elec-tronic power supply to
discharge and rechargebetween changes in settings.
The calibration is superimposed on the film byplacing a
density-graticule DG in the recessbetween the film and the
mechanical shutter of thecamera; therefore, it is only in the path
of thelight reflected from the fundus. A typical graticuleis
illustrated in Fig. fi. The part of the film onwhich the fundus
image is recorded is indicatedby the broken circle; the inner
rectangle indicatesthe position of the optogram image relative to
thegraticule and one frame of the film. The graticulesare made by
exposing a series of strips-for ex-ample, (zo mm long, z mm wide,
spaced z rrrrnapart) on to photographic paper*. For present use,the
exposure time was simply varied in steps duringa trial run and then
the appropriate exposure timeswere selected so as to produce strips
of opticaldensities in the range o'o5-o'r5. The position, size,and
orientation of these calibration steps are deter-mined by the
particular densitometric investigationthat one wishes to perform.
For example, for in-vestigations of the changes in the pigment
con-centration along the vertical meridian, it would beuseful to
orientate these strips horizontally-that is,perpendicular to the
bleaching rectangle. It isessential that an adequate calibration is
recorded onthe same film in the vicinity of the region of
interest.
CALIBRATION OF THE FLASH SOURCE
The flux incident upon the patient's retina duringthe flash
bleaching and photographic steps wascalculated from the radiometric
measurementswhich were taken on the xenon .lish. To do so,a model
eye was formed in front ;f lens L and a*Ilford N+ESo
-
sfl.}..' Clinical assessment of rhodopsin in the eye r37
(c )
FIG. r (a) Schematic side aiew of Zeiss fundus camerashozuing
princip al c omp onent s and mo difi c ations'Tubular housing at
front houses objectiue lens L, andmoaeable holder for aperture
plate P. Also shown are :adjustable, internal fixation target T;
mirrors M;combined heat-filter and beam-splitter BS; filter F2for
photographic step ; heat-absorbent filter HF;deep-red filter Fr;
white zsiewing light Bt; xenon flashtube B2; calibration graticule
DG1' camera shutter S;additionat fixation target, LED' Cylindrical
assembly toteft of lens L is model eye used to measure flux
arriuingat simulated retinal plane. During use, assembly is
pushedoaer mounting tube of lens L and distances are fixedby
spacing rings Sp. Output of photodetector D is fedinto ampffier A
for measurements
(b) Schematic plan of modified fundus camerashowing additional
fixation targets LEDs and aariouscontrol knobs and shafts. Rotation
of Krmoaes plateholder P along optical axis for focus
adiustments.Bleaching aperture is brought into light path by
pullingK2 outwards. Flash can be actiaated by szuitch Sw.This is
electrically connected to be in parallel withthat on shutter
release switch of camera
(c) Front uiew of aperture plate holder P whichcarries tzpo
apertures, A1 for normal aiewing of fundusand A2 for bleaching a
defined area of fundus
(d) Schematic illustration of density-graticule DGu:hich is
placed be4uteen the shutter of camera andfilm so as to impress a
calibration on film duringphotography. B.tken line circle,
corresponding toaperture A1, indilates area within zuhich retinal
imageis formed. Inner rectangular region is area, correspondingto
A2, within which optograrn is present
photodiode was placed within it. This assembly isshown in Fig.
ta to the left of the objective lens L.The lens of the model eye
had a focal length ofr7 mm and an aperture of 8 mm diameter.
Anobjective radiometric method using a photodiodewas used in
preference to a photometric methodusing an eye because it is easier
and more preciseto use routinely in the clinic. The difficulty
inmaking routine photometric measurements by eyewith this fundus
camera should be noted' Theflash source is imaged in the pupil
plane of theobserver's eye; this image is not uniform and isalmost
as large as a fully dilated pupil. Furthermore,the output flux of
the flash varies according to theinterval between firings and the
age of the tube'
The waveform of the xenon flash (measured at1:5oS nm) consisted
of a fast rising front ofabout-o'r ms (measured from 5 per cent of
peakto the peak) followed by an exponential decay with
acharacleristic decay time of about o'4 ms (from thepeak to r/e of
the peak, where e: 2'72).For photo-graphy of the optogram, the
spectral distribution andLt"nsity are defined by the transmittances
of theocular media, the filters, and the optical
componentsr,r,'ithin the fundus camera. The retinal energydensity
during photography is calculated to be7 Jm-' when using setting no.
+ on the flashcontrol unit and filters Fr*Htrr* zElo'+ ND'
Theocular transmittance has been taken as 7 5 percent for this
calculation; details of this measure-ment and the calculation are
given in the Appendix'
For the bleach, F2 and the neutral-densityfilters are removed
from the light path. The increasein the spectral bandwidth and
transmittanceresults in an actinic retinal energy density which
isexpressed by Te x 9oo Jm-', where Te is thetransmittance of the
ocular media. Details of thesecalculations are also given in the
Appendix' Takinga mean value of T":6o per cent over the
spectralrange 43o-63o nm, the bleaching flash is estimatedto
pto"iae an actinic retinal energy density of
05'4X ro" Jm ".- In previous studies on fundus densitometry,the
retinal fluxes have been specified in photo-metric units. These may
be related to the valuesgiven above by means of the following:
r (scotopic) troland second: r'or X ro-* Jm-',for ).:5o5 nm and
a pupil diameter of 8 mm'Thus, while the value given above for
photographycompares well with the value of 4X roa troland swhich
was used by Highman and Weale (rg7Z),the bleaching flash currently
used is about threetimes less intense than their figure of r'8zX
ro7troland s. The relationship between the fraction ofpigrnent
bleached and the retinal illuminance(pig. g, Ripps and Weale, ry6g)
indicates that thepresent flash will bleach about 55 per cent of
thepigment. Thus, if the maximum optical density
(o)
-;;;:)'1r',,'.t,t'jt:')' I| !:iL.:;: I
(d)A2
Sw
K, --l
-
r38 British Journal of Ophthalmology
difference that can be achieved in the eyes ofnormal subjects is
taken to be o.16-o.18 D, wemay expect to measure a density
difference ofo'og-o'ro D in these subjects with the
presentequipment.
The alignment and focus adjustment of thecamera were carried out
by using the red filterF. in the path of the white light from the
bulb Br.On setting z of the Zeiss power supply the
retinalillumination was calculated to be 35o troland. Theluminance
of the image of the source formed in thepupil of the model eye was
measured by meansof a photometer*. The luminances of the
additionalLED fixation targets were adjusted by varyingtheir input
power so that they appeared to havethe same luminosity as the
surrounding field. Thepower spectrum of these LEDs is negligible
atwavelengths shorter than 63o nm and their emissionis confined to
a narrow band in the deep red partof the spectrum.
ProcedureThe patient is seated at the fundus camera in a
darkenedexamination room. The pupil must have been fully dilatedand
dark adaptation allowed to proceed for at least r 5 minbefore this.
The plane of the film and the apertures areadjusted rapidly so as
to be in focus with the retina.Since it is difficult for the
operator to see much retinaldetail in the dim red light, it is
helpful to begin theadjustments while viewing the region around the
opticdisc which has a larger reflectance and is rich in struc-ture.
Note that a slight re-adjustment will be necessaryto view different
parts of the fundus but no correctionfor chromatic aberration is
required. The requiredretinal area is then brought into the centre
of the fieldof view with the moveable internal fixation target or
oneof the LED targets and the focus checked. A retinalarea in which
there are relatively few blood vesselsshould be selected as far as
possible, so that the tracesrecorded by the scanning densitometer
are smooth andthus easier to analyse. The aperture A2 is brought
intothe optical path by pulling the shaft Sz, the xenon flashis
activated by means of the switch Sw, and the shaftis pushed back;
this completes the bleaching step.If the eye is still correctly
placed, the filter F2 is pushedinto the light path, the retina is
photographed, and F2is pulled back to its resting position. The
camerashutter is set nominally to rfz5 s. The film is thenadvanced
by one frame so that the camera is ready foranother photograph or
the next sequence. A readilyavailable sensitive filmt is used for
this reading. Thefilm is processed in complete darkness and
accordingto the manufacturer's instructions.
Careful alignment of the patient's eye to the apparatusis
particularly important in this technique, because it isessential to
transmit all of the available flux into thepatient's eye for
bleaching. During photography, thespurious reflections and scatter
from the eye that canso easily mask the image of the optogram, must
be*Model 4oA, made by UDT Inc, California, USAtKodak z+Zs
avoided. Note that with the subject's fixation on theperiphery
of the apertures A, or Ar, the pupil willappear to be elliptical as
viewed along the optical axisof the apparatus. Thus there is a
reduced margin forthe transverse alignment of the image of the
light source,formed in the subject's pupil. A misalignment
u'ouldmean that a part of the beam would be occluded andthis could
cause a serious reduction in the retinalillumination. For a given
patient, the focus and thefixation target require little, if any,
adjustments onrecalling the patient after a period of rest or
furtherdark-adaptation. In order to ensure accurate fixationduring
the course of this procedure, the fixation targetshould be
presented to the same eye as that used forrecording the
optogram.
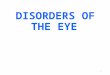
Results and the analysis of the optogramA positive print of a
typical retinal photographtaken with this modified fundus camera is
shownin Fig. z. This was recorded from a subject inrvhom
dark-adaptation and vision were normal.The rectangular optogram can
be clearly seen inthe centre of this photograph as an area of
loweroptical density. This area is crossed by the regularlyspaced
stripes caused by superimposition of thedensity graticule. It is
important to note that theoptical densities are reversed during the
process ofthis photographic printing-that is, the bleachedarea in
reality reflects more bluish-green lightthan the surrounding
unbleached region so thatit is more dense on the photonegative. The
aper-ture A, used for bleaching was centred about r5'temporal to
the fovea, along the horizontal meridian.The backs of the two LED
fixation targets which
FIG. 2 A positiae photographic print cf typicaloptogram recorded
from normal fundus. Subject'spoint of fixation is marked by LED
target at left edge
-
#,"$/
are provided within the lens housing can also beseen; the
subject's fixation is marked by the illu-minated LED target at the
left of the photograph.
In order to obtain quantitative results from thefundus
photograph, the photonegative has to bescanned in a
microdensitometer; a double-beamrecording microdensitometer* was
used for thepresent work. The displacement of the trace-recorder,
due to a change in the optical transmit-tance of the scanned
sample, has to be initiallycalibrated; this u'as done by
introducing knownvalues of neutral-density filters in the path of
themeasurement beam. Then, using common experi-mental conditions
for both measurements-forexample, the same spot size and scan
rate-thedensity-graticule and the photonegative are scannedin turn.
The difference between the scans takenthrough the bleached area and
the adjacent un-bleached area is proportional to the true
opticaldensitlr difference. The proportionality constantis the
transfer characteristic of the particular partof the film (Arnold
and others, rgTr). For a givenregion of the film if the step change
due to thesuperimposed densit-v graticule is the same forboth
scans, then this constant is unity. Thusdeviations from unity can
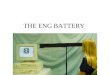
be noted and the resultsscaled accordingly. The procedure can best
beillustrated by referring to Fig. 3 which shorrys thetraces
(corresponding to the scans taken throughthe sections indicated in
Fig. z). The traces aredrawn about a datum line which is taken to
be thebase or fog level of the film. A scan of the
particulardensity graticule which was used for this photo-graph-is
also shown in Fig. 3. Note, however, thatthis third trace has been
drawn inverted so as toillustrate the point that the exposure
received bythe film r,vhich lies under the calibration strips
isreduced. This local reduction of exposure can alsobe seen in the
other two traces which are pulleddown towards the datum in the
regions containingthe calibration strips. The calibration for the
grati-cule is indicated in the centre of this figure. Thetransfer
characteristic of this photonegative can'be*Model 3c, made by
Joyce-Loebl Ltd
Clinical assessment of rhodopsin in the eye r39
seen to be slightly above unity. The density contrastof the
optogram formed in central part of thisphotograph-that i., t5-2o"
temporal-is abouto'r D. The density difference can be
determinedmore easily, in practice, when all three traces
areavailable on sparate sheets of transparent graphpaper. The
sheets containing the scans taken out-side and through the bleached
region are thenviewed against the sheet for the graticule.
Thegraticule is once again held inverted and used as atemplate.
These traces illust:ate several additional interest-ing
features. The traces are noisy and the reflectancevaries across the
retir:a. This variation is due to avariety of reasons, partly in
the instrument andpartly in the subject's eye-for example,
thepresence of blood vessels in the path of the scanor a
non-uniform retinal reflex. Note, however,that the scale of this
variaticn is either much smalleror else much larger than that due
to the modulationimpressed by the graticule on the fundus
photo-graph. Thus it is easy to discriminate between thetrue
density changes and the artefacts. The tracesalso illustrate the
variaticn cf the density differenceacross the retina. This
variation is practically zerofor the part of the retina nearer than
roo temporalto the fovea. It rises rapidly beyond this to abroad
maximum in the region r5-3o' temporal,in general agreement with the
distribution of rodsin the retina. For routine clinical
investigations,one would be interested chiefly in the
centralportion of the photograph. Thus, as indicated above,a
graticule is made so that it provides a densitystep of a value
which is of the order of the densitydifference that one expects to
measure from normalsubjects. A marked reduction in the density
differ-ence recorded in a patient's eye would thus bereadily seen
to be much smaller than this step. Thetwo outermost strips are well
outside the expectedrange. llowever, they illustrate the fact that
evenwhen the illumination on the film is reduced byo.35 density
units, an appreciable density differencecan still be recorded. This
difference can of coursebe achieved only from optograms formed in
regions
>.=
cq,-9.E.v
.o_o
FIG. 3 Trace recordings produced by scanningmicrodensitolneter.
Traces t and z are due toscans taken through corresponding sections
whichare indicated in Fig. z. Lowest trace is scan ofparticular
density graticule used to superimposecalibration. Scan has been
drazun int-terted so as toindicate that exposure of fiInt
underlying densitystrips is reduced. Ordinate represents
opticaldensity ; abscissa represents distance alonghorizontal
meridian on fundus
------!>
*!:.
-t:
-
*br4o British Journal of Ophthalmology
of the retina distal from the macula. Thus thefilm as such
appears to have an operational rangewhich encompasses the gross
variations of retinalreflex across the retina. Note also that in
thisgraticule the densities of the steps increase awayfrom the
vertical midline. Thus a graticule suchas this may be used to
photograph the optogram incorresponding regions of either eye
without requir-ing the replacement of graticules during
measure-ments on both eyes.
DiscussionThis example of the use of the modified funduscamera
was typical; a clinical study of variousretinal disorders using
this apparatus is in progressand full results will be described in
due course.Thus the comments below refer mainly to pointsof
technique. In regular use, this modified funduscamera has proved to
be no more difficult to usethan is the normal camera for routine
fundusphotography. As the method provides a rapid,convenient means
of supporting the measurementsof associated retinal tests in
diseases such as night-blindness, routine densitcmetric
measurementsmay also be carried out in the same clinic with
thisapparatus.
The maximum flux available from the presentequipment is
insufficient to bleach all the visualpigment within a given region.
The flux could beincreased but only by modification,
perhapsextensive, of the optics or the flash unit. Flowever,as
establisheJ by Highman and Weale (1973) incases such es retinitis
pigmentosa, the densitydifference; in a given retinal region are
much lower,and the vis,ral thresholds of the same retinal regionare
much higher, than those in normal subjects.Therefore, for the
assessment of such cases theapparatus may be used without any
further modifi-cations. It shculd be noted that simply
increasingthe incident flux rnay not give a markedly
denseroptogram, because short intense flashes of lightcan bleach
only up to a limit of 7o-8o per cent ofthe available pigment
because of photoregeneration(Williams, rg74. Furthermore, the
associatedheating effect of the intense retinal illuminationmay
well produce a deleterious effect-that is,oedema. The optical
effect of this oedema ispartially to counteract the density
difference dueto the bleach (Weale, r968). Its magnitude, how-ever,
is said to be independent of the wavelengthof light used for the
measurement so that it may bequantified by measurements outside the
absorptionspectrum of the pigment. In order to ascertainwhether
oedema had been caused, a series of fouror five fundus photographs
were taken in deep-red light immediately after the retina had
beenbleached and at half-min intervals subsequently.
The filter F2 was replaced by a suitable deep-redcolour filter*.
In these photographs, no densitydifference corresponding to the
bleaching aperturecould be seen in the region of the optogram.
Theexperimental conditions in the earlier fundusdensitometric
measurements were markedly dif-ferent from those used currently-for
example,Highman and Weale GgZi used a continuous ro sintense
exposure for bleaching-and thereforecomparative assessments of the
various proceduresare difficult to make. In the previous studies,
onlythe photometric effect of the bleaching light wasspecified,
whereas in the present approach, boththe actinic and the total
retinal flux densities areestimated. Thus the total flux entering
the eye canalso be calculated (see Appendix).
This apparatus cannot be used in its presentform at large
viewing angles-that is, no larger thanabout 15' in either the
vertical or the huizontalmeridians. In order to do so, the image of
theflash source which is formed in the subject's pupilwould need to
be reduced without reducing theincident flux. This reduction in the
pupillary areaas a function of the viewing angle was meajured byJay
(r96r). A smaller pupillary image wouldadditionally reduce the
variation in the retinalillumination due to the involuntary eye
movements.These are particularly noticeable in older patientsin
whom more care is required for alignment. Notethat a sli3ht
variation in the retinai illumination-for example, as a result of
ocular absorption orsmall eye movements-does not restrict the use
ofthis reflectometric method of measurement becausea differential
measurement is involved. The reduc-tion in the retinal illumination
during the bleachingstep, however, could be significant since
thedensity contrast of the optogram would be reduced.The reduction
in the flux as a result of absorption-for example, in the
lens-could be compensatedby an appropriate increase in the incident
fluxusing the data established by Said and Weale(rgSg), or by a
specific measurement in a particularcase.
SurnrnaryA technique based on the method of differentialfundus
reflectometry is used to assess the avail-ability of rhodopsin in
the eye. A defined part of thedark adapted fundus is bleached by a
short intenseflash of light. The fundus is subsequently
photo-graphed in order to record the flux reflected fromthe
bleached area, the optogram, and the surround-ing unbleached
region. This procedure requiresonly a few simple modifications to a
Zeiss funduscamera before it can be used routinelv in
theclinic.*Ilford No. 6o8
*'
dr
-
Filter
The use of the Zeiss fundus camera for fundus densito-metry was
suggested by Professor R. A. Weale whosekeen interest during the
modifications and the clinicaltrials was invaluable. The
modifications to the camerawere carried out by Mr G. Mould.
Thanks are also due to Mr P. E. Cleary for collabora-tion with
the clinical development.
AppendixMEASUREMENT AND ASSESSMENT OF THE RETINAL FLUX
The absorbances ,A.1 of the various spectral filters usedin the
procedure and for calibration were measured ina dual-beam scanning
spectrophotometer*. The resultsare tabulated below:
Clinical assessment of rhodopsin in the eye r4t
amplitude points) was less than zo ps, a value con-siderably
less than the rise-time of the xenon flash. Acapacitor of ro pFarad
was used in the feedback pathof the operational amplifier in order
to measure thetotal charge of one pulse of photocurrent.
UsingF2+HFe+zE-lr':ND filters within the light path ofthe fundus
camera and setting no. 4 on the flash controlunit, the output was
r3of 3'7 mV (mean of five flashes,ignoring the first flash). Thus
the charge accumulatedwas r'3 x ro-6 C per flash. The response
sensitivity ofthe photodiode is o'zr7 AlWatt, at tr: 5o5 nm, and
theactive area is 5'r X ro-0 m2. Thus the energy densityreceived by
the photodiode at the simulated retinalplane is lr8 Jm-2. Note that
when the flash is firstfired after a rest period of a few minutes,
the flux fromthe first flash is about 5 per cent higher than that
of thesubsequent flashes which are fired at regular intervalsof,
say, 5 or ro s.
During the retinal photography step, the filtersFr+HFr+zB*t+ ND
are used in the fundus camera.Taking the transmittance of the
ocular media as 75per cent at tr:5o5 nm (Table z'J,Wyszecki and
Stiles,1967) the retinal energy density is 7'o4 Jm-2. Theretinal
energy density may then be calculated for anygiven combination of
filters inserted in the funduscamera, given the spectral
distribution of the xenonflash-discharge source. Although there are
severalnarrow peaks in the 46o-49o nm band, in most applica-tions
the distribution may be taken to be essentiallyflat over the range
4oo-63o nm. Thus the use of abroad spectral band for bleaching,
say, from 43o-63o nm,increases the total flux by about 3oo times
more thanthat used during photography. If we take the
meantransmittance of the ocular media as 70 per cent, theretinal
energy density within this spectral band isabout r'5 x ro3
Jm-'.
In order to calculate the increase in the actinic fluxduring the
bleaching step, the absorption spectrum ofrhodopsin was used
(Crescitelli and Dartnall, r953).In the spectral range 43o-63o nm,
the increase is 9.6times more than that in a ro nm bandwidth
centredat 5o5 nm. Thus, the removal of the neutral densityfilter
and F2 from the light path will increase the actinicflux at the
retinal plane to: r'r8 x9'6xlogro-t (r'9) xTeor 9oo x T" Jm-2.
Absorb-ance(density) .A1 (at 1:5o5 nm)
F2HF,'Wratten zE
o'6oo'07o'o3
(Half power bandwidth: ro nm)
The flux density in the retinal plane which wassimulated within
the model eye was measured by afast-response photodiodef. The
photodiode was oper-ated in the photoconductive mode, using a bias
of-45 V on its guardring electrode. The photocurrentwas fed
directly into an operational amplifier which wasconstructed from an
integrated circuit, type LM 3o8.This was wired so as to perform
either as a linear cur-rent-to-voltage converter or an integrator.
Thus theenvelope of a photocurrent pulse resulting from
thedetection of a xenon flash could be viewed on an oscillo-scope
or the integral of the current pulse could bemeasured by means of a
voltmeter. The linearity ofthe operational-amplifier circuit was
checked by inject-ing pulses of current from a pulse generator and
throughsuitable known values of resistors. The response
time(measured between the ro per cent and 9o per cent*Perkin Elmer,
model 4oztSGD rooA, a silicon PIN type, supplied calibrated by E.
G' andG. Inc, Boston, IJSA
ReferencesARNoLD, c. R., RoLLS, p. J., and srrwaRT, J. c. n.
(rg7r) 'Applied Photography', Focal Press, LondoncREScITELLI, F.,
and DARTNALL, H.J. A. (tsS:) Nature (Lond'), T72' tgsHIGHMAN, v.
N., and wEALE, n. e. (r973) Amer. J. Ophthal',75r 822JAY, B. (r96r)
Vision Res., t, 4r8Rlpps, H., and wEALE, n. e. (1969) J. Physiol.
(Lond.),2oo' r5rsAID, F. s., and wEALE, n. e. (rg59) Gerontologica
(Basel),3t 2r3wEALE, n. a. (1968) Nature (Lond.), zr8,238
GgZ+) Ophthalmologica ( Basel) , 169, 3owrLLrAMS, T. p. Gg7+)
Vision Res., r4r 6o3wrrszEcKl, c., and srILES, w. s. (1967) 'Colour
Science', Wiley, New York

![Rhodopsin Dimers: Molecular Dynamics Simulations Using ... · membranes, support a molecular model of rhodopsin monomers orga-nized into two dimensional arrays of dimers [3]. Specifically,](https://img.pdfslide.us/doc/110x75/61455a0534130627ed50ebd3/rhodopsin-dimers-molecular-dynamics-simulations-using-membranes-support-a.jpg)