Embed Size (px)
Citation preview

“Grigore T. Popa” University of Medicine and Pharmacy - Iași
Faculty of Dentistry
SUMMARY
PH.D THESIS
CLINICAL AND LABORATORY STUDIES
REGARDING CLINICAL-BIOLOGICAL INDICES RELATED TO DENTAL
EROSIONS
Scientific coordinator
Prof. dr. Andrian Sorin
Ph.D student
Arnăuțeanu Cosmin George


i
CONTENT
STAGE OF KNOWLEDGE
Introduction
CHAPTER I. CURRENT DATA ON ENAMEL STRUCTURE AND COMPOSITION
I.1. General considerations
I.2. Physical properties
I.3. Chemical properties
I.4. Structural particularities
CHAPTER II. GENERAL ASPECTS REGARDING DENTAL EROSION.
II.1. Definitions
II.2. Clinical aspects
II.3. Histopatological aspects
II.4. Systems of classification
II.5. Data regarding prevalence and incidence of dental erosions
CHAPTER III. ETHIOPATOGENIC MECHANISMS IN THE INITIATION AND
EVOLUTION OF DENTAL EROSIONS
III.1. Extrinsic factors
III.2. Intrinsic factors
CHAPTER IV. PARACLINICAL METHODS USED IN THE QUANTITATIVE AND
QUALITATIVE OF DENTAL EROSIONS
IV.1. Aspects regarding the methodology of studies investigating dental erosion
processes
IV.2. Quantitative assessment methods
IV.3. Qualitative assessment methods
CHAPTER V. PREVENTION STRATEGIES IN THE TREATMENT OF DENTAL
EROSIONS
V.1.Strategies to prevent dental erosions
V.2. Restorative therapy of dental erosions

ii
PERSONAL SECTION
CAPITOL VI. REASONS FOR RESEARCH THEME CHOICE. THE RESEARCH
METHODOLOGY.
VI.1. The reason for research thema choice
VI.2. Objectives
VI.3. Research directions
CAPITOL VII. PREVALENCE AND DISTRIBUTION OF DENTAL EROSIONS:
EPIDEMIOLOGICAL STUDY
VII.1. The aim of study
VII.2. Materials and method
VII.3. Results and discussions
VII.4. Conclusions
CAPITOL VIII. STUDY IN VITRO REGARDING EROSION PROCESSES
INDUCED BY ACID AGENTS
VIII.1. The aim of study
VIII.2. Materials and method
VIII.3. Results and discussions
VIII.4. Conclusions
CAPITOL IX. THE EVALUATION OF THE EROSION EFFECT OF SOME
BEVERAGES FOR ATHLETES AND THE PROTECTIVE EFFECT OF SOME
REMINERALIZING PRODUCTS ON HARD DENTAL TISSUES
IX.1. The aim of study
IX.2. Materials and method
IX.3. Results and discussions
IX.4. Conclusions
CAPITOL X. STUDY REGARDING KNOWLEDGES AND ATTITUDES OF
DENTISTS ON DIAGNOSTIC AND TREATMENT OF DENTAL EROSIONS
X.1. The aim of study
X.2. Materials and method
X.3. Results and discussions
X.4. Conclusions
GENERAL CONCLUSIONS
REFERENCES

iii
Key words: dental erosions, prevalence, acid agents, demineralisation, remineralisation,
therapeutic management
PhD Thesis contains:
stage of knowledge organised in 5 chapters (44 pages);
personal studies organised in 5 chapters (176 pages);
163 tables and 131 figures;
326 references.
Note: the abstract presents selective references, tables and figures, respecting the content and
counting in pHD Thesis.

1
CHAPTER VI. REASONS FOR RESEARCH THEME CHOICE. THE RESEARCH METHODOLOGY
VI.1. Reasons for the choice of research theme
The quality of dental assistance and technological novelties depend on the
understanding of teeth properties, basic principles and mechanisms implied in the interaction
with surrounding environment.
Last decade the dental erosion and the associated erosion wear are considered high risk
factor for the integrity of hard dental tissues.
The initiation and evolution of dental erosion is influenced by structural characteristics
of teeth, saliva properties, acids sources, parafunctional habits.
A major role in the initiation and evolution of dental erosions is played by the
interaction between chemical factors (composition), biological factors (presence of
saliva/acquired pellicle, salivary rate) as well as behavioural factors (habits regarding the way of
beverages drinking, patterns of teeth abrasion after acid exposure).
Apart from visible clinical defects produced by dental erosion, the prolonged exposure
to acid produces the changes of hard dental tissues physical propertties. The demineralisation
produced by dental erosion reduces the tooth resistance and makes tooth surfaces susceptible to
erosion wear. The dental erosion is also linked by other forms of wear and increases the physical
wear.
The erosion manifests as dental wear, with increasing rate at global level.
Actually there is no accurate data regarding each category of dental wear due to various
indices systems that are not reflecting the ethiology as well as the epidemiological research
models performed on populations with diverse characteristics and age groups. The interpretation
and comparisons of epidemiological data studies is difficult due to the differences in terminology
as well as high number of indices systems used in diagnostic, classification and monitorisation of
erosive lesions categories.
Considering the increasing prevalence and incidence of dental erosion to childrens and
young adults, the early diagnosis of dental erosions for these age categories will allow the
approach for properly preventiv-therapeutical measures.
This approach is important considering the the negative impact of dental erosion on
definitive denture followed by damage of interocclusal and intermaxillary relations requesting
complex prosthetic therapeutical solutions with high financial and psychical costs for patients
with dental erosions.
The dental pratitioners must posess theoretical and practical knowledges regarding the
interaction between chemical, biological and behavioural factors, major feature of patients with
high risk.
Following the concern in current practice and during PhD preparation:
o the collecting of materials that integrate literature data regarding diverse forms of dental
erosions.
o the study of clinical, paraclinical and systemic aspects of patients with dental erosions
taken in research.

2
o the statistical studies, clinical studies, experimental studies, were performed using a
personal database recorded on patients diagnosed and treated in Clinical Base of Dental
Medicine Faculty, U.M.F. “Grigore T.Popa”.
VI.2. Objectives
For the performing of proposed aims, were specified the objectives as follows:
o the structuring of a complex assessment program including diagnostic correlated with
evolution stage and patients characteristics
o the statistical processing of clinical cases from a three years database
o the determination of ethiopathogenic factors
o the description of clinical elements and paraclinical examens used in the epidemiological
study (prevalence, distribution of dental erosion in relation to the investigated
parameters)
o the description of paraclinical examens used in in vitro studies regarding the
demineralization and remineralisation processes to the enamel and dentine surfaces of
teeth affected by dental erosions
o the description of questionnaire used to determine the opinions and therapeutical attitudes
of dental practitioners.
VI.3. Research directions
The study was oriented to the research directions as follows:
o Clinical study regarding the identification of clinical cases with dental erosions and
analysis of dental erosion distribution related to the researched factors (sex, age groups,
dental groups, dental surfaces, sextants)
o The impact of extrinsic and intrinsic factors on prevalence, distribution and severity of
dental erosions
o Chemical analysis of dental surfaces affected by dental erosion under action of chemical
erosive agents like beverages and sports drinks
o Chemical and profilometric analysis of dental enamel and dentine surfaces affected by
dental erosions and submitted to remineralisation processes by using CPP-ACP based
products
o Paraclinical assessment of physical-chemical properties of some beverages and sport
drinks with erosive potential
o The questionnaire-based study regarding the opinions and attitudes of dentists on
diagnostic possibilities, treatment techniques and materials, patients vindicate and
systemic factors analysis.

3
CHAPTER VII. PREVALENCE AND DISTRIBUTION OF DENTAL EROSIONS: EPIDEMIOLOGICAL STUDY
VII.1. AIM OF STUDY
The aim of study was to assess the prevalence, distribution and severity of dental
erosion related to different clinic-biological indices on young adult patients.
VII.2. MATERIALS AND METHOD
The study group included 1296 patients investigated in Clinical Base of Dental
Medicine Faculty U.M.F.”Grigore T.Popa” Iasi. Written consent was obtained for each
patient. The study group included 594 males and 702 females (fig.7.1) . 1074 patient were
age 18-25, 192 patients in age 26-35, 75 patients over 35 years(fig.7.2.). The mean age was
24,45 years. A total number of 72 patients and 396 teeth were diagnosed with dental erosions.
The severity of dental erosions was recorded using BEWE indices system (tabel 6).
Clinical aspects of dental erosions from study group are presented in figures 7.3.a-c.
Fig.7.3.a. M.A., age 25. Dental erosions-anterior maxillary teeth.
Frecvent consumption of sport drinks.
Fig.7.3.b.B.G., age 32. Dental erosions mandibular bicusps. Frecvent consumption of beverages.

4
Fig.7.3.c.M.N., age 35. Dental erosions mandibular bicusps. Frecvent consumption of soft drinks.
For each patient the examiner (PhD student) performed a clinical examen including
localisation, BEWE indices, nutritional habits, lifestyle, parafunctional habits. All teeth were
examined in same conditions of light and magnification. It were recorded data about consume
(frequency, quantity) of beverages, soft drinks, cola drinks, fruit juices, sport drinks, acid
aliments and medication with erosive potential.
Data were recorded as follows:
-presence/absence of dental erosions:
- related to study group;
- related to sex;
- related to age group;
- related to ethiological factor.
-distribution of dental erosion on dental groups/dental surfaces/sextants:
- related to sex
-related to age group;
- related to ethiological factor.
-severity of dental erosion (BEWE system):
-related to sex;
-related to age group;
-related to ethiological factor.
-distribution related to combination sextant/dental surface/ BEWE/sex/age group.
Table 7.I. BEWE system.
SCORE BEWE DESCRIPTION
0 No dental hard tissues loss
1 Low enamel loss
2 Distinct defect, hard dental tissue loss<50% surface area
3 Distinct defect, hard dental tissue loss>50% surface area
The database was created using Microsoft Office EXCEL 2007. The data statistical
processing was performed using software SPSS 17 (SPSS Inc, SUA). The statistical data were
presented as mean values and standard deviations. P<0.05 was considered as having
statistically significant result.

5
VII.3. RESULTS AND DISCUSSIONS
The results regarding the prevalence of dental erosions and their distribution in
relation to sex, age groups, dental surfaces, dental groups, sextants, are presented in the next
graphs.
The prevalence for all study group was 6% (fig.7.4.).
A difference related to dental erosions prevalence was observed between males (7%)
and females (4%) (fig.7.5.a-b).
Fig.7.4. Prevalence of dental erosions
Fig.7.5.a-b.Prevalence of dental erosions related to patients sex

6
Fig.7.6.a-c. Prevalence of dental erosions related to age group
Related to age groups, prevalence of dental erosions is 6% for age group 18-25, 4%
for age group 26-35 and 8% for patients over 35 years (fig.7.6.a-c).
75%
8%
8%8%
Factor eroziv
Bauturi Acidulate
Supliment Sportiv
Medicatie
Gastro intestinali
Fig.7.8.Distribution of ethiological factors in study group
Related to erosive ethiological factors, 75% of patients with dental erosions are
associated with consume of beverages and soft drinks. The consume of sport drinks is
observed for 8% patients with dental erosions, a similar value with patients under erosive
mediaction and patients with GERD (gastro-esophageal reflux disease) (fig.7.8.).
Related to dental surfaces, highest values of prevalence of dental erosions are 23%
for lateral buccal dental surfaces and 16% for buccal anterior maxillary teeth (fig.7.11.).

7
Fig.7.12. Prevalence of dental erosions related to ethiological factors
Related to ethiological factors (fig.7.12.), 32% from total number of dental erosions
are observed to patients consuming sport drinks, 21% to patients frequent consume of
beverages, soft drinks and fruit juices, 19% to patients under erosive medication, and 14% to
patients with GERD.
The distribution of BEWE indices (severity of dental erosions) related to the
investigated factors is presented in the next graphs.
The BEWE mean value is higher for females (5,2) than males (4,7) (fig.7.13.).
Patients over 35 years are associated with highest BEWE mean value (8), followed by age 26-
35 (7) and age 18-25 (4,1) (fig.7.14.).
The sextants S4 and S6 present highest BEWE mean value (1.25) (fig.7.15.).
Fig.7.13. BEWE mean values (sex)
Fig.7.14. BEWE mean values (age groups)
Related to ethiological factors, patients associated with sport drink consume present
highest mean BEWE values (9), followed by medication (8), beverages (4,2) and GERD (4)
(fig.7.16).

8
Fig.7.16. BEWE mean values (ehtiologic factors)
The statistical study aimed to confirm or deny the null hypothesis regarding the
absence of statistical differences regarding prevalence and severity of dental erosions
between different clinical-biological indices.
Statistical analysis regarding prevalence of dental erosions related to sex
(dental erosion study group)
Table 7.III. Mann-Witney, Wilcoxon tests. Grouping variable: Sex
Test Statisticsa
VAR00008
Mann-Whitney U 576.000
Wilcoxon W 1479.000
Z -.625
Asymp. Sig. (2-tailed) .532
a. Grouping Variable: Sex
Table 7.III. indicates Mann-Whitney test, with U value 576, and p = 0.532 > 0.05.
This result confirms the absence of statistically significant differences between mean values
BEWE for males and females.
Statistical analysis regarding prevalence of erosions related to age group
( dental erosion study group)
Non-parametric Kruskal Wallis test was applied for all age groups to confirm or deny
the existance of significant statistically differences between age groups.
Table 7.IV.a. Kruskal Wallis. Prevalence of dental erosions related to age groups
Test Statisticsa,b
VAR00008
Chi-Square 8.875
df 2
Asymp. Sig. .012
a. Kruskal Wallis Test
b. Grouping Variable: Age groups
Statistically significant differences were obtained for the three age groups (tabel
7.IV.a). Mann Whitney test was applied for each pair of age groups.

9
Statistical analysis regarding prevalence of erosions related to age group
( dental erosion study group)
Table 7.b. Kruskall-Wallis test. Prevalence of dental erosions related to dental groups
Test Statisticsa,b
NrErosions
Chi-Square 81.614
df 5
Asymp. Sig. .000
a. Kruskal Wallis Test
b. Grouping Variable: Dental groups
The results of Mann-Whitney test show significant statistically differences between
the investigated dental groups (table 7.V.b.).
Statistical analysis regarding prevalence of erosions related to age group
(dental erosions study group)
Table 7.VI.a. Mann-Whitney, Wilcoxon tests. Beverages vs. medication
Test Statisticsb
NrEroziuni
Mann-Whitney U 162.000
Wilcoxon W 183.000
Z .000
Asymp. Sig. (2-tailed) 1.000
Exact Sig. [2*(1-tailed Sig.)] 1.000a
a. Not corrected for ties.
b. Grouping Variable: Erosive factor
Table 7.VI.a indicates Mann-Whitney test, with U value 162.000, and p = 1.000 >
0.05. This result confirms the absence of statistically significant differences between mean
values BEWE for beverages and medication.
Table 7.VI.b. Mann-Whitney, Wilcoxon tests. Beverages vs. sports drinks
Test Statisticsb
NrEroziuni
Mann-Whitney U 36.000
Wilcoxon W 1521.000
Z -3.168
Asymp. Sig. (2-tailed) .002
Exact Sig. [2*(1-tailed Sig.)] .001a
a. Not corrected for ties.
b. Grouping Variable: FactorEroziv
Table 7.VI.b. indicates Mann-Whitney test, with U value 36.000, and p=0.002< 0.05.
This result confirms the existance of statistically significant differences between mean values
BEWE for ethiological factors beverages and sport drinks. and females.

10
Our study shows reduced values of dental erosions prevalence (6%) comparing with
literature data related to adolescents and young adults: Arnadottir&col. (23.2% în Islanda),
Bardsley&col.(27.1% în Marea Britanie), van Rijkom&col. (16% în Olanda), Vargas-
Fereira&col.(7.2% în Brazilia), Kumar&col.(8.9% în Brazilia), Wang&col.(23.2% în China),
Okunseri&col.(39% în SUA), Margaritis&col.(50% în Grecia) /10, 30, 169, 229, 287, 290,
299/.
Related to ethiological factors, 75% patients consume frequently beverages and soft
drinks, result sustained by the literature data.
Al-Dlaigan&col.(2001) show that 80% adolescents consume beverages with 23%
high and frequent consumers (>22/săptămână) /2/. Chrysanthakopoulos NA(2012) assessed
the prevalence and the associated ethiological factors in Greece on adolescents /52/. The
results show a high rate of dental erosions (33.8%) associated with high frequency of
beverages and fruit juices and with rinsing habits before to swallow. Curcă&Danilă(2010)
investigated prevalence and severity of noncariogenic lesions using Smith&Knight indices on
614 pacienţi with age over 18 years /58/. 2.9% from noncariogenic lesions with indice 1 are
dental erosions, percent that increases to 7.9% for noncariogenic lesions with indice 2. 20%
noncariogenic lesions with indice 3 Smith&Knight are dental erosions. From patients that
consume alchohol, 87% are affected by dental erosions with high rate of indice 3, comparing
with only 50% in control group. Micu Magdalena-Ioana (2010) repports a 7.6% frequency of
pure dental erosions related to all noncariogenic lesions found in patients over 18 /206/.
Ganns C&col.(2001) found a prevalence of 11.6% in Germany, while O’Brian (1993) found
30% in Great Britain/95/.
Kunzel&col.(2000) found specific localisation of dental erosions to buccal surfaces
of lateral and central incisive of dental erosions in study group of childrens that consume high
quantities of orange juices /171/. Also O’Brien(1993) found frequent localisation of dental
erosions to buccal and oral dental surfaces to adolescents and young adults that consume
beverages and fruit juices /225/. Vered Y&col.(2014) performed an epidemiological BEWE-
based study regarding prevalence and distribution of dental erosions in 500 adolescents and
young adults /291/. The results show the presence of dental erosions on over 50% subjects
with 10% having dental erosions more than half of dental surfaces. Mean value of BEWE
increased with age and erosive diet. Holbrook WP.&col.(2014) found 30.7% prevalence of
dental erosions for age group 15 ani (38.3% males, 22.7% females) and BEWE mean values
1.00 for males and 0.42 for females (p<0.001) /132/. Valorile BEWE au prezentat diferenţe
semnificative statistic comparativ cu vârsta 12 ani (19.9% băieţi, 11% fete) cu scoruri medii
BEWE de 0.22 pentru băieţi şi 0.079 pentru fete.
The correlation between beverage consume and prevalence of dental erosions are
explained by superior content of phosphoric acid compared to citric acid, malic acid, lactic
acid pphosphoric acid in cola drinks, with higher erosive potential /303/. The consume of
energy drinks, especially during physical exercises is also associated to increased prevalence
and severity of dental erosions/136/.

11
VII.4. CONCLUSIONS
The prevalence of dental erosions is reduced in Romania (6%) with higher values for
males (8%) and lower values for females (4%).
Related to age group, highest values of dental erosions frequency are associated to
patients over 35 years (8%) and lowest values for patients in age group 26-35 (4 %).
Related to localisation, most affected are sextants S4 and S6, buccal surfaces of lateral
teeth and buccal surfaces of anterior maxillary teeth, and mandibular molars and
bicusps.
Related to ethiological factors, most affected by dental erosions are patients with high
consume frequency of beverages and soft drinks.
Related to severity, the distribution is balanced with 33% for mild dental erosions,
33% for moderate dental erosions and 33% for severe dental erosions.
Higher BEWE mean values BEWE are associated to patients high consumers of sport
drinks (BEWE 9), while patients high consumers of beverages have 4,5. Highest
BEWE values are encountered to females (5.2), patients over 35 years (8.00), sextants
S4 and S6 (BEWE 1.25) and erosive medication (BEWE 8.00).

12
CHAPTER VIII. STUDY IN VITRO REGARDING EROSION PROCESSES INDUCED BY ACID AGENTS
VIII.1. AIM OF STUDY
The aim of study was to investigate the topography and to analyse chemically the
enamel submitted to the action of various acid agents in the presence and absence of acquired
salivary pellicle.
VIII.2. MATERIALS AND METHOD
The study group included 15 unaffected teeth extracted from orthodontic or
periodontal reasons extraşi din motive ortodontice sau parodontale (Fig. 8.1.). The teeth were
sectioned in three slices using diamond discs (Komet Dental, Brasseler GmbH&Co,
Germania), under water cooling (Fig.8.2.). The samples were immersed for 7 days in artificial
saliva AFNOR, changed at every 24 hours. For each tooth one sample was maintained as
control: 1 minute in distilled water, followed by 4 hours immersion in artificial. Another
sample was immersed for 12 hours in acid agents: Red Bull, green tea Lipton, apple juice
Auchan, mineral water Borsec, lemon juice (Fig. 8.3.). The last sample was submitted to a
cycle demineralisation-remineralisation three times: demineralisation by immersion in acid
solution for 1 minute, followed by remineralisation in artificial saliva for 4 hours. These
protocols were selected to simulate the real conditions acid beverages consume in oral cavity.
After each demineralisation the samples were washed in distilled water.
The solutions pH: 3,4 for Red Bull, 3,0 for Lipton –green tea, 3,4 for apple juice, 3,2
for mineral water, 2,4 for lemon juice.
Fig. 8.3 Acid solutions used in study
Fig. 8.1. Teeth in study group
Fig. 8.2. Slices of teeth after sectioning

13
After samples preparation, these were analysed to investigate surface topography,
using electronic microscope VEGA II LSH, TESCAN Cehia; the chemical analysis was
performed using EDX detector QUANTAX QX2, BRUKER/ROENTEC Germany (Fig. 8.4.).
VIII.3. RESULTS AND DISCUSSIONS
The figures 8.5., 8.6., 8.7. present aspects of enamel for control samples, samples
under continuous immersion and alternative immersion in apple juice as erosive agent.
For samples immersed in apple juice the erosion was moderate as observed in figures
8.6. and 8.7.
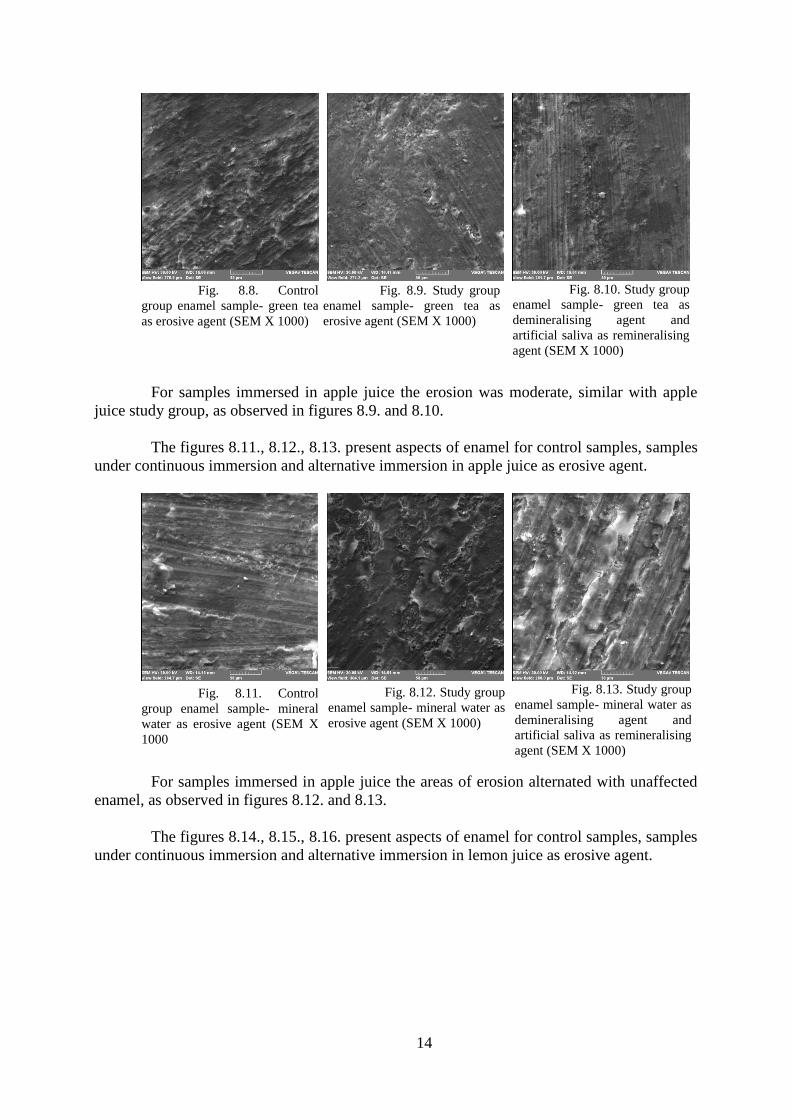
The figures 8.8., 8.9., 8.10. present aspects of enamel for control samples, samples
under continuous immersion and alternative immersion in green tea as erosive agent.
Fig. 8.5. Control
group enamel sample- apple
juice as acid agent (SEM X 500)
Fig. 8.6. Study group
enamel sample-apple juice as
acid agent (SEM X 1000)
Fig. 8.7. Study group
enamel sample- acid juice as
demineralising agent and
artificial saliva as remineralising
agent (SEM X 1000)
Fig. 8.4. Electronic microscope and EDX
detector
14
For samples immersed in apple juice the erosion was moderate, similar with apple
juice study group, as observed in figures 8.9. and 8.10.
The figures 8.11., 8.12., 8.13. present aspects of enamel for control samples, samples
under continuous immersion and alternative immersion in apple juice as erosive agent.
For samples immersed in apple juice the areas of erosion alternated with unaffected
enamel, as observed in figures 8.12. and 8.13.
The figures 8.14., 8.15., 8.16. present aspects of enamel for control samples, samples
under continuous immersion and alternative immersion in lemon juice as erosive agent.
Fig. 8.13. Study group
enamel sample- mineral water as
demineralising agent and
artificial saliva as remineralising
agent (SEM X 1000)
Fig. 8.12. Study group
enamel sample- mineral water as
erosive agent (SEM X 1000)
Fig. 8.11. Control
group enamel sample- mineral
water as erosive agent (SEM X
1000
Fig. 8.10. Study group
enamel sample- green tea as
demineralising agent and
artificial saliva as remineralising
agent (SEM X 1000)
Fig. 8.9. Study group
enamel sample- green tea as
erosive agent (SEM X 1000)
Fig. 8.8. Control
group enamel sample- green tea
as erosive agent (SEM X 1000)

15
In the study group with continuous immersion in lemon juice, a pronounced
dissolution of enamel prisms was observed with the exposure of interprismatic enamel areas
(Fig.8.15.); this aspect is different from study group with alternative immersion (Fig.8.16.)
with more reduced demineralisation areas.
The figures 8.17., 8.18., 8.19. present aspects of enamel for control samples, samples
under continuous immersion and alternative immersion in Red Bull as erosive agent.
The enamel samples immersed in acid solution in the absence of acquired salivary
pellicle were associated with severe dissolution of enamel areas with chipped aspect (Fig.
8.18.). The enamel samples immersed in acid solution in the presence of acquired salivary
pellicle (obtained by previous immersion in artificial saliva) were associated with intact
enamel areas with mild erosion in the adjacent areas (Fig. 8.19.).
Fig. 8.19. Study group
enamel sample- Red Bull as
demineralising agent and
artificial saliva as remineralising
agent tul eroziv Red Bull și
remineralizare în salivă artificală
(SEM X 1000)
Fig. 8.18. Study group
enamel sample- Red Bull as
erosive agent (SEM X 1000)
Fig. 8.17. Control
group enamel sample- Red Bull
as erosive agent (SEM X 1000)
Fig. 8.16. Study group
enamel sample- mineral water as
demineralising agent and lemon
juice as remineralising agent
(SEM X 1000)
Fig. 8.15. Study group
enamel sample- lemon juice as
erosive agent (SEM X 1000)
Fig. 8.14. Control
group enamel sample- lemon
juice as erosive agent (SEM X
1000)

16
The mean values of Ca and P (wt%) in enamel surfaces for all study groups are
presented in table 8.XVI.
Table 8.XVI. Mean values of Ca and P ions (wt%) for study groups
Apple juice Green tea Mineral
water
Lemon juice Red Bull
Ions concentration (wt%) C
Ca
P
P
C
Ca P
P
C
Ca
P
P
C
Ca
P
P
C
Ca
P
P
Control 3
2.65
1
2.67
3
1.84
1
3.56
3
2.65
1
3.58
2
9.09
1
2.67
3
2.09
1
3.20
Continuous
immersion in acid solution
3
0.13
1
2.20
3
0.39
1
2.24
2
9.58
1
2.82
1
8.67
9
.90
2
3.13
1
0.25
Alternative
immersion in acid solution
and saliva
3
1.25
1
2.51
3
1.69
1
2.83
3
1.07
1
2.20
2
8.91
1
1.14
3
1.69
1
2.76
It was observed a tendencty for the decrease of Ca and P ions levels following
immersion in acid solutions.
For all five acid solutions, the values of Ca and P ions concentrations were closer to
control group for alternative immersion study group comparing with continous immersion
study group (Figurile 8.20-8.25).
0
10
20
30
40
Calciu smalt Fosfor smalt
Suc de meremartor
Suc de meresolutie
Suc de meretest
0
5
10
15
20
25
30
35
Calciu smalt Fosfor smalt
Ceai verdemartor
Ceai verdesolutie
Ceai verdetest
0
5
10
15
20
25
30
35
Calciu smalt Fosfor smalt
Apa mineralamartor
Apa mineralasolutie
Apa mineralatest
0
5
10
15
20
25
30
35
Calciu smalt Fosfor smalt
Suc de lamaiemartor
Suc de lamaiesolutie
Suc de lamaietest
0
5
10
15
20
25
30
35
Calciu smalt Fosfor smalt
Red Bullmartor
Red Bullsolutie
Red Bulltest
Fig.8.21. Ca and P variation in enamel for
control, solution, test. Green tea as acid solution. Fig.8.20. Ca and P variation in enamel for
control, solution, test. Apple juice as acid
solution.
Fig.8.24. Ca and P variation in enamel for
control, solution, test. Lemon juice as acid
solution.
Fig.8.23. Ca and P variation in enamel for
control, solution, test. Mineral water as acid
solution.
Fig.8.25. Ca and P variation in enamel for
control, solution, test. Red Bull as acid solution.

17
Values were statistically analysed using Mann-Whitney, Anova and Bonferoni tests.
Tables 8.XX.a-b present the results of Mann-Whitney test for comparison of calcium
ions concentration in solution study group and test study group immersed in RedBull.
Tables 8.XX.a-b.Mann-Whitney test.Comparison of Ca levels between solution study group and test study group
Ranks
lot N Mean Rank Sum of Ranks
Enamel/Ca solution 5 3.00 15.00
test 5 8.00 40.00
Total 10
Test Statisticsb
Enamel/Ca
Mann-Whitney U .000
Wilcoxon W 15.000
Z -2.611
Asymp. Sig. (2-tailed) .009
Exact Sig. [2*(1-tailed Sig.)] .008a
a. Not corrected for ties.
b. Grouping Variable: lot
Statistically significant results were obtained when comparing the concentration of
calcium ions in solution study group and test study group (p=0,009 < 0.05).
Tables 8.XXIII.a-b present the result of Mann-Whitney test used to compare the P
ions concentration between solution study group and test study group immersed in RedBull.
Tables 8.XXIV.a-b. Mann-Whitney test.Comparison of Ca levels between solution study group and test study
group Ranks
lot N Mean Rank Sum of Ranks
Enamel/P solution 5 3.00 15.00
test 5 8.00 40.00
Total 10
Test Statisticsb
Enamel/P
Mann-Whitney U .000
Wilcoxon W 15.000
Z -2.611
Asymp. Sig. (2-tailed) .009
Exact Sig. [2*(1-tailed Sig.)] .008a
a. Not corrected for ties.
b. Grouping Variable: lot
Statistically significant results were obtained when comparing the concentration of P
ions in solution study group and test study group (p=0,009 < 0.05).

18
Tables 8.XXVI.a-b present the result of Anova test used to compare the P ions
concentration between solution study group and test study group immersed .in lemon juice.
Table 8.XXVI. Anova test. Comparison of Ca and P levels between control, solution study group and test study
group. Acid agent- juice lemon
ANOVA
Sum of Squares df Mean Square F Sig.
Ca enamel Between Groups 355.777 2 177.889 88944.333 .000
Within Groups .024 12 .002
Total 355.801 14
enamel P
Between Groups 21.619 2 10.809 4567.394 .000
Within Groups .028 12 .002
Total 21.647 14
Total 27.803 14
With p<0,05 the statistical test demonstrates the existance of statistically significant
differences between the study groups.
Table 8.XXIX presents the results of Anova test for comparison between Ca and P
ions concentration in control group, solution study group and test study group immersed in
mineral water.
Table 8.XXIX. Anova test. Comparison of Ca and P levels between control, solution study group and test study
group. Acid agent- mineral water
ANOVA
Sum of Squares df Mean Square F Sig.
enamel Ca
Between Groups 23.569 2 11.784 6148.435 .000
Within Groups .023 12 .002
Total 23.592 14
enamel P
Between Groups 8.577 2 4.289 4765.185 .000
Within Groups .011 12 .001
Total 8.588 14
Total 2.398 14
With p<0,05 the statistical test demonstrates the existance of statistically significant
differences between the study groups.
Table 8.XXXII presents the results of Anova test for comparison between Ca and P
ions concentration in control group, solution study group and test study group immersed in
green tea.

19
Table 8.XXXII. Anova test. Comparison of Ca and P levels between control, solution study group and test study
group. Acid agent- green tea
ANOVA
Sum of Squares df Mean Square F Sig.
enamel Ca
Between Groups 8.967 2 4.483 2861.809 .000
Within Groups .019 12 .002
Total 8.986 14
enamel P
Between Groups 4.372 2 2.186 2676.939 .000
Within Groups .010 12 .001
Total 4.382 14
Total 24.886 14
With p<0,05 the statistical test demonstrates the existance of statistically significant
differences between the study groups.
Table 8.XXXV presents the results of Anova test for comparison between Ca and P
ions concentration in control group, solution study group and test study group immersed in
apple juice.
Table 8.XXXV. Anova test. Comparison of Ca and P levels between control, solution study group and test study
group. Acid agent- apple juice
ANOVA
Sum of Squares df Mean Square F Sig.
enamel Ca
Between Groups 1.325 2 .663 17.500 .000
Within Groups .454 12 .038
Total 1.779 14
enamel P
Between Groups .277 2 .139 168.510 .000
Within Groups .010 12 .001
Total .287 14
Total 36.051 14
With p<0,05 the statistical test demonstrates the existance of statistically significant
differences between the study groups.
Numerous in vitro and in vivo researches assessed the erosive potential of different
drinks and foods.
The chelating properties of citric acid can increase the erosive process in vivo by the
interaction with saliva, apart from direct demineralisation and mineral dissolution from hard
dental tissues /202/. Some experimental in vitro studies demonstrated more powerful action of
citric acid comparing with phosphoric acid for similar titratable acidity /302/.
The content of Ca and P of drinks is an important factor that influences concentration
gradient in local environment from tooth surface. The adding of Ca and P salts in acid drinks
conducted to promising results regarding the prevention of dental erosions /16, 26, 174/.
The sport drinks have powerful erosive activity especially when consumed during
physical training sessions and associated with dehydration their erosive activity is more
prononunced /136/.

20
Regarding topographic changes, the results obtained by our study, following
immersion of enamel samples unprotected by acquired salivary pellicle in acid solutions, are
similar with literature data /202/
Drinks pH has a direct influence on the dissolution rate of enamel. The phosphoric
acid, citric acid and Na citrate are frequently found in beverages and sport drinks /51/. The
acids with chelating properties can produce dissolutions even at high levels of pH /289/.
The content of Ca and P in foods and drinks influences local environment but despite
the effect of reducing progresssion, not always the minerals addition can completely prevent
the initiation of dental erosions /186/.
In this context the results obtained by personal study have important clinical
implications for dental pratitioners.
VIII.4. CONCLUSIONS
1. The concentrations of Ca and P ions decreased after immersion in the tested acid
solutions;
2. Highest decrease of Ca and P ions from enamel surfaces was recorded for
immersion in lemon juice, followed by Red Bull, mineral water, apple juice and
green tea;
3. The presence of acquired salivary pellicle offered protection to enamel surfaces, as
Ca and P concentrations were less diminished comparing with the enamel surfaces
immersed in acid solutions in the absence of acquired salivary pellicle.

21
CAPITOL IX. THE EVALUATION OF THE EROSION EFFECT OF SOME BEVERAGES FOR ATHLETES AND THE PROTECTIVE EFFECT OF SOME REMINERALIZING PRODUCTS ON HARD DENTAL TISSUES
IX.1. THE AIM OF STUDY:
I. To determine pH and viscosity of three drink sports used to sustain physical
training
II. To assess and compare the effects of these sport drinks on surface hardness of
enamel and dentine
III. To assess and compare the effects of the three sport drinks on enamel and dentine
after remineralisation cycles with fluor-based products.
IX.2. MATERIALS AND METHOD
The three sport drinks used in study are as follows : Gatorade liquid (Pepsico),
energising tablets Isostar lemon (Isostar) CytoMax orange powder (CytoSport). The sport
drink Isostar was obtained by dissolving a tablet in 250 mL pure water (Borsec, Romaqua
Group), and sport drink CytoMax was obtained by dissolving one powder measure (25 mg) in
250 mL pure water (Borsec, Romaqua Group).
The sport drinks pH was determined using electronic pH-meter (Hanna pH 210). 10
measurement were performed for each sport drink repporting mean value.
The reological study was performed using Anton Paar, Physica MCR 501 with
Peltier system of temperature regulating (figure 9.1.). The temperature was regulated in a
range -40 -200oC. The measurement were performed using a geometry with cilinders.
Fig.9.1. Reometer Anton Paar Physica MCR 501
The flow curves were performed using a shear rate between 0.001-100 1/s, at
a temperature 37 oC and a time 5 minutes.
The study group used 33 unaffected teeth extracted for orthodontic reasons.
The teeth were maintained in distilled water. The teeth were sectioned using diamond discs
(Komet Dental, Brasseler GmbH&Co, Germania), under water cooling, aiming to obtain 2
horisontal slices (2 mm thickness). These slices were cut buccal-oral in two halves, obtaining
four slices for every tooth. The dental sections were divided randomly in two groups : study
group I included 40 samples, study group II included 90 samples. In study group I 10 samples

22
were maintained continuously in artificial saliva, as control group (control group 1), 10
samples were submitted to the erosive action of sport drink Isostar (Isostar): 5 series of 3
minutes immersion in sport drinks on 2 hours daily, for 14 days (study group 2). Another 10
samples were submitted to the erosive action of sport drink CytoMax (CytoSport): 5 series of
3 minutes immersion in sport drink on 2 hours daily, for 14 days (study group grup 3) ;
another 10 samples were submitted to the erosive action of sport drink Gatorade (Pepsico): 5
series of 3 minutes immersion 2 hours daily, for 14 days (study group 4).
Between erosive action of sport drinks, slices were maintained in artificial saliva.
Artificial saliva for this study was AFNOR standard S90-701, with pH 8,67 and next
composition: NaCl 0,7g/L; KCl 1,2 g/L; Na2HPO4 0,26 g/L; NaHCO3 1,5g/L; KSCN 0,33
g/L; uree 1,35 g/L. The times of immersion in sport drinks were chosen to simulate the
administration conditions during daily sport training. Each sample was immersed in same
quantity (15 mL) of tested drink, and these were changed after each immersion. The artificial
saliva was changed daily. In study group II, 30 samples were submitted to the previous
immersion protocole in Gatorade (study group 2), 30 samples were submitted in CytoMax
(study group 3), 30 samples were submitted to the previous immersion protocole in Isostar
(grup 4), but for 10 samples in each study group, previous to first immersion, was applied
toothpaste Colgate Total® for 3 minutes (Colgate Company) (subgrup a), to 10 samples fluor
gel Densell Company for 1 minute (subgrup b), and to 10 samples MI Paste Plus for 3
minutes (GC Company) (subgrup c).
The prepared samples were submitted to the analysis of surface microhardness for
enamel and dentine using digital devices CV 400 DAT (Namicon) (figure 9.2.).
Fig.9.2. Digital device CV 400 DAT (Namicon) for microhardness test
The microhardness was tested using Vickers method to compare variation of
mechanical properties of anisotrop materials /259/.
The measuring were performed using a testing device with diamond head at 136º
angle and 2,5 mm diameter. Indentation were performed with 50 g force with a minimal
distance between two consecutive indentation 1 mm. The number of indentaion for each
sample was 3, with mean value recorded after 3 measurings. The criteria for an indentation
were as follows : sharp on diagonal edges, uniform, without unregular areas in tested areas
(figura 9.3.). The microhardness was calculated after formula: D=1854,4·F/d2 (N/mm2)
(D=Vickers microhardness, F= test force, d= lenght of diagonal edge).
Fig 9.3. Proper indentation

23
IX.3. RESULTS AND DISCUSSIONS
The pH values of the three tested drinks were: 4.01 for Isostar, 4.74 for CytoMax,
3.23 for Gatorade.
The flow curves for all tested sport drinks are presented in graph 9.4.
Fig.9.4. Flow curves for the tested beverages
The mean values of viscosity for all sport drinks are presented in table 9.III.
Table 9.III. Viscosity mean values
Sample Gatorade Isostar Cytomax
Shear Rate(s-1) Viscosity
(mPa·s)
Viscosity
(mPa·s)
Viscosity
(mPa·s)
0.0681 6.66 4.64 64.6
0.1 2.58 0.239 58.2
0.147 2.82 0.618 52.7
0.215 2.21 1.56 44.6
0.316 1.18 1.24 33.8
0.464 1.1 1.09 25.7
0.681 1.16 1.11 19
1 0.778 0.648 14
1.47 0.948 0.773 10.4
2.15 0.901 0.808 8.6
3.16 0.915 0.827 6.91
4.64 0.892 0.785 5.91
6.81 0.906 0.795 5.15
10 0.902 0.798 4.57
14.7 0.915 0.821 4.05
21.5 0.94 0.847 3.67
31.6 0.953 0.86 3.36
46.4 0.984 0.891 3.14
68.1 1.04 0.943 2.99
100 1.08 1.05 2.84
0.1
1
10
100
mPa·s
0.01 0.1 1 10 1001/s
Shear Rate .
Gatorade
Viscosity
Isostar
Viscosity
Cytomax
Viscosity

24
Highest viscosity value was recorded for sport drink CytoMax, followed by Gatorade
and Isostar.
The mean values and standard deviations of microhardness values are specified in
table 9.V. Table 9.V. Mean values and standard deviations of hardness values in study group I (MPa)
Descriptive Statistics
N Minimum Maximum Mean Std. Deviation
Statistic Statistic Statistic Statistic Std. Error Statistic
Ctrlsalivadentine 10 55.40 59.10 57.2300 .27731 .87693
Ctrlsalivaenamel 10 186.80 219.80 203.0500 3.25833 10.30375
IsostarIdedentine 10 35.80 37.20 36.5600 .11944 .37771
IsostarIsenamel 10 113.00 114.70 113.8000 .15986 .50553
CytoMaxIdentine 10 22.00 23.60 37.1300 .15420 .48762
CytoMaxIenamel 10 109.40 110.90 110.3000 .17826 .56372
GatoradeIdentine 10 36.00 38.70 22.9000 .25300 .80007
GatoradeIenamel 10 103.90 107.50 105.6600 .38361 1.21308
Valid N (listwise) 10
The mean values of enamel microhardness after immersion in sport drinks were
lower than control group (mean value 113.8 after immersion in Isostar, 110.3 after immersion
in CytoMax and 105.6 after immersion in Gatorade). The same tendency was recorded for
dentine microhardness(mean value 36.56 after immersion in Isostar, 37.13 after immersion in
CytoMax and 22.90 after immersion in Gatorade). The highest values of microhardness were
recorded for Isostar and lowest values were recorded for Gatorade both for enamel and
dentine.
The statistical analysis was performed using Kruskal Wallis test for dentine
microhardness. The statistical results show statistically significant differences between the
four study groups with p = 0.0001 < 0.05 (tables 9.VII.a-b.).
Tables.9.VII.a-b. Kruskal Wallis test. Comparison of dentine hardness values
Ranks
Study group N Mean Rank
Demineralisation Control saliva dentine 10 35.50
Isostar I dentine 10 18.00
CytoMax I dentine 10 5.50
Gatorade I dentine 10 23.00
Total 40
Test Statisticsa,b
Demineralisation
Chi-Square 33.908
df 3
Asymp. Sig. .000
a. Kruskal Wallis Test
b. Grouping Variable: Lot

25
The mean values and standard deviations of microhardness values are specified in
table 9.V. Table 9.XXV.Mean values and standard deviations of hardness values (MPa) in study groupII
Descriptive Statistics
N Minimum Maximum Mean Std. Deviation
Statistic Statistic Statistic Statistic Std. Error Statistic
IsostarIIpastad dentine
10 25.50 26.70 26.1300 .13085 .41379
IsostarIIpastad enamel 10 34.90 36.40 35.7000 .17575 .55578
IsostarIIfluor dentine
10 45.10 46.90 45.0000 .18148 .57388
IsostarIIfluor enamel
10 203.10 205.50 158.3000 .22657 .71647
IsostarIIMiPaste dentine
10 44.00 46.60 46.0600 .29740 .94045
IsostarIIMiPaste enamel
10 154.80 162.60 204.0000 .80567 2.54777
CytomaxIIPastad dentine
10 55.00 57.90 41.2600 .29061 .91900
CytomaxIIPastad enamel
10 185.00 188.30 186.9600 .33106 1.04690
CytomaxIIfluor dentine
10 64.90 67.90 56.5300 .32457 1.02637
CytomaxIIfluor enamel
10 224.30 244.70 202.1600 1.73917 5.49974
CytomaxIIMiPastedentine 10 39.80 42.40 66.1300 .27536 .87076
CytomaxIIMiPasteenamel 10 187.70 219.00 234.6600 3.60753 11.40801
GatoradeIIPastaddentine 10 38.70 40.30 33.7000 .21554 .68158
GatoradeIIPastad enamel
10 129.80 131.90 130.7600 .24459 .77345
GatoradeIIfluor dentine
10 33.10 34.20 38.8300 .11832 .37417
GatoradeIIfluor enamel
10 145.90 146.70 138.9600 .09452 .29889
GatoradeIIMiPastedentine 10 38.50 39.10 39.5300 .06333 .20028
GatoradeIIMiPasteenamel 10 138.30 139.50 146.2600 .13013 .41150
Valid N (listwise) 10
The use of MI Paste and fluoride gel previous to immersion in Isostar conducted to
higher microhardness values of enamel and dentine (204.00 Mpa and 46.06 MPa, respectively
158.30 Mpa and 45.00 Mpa, comparing to values associated to use of toothpaste before
immersion in sport drinks (35.70 Mpa şi 26.13 MPa). Highest enamel and dentine
microhardness values were recorded for the use of MI Paste before immersion in sport drinks
(234.66 MPa and 66.13 Mpa), followed by the use of fluoride gel (202.16 MPa şi 56.53 Mpa)
and toothpaste (186.96 and 41.26 Mpa).
The results of Anova test for dentine microhardness values showed statistically
significant differences with p = 0.0001 < 0.05 (table 9.XXVII).

26
Table 9.XXVII. Anova test. Comparison between dentine hardness values ANOVA
Remineralisation dentine
Sum of Squares df Mean Square F Sig.
Between Groups 11307.358 8 1413.420 2714.699 .000
Within Groups 42.173 81 .521
Total 11349.531 89
Statistically significant differences were recorded between the all
remineralisation products with two exceptions: between the use of toothpaste and the use of
MI Paste before immersion in Gatorade and between the use of fluoride gel and the use of MI
Paste before immersion in Isostar.
The microhardness values for enamel were analysed with Anova test. The results
showed statistically significant differences with p = 0.0001 < 0.05 (tables 9.XXIX.a-b.).
Tables 9.XXIX.a-b. Anova test. Comparison of enamel hardness values
ANOVA
Remineralisation enamel
Sum of Squares df Mean Square F Sig.
Between Groups 269536.921 8 33692.115 1787.317 .000
Within Groups 1526.904 81 18.851
Total 271063.825 89
Statistically significant differences were recorded for all remineralisation products
with exception of the use of fluoride gel before immersion in Isostar and Cytomax.
The epidemiological studies repports direct relation between excesive consume of
soft drinks and the increase of dental erosions prevalence /212,160/. The erosive properties of
beverages, fruite juices, sport drinks are associated significantly with pH values, acidity,
content of fluor and phosphorus ions and enamel surface microhardness /195/. The erosive
properties of liquids are also associated to titratable acidity, acid quantity temperature and
buffering properties /142, 257, /.
The in vitro studies demonstrate that low pH beverages produce erosion to the level
of hard dental tissues /104,174,176 /. Also all tested sport drinks in personal research showed
erosive potential on enamel and dentine, sustaining the literature data/151/.
In personal study the sport drinks with lowest pH had the highest erosive potential
while drinks with high pH, reduced titratable acidity and higher concentrations of calcium,
phosphat and fluore ions present reduced erosive potential /210/.
The samples analysed by flow curves present inverse relation between viscosity and
shear rate due to high water quantity /166/. In personal study the sport drink with highest
viscosity (Gatorade) is not associated with highest erosive potential on enamel and dentine.
This result demonstrates that clearance rate does not influence the erosive properties of
beverages.
The citric acid and phosphoric acid present pronounced erosive effect on hard dental
tissues due to chelating properties on calcium ions/203,259,260/. The erosive potential of
sport drinks tested in personal study is also explained by the content of citric acid.
MI Paste plus combines milk phosphoproteins with calcium phosphate. The agent
CPP stabilises calcium ions and phosphat ions forming complexes with fast adsorbtion. The
same concept is associated to Recaldent product.

27
The classification of erosive potential of various beverages and foods accordingly to
their pH, titratable acidity, calcium, phosphat and fluor ions is complicated, if not impossible.
Also it must be considered behavioural factors and biological factors (eat and drinking habits,
diet content of fruits and vegetables, oral hygiene practices) and biological factors (salivary
rate, buffering ability, acquired pellicle, teeth anatomy).
IX.4. CONCLUSIONS
1. Highest pH value was found for sport drink CytoMax, followed by Isostar and
Gatorade.
2. Highest viscosity value was recorded for sport drink CytoMax, followed by
Gatorade and Isostar.
3. All three tested sport drinks determined the significant decrease of enamel and
dentine microhardness, as effect of their erosive potential on enamel and dentine.
4. Gatorade was associated with highest erosive effect on enamel and dentine,
followed by CytoMax and Isostar.
5. The use of fluor toothpaste, fluor gel MI Paste (caseine, calcium phosphate, fluor)
previous to immersion in sport drinks, reduced the erosive effects of sport drinks both for
enamel and dentine.
6. The most protective effect on enamel and dentine was recorded for MI Paste Plus,
followed by fluoride gel (fluoride gel Densell) and tooth paste (Colgate total).
7. Enamel microhardness associated to the previous use of remineralisation products
was significantly higher than dentine microhardness.

28
CHAPTER X. STUDY REGARDING KNOWLEDGES AND ATTITUDES OF DENTISTS ON DIAGNOSTIC AND TREATMENT OF DENTAL EROSIONS
X.1. AIM OF STUY
The aim of study was to assess the knowledges and attitudes of dentists from Iassy
regarding diagnostic and therapeutical management of dental erosions.
X.2. MATERIALS AND METHOD
A questionaire was send to 79 dentists working to private dental practices in Iassy.
The informations regarding sex, age, experience were collected.
The questionaire included, in first part, 15 questions regarding attitudes in diagnostic
of dental erosions, experience about prevalence, ethiological factors, preventive and
therapeutical means used, options regarding treatment techniques and materials.
Second part included a dental erosions clinical case with photos and anamnesis data
and questions regarding their preventive-therapeutical options and restoration type.
The dentists were classified in three classes of experience: 64 dentists with 0-5 years
experience, 6 dentists with 6-10 years experience and 9 dentists with over 10 years experience
(fig 10.1.). The age range was 25-58 years, and the sex distribution was 23 males, 56 females
(fig 10.2.).
The collected data were recorded, analysed and expressed using Microsoft Excel.
10.3. RESULTS AND DISCUSSIONS
The distribution of dentists opinions in entire study group and related to the
experience category (1-5 years; 6-10 years; over 10 years) is presented in the next graphs.
QUESTIONS I- DIAGNOSTIC ATTITUDE AND EXPERIENCE REGARDING PREVALENCE< DISTRIBUTION AND ETHIOLOGICAL FACTORS.
I.1. Do you record dental erosions in clinical papers?
85% dentists record dental erosions, 100% for 6-10 years experience, 88% for 0-5
years experience and only 56% for dentists over 10 years experience (fig.10.3.a-b).

29
Fig 10.3.a. Dental erosions recording (study group)
Fig 10.3.b.Dental erosion recording (experience)
I.2. What system do you use to record and assess dental erosions?
81% dentists use a simple system to assess dental erosions; 13% do not use any
system, only 6% use a complex system for the recording of dental erosions (Smith&Knight,
BEWE etc) (fig.10.4.a).
85%
15%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Da Nu
1.1
Da88%
Da100%
Da56%
Nu13%
Nu0%
Nu44%
0%
20%
40%
60%
80%
100%
120%
0-5 6-10 10+
1.1

30
Fig 10.4.a. Assessment systems of dental erosion (study group)
Simple assessing systems are used by 88% for 1-5 years experience, 67% for 6-10
years experience and only 44% for dentists over 10 years experience. Complex assessing
systems are used by 66% 6-10 years experience and over 10 years experience, 67% for 6-10
years experience and only 44% for dentists over 10 years experience (fig.10.4.b).
Fig 10.4.b. Assessment systems of dental erosions (experience)
I.8. From your experience, do you consider that actually prevalence of dental
erosions increased comparing with 5-10 years ago?
44% dentists consider that prevalence of dental erosions increased if repported
to 5-10 years ago, 56% can’t appreciate and only 3% consider that prevalence of dental
erosions remained at same level (fig.10.10.a).
81%
6%13%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Simplu Complex Niciunul
1.2
Simplu88%
Simplu67%
Simplu44%
Complex3%
Complex0%
Complex33%
Niciunul9%
Niciunul33%
Niciunul0%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0-5 6-10 10+
1.2

31
Fig 10.10.a. Prevalence dynamics of dental erosion (study group)
The opinion that prevalence of dental erosions increased was accounted for 38%
dentists with 0-5 years experience, 33% dentists with 6-10 years experience, 78% dentists
over 10 years; it can’t be appreciated for 59% dentists with 0-5 years experience, 67% dentists
with 6-10 years experience, 22% dentists with over 10 years experience (fig.10.10.b).
Fig 10.10.b. Prevalence dynamics of dental erosions (experience)
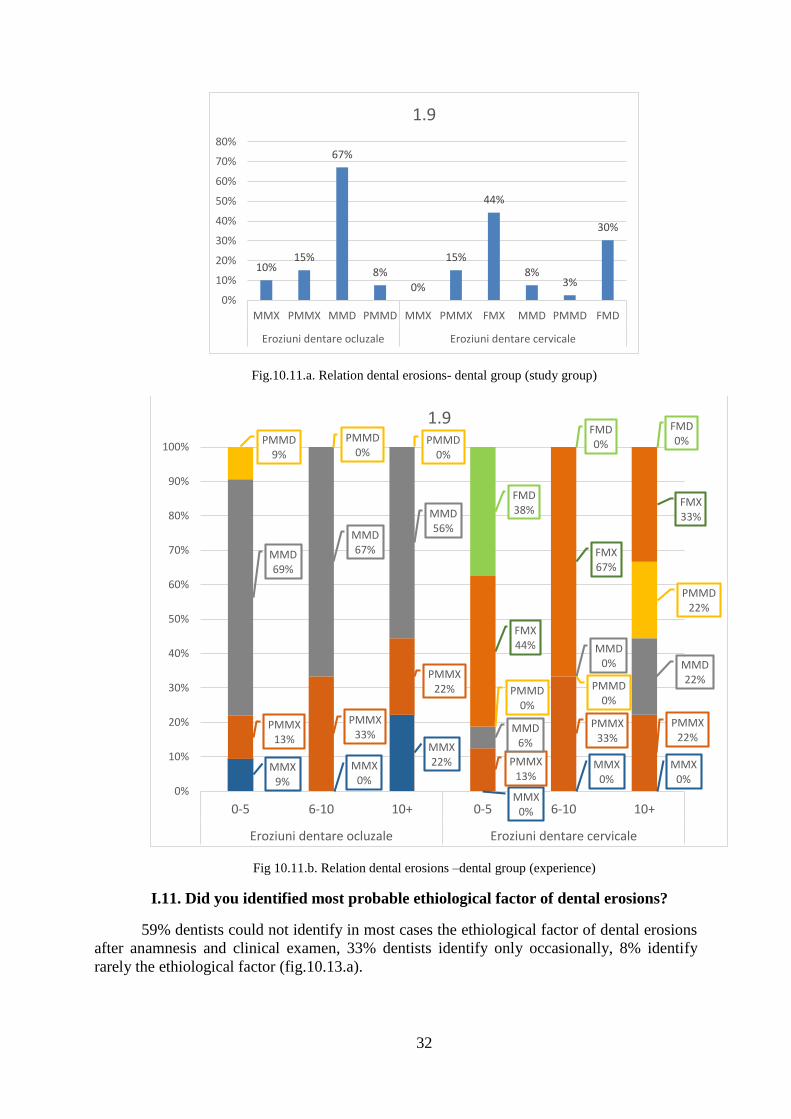
I.9. From your experience, what dental group do you consider as most affected
by dental erosions?
67% dentists consider that mandibular molars are most affected by occlusal
dental erosions, while 44% dentists consider that maxillary anterior teeth are most affected by
cervical erosions (fig.10.11.a).
42%
3%
56%
0%
10%
20%
30%
40%
50%
60%
Da Nu Nu am putut aprecia
1.8
Da38%
Da33%
Da78%
Nu3%
Nu0%
Nu0%
Nu am putut aprecia
59%
Nu am putut aprecia
67%
Nu am putut aprecia
22%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
0-5 6-10 10+
1.8
32
Fig.10.11.a. Relation dental erosions- dental group (study group)
Fig 10.11.b. Relation dental erosions –dental group (experience)
I.11. Did you identified most probable ethiological factor of dental erosions?
59% dentists could not identify in most cases the ethiological factor of dental erosions
after anamnesis and clinical examen, 33% dentists identify only occasionally, 8% identify
rarely the ethiological factor (fig.10.13.a).
10%15%
67%
8%
0%
15%
44%
8%3%
30%
0%
10%
20%
30%
40%
50%
60%
70%
80%
MMX PMMX MMD PMMD MMX PMMX FMX MMD PMMD FMD
Eroziuni dentare ocluzale Eroziuni dentare cervicale
1.9
MMX9%
MMX0%
MMX22%
MMX0%
MMX0%
MMX0%
PMMX13%
PMMX33%
PMMX22%
PMMX13%
PMMX33%
PMMX22%
MMD69%
MMD67%
MMD56%
MMD6%
MMD0% MMD
22%
PMMD9%
PMMD0%
PMMD0%
PMMD0%
PMMD0%
PMMD22%
FMX44%
FMX67%
FMX33%
FMD38%
FMD0%
FMD0%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0-5 6-10 10+ 0-5 6-10 10+
Eroziuni dentare ocluzale Eroziuni dentare cervicale
1.9

33
Fig.10.13.a.Identification of ethiological factors (study group)
Related to dentists with 0-5 years experience, 59% dentists can identify usually the
probable ethiological factor, 34% identify ocasionally, 6% identify rarely. Related to dentists
with over 10 years experience, 78% dentists can identify usually the probable ethiological
factor, while 22% identify rarely. (fig.10.13.b).
Fig 10.13.b.Identification of ethiological factors (experience)
QUESTIONS II- THERAPEUTICAL ATTITUDE, TECHNIQUES AND
MATERIALS USED FOR THERAPY OF DENTAL EROSIONS
II.1. Do you treat always, sometimes, never dental erosions?
42% dentists treat always the diagnosed dental erosions, 33% dentists treat some of
the diagnosed dental erosions, and 25% send patients to specialists if diagnose complex
pathology of dental erosions (fig.10.18.a).
59%
33%
8%
0%
10%
20%
30%
40%
50%
60%
70%
De obicei Ocazional Rar
1.11
De obicei59%
De obicei33%
De obicei78%
Ocazional34%
Ocazional67%
Ocazional0%
Foarte rar6% Foarte rar
0%
Foarte rar22%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
0-5 6-10 10+
1.11

34
Fig.10.18.a. Treatment decision in dental erosions (study group)
The dental erosions are treated always by 47% from dentists with 0-5 years
experience, 33% from dentists with over 10 years experience; the diagnosed dental erosions
are treated but not all by 25% dentists with 0-5 years experience and by 44% dentists with
over 10 years experience (fig.10.18.b).
Fig.10.18.b. Treatment decision in dental erosions (experience)
II.4. For patients with dental erosions what type of preventive/therapeutical
measures do you used?(scale from 1 to 8): A.Advices about oral hygiene; B.Advices
about diet; C.Correction of salivary rate; D. Fluoride mouthwashes; E. Fluoride gels; F.
CPP-ACP products (Recaldent, Tooth Mooth); G. Clorhexidine mouthwashes/gels;
H.Correction of systemic factors implied in dental erosions ethiology.
42%
33%
25%
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
Tratati intotdeuna toateeroziunile dentare
Tratati partialeorziuniledentare
Uneori trimiteti pacientiicu patologie complexa la
alti specialisti
2.1
47%
0%
33%25%
100%
44%28%
0%22%
0%
50%
100%
150%
0-5 6-10 10+
2.1
Tratati intotdeuna toate eroziunile dentare
Tratati partial eroziunile dentare
Uneori trimiteti pacientii cu patologie complexa la alti specialisti

35
Fig.10.21.a. Preventive/therapeutical measures (study group)
Fig.10.21.b. Preventive/therapeutical measures (experience)
The advices about oral hygiene (17%) and diet(16%) and fluoride mouthwashes
(13%) with are the most used preventive/therapeutical measures for patients with dental
erosions. There is no significant differences between dentists related to experience regarding
the investigated preventive and therapeutical measures (fig.10.21.a-b).
17%
16%
12%13%
11% 10%10%
11%
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
20%
A B C D E F G H
2.4
18% 17% 15%
16% 14% 13%
11%12% 21%
13% 14%14%
11% 11%7%
10% 10%13%
9% 10%9%
11% 11% 8%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0-5 6-10 10+
2.4Corectarea factorilorsistemici implicaţi înetiologia eroziunii dentareAdministrare de ape de gura și geluri ce conțin clorhexidinăAdministrare de geluri pebază de CPP-ACP
Administrare de geluri cufluor
Administrare de ape de gurăcu fluor
Corectarea ratei fluxuluisalivar

36
II. Do you treat cervical erosive lesions always, sometimes, never ?
Fig.10.23.a. Treatment of cervical dental erosion (study group)
67% dentists treat always and 33% treat sometimes cervical dental erosions
(fig.10.23.a).
Fig.10.23.b. Treatment of cervical erosive lesions (experience)
Regarding cervical erosive lesions and related to experience, 72% dentists with
0-5 years experience treat always, 28% sometimes; 56% dentists with over 10 years
experience treat always, 44% sometimes (fig.10.23.b).
67%
33%
0%0%
10%
20%
30%
40%
50%
60%
70%
80%
Intotdeuna Uneori NU
2.6
Intotdeauna72%
Intotdeauna33%
Intotdeauna56%
Uneori28%
Uneori67%
Uneori44%
Niciodata0%
Niciodata0%
Niciodata0%
0%
10%
20%
30%
40%
50%
60%
70%
80%
0-5 6-10 10+
2.6

37
II.7. What kind of materials do you use in treatment of dental erosions? (scale
from 1 to 7): A. Amalgam; B. Hibrid composite resins; C. Compomers; D.Glassionomer
cements; E. Ceramic veneers; F. Metal or ceramo-metal crowns.
Fig.10.24.a. Materials used in restorative therapy of dental erosions
(study group)
Fig.10.24.b Materials in restorative therapy of dental erosions (experience)
In the treatment of dental erosions, amalgam is most used by 17% dentists, followed
by composite resins (16%), compomers (16%) s glassionomer cements (15%). Dentists with
0-5 years experience used most frequently glassionomer cements (18%), dentists with 6-10
years experience used most frequently composite resins(19%), and dentists with over 10 years
experience used most frequently composites flow (19%) (fig.10.24.a-b).
Despite increasing focus of researchers on dental erosions, Dugmore&Rock (2003)
proved that most dentists motivate ocasionally or rarely patients to treat this pathology /68/.
17%16% 16%
15%
17%
8%
10%
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
20%
A B C D E F G
2.7
18%12%
16%
17%
19% 7%
16%
11%19%
14%
17%21%
07%
12%
11%
9%16%
12%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0-5 6-10 10+
2.7Coroane de înveliș
Fațete ceramică
Cimenturi glassionomere tradiționale
Compomeri
Compozite fluide
Rășini compozite
CGI mr

38
Mulic A&col. (2010; 2012) identified an improper level of informations regarding dental
erosions and erosive wear from dentists to patients included in risk categories /214, 215, 216/.
The personal study proved that actually the dentists working in private practices in
rare aware on the importance of dental erosion pathology, diagnostic possibilities and
treatment. However most dentists do not use a specific indices system to record dental
erosion. Also there are no uniform opinions regarding distribution of dental erosions in
relation to parameters like sex and age. However most dentists are aware that dental erosions
predominate to males patients age 15-25, associated with high consume of beverages and soft
drink, result similar with literature data /93, 189/.
The result of personal study sustain the results of Sabahipour L.&Bartlett D(2009)
which found that most dentists in Great Britain use composite resins as materials for the
therapy of dental erosions, while in Europe this percent reduces to 33%, 50% decide not to
treat teeth affected by dental erosions, and 10% treat with ceramo-metal crowns /261/.
10.4. CONCLUSIONS
Most dentists in private dental cabinet in Iassy are aware of the importance to
diagnose and treat dental erosions.
The ethiological factors is detected most by dentists with experience over 10 years
(78%).
Dentists consider that most affected teeth are mandibular molars (occlusal erosions)
and anterior maxillary teeth (cervical erosions).
The preventive-therapeutical measures related to oral hygiene advices, diet advices,
fluoride mouthwashes are largely used both by dentists under 5 years experience and
dentists over 10 years experience.
In therapy of dental erosions, amalgam is most used by 17% dentists, followed by
composite resins (16%), compomers (16%) glassionomer cements (15%).

39
GENERAL CONCLUSIONS
o The dental erosion prevalence is low (6%) with higher values (8%) in the male
population and smaller values (4%) in the female population.
o In relation to the age group, the highest values of dental erosion prevalence (8%) are
found at patients older than 35 years; the lowest values of dental erosion prevalence
are found at patients betweenthe ages of 18 to 25 years (4%).
o In relation to etiological factors, the highest values of dental erosion prevalence were
found at patients associated with consume of beverages and soft drinks; 75% of the
patients sample with dental erosion patients frequent consume beverages, soft drinks
and fruit juices.
o The highest mean BEWE values were found at patients consuming sport drinks
(BEWE 9); patients associated with consume of beverages and soft drinks have mean
BEWE 4.5. The BEWE mean value is higher for females (BEWE 5,2), patients over
35 years (BEWE 8.00), the sextants S4 and S6 (BEWE 1.25) and patients under
erosive mediacation (BEWE 8.00).
o Highest decrease of Ca and P ions from enamel surfaces was recorded for immersion
in lemon juice, followed by Red Bull, mineral water, apple juice and green tea;
o The presence of acquired salivary pellicle offered protection to enamel surfaces, as Ca
and P concentrations were less diminished comparing with the enamel surfaces
immersed in acid solutions in the absence of acquired salivary pellicle.
o Highest pH value was found for sport drink CytoMax, followed by Isostar and
Gatorade.
o Gatorade was associated with highest erosive effect on enamel and dentine, followed
by CytoMax and Isostar
o The use of fluor toothpaste, fluor gel MI Paste (caseine, calcium phosphate, fluor)
previous to immersion in sport drinks, reduced the erosive effects of sport drinks both
for enamel and dentine.
o The most protective effect on enamel and dentine was recorded for MI Paste Plus,
followed by fluoride gel (fluoride gel Densell) and tooth paste (Colgate total).
o Most of the private dental practitioners in Iași are well aware of the importance of
diagnosing and treatment of the tooth erosion.
o Preventive measures (advice on oral hygene, diet, and the use of mouth wash that
contain fluoride) are widely used by all three groups (0-5, 6-10, 10+ experience).
o In the dental erosion therapy, the amalgam material is the most used by 17% of the
people questioned, followed by composite resins (16%), compomer material (16%)

40
and CGI (15%). Dentists with 0-5 years of experience use most of the time CGI
(18%), the ones with 6-10 years of experience use composite resins (19%) and the
ones with over 10 years of experience use composite flow (19%).

41
SELECTIVE BIBLIOGRAPHY
2.Al-Dlaigan YH, Shaw L, Smith A Dental erosion in a group of British 14-year-old, school children Part
I: Prevalence and influence of differing socioeconomic backgrounds Br Dent J 2001 Feb 10;190(3):145-9.
5.Alvarez Loureiro L, Fabruccini Fager A, Alves LS, Alvarez Vaz R, Maltz M Erosive Tooth Wear
among 12-Year-Old Schoolchildren: A Population-Based Cross-Sectional Study in Montevideo, Uruguay
Caries Res 2015 Feb 28;49(3):216-225.
8.Amaechi BT, Ramalingam K, Mensinksai PK, Narjibfard K, Mackey AC, Karlinsey
RLRemineralization of eroded enamel by a NaF rinse containing a novel calcium phosphate agent in an in
situ model: a pilot study Clin Cosm Invest Dent 2010;2:93–100.
9.Andrian S Tratamentul minim invaziv al cariei dentare Editura Princeps Edit, Iaşi, 2002.
10.Arnadottir IB, Holbrook WP, Eggertsson H, Gudmundsdottir H, Jonsson SH, Gudlaugsson JO.
Prevalence of dental erosion in children: a national survey Community Dentistry Oral Epidemiology
2010;38:521–6.
11.Ashley P, Di Iorio A, Cole E, Tanday A, Needleman IOral health of elite athletes and association with
performance: a systematic review Br J Sports Med 2015 Jan;49(1):14-9.
16.Attin T, Meyer K, Hellwig E, Buchalla W, Lennon AM.Effect of mineral supplements to citric acid on
enamel erosion Arch Oral Biol 2003;48:753–759.
22.Balan A., Andrian S., Savin C., Sandu A.V., Petcu A., Stoleriu S. Comparative Study Regarding the
Effect of Remineralizing Products on Primary Teeth Dissolution Induced by Acidic Drinks. Revista de
chimie 2015; 66 (4): 562-564.
26.Barbour ME, Parker DM, Allen GC, Jandt KD: Human enamel erosion in constant composition citric
acid solutions as a function of degree of saturation with respect to hydroxyapatite J Oral Rehabil
2005a;32:16–21.
30.Bardsley PF, Taylor S, Milosevic A Epidemiological studies of tooth wear and dental erosion in 14-
year old children in North West England 1 The relationship with water fluoridation and social deprivation
Br Dent J 2004; 197:413–416.
47.Caruntu Irina-Draga“Histologia sistemului stomatognat”, Editura Apollonia, Iași, 2001: pag 17-76;
109-118.
51.Cheng ZJ, Wang XM, Cui FZ, Ge J, Yan JXThe enamel softening and loss during early erosion
studied by AFM, SEM and nanoindentation Biomed Mater 2009;4:1–7.
52.Chrysanthakopoulos NA Prevalence of tooth erosion and associated factors in 13-16-year old
adolescents in Greece J Clin Exp Dent 2012 Jul 1;4(3):160-6.
53.Cochrane NJ, Cai F, Huq NL, Burrow MF, Reynolds EC New approaches to enhanced
remineralisation of tooth enamel J Dent Res 2010;89:1187–1197.
56.Cosmin Arnăuţeanu, Simona Stoleriu, Gianina Iovan, Andrei Victor Sandu, Sorin Andrian,
Comparative Study Regarding the Impact of Saliva on Chemical Disolution of Enamel Induced by
Various Acidic Beverages, Revista de chimie 2013; 64 (11): 1324-1328.
58.Curcă M, Dănilă I Evaluarea leziunilor dentare necariogene în funcţie de indicii Smith&Knight
Revista Medico-Chirurgicalã 2010 nr2, vol114: 547-550.
69.Dugmore CR, Rock WP. A multifactorial analysis of factors associated with dental erosion. Br Dent J.
2004;196(5):283-6.
70.Dugmore CR, Rock WP. The progression of tooth erosion in a cohort of adolescents of mixed
ethnicity. Int J Paediatr Dent 2003 Sep;13(5):295-303.
76.El Aidi H, Bronkhorst EM, Huysmans MC, Truin GJ Multifactorial analysis of factors associated with
the incidence and progression of erosive tooth wearCaries Res2011;45(3):303-12.
77.El Aidi H, Bronkhorst EM, Huysmans MC, Truin GJ.Dynamics of tooth erosion in adolescents: a 3-
year longitudinal study J Dent 2010 Feb;38(2):131-7.
85.Field J, Waterhouse P, German M Quantifying and qualifying surface changes on dental hard tissues in
vitro J Dent 2010;38:182–190.

42
91.Francisco J, Lizerr CC, Jenifer MG, Jose MLC, Juan JSE Clinical measurement of tooth wear: Tooth
wear indices Journal of Clinical and Experimental Dentistry 2012; 4(1): 48-53.
93.Gambon DL, H S Brand, C Boutkabout, D Levie, E C I Veerman. Patterns in consumption of
potentially erosive beverages among adolescent school children in the Netherlands International Dental
Journal, 2011, vol 61(5):247–251.
96.Ganss C, Lussi A Diagnosis of erosive tooth wear Monogr Oral Sci 2014;25:22-31.
102.Ghiorghe A. Elemente de cariologie Edit.PIM, Iasi, 2008.
104.Grando LJ, Tames DR, Cardoso AC, Gabilan NH. In vitro study of enamel erosion caused by soft
drinks and lemon juice in deciduous teeth analysed by stereomicroscopy and scanning electron
microscopy. Caries Res.1996;30(5):373-8.
105.Gupta R, Prakash V CPP-ACP complex as a new adjunctive agent for remineralisation: a review Oral
Health Prevent Dent 2011;9:151–165.
128.Heurich E, Beyer M, Jandt KD, Reichert J, Herold V, Schnabelrauch M, Sigusch BW Quantification
of dental erosion – a comparison of stylus profilometry and confocal laser scanning microscopy (CLSM)
Dent Mater 2010;26:326–336.
131.Holbrook WP, Árnadóttir IB, Hlöðversson SO, Arnarsdóttir E, Jónsson SH, Sæmundsson SR The
Basic Erosive Wear Examination (BEWE) applied retrospectively to two studies Clin Oral Investig 2014
Jul;18(6):1625-9.
136.Hooper SM, Hughes JA, Newcombe RG, Addy M, West NX. A methodology for testing the erosive
potential of sports drinks. J Dent 2005;33:343–348.
142.Hughes JA, West NX, Parker DM,Newcombe RG, Addy M. Development and evaluation of a low
erosive blackcurrant juice drink in vitro and in situ. Comparison with orange juice. J Dent. 1999;
27(4):285-9.
147.Iliescu A, Gafar M – Cariologie şi odontoterapie restauratoare. Ed Medicală, Bucureşti, 2001.
148.Iovan G. Caria dentară. Repere etiologice si patogenice. EditUMF”GrTPopa”Iasi, 2011.
151.J. Rees, T. Loyn, R. McAndrew. The acidic and erosive potential of five sports drinks, European
Journal of Prosthodontic Restorative Dentistry, 2005, 13, 4:186-90.
152.Jaeggi T, Lussi APrevalence, incidence and distribution of erosion Monogr Oral Sci 2014;25:55-73.
160.Johansson AK, Johansson A, Birkhed D, Omar R, Baghdadi S, Carlsson GE. Dental erosion, soft-
drink intake, and oral health in young saudi men, and the development of a system for assessing erosive
anterior tooth wear. Acta Odontol Scand. 1996;54(6):369-78.
164.Kato MT, Leite AL, Hannas AR, Buzalaf MA: Gels containing MMP inhibitors prevent dental
erosion in situ. J Dent Res 2010;89:468–472.
166.Keshani, S., Luqman Chuah, A. ,Russly, A. R., Effect of temperature and concentration on the
rheological properties pomelo juice concentration, International Food Research Journal, 19(2), 2012, 553-
562.
168.Kreulen CM, van ‘t Spijker A, Rodriguez JM, Bronkhorst EM, Creugers NH, Bartlett DW.
Systematic review of the prevalence of tooth wear in children and adolescents Caries Res 2010;44:151–
159.
169.Kumar S, Acharya S, Mishra P, Debnath N, Vasthare RPrevalence and risk factors for dental erosion
among 11- to 14-year-old school children in South India Journal of Oral Science 2013;55:329–36.
174.Larsen MJ, Nyvad B. Enamel erosion by some soft drinks and orange juices relative to their pH,
buffering effect and contents of calcium phosphate. Caries Res. 1999;33(1):81-7.
176.Larsen MJ. Prevention by means of fluoride of enamel erosion as caused by soft drinks and orange
juice. Caries Res. 2001;35(3):229-34.
188.Lussi A, Jaeggi T, Jaeggi-Schärer SPrediction of the erosive potential of some beverages Caries Res
1995;29:349–354.
194.Lussi A, Schaffner M, Hotz P, Suter P. Dental erosion in a population of Swiss adults. Comm Dent
Oral Epidemio 2005;19(5):286- 290.
198.Manjunatha, S. S., Raju, P. S., Bawa, A. S., Modelling the rheological behaviour of enzyme clarified
Lime (Citrus aurantifolia L.) juice concentrate. Czech J. Food Sci., 2012, Vol.30, No. 5:456-466.

43
199.Manton DJ, Cai F, Yuan Y, Walker GD, Cochrane NJ, Reynolds C, Brearley-Messer LJ, Reynolds
EC. Effect of casein phosphopeptide-amorphous calcium phosphate added to acidic beverages on enamel
erosion in vitro. Aust Dent J 2010;55:275–279.
200.Margaritis V, Mamai-Homata E, Koletsi-Kounari H,Polychronopoulou A. Evaluation of three
different scoring systems for dental erosion: a comparative study in adolescents. Journal of Dentistry
2011;39:88–93.
202.Meurman JH, Frank RM Scanning electron microscopic study of the effect of salivary pellicle on
enamel erosion. Caries Res 1991;25(1):1-6.
203.Meurman JH, Harkonen M, Naveri H, Koskinen J, Torkko H, Rytomaa I, Jarvinen V, Turunen R.
Experimental sports drinks with minimal dental erosion effect. Scand J Dent Res 1990; 98: 120-128.
206.Micu Magdalena-Ioana Teza de doctorat Leziunile dentare necariogene-metode moderne de abordare
şi tratament UMF “Grigore TPopa” Iasi, 2010.
209.Milosevic A, Young PJ, Lennon MA The prevalence of tooth wear in 14-year-old school children in
Liverpool Comm Dent Health 1994; 11:83-86
210.Milosevic A. Sports drinks hazard to teeth. Br J Sports Med 1997; 31:28-30.
212.Moazzez R, Smith BG, Bartlett DW. Oral pH and drinking habit during ingestion of a carbonated
drink in a group of adolescents with dental erosion. J Dent. 2000;28(6):395-7.
214.Mulic A, A B Tveit, D Songe, H Sivertsen, A B Skaare Dental erosive wear and salivary flow rate in
physically active young adults BMC Oral Health, 2012,vol 12,no 1:1-8.
215.Mulic A, A B Tveit, L H Hove, A B Skaare. Dental erosive wear among Norwegian wine tasters Acta
Odontologica Scandinavica, 2010, vol 69, no 1:21–26.
216.Mulic A, SVidnes-Kopperud, AB Skaare, Tveit, A. Young Opinions on Dental Erosive Lesions,
Knowledge of Diagnosis, and Treatment Strategies among Norwegian Dentists:A Questionnaire Survey
Int J Dent 2012; vol.2012: 1-8.
217.Murrell S, Marshall TA, Moynihan PJ, Qian F, Wefel JS. Comparison of in vitro erosion potentials
between beverages available in the United Kingdom and the United States J Dent 2010;38:284–289.
219.Needleman I, Ashley P, Petrie A, Fortune F, Turner W, Jones J, Niggli J, Engebretsen L, Budgett R,
Donos N, Clough T, Porter S. Oral health and impact on performance of athletes participating in the
London 2012 Olympic Games: a cross-sectional study Br J Sports Med 2013 Nov;47(16):1054-8.
225.O’Brien M. Children’s dental health in the UK, 1993 London: HMSO.
229.Okunseri C, Okunseri E, Gonzalez C, Visotcky A, Szabo A. Erosive tooth wear and consumption of
beverages among children in the United States Caries Research 2011;45:130–5.
230.Olley RC, Wilson R, Bartlett D, Moazzez R. Validation of the Basic Erosive Wear Examination
Caries Res 2014;48(1):51-6.
234.Pancu G., Andrian S., Moldovanu A., Nica I., Sandu A.V., Stoleriu S. Effect of Some Food Intake on
Erosive Beverage Action on Dental Enamel and Cement. Materiale plastice 2014; 51(4): 428-431.
257.Rugg-Gunn AJ, Maguire A, Gordon PH,McCabe JF, Stephenson G. Comparison of erosion of dental
enamel by four drinks using an intra-oral appliance. Caries Res.1998;32(5):337-43.
259.S. Stoleriu, G. Iovan, A. Georgescu, A. V. Sandu, M. Roşca, S.Andrian. Study Regarding the Effect
of Acid Beverages and Oral Rinsing Solutions on Dental Hard Tissues. Revista de chimie,2012, 63, 1:68-
73.
260.S. Stoleriu, G. Iovan, G. Pancu, A. Georgescu, A. V. Sandu, S. Andrian. In vitro evaluation of acidic
beverages effect in dentine and cement, with and without storage in artificial saliva. Revista de materiale
plastice, 2014, 2:162-166.
261.Sabahipour L, D Bartlett A. questionnaire based study to investigate the variations in the
management of tooth wear by UK and prosthodontists from other countries. European Journal of
Prosthodontics and Restorative Dentistry, 2009,vol17(2):61–66.
262.Salas MM, Nascimento GG, Huysmans MC, Demarco FF. Estimated prevalence of erosive tooth
wear in permanent teeth of children and adolescents: an epidemiological systematic review and meta-
regression analysis. J Dent 2015 Jan;43(1):42-50.

44
268.Schlueter N, Hara A, Shellis RP, Ganss C. Methods for measurement and characterization of erosion
in enamel and dentine. Caries Res 2011;45(suppl 1):13–23.
272.Shellis RP, Ganss C, Ren Y, Zero DT, Lussi A Methodology and models in erosion
research:discussions and conclusions Caries Research 2011; 45:69–77.
274.Shen P, Manton DJ, Cochrane NJ, Walker GD, Yuan Y, Reynolds C, Reynolds EC.Effect of added
calcium phosphate on enamel remineralization by fluoride in a randomized controlled in situ trial J Dent
2011;39:518–525.
275.Simona Stoleriu, Gianina Iovan, Andrei Georgescu, Andrei Victor Sandu, Mihaela Roşca, Sorin
Andrian, Study Regarding the Effect of Acid Beverages and Oral Rinsing Solutions on Dental Hard
Tissues, Revista de chimie 2012; 63 (1): 68-73.
276.Simona Stoleriu, Gianina Iovan, Galina Pancu, Andrei Georgescu, Andrei Victor Sandu, Sorin
Andrian, In vitro evaluation of acidic beverages effect in dentine and cement, with and without storage in
artificial saliva, Revista de materiale plastice 2014 2: 162-166.
279.Srinivasan N, Kavitha M, Loganathan SC Comparison of the remineralization potential of CPP-ACP
and CPP-ACP with 900 ppm fluoride on eroded human enamel: an in situ study. Arch Oral Biol 2010;
55:541–544.
280.Steiner-Oliveira C, Nobre-dos-Santos M, Zero DT, Eckert G, Hara AT Effect of a pulsed CO2 laser
and fluoride on the prevention of enamel and dentine erosionArch Oral Biol 2010 Feb;55(2):127-33.
287.van Rijkom HM, Truin GJ, Frencken JE, Konig KG, van’t Hof MA, Bronkhorst EM, Roeters FJ
Prevalence, distribution and background variables of smooth-bordered tooth wear in teenagers in The
Hague, The Netherlands Caries Res 2002; 36: 147–154.
289.Vanuspong W, Eisenburger M, Addy MCervical tooth wear and sensitivity: erosion, softening and
rehardening of dentine; effects of pH, time and ultrasonication J Clin Periodontol 2002;29:351–357.
290.Vargas-Ferreira F, Praetzel JR, Ardenghi TM Prevalence of tooth erosion and associated factors in
11–14-year-old Brazilian schoolchildren Journal of Public Health Dentistry 2011;71:6–12.
291.Vered Y, Lussi A, Zini A, Gleitman J, Sgan-Cohen HD Dental erosive wear assessment among
adolescents and adults utilizing the basic erosive wear examination (BEWE) scoring system Clin Oral
Investig 2014 Nov;18(8):1985-90.
298.Wang P, Lin HC, Chen JH, Liang HY The prevalence of dental erosion and associated risk factors in
12–13-year-old school children in Southern China. BMC Public Health 2010;10:478.
299.Wang X, Megert B, Hellwig E, Neuhaus KW, Lussi A Preventing erosion with novel agents. J Dent
2011; 39:163–170.
302.West NX, Hughes JA, Addy M. The effect of pH on the erosion of dentine and enamel by dietary
acids in vitro. J Oral Rehabil 2001;28:860–864.
305.Wiegand A, Attin TDesign of erosion/abrasion studies: insights and rational concepts. Caries
Research 2011;45: 53-59.
310.Wiegand A, Hiestand B, Sener B, Magalhaes AC, Roos M, Attin T Effect of TiF4, ZrF4, HfF4 and
AmF on erosion and erosion/abrasion of enamel and dentin in situ Arch Oral Biol. 2010;55:223–228.
322.Zahara AM, Tee LM, Hazirah MA, Selvamary S, Phor YJ, Hasnani IN, Ying YB, Seng YE, Asyikin
YNRelationship between Food Habits and Tooth Erosion Occurrence in Malaysian University Students
Malays J Med Sci 2012 Apr-Jun; 19(2): 56–66.
323.Zebrauskas A, Birskute R, Maciulskiene VPrevalence of Dental Erosion among the Young Regular
Swimmers in Kaunas, Lithuania J Oral Maxillofac Res 2014 Jul 1;5(2):e6.





























