Embed Size (px)
Citation preview

Central Journal of Liver and Clinical Research
Cite this article: Marroni CA, Bona S, Fleck Junior AM, Moreira AJ, Mariante-Neto G, et al. (2016) Clinical and Experimental Alcoholic Liver Disease. J Liver Clin Res 3(2): 1028.
*Corresponding authorClaúdio Augusto Marroni. Rua José Kanan Aranha, 102 - Porto Alegre - RS – Brazil, CEP: 91760470; Tel: 55-5199643011; Fax: 55-5132483202; Email: [email protected]
Submitted: 29 September 2016
Accepted: 02 Novemebr 2016
Published: 11 Novemebr 2016
ISSN: 2379-0830
Copyright© 2016 Marroni et al.
OPEN ACCESS
Keywords•Alcohol•Alcoholic liver disease•Epidemiology; disability-adjusted life years•Risk factors•Non-invasive tests•Cirrhosis•Pathology•Biomarkers•Physiopathology•Experimental models
Review Article
Clinical and Experimental Alcoholic Liver DiseaseMarroni CA1, Bona S2, Fleck Junior AM3, Moreira AJ4, Mariante-Neto G5, Rodrigues G6, Marroni CP7, Coral GP8, Ayres R9, Schneider ACR10, da Silveira TR11, Brandão ABM12, and Marroni NP13
1Department of Hepatology, Universidade Federal de Ciências da Saúde de Porto Alegre, Brazil 2Department of Medical Sciences: Medicine, Universidade Federal do Rio Grande do Sul, Brazil3Department of Hepatology, Universidade Federal de Ciências da Saúde de Porto Alegre, Brazil4Department of Biological Sciences, Universidade Federal do Rio Grande do Sul, Brazil5Department of Hepatology, Universidade Federal de Ciências da Saúde de Porto Alegre, Brazil6Department of Medicine, Universidade Federal do Rio Grande do Sul, Brazil7Department of Hepatology, Universidade Federal de Ciências da Saúde de Porto Alegre, Brazil8Department of Internal Medicine-Gastroenterology, Universidade Federal de Ciências da Saúde de Porto Alegre, Brazil9Department of Adolescent Health, Universidade Federal do Rio Grande do Sul, Brazil10Department of Medical Science- Gastroenterology, Universidade Federal do Rio Grande do Sul, Brazil11Department of Gastroenterologist, Universidade Federal do Rio Grande do Sul, Porto Alegre-RS, Brazil12Department of Hepatology, Universidade Federal de Ciências da Saúde Brazil. 13Department of Biological Sciences: Physiology, Universidade Federal do Rio Grande do Sul, Brazil
Abstract
Alcoholism, or alcohol use disorder is a chronic relapsing medical disease of the brain, and alcoholic liver disease is an important public health problem worldwide implicated in million deaths annually, in millions of disability-adjusted life years (DALY), and has neuro-psychological distress. The complete physiopathology of alcoholic liver disease is still unknown and has implications in ideal experimental models. There has been little progress in the management of alcoholic liver disease, and there are no modern diagnostic tools to assess individual susceptibility to the development of alcoholic liver disease in patients with severe clinical conditions. No drugs for alcoholic liver disease (ALD) have been successfully developed in recent years, and this poor therapeutic progress has resulted from a lack of experimental models of advanced ALD. It is difficult to perform clinical trials in patients with an active addiction. The most important therapeutic action is abstinence. The development of new experimental models is fundamental in order to advance new physiopathological and therapeutic targets of alcoholic liver disease based in new concepts and techniques. Future areas of investigation should take into account the patient’s genome, genetics in general, and epigenetics to evaluate alcohol’s actions in real time and treatment targets for ALD. Such information provides elements that allow health authorities and professionals to take optimal decisions in the public health sphere.
ABBREVIATIONSDALY: Disability-Adjusted Life Years; ALD: Alcoholic Liver
Disease; GBD: Global Burden Of Disease; NHANES III: Third National Health And Nutrition Examination Survey; WHO: World Health Organization; NASH: Non-Alcoholic Steatohepatitis; MAST: Michigan Alcoholism Screening Test; AUDIT: Alcohol Use Disorders Identification Test; AASLD: American Association For The Study Of Liver Diseases; AHHS: Alcoholic Hepatitis Histological Score; MELD: Model For End-Stage Liver Disease; PT: Prothrombin Time; INR: International Normalized Ratio; HCC: Hepatocellular Carcinoma; AST: Aspartate Aminotransferase;
ALT: Alanine Aminotransferase; GGT: Gamma-Glutamyl Transpeptidase; AH: Alcoholic Hepatitis; CDT: Carbohydrate-Deficient Transferring; MCV: Mean Corpuscular Volume; ESR: Erythrocyte Sedimentation Rate; LSM: Liver Stiffness Measurement; US: Ultrasound; CT: Computed Tomography Scan; MRI: Magnetic Resonance Imaging; ESPEN: European Society For Clinical Nutrition And Metabolism; AASLD: American Association For The Study Of Liver Diseases; ACG: American College Of Gastroenterology; AAU: Alcohol Addiction Unit; CNS: Central Nervous System; CS: Corticosteroids; PTX: Pentoxifylline; TNF-Α: Tumor Necrosis Factor Alpha; HRS: Hepatorenal Syndrome;

Central
Marroni et al. (2016)Email:
J Liver Clin Res 3(2): 1028 (2016) 2/24
NAC: N-Acetylcysteine; LT: Liver Transplant; EASL: Study Of The Liver; LPS: Lipopolysaccharide; Kcs: Activation Of Kupffer Cells; ROS: Reactive Oxygen Species; ER: Endoplasmic Reticulum; Tgfß1: Transforming Growth Factor B1; PDGF: Platelet-Derived Growth Factor; GSH: Glutathione; NF-Κb: Nuclear Factor Kappa B; MAPK: Mitogen-Activated Protein Kinase; NOS: Nitric Oxide Synthase; COX-2: Cyclooxygenase-2; NO: Nitric Oxide; PGE2: Prostaglandin E2; MDA: Malondialdehyde; SOD: Superoxide Dismutase; Gpx: Glutathione Peroxidase; Nrf2: Nuclear Factor (Erythroid-Derived 2)-Like 2; UPR: Unfolded Protein Response; Bip: Binding Immunoglobulin Protein; GRP78: Glucose-Regulated Protein 78; IRE: Inositol Requiring; PERK: PKR-Like ER Kinase; ATF: Activating Transcription Factor; JNK: C-Jun N-Terminal Kinase; TLR: Toll-Like Receptor; GIT: Gastrointestinal Tract: TLR4: Toll-Like Receptor 4; LCFA: Long-Chain Fatty Acids; OPN: Osteopontin; Mtorc1: Mammalian Target Of Rapamycin Complex 1; TFEB: Nuclear Transcription Factor EB; Ampk: Adenosine Monophosphate-Activated Protein Kinase; SIRT: Sirtuins; Inos: Inducible Nitric Oxide Synthase; Hifs: Hypoxia-Inducible Factors.
INTRODUCTIONAlcoholism is still considered by many individuals and
clinicians as a bad habit; however, research in neuroscience has improved dramatically recent decades, and it is now known that alcoholism is a chronic relapsing medical disease of the brain, not a bad habit [1-3]. Alcoholism, or alcohol use disorder, is defined by the Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5) [4], as a problematic pattern of alcohol use that leads to clinically significant impairment or psychological distress. There has been little progress in the management of alcoholic liver disease in patients with severe clinical conditions, and there are no modern diagnostic tools to assess individual susceptibility to the development of alcoholic liver disease (ALD). Moreover, the pathogenesis of ALD in humans is incompletely understood [5].
No drugs for ALD have been successfully developed in recent years, and this poor therapeutic progress has resulted from a lack of experimental models of advanced ALD [5,6]. It is difficult to perform clinical trials in patients with an active addiction [5]. Moreover, there are no approved antifibrotic drugs to prevent disease progression in patients with moderate ALD [5].
Epidemiology of Alcoholic Liver Disease: A Global Perspective
A large proportion of publications on the epidemiology of ALD consider data on cirrhosis, probably because this condition is more easily diagnosed. Thus, death from cirrhosis is often used as an index, but it is impossible to reliably separate the data for death from cirrhosis in general to that related specifically to the consumption of alcohol (Table 1) [7]. It should be highlighted that both retrospective and prospective studies have limitations, including a lack of both reliability and standardization of the information collected on (i) the consumption of alcoholic beverages; (ii) the types of beverage consumed; (iii) the amounts ingested; (iv) drinking habits, etc [7,8]. Therefore, at present, our best estimates on the size of the effect of ALD on mortality rates should be interpreted with caution [7]. It is estimated that alcohol is responsible for approximately 2.7 million
deaths annually and 3.9% of disorders in general, also being implicated in 4.6% of disability-adjusted life-years (DALYs) lost due to premature death [7,9]. Although most adults do not drink alcoholic beverages, it is estimated that almost half the world population consumed some form of alcohol in 2012 [10]. A matter of concern is the finding that fewer than half of the individuals with alcohol-related problems are diagnosed by their physicians, with women and older people being less likely to be identified and cared for [11]. In Brazil, a study evaluating alcohol intake among patients of the family heath teams in a southeast city concluded that alcohol consumption is frequent among the patients cared for at the basic health units and is little recognized by health agents [12]. The Global Burden of Disease (GBD) study showed that more than one million deaths around the world (1,030,800 deaths, accounting for 2.0% of all deaths, 1.4% of all deaths of women and 2.4% of all deaths of men) and 31,027,000 DALYs (1.2% of all DALYs, 0.8% of all DALYs for women and 1.6% of all DALYs for men) could be ascribed to cirrhosis of any etiology [13,14], DALY represents a measure of the extent of a disease and is defined as the sum of years of life lost due to early death and years of life lost from disability [10]. Another 752,100 deaths (accounting for 1.4% of all deaths) and 19,111,000 DALYs (0.8% of all DALYs) were due to liver cancer [13,14]. In the study evaluating specifically the weight of liver diseases associated with abuse of alcohol [10], it was found that the extent of both affections (cirrhosis and liver cancer) was more pronounced in males. Of the totality of deaths from cirrhosis, 493,300 were ascribed to alcohol (47.9% of all deaths from cirrhosis), representing 0.9% of all deaths from any cause. In addition, worldwide, 7.2 deaths/100,000 people (4.6 deaths/100,000 women and 9.7 deaths/100,000 men) were caused by alcoholic cirrhosis in 2010 [10]. In this series, the number of deaths from cirrhosis, corrected for population size, ascribed to alcohol consumption was much greater among individuals 65 years of age or older (31.1 deaths/100,000 people) compared to individuals 15-34 years (1.0 death/100,000 people) and 35–64 years of age (13.1 deaths/100,000 people) ; this result was found for both genders [10]. Concerning relative contribution, the impact of alcoholic cirrhosis was greater in the 35-64 years age bracket (62.1%). DALYs lost to cirrhosis (corrected for population size) and related to alcohol consumption were higher in individuals 35-64 years of age (459.4 DALYs/100,000 people), compared to individuals 15-34 years of age (59.7 DALYs/100,000 people) and 65 years or older (448.5 DALYs/100,000 people). The connection between DALYs and alcoholic cirrhosis was found for both men and women [10].
In Latin America, a study concluded that alcohol consumption is far higher than the world average [15]. According to the
Table 1: Alcoholism and Alcoholic Liver Disease.1. Alcoholism is a chronic relapsing medical disease of the brain, not a bad habit2. The studies about alcoholism and ALD have limitations (lack reliability and standardization of informations)3. The date do not reflect accurately the actual extent of the real problem of ALD4. ALD is an important cause of morbility and mortality across the globe5. Harm reduction measures are efficacious, cost-effective and needed

Central
Marroni et al. (2016)Email:
J Liver Clin Res 3(2): 1028 (2016) 3/24
GBD, Central America showed the second highest death rate ascribed to alcoholic cirrhosis: 15.8 deaths/100,000 people (7.8 deaths/100,000 women, and 23.6 deaths/100,000 men) [10, 13]. In Mexico [16], it is estimated that almost two million cases of chronic liver disease will be diagnosed by 2050 and that ALD will be the most prevalent. In Brazil, specifically, 54% of the population consumes alcoholic beverages on a regular basis, i.e., at least once a week [17]. Liver disease is the eighth leading cause of death in Brazil, behind infectious and parasitic diseases. [18] Between 2001 and 2010, there were 117,979,343 hospital admissions in Brazil. Of these, 853,571 were due to liver disease, which corresponds to 0.72%. Of all hospitalizations due to liver disease, 573,293 (67.16%) involved male patients and 280,275 [32.83%] involved female patients (P < 0.001). The mean age at hospital admission for liver disease was 48.05 years. The absolute number of hospital admissions due to liver disease in Brazil has been on the rise, especially since 2007 [18]. Recent data indicate that, in Brazil, alcoholic and non-viral cirrhosis were responsible for 3% and 1% of total DALYs, respectively. In both diseases, men contributed to a greater proportion of DALYs. Among the first ten causes of DALYs, alcohol use disorders occupied the second, third and sixth positions at the ages of 15-29, 30-44 and 45-59, respectively [19].
In the United States of America (USA), cirrhosis was the twelfth leading cause of death in 2000, accounting for 1.1% of all deaths, with a rate adjusted for population age of 9.6/100,000 [20], ALD is one of the main causes of death [21-23]. One study used population data of the Third National Health and Nutrition Examination Survey (NHANES III) to assess the impact of ALD on overall mortality and cause-specific mortality in the general USA population. This study showed that patients with ALD are at increased risk for liver-related death [24]. In the USA, the prevalence of drinking increased between 2001–2002 and 2012–2013, as did the volume and frequency of drinking and the prevalence of monthly heavy episodic drinking among drinkers. These increases were greater for women than men for all measures. In contrast, the increases were smaller for consumption among drinkers among the married individuals. The increase in overall drinking prevalence was magnified among all race-ethnic minorities, whereas the increase in ≥ monthly consumption was magnified only among blacks (all relative to whites) [25].
ALD is the most prevalent cause of advanced liver disease in Europe [7]. Its extent in the continent, with 6.5% of all deaths and 11.6% of DALYs ascribed to alcohol, is the largest among the regions considered by the World Health Organization (WHO) [7,26]. The death rates ascribed to alcohol are higher in men [11%] than in women (1.8%). The impact of alcoholic disease is greater among young people, where mortality associated with alcohol is above 10% and 25% in females and males, respectively [7]. Death rates from cirrhosis, however, vary considerably and mortality trends show quite heterogeneous patterns across countries for the last 30 years. Regardless, it seems clear that Eastern Europe countries have the highest death rates [7]. About half the countries in Europe, including Austria, France, Germany, Italy, Portugal, Denmark [27] and Spain, as well as Eastern Europe countries (Hungary and Romania), exhibited sharp falls in mortality. In contrast, Western countries, Finland, Ireland and United Kingdom, as well as most of Eastern Europe,
including Estonia, Lithuania, Poland and Russia, have rising rates. As regards alcohol-related hospital admissions, for instance, alongside the rise in death from cirrhosis, there was a sharp increase in admission rates to intensive care unit (ICUs) and general hospitals in the United Kingdom [7]. Eastern Europe showed the highest intake of alcohol per capita, with 15.7 L total consumption per individual (8.1 L for women and 24.9 L for men [10]. Central Europe showed the highest proportion of deaths from alcoholic cirrhosis and of DALYs ascribed to alcohol [10]. Central Asia has the highest number of deaths from cirrhosis due to alcohol per 100,000 people: 17.5 deaths/100,000 people (14.6 deaths/100,000 for women and 20.4 deaths/100,000 for men) [10]. Additionally, data for Central Asia shows 546 DALYs/100,000 individuals (435.1 DALYs/100,000 women and 655.0 DALYs/100,000 men), followed by Eastern Europe, with 456.1/DALYs per 100,000 population [10].
In contrast, Northern Africa and Middle East showed the smallest proportion of deaths from cirrhosis and DALYs ascribed to alcohol consumption, with 14.0% of all deaths from liver cirrhosis and 15.9% of all DALYs from alcoholic cirrhosis [10].
Even with data that perhaps do not reflect accurately the actual extent of the problem, ALD is an important cause of morbidity and mortality across the globe [7,10]. Therefore, harm reduction measures are efficacious, cost-effective, and needed [10].
Risk Factors
There is a clear dose relationship between the amount of alcohol and the likelihood of developing ALD. Alcoholic steatosis can be found in 60% of individuals who drink >60 g of alcohol per day, and the risk of developing cirrhosis is highest in those with a daily consumption of above 120 g of alcohol [28,29]. However, lower daily amounts of alcohol may also lead to significant liver injury in some individuals. The consumption of >40 g of alcohol per day increases the risk of progression to liver cirrhosis to 30% in patients with uncomplicated alcoholic fatty liver and to 37% in those with established alcoholic fibrosis [30]. The amount of alcohol ingested is the most important risk factor for the development of ALD; however, the likelihood of developing progressive alcohol-induced liver disease or cirrhosis is not exclusively dose-dependent is it occurs in only a subset of patients [31]. The risk of developing cirrhosis increases with the ingestion of >60-80 g/day of alcohol for 10 years or longer in men and >20 g/day in women [29,32]. Yet, even drinking at these levels, only 6%-41% of individuals develop cirrhosis [20,32]. A recent consensus meeting concluded that, for the purposes of candidate eligibility in non-alcoholic steatohepatitis [NASH] clinical trial, significant alcohol consumption should be defined as >21 drinks per week in men and >14 drinks per week in women over a 2-year period prior to baseline liver histology [33]. One drink “unit”, or one standard drink, is equivalent to a 12-ounce beer, a 4-ounce glass of wine, or a 1-ounce shot of hard liquor [33]. Furthermore, this consensus group recommended that validated questionnaires should be used to quantify the amount of alcohol consumption in the context of clinical trials. A number of risk factors have been identified that influence the risk of development and progression of liver disease. It is unclear whether the effect of different beverages on disease risk is direct

Central
Marroni et al. (2016)Email:
J Liver Clin Res 3(2): 1028 (2016) 4/24
or related to confounding factors, such as diet. Patterns of drinking vary substantially among patients with ALD and may influence the risk of ALD [7]. Drinking outside of meals increases the risk of ALD compared to drinking only with meals [29,34]. Studies in humans have demonstrated that women are more susceptible to the hepatotoxic effects of alcohol and develop ALD more quickly than men with equal daily alcohol consumption [28, 35-38]. The pathophysiology behind this increased sensitivity to alcohol is not fully understood, but it is probably related to estrogens and their synergistic impact on oxidative stress and inflammation [39]. Several studies have shown differing blood alcohol levels in women versus men after consumption of equal amounts of alcohol [40]. This result might be explained by differences in the relative amount of gastric alcohol dehydrogenase, a higher proportion of body fat in women, or changes in alcohol absorption with the menstrual cycle [41]. Studies of twins have indicated the importance of genetic susceptibility to ALD, demonstrating that monozygotic twins have a higher concordance rate for alcohol-related cirrhosis than dizygotic twins [42,43].
There are notable differences in the prevalence of ALD and associated mortality among different ethnic groups [32,44,45]. The highest mortality rates of alcoholic patients with cirrhosis for men are found in white Hispanics, followed by black non-Hispanics, white non-Hispanics, and black Hispanics. In women, this order is black non-Hispanics, white Hispanics, white non-Hispanics, and black Hispanics [46]. However, it remains unclear whether ethnic differences in rates of alcoholic cirrhosis and ALD are due to genetic differences, differences in the amount and type of alcohol consumed, or differences in socioeconomic status and access to medical care [7]. The presence and extent of protein calorie malnutrition play an important role in determining the outcome of patients with ALD [31]. Mortality increases in direct proportion to the extent of malnutrition, approaching 80% in patients with severe malnutrition [i.e., less than 50% of normal] [47]. Obesity and excess body weight have been associated with an increased risk of ALD [47,48].
There is a clear synergistic relationship between chronic viral hepatitis and alcohol, with more advanced liver disease resulting when these factors occur jointly rather than separately. The combination of hepatitis C virus infection and alcohol predisposes individuals to more advanced liver injury than alcohol alone [50,51], causing disease at a younger age, more severe histological features, and a decreased survival[52]. In a large cohort study of the effect of heavy alcohol abuse in patients with post-transfusion hepatitis C, the risk of cirrhosis was elevated 30-fold [53]
Lastly, polymorphisms in genes involved in the metabolism of alcohol (including alcohol dehydrogenase, acetaldehyde dehydrogenase and the cytochrome P450 system) and in those that regulate endotoxin-mediated cytokine release have been associated with ALD [54,55]. However, to date, specific genetic abnormalities for susceptibility to alcohol abuse and the development of ALD have not been firmly established [31]. There is strong evidence supporting genetic background as an important modulator of the susceptibility to alcoholic hepatopathy, with the allele PNPLA3 rs738409 being the first confirmed genetic risk factor [5].
Diagnosis
A thorough clinical history, especially with regard to the amount of alcohol consumption, is essential for determining the role of alcohol in the etiology of abnormal liver test results.
Obtaining an accurate alcohol use history in patients with suspected alcoholic liver disease can be difficult because many patients do not readily admit to heavy alcohol use. In some cases, speaking with the patient’s family or friends may help in obtaining a more accurate history. Patients should be asked about their pattern of alcohol use, the type of alcohol consumed, and the amount of alcohol ingested [56].
Various questionnaires have been used to detect alcohol dependence or abuse and include the CAGE, the Michigan Alcoholism Screening Test (MAST), and the Alcohol Use Disorders Identification Test (AUDIT) [57,58]. The use of a structured interview, using instruments such as the Lifetime Drinking History, is often used as a gold standard for quantifying lifetime alcohol consumption [59]. The CAGE questionnaire [Table 2] was originally developed to identify hospitalized in patients with alcohol problems and remains among the most widely used screening instruments [31,60]. This tool has been faulted, however, on several measures: it focuses on the consequences of alcohol consumption rather than on the amount of actual drinking. Moreover, it refers to lifetime patterns of behavior rather than short-term or recent changes. Its virtues, however, include its ease of implementation [61].
The AUDIT (Table 3) is a 10-item questionnaire developed by the WHO to avoid ethnic and cultural bias and focuses on the identification of heavy drinkers [62]. It has a higher sensitivity and specificity than shorter screening instruments (with a sensitivity ranging from 51%-97% and a specificity of 78%-96% in primary care) [63]. It has been suggested that the AUDIT has three advantages over other screening tests: (i) it can identify drinkers at risk who are not yet alcohol-dependent; (ii) it includes a measure of consumption; and lastly, (iii) it includes both current and lifetime drinking time spans. The AUDIT is more likely to detect problem drinking before overt alcohol dependence or abuse might be diagnosed and thus may be more robust and effective across a variety of populations [64-66].
Clinical and laboratory features are often adequate for establishing the diagnosis of ALD in a patient with a history of significant alcohol use, provided the patient does not have risk factors for other causes of liver disease and testing for other common causes of liver disease is negative[56]. Biochemical tests have been considered to be less sensitive than questionnaires in screening for alcohol abuse [57,67], but may be useful in identifying relapse[68,69].
Table 2: The CAGE Questionnaire (60).
1. Have you ever felt you should cut down on your drinking?
2. Have people annoyed you by criticizing your drinking?
3. Have you ever felt bad or guilty about your drinking?4. Have you ever had a drink first thing in the morning to steady your nerves or to get rid of a hangover (eye-opener)?

Central
Marroni et al. (2016)Email:
J Liver Clin Res 3(2): 1028 (2016) 5/24
Table 3: AUDIT Questionnaire (260).
Questions 0 1 2 3 4
1. How often do you have a drink containing alcohol? Never Monthly or less 2 to 4 times a month 2 to 3 times a week
4 or more times a week
2. How many drinks containing alcohol do you have on a typical day when you are drinking? 1 or 2 3 or 4 5 or 6 7 to 9 10 or more
3. How often do you have 5 or more drinks on one occasion? Never Less than monthly Monthly Weekly Daily or almost
daily4. How often during the last year have you found that you were not able to stop drinking once you had started?
Never Less than monthly Monthly Weekly Daily or almost daily
5. How often during the last year have you failed to do what was normally expected of you because of drinking?
Never Less than monthly Monthly Weekly Daily or almost daily
6. How often during the last year have you needed a first drink in the morning to get yourself going after a heavy drinking session?
Never Less than monthly Monthly Weekly Daily or almost daily
7. How often during the last year have you had a feeling of guilt or remorse after drinking? Never Less than monthly Monthly Weekly Daily or almost
daily8. How often during the last year have you been unable to remember what happened the night before because of your drinking?
Never Less than monthly Monthly Weekly Daily or almost daily
9. Have you or someone else been injured because of your drinking? No Yes, but not in the
last yearYes, during the
last year10. Has a relative, friend, doctor or other health care worker been concerned about your drinking or suggested you cut down?
No Yes, but not in the last year
Yes, during the last year
TotalTo score the AUDIT questionnaire, sum the scores for each of the 10 questions. A total ≥ 8 for men up to age 60, or ≥4 for women, adolescents, or men over age 60 is considered a positive screening test.
Both the physical findings and laboratory evidence for ALD may be non-diagnostic, especially in patients with mild ALD or early cirrhosis [70]. No single laboratory marker definitively establishes alcohol to be the etiology of liver disease. Furthermore, alcohol may be one of a number of factors causing liver injury, and the specific contributory role of alcohol alone may be difficult to assess in a patient with multi factorial liver disease [31]. ALD may be suspected in a patient with a compatible history who has elevated serum transaminases, a suggestion of fatty liver on imaging tests, or who is found to have steatosis on liver biopsy. Liver tests are generally normal or modestly elevated, and jaundice is unusual. The diagnosis is established after excluding other causes of fatty liver or cirrhosis [56]. The 2010 American Association for the Study of Liver Diseases [AASLD] clinical practice guideline for ALD recommends the following for diagnosis [31]. If alcohol abuse or excess is suspected from a discussion of alcohol use with the patient, screen the patient for alcohol abuse using a structured questionnaire, such as the AUDIT;
If the patient’s history or a screening test indicates alcohol abuse, use laboratory testing to verify the diagnosis of ALD and rule out other considerations;
If ALD is confirmed, test for other alcohol-related organ damage.
Fatty liver occurs commonly after the ingestion of a moderate or large amount of alcohol, even for a short period of time. Alcohol-induced steatosis usually is asymptomatic in ambulatory patients.
Severe fatty infiltration of the liver can result in symptoms of malaise, weakness, anorexia, nausea, and abdominal discomfort. Jaundice is present in 15% of patients admitted to the hospital for symptoms of fatty infiltration of the liver [71].
Alcoholic Fatty Liver-Pathology
The morphologic spectrum of ALD includes the following: simple steatosis, steatohepatitis (alcoholic hepatitis) and cirrhosis. Steatosis is the earliest histological manifestation of alcohol injury and develops in approximately 90% of individuals who drink more than 60 g/day of alcohol [30,72]. Steatosis is defined as the accumulation of lipid droplets in the hepatocyte cytoplasm and is usually macrovesicular or mixed micro vesicular and macro vesicular. It is postulated that patients with a mixed pattern have a higher risk of progressing to advanced liver disease in comparison with pure macrovesicular steatosis due to micro vesicular steatosis causing more severe oxidative stress, inducing mitochondrial injury [30,73]. Triglycerides accumulate in the cytoplasm of hepatocytes as a result of impaired hepatic fatty acid synthesis. In fact, steatosis occurs predominantly in perivenular hepatocytes, which have the highest concentration of enzymes involved with alcohol metabolism. In more severe cases, steatosis may involve all hepatic zones [74]. Steatohepatitis represents hepatic injury and is histologically characterized by steatosis, ballooning degeneration of hepatocytes and lobular infiltration by inflammatory cells. A liver biopsy is the gold standard for establishing a diagnosis of steatohepatitis. Ballooning degeneration is a result of damage to cytoskeleton, is the predominant mode of cellular injury in alcoholic hepatitis,

Central
Marroni et al. (2016)Email:
J Liver Clin Res 3(2): 1028 (2016) 6/24
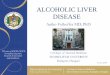
and represents a critical step in the pathogenesis of progressive liver injury [75]. Lobular inflammation typically involves a mixed population of cells, particularly polymorphonuclear cells (Figures 1A,1B]. In some cases, satellitosis can occur as a result of neutrophils surrounding ballooned hepatocytes [76].
The most important consequence of centrilobular injury (ballooning degeneration and inflammation] is the development of fibrosis. Fibrous tissue in alcoholic steatohepatitis is typically perisinusoidal/pericellular and localizes in the central zone (zone 3), frequently resulting in the typical “chicken-wire fibrosis” (Figure 1-C; 1-D) [76,77]. The fibrous tissue can also accumulate in the terminal hepatic vein; this pattern is called perivenular fibrosis and may result in varying degrees of narrowing of the hepatic vein lumen, which can contribute to the development of pre-cirrhotic portal hypertension [78] enules (central-central bridging) and portal tracts (central portal bridging), leading to the development of regenerative nodules and micronodular cirrhosis[79]. Additional findings found in alcoholic steatohepatitis include the presence of megamitochondria, lipogranulomas and Mallory bodies. Periportal ductular proliferation, ductular bilirubinostasis, and intraparenchymal cholestasis may also be observed [80]. In severe alcoholic hepatitis, the liver biopsy can be utilized to confirm the diagnosis and give information regarding the prognosis [81]. Sphar et al., assessed liver biopsies of 163 patients with severe alcoholic hepatitis and demonstrated that intraparenchymal cholestasis was more prevalent in non-survivors compared to survivors [70% vs 25%] using multivariate analysis. Moreover, serum bilirubin levels were higher in patients with severe intraparenchymal cholestasis [82]. Recently, Altamirano et al. [83], identified four histological findings (fibrosis, neutrophil infiltration, type of bilirubinostasis, and presence of megamitochondria) that were associated with mortality at day 90 in alcoholic hepatitis. These Histologic features were further graded and classified using the Alcoholic Hepatitis Histological Score (AHHS). The scores for
this classification were low (0-3 points), moderate (4-5 points), or high (6-9 points) according to the risk of mortality over 90 days (3%, 19% and 51%, respectively). In addition, in patients treated with corticosteroids, the three-month survival rate was 85% when the AHHS was less than 5 and only 51% when the score was equal or higher than 5. Interestingly, when analyzing patients with a Model for End-Stage Liver Disease (MELD) score less than 21, a score that is traditionally associated with a better outcome, the AHHS was also able to discriminate two different rates of survival. Specifically, 3-month survival rate in this group was 94% in patients with AHHS less than 5 vs 72% in those with scores equal to or higher than 5. Therefore, the application of the AHHS in patients with a MELD score less than 21 may further differentiate patients who might benefit from treatment. Moreover, in this previous study, bilirubinostasis predicted (in nearly half of the patients) the development of bacterial infections, a severe complication associated with alcoholic hepatitis.
Clinical Course
Progressive ALD can lead to alcoholic cirrhosis, which is defined by the occurrence of extensive fibrosis and regenerative nodules. In some patients, alcohol abuse coexists with other known causes of liver disease, such as hepatitis C and B virus infection, which are also etiological agents of liver cirrhosis [7]. As with other etiologies, patients with alcoholic cirrhosis are prone to develop clinical decompensations due to portal hypertension and liver failure and are at risk for developing hepatocellular carcinoma (HCC) [84]. The clinical course of alcoholic cirrhosis is influenced by the pattern of alcohol intake. Thus, periods of excessive alcohol intake can lead to superimposed alcoholic steatohepatitis and the subsequent clinical exacerbations, while prolonged abstinence can compensate previously complicated cirrhosis [7]. Alcoholic cirrhosis is associated with multiple complications. Laboratory findings often include hypoalbuminemia, hyperbilirubinemia, thrombocytopenia, prolonged prothrombin time [PT], and an increased international normalized ratio (INR) [7]. These abnormalities typically worsen with the progression of cirrhosis. Imaging studies often demonstrate findings that are consistent with cirrhosis, including a small, shrunken liver, hepatic nodularity, abnormal tortuous vessels from intra-abdominal varices, and other abnormalities, such as ascites or focal hepatic lesions [85,86]. These findings assist in diagnosing cirrhosis, but cannot establish alcohol as the etiology by themselves [7,31,87]. Ascites is typically the first complication, but other complications, such as jaundice, variceal bleeding, and hepatic encephalopathy are also prevalent [88-90]. Importantly, patients with alcoholic cirrhosis are particularly prone to bacterial infections [91]. The incidence of HCC among patients with alcoholic cirrhosis ranges range from 7% to 16% after 5 years to as much as 29% after 10 years [92]. Therefore, screening for HCC should be performed as recommended for any patient with liver cirrhosis. Importantly, patients with alcoholic cirrhosis should be screened for alcohol-induced damage in other organs, including the heart (alcoholic myocardiopathy), kidney (IgA-induced nephropathy), nervous system (central and peripheral involvement), and the pancreas (chronic pancreatitis) [7]. Importantly, in patients with impaired cognitive function, the existence of alcoholic dementia, withdrawal syndrome, and Wernicke’s encephalopathy should be ruled out. Patients with alcoholic cirrhosis are often
Figure 1 Histological changes alcoholic liver disease: In (A) Mallory-Denk bodies (HE-400 X); (B) Lobular inflammation (HE-200 x); (C) pericellular fibrosis (masson trichrome 200 x) and (D) pericellular fibrosis-detail (masson trichrome 400 x).

Central
Marroni et al. (2016)Email:
J Liver Clin Res 3(2): 1028 (2016) 7/24
malnourished. A careful clinical and analytical evaluation of the nutritional status is advised, and proper nutrition should be ensured [7].
Laboratory Tests
There are several characteristic laboratory abnormalities in patients with ALD, but none are diagnostic [56]. The classic finding is moderately elevated transaminases, with an aspartate amino transferase (AST) to alanine aminotransferase (ALT) ratio >1 (and often >2). Serum amino transferase levels may be normal or moderately elevated in the setting of alcoholic fatty liver disease and alcoholic cirrhosis [93,94]. The AST elevation is usually less than eight times the upper limit of normal, and the ALT elevation is typically less than five times the upper limit of normal. The degree of elevation does not correlate with the severity of the underlying liver disease [95]. Unlike other forms of liver disease in which the serum ALT level often is higher than the serum AST level, the most common pattern of liver biochemical test abnormalities in ALD is a disproportionate elevation of the AST compared with the ALT, resulting in a ratio greater than one [93,94,95-98]. An AST to ALT ratio >1 is occasionally seen in patients with NASH and is frequently seen in patients who have developed nonalcoholic cirrhosis [56]. However, if the ratio is greater than two, the transaminase elevations are likely due to ALD given that values greater than two are rarely seen in other forms of liver disease [96,97]. In a study of 271 patients with biopsy-confirmed liver disorders, more than 90 percent of patients with an AST to ALT ratio ≥2 had ALD. The percentage increased to greater than 96 percent when the ratio was ≥3 [99]. AST is typically elevated to 2-6 times the upper limits of normal in severe AH [31]. Levels of AST more than 500 IU/L or an ALT > 200 IU/L are uncommon with alcoholic hepatitis (AH) (other than with alcoholic foamy degeneration or concomitant acetaminophen overdose) and should suggest another etiology [31,100].
Gamma-glutamyl transpeptidase (GGT) levels are often elevated in patients with ALD and have been evaluated in a number of settings, including large population surveys [94, 101-103]. In a study of 123 patients who abused alcohol, all of the patients with liver disease had GGT elevations that were approximately 8 to 10 times the upper limit of normal [28]. Unfortunately, with respect to diagnosing alcohol abuse, a low sensitivity and specificity limit the usefulness of elevated GGT, the levels of which may fluctuate with extensive liver injury [104-107]. More recently, it has been shown that serum GGT activity is influenced not only by the amount of alcohol consumed but also by body mass index (BMI) and sex [108]. Macrocytosis suggests longstanding disease and may result from vitamin B12 or folate deficiency, alcohol toxicity, or increased lipid deposition in red cell membranes. Macrocytosis is seen in individuals abusing alcohol, but this condition lacks sensitivity. A combination of raised GGT levels and mean corpuscular volume or changes in these values over time in hospitalized patients may improve the sensitivity for diagnosing alcohol abuse [31]. Multiple other candidate biomarkers that may detect alcohol use or abuse objectively have been studied [109,110]. Carbohydrate-deficient transferrin (CDT) has been the best studied, but it has limited sensitivity and specificity [111]. The test results for CDT are also influenced by a
number of other factors, including age, sex, body mass index, and other chronic liver diseases [112-114]. Despite enthusiasm about a possible quantitative, reliable assay of alcohol consumption or abuse, the lack of sensitivity and specificity prevent reliance on any single biomarker [115]. Haller and colleagues [116] suggest that a hair toxicology analysis provides a longer window of ascertainment [90 days] and can identify alcohol and other drug use. Ethyl glucuronide in the hair is a novel reliable marker for the assessment of alcohol consumption [117] Elevated bilirubin levels are frequently seen in patients with decompensated cirrhosis from any cause, including ALD. The elevation of bilirubin levels in a patient who does not have cirrhosis should raise concern for AH. Hematologic findings in patients with ALD may include thrombocytopenia, anemia, an elevated mean corpuscular volume (MCV), a decreased lymphocyte count, an elevated erythrocyte sedimentation rate (ESR), and an elevated INR [56,93,118]. Patients who are malnourished or who have cirrhosis may also have low albumin levels [56].
Non-Invasive Tests to Estimate Liver Fibrosis
Serum markers: Several new blood tests that combine different biomarkers of fibrosis are now available. Although these tests were initially designed for patients with hepatitis C, some of these analyses seem to be effective in patients with ALD. However, different cut-offs may must be considered when using such biomarkers for ALD instead of hepatitis C [7].
FibroTest® is a serum biomarker of fibrosis combining data for alpha-2-macroglobulin, haptoglobin, GGT, ApoA1, and bilirubin, all corrected for age and sex. FibroTest® seems to have a high diagnostic potential for the detection of significant fibrosis in patients with ALD [7]. In a study of 221 consecutive patients with biopsy-proven ALD, the mean FibroTest® value ranged from 0.29 in those without fibrosis to 0.88 in those with cirrhosis, and its area under the receiver operating characteristic curve [AUROC] for the diagnosis of cirrhosis was at 0.95 [119]. FibrometerA® combines PT, alpha-2-macroglobulin, hyaluronic acid, and age and has a similar diagnostic accuracy in ALD as FibroTest [120]. With respect to validation, the AUROC curve for Fibrometer® was 0.892 in all patients and 0.962 in patients with ALD. Hepascore® combines bilirubin, GGT, hyaluronic acid, alpha-2-macroglobulin, age, and sex. The diagnostic accuracies of Fibrotest®, Fibrometer®, and Hepascore® were compared in patients with ALD [121]. The diagnostic values of Fibrometer A® and Hepascore® did not differ from that of FibroTest® for advanced fibrosis (AUROCs of approximately 0.80) and cirrhosis (AUROCs approximately 0.90). These scores were significantly greater than those for non-patented biomarkers (e.g., APRI, Forns, FIB4). The combination of any of these tests did not improve diagnostic performance [121].
Transient Elastography: The existence of inflammation, cholestasis or liver congestion may interfere with the liver stiffness measurement [LSM], independent of fibrosis [122]. As all of these conditions may occur during ALD, LSM should always be interpreted in the context of clinical, imaging and laboratory findings. A decision tree taking into account these additional parameters has been proposed for the use of transient elastography in heavy drinkers [7,123]. Importantly, elevated liver stiffness values in patients with ALD and AST serum levels

Central
Marroni et al. (2016)Email:
J Liver Clin Res 3(2): 1028 (2016) 8/24
>100 U/L should be interpreted with caution due to the possibility of falsely elevated liver stiffness as a result of superimposed alcoholic steatohepatitis [124]. In addition, alcohol consumption may also modify the LSM as shown by decreased liver stiffness among abstainers and the increase in relapsers [124, 125].
Hepatic Imaging: Imaging studies have been used to diagnose the presence of liver disease but do not have a role in establishing alcohol as the specific etiology of liver disease [31]. However, the diagnosis of fatty change, established cirrhosis and HCC may be suggested by ultrasound (US), computed tomography scan (CT), or magnetic resonance imaging (MRI) and confirmed by other laboratory investigations [126,127]. The major value of imaging studies is to exclude other causes of abnormal liver tests in a patient who abuses alcohol, such as obstructive biliary pathology or infiltrative and neoplastic diseases of the liver [7,128]. Specific features that may be suggestive of alcoholic cirrhosis include a higher volume index of the caudate lobe, more frequent visualization of the right posterior hepatic notch, and a smaller size of regenerative liver nodules in patients with cirrhosis due to ALD versus chronic viral hepatitis [7,86]. Abdominal US, abdominal CT, and abdominal RMI may show signs of hepatic steatosis or cirrhosis in patients with ALD. Liver imaging may provide evidence of hepatic steatosis or cirrhosis, but it is not able to differentiate ALD from other causes. US is always indicated to confirm that the liver is homogeneous and to exclude other causes of abnormal liver tests (e.g., biliary obstruction, hepatic masses) [56].
Ultrasound in patients with fatty liver disease may reveal a liver with a hyperechoic texture [129-131]. In patients with fibrosis, the US may reveal a coarse echo pattern. If cirrhosis has developed, nodules may be seen, causing an irregular outline of the liver surface [56]. In clinical practice, US may be proposed in heavy drinkers as a screening procedure for steatosis [132]. US can also be useful in detecting signs of advanced stages of ALD, such as liver dysmorphism, portal-systemic collaterals and splenomegaly [7].
More detailed liver imaging (e.g., CT scan or MRI) is obtained for patients with suspected cirrhosis or US evidence of biliary tract obstruction (e.g., jaundice, elevation of liver tests in a cholestatic pattern). Hepatic steatosis is readily detected by CT scan [133]. CT findings in patients with cirrhosis may include atrophy of the right lobe of the liver, hypertrophy of the caudate lobe, hypertrophy of the lateral segment of the left lobe, parenchymal nodularity, and attenuation of hepatic vasculature, splenomegaly, venous collaterals, and ascites. In some cases, the liver may be diffusely atrophic or hepatomegaly may be seen. On MRI, specific features that are suggestive of alcoholic cirrhosis versus cirrhosis due to viral hepatitis include a higher volume index of the caudate lobe, a smaller size of regenerative nodules of the liver, and more frequent visualization of the right posterior hepatic notch [86].
Treatment of Alcoholic Liver Disease
Abstinence is the cornerstone of ALD therapy and improves overall survival, primarily in those with advanced disease. Nutritional, psychological and pharmacologic therapies can support abstinence. Prophylaxis, surveillance, and aggressive
treatment prevent significant morbidity and mortality [5,6,87, 134]. To treat the clinical complications of ALD is the most important and urgent therapeutic action required, but in cannot be forgotten to treat the underlying alcoholism. Moreover, alcohol dependence remains a life-long disease, carrying the potential for relapse and subsequent consequences. The probability of long-term sobriety becomes robust after only 5 years of sustained abstinence [134-138]. Relapse rates as high as 80% - 95% are found in the treatment of alcoholics without ALD [139]. ALD patients are at a higher risk of psychological and psychosocial dysfunction when compared with non-ALD patients [140].
Nutritional Treatment of Alcoholic Liver Disease
Alcoholic patients often experience protein-calorie malnutrition. Undernourished alcoholic patients with cirrhosis exhibit muscle wasting, weight loss, and nutritional deficiencies, which can promote bacterial infections; these patients also exhibit increased morbidity and mortality [5,141,142].
These complications are multifactorial, including poor dietary intake due to anorexia, dysgeusia, an altered sense of smell, nausea, and vomiting; malabsorption; a hyper metabolic state; and impaired protein synthesis from cytokine-induced inflammatory responses [141-144]. Nutritional deficiencies can include those for fat-soluble vitamins (A, D, E and K), folate, thiamine, niacin, and pyridoxine; and for the trace elements zinc, magnesium, and selenium. Each deficiency produces specific symptoms, signs, and complications. For example, thiamine deficiency causes Wernicke’s encephalopathy [141]. Nutritional support in patients with ALD improves liver function and histological liver findings; significantly increase survival times; reverses muscle wasting, weight loss, and vitamin and trace element deficiencies; and reduces infections associated with ALD [139,143-145]. A recent Cochrane review of 37 randomized controlled trial (RCTs) found no significant difference in mortality in patients with advanced liver disease receiving either enteral or parenteral nutritional support vs those receiving neither. However, improvement was observed in serum bilirubin levels, nitrogen balance, hepatic encephalopathy, and a reduced incidence of post-operative complications, particularly infections [144].
The European Society for Clinical Nutrition and Metabolism (ESPEN) recommends enteral or parenteral nutritional support for patients with liver disease to improve nutritional status, liver function, mental status and overall survival [141,142]. The American Association for the Study of Liver Diseases (AASLD) and American College of Gastroenterology (ACG) recommend regular assessment of patients for nutritional, vitamin, and mineral deficiencies; appropriate supplementation for identified deficiencies; enteral nutritional therapy for severe ALD; and frequent interval feedings, emphasizing breakfast and a nighttime snack [31,87]. These recommendations revise prior recommendations to reduce protein intake to prevent hepatic encephalopathy. A diet containing 1.2-1.5 g of protein/kg per day is currently recommended to maintain positive protein balance and to prevent muscle wasting in cirrhotic [87,139,143-146].
Pharmacotherapy for Alcoholic Liver Disease
Treatment with drugs to achieve and maintain abstinence and to mitigate hepatic damage in patients with ALD is one of

Central
Marroni et al. (2016)Email:
J Liver Clin Res 3(2): 1028 (2016) 9/24
the main aspects of the multidisciplinary management of these patients [5,6,87,134,147-150]. Most reviews of ALD concentrate on treatment of the liver disease and do not address the underlying addiction. In practice, understanding the addiction is the key to understanding the continuum from alcoholic fatty liver to alcoholic cirrhosis [134].
ALD is a prominent and preventable cause of morbidity and mortality [87].
There are currently limited pharmaco therapeutic options for managing ALD, and individual variation in the severity, presentation, and complex pathogenesis of ALD are barriers to effective treatment [6].
There are no reports of randomized controlled trials using approved medications for the treatment of alcohol dependence in ALD-spectrum disorders [5,6,87]. Some ALD patients require specific pharmacologic treatment with special drugs with anticraving actions that can effectively treat alcohol dependence and prevent relapse but which have potentially severe hepatotoxicity [5,6]. Scoring of disease severity using validated assessment instruments should guide treatment approaches [6].
The most commonly used drugs are as follows:
Disulfiram: An irreversible inhibitor of alcohol dehydrogenase prescribed to treat alcoholism. This drug is not recommended for patients with advanced ALD because of potential severe hepatotoxicity [5,6 Acamprosate
An anticraving drug that is effective at preventing relapses; however, special care must be taken due to potential hepatotoxicity [5,6].
Baclofen: An agonist of the gamma-aminobutyric acid B receptor, has been found to be effective in maintaining abstinence and is safe even for cirrhotic patients [5,6, 147-149,151]. Baclofen is the only medication available in the United States with demonstrated safety and efficacy in reducing alcoholic behavior that has been formally tested in clinical trials in patients with ALD [6,152].
Naltrexone: An opioid antagonist reduces relapse, although its efficacy is modest [5,6].
Addiction to Alcohol: Addictions usually arise from pleasurable actions, and immediate gratification is the most common foundation for addiction. Ask an alcoholic person why they continue to drink and they will often say, ‘‘I drink because I like it’’ [134]. The combination of gratification from the substance with the unwanted effects of the treatment, such as the inconvenience of attending psychological therapy, embarrassment, financial disincentives, and ambivalence about the addictive behavior, can all contribute to the persistence of addiction. Substance abuse and addiction are disorders of remission and relapse [134]. Addiction specialists define relapse as a daily alcoholic intake of more than 4 drinks or an overall consumption of 14 drinks or more per week during at least 4 weeks; a lapse (slip) is defined as any episode of alcohol consumption not classified as a relapse [1,152]. When counseling an alcoholic patient, addiction specialists distinguish between a slip and a relapse [153]. A slip is a temporary return to drinking
that is recognized by the patient as potentially harmful and which leads to renewed efforts toward abstinence. A relapse suggests a more sustained resumption of drinking. These events are occasionally characterized as ‘‘harmful,’’ ‘‘abusive,’’ or ‘‘addictive drinking,’’ whereas the term ‘‘recidivism’’ is abjured on account of its pejorative connotations [134].
The evaluation of patients with ALD should be conducted in a multi-disciplinary manner and include a thorough medical evaluation, as well as the evaluation of a psychiatrist or addiction specialist to identify those at high risk of relapse [154]. Addolorato et al. [148], emphasizes the presence of an Alcohol Addiction Unit [AAU], in which patients received a multimodal treatment. In particular, clinical and medical management, including counseling and attending support groups, was strongly recommended but not mandatory. Patients in such units would able to participate in a rehabilitation program or individual counseling, with regular updates from the addiction program and provider teams of the patient’s treatment progress [155]. The psychiatric and psychosocial evaluation as well as the follow-ups with physicians, psychiatrists and addiction specialists is important for reversing these problems. Specifically, these professionals help identify patients at risk for relapse and those who have relapsed, enabling responsive actions [1]. Factors that predict freedom from alcohol recidivism include acknowledgment by patient of his or her addiction; strong social support; integration; medical compliance; the ability to substitute alternative activities that diminish temptation to return to alcohol use, including pursuits that improve self-esteem or hope; a rehabilitative relationship with a healthcare professional, friend, or family member; and a perception by the drinker of the negative consequences of alcoholic relapse [1,87,135,156].
Factors that predict alcohol relapse include psychiatric co-morbidity, a high score on standardized high-risk alcohol relapse scale, a diagnosis of DSM-IV alcohol dependence, multiple treatment failures, illicit drug use, continued use despite consequences, and a family history of alcoholism [31,87,135,157-161]. The targeted detection of factors that are predictive of relapse could support sobriety and adherence with medications and appointments [150,157]. The patient should be monitored continuously for relapse during treatment for alcoholism [31,162].
Monitoring for relapse relies heavily on the candidate’s candor in answering routine questioning regarding alcohol use. It is important to try to establish a balance between supporting patients in their efforts to maintain abstinence and honesty and identifying those who may need more aggressive treatment and management while adhering to the abstinence policy [6]. Screening, when combined with a structured management program, can discriminate between complete abstainers and those who drink. Specifically, research suggests that screening can reveal individuals who are vulnerable to alcohol relapse and who should receive targeted intervention [135]. Random toxicology screens using blood or urine samples should also be used for monitoring, and patients should be given a limited time in which they may participate in these screens [162]. Random blood or urine alcohol testing frequently is inadequate to detect drinking. More robust abstinence support and better assessment measures might improve outcomes [163].

Central
Marroni et al. (2016)Email:
J Liver Clin Res 3(2): 1028 (2016) 10/24
Ethyl glucuronide in the hair is a new reliable marker for the assessment of alcohol consumption, with a specificity of 98% and a positive predictive value of 92%. In 52% of patients denying alcohol consumption within the last 6 months, alcohol abstention was disproved in 83% of cases by hEtG testing [116,117].
Treatment of Acute Alcoholic Hepatitis
Severe cases of Acute Alcoholic Hepatitis require admission to an intensive care unit. Protect the airway, and do not use benzodiazepines due to the pre-existing central nervous system (CNS) depression and hepatic encephalopathy. Use B-complex vitamins to prevent Wernicke encephalopathy. Nutritional support should consist of a daily protein intake of 1.5 g\kg body wt. Detect infections early so it will be possible to begin empiric antibiotics [5,164]. The efficacy of corticosteroids [CS] in treating severe acute alcoholic hepatitis is controversial, and different results have been reported. Certain studies reported increased patient survival times [165], whereas other studies did not support CS use due to heterogeneity and increased infections, with a poor prognosis [166,167]. The AASLD practice guidelines recommend the use of CS in severe alcoholic hepatitis, i.e., with a Maddrey discriminant function > 32 or hepatic encephalopathy [31]. A Lille Model score greater than 0.45 after 7 days of treatment with CS indicates failure of treatment and predicts a 6-month survival of less than 25% [168,169]. The addition of the Lille score helps to better identify the nearly 40% of patients who do not respond to CS therapy; in these cases, CS should be discontinued, and alternative therapies can be considered. Non-responders have a very poor prognosis, an increased risk of infections and a negligible response to subsequent treatment with pentoxifylline (PTX) [164,169,170].
Pentoxifylline, a nonspecific phosphodiesterase inhibitor, decreases tumor necrosis factor alpha (TNF-α) gene expression. In ALD, a cytokine- induced acute inflammatory response was shown to increase circulating TNF-α, indicating that TNF-α is a possible target for therapy [164]. A double blind placebo-controlled RCT showed a survival benefit of treatment with PTX (400 mg tablets, three times daily for 28 days). This decreased mortality arises primarily from the prevention of hepatorenal syndrome (HRS) [171]. Another RCT comparing PTX and CS showed improved survival with PTX at 3 and 12 months, an effect that was attributed to a decreased incidence of HRS and gastrointestinal bleeding [172]. Studies comparing treatment with a combination therapy of PTX and CS to standard CS treatment did not show a survival benefit in combination therapy [169,173]. N-acetylcysteine (NAC) is a potent antioxidant. One of the mechanisms of hepatocellular death in acute ALD is the increased production of reactive oxygen species by damaged hepatocytes, an effect that is exacerbated by the depletion of glutathione, the primary mitochondrial antioxidant [164]. A large RCT compared IV NAC plus CS to CS alone, showing improved survival and decreased HRS and infections in the NAC plus CS group [174]. TNF-α is an important mediator of immune function and is involved in hepatocyte regeneration [175]. Moreover, this protein plays a role in the pathogenesis of alcoholic hepatitis, and anti-TNF-α treatment decreases mortality in experimental animals [176]. An RCT comparing infliximab or etanercept in combination with CS compared to CS was discontinued
prematurely due to an increased rate of infections and death in the groups using inhibitors of TNF-α [177-181].
Liver Transplantation in Alcoholic Liver Disease
The primary effective strategy for patients with ALD is total alcohol abstinence [182], and when impossible, liver transplant (LT) represents the gold standard treatment for end-stage ALD [148, 183].
ALD is the second most common diagnosis among patients undergoing LT [184] and has better survival times than for other etiologies. Even when recidivism occurs, the risk of developing ALD and graft loss is unpredictable [148,154-156,184-188]. These excellent results for LT are in contrast to the dismal survival outcomes in patients with decompensated ALD who do not undergo LT [185]. LT for ALD still generate controversy because of the perception that the patient’s liver disease was self-inflicted and due to concerns related to alcohol recidivism after transplantation [148,154,185,187,188]. The general public, and even some physicians, would give alcoholics lower priority in regard to allocating scarce resources, such as a LT [184, 188]. Moreover, alcoholism is still considered a bad habit, and there is a general reluctance to perform transplants in these patients. In the field of neuroscience, it is now known that alcoholism is a chronic relapsing medical disease of the brain, not a bad behavior [2]. Ethical principles recommend active treatment of these patients, without discrimination [189].
ALD was the second most common indication for LT, accounting for greater than 17.1% of all cases [116, 154,156,190]. Liver transplantation restores the physiological function of the liver and reverses the complications of ESLD. LT also improves the duration and quality of life but does not treat the underlying alcoholism and alcohol dependence, which carries the potential for relapse. The probability of long-term sobriety becomes robust only after 5 years of sustained abstinence [1,159,191].
The recidivism prevalence ranges from 10% to 90% [156,159,185,192]. Patients will admit to some alcohol use within 5 years [20% to 50%] of LT, and approximately 10% to 15% resume heavy drinking [7,116,154,159]. Many transplant centers use the six-month rule of abstinence to determine whether ALD patients should receive livers. The “6-mo rule” [135,155,184] has two purposes: allowing the liver a chance to recover, and reducing the risk of alcohol relapse [150]. Six months is an arbitrary threshold and has never been shown to affect survival after LT [135,155,184], and there is only a weak association between sobriety and outcome [152]. The European Association for the Study of the Liver (EASL), AASLD, and UK guidelines no longer adhere to this policy, instead recommending a balanced analysis of each patient [7,187]. The optimal period of pre-transplant abstinence remains unclear [188].
Addolorato et al. [148], and the Group of Italian Regions [184] suggests that the pre-LT abstinence time could be shortened, at least for selected patients who participate in self-help groups and who are evaluated in a multidisciplinary transplant team, including an addiction specialist/hepato-alcohologist. Addolorato et al. [148], recommends a specialized AAU. The patient evaluation could be individualized and not subject to

Central
Marroni et al. (2016)Email:
J Liver Clin Res 3(2): 1028 (2016) 11/24
arbitrary rules that cannot be scientifically supported. It is time to rethink the 6-month rule.
In a post-LT population, 80% of patients were abstinent or consumed only small amounts of alcohol occasionally, whereas the remaining 20% exhibited two patterns of alcohol recidivism: early-onset moderate-to-heavy consumption or late-onset moderate use. The outcomes are generally excellent for individuals who consume small amounts of alcohol [193]. Most of these relapsed patients remain compliant with their immunosuppressive regimens, with only a small number developing significant histologic injury on liver biopsy [193,194]. In contradistinction, significant and excessive alcohol consumption after LT may be associated with rapidly progressive liver injury, alcoholic hepatitis and reduced survival [157,160]. In relapsing patients [23%], more than 50% were found to have an alcohol-related graft injury [195]. The survival of patients with ALD (77.0%) was similar to those without (79.0%) up to the fifth post-LT year. However, survival was worse during the five subsequent years among the five-year survivors (70.6% vs 92.9%). ALD was an independent risk factor for poorer survival beyond the fifth post-LT year but not earlier, and this effect was not attributable to relapse. Conversely, alcohol relapse increased the risk of death only during the first five post-LT years [116]. Excessive alcohol use was associated with decreased survival for all primary causes of LT and not just for ALD [163]. A dramatically lower 10-year survival rate for those who relapsed is due to malignancy and cardiovascular death and not recurrent liver failure [196]. Those with acute alcoholic hepatitis were declined LT because it was seen as a contraindication, largely because these patients were generally imbibing alcohol up until the point of decompensation [195]. Mathurin and colleagues [165,169] demonstrated that with careful selection, these patients can be transplanted and have comparable survival outcomes, leading to a renewed debate with respect to the selection and evaluation of those with liver disease attributable to alcohol.
Experimental Models for the Study of Alcoholic Liver Disease
Over the years, a number of animal models have been described to aid in the study of ALD. The purpose of establishing animal models is to be able to investigate the development of ALD; elucidate its onset and progression; and to understand the relationships between this disorder and the associated oxidative stress, bacterial translocation and metabolic responses (Quadro 1).
An experimental animal model should replicate the clinical conditions of ALD, mimicking its biochemical and morphological manifestations. According to Terblanche and Hickman [197], the ideal model should meet a number of requirements, including (Table 4) Reversibility: the model should produce ALD and allow the animals to survive to the end of the process; 2) Reproducibility: the clinical aspects and the extent of liver injury should be reproduced and assessable; 3) Replicability: other researchers should be able to follow the steps of the model and observe results consistent with ALD; 4) Death: the animal’s death should be consistent with ALD and should be a direct result of the damage caused by the disease; 50 Provides a therapeutic window:
the window should be long enough to allow investigation and treatment between the time the injury develops and the death of the animals; 6) Adequate choice of animal: the choice of animal should permit handling and development of the disease; 7) Low risk for the researcher.
Due to the complexity of the pathophysiological mechanism of ALD, establishing an animal model that addresses all of these phases and changes becomes a very challenging task. Numerous factors can interfere with the establishment of an animal model of ALD (Table 5). First, the species must be easily handled (the most common animals are rodents and zebrafish). In addition, the mechanism of alcohol metabolism in the animal should be known given that alcohol will be the toxic agent that is used. In humans, an exaggerated consumption of alcohol leads to fibrosis, but this is not clearly evidenced in rats. Genetic differences in enzyme activity are believed to exist between humans and animals. In humans, the protein ubiquitin is essential for the formation of abnormal structures, called Mallory bodies, in the liver cells of patients with ALD. However, the DNA sequence of ubiquitin is different in rats, preventing rat liver cells from forming Mallory bodies in response to excessive alcohol intake. This difference is why mice and rats seldom develop fibrosis or cirrhosis due to short- and long-term alcohol use alone [198-202]. Therefore, animal models for ALD using rodents must use alcohol in combination with another fibrinogenic agent, such as iron (i.e., the Fenton reaction), a fat-rich diet (steatosis), vitamin supplementation, and LPS injection (endotoxin) [199,203,204]. Other aspects that may influence the development of ALD in animal models are the amount and type of alcohol administration, its metabolism, the type and quality of animal nutrition, and oxygen deprivation. Based on these potential confounds, the model can make use of a systematic administration of alcohol at a known dose by gavage. This method ensures the same concentration of ethanol is administered for all animals. Alcohol diluted in drinking water mimics continuous intake at lower doses; however, differences between animals may exist, with some drinking more and some drinking less. The induction of liver injury by alcohol is associated with the ability to metabolize ethanol. This ability is intrinsic to a given strain of animal. Indeed, a study with controlled isocaloric feeding and a liquid diet of
Table 4: Experimental animal models: Characteristics of an ideal model (197).1. Reversibility
2. Reproducibility
3. Replicability4. Death5. Therapeutic window6. Adequate choice of animal7. Low risc for the researcher
Table 5: The pathophysiology of alcoholic liver disease depends.
1. Animal model
2. Mechanism of alcohol metabolism in the animal model3. Genetic and metabolic similarity and difference between animal model and human4. Amount and type of alcohol administration

Central
Marroni et al. (2016)Email:
J Liver Clin Res 3(2): 1028 (2016) 12/24
alcohol for 8 weeks compared induction, onset and progression of ALD in three different rat strains (Long Evans, Sprague Dawley and Fischer 344). This study found that, although the serum levels of alcohol were similar, weight gain was different across the rat strains (Long>Sprague Dawley>Fischer), and there was difference in the expressions of enzymes that metabolize ethanol (CYP2E1, ALDH1 and ADH1, 3 and 7) 7 ) [205,206]. In the literature, there are animal models in which ALD develops acutely or chronically, with controlled or ad libitum dosages, and with or without the addition of a secondary insult. Among the published animal models, we highlight the following: chronic binge feeding (Gao-binge model); chronic ethanol feeding (10 days or longer) plus a single binge (the NIAAA model); chronic ethanol feeding (4–6 weeks or longer) plus multiple binges (twice per week during the chronic feeding) (the NIAAA model); chronic ethanol feeding (4 weeks) plus three binges during the last 3 days of feeding; chronic feeding (a 4- to 6-week feeding model is widely used; some studies used a 12-week feeding); intragastric chronic ethanol feeding infusion (Tsukamoto-French model); acute gavage; ad libitum oral alcohol in drinking water; oral liquid diet or chronic ethanol feeding (Lieber-DeCarli model); acute binge feeding; and alcohol-preferring rodents.
Chronic binge feeding model (Gao-binge model): This model is easy to perform and induces a moderate inflammatory process, with an increased number of neutrophils and moderate levels of AST and ALT (Table 6). The etiological mechanism is
an increase in the inflammatory infiltrate. This effect leads to liver injury, promotes hepatocyte damage and mitochondrial dysfunction, and aggravates oxidative stress [207].
Chronic ethanol feeding (10 days or longer) plus a single binge (the NIAAA model)
This model is easily implemented and fairly simple. The main manifestation is steatosis, which occurs within 10 days, and an elevation in ALT levels. The disadvantage is that liver fibrosis does not develop (Table 6). In this model, the mortality rate is virtually null [207,208].
Chronic ethanol feeding (4–6 weeks or longer) plus multiple binges (twice per week during the chronic feeding) (NIAAA model): This model is easily performed and permits the study of ALD onset. The model induces a mild elevation of ALT levels and intense steatosis in the long term (Table 6). Because of the multiple binges, the mortality rate is high. This model is not indicated to study the progression stage as it does not induce fibrosis [207].
Chronic ethanol feeding (4 weeks) plus three binges during the last 3 days of feeding: This model is easily performed. Although fibrosis is not reported, there is a marked increase in ALT levels and intense steatosis (Table 6) [207,209].
Chronic feeding (4- to 6-week feeding model is widely used; some studies used 12-week feeding)?
Table 6: Main experimental models used for the study of alcoholic liver disease.
Models Characteristics
Chronic binge feeding model (Gao-binge model)Moderate elevation of serum ALT, AST;Moderate liver inflammation with an increase in neutrophils;Easy to perform.
Chronic ethanol feeding (10 days or longer) plus a single binge (the NIAAA model)
Animals developed steatosis;Animals do not develop liver fibrosis;Easy to perform.
Chronic ethanol feeding (4–6 weeks or longer) plus multiple binges (twice a week during the chronic feeding) (the NIAAA model)
Animals develop steatosis; Mild elevation of serum ALT; Animals do not develop liver fibrosis; High mortality; Easy to perform.
Chronic ethanol feeding (4 weeks) plus three binges during the last 3 days of feeding
High elevation of serum ALT; Animals developed steatosis; Easy to perform.
Chronic feeding (4- to 6-week feeding model is widely used; some studies used 12-week feeding)
Mild elevation of serum ALT; Animals developed steatosis; Animals do not develop liver fibrosis; Easy to perform.
Intragastric chronic ethanol feeding (Tsukamoto-French model)Moderate elevation of serum ALT, AST; Moderate liver inflammation with an increase in macrophages but low levels of neutrophils; Animals developed steatosis, necrosis and fibrosis; Difficult to perform.
Tsukamoto-hybrid model with high-cholesterol and high-fat diet plus chronic ethanol and binge ethanol feeding
Significant elevation of serum ALT, AST; Significant liver inflammation with an increase in neutrophils; Mild liver fibrosis; Difficult to perform.
Acute gavage Mild elevation of serum ALT; Animals developed mild steatosis; Animals do not develop liver fibrosis; Easy to perform.
Ad libitum oral alcohol in drinking water
Animals develop steatosis, minor inflammatory infiltrates; Activation of Kupffer cells by increased LPS; Pathological changes do not progress beyond steatosis, metabolic and oxidative stress in the absence of a secondary stress.
Oral liquid diet or Chronic ethanol feeding (Lieber-DeCarli model)
Mild elevation of serum AST, ALT; Animals developed steatosis; Low levels of liver inflammation with increase in macrophages; Damages hepatocyte mitochondrial functions and produces oxidative stress; Easy to perform.
Alcohol preferring rodents Animals do not develop cirrhosis; Animals progressively develop HCC in the absence of cirrhosis (rats).
Fonte: Adapted (207).

Central
Marroni et al. (2016)Email:
J Liver Clin Res 3(2): 1028 (2016) 13/24
This model is very similar to the Chronic ethanol feeding (4–6 weeks or longer) plus multiple binges model, differing in its mild elevation of ALT levels and steatosis and low mortality in the long term (Table 6) . Hepatic fibrosis is not seen [207,210-212].
Infusion (Tsukamoto- French Intragastric Chronic Ethanol Feeding Model): This model is difficult to perform as is requires trained personnel and intensive care. Because of the enteral administration, an experienced surgeon is required for cannula placement. Its caloric content is equivalent to 500 mg/dl. The main characteristics of the model are elevated ALT levels and steatosis and mild fibrosis; it is indicated for studying the transition stage between onset and progression. This model has a high mortality rate in the long term and can be combined with a fat or cholesterol-rich diet. The hybrid model allows enhanced AST and ALT level elevation and a stronger inflammatory process, with intense inflammatory infiltrate and mild fibrosis (Table 6). If a fat-rich diet is added to the Tsukamoto-French model, oxidative stress is enhanced due to the oxidation of hepatic lipids [201].
Acute gavage: The administration of ethanol by gavage is considered an acute form of ALD induction. The calorie content is equivalent to 500 mg/dl. The methodology is simple and easy (Table 6), only requiring training for gavage administration. The administration induces mild steatosis, a mild ALT elevation, low mortality in the short term, and no fibrosis [213, 214].
Ad libitum oral alcohol in drink water” This animal model is very simple, requiring only that the water consumed each day be measured (for determination of the amount of alcohol consumed). There may be differences across animals due to different consumptions. On average, the calorie content is 50-100 mg/dl. The observed manifestations include a mild increase in ALT levels and minimum steatosis. There is no fibrosis, and the mortality rate is practically null. The ad libitum oral alcohol in drink water model mimics the consumption of alcohol through the gastrointestinal tract. Clinically, this model simulates ALD in its mildest form [215].
Oral liquid diet or chronic ethanol feeding (Lieber-DeCarli model): This model corresponds to a calorie content of approximately 100-160 mg/dl. Because the calorie content for the experimental animals is known, it is possible to provide control animals with an isocaloric diet. AST and ALT serum levels are elevated, there are histological signs of steatosis, and mild hepatic inflammation with the presence of macrophages (Table 6). The inflammation is mediated through increased gut permeability, the effects of lipopolysaccharide [LPS] and the activation of Kupffer cells (KCs). These changes cause damage to the mitochondrial function of hepatocytes, resulting in an imbalance of the redox status.
Alcohol preferring rodents: The main characteristic of this model is it that mimics the human behavior of alcohol consumption, i.e., oral alcohol intake (Table 6). The intake usually corresponds to a calorie content of 40-130 mg/dl, depending on the quantity of ethanol, and may reach as high as 200 mg/dl. In the long term, continuous, chronic intake can lead to hepatocellular carcinoma without cirrhosis [216].
Many of the above-mentioned models add fat-rich diets because there is a deficiency of methyl donors in the presence
of alcohol; thus, fat accumulates in the liver, leading to organ dysfunction [217]. Another compound that may be added is a transition metal. Rats that are fed with alcohol and supplemented with dietary iron for 16 weeks develop severe damage to the liver [218]. It is believed that alcohol in the presence of iron generates reactive oxygen species (ROS) through the Fenton reaction, enhancing oxidative stress. Diets with carbohydrate complementation help to avoid alcohol-related liver damage. Therefore, it is occasionally necessary to associate food restriction (approximately 16 g/day/rat) to avoid the possibility that macronutrients delay the development of liver disease.
Possible theories regarding the physiopathology of ALD include increased oxidative stress, hepatic chronic inflammatory processes, and intestinal bacterial translocation. The continuous and sustained presence of ethanol increases cytochrome P4502E1 (CYP2E1) activity. This enzyme acts in the liver to metabolize drugs. As enzymatic liver reactions are increased, ROS are generated and antioxidant resources are depleted. As ROS formation increases, there is an increased risk of lipid, protein and DNA oxidation. These constant oxidation events change membrane permeability, modify membrane fluidity, inactivate protein-based enzymes, and damage DNA bases, resulting in genome instability. All of these insults that result from increased oxidative stress aggravate hepatic dysfunction. Added to this redox imbalance, the liver tissue undergoes its own inflammatory process or exhibits inflammation as a result of alcohol-induced alterations in gut permeability. These changes in permeability favor bacterial translocation and endotoxin release.
Model Alcoholic Liver Disease in Zebrafish: Danio rerio, a small freshwater teleost fish (3-4 cm), is popularly known as the zebrafish and belongs to the Cyprinidae family. In the last 30 years, the zebrafish has been established as translational tool for the study of human diseases [219]. Zebrafish are transparent for the first days of life, allowing visualization of digestive and hepatobiliary systems development [220]. The liver is fully formed and functioning 72 hours after fertilization [221]. The genome of this species has been fully mapped [http://www.sanger.ac.uk/Projects/D rerio /] and exhibits high homology with the human genome [222, 223]. Moreover, there is ample opportunity for tracing genetic traits [224]. Furthermore, zebrafish have characteristics that are commonly found in mammals, including innate and adaptive immune systems [225-228].
The gastrointestinal system of the zebrafish contains a liver, pancreas, gall bladder and intestines, but not a stomach [229, 230]. The zebrafish liver has similar functionality to mammals [231], and several human liver intoxicants, such paracetamol [232], fructose [233] and ethanol [234], have been studied in zebrafish. The zebrafish has been established as an excellent animal model for studying alcoholic hepatic steatosis.
The earliest stage of ALD is the accumulation of lipid droplets in hepatocytes (steatosis). Lipid-laden hepatocytes are prone to further injury, but it is unclear whether this is a primary result of lipotoxicity or secondary to underlying hepatocellular deficiency or stress [235]. Multiple factors can cause steatosis, including ethanol metabolism in the liver, a decreased ratio of nicotinamide adenine dinucleotide to nicotinamide adenine

Central
Marroni et al. (2016)Email:
J Liver Clin Res 3(2): 1028 (2016) 14/24
dinucleotide hydrogen (NAD/NADH), decreased triglyceride metabolism, increased lipid import or synthesis, reduced secretion of lipoprotein triglyceride particles, oxidative stress, and disturbances of molecular pathways [81,236,237]. Schneider and colleagues used adult animals, which were subjected to chronic exposure to ethanol (0.5% v / v). This ethanol concentration was chosen after a study by Gerlai et al. [238], which demonstrated an “alcoholic state” in zebrafish exposed to 0.05% ethanol. Our results showed that at the 14th day, animals exposed to ethanol showed a light steatosis, which worsened by the 28th day. The practicality of this model lies on that ethanol can be directly added into the tank water. Care must be taken to exchange the tank water every two days to avoid decreased in ethanol concentrations [234]. The effects of the gut-liver axis were also demonstrated in that treatment with Lactobacillus rhamnosus GG reduced the alcoholic hepatic steatosis [234].
Zebrafish that are exposed acutely or chronically to ethanol develop hepatic steatosis and have become an excellent platform for the study of ethanol damages in the liver, facilitating the understanding of the important onset mechanisms of steatosis and the development of novel therapies to treat ALD.
Biomarkers Involved in Alcoholic Liver Disease
Most of the animal models available today for studying the pathogenesis of ALD culminate with damage to hepatocytes, changes in mitochondrial function, an inflammatory process, oxidative stress, endoplasmic reticulum [ER] stress, an increase in gut permeability, and the release of various cytokines, aggravating liver injury [207, 239].
Physiopathology of Alcoholic Liver Disease and the Involvement of Oxidative Stress: The physiopathology of ALD is characterized by the presence of steatosis, which is attributed to the increased absorption and accumulation of hepatic fat and triglycerides and the decreased oxidation of fatty acids [240]. There is also increased hepatic uptake of intestinal endotoxins, resulting in the activation of Kupffer cells and the release of pro-inflammatory and fibrogenic cytokines; the induction of cytochrome P4502E1, a source of acetaldehyde and ROS; and hyperhomocysteinemia, in which elevated hepatic homocysteine results in ER stress promoting necro-inflammation [6,239]. Interleukin-8 and monocyte chemotactic protein attract neutrophils, and transforming growth factor b1 (TGFß1) and platelet-derived growth factor (PDGF) activate hepatic stellate cells, which are major sources of fibrous matrix [239].
The increase in triglyceride levels in hepatocytes and the release of pro-inflammatory cytokines constitute a “two-hit” process that is responsible for the development of steatosis. The first hit consists of the release of free fatty acids from adipose tissue. Together with adipocytokines, these free fatty acids flow through the portal vein and cause insulin resistance in the liver. The second hit can be any additional stressor, such as increased oxidative stress; lipid peroxidation; or decreased levels of antioxidants, adipocytokines, and peroxisomes [6]. Oxidative stress and redox imbalance play important roles in the genesis of alcohol-induced liver damage [241, 242]. Oxidative stress decreases proteasome activity, contributing to the formation of Mallory bodies and strongly eosinophilic hyaline bodies, leading
to cytokeratin filament aggregation in the cytoplasm of clear hepatocytes and the aggravation of liver damage [242].
ROS and nitrogen reactive substances (RNS) that form during CYP2E1-mediated alcohol metabolism are associated with fat accumulation, inflammation, and fibrosis and DNA damage. In addition to perpetuating hepatocyte damage, ROS also lead to the depletion of glutathione (GSH), thereby promoting progression to ALD [6,243]. Due to these effects, biological processes are altered, and hepatocytes are sensitized to the action of cytokines, such as TNF-α. Liver cells are also sensitized to the action of endotoxins, leading to the activation of signaling pathways, such as those controlled by nuclear factor kappa B (NF-κB), extracellular signal regulated kinases, and mitogen-activated protein kinase (MAPK). The activation of these pathways in turn accelerates the production of oxidants and inflammatory factors [244]. Oxidation and inflammation are closely related in alcohol-induced liver injury because inflammatory cytokines favor ROS production. Moreover, the depletion of mitochondrial GSH increases liver sensitivity to alcohol through TNF-α-mediated hepatocellular death [245]. Alcohol increases the hepatic activities of nitric oxide synthase (NOS ) and cyclooxygenase-2 (COX-2) as well as the formation of nitric oxide (NO) and prostaglandin E2 (PGE2), which is closely related to necro inflammatory injury [245]. Oxidative stress was observed to aggravate ALD in a study using Lieber-DeCaril’s model (ethanol liquid diet). In this study, alcohol increased CYP2E1 expression, ROS production, and malondialdehyde (MDA), TNF-α and IL-6 levels. In contrast, activities of the antioxidant enzymes superoxide dismutase (SOD), GSH and glutathione peroxidase (GPx) were reduced. In this model, the expression of nuclear factor (erythroid-derived 2)-like 2 (Nrf2) and heme oxygenase (HO-1) genes, which are involved in the antioxidant defense system, were also down-regulated [246].
Physiopathology of Alcoholic Liver Disease and the Involvement of Endoplasmic Reticulum Stress: The ER plays a key role in Ca2+ homeostasis and is the primary site where proteins and lipids are synthesized in the cell. Sustained dysregulation in protein folding or altered lipid homeostasis in the ER results in ER stress, which may ultimately lead to cell death if the stress is not resolved. To restore homeostasis, the ER activates the unfolded protein response (UPR). The UPR is chiefly controlled by the binding immunoglobulin protein (BiP)/glucose-regulated protein 78 (GRP78) protein, which regulates three specific transducers: inositol requiring (IRE) 1α, PKR-like ER kinase (PERK), and activating transcription factor (ATF) 6α. These factors act in concert to increase ER content, expand the ER protein folding capacity, degrade mis folded proteins, and reduce the load of new proteins entering the ER [247].
An impaired UPR can lead to ER stress, and prolonged ER stress may result in inflammation and apoptosis, which is observed in ALD. The downstream effects of ER stress include the activation of autophagy: the c-Jun N-terminal kinase (JNK) pathways: modulation of Toll-like receptor (TLR) signaling: and macrophage activation in alcohol- and obesity-induced synergistic liver injury [248]. The liver-specific deletion of GRP78 impairs global UPR, exacerbating ER stress and alcohol-mediated liver injury [248].

Central
Marroni et al. (2016)Email:
J Liver Clin Res 3(2): 1028 (2016) 15/24
The redox potential of iron, an effective agent in ROS generation, induces to tissue oxidative stress through the Fenton reaction. This stress leads to the lipid peroxidation of cell membranes, fibrosis, and damage to cell organelles, such as lysosomes and mitochondria [248]. Rats that are fed with iron-overloaded ethanol develop cirrhosis associated with lipid peroxidation, and multiple genes are activated [218]. Iron accumulation can activate Kupffer cells and release pro-inflammatory cytokines [248].
The pathogenic interactions between iron, fat, and alcohol in the liver highlight the potentially crucial role of iron toxicity-mediated ER stress and impaired autophagy in the pathogenesis of liver fibrosis [248].
Bacterial Translocation in Alcoholic Liver Disease: The chronic consumption of alcohol is accompanied by intestinal dysbiosis. This effect is an important factor in the development of ALD, the progression of which is influenced by the presence of bacterial products from the intestines [249]. Alcoholic dysbiosis is characterized by reduced proportions of commensal probiotic bacteria, such as Lactobacillus species, in animal models and humans with cirrhosis [249]. The interaction between the microbiome and the liver is of particular interest because increased levels of bacterial endotoxins are found in the portal circulation in ALD [250]. Alcohol intake modifies the epithelial barrier of the gastrointestinal tract (GIT) in dose-dependent manner, contributing to abnormalities in the gut-liver axis in ALD [251,252]. When consumed, 90% of the ingested alcohol is absorbed in the upper GIT, where it spreads throughout the body [241]. Endotoxins derive predominantly from Gram-negative bacteria and bind to and activate KCs. KCs secrete cytokines, including TNF-α, leading to hepatic inflammation [239]. In liver, KCs and recruited macrophages are activated by the LPS through Toll-like receptor 4 (TLR4). In addition, the level of LPS is increased in both the portal and systemic circulation after excessive alcohol intake [250,253]. LPS is translocated from the gut and binds to TLR4 receptors in cells of the hepatic parenchyma, resulting in hepatic inflammation and hepatocyte death [249]. LPS activation of TRL4 stimulates KCs to release ROS and cytokines that attract neutrophils, inhibit NK function, and alter allogenic antigen presentation [253].
The analyses of intestinal contents from mice submitted to an experimental model of ALD known as the Tsukamoto-French model revealed alcohol-associated changes to the intestinal metagenome and metabolome, characterized by reduced synthesis of saturated long-chain fatty acids (LCFA) [249, 252].
The Osteopontin Pathway in Alcoholic Liver Disease: The osteopontin (OPN) pathway has an important role in the pathogenicity of liver injury and is positively correlated with disease severity in patients with progressive stages of ALD [254]. OPN is an extracellular matrix protein secreted by various tissues that has been shown to modulate inflammation, steatosis, immune responses, and tumor formation in several tissues, including the liver [207].
An in vivo study showed that a single acute dose of alcohol significantly increases the hepatic expression of OPN in dose-dependent manner, in addition to activating OPN receptors
[αvβ3-integrin and CD44] and hepatic stellate cells. These effects were accompanied by Akt and Erk phosphorylation and increases in the expression of various genes. These genes were found to be in pathways related to fibrogenesis, fibrinolysis and the extracellular matrix, indicating the activation of fibrotic events. OPN is a key mediator of acute alcohol-induced activation and the initiation of pro-fibrogenic processes in hepatic stellate cells [254].
Autophagy in Alcoholic Liver Disease: Autophagy and apoptosis are important cellular functions that are required for the mitigation of cellular stress and in the prevention of disease. Although they are described as acting independently, autophagy can modulate apoptosis. Autophagy is primarily a mechanism of cell survival, while apoptosis is primarily a mechanism of cell death [255].
Autophagy represents a preserved catabolic process that is dependent on lysosomes, which degrade damaged and/or unnecessary proteins and cell organelles [240,255,256]. In in vivo mouse studies and in vitro hepatocyte culture experiments, the activation of autophagy protects against alcohol-induced liver injury and steatosis [240]. Autophagy occurs in four steps: a) Induction: autophagy begins with the dissociation of mammalian target of rapamycin complex 1 (mTORC1) from the ULK1 complex; b) Vesicle nucleation: during this step, proteins and lipids are recruited for autophagosome formation; c) Vesicle expansion and completion: membranes assemble at the PAS directly from the endoplasmic reticulum or by de-novo vesicular addition; the membranes then seal to form the autophagosome; and d) Autolysosome formation: the outer layer of the autophagosomes fuses with the lysosomes (forming an autolysosome), resulting in degradation of the sequestered material [255]. Autophagy and lysosome biogenesis is controlled by the nuclear transcription factor EB (TFEB). In mice, the acute administration of alcohol increases hepatic levels of TFEB and enhances the autophagy process, while chronic administration of alcohol precludes autophagy and decreases hepatic levels of TFEB [257]. Autophagy decreases in ALD, resulting in protein accumulation and decreased hepatocyte depuration. In experimental mice with autophagy loss, intracellular inclusions referred to as Mallory-Denk bodies are formed in hepatocytes [258]. The mechanism proposed for the decreased autophagy observed with the chronic use of alcohol is decreased activity of adenosine monophosphate-activated protein kinase (AMPk). This effect leads to decreased autophagy via the mTOR pathway and disrupted intracellular vesicle transport due to altered functions of microtubules and microfilaments [255].
Role of Sirtuins in Alcoholic Liver Disease: Acetylation is an important posttranslational modification that regulates proteins, and in this context, sirtuins (SIRT), a family of NAD+ dependent deacetylases, have recently been implicated in the pathogenesis of ALD [241]. The chronic administration of ethanol to rodents impairs hepatic lipid metabolism pathways by modulating SIRT1 and inducing the development of fatty liver through the regulation of mitochondrial energy metabolism and mitochondrial biogenesis [241,259]. Male mice with liver-specific deletion of SIRT1 that are administered Lieber-DeCarli ethanol-containing diets accumulate more lipids in the liver,

Central
Marroni et al. (2016)Email:
J Liver Clin Res 3(2): 1028 (2016) 16/24
causing failure in their metabolism. This effect primarily occurs via increased activity of lipin-1, an important transcriptional regulator of lipid metabolism [259]. Decreased SIRT1 and increased lipin-1 aggravate ALD and are associated with a rapid onset and progression of steatosis, inflammation and fibrosis [243,259].
Sirtuins are also implicated in the modulation of ROS levels and in the inflammatory process. A reduction in ROS levels is related to SIRT3 and occurs through deacetylation and activation of the antioxidant SOD. While SIRT1 inactivates subunit P65 of NF-κB through direct acetylation, NF-κB inhibition suppresses inducible nitric oxide synthase (iNOS] and nitrous acid production [241].
The Role of Hypoxia in Alcoholic Liver Disease: Chronic consumption of ethanol increases the consumption of hepatic oxygen, resulting in hypoxia and steatosis and leading to cell death by apoptosis and necrosis, factors that contribute to the pathogenesis of ALD [240].
Hypoxia-inducible factors (HIFs) constitute a family of transcription factors that are activated in response to hypoxia. HIFs are transcription factors composed of an oxygen-sensitive α subunit and an oxygen insensitive, constitutively expressed b subunit. There are three HIF-α subunits (HIF1-α, HIF-2α and HIF-3α), and all are expressed in the liver. Under normoxic conditions, the α subunit is hydroxylated at specific proline residues, which targets it for ubiquitination by the von Hippel-Lindau (VHL) tumor suppressor [240]. Hepatocyte-specific HIF-1β knockout mice were resistant to alcohol-induced steatosis and liver injury following Gao-binge treatment [240]. These mice are resistant to alcohol-induced steatosis and liver injury in the Gao-binge model, and this protection was associated with activation of FoxO3a-mediated hepatic autophagy, suggesting a possible detrimental role of alcohol-induced HIF-1 activation in ALD [240].
DISCUSSION & CONCLUSIONTherefore, alcohol metabolites, oxidative stress, ER stress,
increased intestinal permeability to bacterial products, and inflammation play major roles in alcohol-induced liver injury [242].
In an attempt to investigate treatment targets, a number of new concepts and new techniques, presented here, can benefit research on ALD. Future areas of investigation should take into account the patient’s genome, genetics in general, and epigenetics to evaluate alcohol’s actions in real time and treatment targets for ALD.
CONFLICT OF INTERESTThe authors of this article declare that they have no conflicts
of interest.
ACKNOWLEDGEMENTSThis study was supported by grants from the following
Brazilian agencies: Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES), Fundação de Amparo à Pesquisa do Estado do Rio Grande do Sul (FAPERGS), and National Counsel of Technological and Scientific Development (Conselho Nacional de Desenvolvimento Científico e Tecnológico – CNPq
REFERENCES1. Iruzubieta P, Crespo J, Fábrega E. Long-term survival after liver
transplantation for alcoholic liver disease. World J Gastroenterol. 2013; 19: 9198-9208.
2. Addolorato G1. Alcoholic Hepatitis and Liver Transplantation: The Good News and What to Do about It. Front Psychiatry. 2012 Jan 10; 2: 80.
3. Marroni CA. Management of alcohol recurrence before and after liver transplantation. Clin Res Hepatol Gastroenterol. 2015; 39 Suppl 1: 109-114.
4. DSM. Diagnostic and Statistical Manual of Mental Disorders. 5 ed. Washington: American Psychiatric Association press; 2013.
5. Gao B, Bataller R. Alcoholic liver disease: pathogenesis and new therapeutic targets. Gastroenterology. 2011; 141: 1572-1585.
6. Vuittonet CL, Halse M, Leggio L, Fricchione SB, Brickley M, Haass-Koffler CL, et al. Pharmacotherapy for alcoholic patients with alcoholic liver disease. Am J Health Syst Pharm. 2014; 71: 1265-1276.
7. Zaridze D, Lewington S, Boroda A, Scélo G, Karpov R, Lazarev A, et al. Alcohol and mortality in Russia: prospective observational study of 151,000 adults. Lancet. 2014; 383: 1465-1473.
8. Rehm J, Mathers C, Popova S, Thavorncharoensap M, Teerawattananon Y, Patra J, et al. Global burden of disease and injury and economic cost attributable to alcohol use and alcohol-use disorders. Lancet. 2009; 373: 2223-2233.
9. Rehm J, Samokhvalov AV, Shield KD. Global burden of alcoholic liver diseases. J Hepatol. 2013; 59: 160-168.
10. Wang YP, Andrade LH. Epidemiology of alcohol and drug use in the elderly. Curr Opin Psychiatry. 2013; 26: 343-348.
11. Taufick ML, Evangelista LA, Silva M, Oliveira LC. Alcohol consumption patterns among patients in primary health care and detection by health professionals. Cad Saude Publica. 2014; 30: 427-432.
12. Murray CJ, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012; 380: 2197-2223.
13. Monteiro MG. Alcohol and public health in Latin America: how to prevent a health disaster?]. Adicciones. 2013; 25: 99-105.
14. Méndez-Sánchez N, Villa AR, Chávez-Tapia NC, Ponciano-Rodriguez G, Almeda-Valdés P, González D, et al. Trends in liver disease prevalence in Mexico from 2005 to 2050 through mortality data. Ann Hepatol. 2005.4: 52-55.
15. Laranjeira R, Madruga CS, Pinsky I, Caetano R, Mitsuhiru S. II Levantamento Nacional de lcool e Drogas - Consumo de lcool no Brasil: Tendncias entre 2006/2012 So Paulo: INPAD; 2013.
16. Nader LA, de Mattos AA, Bastos GA. Burden of liver disease in Brazil. Liver Int. 2014; 34: 844-849.
17. Portugal FB, Campos MR, de Carvalho JR, Flor LS, Schramm JM, Costa Mde F. Disease burden in Brazil: an investigation into alcohol and non-viral cirrhosis. Cien Saude Colet. 2015; 20: 491-501.
18. Paula H, Asrani SK, Boetticher NC, Pedersen R, Shah VH, Kim WR. Alcoholic liver disease-related mortality in the United States: 1980-2003. Am J Gastroenterol. 2010; 105: 1782-1787.
19. Day CP. Who gets alcoholic liver disease: nature or nurture? J R Coll Physicians Lond. 2000; 34: 557-562.
20. Lucey MR, Mathurin P, Morgan TR. Alcoholic hepatitis. N Engl J Med. 2009; 360: 2758-2769.

Central
Marroni et al. (2016)Email:
J Liver Clin Res 3(2): 1028 (2016) 17/24
21. Trimble G, Zheng L, Mishra A, Kalwaney S, Mir HM, Younossi ZM. Mortality associated with alcohol-related liver disease. Aliment Pharmacol Ther. 2013; 38: 596-602.
22. Wang H, Dwyer-Lindgren L, Lofgren KT, Rajaratnam JK, Marcus JR, Levin-Rector A, et al. Age-specific and sex-specific mortality in 187 countries, 1970-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012; 380: 2071-2094.
23. Dawson DA, Goldstein RB2, Saha TD3, Grant BF3. Changes in alcohol consumption: United States, 2001-2002 to 2012-2013. Drug Alcohol Depend. 2015; 148: 56-61.
24. WHO. European Status Report on Alcohol and Health Copenhagen: World Health Organization Regional Office for Europe. 2010.
25. Deleuran T, Vilstrup H, Becker U, Jepsen P. Epidemiology of alcoholic liver disease in Denmark 2006-2011: a population-based study. Alcohol Alcohol. 2015; 50: 352-357.
26. Shah VH. Alcoholic liver disease: the buzz may be gone, but the hangover remains. Hepatology. 2010; 51:1483-1484.
27. Becker U, Deis A, Sørensen TI, Grønbaek M, Borch-Johnsen K, Müller CF, et al. Prediction of risk of liver disease by alcohol intake, sex, and age: a prospective population study. Hepatology. 1996; 23:1025-1029.
28. Bellentani S, Saccoccio G, Costa G, Tiribelli C, Manenti F, Sodde M, et al. Drinking habits as cofactors of risk for alcohol induced liver damage. The Dionysos Study Group. Gut. 1997; 41: 845-850
29. Teli MR, Day CP, Burt AD, Bennett MK, James OF. Determinants of progression to cirrhosis or fibrosis in pure alcoholic fatty liver. Lancet. 1995; 346: 987-990.
30. O’Shea RS, Dasarathy S, McCullough AJ. Alcoholic liver disease. Am J Gastroenterol. 2010; 105: 14-32.
31. Mandayam S, Jamal MM, Morgan TR. Epidemiology of alcoholic liver disease. Semin Liver Dis. 2004; 24: 217-232.
32. Sanyal AJ, Brunt EM, Kleiner DE, Kowdley KV, Chalasani N, Lavine JE, et al. Endpoints and clinical trial design for nonalcoholic steatohepatitis. Hepatology. 2011; 54: 344-353.
33. Lu XL, Luo JY, Tao M, Gen Y, Zhao P, Zhao HL, et al. Risk factors for alcoholic liver disease in China. World J Gastroenterol. 2004; 10: 2423-2426.
34. Loft S, Olesen KL, Døssing M. Increased susceptibility to liver disease in relation to alcohol consumption in women. Scand J Gastroenterol. 1987; 22: 1251-1256.
35. Norton R, Batey R, Dwyer T, MacMahon S. Alcohol consumption and the risk of alcohol related cirrhosis in women. Br Med J (Clin Res Ed). 1987; 80-82.
36. Parés A, Caballería J, Bruguera M, Torres M, Rodés J. Histological course of alcoholic hepatitis. Influence of abstinence, sex and extent of hepatic damage. J Hepatol. 1986; 2: 33-42.
37. Sato N, Lindros KO, Baraona E, Ikejima K, Mezey E, Järveläinen HA, et al. Sex difference in alcohol-related organ injury. Alcohol Clin Exp Res. 2001; 25: 40-45.
38. Eagon PK. Alcoholic liver injury: influence of gender and hormones. World J Gastroenterol. 2010; 16: 1377-1384.
39. Baraona E, Abittan CS, Dohmen K, Moretti M, Pozzato G, Chayes ZW, et al. Gender differences in pharmacokinetics of alcohol. Alcohol Clin Exp Res. 2001; 25: 502-507.
40. Frezza M, di Padova C, Pozzato G, Terpin M, Baraona E, Lieber CS, et al. High blood alcohol levels in women. The role of decreased gastric alcohol dehydrogenase activity and first-pass metabolism. N Engl J Med. 1990; 322: 95-99.
41. Hrubec Z, Omenn GS. Evidence of genetic predisposition to alcoholic cirrhosis and psychosis: twin concordances for alcoholism and its biological end points by zygosity among male veterans. Alcohol Clin Exp Res. 1981; 5: 207-215.
42. Reed T, Page WF, Viken RJ, Christian JC. Genetic predisposition to organ-specific endpoints of alcoholism. Alcohol Clin Exp Res. 1996; 20: 1528-1533.
43. Stewart SH, Connors GJ. Ethnicity, alcohol drinking and changes in transaminase activity among heavy drinkers. J Natl Med Assoc. 2007; 99: 564-569.
44. Wickramasinghe SN, Corridan B, Izaguirre J, Hasan R, Marjot DH. Ethnic differences in the biological consequences of alcohol abuse: a comparison between south Asian and European males. Alcohol Alcohol. 1995; 30: 675-680.
45. Stinson FS, Grant BF, Dufour MC. The critical dimension of ethnicity in liver cirrhosis mortality statistics. Alcohol Clin Exp Res. 2001; 25: 1181-1187.
46. Mendenhall C, Roselle GA, Gartside P, Moritz T. Relationship of protein calorie malnutrition to alcoholic liver disease: a reexamination of data from two Veterans Administration Cooperative Studies. Alcohol Clin Exp Res. 1995; 19: 635-641.
47. Iturriaga H, Bunout D, Hirsch S, Ugarte G. Overweight as a risk factor or a predictive sign of histological liver damage in alcoholics. Am J Clin Nutr. 1988; 47: 235-238.
48. Naveau S, Giraud V, Borotto E, Aubert A, Capron F, Chaput JC, et al. Excess weight risk factor for alcoholic liver disease. Hepatology. 1997; 25: 108-11.
49. Degos F. Hepatitis C and alcohol. J Hepatol. 1999; 31 Suppl 1: 113-118.
50. Monto A, Patel K, Bostrom A, Pianko S, Pockros P, McHutchison JG, et al. Risks of a range of alcohol intake on hepatitis C-related fibrosis. Hepatology. 2004; 39: 826-834.
51. Befrits R, Hedman M, Blomquist L, Allander T, Grillner L, Kinnman N, et al. Chronic hepatitis C in alcoholic patients: prevalence, genotypes, and correlation to liver disease. Scand J Gastroenterol. 1995; 30:1113-1138.
52. Harris DR, Gonin R, Alter HJ, Wright EC, Buskell ZJ, Hollinger FB, et al. The relationship of acute transfusion-associated hepatitis to the development of cirrhosis in the presence of alcohol abuse. Ann Intern Med. 2001; 134: 120-124.
53. McClain CJ, Song Z, Barve SS, Hill DB, Deaciuc I. Recent advances in alcoholic liver disease. IV. Dysregulated cytokine metabolism in alcoholic liver disease. Am J Physiol Gastrointest Liver Physiol. 2004; 287: 497-502.
54. Monzoni A, Masutti F, Saccoccio G, Bellentani S, Tiribelli C, Giacca M, et al. Genetic determinants of ethanol-induced liver damage. Mol Med. 2001; 7: 255-262.
55. Friedman SL, Runyon BA, Travis AC. Clinical manifestations and diagnosis of alcoholic fatty liver disease and alcoholic cirrhosis: UP TO DATE. 2015.
56. Girela E, Villanueva E, Hernandez-Cueto C, Luna JD. Comparison of the CAGE questionnaire versus some biochemical markers in the diagnosis of alcoholism. Alcohol Alcohol. 1994; 29: 337-343.
57. Soderstrom CA, Smith GS, Kufera JA, Dischinger PC, Hebel JR, McDuff DR, et al. The accuracy of the CAGE, the Brief Michigan Alcoholism Screening Test, and the Alcohol Use Disorders Identification Test in screening trauma center patients for alcoholism. J Trauma. 1997; 43: 962-969.
58. Skinner HA, Sheu WJ. Reliability of alcohol use indices. The Lifetime

Central
Marroni et al. (2016)Email:
J Liver Clin Res 3(2): 1028 (2016) 18/24
Drinking History and the MAST. J Stud Alcohol. 1982; 43: 1157-1170.
59. Ewing JA. Detecting alcoholism. The CAGE questionnaire. JAMA. 1984; 252: 1905-1907.
60. Bataille V, Ruidavets JB, Arveiler D, Amouyel P, Du Ducimetière Pcimeti re P, Perret B, et al. Joint use of clinical parameters, biological markers and CAGE questionnaire for the identification of heavy drinkers in a large population-based sample. Alcohol Alcohol. 2003; 38: 121-127.
61. Saunders JB, Aasland OG, Babor TF, de la Fuente JR, Grant M. Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO Collaborative Project on Early Detection of Persons with Harmful Alcohol Consumption--II. Addiction. 1993; 88: 791-804.
62. Fiellin DA, Reid MC, O’Connor PG. Screening for alcohol problems in primary care: a systematic review. Arch Intern Med. 2000; 160: 1977-1989.
63. MacKenzie D, Langa A, Brown TM. Identifying hazardous or harmful alcohol use in medical admissions: a comparison of audit, cage and brief mast. Alcohol Alcohol. 1996; 31: 591-599.
64. Bradley KA, Bush KR, McDonell MB, Malone T, Fihn SD, Project ACQI, et al. Screening for problem drinking : Comparison of CAGE and AUDIT. J Gen Intern Med. 1998; 13: 379-388.
65. Steinbauer JR, Cantor SB, Holzer CE 3rd, Volk RJ. Ethnic and sex bias in primary care screening tests for alcohol use disorders. Ann Intern Med. 1998; 129: 353-362.
66. Levine J. The relative value of consultation, questionnaires and laboratory investigation in the identification of excessive alcohol consumption. Alcohol Alcohol. 1990; 25: 539-553.
67. Helander A, Eriksson CJ, Investigators WISoSaTMoUaD. Laboratory tests for acute alcohol consumption: results of the WHO/ISBRA Study on State and Trait Markers of Alcohol Use and Dependence. Alcohol Clin Exp Res. 2002; 26: 1070-1077.
68. Aalto M, Seppa. Use of laboratory markers and the audit questionnaire by primary care physicians to detect alcohol abuse by patients. Alcohol & Alcoholism. 2005; 40: 520-523.
69. Sharpe PC. Biochemical detection and monitoring of alcohol abuse and abstinence. Ann Clin Biochem. 2001; 38: 652-664.
70. Sears D. Fatty Liver. Medscape. 2015.
71. Crabb DW. Pathogenesis of alcoholic liver disease: newer mechanisms of injury. Keio J Med. 1999; 48: 184-188.
72. Fromenty B, Grimbert S, Mansouri A, Beaugrand M, Erlinger S, Rötig A, et al. Hepatic mitochondrial DNA deletion in alcoholics: association with microvesicular steatosis. Gastroenterology. 1995;108:193-200.
73. Hubscher S. Alcohol-induced liver disease. In: Saxena R, editor. Pratical Hepatic Pathology a diagnostic approach: Elsevier Saunders; 2011.
74. Crawford JM. Histologic findings in alcoholic liver disease. Clin Liver Dis. 2012; 16: 699-716.
75. Lefkowitch JH. Morphology of alcoholic liver disease. Clin Liver Dis. 2005; 9: 37-53.
76. Mathurin P, Beuzin F, Louvet A, Carrié-Ganne N, Balian A, Trinchet JC, et al. Fibrosis progression occurs in a subgroup of heavy drinkers with typical histological features. Aliment Pharmacol Ther. 2007; 25:1047-1054.
77. Goodman ZD, Ishak KG. Occlusive venous lesions in alcoholic liver disease. A study of 200 cases. Gastroenterology. 1982; 83: 786-996.
78. Neil D, Theise M. Histopathology of Alcoholic Liver Disease. Clin Liver Dis. 2013; 2: 64-67.
79. Sakhuja P. Pathology of alcoholic liver disease, can it be differentiated
from nonalcoholic steatohepatitis? World J Gastroenterol. 2014; 20:16474-16479.
80. O’Shea RS, Dasarathy S, McCullough AJ; Practice Guideline Committee of the American Association for the Study of Liver Diseases; Practice Parameters Committee of the American College of Gastroenterology. Alcoholic liver disease. Hepatology. 2010; 51: 307-328.
81. Spahr L, Rubbia-Brandt L, Genevay M, Hadengue A, Giostra E. Early liver biopsy, intraparenchymal cholestasis, and prognosis in patients with alcoholic steatohepatitis. BMC Gastroenterol. 2011; 11: 115.
82. Altamirano J, Miquel R, Katoonizadeh A, Abraldes JG, Duarte-Rojo A, Louvet A, et al. A histologic scoring system for prognosis of patients with alcoholic hepatitis. Gastroenterology. 2014; 146: 1231-1239.
83. Saunders JB, Walters JR, Davies AP, Paton A. A 20-year prospective study of cirrhosis. Br Med J (Clin Res Ed). 1981; : 263-6.
84. Pateria P, de Boer B, MacQuillan G. Liver abnormalities in drug and substance abusers. Best Pract Res Clin Gastroenterol. 2013; 27: 577-596.
85. Okazaki H, Ito K, Fujita T, Koike S, Takano K, Matsunaga N, et al. Discrimination of alcoholic from virus-induced cirrhosis on MR imaging. AJR Am J Roentgenol. 2000; 175: 1677-1681.
86. Jaurigue MM, Cappell MS. Therapy for alcoholic liver disease. World J Gastroenterol. 2014; 20: 2143-2158.
87. Jepsen P, Ott P, Andersen PK, S Sørensen HT, Vilstrup H. Clinical course of alcoholic liver cirrhosis: a Danish population-based cohort study. Hepatology. 2010; 51: 1675-1682.
88. Fleming KM, Aithal GP, Card TR, West J. The rate of decompensation and clinical progression of disease in people with cirrhosis: a cohort study. Aliment Pharmacol Ther. 2010; 32: 1343-1350.
89. Chedid A, Mendenhall CL, Gartside P, French SW, Chen T, Rabin L , et al. Prognostic factors in alcoholic liver disease. VA Cooperative Study Group. Am J Gastroenterol. 1991; 86: 210-216.
90. Tandon P, Garcia-Tsao G. Bacterial infections, sepsis, and multiorgan failure in cirrhosis. Semin Liver Dis. 2008; 28: 26-42.
91. N’Kontchou G, Paries J, Htar MT, Ganne-Carrie N, Costentin L, Grando-Lemaire V, et al. Risk factors for hepatocellular carcinoma in patients with alcoholic or viral C cirrhosis. Clin Gastroenterol Hepatol. 2006; 4:1062-1068.
92. Kazemi-Shirazi L, Veloso MP, Frommlet F, Steindl-Munda P, Wrba F, Zehetmayer S, et al. Differentiation of nonalcoholic from alcoholic steatohepatitis: are routine laboratory markers useful? Wien Klin Wochenschr. 2008; 120: 25-30.
93. Morita Y, Ueno T, Sasaki N, Kuhara K, Yoshioka S, Tateishi Y, et al. Comparison of liver histology between patients with non-alcoholic steatohepatitis and patients with alcoholic steatohepatitis in Japan. Alcohol Clin Exp Res. 2005; 29: 277-281.
94. Diehl AM. Liver disease in alcohol abusers: clinical perspective. Alcohol. 2002; 27: 7-11.
95. Sorbi D, Boynton J, Lindor KD. The ratio of aspartate aminotransferase to alanine aminotransferase: potential value in differentiating nonalcoholic steatohepatitis from alcoholic liver disease. Am J Gastroenterol. 1999; 4: 1018-1022.
96. Nyblom H, Berggren U, Balldin J, Olsson R. High AST/ALT ratio may indicate advanced alcoholic liver disease rather than heavy drinking. Alcohol Alcohol. 2004; 39: 336-339.
97. Diehl AM, Potter J, Boitnott J, Van Duyn MA, Herlong HF, Mezey E, et al. Relationship between pyridoxal 5’-phosphate deficiency and aminotransferase levels in alcoholic hepatitis. Gastroenterology.

Central
Marroni et al. (2016)Email:
J Liver Clin Res 3(2): 1028 (2016) 19/24
1984; 86: 632-636.
98. Cohen JA, Kaplan MM. The SGOT/SGPT ratio--an indicator of alcoholic liver disease. Dig Dis Sci. 1979; 24: 835-838.
99. Uchida T, Kao H, Quispe-Sjogren M, Peters RL. Alcoholic foamy degeneration--a pattern of acute alcoholic injury of the liver. Gastroenterology. 1983; 84: 683-692.
100. Moussavian SN, Becker RC, Piepmeyer JL, Mezey E, Bozian RC. Serum gamma-glutamyl transpeptidase and chronic alcoholism. Influence of alcohol ingestion and liver disease. Dig Dis Sci. 1985; 30: 211-214.
101. Yersin B, Nicolet JF, Dercrey H, Burnier M, van Melle G, Pécoud A, et al. Screening for excessive alcohol drinking. Comparative value of carbohydrate-deficient transferrin, gamma-glutamyltransferase, and mean corpuscular volume. Arch Intern Med. 1995; 155:1907-1911.
102. Conigrave KM, Degenhardt LJ, Whitfield JB, Saunders JB, Helander A, Tabakoff B, et al. WHO/ISBRA Study Group. CDT, GGT, and AST as markers of alcohol use: the WHO/ISBRA collaborative project. Alcohol Clin Exp Res. 2002; 26: 332-339.
103. Sillanaukee P, Massot N, Jousilahti P, Vartiainen E, Sundvall J, Olsson U, et al. Dose response of laboratory markers to alcohol consumption in a general population. Am J Epidemiol. 2000; 152: 747-751.
104. Alte D, Luedemann J, Rose HJ, John U. Laboratory markers carbohydrate-deficient transferrin, gamma-glutamyltransferase, and mean corpuscular volume are not useful as screening tools for high-risk drinking in the general population: results from the Study of Health in Pomerania (SHIP). Alcohol Clin Exp Res. 2004; 28: 931-940.
105. Reynaud M, Schellenberg F, Loisequx-Meunier MN, Schwan R, Maradeix B, Planche F, et al. Objective diagnosis of alcohol abuse: compared values of carbohydrate-deficient transferrin (CDT), gamma-glutamyl transferase (GGT), and mean corpuscular volume (MCV). Alcohol Clin Exp Res. 2000; 24:1414-1419.
106. Poynard T, Zourabichvili O, Hilpert G, Naveau S, Poitrine A, Benatar C, et al. Prognostic value of total serum bilirubin/gamma-glutamyl transpeptidase ratio in cirrhotic patients. Hepatology. 1984;4: 324-327.
107. Puukka K, Hietala J, Koivisto H, Anttila P, Bloigu R, Niemelä O, et al. Additive effects of moderate drinking and obesity on serum gamma-glutamyl transferase activity. Am J Clin Nutr. 2006; 83: 1351-1354.
108. Hartmann S, Aradottir S, Graf M, Wiesbeck G, Lesch O, Ramskogler K, et al. Phosphatidylethanol as a sensitive and specific biomarker: comparison with gamma-glutamyl transpeptidase, mean corpuscular volume and carbohydrate-deficient transferrin. Addict Biol. 2007; 12: 81-84.
109. Hannuksela ML, Liisanantti MK, Nissinen AE, Savolainen MJ. Biochemical markers of alcoholism. Clin Chem Lab Med. 2007; 45: 953-961.
110. Bortolotti F, De Paoli G, Tagliaro F. Carbohydrate-deficient transferrin (CDT) as a marker of alcohol abuse: a critical review of the literature 2001-2005. J Chromatogr B Analyt Technol Biomed Life Sci. 2006 ; 841: 96-109.
111. Wurst FM, Alling C, Aradottir S, Pragst F, Allen JP, Weinmann W, et al. Emerging biomarkers: new directions and clinical applications. Alcohol Clin Exp Res. 2005; 29: 465-473.
112. Hock B, Schwarz M, Domke I, Grunert VP, Wuertemberger M, Schiemann U, et al. Validity of carbohydrate-deficient transferrin (%CDT), gamma-glutamyltransferase (gamma-GT) and mean corpuscular erythrocyte volume (MCV) as biomarkers for chronic alcohol abuse: a study in patients with alcohol dependence and
liver disorders of non-alcoholic and alcoholic origin. Addiction. 2005;100:1477-1486.
113. Anttila P, Järvi K, Latvala J, Romppanen J, Punnonen K, Niemelä O, et al. Biomarkers of alcohol consumption in patients classified according to the degree of liver disease severity. Scand J Clin Lab Invest. 2005; 65:141-151.
114. The Role of Biomarkers in the Treatment of Alcohol Use Disorders. Substance Abuse Treatment Advisory . Center for Substance Abuse Treatment. 2006.
115. Haller DL, Acosta MC, Lewis D, Miles DR, Schiano T, Shapiro PA, et al. Hair analysis versus conventional methods of drug testing in substance abusers seeking organ transplantation. Am J Transplant. 2010; 10: 1305-1311.
116. Sterneck M, Yegles M, Rothkirch von G, Staufer K, Vettorazzi E, Schulz KH, et al. Determination of ethyl glucuronide in hair improves evaluation of long-term alcohol abstention in liver transplant candidates. Liver Int. 2014; 34: 469-476.
117. Das SK, Mukherjee S, Vasudevan DM, Balakrishnan V. Comparison of haematological parameters in patients with non-alcoholic fatty liver disease and alcoholic liver disease. Singapore Med J. 2011; 52:175-81.
118. Naveau S, Raynard B, Ratziu V, Abella A, Imbert-Bismut F, Messous D, et al. Biomarkers for the prediction of liver fibrosis in patients with chronic alcoholic liver disease. Clin Gastroenterol Hepatol. 2005; 3: 167-174.
119. Calès P, Oberti F, Michalak S, Hubert-Fouchard I, Rousselet MC, Konaté A, et al. A novel panel of blood markers to assess the degree of liver fibrosis. Hepatology. 2005; 42:1373-1381.
120. Naveau S, Gaudé G, Asnacios A, Agostini H, Abella A, Barri-Ova N, et al. Diagnostic and prognostic values of noninvasive biomarkers of fibrosis in patients with alcoholic liver disease. Hepatology. 2009; 49: 97-105.
121. Castera L, Pinzani M. Biopsy and non-invasive methods for the diagnosis of liver fibrosis: does it take two to tango? Gut. 2010; 59: 861-866.
122. Mueller S, Sandrin L. Liver stiffness: a novel parameter for the diagnosis of liver disease. Hepat Med. 2010; 2: 49-67.
123. Mueller S, Millonig G, Sarovska L, Friedrich S, Reimann FM, Pritsch M, et al. Increased liver stiffness in alcoholic liver disease: differentiating fibrosis from steatohepatitis. World J Gastroenterol. 2010;16: 966-972.
124. Gelsi E, Dainese R, Truchi R, Mariné-Barjoan E, Anty R, Autuori M, et al. Effect of detoxification on liver stiffness assessed by Fibroscan in alcoholic patients. Alcohol Clin Exp Res. 2011; 35: 566-570.
125. Schiano TD, Bodian C, Schwartz ME, Glajchen N, Min AD. Accuracy and significance of computed tomographic scan assessment of hepatic volume in patients undergoing liver transplantation. Transplantation. 2000; 69: 545-550.
126. Bird GL. Investigation of alcoholic liver disease. Baillieres Clin Gastroenterol. 1993; 7: 663-82.
127. Vilgrain V. Ultrasound of diffuse liver disease and portal hypertension. Eur Radiol. 2001; 11: 1563-1577.
128. Palmentieri B1, de Sio I, La Mura V, Masarone M, Vecchione R, Bruno S, et al. The role of bright liver echo pattern on ultrasound B-mode examination in the diagnosis of liver steatosis. Dig Liver Dis. 2006; 38: 485-9.
129. Saverymuttu SH, Joseph AE, Maxwell JD. Ultrasound scanning in the detection of hepatic fibrosis and steatosis. Br Med J (Clin Res Ed).

Central
Marroni et al. (2016)Email:
J Liver Clin Res 3(2): 1028 (2016) 20/24
1986; : 13-15.
130. Mathiesen UL, Franzén LE, Aselius H, Resjö M, Jacobsson L, Foberg U, et al. Increased liver echogenicity at ultrasound examination reflects degree of steatosis but not of fibrosis in asymptomatic patients with mild/moderate abnormalities of liver transaminases. Dig Liver Dis. 2002; 34: 516-522.
131. Ratziu V, Bellentani S, Cortez-Pinto H, Day C, Marchesini G. A position statement on NAFLD/NASH based on the EASL 2009 special conference. J Hepatol. 2010; 53: 372-384.
132. Mortele KJ, Ros PR. Imaging of diffuse liver disease. Semin Liver Dis. 2001; 21: 195-212.
133. Lucey MR. Management of alcoholic liver disease. Clin Liver Dis. 2009; 13: 267-275.
134. Rustad JK, Stern TA, Prabhakar M, Musselman D. Risk factors for alcohol relapse following orthotopic liver transplantation: a systematic review. Psychosomatics. 2015; 56: 21-35.
135. Pfitzmann R, Schwenzer J, Rayes N, Seehofer D, Neuhaus R, N ssler NC. Long-term survival and predictors of relapse after orthotopic liver transplantation for alcoholic liver disease. Liver Transpl. 2007 ; 13: 197-205.
136. Lamba S, Nagurka R, Desai KK, Chun SJ, Holland B, Koneru B, et al. Self-reported non-adherence to immune-suppressant therapy in liver transplant recipients: demographic, interpersonal, and intrapersonal factors. Clin Transplant. 2012; 26: 328-335.
137. Björnsson E, Olsson J, Rydell A, Fredriksson K, Eriksson C, Sjöberg C, et al. Long-term follow-up of patients with alcoholic liver disease after liver transplantation in Sweden: impact of structured management on recidivism. Scand J Gastroenterol. 2005; 40: 206-216.
138. Plauth M, Cabré E, Riggio O, Assis-Camilo M, Pirlich M, Kondrup J; DGEM (German Society for Nutritional Medicine), et al. ESPEN Guidelines on Enteral Nutrition: Liver disease. Clin Nutr. 2006; 25: 285-94.
139. Pegum N, Connor JP, Young RM, Feeney GF. Psychosocial functioning in patients with alcohol-related liver disease post liver transplantation. Addict Behav. 2015; 45:70-73.
140. McClain CJ, Barve SS, Barve A, Marsano L. Alcoholic liver disease and malnutrition. Alcohol Clin Exp Res. 2011; 35: 815-820.
141. Tsiaousi ET, Hatzitolios AI, Trygonis SK, Savopoulos CG. Malnutrition in end stage liver disease: recommendations and nutritional support. J Gastroenterol Hepatol. 2008; 23: 527-533.
142. Huisman EJ, Trip EJ, Siersema PD, van Hoek B, van Erpecum KJ. Protein energy malnutrition predicts complications in liver cirrhosis. Eur J Gastroenterol Hepatol. 2011; 23: 982-989.
143. Koretz RL, Avenell A, Lipman TO. Nutritional support for liver disease. Cochrane Database Syst Rev. 2012 16; 008344.
144. Plauth M, Cabré E, Campillo B, Kondrup J, Marchesini G, Schütz T, et al. ESPEN Guidelines on Parenteral Nutrition: hepatology. Clin Nutr. 2009; 28: 436-444.
145. Poh Z, Chang PE. A current review of the diagnostic and treatment strategies of hepatic encephalopathy. Int J Hepatol. 2012: 480309.
146. Addolorato G, Leggio L, Ferrulli A, Cardone S, Vonghia L, Mirijello A, et al. Effectiveness and safety of baclofen for maintenance of alcohol abstinence in alcohol-dependent patients with liver cirrhosis: randomised, double-blind controlled study. Lancet. 2007; 370:1915-1922.
147. Addolorato G, Mirijello A, Leggio L, Ferrulli A, D’Angelo C, Vassallo G,
et al. Liver transplantation in alcoholic patients: impact of an alcohol addiction unit within a liver transplant center. Alcohol Clin Exp Res. 2013; 37: 1601-1618.
148. Leggio L, Ferrulli A, Zambon A, Caputo F, Kenna GA, Swift RM, et al. Baclofen promotes alcohol abstinence in alcohol dependent cirrhotic patients with hepatitis C virus (HCV) infection. Addict Behav. 2012; 37: 561-564.
149. Rice JP, Eickhoff J, Agni R, Ghufran A, Brahmbhatt R, Lucey MR, et al. Abusive drinking after liver transplantation is associated with allograft loss and advanced allograft fibrosis. Liver Transpl. 2013 ; 19:1377-1386.
150. Addolorato G, Caputo F, Capristo E, Domenicali M, Bernardi M, Janiri L, et al. Baclofen efficacy in reducing alcohol craving and intake: a preliminary double-blind randomized controlled study. Alcohol Alcohol. 2002; 37: 504-508.
151. Dew MA, DiMartini AF, Steel J, De Vito Dabbs A, Myaskovsky L, Unruh M, et al. Meta-analysis of risk for relapse to substance use after transplantation of the liver or other solid organs. Liver Transpl. 2008; 14: 159-172.
152. Fuller RK. Definition and diagnosis of relapse to drinking. Liver Transpl Surg. 1997; 3: 258-62.
153. Leong J, Im GY. Evaluation and selection of the patient with alcoholic liver disease for liver transplant. Clin Liver Dis. 2012; 16: 851-863.
154. Dutkowski P, Linecker M, DeOliveira ML, Müllhaupt B, Clavien PA. Challenges to liver transplantation and strategies to improve outcomes. Gastroenterology. 2015; 148: 307-323.
155. Lucey MR. Liver transplantation in patients with alcoholic liver disease. Liver Transpl. 2011; 17: 751-759.
156. Pageaux GP, Bismuth M, Perney P, Costes V, Jaber S, Possoz P, et al. Alcohol relapse after liver transplantation for alcoholic liver disease: does it matter? J Hepatol. 2003; 38: 629-634.
157. Raynard B, Balian A, Fallik D, Capron F, Bedossa P, Chaput JC, et al. Risk factors of fibrosis in alcohol-induced liver disease. Hepatology. 2002; 35: 635-638.
158. Tome S, Lucey MR. Timing of liver transplantation in alcoholic cirrhosis. J Hepatol. 2003; 39: 302-307.
159. De Gottardi A, Spahr L, Gelez P, Morard I, Mentha G, Guillaud O, et al. A simple score for predicting alcohol relapse after liver transplantation: results from 387 patients over 15 years. Arch Intern Med. 2007; 167: 1183-1188.
160. Faure S, Herrero A, Jung B, Duny Y, Daures JP, Mura T, et al. Excessive alcohol consumption after liver transplantation impacts on long-term survival, whatever the primary indication. J Hepatol. 2012; 57: 306-312.
161. DiMartini A, Crone C, Dew MA. Alcohol and substance use in liver transplant patients. Clin Liver Dis. 2011; 15: 727-751.
162. Kendrick S, Elsharkawy A, Latimer S, Hudson M, Masson S. An “alcohol contract” has not reduced rates of post-transplant drinking following transplantation for alcoholic liver disease. Gut. 2012; 61: 210-211.
163. Spengler EK, Dunkelberg J, Schey R. Alcoholic hepatitis: current management. Dig Dis Sci. 2014; 59: 2357-2366.
164. Mathurin P, Moreno C, Samuel D, Dumortier J, Salleron J, Durand F, et al. Early liver transplantation for severe alcoholic hepatitis. N Engl J Med. 2011; 365: 1790-1800.
165. Rambaldi A, Saconato HH, Christensen E, Thorlund K, Wetterslev J, Gluud C, et al. Systematic review: glucocorticosteroids for alcoholic

Central
Marroni et al. (2016)Email:
J Liver Clin Res 3(2): 1028 (2016) 21/24
hepatitis--a Cochrane Hepato-Biliary Group systematic review with meta-analyses and trial sequential analyses of randomized clinical trials. Aliment Pharmacol Ther. 2008 ; 27: 1167-1178.
166. Louvet A, Wartel F, Castel H, Dharancy S, Hollebecque A, Canva-Delcambre V, et al. Infection in patients with severe alcoholic hepatitis treated with steroids: early response to therapy is the key factor. Gastroenterology. 2009; 137: 541-548.
167. Louvet A, Naveau S, Abdelnour M, Ramond MJ, Diaz E, Fartoux L, et al. The Lille model: a new tool for therapeutic strategy in patients with severe alcoholic hepatitis treated with steroids. Hepatology. 2007 ;45: 1348-1354.
168. Mathurin P, Louvet A, Duhamel A, Nahon P, Carbonell N, Boursier J, et al. Prednisolone with vs without pentoxifylline and survival of patients with severe alcoholic hepatitis: a randomized clinical trial. JAMA. 2013; 310: 1033-1041.
169. Louvet A, Diaz E, Dharancy S, Coevoet H, Texier F, Thévenot T, et al. Early switch to pentoxifylline in patients with severe alcoholic hepatitis is inefficient in non-responders to corticosteroids. J Hepatol. 2008; 48: 465-470.
170. Akriviadis E, Botla R, Briggs W, Han S, Reynolds T, Shakil O, et al. Pentoxifylline improves short-term survival in severe acute alcoholic hepatitis: a double-blind, placebo-controlled trial. Gastroenterology. 2000; 119: 1637-1648.
171. De BK, Gangopadhyay S, Dutta D, Baksi SD, Pani A, Ghosh P, et al. Pentoxifylline versus prednisolone for severe alcoholic hepatitis: a randomized controlled trial. World J Gastroenterol. 2009; 15:1613-1619.
172. Sidhu SS, Goyal O, Singla P, Gupta D, Sood A, Chhina RS, et al. Corticosteroid plus pentoxifylline is not better than corticosteroid alone for improving survival in severe alcoholic hepatitis (COPE trial). Dig Dis Sci. 2012; 57: 1664-1671.
173. Nguyen-Khac E, Thevenot T, Piquet MA, Benferhat S, Goria O, Chatelain D, et al. Glucocorticoids plus N-acetylcysteine in severe alcoholic hepatitis. N Engl J Med. 2011; 365: 1781-9.
174. Strieter RM, Kunkel SL, Bone RC. Role of tumor necrosis factor-alpha in disease states and inflammation. Crit Care Med. 1993; 21: 447-463.
175. Iimuro Y, Gallucci RM, Luster MI, Kono H, Thurman RG. Antibodies to tumor necrosis factor alfa attenuate hepatic necrosis and inflammation caused by chronic exposure to ethanol in the rat. Hepatology. 1997; 26: 1530-1537.
176. Sharma P, Kumar A, Sharma BC, Sarin SK. Infliximab monotherapy for severe alcoholic hepatitis and predictors of survival: an open label trial. J Hepatol. 2009; 50: 584-591.
177. Tilg H, Jalan R, Kaser A, Davies NA, Offner FA, Hodges SJ, et al. Anti-tumor necrosis factor-alpha monoclonal antibody therapy in severe alcoholic hepatitis. J Hepatol. 2003; 38: 419-425.
178. Spahr L, Rubbia-Brandt L, Frossard JL, Giostra E, Rougemont AL, Pugin J, et al. Combination of steroids with infliximab or placebo in severe alcoholic hepatitis: a randomized controlled pilot study. J Hepatol. 2002; 37: 448-455.
179. Naveau S, Chollet-Martin S, Dharancy S, Mathurin P, Jouet P, Piquet MA, et al. A double-blind randomized controlled trial of infliximab associated with prednisolone in acute alcoholic hepatitis. Hepatology. 2004; 39: 1390-1397.
180. Boetticher NC, Peine CJ, Kwo P, Abrams GA, Patel T, Aqel B, et al. A randomized, double-blinded, placebo-controlled multicenter trial of etanercept in the treatment of alcoholic hepatitis. Gastroenterology. 2008; 135: 1953-1960.
181. Yates WR, Labrecque DR, Pfab D. The reliability of alcoholism history in patients with alcohol-related cirrhosis. Alcohol Alcohol. 1998; 33: 488-494.
182. Varma V, Webb K, Mirza DF. Liver transplantation for alcoholic liver disease. World J Gastroenterol. 2010; 16: 4377-4393.
183. Testino G, Burra P, Bonino F, Piani F, Sumberaz A, Peressutti R, et al. Acute alcoholic hepatitis, end stage alcoholic liver disease and liver transplantation: an Italian position statement. World J Gastroenterol. 2014; 20: 14642-14651.
184. Gaglio PJ Jr, Gaglio PJ Sr. Complications in patients with alcohol-associated liver disease who undergo liver transplantation. Clin Liver Dis. 2012; 16: 865-875.
185. Burra P, Senzolo M, Adam R, Delvart V, Karam V, Germani G, et al. Liver transplantation for alcoholic liver disease in Europe: a study from the ELTR (European Liver Transplant Registry). Am J Transplant. 2010; 10: 138-148.
186. Gramenzi A, Gitto S, Caputo F, Biselli M, Lorenzini S, Bernardi M, et al. Liver transplantation for patients with alcoholic liver disease: an open question. Dig Liver Dis. 2011; 43: 843-849.
187. Neuberger J, Adams D, MacMaster P, Maidment A, Speed M. Assessing priorities for allocation of donor liver grafts: survey of public and clinicians. BMJ. 1998; 317: 172-175.
188. Donckier V, Lucidi V, Gustot T, Moreno C. Ethical considerations regarding early liver transplantation in patients with severe alcoholic hepatitis not responding to medical therapy. J Hepatol. 2014; 60: 866-871.
189. UNOS. United Network for Organ Sharing 2003.
190. Vaillant GE. A 60-year follow-up of alcoholic men. Addiction. 2003; 98: 1043-51.
191. Perut V, Conti F, Scatton O, Soubrane O, Calmus Y, Vidal-Trecan G, et al. Might physicians be restricting access to liver transplantation for patients with alcoholic liver disease? J Hepatol. 2009; 51: 707-714.
192. DiMartini A, Dew MA, Day N, Fitzgerald MG, Jones BL, deVera ME, et al. Trajectories of alcohol consumption following liver transplantation. Am J Transplant. 2010; 10: 2305-2312.
193. Fábrega E, Crespo J, Casafont F, De las Heras G, de la Peña J, Pons-Romero F, et al. Alcoholic recidivism after liver transplantation for alcoholic cirrhosis. J Clin Gastroenterol. 1998; 26: 204-206.
194. De Simone P, De Geest S, Ducci J, Carrai P, Petruccelli S, Baldoni L, et al. Alcohol drinking after liver transplantation is associated with graft injury. Minerva Gastroenterol Dietol. 2011; 57: 345-359.
195. Cuadrado A, Fábrega E, Casafont F, Pons-Romero F. Alcohol recidivism impairs long-term patient survival after orthotopic liver transplantation for alcoholic liver disease. Liver Transpl. 2005; 11: 420-426.
196. Terblanche J, Hickman R. Animal models of fulminant hepatic failure. Dig Dis Sci. 1991; 36: 770-774.
197. McKillop IH, Schrum LW. Role of alcohol in liver carcinogenesis. Semin Liver Dis. 2009; 29: 222-232.
198. Karaa A, Thompson KJ, McKillop IH, Clemens MG, Schrum LW. S-adenosyl-L-methionine attenuates oxidative stress and hepatic stellate cell activation in an ethanol-LPS-induced fibrotic rat model. Shock. 2008; 30:197-205.
199. Thompson KJ, McKillop IH, Schrum LW. Targeting collagen expression in alcoholic liver disease. World J Gastroenterol. 2011; 17: 2473-2481.
200. Tsukamoto H, French SW, Benson N, Delgado G, Rao GA, Larkin EC, et al. Severe and progressive steatosis and focal necrosis in rat liver induced by continuous intragastric infusion of ethanol and low fat diet. Hepatology. 1985; 5: 224-232.
201. Tsukamoto H, Machida K, Dynnyk A, Mkrtchyan H. “Second hit” models of alcoholic liver disease. Semin Liver Dis. 2009; 29: 178-187.

Central
Marroni et al. (2016)Email:
J Liver Clin Res 3(2): 1028 (2016) 22/24
202. de la M Hall P, Lieber CS, DeCarli LM, French SW, Lindros KO, Järveläinen H, et al. Models of alcoholic liver disease in rodents: a critical evaluation. Alcohol Clin Exp Res. 2001; 25: 254S-261S.
203. Nanji AA, French SW. Animal models of alcoholic liver disease--focus on the intragastric feeding model. Alcohol Res Health. 2003; 27: 325-330.
204. Denucci SM, Tong M, Longato L, Lawton M, Setshedi M, Carlson RI, et al. Rat strain differences in susceptibility to alcohol-induced chronic liver injury and hepatic insulin resistance. Gastroenterol Res Pract. 2010; 2010.
205. Tsuchiya M, Ji C, Kosyk O, Shymonyak S, Melnyk S, Kono H, et al. Interstrain differences in liver injury and one-carbon metabolism in alcohol-fed mice. Hepatology. 2012; 56: 130-9.
206. Mathews S, Xu M, Wang H, Bertola A, Gao B. Animals models of gastrointestinal and liver diseases. Animal models of alcohol-induced liver disease: pathophysiology, translational relevance, and challenges. Am J Physiol Gastrointest Liver Physiol. 2014; 306: G819-823.
207. Ki SH, Park O, Zheng M, Morales-Ibanez O, Kolls JK, Bataller R, et al. Interleukin-22 treatment ameliorates alcoholic liver injury in a murine model of chronic-binge ethanol feeding: role of signal transducer and activator of transcription 3. Hepatology. 2010 ;52: 1291-1300.
208. Petrasek J, Bala S, Csak T, Lippai D, Kodys K, Menashy V, et al. IL-1 receptor antagonist ameliorates inflammasome-dependent alcoholic steatohepatitis in mice. J Clin Invest. 2012; 122: 3476-3489.
209. Cohen JI, Roychowdhury S, McMullen MR, Stavitsky AB, Nagy LE. Complement and alcoholic liver disease: role of C1q in the pathogenesis of ethanol-induced liver injury in mice. Gastroenterology. 2010; 139: 664-674.
210. Mandrekar P, Ambade A, Lim A, Szabo G, Catalano D. An essential role for monocyte chemoattractant protein-1 in alcoholic liver injury: regulation of proinflammatory cytokines and hepatic steatosis in mice. Hepatology. 2011; 54: 2185-2197.
211. Nath B, Levin I, Csak T, Petrasek J, Mueller C, Kodys K, et al. Hepatocyte-specific hypoxia-inducible factor-1a is a determinant of lipid accumulation and liver injury in alcohol-induced steatosis in mice. Hepatology. 2011; 53:1526-1537.
212. Zhou Z, Sun X, James Kang Y. Metallothionein protection against alcoholic liver injury through inhibition of oxidative stress. Exp Biol Med. 2002; 227: 214-222.
213. Zhou Z, Wang L, Song Z, Lambert JC, McClain CJ, Kang YJ, et al. A critical involvement of oxidative stress in acute alcohol-induced hepatic TNF-alpha production. Am J Pathol. 2003; 163: 1137-1146.
214. Meadows GG1, Blank SE, Duncan DD. Influence of ethanol consumption on natural killer cell activity in mice. Alcohol Clin Exp Res. 1989; 13: 476-479.
215. Brandon-Warner E, Schrum LW, Schmidt CM, McKillop IH. Rodent models of alcoholic liver disease: of mice and men. Alcohol. 2012; 46: 715-725.
216. Tsukamoto H, Lu SC. Current concepts in the pathogenesis of alcoholic liver injury. FASEB J. 2001; 15: 1335-1349.
217. Tsukamoto H, Horne W, Kamimura S, Niemelä O, Parkkila S, Ylä-Herttuala S, et al. Experimental liver cirrhosis induced by alcohol and iron. J Clin Invest. 1995; 96: 620-630.
218. de David C, Rodrigues G, Bona S, Meurer L, González-Gallego J, Tuñón MJ, et al. Role of quercetin in preventing thioacetamide-induced liver injury in rats. Toxicol Pathol. 2011; 39: 949-57.
219. Bryson-Richardson RJ, Berger S, Schilling TF, Hall TE, Cole NJ, Gibson AJ, et al. FishNet: an online database of zebrafish anatomy. BMC Biol. 2007 Aug 17; 5: 34.
220. Passeri MJ, Cinaroglu A, Gao C, Sadler KC. Hepatic steatosis in response to acute alcohol exposure in zebrafish requires sterol regulatory element binding protein activation. Hepatology. 2009; 49: 443-452.
221. Cremonese RV, Pereira-Filho AA, Magalhães R, de Mattos AA, Marroni CA, Zettler CG, et al. Experimental cirrhosis induced by carbon tetrachloride inhalation: adaptation of the technique and evaluation of lipid peroxidation. Arq Gastroenterol. 2001; 38: 40-47.
222. Rosa DP, Martinez D, Picada JN, Semedo JG, Marroni NP. Hepatic oxidative stress in an animal model of sleep apnoea: effects of different duration of exposure. Comp Hepatol. 2011; 10: 1.
223. Rosa DP1, Bona S, Simonetto D, Zettler C, Marroni CA, Marroni NP. Melatonin protects the liver and erythrocytes against oxidative stress in cirrhotic rats. Arq Gastroenterol. 2010; 47: 72-78.
224. Di Naso FC, de Mello RN, Bona S, Dias AS, Porawski M, Ferraz AeB, et al. Effect of Agaricus blazei Murill on the pulmonary tissue of animals with streptozotocin-induced diabetes. Exp Diabetes Res. 2010; 2010: 543926.
225. Filippin LI, Cuevas MJ, Lima E, Marroni NP, Gonzalez-Gallego J, Xavier RM, et al. The role of nitric oxide during healing of trauma to the skeletal muscle. Inflamm Res. 2011; 60: 347-356.
226. Ogryzko NV, Hoggett EE, Solaymani-Kohal S, Tazzyman S, Chico TJ, Renshaw SA, et al. Zebrafish tissue injury causes upregulation of interleukin-1 and caspase-dependent amplification of the inflammatory response. Dis Model Mech. 2014; 7: 259-264.
227. Vojtech LN, Scharping N, Woodson JC, Hansen JD. Roles of inflammatory caspases during processing of zebrafish interleukin-1β in Francisella noatunensis infection. Infect Immun. 2012; 80: 2878-2885.
228. Tieppo J, Vercelino R, Dias AS, Silva Vaz MF, Silveira TR, Marroni CA, et al. Evaluation of the protective effects of quercetin in the hepatopulmonary syndrome. Food Chem Toxicol. 2007; 45: 1140-1146.
229. Vercelino R, Tieppo J, Dias AS, Marroni CA, Garcia E, Meurer L, et al. N-acetylcysteine effects on genotoxic and oxidative stress parameters in cirrhotic rats with hepatopulmonary syndrome. Basic Clin Pharmacol Toxicol. 2008; 102: 370-376.
230. Lorent K, Yeo SY, Oda T, Chandrasekharappa S, Chitnis A, Matthews RP, et al. Inhibition of Jagged-mediated Notch signaling disrupts zebrafish biliary development and generates multi-organ defects compatible with an Alagille syndrome phenocopy. Development. 2004; 131: 5753-5566.
231. North TE, Babu IR, Vedder LM, Lord AM, Wishnok JS, Tannenbaum SR, et al. PGE2-regulated wnt signaling and N-acetylcysteine are synergistically hepatoprotective in zebrafish acetaminophen injury. Proc Natl Acad Sci U S A. 2010; 107: 17315-17320.
232. Sapp V, Gaffney L, EauClaire SF, Matthews RP. Fructose leads to hepatic steatosis in zebrafish that is reversed by mechanistic target of rapamycin (mTOR) inhibition. Hepatology. 2014; 60: 1581-1592.
233. Schneider AC, Machado AB, de Assis AM, Hermes DM, Schaefer PG, Guizzo R, et al. Effects of Lactobacillus rhamnosus GG on hepatic and serum lipid profiles in zebrafish exposed to ethanol. Zebrafish. 2014;11: 371-378.
234. Howarth DL, Yin C, Yeh K, Sadler KC. Defining hepatic dysfunction parameters in two models of fatty liver disease in zebrafish larvae. Zebrafish. 2013; 10: 199-210.
235. Tilg H, Moschen AR, Kaneider NC. Pathways of liver injury in alcoholic liver disease. J Hepatol. 2011; 55: 1159-1161.

Central
Marroni et al. (2016)Email:
J Liver Clin Res 3(2): 1028 (2016) 23/24
236. Sozio M, Crabb DW. Alcohol and lipid metabolism. Am J Physiol Endocrinol Metab. 2008; 295: 10-16.
237. Gerlai R, Lahav M, Guo S, Rosenthal A. Drinks like a fish: zebra fish (Danio rerio) as a behavior genetic model to study alcohol effects. Pharmacol Biochem Behav. 2000; 67: 773-782.
238. Stickel F, Seitz HK. Alcoholic steatohepatitis. Best Pract Res Clin Gastroenterol. 2010; 24: 683-693.
239. Ni HM, Bhakta A, Wang S2, Li Z, Manley S, Huang H3, et al. Role of hypoxia inducing factor-1β in alcohol-induced autophagy, steatosis and liver injury in mice. PLoS One. 2014; 23; 9: 115849.
240. Nassir F, Ibdah JA. Role of mitochondria in alcoholic liver disease. World J Gastroenterol. 2014; 20: 2136-2142.
241. Teixeira-Clerc F. Effets hpatiques de l’alcool. Mdecine et Nutrition. 2015.
242. Zhang P, Qiang X, Zhang M, Ma D, Zhao Z, Zhou C, et al. Demethyleneberberine, a natural mitochondria-targeted antioxidant, inhibits mitochondrial dysfunction, oxidative stress, and steatosis in alcoholic liver disease mouse model. J Pharmacol Exp Ther. 2015; 352: 139-147.
243. Galicia-Moreno M, Gutiérrez-Reyes. The role of oxidative stress in the development of alcoholic liver disease. Rev Gastroenterol Mex. 2014; 79: 135-144.
244. Yan SL, Yang HT2, Lee HL3, Yin MC4. Protective effects of maslinic acid against alcohol-induced acute liver injury in mice. Food Chem Toxicol. 2014; 74: 149-155.
245. Cao YW, Jiang Y, Zhang DY, Wang M, Chen WS, Su H, et al. Protective effects of Penthorum chinense Pursh against chronic ethanol-induced liver injury in mice. J Ethnopharmacol. 2015; 161: 92-98.
246. García-Ruiz C, Kaplowitz N, Fernandez-Checa JC. Role of Mitochondria in Alcoholic Liver Disease. Curr Pathobiol Rep. 2013; 1: 159-168.
247. Tan TC, Crawford DH, Jaskowski LA, Subramaniam VN, Clouston AD, Crane DI, et al. Excess iron modulates endoplasmic reticulum stress-associated pathways in a mouse model of alcohol and high-fat diet-induced liver injury. Lab Invest. 2013; 93:1295-1312.
248. Chen P, Torralba M, Tan J, Embree M, Zengler K, Stärkel P, et al.
Supplementation of saturated long-chain fatty acids maintains intestinal eubiosis and reduces ethanol-induced liver injury in mice. Gastroenterology. 2015; 148: 203-214.
249. Szabo G. Gut-liver axis in alcoholic liver disease. Gastroenterology. 2015; 148: 30-36.
250. Uesugi T, Froh M, Arteel GE, Bradford BU, Thurman RG. Toll-like receptor 4 is involved in the mechanism of early alcohol-induced liver injury in mice. Hepatology. 2001; 34: 101-108.
251. Tilg H, Gao B. Dietary saturated lipids in alcoholic liver disease: new microbiota-targeting bullets? Gastroenterology. 2015; 148: 16-19.
252. Ceni E, Mello T, Galli A. Pathogenesis of alcoholic liver disease: role of oxidative metabolism. World J Gastroenterol. 2014; 20:17756-17772.
253. Seth D, Duly A, Kuo PC, McCaughan GW, Haber PS. Osteopontin is an important mediator of alcoholic liver disease via hepatic stellate cell activation. World J Gastroenterol. 2014; 20:13088-13104.
254. Puri P, Chandra A. Autophagy modulation as a potential therapeutic target for liver diseases. J Clin Exp Hepatol. 2014; 4: 51-59.
255. Dolganiuc A, Thomes PG, Ding WX, Lemasters JJ, Donohue TM Jr. Autophagy in alcohol-induced liver diseases. Alcohol Clin Exp Res. 2012; 36: 1301-1308.
256. Donohue TM, Thomes PG. Ethanol-induced oxidant stress modulates hepatic autophagy and proteasome activity. Redox Biol. 2014; 3: 29-39.
257. Harada M, Hanada S, Toivola DM, Ghori N, Omary MB. Autophagy activation by rapamycin eliminates mouse Mallory-Denk bodies and blocks their proteasome inhibitor-mediated formation. Hepatology. 2008; 47: 2026-2035.
258. Yin H, Hu M, Liang X, Ajmo JM, Li X, Bataller R, et al. Deletion of SIRT1 from hepatocytes in mice disrupts lipin-1 signaling and aggravates alcoholic fatty liver. Gastroenterology. 2014; 146: 801-811.
259. Helping Patients Who Drink Too Much: A Clinician’s Guide. National Institute on Alcohol Abuse and Alcoholism. 2005.

Central
Marroni et al. (2016)Email:
J Liver Clin Res 3(2): 1028 (2016) 24/24
Marroni CA, Bona S, Fleck Junior AM, Moreira AJ, Mariante-Neto G, et al. (2016) Clinical and Experimental Alcoholic Liver Disease. J Liver Clin Res 3(2): 1028.
Cite this article