Embed Size (px)
Citation preview
Clinica patologie del fegato 20142015 Clinical Activity
Basovizza 19 novembre 2015
Clinical Activity and research
Diagnosis and treatment
Hypobetalipoproteinaemia and steatosis
NAFLD – NASH (metabolic syndrome)
Acute and chronic AFLD
HBV +/- HDV
HCV – direct antiviral treatment
Primary biliary Cirrhosis, Primary Sclerosing Cholangitis
Autoimmune hepatitis
Decompensated Cirrhosis
Hepatocellular carcinoma (HCC)
Cirrhotic patients surveillance
Loco-regional treatment in DH regimen
Outpatient activity
First visit and control (three outpatient units from Monday to Friday)
Day Hospital Activity. More frequent procedures in DH:
Liver biopsies
Blood and derivatives transfusions in liver disease patients
Martial treatment
Paracentesis
Acute hepatic encephalopathy
Diagnostic angiography
Orthotopic Liver Transplant's Staging (OLT)
Focal Liver Lesion treatment (CEAT, thermoablation)
Cysts drainage / Alcoholization
After variceal ligature monitoring
Share wave elastography: a non invasive instrument for Chronic Liver Disease staging, standardized in HCV
Clinical Activity
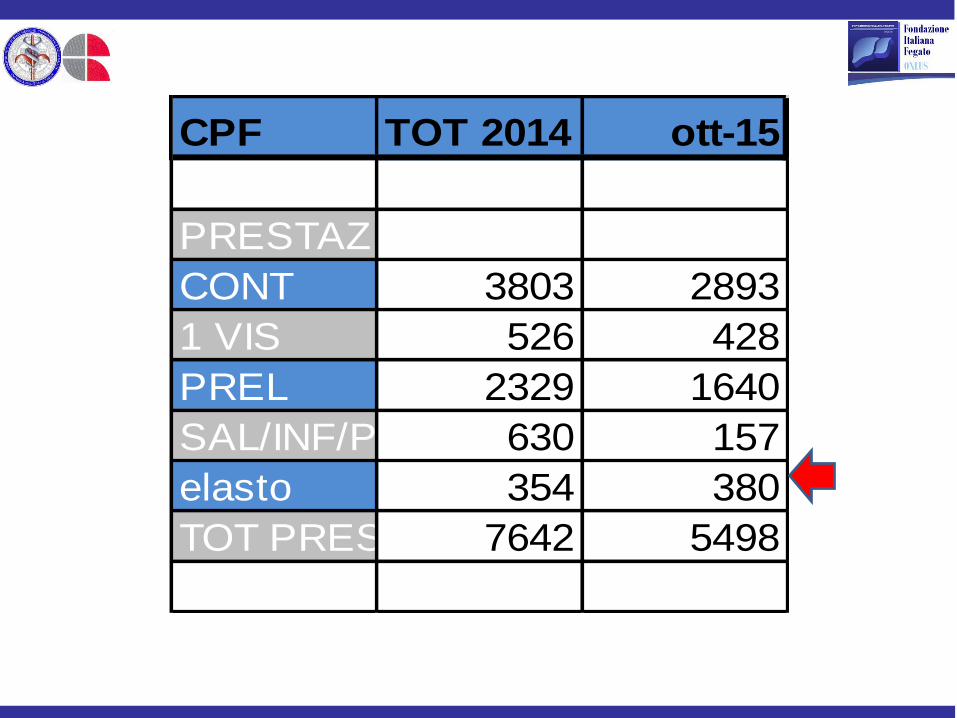
CPF TOT 2014 ott-15
PRESTAZ
CONT 3803 2893
1 VIS 526 428
PREL 2329 1640
SAL/INF/PARAC/INIEZ/MEDIC630 157
elasto 354 380
TOT PREST. 7642 5498
Tutoring CPF 2014
Medical school degree Tutoring
Specialisation in Internal Medicine tutoring
Nursing science degree tutoring
Specialisation in Gastroenterology (2014)
Terminated clinical studies:
BR129
Prophesys
Gideon
Astro (stopped for recruitments problems)
STEP
HCC NASH EASL
Dionysos 1-2
Por Fesr (HCC)
Clinical studies 2010-2014
Ongoing clinical studies:
PBC (Invernizzi)
NECTE (HCC)
FRA 2014 Staminal cell
FRA Bariatric
Silimet (coordination)
Projects
CPF coordination in RER (Regional liver network )
AIFA drug control for DAA
Alcohol
Clinical studies 2015
SILIMET e NAFLD
Background and motivations of the study
The frequency of steatosis in general population is about 35-40 %
Increasing NAFLD prevalence in Italy and occidental world secondary to diabetes and obesity
It seems that NAFLD will become the most frequent liver disease cause in the next decades
Second aetiology for liver transplantation in USA
NAFLD as marker for cardiovascular disease, diabetes or metabolic syndrome. It also can lead to more sever liver disease, steatohepatitis (NASH), cirrhosis and hepatocellular carcinoma (HCC)
At now not sure drugs or nutraceutical are available for NAFLD or NASH treatment, even if there are a lot of molecules in experimentation
Characteristics of the study
Multicentric (60 Italian centers)
Controlled
Randomized by center
The major criteria for entering the study is the presence of steatosic ultrasound pattern in the liver
The aim of the study is to assess efficacy and safety of Legalon E in association with diet regimen and movement in a 6 month treatment in patients with NAFLD
The study is controlled with a group of patients treated with diet regimen and movement only
The primary objective of the study is to assess the responder frequency (measured by HIS reduction of at least 2 points) in sperimental groups
The secondary objective are assessment of the difference between the two groups in term of:
FLI (Fatty Liver Index)
LAP (Lipid Accumulation Product)
AST/ALT
Insulin resistance by HOMA reduction
In SF-12 score questionary reduction
Safety and tolerability
Steatosys improvement
Multicentric, randomized and controlled clinical trial, on efficacy and safety of use of a nutraceutical (Legalon E) associated with dietary and behavioral norms in patients
with nonalcoholic fatty liver disease (NAFLD)
Males and females > 18 anni e < 75 years of age
Alcohol consumption < 30 gr/die
Informed consent module signed
US, done in the last 3 months,with ultrasound pattern of steatosys (NAFLD, in the absence of cirrhosis evidence)
ALT or AST > 40UI/L or AST/ALT < 1 during screening period
Weist circonference >94 cm (males) or 80 cm (females)
Glicemia > 5.6 mmol/L (100 mg/dl)
Triglyceridemia > 1.7 mmol/L (150 mg/dl)
No changes in anti diabetic treatment (if applicable) between screening and treatment
Inclusion criteria
Alcohol consumption > 30 gr/day
Use of silimarine or other preparation containing marian in the 30 days before the screening
Other antiossidant product as vitamin E, vitamin C, glutathione in the 30 days before the screening
use of pentossifillina o gemfibrozil entro i 30 giorni precedenti lo screening
Allergy or o intollerance to silimarine or Marian card extract
BMI ≥40
Pregnancy or Brest feeding
Clinical evidence of actual chronic or active hepatitis
Esclusion criteria
Each centre will use his own randomisation list on which the patient will be randomised in
Group A: diet and exercise
Group B: to these patients, in addition to the requirements for group A, it will be directed even daily intake, for 6 months, of 2 tablets of Legalon E
Every collaborator received login e password for e-crf
Group of 10 consecutive patients that fits inclusion and exclusion criteria will be randomised
When the e-crf will be completed the system will assign the patient to the treatment or diet exercise only
Randomization
SILIMET e NAFLD
CPF: 14 patients enrolled
New direct antiviral drugs for HCV positive chronic
liver disease (DAA)
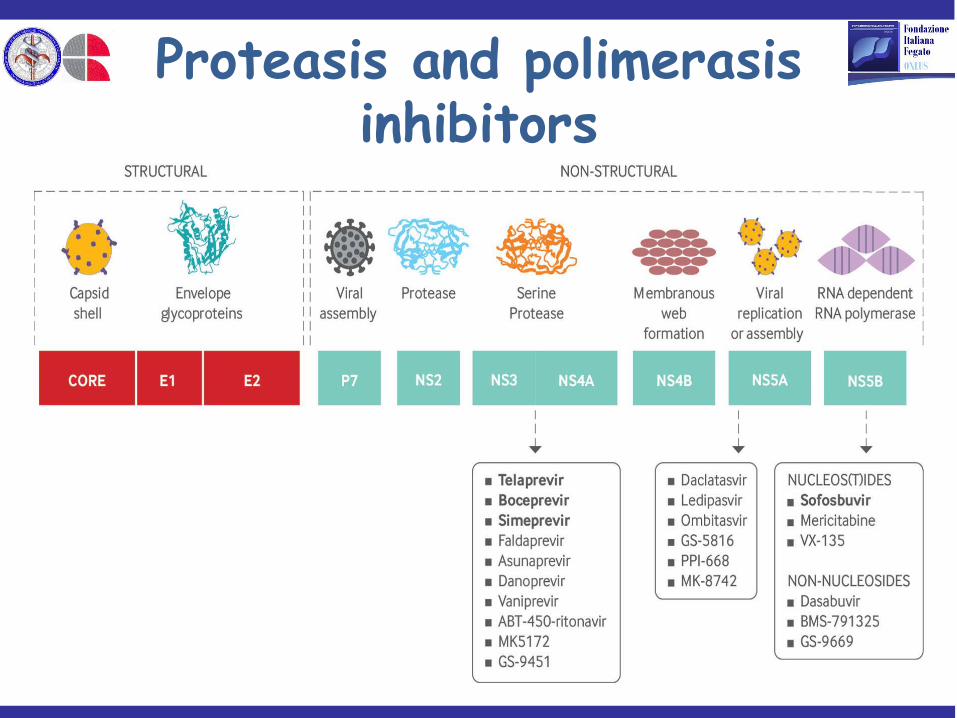
Proteasis and polimerasis inhibitors
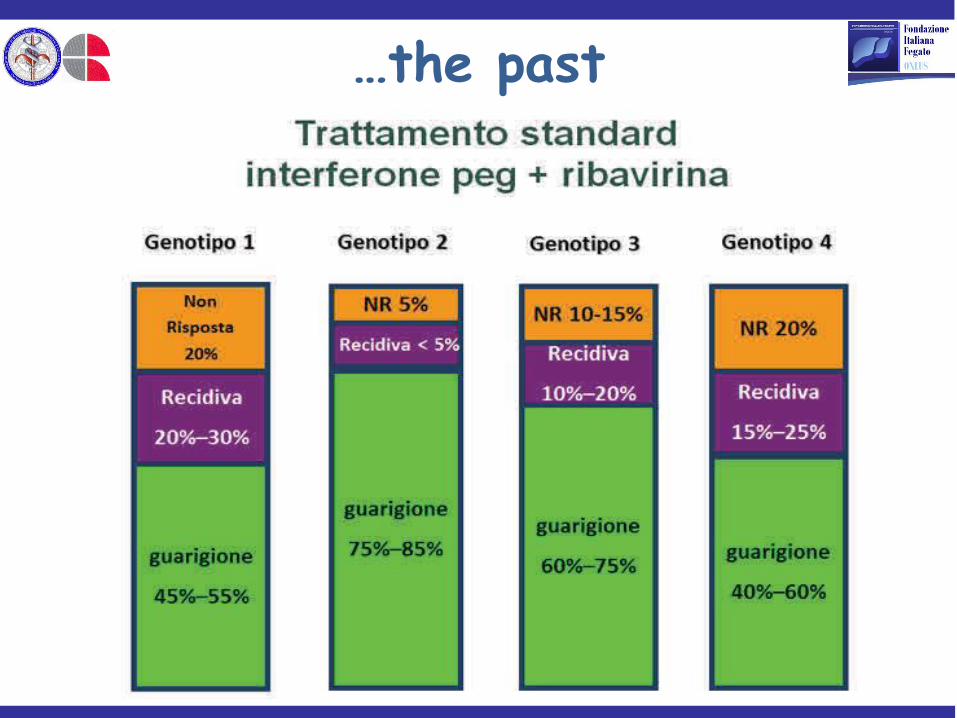
…the past
87-99 % SVR 12
…the present
New direct antiviral drugs for chronic HCV positive (DAA):
efficacy
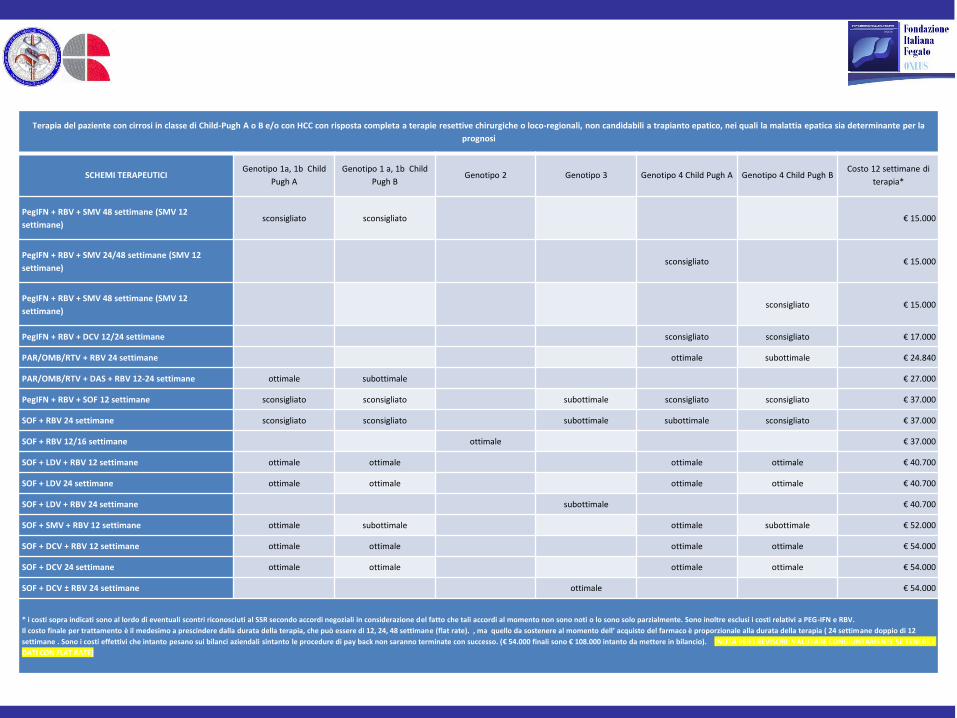
Terapia del paziente con cirrosi in classe di Child-Pugh A o B e/o con HCC con risposta completa a terapie resettive chirurgiche o loco-regionali, non candidabili a trapianto epatico, nei quali la malattia epatica sia determinante per la
prognosi
SCHEMI TERAPEUTICI Genotipo 1a, 1b Child
Pugh A
Genotipo 1 a, 1b Child
Pugh B Genotipo 2 Genotipo 3 Genotipo 4 Child Pugh A Genotipo 4 Child Pugh B
Costo 12 settimane di
terapia*
PegIFN + RBV + SMV 48 settimane (SMV 12
settimane) sconsigliato sconsigliato € 15.000
PegIFN + RBV + SMV 24/48 settimane (SMV 12
settimane) sconsigliato € 15.000
PegIFN + RBV + SMV 48 settimane (SMV 12
settimane) sconsigliato € 15.000
PegIFN + RBV + DCV 12/24 settimane sconsigliato sconsigliato € 17.000
PAR/OMB/RTV + RBV 24 settimane ottimale subottimale € 24.840
PAR/OMB/RTV + DAS + RBV 12-24 settimane ottimale subottimale € 27.000
PegIFN + RBV + SOF 12 settimane sconsigliato sconsigliato subottimale sconsigliato sconsigliato € 37.000
SOF + RBV 24 settimane sconsigliato sconsigliato subottimale subottimale sconsigliato € 37.000
SOF + RBV 12/16 settimane ottimale € 37.000
SOF + LDV + RBV 12 settimane ottimale ottimale ottimale ottimale € 40.700
SOF + LDV 24 settimane ottimale ottimale ottimale ottimale € 40.700
SOF + LDV + RBV 24 settimane subottimale € 40.700
SOF + SMV + RBV 12 settimane ottimale subottimale ottimale subottimale € 52.000
SOF + DCV + RBV 12 settimane ottimale ottimale ottimale ottimale € 54.000
SOF + DCV 24 settimane ottimale ottimale ottimale ottimale € 54.000
SOF + DCV ± RBV 24 settimane ottimale € 54.000
* i costi sopra indicati sono al lordo di eventuali scontri riconosciuti al SSR secondo accordi negoziali in considerazione del fatto che tali accordi al momento non sono noti o lo sono solo parzialmente. Sono inoltre esclusi i costi relativi a PEG-IFN e RBV.
Il costo finale per trattamento è il medesimo a prescindere dalla durata della terapia, che può essere di 12, 24, 48 settimane (flat rate). , ma quello da sostenere al momento dell’ acquisto del farmaco è proporzionale alla durata della terapia ( 24 settimane doppio di 12
settimane . Sono i costi effettivi che intanto pesano sui bilanci aziendali sintanto le procedure di pay back non saranno terminate con successo. (€ 54.000 finali sono € 108.000 intanto da mettere in bilancio). [NOTA PER I REVISORI: VALUTARE CONGIUNTAMENTE SE TENERE I
DATI CON FLAT RATE]
DAA prescribing centre in FVG (Hub)
Udine (Clinica medica, Malattie infettive)
Pordenone (divisione di Medicina)
Trieste (CLINICA PATOLOGIE DEL FEGATO, Malattie infettive)

Clinica patologie del fegato's activity DAA for HCV
50 patients in treatment with DAA
1 February-19 November 2015
Problems
Lack of FVG register for HCV positive patients reporting CLD staging (as in Veneto or other regions)
Restrictive AIFA criteria
Impact of press agency and patients associations
Not clear timing of price reduction for new DAA
Prescribing centre cooperation
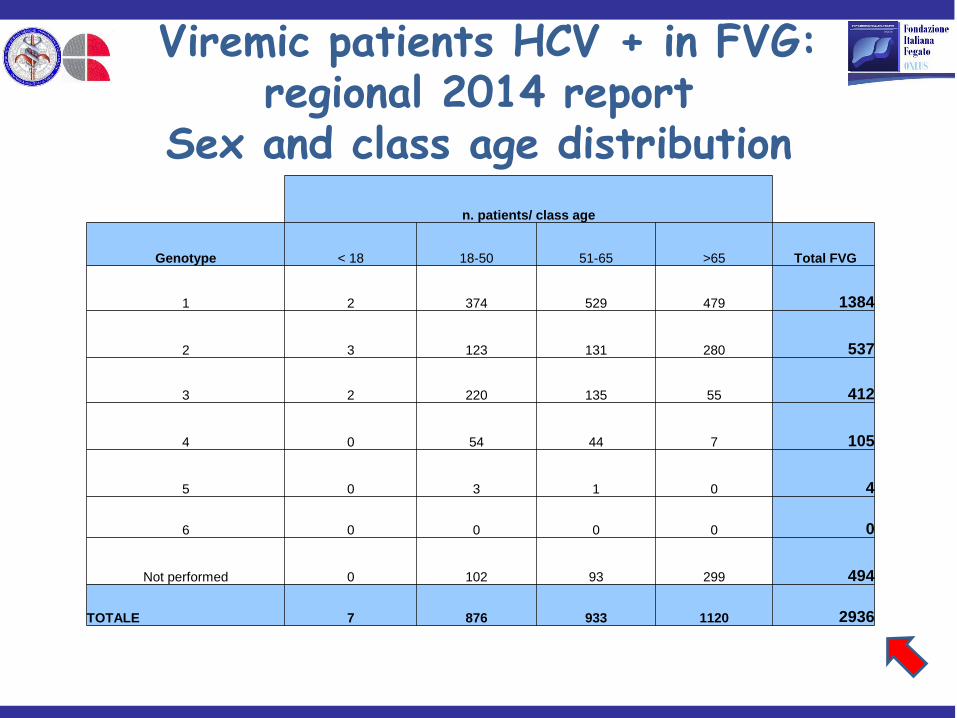
n. patients/ class age
Genotype < 18 18-50 51-65 >65 Total FVG
1 2 374 529 479 1384
2 3 123 131 280 537
3 2 220 135 55 412
4 0 54 44 7 105
5 0 3 1 0 4
6 0 0 0 0 0
Not performed 0 102 93 299 494
TOTALE 7 876 933 1120 2936
Viremic patients HCV + in FVG: regional 2014 report
Sex and class age distribution
New DAA FVG 2015
Monthly report
Coordination of RER
Second opinion

AIFA drug control for DAA
Multiregional project sponsored by AIFA (80.000 euros)
Regions: Fvg and Liguria
Cohordinator: Liguria (HIV-HCV)
Data base of HCV patients treated (2015-2016): clinical and drug control peculiarity
Fellowship
Future perspectives
Developement of a personalizzed treatment strategy
More attention in patient education in particular for metabolic diseases
Prognostic algoritms development for major CLD in particular HCC
Treatment of decompensate liver cirrhosis
Biobank organisation
Database riorganisation (Elastography, HCV, HBV, HCC) for best clinical and research operativity
Clinical staff Cristiana Abazia permanent staff medical doctor Antonella Copez Administrative operator Caterina Cecchi secretary Medical department
Saveria Lory Crocè Responsable
Valentina Lanzilotti Specialist in formation (c/o Med Clin) Daniele Macor Specialist in formation (Gastroent) Flora Masutti permanent staff medical doctor Daniela Mattiazzi Nurse Loredana Sumas Nurse
Milva Pagotto Nurse
Riccardo Patti Specialist in formation (c/o Clin Med )
Patrizia Piriavic Nurse
Claudio Tiribelli Director
Cinzia Ursic OSS
Paola Concas OSS
Cester Giulia Medical doctor

Thank you!





























![PDF] DOF - umfcd.ro-Patologie pulmonara -Leziunile pleurei 4. Patologia aparatului respirator -Patologie mediastinala -Citodiagnostic 5. Patologia tubului digestiv, anexelor si peritoneului](https://img.pdfslide.us/doc/110x75/612d54b71ecc515869421f6b/-dof-umfcdro-patologie-pulmonara-leziunile-pleurei-4-patologia-aparatului.jpg)