-
GLOBAL CHANGE & HUMAN HEALTH, VOLUME 3, NO. 1 (2002) 42
Kluwer Academic Publishers
Malaria continues to signifi cantly affect African health,
society and economy. In sub-Saharan Africa, malaria remains the
most common parasitic disease and is the main cause of morbidity
and mortality among children less than fi ve years of age and among
pregnant women[1]. The 1990 Global Burden of Disease study
estimated that malaria accounted for approximately 10.8% of years
of life lost across all sub-Saharan Africa[2]. A recent review
concluded that roughly 1 million deaths (range 0.74 to 1.3 million)
from the direct
effects of malaria occur annually in Africa, more than 75% of
them in children[3]. This estimate may double when the indirect
effects of malaria, including malaria-related anemia, hypoglycemia,
respiratory distress and low birth weight, are included when defi
ning the burden of malaria[4].
There has been a global resurgence of malaria over the past two
decades; reasons suggested include failure of malaria control
programs, population redistribution and growth, changes in land
use, increasing prevalence
Climate suitability for stable malaria transmission in Zimbabwe
under different climate change scenarios
As climate is one factor determining the potential range of
malaria, climate change may work with or against
efforts to bring malaria under control. We developed a model of
future climate suitability for stable Plasmodium
falciparum malaria transmission in Zimbabwe. Current climate
suitability for stable malaria transmission is
based on the MARA/ARMA model of climatic constraints on the
survival and development of the Anopheles
vector and the Plasmodium falciparum malaria parasite. We
explored potential future geographic distributions
of malaria using sixteen projections of climate in 2100. The
results suggest that, assuming no future human-
imposed constraints on malaria transmission, changes in
temperature and precipitation could alter the geographic
distribution of malaria in Zimbabwe, with previously unsuitable
areas of dense human population becoming
suitable for transmission. Among all scenarios, the highlands
become more suitable for transmission, while the
lowveld and areas currently limited by precipitation show
varying degrees of change, depending on climate sensi-
tivity and greenhouse gas emission stabilization scenarios, and
depending on the general circulation model used.
The methods employed can be used within or across other African
countries.
Jessica Hartman(A Corresponding author), Kristie Ebi(B), K. John
McConnell(C), Nathan Chan(D) and John Weyant(E)
A Stanford University 205 E. 78th Apt. 19A, NY, NY 10021 tel
(917) 855-9537 e-mail [email protected]
B EPRI, 3412 Hillview Ave, Palo Alto, CA 94304
tel (650) 855-2735, e-mail [email protected]
C University of California at San Francisco, Institute for
Health Policy Studies, San Francisco, CA 94118
tel (415) 502-4076, e-mail [email protected]
D Stanford University, 685 Mariposa Ave #6, Mountain View, CA
94041
tel (650) 903-0951, e-mail [email protected]
E Stanford University, Stanford, CA 94305-4023
tel (650) 723-3506, e-mail [email protected]
-
feature
GLOBAL CHANGE & HUMAN HEALTH, VOLUME 3, NO. 1 (2002)43
Kluwer Academic Publishers
research article
of drug and pesticide resistance, denigration of public health
infrastructure and climate variability and change[5,6]. Climate
change may work against efforts to bring malaria under control,
with a recent model suggesting that increasing temperatures could
create environmental conditions that would allow a net increase in
the geographic range of areas climatically hospitable for malaria
vectors[7]. With some degree of anthropogenic alteration of the
climate system highly probable over the next 100 years - recent
estimates suggest a global mean surface temperature increase of 1.4
to 5.8C - understanding the range of possible impacts of these
climatic changes on efforts to control malaria is imperative,
particularly on national and sub-national scales[8,9].
While climate is an important driver of malaria, it is not the
only one. The many determinants of malaria rarely act in isolation;
these determinants form a web of interconnected infl uences, often
with positive feedbacks between malaria transmission and other
drivers[10-12]. Determinants of malaria can be divided into
climatic and non-climatic drivers. The non-climatic socioeconomic
and biological drivers that have a direct impact on malaria include
drug and pesticide resistance, deterioration of health care,
deterioration of the public health infrastructure (including
disease and vector control efforts), demographic change, and
changes in land use
patterns. We focused solely on climate in this model; future
models will include qualitative or quantitative representations of
non-climatic drivers of malaria and their interactions.
Climate and anomalous weather events have a direct infl uence on
malaria transmission by either hindering or enhancing vector and
parasite development and survival. Numerous laboratory and fi eld
studies have analyzed the infl uence of precipitation and
temperature, and can be summarized as follows: Climate suitability
is a primary determinant of
whether the conditions in a particular location are suitable for
stable malaria transmission[13,14].
A change in temperatures may lengthen or shorten the season in
which mosquitoes or parasites can survive.
Changes in precipitation or temperature may result in conditions
during the season of transmission that are conducive to increased
or decreased parasite and vector populations.
Changes in precipitation or temperature may cause previously
inhospitable altitudes or ecosystems to become conducive to
transmission. Higher altitudes that were formerly too cold or
desert fringes that were previously too dry for mosquito
populations to develop may be rendered hospitable by small changes
in temperature or precipitation.
Despite more than 50 years of vector control, malaria is still a
substantial public health threat[37]. More than 4 million of
Zimbabwes 12 million inhabitants live in malarious areas. Even with
widespread under-reporting and self-treatment, 9,696 deaths and 6.4
million cases of malaria were reported between 1989-96[37]. Three
parasites have been identifi ed as causing malaria in Zimbabwe,
with Plasmodium falciparum responsible for about 98% of all
cases[22]. Of the 38 species of Anopheline mosquitoes in Zimbabwe,
Anopheles arabiensis is the only formidable vector of malaria. A.
funestus s.s. (endophilic), A. merus (breeds in salt water), and A.
quadriannulatus (zoophilic) are also present, yet are not believed
to be substantial threats either due to past control efforts or
their ecological constraints[38].
Transmission is highly seasonal with the bulk of cases recorded
between February and May, and with peak transmission typically
occurring in March[22]. Stable transmission is partially defi ned
by
temperature and precipitation, with altitude a proxy indicator
of temperature. Some areas of Zimbabwe, particularly the northern
and southern lowveld regions, have year round malaria transmission
with peaks in the austral summer months. Like much of southern
Africa, this transmission season corresponds to the onset of summer
and the single rainy season. Also similar to many southern and
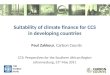
eastern African countries, Zimbabwe has dramatic elevation ranges
(Figure 1). The marked gradient of elevation correlates with
maximum and minimum temperatures. Figures 2 and 3 show annual mean
temperature and total precipitation. This heterogeneity coupled
with interannual climatic variability results in constantly
shifting fringe areas that are prone to malaria outbreaks, similar
to many countries in southern and eastern Africa[38]. High altitude
regions, which also are the areas of densest human population, are
currently malaria free due to climatic constraints and to a long
policy of barrier spraying in the transitional elevation
zone[39].
Box The epidemiology of malaria in Zimbabwe
-
GLOBAL CHANGE & HUMAN HEALTH, VOLUME 3, NO. 1 (2002) 44
Kluwer Academic Publishers
Death, disease and deformityClimate change and malaria in
Zimbabwe
Our study investigates the impact of various climate change
scenarios on the projected spatial distribution of climatic
suitability for stable Plasmodium falciparum malaria transmission.
We chose to initially populate our model with data from Zimbabwe
because of its heterogeneity of climatic suitability for malaria
transmission (see Box for a discussion of the epidemiology of
malaria in Zimbabwe). Specifi cally, there are areas in Zimbabwe
where the climate is suitable for endemic malaria transmission,
areas where transmission is absent, and areas representing
gradations of transmission in between. The benefi t of using a
country with multiple levels of climatic suitability is that, for
each scenario of climate change, we can observe the range of
projected fl uctuations in the levels of suitability and we can
identify key areas that appear the most vulnerable.
MethodsWe utilized the COSMIC program[15] to generate
Zimbabwe-specifi c scenarios of climate change, which we then used
as inputs for a model of climate suitability for stable Plasmodium
falciparum malaria transmission to generate maps of future
transmission potential. Our model was based on the MARA/ARMA
decision rules[13,14] and developed using the ArcView 3.2
Geographic Information System[16].
Climate suitability for stable malaria transmission
The MARA/ARMA climatic suitability model for malaria
transmission was one tool we used to create projections of future
climate suitability in Zimbabwe. This biological model defi nes a
set of decision rules based on minimum and mean temperature
constraints on the development of the Plasmodium falciparum
parasite and the Anopheles vector, and on precipitation constraints
on the survival and breeding capacity of the mosquito. MARA/ARMA
determined the decision rules by reviewing laboratory and fi eld
studies throughout Africa and by evaluating current malaria
distribution maps[13,14]. This biological model approximates the
current boundaries of malaria distribution across the continent
quite well.
MARA/ARMA uses three variables to determine climatic suitability
for a particular geographic location: mean monthly temperature, the
monthly mean of daily minimum temperatures, and total cumulative
monthly precipitation. An important distinction between this model
and others is that the MARA/ARMA decision rules were developed
using fuzzy logic to resolve the uncertainty in defi ning distinct
boundaries to divide malarious from non-malarious regions. Rather
than using a Boolean designation of climatically suitable or
not, an area can be assigned a fuzzy logic suitability value
ranging from zero (not suitable) to one (suitable). A value of one
means that malaria transmission is most likely stable, and zero
means that transmission is very unstable, with malaria either
absent or with rare epidemics. Values between zero and one (0.1 to
0.9) represent a gradient from unstable to increasingly stable
transmission. For all variables, assignment of fuzzy logic values
between zero and one were based on a sigmoid curve, as shown in
Figure 4. Utilizing fuzzy logic over Boolean sets allows for a more
fl uid spatial and temporal defi nition of the geographic extent of
malaria transmission. The MARA/ARMA set of decision rules does not
project transmission intensity.
Temperature is a major factor determining the distribution and
incidence of malaria. Temperature affects both the Plasmodium
parasite and the Anopheles mosquito, with thresholds at both
temperature extremes limiting the survival or development of the
two organisms[13,14]. Anopheles must live long enough to bite an
infected person, allow the parasite to develop and then bite a
susceptible human. MARA/ARMA determined the lower mean monthly
temperature threshold of 18C from parasite development time and
mosquito survivorship. The lower limit resulted from the fact that
below 18C few mosquitoes live long enough for the parasite to
complete development. At 22C, parasite development time is suffi
ciently short and mosquito development suffi ciently high for
stable Plasmodium falciparum malaria transmission. Mean temperature
conditions are suitable until 31C, when the survivorship rate
peaks. At this point, less than 40% of the mosquitoes survive long
enough for the parasite to complete its development cycle. As
temperatures rise above 32C, the mosquitos probability of survival
decreases. However, higher temperatures enable the mosquitoes to
digest blood meals more rapidly, which in turn increases the rate
at which they bite. This increased biting rate coupled with faster
development of the parasite leads to increased infective mosquito
bites for those mosquitoes that do survive[13,14]. 40C is the upper
temperature threshold for both mosquitoes and larvae to
survive.
Based on these biological constraints on the vector and
parasite, the MARA/ARMA decision rules for assigning fuzzy logic
values to mean temperature were as follows: The fuzzy logic value
increased from zero to 18C
to one at 22C; 22C to 32C was considered 100% suitable for
stable transmission and a fuzzy logic value of one was assigned;
and
-
Death, disease and deformity
GLOBAL CHANGE & HUMAN HEALTH, VOLUME 3, NO. 1 (2002)45
Kluwer Academic Publishers
Climate change and malaria in Zimbabwe
Fuzzy logic values decreased from one at 32C to zero at 40C.
The second climate variable was the monthly average of the daily
minimum temperatures during the winter season. Ground frost (or
ambient temperatures of 4 - 5C) kills mosquito populations and
prevents the persistence of a stable year round mosquito
population[13,14]. In the MARA/ARMA decision rules, if the monthly
average of the daily minimum temperatures reached low enough for
frost to form during a given month, then it was assumed that vector
populations could not become established. The lowest monthly
average of daily minimum temperature conducive for frost was set at
4C (fuzzy value of zero), with the upper limit designated 6C (fuzzy
value of one).
Total monthly precipitation was the third climate variable used
in the MARA/ARMA decision rules. Mosquitoes require water for their
eggs to develop into larvae and ultimately emerge as winged adults.
Given the ill-defi ned relationship between precipitation and
mosquito survivorship and abundance, the MARA/ARMA team examined
current precipitation and temperature requirements in areas where
the epidemiology of malaria was well understood[13,14]. Based on
these examinations, they established 80mm of precipitation per
month as suitable for stable transmission in southern Africa. Where
there was no precipitation, a fuzzy value of zero was assigned.
Fuzzy values from zero to one were assigned across the continuum of
precipitation levels from 0mm to 80mm.
The MARA/ARMA decision rules further stipulate that both
temperature and precipitation have to be favorable at the same time
of the year to allow transmission, and suitable conditions have to
continue long enough for the transmission cycle to be completed. A
fi ve-month period was considered a suffi cient length of time for
conditions to be suitable for stable transmission. Consistent with
the MARA/ARMA decision rules, for each month and geographic
location, we assigned a fuzzy logic value for each of the three
climate variables. We determined the lowest precipitation or mean
temperature fuzzy value for each month and location. Then we
established the minimum fuzzy value of a moving 5-month period. For
example, the lowest fuzzy logic value for mean temperature or
precipitation for the months January through May was determined,
then the 5-month minimum fuzzy value for February through June was
determined, et cetera. Finally, we compared the minimum 5-month
fuzzy value of precipitation and temperature with the fuzzy value
corresponding to the lowest monthly average of daily minimum
temperature in the winter period and assigned the lowest fuzzy
value
(i.e. the most constraining variable) to the geographic
location. This approach of choosing the lowest fuzzy value of all
variables produced a conservative climatic suitability value.
Baseline climatology
Our baseline climate scenario was a mean monthly climatology in
a 0.05 latitude by 0.05 longitude raster format, compiled from data
spanning 1920-1980 for all of Africa[17]. We extracted monthly
total precipitation, monthly mean temperature and the mean range
between minimum and maximum daily temperatures in all months for
Zimbabwe.
As an average climate representing over sixty years of data,
this baseline climatology is not necessarily representative of any
given year or even the most recent decade. This is important to
note as Zimbabwe experiences signifi cant interannual and decadal
variability. In particular, total annual precipitation in Zimbabwe
is characterized by strong variability, with global
oceanic-atmospheric processes, such as the El Nio Southern
Oscillation (ENSO), the dominant cause of precipitation variability
(low rainfall is associated with El Nio years)[18,19].
Zimbabwe experienced a warming and drying trend over the past
100 years that overshadows the strong decadal and interannual
variability. The instrumental surface air temperature suggests an
increase of up to 0.8C in some parts of Zimbabwe, with the winter
months (June to November) showing a slightly larger warming than
the summer months (December to May)[20,21]. This warming trend was
accompanied by a 10% reduction in rainy season precipitation.
The baseline climatology of Zimbabwe is infl uenced by this
variability, as well as by the topography of Zimbabwe and its
geographic placement within the African continent. Zimbabwe lies at
the southern distribution limit of malaria in Africa[22]. A central
watershed lying above 1200 meters that runs from northeast to
southwest divides Zimbabwe. Rivers arising from this watershed
drain into the Zambezi system in the north and the Sabi-Limpopo
systems in the south. Low-lying areas where malaria transmission
normally occurs fl ank the central plateau. The central plateau
rises to peaks as high as 2592 meters along the border with
Mozambique. The middle and lowveld regions descend from the central
plateau to an elevation of 162 meters at the lowest point in the
country (Figure 1). Annual mean temperatures correspond to the
elevation gradient and range from 12C to greater than 25C (Figure
2).
The climate of Zimbabwe can be broadly divided into three
seasons: the cool dry season (April to
-
GLOBAL CHANGE & HUMAN HEALTH, VOLUME 3, NO. 1 (2002) 46
Kluwer Academic Publishers
Death, disease and deformityClimate change and malaria in
Zimbabwe
August); the hot dry season (August to October); and the hot wet
season (November to March). Typically, precipitation ranges from
less than 400 mm during the average rainy season in the southern
lowveld region to upwards of 800 mm in the highveld regions near
the capitol, Harare, and in the eastern highlands (Figure 3).
Climate projections
Future climate projections were created in COSMIC, the output of
which was the change in mean temperature (C) and monthly
precipitation from 1990 to 2100, on a countrywide basis. These
changes in mean temperature and precipitation were added to the
baseline climatology (which has 14,000 grid cells) to present
different scenarios of climate in the year 2100.
Analyses of the regional impact of projected global climate
change in southern Africa suggest an increase in temperature of 0.7
- 4.7C by the 2050s (dependent on emissions scenario, climate
sensitivity and general circulation model (GCM) used), relative to
the average 1961-1990 climate[20,21]. The magnitude and direction
of projected changes in precipitation is less consistent, with some
GCMs suggesting an increase and others a decrease. This variability
is primarily due to the current inability of GCMs to represent
interannual and decadal variability, and dynamic land
cover-atmospheric interactions; both of these have and will most
likely continue to infl uence precipitation in southern Africa.
Additionally, GCMs respond differently to greenhouse gas forcing,
resulting in a range of possible outcomes[20,21].
To represent this range of possible future climates, we chose
four of the fourteen GCM-based climate projections generated from
the COSMIC program[15,23,24] to create Zimbabwe specifi c
projections of monthly precipitation and mean temperature starting
in 1990 and carried out to 2100. COSMIC uses an
energy-balance-climate/upwelling-diffusion-ocean model to calculate
the annual changes in global mean temperature under different
radiative forcing scenarios. COSMIC then scales the projected
geographic and seasonal climate patterns produced by the fourteen
GCMs to individual countries using an intertemporal scaling
procedure. The four GCMs chosen were: the Canadian Centre for
Climate Research (CCC)[25], United Kingdom Meteorological Offi ce
(UKMO)[26], Goddard Institute for Space Studies (GISS)[27], and the
Henderson-Sellers model using the CCM1 at NCAR (HEND)[28]. We used
climate sensitivities of 4.5C (high) and 1.4C (low), where climate
sensitivity is the estimated increase in the global mean surface
air temperature after a doubling of atmospheric CO2 concentrations
relative to the atmospheric concentrations before the industrial
revolution. Finally, we chose the equivalent carbon dioxide (ECD)
analogues to the 350 ppmv and 750 ppmv greenhouse gas emission
stabilization scenarios of the IPCC Second Assessment Report (ECD
concentration is the amount of CO2 that gives the same radiative
forcing as the radiative forcing by all greenhouse gases combined,
i.e. CO2, N2O, CH4 and CFCs). Figure 5
elevation (meters)
150 - 300300 - 450450 - 600600 - 750750 - 900900 - 10501050 -
12001200 - 13501350 - 15001500 - 16501650 - 18001800 - 20002000 -
2300
HarareHarare
KwekweKwekwe MutareMutare
HarareKadomaKadoma
Kwekwe
GweruGweruGweru
Mutare
BulawayoBulawayoBulawayo
Figure 1 Elevation (Zimbabwe)
annual mean temperature (degrees c)
12 - 1414 - 1616 - 1818 - 2020 - 2222 - 2424 - 2626 - 28
HarareHarare
KwekweKwekwe MutareMutare
HarareKadomaKadoma
Kwekwe
GweruGweruGweru
Mutare
BulawayoBulawayoBulawayo
Figure 2 Annual mean temperature 1920-1980 (Zimbabwe)
October - April precipitation (mm)
250 - 350 350 - 450450 - 550550 - 650650 - 750750 - 850850 -
950950 - 10501050 - 11501150 - 12501250 - 13501350 - 14501450 -
15501550 - 1700
HarareHarare
KwekweKwekwe MutareMutare
HarareKadomaKadoma
Kwekwe
GweruGweruGweru
Mutare
BulawayoBulawayoBulawayo
Figure 3 Cumulative rainy season precipitation (October
April)
1920-1980 (Zimbabwe)
-
Death, disease and deformity
GLOBAL CHANGE & HUMAN HEALTH, VOLUME 3, NO. 1 (2002)47
Kluwer Academic Publishers
Climate change and malaria in Zimbabwe
fuzz
y va
lue
0
0.2
0.4
0.6
0.8
1
1.2
17.5
19.5
21.5
23.5
25.5
27.5
29.5
31.5
33.5
35.5
37.5
39.5
mean temperature (C)
fuzzy logic value for mean temperature
fuzz
y va
lue
0
0.2
0.4
0.6
0.8
1
1.2
0 3 6 9 12
15 18
21
24
27
30
33 36
39
42
45
48
51
54
57
60
63
66
69
72
75
78
81
84
precipitation (mm)
fuzzy logic value for precipitation
fuzz
y va
lue
0
0.2
0.4
0.6
0.8
1
1.2
3.5
3.7
3.9
4.1
4.3
4.5
4.7
4.9
5.1
5.3
5.5
5.7
5.9
6.1
6.3
6.5
minimum temperature (C)
fuzzy logic value for minimum temperature
Figure 4 Assignment of fuzzy logic values to climate
variables
conc
entr
atio
n (p
pmv)
0
1950 2000 2050 2100 2150 2200 2250
200
400
600
800
1000
1200
CO2/350
ECD/350
CO2/750
ECD/750
year
Figure 5 Equivalent Carbon Dioxide (ECD) and CO2 Emissions
under the IPCC 350 ppmv and 750 ppmv stabilization scenarios
shows the greenhouse gas emission trajectories for the ECD
equivalent and the IPCC 350 ppmv and 750 ppmv stabilization
scenarios in which CO2 is the sole greenhouse gas. Due to the many
uncertainties related to modeling the radiative forcing of aerosols
on the climate system, we excluded them from the climate change
scenarios, focusing solely on the infl uence of a suite of
greenhouse gases[9].
Creating maps of future malaria climate suitability for
stable
malaria transmission in Zimbabwe
COSMIC projected the change in monthly mean temperature and
monthly total precipitation for each month from the 1990 baseline
year to 2100. These changes on a national level were added to the
baseline 0.05-latitude by 0.05-longitude gridded climatology of
Zimbabwe. The MARA/ARMA decision rules were then applied to the
future climate scenarios and were used to determine a fuzzy logic
climate suitability value for each grid cell in Zimbabwe.
In order to incorporate the climate projection from the GCMs
into the climatic suitability model, we made three assumptions. The
fi rst was that the range between minimum and maximum temperatures
would not decrease over the next 100 years. While the global trend
has suggested a decrease in the diurnal temperature range, with
nighttime minimum temperatures rising at double the rate of daytime
maximum temperatures, the trend in Zimbabwe has been an increase in
the diurnal range due to increases during the rainy season[20,21].
Because of this uncertainty, we chose to keep the range between
minimum and maximum temperatures during the baseline period
(1920-1980) constant for the climate projections. A second
assumption was that permanent water bodies do not negate the
MARA/ARMA precipitation requirements for a given geographic
location. Finally, we assumed that climate did not change between
the baseline and our starting year of 1990.
ResultsFigure 6 shows the baseline fuzzy logic climate
suitability for stable Plasmodium falciparum transmission in
Zimbabwe. Areas where malaria is endemic in the average year are
denoted with a dark red coloring (fuzzy value of >0.9). White
designates locations where climatic conditions inhibit malaria
transmission (fuzzy value of zero). For fuzzy logic values between
0.9 and zero, malaria transmission likely varies between years,
with epidemics or strongly seasonal malaria present. The highland
areas are clearly identifi ed by their low fuzzy logic values. Due
to the inaccessibility and inconsistent
-
GLOBAL CHANGE & HUMAN HEALTH, VOLUME 3, NO. 1 (2002) 48
Kluwer Academic Publishers
Death, disease and deformityClimate change and malaria in
Zimbabwe
nature of historical malaria data for Zimbabwe, we did not
validate this map against reported malaria cases.
Figure 7 shows the change in temperature from the baseline
climatology to the year 2100 for the climate change scenarios
evaluated. The scenarios represented a range of possible future
temperatures, from marginal increases in temperature to an increase
of 4 to 5C in the HEND 750 ppmv stabilization scenario with a
climate sensitivity of 4.5C.
Figure 8 shows the change in precipitation from baseline
climatology to the year 2100 for the climate change scenarios
evaluated. Note that projected changes in precipitation differ both
in magnitude and direction of change. While all scenarios projected
an increase in temperature, the GISS and UKMO scenarios projected a
net increase in precipitation while the HEND and CCC scenarios
suggested a net decrease. The HEND 750 ppmv stabilization scenario
with a climate sensitivity of 4.5C projected the most dramatic
variation in precipitation, with an increase of over 30 mm in the
spring months (November to January) and a decrease of over 60 mm in
the summer (February to April).
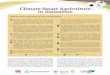
The results of our model are shown in Figure 9 and Table 1. In
the baseline climate suitability scenario, 40% of Zimbabwe was
suitable for stable transmission (fuzzy value >0.9). The
magnitude and direction of change varied for the four GCMs,
following the direction and amplitude of projected precipitation
change. Under the scenario with the smallest change, with a climate
sensitivity of 1.4C and a stabilization of greenhouse gases at 350
ppmv, the projected net change was small
chan
ge in
deg
rees
cel
cius
0sep oct nov dec jan feb mar apr may jun jul aug sep oct nov
dec
CCC_350_1.4
CCC_350_4.5
CCC_750_1.4
CCC_750_4.5
GISS_350_1.4
GISS_350_4.5
GISS_750_1.4
GISS_750_4.5
HEND_350_1.4
HEND_350_4.5
HEND_750_1.4
HEND_750_4.5
UKMO_350_1.4
UKMO_350_4.5
UKMO_750_1.4
UKMO_750_4.5
1
2
3
4
5
6
month
CCC_350_1.4
CCC_350_4.5
CCC_750_1.4
CCC_750_4.5
GISS_350_1.4
GISS_350_4.5
GISS_750_1.4
GISS_750_4.5
HEND_350_1.4
HEND_350_4.5
HEND_750_1.4
HEND_750_4.5
UKMO_350_1.4
UKMO_350_4.5
UKMO_750_1.4
UKMO_750_4.5
chan
ge in
deg
rees
cel
cius
-60
-50
-20
-30
-40
0
10
-10
20
30
40
sep oct nov dec jan feb mar apr may jun jul aug sep oct nov
dec
month
Figure 7 Change in temperature to the year 2100 from baseline
climate (1920-1980) under various climate change scenarios in
Zimbabwe
Figure 8 Change in precipitation to the year 2100 from baseline
climate (1920-1980) under various climate change scenarios in
Zimbabwe
Figure 6 Baseline fuzzy logic climate suitability for stable
malaria
transmission in Zimbabwe
fuzzy climatic suitability (range 0-1)*
* 0 = not suitable (transmission is very unstable)
1 = suitable (transmission is most likely stable)
0>0 - 0.10.1 - 0.20.2 - 0.30.3 - 0.40.4 - 0.50.5 - 0.60.6 -
0.70.7 - 0.80.8 - 0.90.9 - 11
HarareHarare
KwekweKwekweMutareMutare
HarareKadomaKadoma
KwekweGweruGweruGweru
Mutare
BulawayoBulawayoBulawayo
-
Death, disease and deformity
GLOBAL CHANGE & HUMAN HEALTH, VOLUME 3, NO. 1 (2002)49
Kluwer Academic Publishers
Climate change and malaria in Zimbabwe
Table 1 Percentage of Zimbabwe with climate suitability for
stable malaria transmission in 2100
general circulation model
scenario CCC UKMO GISS HEND
ppmv/C
Baseline 40%
350/1.4 * 39% 45% 45% 41%
350/4.5 * * 37% 68% 66% 34%
750/1.4 * * * 34% 77% 76% 25%
750/4.5 * * * * 10% 96% 86% 3%
fuzzy logic value of 0.9
* emissions stabilization scenario of 350 ppmv and a climate
sensitivity of 1.4C CCC general circulation model of the Canadian
Centre for Climate Research
* * emissions stabilization scenario of 350 ppmv and a climate
sensitivity of 4.5C UKMO general circulation model of the United
Kingdom Meteorological Offi ce
* * * emissions stabilization scenario of 750 ppmv and a climate
sensitivity of 1.4C GISS general circulation model of the Goddard
Institute for Space Studies
* * * * emissions stabilization scenario of 750 ppmv and a
climate sensitivity of 4.5C HEND the Henderson-Sellers general
circulation model using the CCM1 at NCAR
350/1.4 *
CCCscenarioppmv/C UKMO
general circulation model
GISS HEND
350/4.5 * *
750/1.4 * * *
750/4.5 * * * *
0>0 - 0.10.1 - 0.20.2 - 0.30.3 - 0.40.4 - 0.50.5 - 0.60.6 -
0.70.7 - 0.80.8 - 0.90.9 - 11
fuzz
y cl
imat
ic s
uita
bilit
y (r
ange
0-1
)*
* emissions stabilization scenario of 350 ppmv and a climate
sensitivity of 1.4C* * emissions stabilization scenario of 350 ppmv
and a climate sensitivity of 4.5C* * * emissions stabilization
scenario of 750 ppmv and a climate sensitivity of 1.4C* * * *
emissions stabilization scenario of 750 ppmv and a climate
sensitivity of 4.5C
CCC general circulation model of the Canadian Centre for Climate
ResearchUKMO general circulation model of the United Kingdom
Meteorological OfficeGISS general circulation model of the Goddard
Institute for Space StudiesHEND the Henderson-Sellers general
circulation model using the CCM1 at NCAR
* 0
= n
ot s
uita
ble
(tra
nsm
issi
on is
ver
y un
stab
le)
1 =
sui
tabl
e (t
rans
mis
sion
is m
ost
likel
y st
able
)
Figure 9 Climate suitability for stable malaria transmission in
2100 under various climate change scenarios in Zimbabwe
-
GLOBAL CHANGE & HUMAN HEALTH, VOLUME 3, NO. 1 (2002) 50
Kluwer Academic Publishers
Death, disease and deformityClimate change and malaria in
Zimbabwe
-1 -0.9-0.9 -0.8-0.8 -0.7-0.7 -0.6-0.6 -0.5-0.5 -0.4-0.4
-0.3-0.3 -0.2 -0.2 -0.1-0.1 00 0 0.10.1 0.20.2 0.30.3 0.40.4 0.50.5
0.6 0.6 0.70.7 0.80.8 0.90.9 11
Cha
nge
in fu
zzy
clim
ate
suita
bilit
y fr
om b
asel
ine
peri
od
350/1.4 *
CCCscenarioppmv/C UKMO
general circulation model
GISS HEND
350/4.5 * *
750/1.4 * * *
750/4.5 * * * *
* emissions stabilization scenario of 350 ppmv and a climate
sensitivity of 1.4C* * emissions stabilization scenario of 350 ppmv
and a climate sensitivity of 4.5C* * * emissions stabilization
scenario of 750 ppmv and a climate sensitivity of 1.4C* * * *
emissions stabilization scenario of 750 ppmv and a climate
sensitivity of 4.5C
CCC general circulation model of the Canadian Centre for Climate
ResearchUKMO general circulation model of the United Kingdom
Meteorological OfficeGISS general circulation model of the Goddard
Institute for Space StudiesHEND the Henderson-Sellers general
circulation model using the CCM1 at NCAR
with a maximum increase of 5% in the area of stable malaria
transmission in the UKMO and GISS models, and a decrease of 1% in
the CCC GCM. Under the scenario with the highest change, where the
climate sensitivity was set at 4.5C and the stabilization scenario
was equivalent to 750 ppmv, the projected net change varied from
the HEND model projecting that only 3% of Zimbabwe may be suitable
for malaria transmission to the UKMO model suggesting that 96% of
Zimbabwe may have climate suitable for stable transmission.
As seen in Figure 10, even with little net change in climate
suitability, as in the CCC 350_1.4C scenario, there is the
potential for a redistribution of areas that are suitable, with the
central plateau becoming more suitable for transmission (green) and
the lowveld areas becoming slightly less suitable (bright blue).
The central plateau, where the human population is currently
concentrated, potentially becomes more suitable for malaria
transmission in all but the HEND 750_4.5C
scenario. The anomalous change for this scenario can be
accounted for by the dramatic decrease in precipitation,
particularly in the crucial month of March, rendering all but the
highest elevations in Zimbabwe unsuitable for malaria
transmission.
DiscussionAlthough climate is a major factor determining the
potential range of malaria, there is a scarcity of detailed
multivariate maps and models describing its distribution[29].
Determining the baseline distribution of malaria is the fi rst step
in understanding how the future distribution might be altered with
changing climate; this is one of the achievements of the MARA/ARMA
project. The maps created using the MARA/ARMA model approximate the
edge of malaria distribution across the African continent quite
well[13]. Our model is a fi rst step in developing a range of
possible scenarios of the potential future geographic distribution
of malaria in
Figure 10 Change in climate suitability for stable malaria
transmission from baseline climate (1920-1980) to 2100 in
Zimbabwe
-
Death, disease and deformity
GLOBAL CHANGE & HUMAN HEALTH, VOLUME 3, NO. 1 (2002)51
Kluwer Academic Publishers
Climate change and malaria in Zimbabwe
and deaths for severe malaria; this trend is expected to
continue over at least the short-term[31].
Demographic changes, such as increased human mobility,
population growth and redistribution, affect malaria risk[6].
Population redistribution is a result of urbanization, labor
migration and confl ict, and allows the transport of both vector
and parasite, often exposing immunologically nave populations to
malaria[32]. Dramatic climatic changes could create environmental
refugees as populations are forced to migrate from areas where
resources are few to urban areas or regions where they may have a
means of support[8]. Environmental refugees present an enormous
opportunity for parasite and vector migration.
Pressures placed on environmental resources, which are often
linked to population pressures, can also alter the landscape of
malaria transmission. Altered vegetation coverage, surface water fl
ows and water storage methods as a result of agricultural intensifi
cation or population needs may alter the quantity and quality of
breeding habitats for mosquitoes and the species composition of the
community[33]. In addition, climate change is likely to alter land
use patterns (agricultural use, urban areas, de- or afforestation)
and so could potentially infl uence the mosquito population
composition and size, resulting in changes in malaria
transmission[8].
The objective of the Roll Back Malaria (RBM) partnership is to
halve the malaria burden in participating countries by the year
2010 through interventions that are adapted to local needs and by
reinforcement of the health sector[34]. Intensifi ed national
action will take place within a framework of country-level
partnerships supported by a global partnership, with technical
support networks available for assistance. Success of these and
other intervention programs, including the development of an
effective and inexpensive malaria vaccine, would reduce the burden
of malaria both today and in the future.
Other factors that could infl uence malaria mortality in Africa
include civil unrest, deterioration of public health systems and
HIV proliferation[7].
National expenditures on such public goods as vector control,
health care delivery and infrastructure, disease surveillance,
public education and basic malaria research might dominate the
future determinants of malaria risk and are typically limited by a
countrys GDP. Just as a countrys GDP infl uences malaria risk,
malaria has been shown to decrease economic growth in severely
malarious countries by 1.3% per year[35]. The result is that a
disease such as malaria creates something of a vicious cycle for
poorer countries. Malaria is likely to persist without the creation
and maintenance of an appropriate public health infrastructure;
however, the economic
Zimbabwe. The methods employed can be used within or across
other African countries.
The climate scenarios chosen produce a range of possible climate
suitability futures where stable malaria transmission might either
increase or decrease depending on the climate sensitivity, the
greenhouse gas emission stabilization scenario and the general
circulation model used. Despite the wide range in the resulting
percent of the area that may become suitable, the predominant
pattern across the scenarios suggests that climate suitability for
malaria transmission in Zimbabwe is more likely to increase than
decrease in the central plateau, where the population is currently
concentrated. Evaluation of the results by decade (not shown)
suggests that most of Zimbabwe could have near complete climate
suitability for stable malaria transmission by 2050 under the
scenario showing the greatest change (UKMO_750_4.5C). Within this
scenario, precipitation and temperature increase linearly and there
is no interannual or decadal variability.
An important question for decision makers is how quickly climate
suitability might change, because abrupt climate change might
require different mitigation and adaptation options than a gradual
change in climate[9]. The uncertainty in the rate and geographic
range of change emphasizes the importance of establishing the
capacity to monitor changing temperature and precipitation patterns
to determine when and where climate suitability for malaria
transmission might change; and to establish surveillance programs
to determine changes in malaria incidence or intensity along the
edges of its established range.
It is important to emphasize that the potential geographic
distribution modeled in this study does not directly translate into
actual cases of malaria. Areas of the United States and Europe have
climates suitable for malaria transmission, yet only a limited
number of cases occur (and those are generally imported) because of
the strength of the public health infrastructure and other
factors[30]. In addition to climatic variables, a number of other
factors will infl uence whether or not the future geographic
distribution of malaria is different from today, including parasite
drug resistance, demographic change, changes in land use patterns
and the success of intervention programs such as Roll Back
Malaria.
A factor of concern over the short term is increasing parasite
drug resistance. Although the current malaria control and
prevention measures used in Africa include personal protection,
drug use and vector control strategies, most control is based
almost exclusively on chemotherapy[4]. Increasing drug resistance
has resulted in a two- to three-fold increase in malaria
admissions
-
GLOBAL CHANGE & HUMAN HEALTH, VOLUME 3, NO. 1 (2002) 52
Kluwer Academic Publishers
Death, disease and deformity
development necessary for these improvements is directly
hindered by the presence of malaria itself. Changes in climate have
the potential to make it even more diffi cult for poor countries to
reduce the burden of malaria. A key research goal is to identify
which of these many factors are most likely to drive the future
distribution of malaria and to include modules for these factors
into models such as ours.
A number of other research groups have modeled the potential for
spread of malaria as a consequence of global climate change; these
models include both climate suitability and data on populations at
risk.
Martens and colleagues developed a partial integrated
mathematical model[7]. In this model, climate change scenarios were
linked with a module that uses the formula for the basic
reproduction rate to calculate the transmission or epidemic
potential for a population of mosquitoes that can transmit malaria.
The basic reproductive rate is the number of new cases of a disease
that will arise from one case introduced into a non-immune host
population during a single transmission cycle. Included within the
basic reproductive rate are a number of variables that are
sensitive to temperature, including mosquito density, feeding
frequency, survival and extrinsic incubation period (the
development of the parasite in the mosquito). Incorporating
knowledge about the current distributions and characteristics of
the main mosquito species of malaria resulted in global projections
of 300 million additional people at risk of falciparum malaria in
2080 under the HadCM2 scenario and of an additional 260 to 320
million at risk under the HadCM3 scenario. Most of the changes in
potential transmission were projected to occur in temperate zones
in areas where vectors are present, but it is currently too cold
for transmission.
In contrast to this biological approach, Rogers and Randolph
developed a statistical model of the present-day global
distribution of malaria that they used to establish the current
multivariate climatic constraints[36]. The recorded global limits
of malaria were digitized and turned into a raster grid with a
longitude and latitude resolution of 0.5. The statistical model was
based on the mean, maximum and minimum of temperature,
precipitation and saturation vapor pressure. The covariance between
variables also was important for setting distributional limits.
This multivariate model agreed relatively well with the actual
present-day global distribution. The model was then applied to the
HadCM2 scenarios for future climate. The high scenario projected
mean global land surface changes of +3.45, +3.63 and +3.29C in
mean, minimum and maximum temperatures by the year 2050. The
statistical model predicted no
signifi cant net change in the future global population living
in malarious zones. Small differences between the current and the
projected malaria distributions occurred at the edges of the
current range.
Although using very different methods, both modeling efforts
reached similar conclusions; that is, that the future spread of
malaria is likely to occur at the edges of its geographical
distribution where current climate constrains transmission. These
results are consistent with our fi ndings in Zimbabwe.
Our results also are consistent with a model for Zimbabwe
developed by Lindsay and Martens that included three scenarios: an
increase of 2C; an increase of 2C with a 20% increase in
precipitation; and an increase of 2C with a 20% decrease in
precipitation[12]. The results showed that the effect of a
temperature increase would be greatest on malaria transmission
potential at higher altitudes. In the relatively drier lower
altitudes, a temperature increase of 2C combined with a 20%
decrease in precipitation resulted in areas becoming too dry for
malaria transmission, while a 20% increase in precipitation
increased transmission potential. We found a similar variation with
changes in temperature and precipitation across the climate
scenarios used.
Both Martens et al. and Rogers and Randolph used climate
scenarios based on simulations from the Hadley Centre (HadCM2 for
both and HadCM3 for Martens et al. 1999)[7,36]. The UKMO scenario
used in our model is an older version of these scenarios. Because
of large number of differences among the simulations, it is not
possible to directly compare our results with those from Rogers and
Randolph, and Martens et al.
Our results illustrate the importance of using several climate
scenarios to illustrate the range of possible future geographical
distributions of malaria. The net change in area suitable for
malaria transmission varies dramatically depending on which
scenario is used, with a 37% decrease in suitability using the
HEND_750_4.5C scenario in contrast to a 56% increase with the
UKMO_750_4.5C scenario. Our model also utilized a high-resolution
climate baseline capable of showing the climatic heterogeneity that
exists in Zimbabwe. This allowed us to examine the fl uctuations in
suitability under different scenarios and enables decision makers
to identify localized areas vulnerable to climate change. Given
spatial information on areas where climate suitability for malaria
transmission may change, decision makers can take these possible
changes into account when prioritizing actions to enhance the
capacity of future generations to effectively handle malaria
risk.Climate change and malaria in Zimbabwe
Key words climate change, malaria, methodology, scenarios,
Africa
-
Death, disease and deformity
GLOBAL CHANGE & HUMAN HEALTH, VOLUME 3, NO. 1 (2002)53
Kluwer Academic Publishers
Climate change and malaria in Zimbabwe
AcknowledgementThis works was supported by the Electric Power
Research Institute (EPRI) under contract numbers WO009242 and
WO043518, and by the California Energy Commission under contract
500-97-043. This paper does not neces-sarily represent the views
and policies of the California Energy Commission or the State of
California. The authors gratefully acknowledge Drs. Williams and
Schlesinger for the support they provided on COSMIC. The authors
also would like to acknowledge Dr. David LeSueur, whose untimely
death prevented him from completing his review. Davids practical
expertise in malaria, gentle good humor and wonderful stories will
be sorely missed.
References[1] Anonymous. Blair Research Institute 1996 Annual
Report: Epidemiology of Plasmo-
dium falciparum drug resistance in Zimbabwe. Harare, Zimbabwe:
Blair Research Institute, 1995.
[2] Murray, C and A Lopez. The Global Burden of Disease. Boston:
Harvard Univer-sity Press, 1996.
[3] Snow, RW, M Craig, U Deichmann and K Marsh. Estimating
mortality, morbid-ity, and disability due to malaria among Africas
non-pregnant population. Bul-letin of the World Health Organization
1999; 77(8): 624-40.
[4] Breman, J. The ears of the hippopotamus: manifestations,
determinants and esti-mates of the malaria burden. American Journal
of Tropical Medicine and Hygiene 2001; 64(suppl 1): 76-84.
[5] Githeko, AK and W Ndegwa. Predicting malaria epidemics in
the Kenyan high-lands using climate data: a tool for decision
makers. Global Change and Human Health 2001; 2(1): 54-63.
[6] Greenwood, B and T Mutabingwa. Malaria in 2002. Nature 2002;
415:670-2.[7] Martens, P, et al. Climate change and future
populations at risk of malaria.
Global Environmental Change 1999; 9: S89-S107.[8] IPCC. Climate
Change 2001: Impacts, adaptation, and vulnerability. Contribution
of
Working Group II to the Third Assessment Report. eds. McCarthy
J, Canziani OF, Leary N, Dockken D, White KS. Cambridge: Cambridge
University Press, 2001.
[9] IPCC. Climate Change 2001: The scientifi c basis.
Contribution of Working Group I to the Third Assessment Report.
eds. Houghton JT et al. Cambridge: Cambridge University Press,
2001.
[10] Janssen, M and P Martens. Modeling malaria as a complex
adaptive system. Artifi cial Life 1997; 3:213-36.
[11] Chan, NY, KL Ebi, F Smith, TF Wilson and AE Smith. An
Integrated Assess-ment Framework for Climate Change and Infectious
Diseases. Environmental Health Perspectives 1999; 107(5):
329-37.
[12] Lindsay, SW and WJM Martens. Malaria in the African
highlands: past, present and future. WHO Bulletin OMS 1998;
76:33-45.
[13] Craig, MH, RW Snow and Dl Sueur. A climate-based
distribution model of malaria transmission in sub-Saharan Africa.
Parasitology Today 1999; 15(3): 105-11.
[14] MARA/ARMA. Towards an atlas of malaria risk in Africa.
Durban: MARA, 1998.[15] Schlesinger, ME and LJ Williams. COSMIC -
Country specifi c model for intertem-
poral climate. Palo Alto: EPRI, 1997.[16] ESRI. ArcView 3.2.
Redlands, CA: ESRI, 2001.[17] Hutchinson, M, H Nix, J McMahon and K
Ord. Africa: a topographic and climatic
database. Canberra: Centre for Resource and Environmental
Studies Australian National University, 1995.
[18] Lindesay, JA. South African rainfall, the Southern
Oscillation and a Southern Hemisphere semi-annual cycle. Journal of
Climatology 1988; 8:17-30.
[19] Ropelewski, CF and MS Halpert. Global and regional scale
precipitation pat-terns associated with the El Nio-Southern
Oscillation. Monthly Weather Review 1987; 115:1606-26.
[20] Hulme, M, R Doherty, T Ngara, M New and D Lister. African
Climate Change: 1900-2100. Climate Research 2001; 17:145-68.
[21] Unganai, LS. Historic and future climatic change in
Zimbabwe. Climate Research 1996; 6:137-45.
[22] Taylor, P and SL Mutambu. A review of the malaria situation
in Zimbabwe with special reference to the period 1972-1981.
Transactions of the Royal Society of Tropical Medicine and Hygiene
1986; 80:12-9.
[23] Williams, L, D Shaw and R Mendelsohn. Evaluating GCM output
with impact models. Climatic Change 1998; 39:111-33.
[24] Mendelsohn, R, M Schlesinger and L Williams. Comparing
impacts across cli-mate models. Integrated Assessment 2000;
1:37-48.
[25] McFarlane, NA, GJ Boer, J-P Blanchet and M Lazare. The
Canadian Climate Centre Second-Generation General Circulation Model
and its equilibrium cli-mate. Journal of Climate 1992;
5:1013-77.
[26] Wilson, CA and JFB Mitchell. A doubled CO2 climate
sensitivity experiment with a global climate model including a
simple ocean. Journal of Geophysical Research 1987; 92(D11):
13315-43.
[27] Hansen, J, et al. Global climate changes as forecast by
Goddard Institute for Space Studies Three-Dimensional Model.
Journal of Geophysical Research 1988; 93(D8): 9341-64.
[28] Henderson-Sellers, A, et al. Tropical deforestation:
modeling local - to regional-scale climate change. Journal of
Geophysical Research 1993; 98(D4): 7289-315.
[29] Watson, ER, M Zinyowera, R Moss and D Dokken. The Regional
Impacts of Cli-mate Change: An Assessment of Vulnerability. A
special report of IPCC Working Group II. Cambridge: Cambridge
University Press, 1998.
[30] Reiter, P. Climate change and mosquito-borne disease.
Environmental Health Perspectives 2001; 109:141-61.
[31] Trape, J. The public health impact of chloroquine
resistance in Africa. American Journal of Tropical Medicine and
Hygiene 2001; 64(suppl 1): 12-7.
[32] Trape, J, et al. Malaria in and urbanization in Central
Africa: the example of Brazzaville. Part B: Pernicious attacks and
mortality. Transactions of the Royal Society of Tropical Medicine
and Hygiene 1987; 81(suppl 2): 34-42.
[33] Lindblade, K, E Walker, A Onapa, J Katungu and M Wilson.
Land use change alters malaria transmission parameters by modifying
temperature in a highland area of Uganda. Tropical Medicine and
International Health 2000; 5:263-74.
[34] Remme, J, F Binka and D Nabarro. Toward a framework and
indicators for monitoring Roll Back Malaria. American Journal of
Tropical Medicine and Hygiene 2001; 64(suppl 1): 1-11.
[35] Gallup, J and J Sachs. The economic burden of malaria.
American Journal of Tropical Medicine and Hygiene 2001; 64(suppl
1): 85-96.
[36] Rogers, DJ and SE Randolph. The global spread of malaria in
a future, warmer world. Science 2000; 289:1763-9.
[37] Makono, R and S Sibanda. Review of the prevalence of
malaria in Zimbabwe with specifi c reference to parasite drug
resistance (1984-96). Transactions of the Royal Society of Tropical
Medicine and Hygiene 1999; 93(5): 449-52.
[38] Freeman, T. Malaria: Zimbabwe 1995. A review of the
epidemiology of malaria trans-mission and distribution in Zimbabwe
and the relationship of malaria outbreaks to preceding
meteorological conditions. Harare, Zimbabwe: GTZ, 1995.
[39] Freeman, T and M Bradley. Temperature is predictive of
severe malaria years in Zimbabwe. Transactions of the Royal Society
of Tropical Medicine and Hygiene 1996; 90:232.
-
GLOBAL CHANGE & HUMAN HEALTH, VOLUME 3, NO. 1 (2002) 54
Kluwer Academic Publishers
Death, disease and deformityClimate change and malaria in
Zimbabwe
The authorsJessica Hartman has been involved with several
research projects investigating the rela-tionships between
vector-born disease and anthropogenic cli-mate change or natural
climate variability. Jessica is at the
New York Academy of Medicine working with the NYC Department of
Health to develop new methods for early warning and detection of
infectious diseases outbreaks for bioterrorism surveillance and
West Nile Virus. Her research focuses on creating early warn-ing
systems that integrate disease, climate, weather, and environmental
data on multiple spatial-temporal scales for the early detection of
vulnerable populations and disease outbreaks.
Nathan Chan has worked on a number of research areas involving
climate change science and impacts. While a consultant at Decision
Focus, Inc., he performed integrated assessments for EPRI and the
U.S. Environmental Protection
Agency, and analytical modeling of heat stress and vector
disease impacts of climate change. His research interests include
health effects, land-use changes, and economic impacts of global
change.
John P. Weyant is Professor of Management Science and
Engineering and director of the Energy Modeling Forum (EMF) at
Stanford University. Prof. Weyant earned a B.S./M.S. in
Aeronautical Engi-neering and Astronautics, M.S.
degrees in Engineering Management and in Opera-tions Research
and Statistics all from Rensselaer Poly-technic Institute, and a
Ph.D. in Management Sci-ence with minors in Economics, Operations
Research, and Organization Theory from University of Cali-fornia at
Berkeley. His current research focuses on analysis of global
climate change policy options, and models for strategic
planning.
Kristie L. Ebi is an epidemiol-ogist who heads the Global
Cli-mate Change and Health Pro-gram at EPRI and is a Scien-tist in
the Global Change and Health Program at the WHO European Centre for
Environ-ment and Health. Kris was a
Lead Author for the Health Sector of the United States National
Assessment of the Potential Health Consequences of Climate
Variability and Health, and a Contributing Author to the Health
Chapter of the Third Assessment Report of the Intergovernmental
Panel on Climate Change. One focus of her research is integrated
assessment modeling.
K. John McConnell is an economist at the Institute for Health
Policy Studies at the University of California at San Francisco.
John has worked on the analysis of predictive information for
public health, from an evaluation of an early
warning system for dengue fever to an assessment of US national
guidelines for screening for cervical neoplasia.