Embed Size (px)
Citation preview

Climate Change Vulnerability
Assessment in Ghana (2006 -2008)
Edith Clarke
Occupational & Environmental Health Unit
Ghana Health Service
Ministry of Health, Ghana
San Jose, Costa Rica (20-23 July 2010)

Ghana• Land Area: 240,000km2
• Bordered in south by 560km long coastline & north by Latitude 11.15o
• Population:22 million
• Workforce: >50% in agricul-ture contributing 30% GDP
• High Illiteracy rate: 40%
• Life Expectancy: 60.5yrs

Vulnerability Assessment & Health
Adaptation : Mechanisms
I. Integrated Assessment of Sectoral Vulnerabilities & Adaptation : 2006 – 2008
II. Adaptation Project : Development of Proposal : To be co-sponsored by GEF Facility
III. Consideration of Climate Change within the SANA process of the Libreville Declaration

Integrated Assessment
• 2006- 2008 : Integrated assessment of sectoral
Vulnerabilities & Adaptation led by the EPA /MEST
• Purpose: Was to provide inputs towards the
formulation of an Integrated National Climate
Change Adaptation Policy Framework.
• Health Vulnerability & Adaptation assessment was
conducted as part of integrated national
assessment

Health Assessment within Integrated
Assessment Objective:
• Examine the association between climate change and human health vulnerability.
• Identify impact of climate change on 5 endemic tropical diseases: malaria, diarrhoeal diseases, guinea worm, measles and cerebrospinal meningitis
• Investigate consequences of climate change on the livelihood systems of poor communities.
2009 Draft WHO Guidelines for V&A assessment for the assessment not yet available

The Process
• Process led by Environmental Protection Agency :
focal point for Climate Change
• Study conducted by researchers from the
University of science & Technology
• Stakeholder involvement : at inception and
dissemination of results
: though involved MOH, excluded managers of
environmental health programme and disease
programme areas under consideration

Methodology i. Observation of time series data of;
• Monthly incidence of outpatient morbidity from 2 regions :Ashanti and Upper West Regions : 1999 -2004
• Climate variables (mean, maximum & minimum air temperature, rainfall and relative humidity data for period 1961 - 1990 for of Ghana.
ii. studied above against their seasonal changes & modelling scenarios for 2020, 2050 and 2080
iii. Estimation of the socio-economic burden :direct & indirect cost of treating malaria.

Major Findings:
Results:
• Analysis predicts general increases in temperature
and decreases in rainfall
• Predicts: upsurge of diarrhoeal diseases, meningitis
and guinea worm and
:decreases in incidence of malaria
• Total Disease Cost/Direct & Indirect to patient &
carers : Approximately $5 million Dollars per annum
(2003)

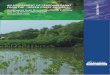
Results. Fig. 1 Climate scenario for baseline and the years 2020, 2050 and 2080
26.5
27.1
28.5
29.6
27.9 27.9
27.6
27
25.8
24.924.8
25.3
26
26.6
26.1
28.628.6
28.2
27.2
26.3
25.4 25.3
25.8
26.5
27.2
26.7
30.130 29.9
29.2
27.7
26.6 26.6
26.9
27.6
28.6
28.1
30.1
30.5
29.4
28.528.2
28.4
31.4
32.132.132.1
30.6
24
25
26
27
28
29
30
31
32
33
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Period (Months)
Mean air temperature
Mean air temperature baseline
Mean air temperature 2020
Mean air temperature2050
Mean air temperature2080
M

Distribution of number of malaria cases and mean air temperature : Inverse relation (1999 –
2004).
Dec-01
40463
Jan-00
17941
Sep-04
71416
Aug-02
80323
May-01
60280Jun-00
55983
Jun-99
48013
Feb-03
39886
Jul-04
38343
Oct-03
68043
Aug-04
24.8Aug-03
24.5
Aug-02
24.22Aug-01
24.5
Jul-00
24.6
Sep-99
25.1
Mar-04
27.9
Mar-03
29.3
Feb-02
29.6
Feb-01
28.8
Mar-00
29.3
Mar-99
28.1
10000
20000
30000
40000
50000
60000
70000
80000
90000
Jan-
99
Apr-
99
Jul-
99
Oct-
99
Jan-
00
Apr-
00
Jul-
00
Oct-
00
Jan-
01
Apr-
01
Jul-
01
Oct-
01
Jan-
02
Apr-
02
Jul-
02
Oct-
02
Jan-
03
Apr-
03
Jul-
03
Oct-
03
Jan-
04
Apr-
04
Jul-
04
Oct-
04
Time (1999 - 2004)
Number of malaria cases
24
25
26
27
28
29
30
Mean air temperature
Number of malaria cases Mean air temperature
Generally high mean air temperature values corresponds to periods of
low number of malaria cases and vice versa.

Baseline values of Rainfall and Average Number of Outpatient Malaria Cases.
17.1
54.8
114.9
135.0
169.4
121.9
153.8
67.080.9
31.9
142.0
215.2
20000
25000
30000
35000
40000
45000
50000
55000
60000
65000
January
February
March
April
May
June
July
August
Septem
ber
October
Novem
ber
Decem
ber
Period (1999 - 2004)
Number of outpatient malaria cases (Averaged)
0.0
50.0
100.0
150.0
200.0
250.0
Baseline rainfall amount(mm)
Average number of malaria cases
Rainfall baseline
The maximum number of malaria cases occurs in June and the mean air
temperature is 25.8°C. Low number of malaria cases occur in February,
March and Aril where mean air temperature ranges from 27.6°C in April,
27.9°C in both February and March respectively.

Meningitis and Climate Change
Distribution of meningitis cases and mean air temperature.
Mar-00
18
Mar-99
28.1
Feb-01
28.8
Feb-02
29.6Mar-03
29.3
Feb-04
27.9
0
10
20
30
40
50
60
70
80
Jan-99Apr-99Jul-99
Oct-99Jan-00Apr-00Jul-00
Oct-00Jan-01Apr-01Jul-01
Oct-01Jan-02Apr-02Jul-02
Oct-02Jan-03Apr-03Jul-03
Oct-03Jan-04Apr-04Jul-04
Oct-04
Period (1999 - 2004)
Number of meningitis cases
24
25
26
27
28
29
30
Mean air temperature
Number of meningitis cases
Mean air temperature
High meningitis cases corresponds to periods of high
mean air temperature and vice versa.

Process of the GEF Adaptation Project
• Process initiated by EPA / UNDP
• An Adaptation project (for 3 diseases) NOT Vulnerability Assessment Project
• Did not take cognizance of gaps in Health assessment within the Integrated assessment
• Health sector’s /WHO input received only after agreement to project , Hence limiting extent of inclusion of comprehensive sector Vulnerability Assessment & Health System Strengthening approach it proposed.
• Final proposal submitted

GEF Adaptation Project• Objective
Identify, implement & evaluate adaptations to
reduce current & likely future burdens of Malaria,
Diarrhoeal diseases & meningococcal meningits
Project Components
i. Strengthening technical capacities to manage
climate change related health risks
ii. Mainstreaming CC into decision making
iii.Strengthen CC health risk knowledge

SANA: 19 Country Task Team MembersLed by 2 Focal Persons : Hlth & Env
• MOH:1
• GHS : 3 – PPME, Environmental Health, Disease Control
• Min of Env: 1
• EPA : 3
• Ministry of Local Government :Env Health Dept
• Min of Agriculture
• Min of Finance
• National Development Planning Commission
• Academia
• Community Water & Sanitation
• Standards Board
• WHO
• (UNDP)

Analysis by Country Task Team of SANA
Driving Forces for Health
Effects of Climate Change
Potential Impacts on Health
Drought
Flooding
Heat Waves
Dry winds
Pre-existing Poor Sanitation
• Increase in Vectors of disease
transmission eg mosquitoes
•Increase or decrease in vector –borne
diseases : Malaria, yellow fever, filariasis
•Increase in water-related diseases eg
diarrhoeal diseases, Guinea worm,
•Increasing malnutrition
•Increase in Cardiovascular & respiratory
ailments
•Risks to vaccine potency due to
increasing unreliability of energy supply
•Increasing pressure on National Health
Insurance Scheme

Major Challenges to Integrated
Assessment As assessed also by SANA process-
Limitations of study include:
i. Inadequate Data
• daily morbidity data not available at regional
level to compare with meteorological data;
• short period of disease incidence data used for
establishing time series trends
ii. Influence of natural increases in population on
incidence of the diseases studied not explicitly
factored into projections of disease incidences

Limitations of study (II)
iii. Limited scope of analysis: eg
• Absence of research into CC impacts on vectors of disease transmission eg mosquito vector of malaria
• Does not consider information on perceptions of the population regarding knowledge and understanding of the disease conditions & local prevention & treatment practices
• excludes potential impacts of health systems and impact of on-going disease control interventions /programmes including vulnerability of infrastructure & support services like energy supplies for cold chain maintenance on evolution of selected diseases

19
Views of a ravaged Health Center in Northern Ghana
(roof blown off by storm) due to bad weather (2008)

Limitations of study (III)
iv. Involvement of stakeholders in health not broad
enough eg program managers, field service staff
excluded
v. Health implications of potential impact of climate
variability on other sectors not determined e.g.
�agricultural productivity increasing malnutrition as
a result of decreased food security

Utility of Assessment of Integrated Study
• Study succeeded in demonstrating that there is a linkage between trends of some common endemic communicable diseases and climate variability.
• It demonstrated fact of increase in disease burden over time but does not analyse the extent to which CC effects contribute to additional burden of disease
• Demonstrated cost of managing malaria but does not relate it to earning capacity / ability to pay
• Since modifying effects of disease control programs, human treatment seeking behaviours etc omitted, may weaken evidence base for some of the adaptation decisions

Lessons Learnti.Processes employed in integrated assessment have
led to incomplete health V & A assessment
ii. Need for thorough stakeholder analysis at onset of
V & A projects cannot be overemphasized
iii. Need for health sector to be more pro-active in CC
issues
iv. Urgent Need for a more comprehensive
assessment incorporating all the elements in
WHO’s V&A guidelines still exists via
? modification of GEF Adaptation project or
?New project within Libreville Declaration framework