Embed Size (px)
Citation preview
CLEVELAND ACUTE STROKE EXPERIENCE
• Cleveland Health Quality Choice– stroke data collected by trained abstractors since 1991– IV tPA datapoints added 1996– disbanded 1998
• Cuyahoga County Operation Stroke 1999– data collection instrument designed by the Medical Committee and
The Stroke Group (ETHOSR)
• grants from Genentech/Astra Zeneca
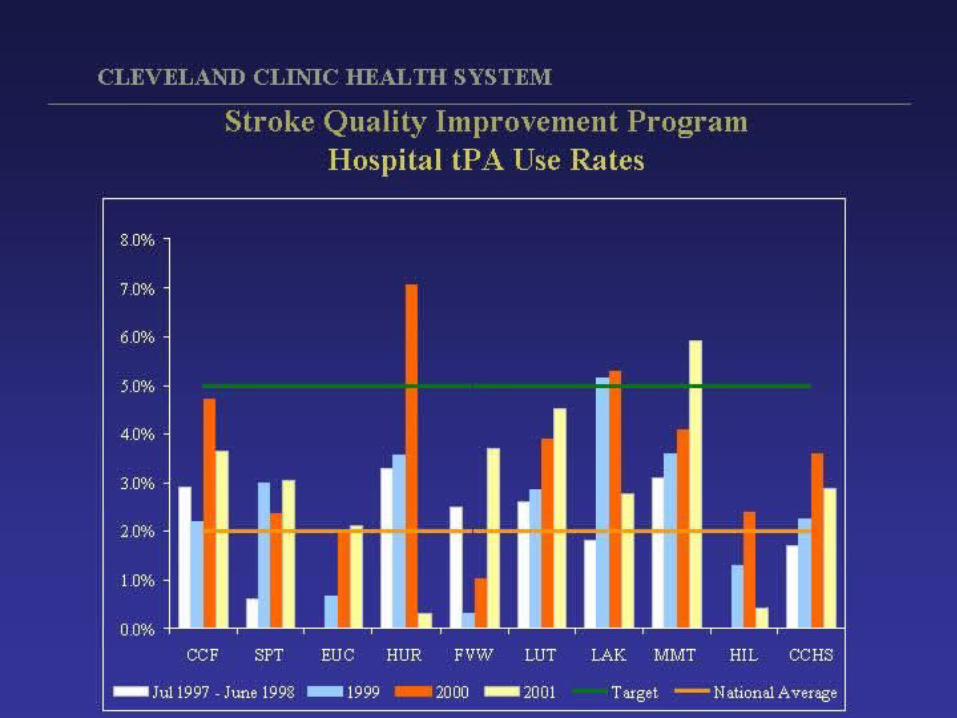
• Cleveland Clinic Health System Stroke QI Program– presented to JCAHO 4/01
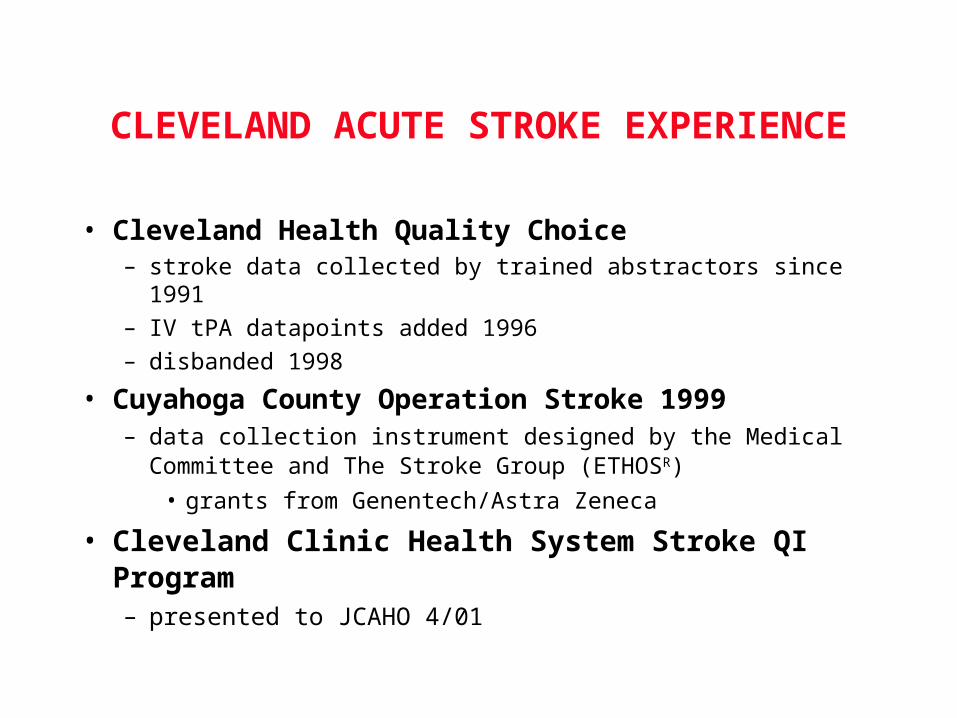
Cleveland Health Quality Choice IV tPA Utilization: Ischemic Strokes
July 1997 - June 1998
n=4275
n=70
tPA 1.8%
No tPA
98.2%
Katzan IL etal. JAMA 2000;283:1151
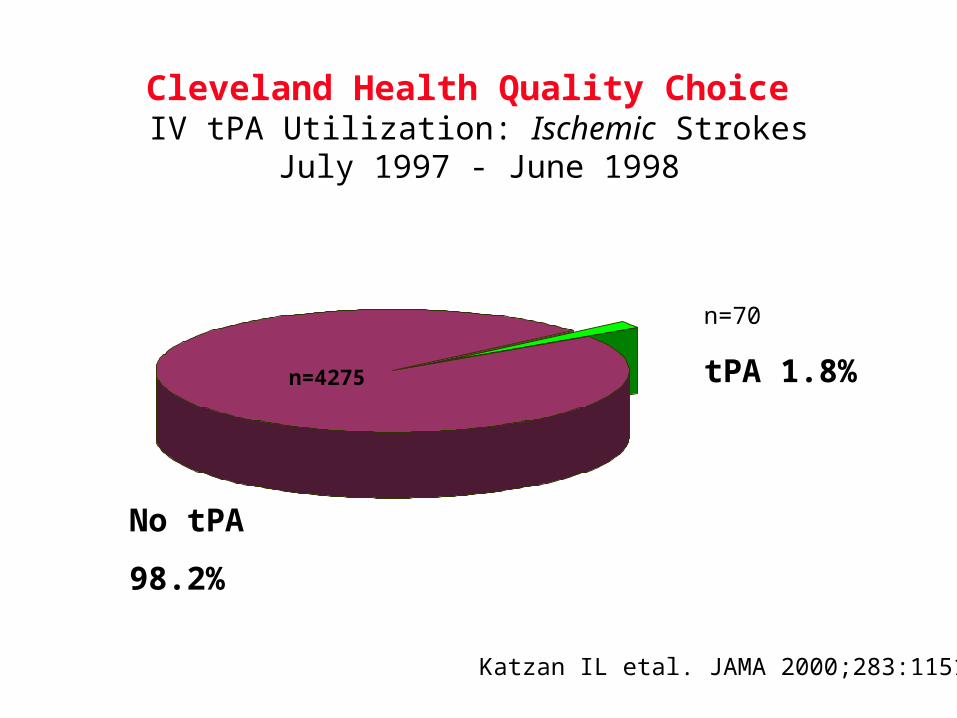
Cleveland Health Quality Choice IV tPA Utilization by Hospital
July 1997 - June 199811
5
32 2
12
1
0
2
4
6
8
10
12
0 1 2 4 5 6 9 17
# tPA cases
# H
ospi
tals
Katzan IL etal. JAMA 2000;283:1151
N = 27
(N = 70)
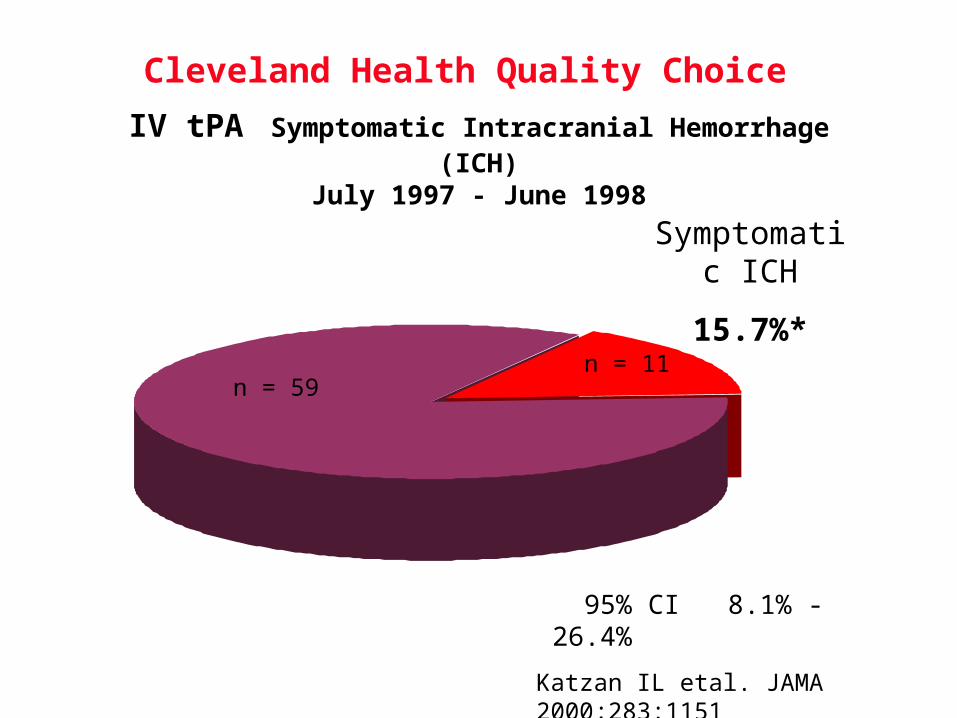
Cleveland Health Quality Choice IV tPA Symptomatic Intracranial Hemorrhage (ICH)
July 1997 - June 1998
n = 59n = 11
Symptomatic ICH
15.7%*
* 95% CI 8.1% - 26.4%
Katzan IL etal. JAMA 2000;283:1151
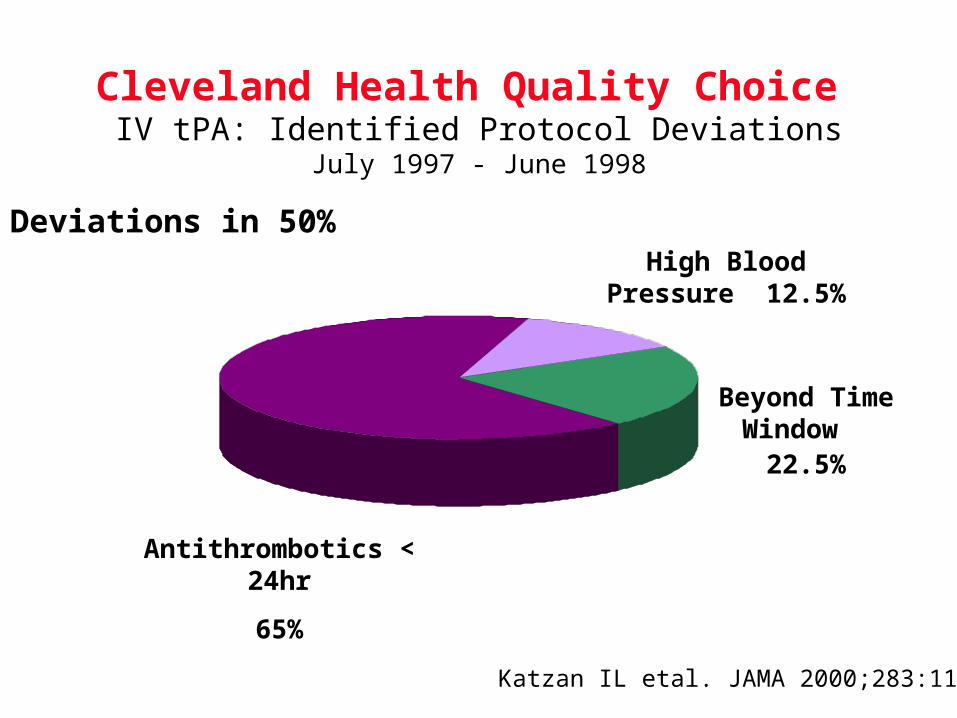
Cleveland Health Quality Choice IV tPA: Identified Protocol Deviations
July 1997 - June 1998
Antithrombotics < 24hr
65%
Beyond Time Window
22.5%
High Blood Pressure 12.5%
Katzan IL etal. JAMA 2000;283:1151
Deviations in 50%
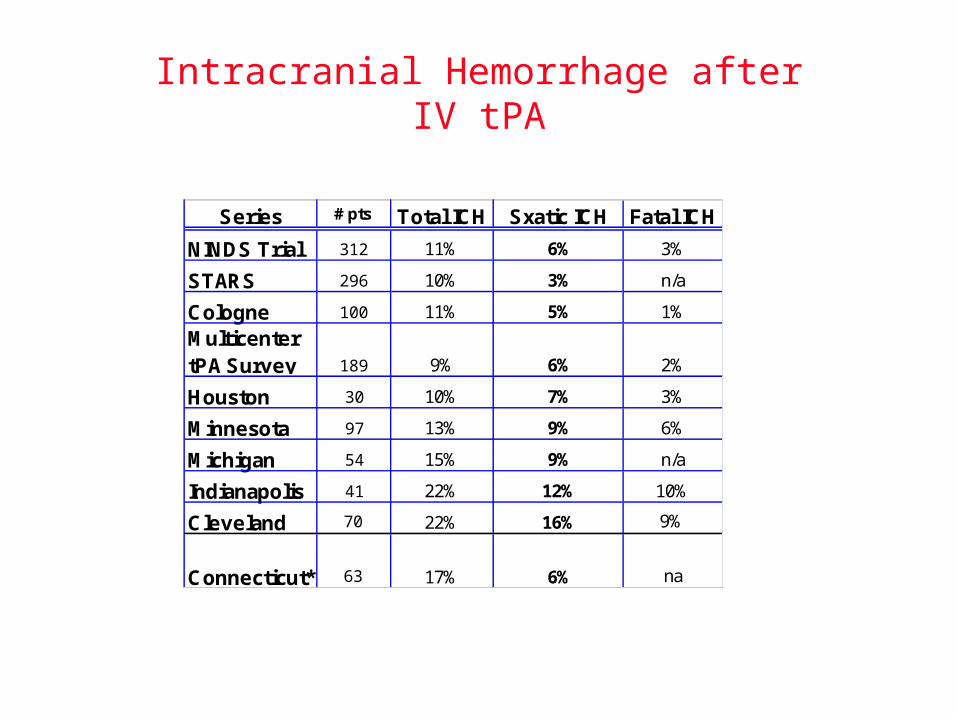
Intracranial Hemorrhage after IV tPA
Series # pts Total ICH Sxatic ICH Fatal ICH
NINDS Trial 312 11% 6% 3%
STARS 296 10% 3% n/a
Cologne 100 11% 5% 1%
Multicenter tPA Survey 189 9% 6% 2%
Houston 30 10% 7% 3%
Minnesota 97 13% 9% 6%
Michigan 54 15% 9% n/a
Indianapolis 41 22% 12% 10%
Cleveland 70 22% 16% 9%
Connecticut* 63 17% 6% na
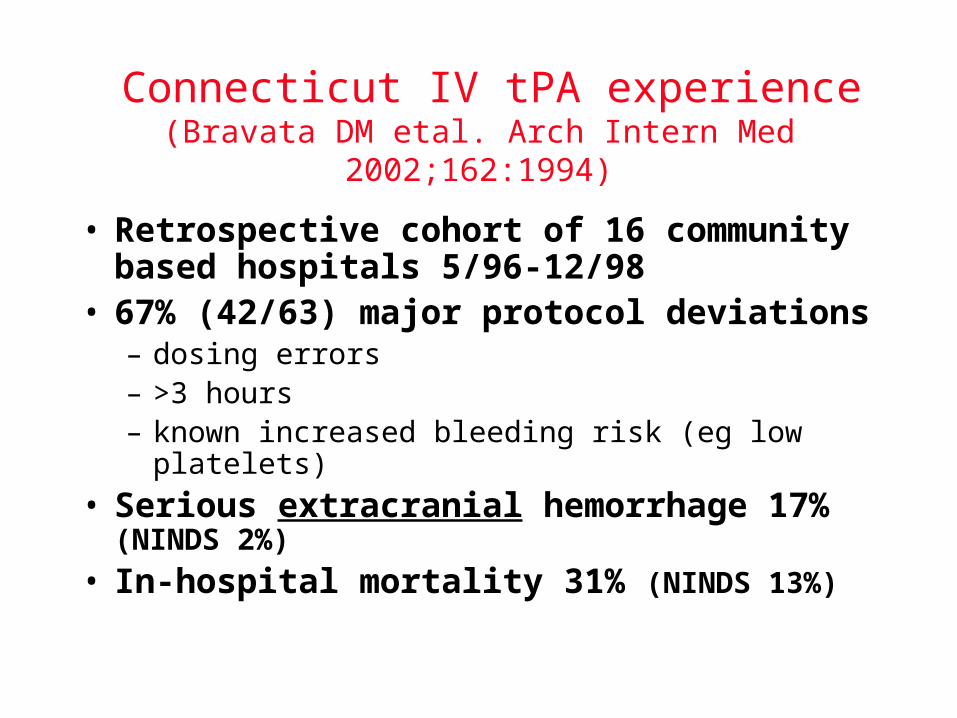
Connecticut IV tPA experience(Bravata DM etal. Arch Intern Med 2002;162:1994)
• Retrospective cohort of 16 community based hospitals 5/96-12/98
• 67% (42/63) major protocol deviations– dosing errors– >3 hours– known increased bleeding risk (eg low platelets)
• Serious extracranial hemorrhage 17% (NINDS 2%)
• In-hospital mortality 31% (NINDS 13%)
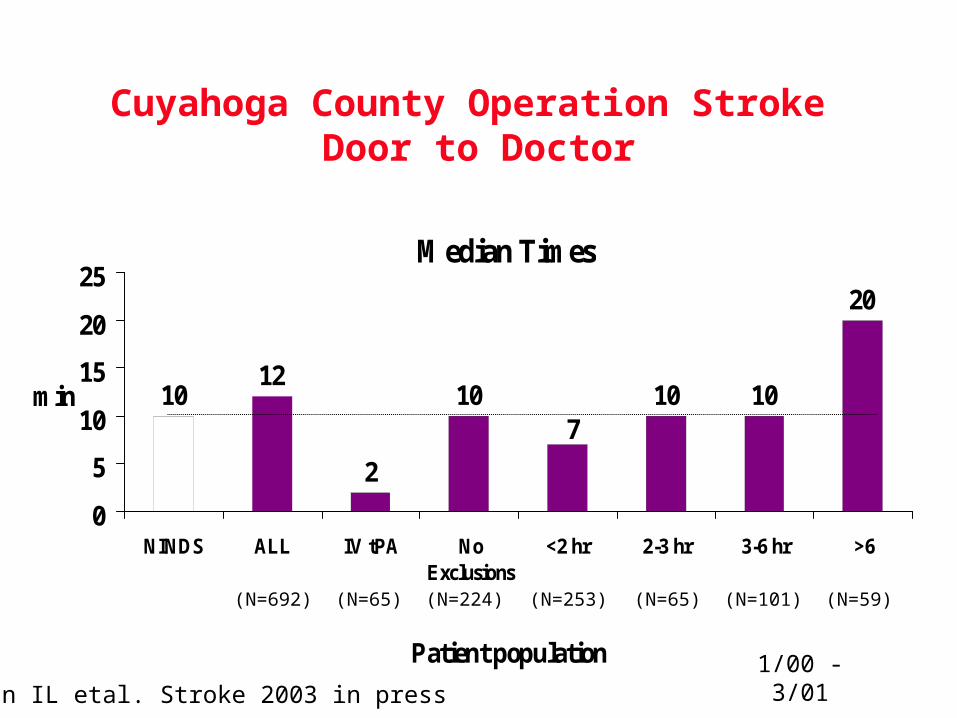
Cuyahoga County Operation Stroke Door to Doctor
Median Times
1012
2
10 10 10
20
7
0
5
10
15
20
25
NINDS ALL IV tPA NoExclusions
<2 hr 2-3 hr 3-6 hr >6
Patient population
min
1/00 - 3/01
(N=65) (N=224) (N=253) (N=65)(N=692) (N=101) (N=59)
Katzan IL etal. Stroke 2003 in press
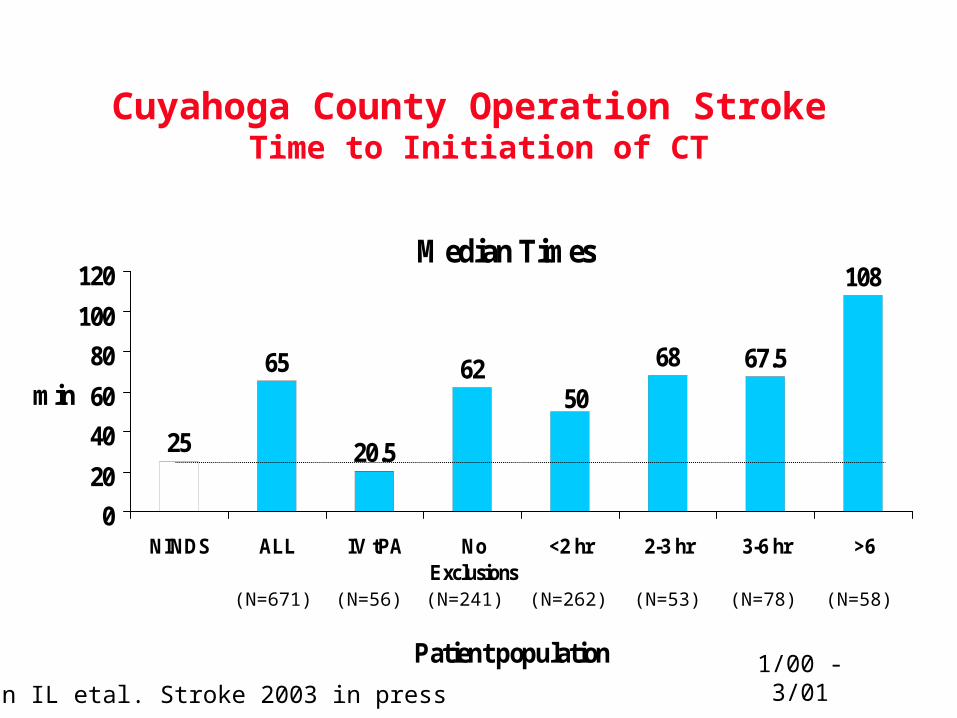
Cuyahoga County Operation Stroke Time to Initiation of CT
Median Times
25
65
20.5
62 68 67.5
108
50
0
20
40
60
80
100
120
NINDS ALL IV tPA NoExclusions
<2 hr 2-3 hr 3-6 hr >6
Patient population
min
1/00 - 3/01
(N=56) (N=241) (N=262) (N=53)(N=671) (N=78) (N=58)
Katzan IL etal. Stroke 2003 in press
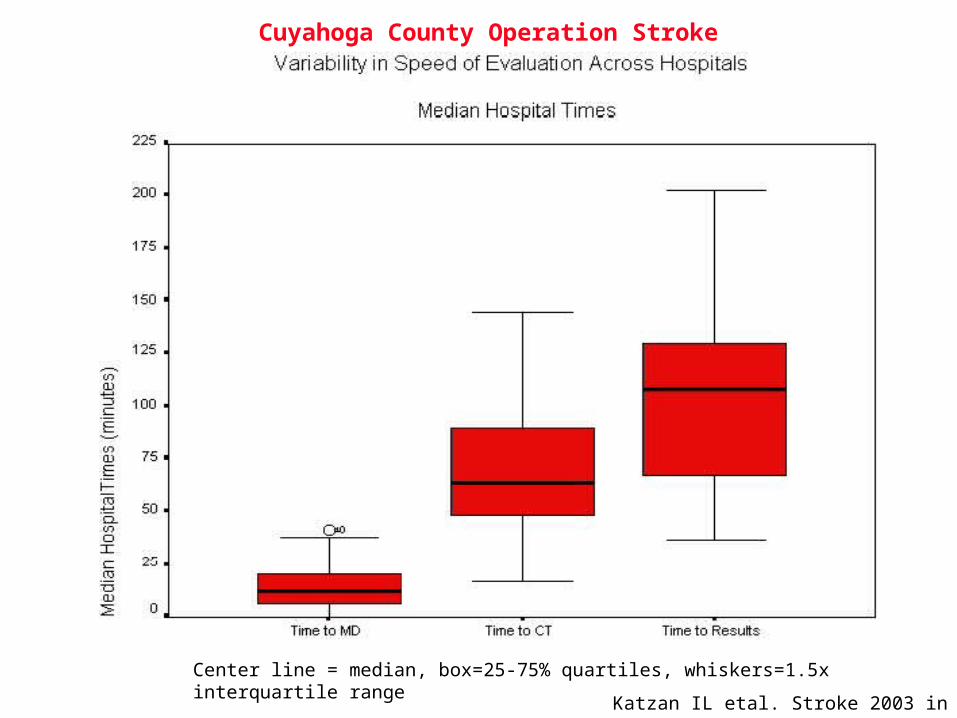
Center line = median, box=25-75% quartiles, whiskers=1.5x interquartile range
Katzan IL etal. Stroke 2003 in press
Cuyahoga County Operation Stroke
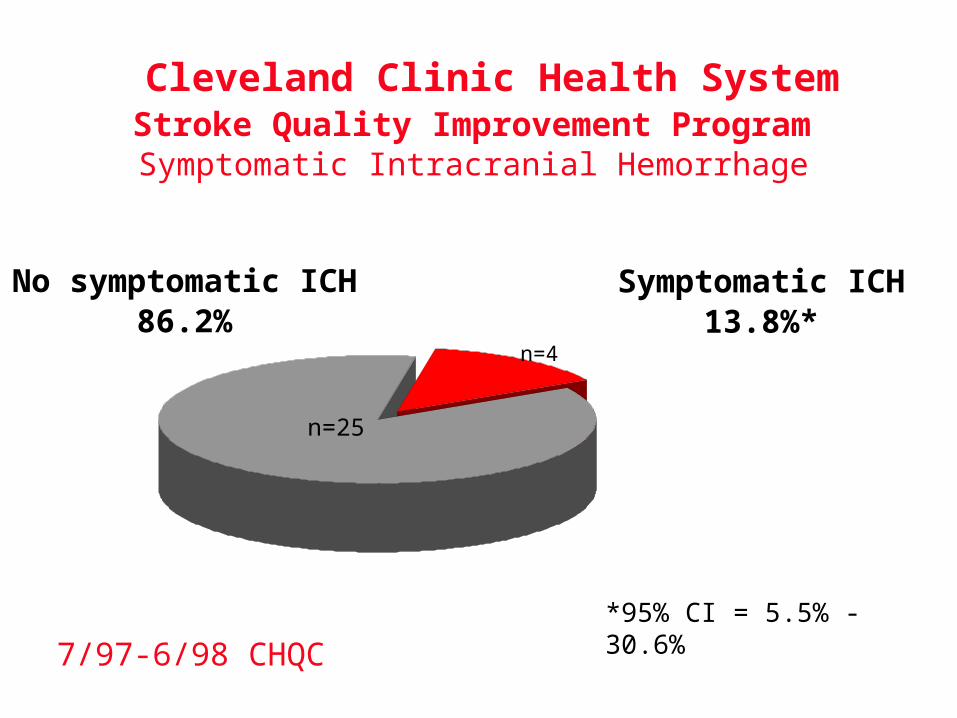
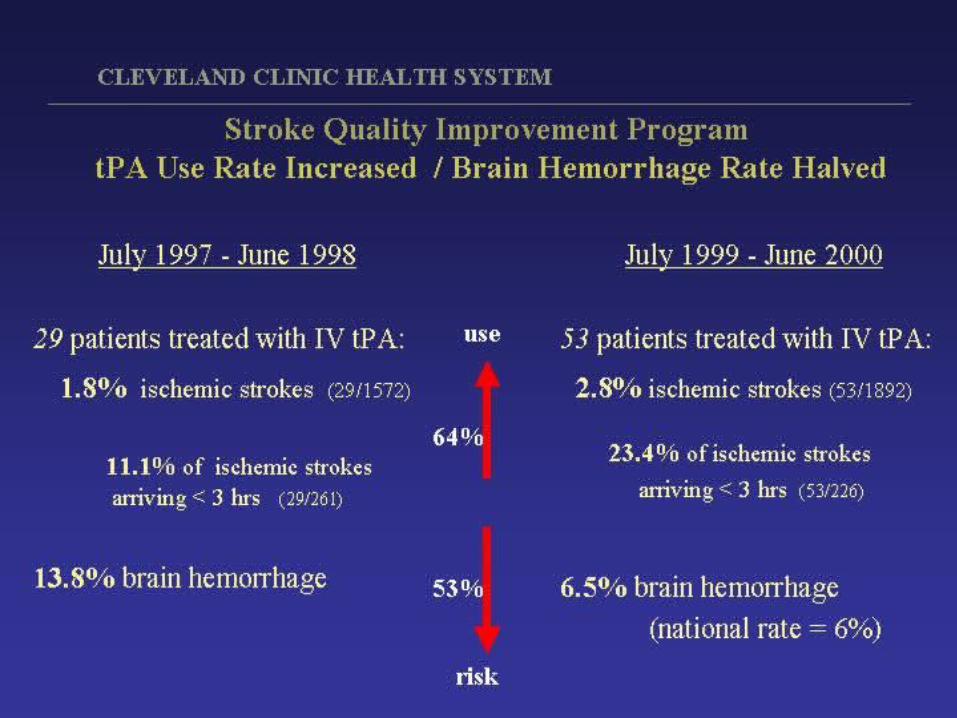
Cleveland Clinic Health SystemStroke Quality Improvement Program Symptomatic Intracranial Hemorrhage
Symptomatic ICH13.8%*
n=4
No symptomatic ICH86.2%
n=25
*95% CI = 5.5% - 30.6%
7/97-6/98 CHQC
CLEVELAND ACUTE STROKE EXPERIENCE
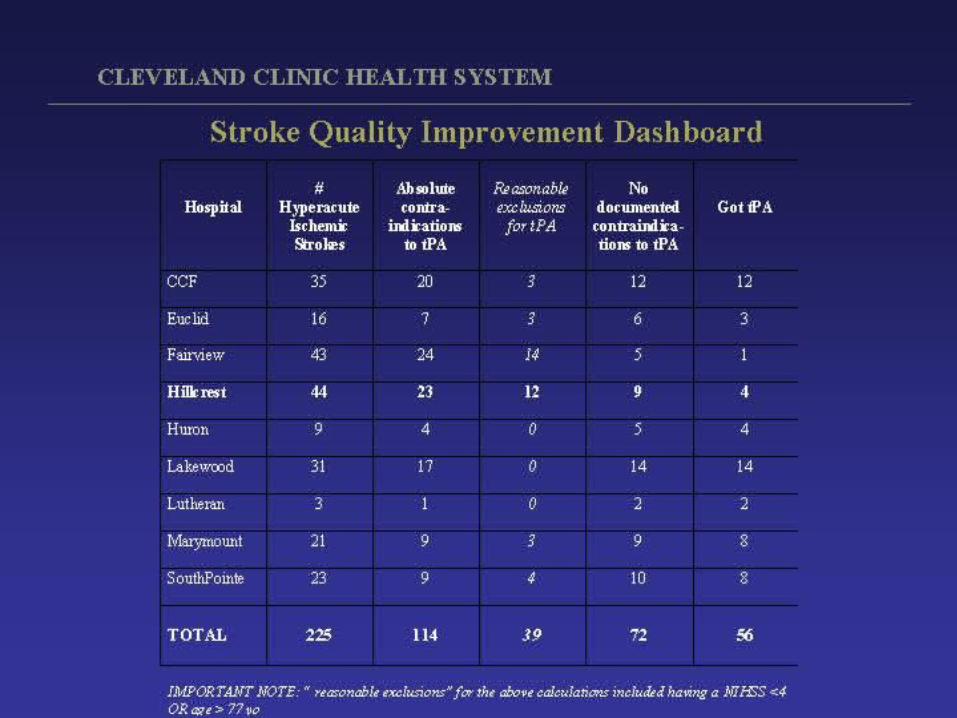
• Stroke QI requires data– quality of data varies (many hospitals = no data)– multiple barriers must be overcome (behavioral, political, resources)– team building through trust building
• Performance varies widely across hospitals– physicians and hospitals may not like their data– outliers may not mean bad care– community effectiveness may differ from NINDS efficacy
• Protocol deviations are very common – linked with bad outcomes
• Data can change behavior and improve stroke care – community performance improves over time with systematic QI
• Community hospitals can & should give IV tPA IF they are able to demonstrate they know how