Embed Size (px)
Citation preview

Department of orthodontics & dentofacial orthopedics
k.s.r.institute of dental science & research
CLEFT LIP AND PALATE
Guided byDr.S.Tamizharasi.M.D.SProfessor
Presented byDr.N.Meiyappan3rd yr PG student

Introduction
Epidemiology
Etiology
Classification
Diagnosis(Investigations) Of Cleft Lip And Palate
Orthodontic management
- Treatment In Primary Dentition
- Treatment In Mixed Dentition
- Treatment In Permanent Dentition
- Surgical management
- Distraction Osteogenesis
Conclusion
References
SYNOPSIS

INTRODUCTION

One in 700 live births globally.
Afghans (4.9%)
Negroids (0.4%)
In south india , cleft lip and palate is 1.15 and isolated
cleft palate 0.08 /1000
The incidence of oral clefts is seen more in males than
in females.
Text book of Orthodontics- O.P.Kharbanda
EPIDEMIOLOGY

Cleft lip alone- males › female
Cleft palate- females › males
Unilateral is more common than bilateral
Left is 2 times more common than right
Text book of Orthodontics- O.P.Kharbanda

ETIOLOGY
Heredity
Environmental
Malnutrition
Infections during pregnancy

ETIOLOGY
1) HEREDITY
Transmitted through a male as sex linked recessive gene.
a) Monogenic/ single gene disorder
b) Polygenic/ multifactorial inheritance
c) Chromosomal abnormalities:
- Down’s Syndrome
- Edwards Syndrome (Trisomy 18)
2. ENVIRONMENTAL FACTORS:
Usually occurs due to various influences
Excessive Alcohol
Cigarette smoking
Anti epileptic drugs. - diphenyl hydantion and
trimethadione

3. MALNUTRITION:
Folic Acid
Deficiency of folic acid affects the neural
tube- neural crest cell migration and differentiation.
4. INFECTION DURING PREGNANCY

Davis And Ritchie’s Classification -1922
Veau’s Classification - 1931
Fogh-anderson Classification - 1942
Schuchardt And Pfiefer’s Classification
Kernahan And Stark Classification - 1958
Kernahan’s Striped Y Classification
CLASSIFICATION

Millard’s Modification Of Kernahan’s Classification
Lahshal Classification
American Cleft Palate Association -1962
Internationally approved classification- 1967
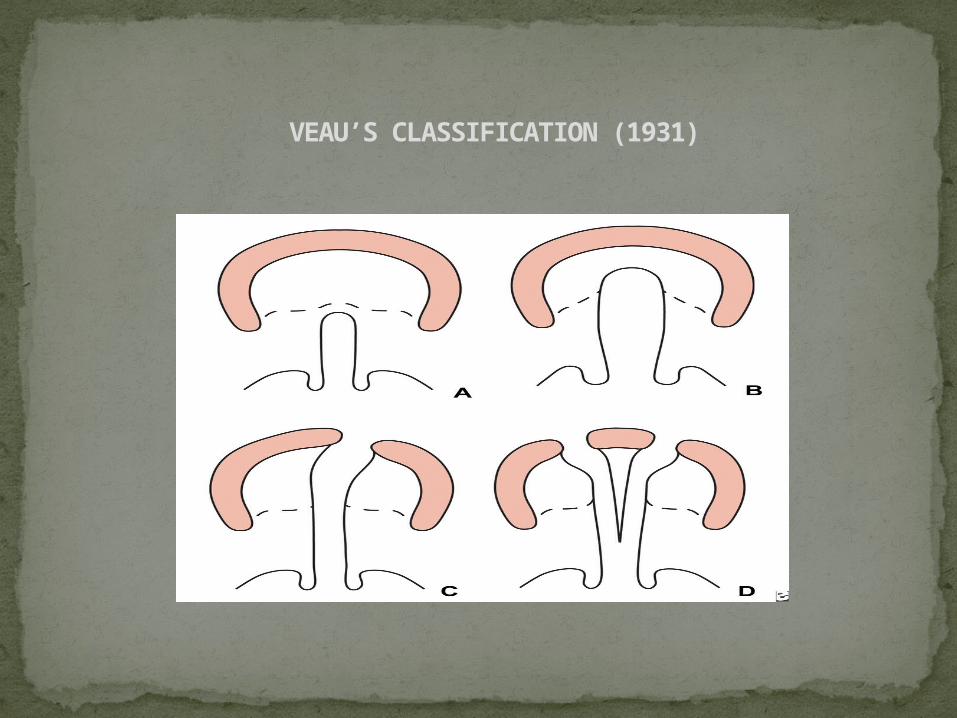
VEAU’S CLASSIFICATION (1931)

KERNAHAN AND STARK CLASSIFICATION 1958
GROUP A : Clefts of the primary palate
GROUP B : Clefts of the secondary palate
GROUP C : Clefts of the primary and secondary palate
SCHUCHARDT AND PFIEFER’S CLASSIFICATION
LIP
ALVEOLUS
HARD PALATE
SOFT PALATE

KERNAHAN’S STRIPED “Y” CLASSIFICATION (1971)

MILLARD’S MODIFICATION OF KERNAHAN’S CLASSIFICATION (1977)

LAHSHAL CLASSIFICATION
L - Lip
A - Alveolus
H - Hard palate
S – Soft palate
H – Hard palate
A - Alveolus
L - Lip

AMERICAN CLEFT PALATE ASSOCIATION
A. CLEFTS OF THE PRE –PALATE :
Cleft of the lip
Cleft o f the alveolus
Cleft of the primary palate
B. CLEFTS OF THE PALATE :
Cleft of the hard palate
Cleft of the soft palate

INTERNATIONALLY APPROVED CLASSIFICATION- 1967

DIAGNOSIS

PRENATAL DIAGNOSIS
Ultrasonography is a non invasive diagnostic tool which is now
routinely used as a part of prenatal diagnosis.
TIMING OF DETECTION :
Christ and Meninger :
Optimal imaging of the fetal face is not reliable with
transabdominal
ultrasonograpy until gestational week 15.
Robinsen et al :
Greatly improved when performed after 20 weeks of
gestation.

ADVANTAGES :
Psychological preparation of the parents and caregivers
Education of parents on management of cleft
Preparation for neonatal care and feeding
Opportunity to investigate for other abnormalities
DISADVANTAGES :
Emotional disturbance and high maternal anxiety
Chances to terminate pregnancy.

MANAGEMENT TEAM

NEONATAL AND INFANT MANAGEMENT
THREE MAIN PRINCIPLES:
Establishment Of Feeding
Pre-surgical Maxillary Orthopedics
Naso-alveolar Moulding

CLEFT PALATE :
1. Inability to create negative pressure for suckling
2. Nasal regurgitation
3. Chances of choking and cyanosis
4. Engulfing of trapped air which needs frequent
burping
ESTABLISHMENT OF FEEDING

FEEDING POSITION FOR A CLEFT CHILD
A semi upright position ( 30˚ to 45˚ ) – reduces nasal regurgitation
Feeding should not be hurried

FEEDING OBTURATOR
The feeding obturator is a prosthetic aid that is
designed to obturate the cleft and restore the
separation between the oral and nasal cavities.

INFANT / PRE SURGICAL ORTHOPEDICS
Pre surgical orthodontic or neonatal maxillary
orthopedics is initiated during the 1st or 2nd week
following birth.
Introduced by McNeil and popularized by Burstone
in 1950s .
Good functioning palate, normalise tongue
positions and help in speech development.

Two movements must be carried out
Expansion of the collapsed segments and
Pressure against pre maxilla to its correct position.
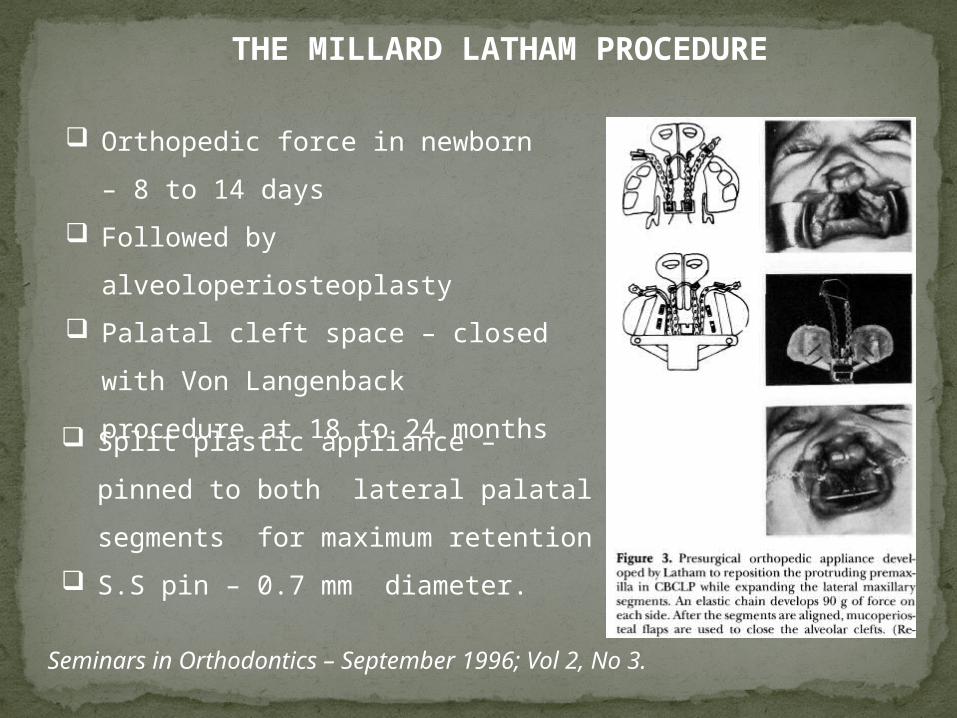
THE MILLARD LATHAM PROCEDURE
Split plastic appliance – pinned to
both lateral palatal segments for
maximum retention
S.S pin – 0.7 mm diameter.
Orthopedic force in newborn – 8
to 14 days
Followed by
alveoloperiosteoplasty
Palatal cleft space – closed with
Von Langenback procedure at
18 to 24 months
Seminars in Orthodontics – September 1996; Vol 2, No 3.

NASO ALVEOLAR MOULDING
Nasoalveolar molding is a new nonsurgical method of
reshaping the gums, lip and nostrils before cleft lip and palate
surgery, reducing the severity of the cleft.
Initiated within 4-8 weeks of birth and finished before primary
closure of lip.
Used for 4-6 months


ADVANTAGES
Proper alignment of the lip, alveolus and nose helps the
surgeon to achieve a better and more predictable surgical
result
The cleft deformity is significantly reduced in size.
Studies have demonstrated that 60 % of patients who
underwent NAM and gingivoperioplasty did not require
secondary bone grafting.
COMPLICATIONS
Irritation to the oral mucosa, gingival tissue or nasal mucosa.
Irritation to the cheeks

LIP CLOSURE
A good lip seal is essential for phonation ,
articulation and for optimal balance of muscular
forcesin the orofacial region.
TIMING OF LIP CLOSURE :
At the age of 3 months (or) 10 weeks.

Techniques
1. Tennison’s triangular flap
2. Millard rotation flap
‘THE RULE OF 10’
Weight - 10 lbs
Age - 10 weeks
Hb - 10 gm %

PALATE CLOSURE
Objective:
Join the cleft palatal edges,
Lengthen the soft palate,
The timing of closure is controversial. Can be
done early at 12-18 months or at 9-12year
Surgery and scarring shouldnot adversely affect
the dentition and growth of the maxilla

RECENT THOUGHT
Closure of soft palate –age of 12 month
Help in development of Speech
No growth retardation with early soft palate
closure
Closure of hard palate –age of 5-6year
Hard palate repair timing and facial growth in cleft lip and palate : A systematic
review - Yu-Fang Liao, Michael Mars . Cleft palate – Craniofacial Journal,
September 2006, Vol 43, No 5.

Velopharyngeal insufficiency is a disorder resulting in
the improper closing of the velopharyngeal sphincter
(soft palate muscle in the mouth) during speech,
allowing air to escape through the nose instead of the
mouth.
VELOPHARYNGEAL INSUFFICIENCY
During speech, the velopharyngeal sphincter must
close off the nose to properly pronounce strong
consonants such as "p," "b," "g," "t" and "d."

The two main speech symptoms of velopharyngeal
insufficiency are:
Hypernasality and Nasal air emission.

Speech Therapy
Some speech problems linked with VPI, such as
mispronouncing words, can be treated by speech therapy.
TREATMENT OF VPI
Sometimes an obturator is recommended to treat VPI.
Modified obturator called speech bulb appliances are
useful where palatal lift or soft palate closure is needed .
Pharyngoplasty and palate lengthening are performed to
maintain velo-pharyngeal seal

Orthodontic Intervention
During Mixed Dentition(7-
12 yrs )

GOALS IN MIXED DENTITION
Maxillary Expansion
Alveolar Bone Graft
Primary
Secondary

Aimed at providing a bony bridge to the cleft in the
alveolus area.
Primary - first few days – 2.5 yrs of age .
Early secondary - 2- 5 yrs
Intermediate or secondary – 6- 13 yrs
Late – after 13 yrs .
Primary and early secondary are not in practice bec of
additional surgery required.
ALVEOLAR BONE GRAFT

Boyne and Sands in 1972.
Aimed to bridge the cleft segment with grafted
cancellous bone.
MERITS
Elimination of bony clefts and encouraging normal
eruption of lateral incisor and canine through
cancellous bone.
Secondary alveolar bone grafting

Orthodontic closure of cleft space becomes possible .
Helps in closure of oronasal fistulas.
Provides bony support to alar base and improvement in
aesthetics.
Stabilization of maxillary segments – helpful during surgery
TIMING OF SURGERY
Based on root formation of lateral incisor and canine.
Favor of 8-10 year of age (when canines about to erupt-
one quarter to two thirds of root complete)- Bergland et
al
Erupting tooth is a potent stimulus for bone formation.
After tooth eruption is complete, it can be very difficult to
induce the formation of new bone.

PRE –BONE GRAFT ORTHODONTICS
Contributes to better access of site for the surgeon.
Maxillary arch expansion using Quad helix appliance


Bergland and coworkers – index to evaluate success of the
grafted bone based on the height of interdental septum on
IOPA .
TYPE I – normal
TYPE II – 75% of normal bone height
TYPE III- less than 75%
TYPE IV – no bony ridge
POST BONE GRAFT FOLLOWUP


Orthodontic management in permanent dentition stage

Two to three years after bone graftng ,
comprehensive orthodontic treatment can be
started.
If the lateral incisor is present and viable in cleft
region . Every attempt shouldbe made to preserve
it.
Completed by 15 yrs of age.
Rigid palatal retainers – wire framework soldered
on molar bands are considered to maintain arch
alignment and expansion.
ORTHOGNATHIC SURGERY COMBINED WITH ORTHODONTICS
Due to severe skeletal discrepancy, there is
Deterioration of esthetics and occlusion,
Psychological implications leading to low self
esteem,
Defective speech,
Oronasal fistulas.
Such cases require a combined orthodontic and
orthognathic approach.

Maxillary advancement
To correct the size and position of
maxilla.
Multiple segment LeFort I osteotomies –
To correct the transverse problem.
For a bilateral CLCP three-piece maxillary surgery (allows
rotation of segments )
For unilateral CLCP a two piece is sufficient.(Vlachos 1996)
SURGICAL PROCEDURES IN A CLEFT PATIENT


Severe cases - May require bi jaw surgery.
Proffit recommends overcorrecting the anterior cross bite
in excess of positive over jet- compensate for post surgical
relapse.
In cases with an over jet of more than 8mm mandibular
surgery (BSSO) also must be considered. Skeletal facial balance and harmony in the cleft patient- principles and
techniques in orthognathic surgeryIndian J Plast Surg 2009 vol 42 No 1

DISTRACTION OSTEOGENESIS
1903 .- Dr. Gavril of Russia-Bone lengthening of leg.
Introduced in ORTHODONTICS BY ILIZAROV IN 1950
It is a procedure by which formation of new bone is induced
by external tension created by distracting devices at the site of
osteotomy.
The distractor is gradually adjust over a period of days or week
to stretch the osteotomy site so that new tissue fills it.

Ross and Subtenly
Distraction osteogenesis
Allows soft tissue adaptation, including scar tissue.
Doesn’t cause a problem with velo- pharyngeal
insufficiency .
Distraction Of maxilla first proposed by Molina & Oritz-
Monasterio(1998)
Maxillary distraction devices
External distractors Internal distractors
External frame distraction of the midface in cleft palate patientsEur J Orthod 2009 vol 41

EXTERNAL DISTRACTORS
Advantage:
Direction of force is well controlled
Dis advantage:
Cranial surgery is required
Esthetics are compromised

INTERNAL DISTRACTORS
Advantage:
Esthetics
Psychological relief
Disadvantage:
Difficult to control the direction of force

Prosthodontic Treatment:
It may be required in cases where replacement of missing
teeth is essential. Removable or fixed prosthesis may be
given. It allows for improved speech and better esthetics.


CONCLUSION
Treatment of a child with cleft lip and cleft palate begins
from the day of born. psychological counselling of the
parent and full team effort in which an orthodontist plays a
vital role and works with various specialists to provide
quality care to the patient and to start hloistic treatment
planning.

REFERENCES
Orthodontic Current Principles and techniques –
Graber and Vanarsdall - 5th Edition
William R. Proffit. Contemporary Orthodontics. 5TH
Edition
Textbook of Orthodontics – O.P.Kharbhanda
Cleft lip and cleft palate – diagnosis and management
2nd edition – Samuel Berkowitz

Cleft lip and cleft palate – Seminars in Orthodontics –
September 1996; Vol 2, No 3.
Pre surgical Naso alveolar molding treatment in cleft
lip and palate patients – Barry H. Grayson, Indian
J Plast Surg Supplement 1 2009 vol 42.
Indian J Plast Surg Supplement 1 2009, vol 42.

External frame distraction of midface in cleft patients - Indian
J Plast Surg
supplement 1 2009 Vol 42.
Velopharyngeal impairment in orthodontic population-
Seminars in Orthodontics – September 1996; Vol 2, No 3.
Alveolar grafting - Indian J Plast Surg 2009 vol 42 no 1
Hard palate repair timing and facial growth in cleft lip and
palate : A systematic review - Yu-Fang Liao, Michael Mars .
Cleft palate – Craniofacial Journal, September 2006, Vol 43, No
5.

Thank you























![Cleft Lip Palate[1]](https://img.pdfslide.us/doc/110x75/577cdb8f1a28ab9e78a88308/cleft-lip-palate1.jpg)

