Embed Size (px)
Citation preview

wps
Classification and Prognostic Evaluation ofMyelodysplastic Syndromes
Mario Cazzola, Matteo G. Della Porta, Erica Travaglino, and Luca Malcovati
Myelodysplastic syndromes (MDS) are myeloid neoplasms characterized by dysplasia in one ormore cell lines and increased risk of development of acute myeloid leukemia (AML). The currentdiagnostic approach to MDS includes peripheral blood and bone marrow morphology to evaluateabnormalities of peripheral blood cells and hematopoietic precursors; bone marrow biopsy toassess marrow cellularity, fibrosis, and topography; and cytogenetics to identify non-randomchromosomal abnormalities. The 2008 World Health Organization (WHO) classification currentlyprovides the best diagnostic approach to MDS and also has considerable prognostic relevance. TheWHO classification-based prognostic scoring system (WPSS) is able to classify MDS patients intofive risk groups showing different survivals and probabilities of leukemic evolution. The WPSSis able to predict survival and leukemia progression at any time during follow-up, and cantherefore be used for implementing risk-adapted treatment strategies in patients with primaryMDS. Since comorbidities have a significant impact on the outcome of patients with MDS,accounting for both disease status and comorbid conditions considerably improves riskstratification.Semin Oncol 38:627-634 © 2011 Elsevier Inc. All rights reserved.
Myelodysplastic syndromes (MDS)1 are in-cluded in the World Health Organization(WHO) classification of the myeloid neo-
plasms2 together with myeloproliferative neoplasms(MPN), myelodysplastic/myeloproliferative neoplasms(MDS/MPN),3,4 and acute myeloid leukemia (AML).
MDS typically occur in elderly people and representone of the most common hematologic malignancies inWestern countries, their annual incidence exceeding 20per 100,000 persons over the age of 70 years.5 MDS arecharacterized by clonal proliferation of hematopoieticcells, which partly retain their capacity to differentiateand maturate, but do so in an inefficient manner, basicallyas a result of excessive apoptosis of hematopoietic pre-cursors.1 The bone marrow is generally hypercellular
hile peripheral blood cells are variably reduced (cyto-enia), and several morphological abnormalities are ob-erved in these two compartments.6 In addition, clones of
hematopoietic cells carrying non-random cytogenetic ab-normalities are typically found in these patients.7 Withtime there is a progressive impairment in the capacity of
Department of Hematology Oncology, Fondazione IRCCS PoliclinicoSan Matteo and University of Pavia Medical School, Pavia, Italy.
Address correspondence to Mario Cazzola, MD, Department of Hema-tology Oncology, Fondazione IRCCS Policlinico San Matteo, VialeGolgi 19, 27100 Pavia, Italy. E-mail: [email protected]
0270-9295/ - see front matter© 2011 Elsevier Inc. All rights reserved.
doi:10.1053/j.seminoncol.2011.04.007Seminars in Oncology, Vol 38, No 5, October 2011, pp 627-634
hematopoietic cells to differentiate and maturate: blastcells may appear in the bone marrow and peripheralblood, and there is an increasingly high risk of evolutionto overt AML.
CLASSIFICATION OF MDS
The current diagnostic approach to MDS includesperipheral blood and bone marrow morphology toevaluate abnormalities of peripheral blood cells andhematopoietic precursors; bone marrow biopsy to as-sess marrow cellularity, fibrosis, and topography; andcytogenetics to identify non-random chromosomal ab-normalities. The combination of overt marrow dyspla-sia and clonal cytogenetic abnormality allows a conclu-sive diagnosis of MDS, but this is found in only aportion of patients.1 Standardization of flow cytometrymight improve diagnosis of MDS in the future.8–10
Although bone marrow biopsy may be consideredtoo invasive for elderly patients, it provides extremelyuseful diagnostic and prognostic information regardingcellularity, fibrosis, and CD34� cell topography.11 Hyp-oplastic MDS needs to be distinguished from bothaplastic anemias and hypocellular AML.12 Bone marrowfibrosis identifies a distinct subgroup of MDS with mul-tilineage dysplasia, high transfusion requirement, andpoor prognosis, while the presence of CD34� cell clus-ters is an independent risk factor for progression to
acute leukemia.11627

W(smaa
628 M. Cazzola et al
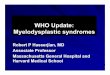
MDS were defined and classified in 1982 by theFrench-American-British (FAB) group.13 The FAB classifi-cation included five categories and is described in Table 1.From a prognostic point of view, this classification wasessentially able to identify two risk groups based on theabsence or presence of blast excess14 (Figure 1).
In 2001 the WHO classification was developed.15
This classification, updated in 2008 and illustrated inTable 2,16 carries relevant prognostic information asshown in Figure 2.14,17
PROGNOSTIC EVALUATION OF MDS
Although the FAB classification has been relativelyeffective for categorizing MDS patients since 1982,
Figure 1. Kaplan-Meier survival curves of 943 patientsdiagnosed with MDS according to the 2008 WHO criteriaand here grouped according to the FAB classification (pa-tients with 5%–19% bone marrow blasts and Auer rodswere classified as RAEB-t). Reproduced from Cazzola with
Table 1. FAB Classification of Myelodysplastic Sy
Category
Peripheral Blood
Monocytes(109/L) Blast (%)
Refractory anemia (RA) �1 �1%RA with ring
sideroblasts (RARS)�1 �1%
RA with excess of blasts(RAEB)
�1 �5%
Chronicmyelomonocyticleukemia (CMML)
�1 �5%
RAEB “intransformation”(RAEB-t)
�1 �5%
permission.14
its limitations soon became evident. According toGreenberg et al18 these limitations include the widerange of marrow blast percentages for patients withrefractory anemia with excess blasts (RAEB) andchronic myelomonocytic leukemia (CMML), lack ofinclusion of critical biological determinants such asmarrow cytogenetics, and the degree and number ofmorbidity-associated cytopenias. These limitationsled to the development of additional risk-based strat-ification systems.18
The International MDS Risk Analysis Workshop(IMRAW) concluded that the percentage of marrowblasts, cytogenetic pattern, and number and degreeof cytopenias were the most powerful prognosticindicators in MDS, and this resulted in the definitionof the International Prognostic Scoring System (IPSS;Table 3).19
After introduction of the WHO classification, wefound that WHO categories, cytogenetic pattern, andtransfusion dependency were the most powerful prog-nostic indicators. We therefore developed a prognosticmodel that accounted for these parameters.20 This
HO classification-based prognostic scoring systemWPSS) could classify patients into five risk groupshowing different survivals and probabilities of leuke-ic evolution. A refined version of the WPSS, based onstudy on prognostic significance of the degree of
nemia,21 is reported in Table 4.Kantarjian and coworkers22 performed a multivari-
able analysis of prognostic factors in 1,915 MDSpatients. They identified the following adverse, inde-pendent factors: poor performance, older age,thrombocytopenia, anemia, increased bone marrowblasts, leukocytosis, chromosome 7 or complex (�2)abnormalities, and prior transfusions. Based on these
es13
Bone Marrow
ed Sideroblasts (%) Blast (%) Auer Rods
�15% �5% —�15% �5% —
d sideroblasts may ben
5%–20% —
d sideroblasts may ben
0%–20% —
d sideroblasts may ben
21%–30% �
ndrom
Ring
Ringesee
Ringesee
Ringesee
parameters, a new MDS prognostic model divided

Classification of myelodysplastic syndromes 629
Table 2. 2008 WHO Classification of Myelodysplastic Syndromes: Basic Criteria, Improvements, andOpen Questions*
Condition Blood Findings Bone Marrow Findings Remarks
Refractory cytopeniawith unilineagedysplasia (RCUD)†
Unicytopenia (anemia,neutropenia, orthrombocytopenia),no or rare blasts(�1%). Bicytopeniamay occasionally beobserved.
Unilineage dysplasia (�10%of the cells in one myeloidlineage) �5% blasts,�15% ringed sideroblastswithin erythroidprecursors.
The diagnosis of this conditionis definitely easier when acytogenetic abnormality isfound.
Refractory anemiawith ringedsideroblasts (RARS)
Anemia, no blasts. Erythroid dysplasia only, �5%blasts, �15% ringedsideroblasts withinerythroid precursors.
Ringed sideroblasts represent arobust marker of abnormalerythropoiesis. They must bedistinguished from ferritinsideroblasts: consensuscriteria have been publishedfor the definition andenumeration of ringedsideroblasts.6
Refractory cytopeniawith multilineagedysplasia (RCMD)
Cytopenia(s)(unicytopenia,bicytopenia orpancytopenia), no orrare blasts (�1%), noAuer roads, �1x109/Lmonocytes.
Dysplasia in �10% of cellsin 2 or more myeloid celllineages (erythroidprecursors and/orneutrophil precursors and/or megakaryocytes), �5%blasts, no Auer roads (thepercentage of ringedsideroblasts is irrelevant).
Multilineage dysplasia wasintroduced in 2001 and wascriticized as a feature thatrequires considerable expertiseand is poorly reproducible.However, this is true for manyother morphological featuresof myeloid and lymphoidneoplasms. More importantly,multilineage dysplasia hasrelevant negative prognosticimplications (see Figure 2).17
Refractory anemiawith excess blasts-1 (RAEB-1)
Cytopenia(s), �5%blasts, no Auer roads,�1x109/L monocytes(cases with Auer rodsand �5% blasts inthe peripheral bloodand �10% blasts inthe marrow should beclassified as RAEB-2).
Unilineage or multilineagedysplasia, 5% to 9%blasts, no Auer roads(cases with Auer rods and�5% blasts in theperipheral blood and�10% blasts in themarrow should beclassified as RAEB-2). RAEB-1 includes also cases with2–4% blasts in theperipheral blood and �5%in the bone marrow.
Consensus criteria have beenpublished for the definitionand enumeration of blasts.6
Refractory anemiawith excess blasts-2 (RAEB-2)
Cytopenia(s), 5–19%blasts, occasional Auerroads, �1x109/Lmonocytes.
Unilineage or multilineagedysplasia, 10% to 19%blasts, occasional Auerroads.
Consensus criteria have beenpublished for the definitionand enumeration of blasts.6
Myelodysplasticsyndromeassociated withisolated del(5q)
Anemia, normal toincreased plateletcount, no or rareblasts (�1%).
Normal to increasedmegakaryocytes withhypolobated nuclei, �5%blasts, no Auer roads,isolated del(5q).
Diagnosis of MDS with isolateddel(5q) is generally easy dueto its typical hematologicpicture, morphologicalabnormalities, andcytogenetic aberration.

630 M. Cazzola et al
patients into four prognostic groups with signifi-cantly different outcomes (Table 5). The authorsconcluded that this new risk model (M.D. AndersonPrognostic Scoring System [MPSS]) refines the prog-nostic precision of the IPSS and is applicable to allpatients with primary or secondary MDS and to thosewith CMML rather than only to patients with un-treated primary MDS.
In conclusion, there are 3 risk models at present;their advantages and disadvantages are summarized inTable 6.
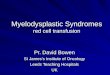
Figure 2. Kaplan-Meier survival curves of 943 patientsdiagnosed with MDS according to the 2008 WHO criteria.Patients classified as RA or RARS according to the FABclassification in Figure 1 are split here into two subgroupswith different survival based on the presence of unilineage[RCUD or RARS, including also MDS with del(5q)] or multi-lineage dysplasia (RCMD). Moreover, patients with RAEB inFigure 1 are also split here into two subgroups according totheir blast percentage (5–9% in RAEB-1, 10–19% in RAEB-
Table 2. Continued
Condition Blood Findings Bo
Myelodysplasticsyndrome,unclassifiable(MDS-U)
Cytopenia (variouscombinations), no orrare blasts (�1%).
DyspofmyacccytconeviMD
*Information on the WHO classification is from Brunning et al.1†Refractory anemia (RA), refractory neutropenia (RN), or refract
2). Reproduced from Cazzola.14
PROGNOSTIC RELEVANCE OF COMORBIDITIESIN MDS PATIENTS
Most patients with MDS are elderly and typicallyhave comorbid diseases that have a significant impacton their clinical outcome.25,26
We recently performed a study aimed to developa scoring model that accounted for comorbiditiescommonly found in MDS patients and to establishhow these comorbid conditions affected survival.27
Comorbidity was present in 54% of patients and hada significant impact on both non-leukemic death andoverall survival. Cardiac disease was the most fre-quent comorbidity and the main cause of non-leuke-mic death. Cardiac, liver, renal, and pulmonary
rrow Findings Remarks
less than 10%one or moreell lines whenied by aic abnormalityd as presumptivefor a diagnosis of% blasts.
These patients need to befollowed closely in order tobetter define their condition.
mbocytopenia (RT).
Table 3. International Prognostic Scoring Sys-tem (IPSS) of Myelodysplastic Syndromes19
Variable
Points
0 0.5 1 1.5 2
Marrowblasts (%)
�5 5–10 11–20 21–30
Karyotype* Good Intermediate PoorCytopenias† 0 or 1 2 or 3
IPSS RiskGroup Score
Low 0Intermediate 1 0.5–1.0Intermediate 2 1.5–2.0High 2.5–3.5
*Good: normal, del(5q) only, del(20q) only, –Y only; Poor:very complex (�2) abnormalities, chromosome 7 anoma-lies; Intermediate: other abnormalities.
†Cytopenias: hemoglobin �10 g/dL, neutrophil count � 1.8� 109/L, platelet count � 100 � 109/L.
ne Ma
lasia incells ineloid companogenetsidere
denceS, �5
6
ory thro

Classification of myelodysplastic syndromes 631
disease and solid tumors were found to indepen-dently affect the risk of non-leukemic death. Usingthis information, a time-dependent MDS-Specific Co-morbidity Index (MDS-CI) was developed for predict-ing the effect of comorbidity on outcome. This iden-tified three groups of patients that showed significantlydifferent probabilities of survival as shown in Figure 3.We concluded that accounting for both disease statusby means of the WPSS and comorbidity through the
Table 4. Refined WHO Classification–Based ProSyndromes
Variable
WHO category RA, RARS,deletion
Karyotype* GoodSevere anemia (Hb �9 g/dL in males
or �8 g/dL in females)Absent
WPSS Risk Group
Very lowLowIntermediateHighVery highNOTE. The original criterion of transfusion requirement20 has no
or �8 g/dL in females). This latter definition is based on a re*Good: normal, del(5q) only, del(20q) only, –Y only; Poor: very
other abnormalities.
Table 5. M.D. Anderson Prognostic Scoring Syst
Variable 1
Performance statusAge, yr 60–64Platelet, x 109/L 50–199Hemoglobin, g/dLBone marrow blasts, % 5–10WBC, x 109/LKaryotype
Prior transfusion Yes
MPSS Risk Group
LowIntermediate 1Intermediate 2High
MDS-CI considerably improves risk stratification inMDS, particularly in the lower risk groups according todisease-related criteria.
More recently, Naqvi et al28 reported on the effectof comorbidities on the survival of 600 consecutivepatients with MDS followed at the M.D. AndersonCancer Center. They used the Adult ComorbidityEvaluation-27 (ACE-27), an instrument specificallydesigned for patients with cancer,29 to measure the
ic Scoring System (WPSS) of Myelodysplastic
Points
1 2 3
ith isolated RCMD RAEB-1 RAEB-2
Intermediate Poor —Present — —
Score
012
3–45–6
eplaced by severe anemia (hemoglobine [Hb] �9 g/dL in malesy on prognostic significance of the degree of anemia.21
x (�2) abnormalities, chromosome 7 anomalies; Intermediate:
PSS) of Myelodysplastic Syndromes22
Points
2 3
�2�65
30–49 �30�12
11–29�20
chromosome 7 abnormality orcomplex � 2 abnormalities
Score
0–45–67–8� 9
gnost
0
MDS w(5q)
w been rcent stud
comple
em (M

darbtia
632 M. Cazzola et al
severity of comorbidities, and found that 35% of MDSpatients had moderate to severe comorbid condi-tions.28 In particular, 55% of MDS patients had a
isease of the cardiovascular system, and this wasssociated with worse survival. Median survivalanged from 32 months in patients with no comor-idity to 10 months in those with severe comorbidi-ies. Of note, these latter subjects had a 50% decreasen overall survival, which was independent of agend IPSS risk group. Finally, Naqvi et al28 built up a
prognostic model based on age, IPSS score, andACE-27 score. This model identified three risk
Table 6. Advantages and Limitations of CurrenPatients
Risk Model In Favor (pros)
IPSS The presence of three variables makes it easyto use in clinical practice.
Largely utilized in the last 12 years for riskassessment both in clinical practice andclinical trials.
Adopted by the Food and DrugAdministration (FDA) and the EuropeanMedicines Agency (EMA) for approval ofnovel drugs for treatment of MDS(azacitidine, decitabine and lenalidomide).
WPSS The presence of three variables makes it easyto use in clinical practice.
This scoring system is able to classify patientinto five risk groups showing differentsurvivals and probabilities of leukemicevolution.
It predicts survival and leukemia progression aany time during follow-up. WPSS maytherefore be used for implementing risk-adapted treatment strategies and forstratifying patients enrolled in clinical trials.
WPSS have a relevant prognostic value inpost-transplantation outcome of MDSpatients.24
MPSS MPSS can be used both in untreated andtreated MDS patients.
MPSS can be used for risk assessment inCMML and in therapy-related MDS.However, this latter condition has almostalways an unfavorable outcome.
groups, whose median survivals were 43 months
(low risk), 23 months (intermediate risk), and 9months (high risk), respectively.
CONCLUSIONS AND PERSPECTIVES
The 2008 WHO classification currently provides thebest diagnostic approach to MDS and has considerableprognostic relevance. For the optimal management ofMDS, its implementation into clinical practice is man-datory.
As far as risk assessment is concerned, the WPSS can
ilable Risk Models for Prognostication in MDS
rguments
Against (cons)
IPSS was derived from a multivariate analysis of hematologicalcharacteristics of 816 patients at clinical onset and thereforeuntreated. It included also individuals with 20–30%marrow blasts (now diagnosed as AML) and patients withchronic myelomonocytic leukemia (now categorized asMDS/ myeloproliferative neoplasms [MPN]).
This scoring system does not consider the severity of anemia,in particular transfusion dependency, which represents oneof the most important negative prognostic factors in MDS.Furthermore, it underestimates the negative impact of poorcytogenetics (especially relative to blast count).
IPSS is inferior to both WPSS23 and MPSS22 in riskstratification of MDS patients.
Finally, a major limitation is lack of applicability to MDSpatients on investigational programs, because most of themwould have had the disease for a significant time andwould have received prior therapies.
This scoring system was developed in patients with primaryMDS, and therefore is not applicable to patients withsecondary MDS. However, the 2008 WHO classification ofmyeloid neoplasms has introduced the unique category oftherapy-related neoplasms,2 which includes therapy-relatedAML, therapy-related MDS and therapy-related MDS/MPN.These conditions are always associated with an unfavorableoutcome, and do not require a specific risk assessment.
Evaluation of multilineage dysplasia requires considerableexpertise, but this is true for many other cytologic andhistologic features regarding tumors of hematopoietic andlymphoid tissues.
The current use of specific hemoglobin thresholds (�9 g/dLin males and �8 g/dL in females) for defining severeanemia has improves the reproducibility of WPSS.
The presence of 8 variables makes it uneasy to use in clinicalpractice.
MPSS ignores the WHO classification, which provides the bestdiagnostic approach to MDS and has considerableprognostic relevance.
The hemoglobin cut-off of 12 g/dL (weight 2 in Table 5)appears to be overestimated compared to the WPSSdefinition of severe anemia (see Table 4).
The bone marrow blast range includes cases classified as AMLaccording to WHO criteria.
tly Ava
A
s
t
be used reliably in all patients with primary MDS, while

1
1
1
1
1
1
1
1
1
1
2
2
Classification of myelodysplastic syndromes 633
the MPSS allows risk assessment also in those withsecondary MDS and in patients with CMML.
Since comorbidities have a significant impact on theoutcome of patients with MDS, accounting for bothdisease status and comorbid conditions considerablyimproves risk stratification. Both the MDS-CI27 and theACE-2729 can be employed for assessing the severity ofcomorbidities in MDS patients.
In perspective, the available evidence indicatesthat advances in our ability to improve diagnosis andprognostication of MDS likely will be made possibleby a better understanding of the molecular basis ofthese myeloid neoplasms. A very recent work stud-ied the clinical impact of point mutations in a cohortof 439 patients with MDS.30 Somatic mutations ofTP53, EZH2, ETV6, RUNX1, and ASXL1 were foundto be independent predictors of decreased survivaland to improve the risk stratification provided by theIPSS. These observations suggest that incorporationof somatic mutations may add relevant informationto the risk stratification systems currently used inclinical practice.
REFERENCES1. Cazzola M, Malcovati L. Myelodysplastic syndromes—
coping with ineffective hematopoiesis. N Engl J Med.2005;352:536–8.
2. Swerdlow SH, Campo E, Harris NL, et al. WHO classifi-cation of tumours of haematopoietic and lymphoid tis-sues. Lyon: IARC; 2008.
3. Malcovati L, Cazzola M. Myelodysplastic/myeloprolifera-tive disorders. Haematologica. 2008;93:4–6.
4. Reiter A, Invernizzi R, Cross NC, Cazzola M. Molecularbasis of myelodysplastic/myeloproliferative neoplasms.Haematologica. 2009;94:1634–8.
5. Tefferi A, Vardiman JW. Myelodysplastic syndromes.N Engl J Med. 2009;361:1872–85.
6. Mufti GJ, Bennett JM, Goasguen J, et al. Diagnosis and
Figure 3. Relationship between MDS-specific comorbidityindex (MDS-CI) and overall survival in MDS patients. Re-produced from Della Porta et al with permission.27
classification of myelodysplastic syndrome: International
Working Group on Morphology of myelodysplasticsyndrome (IWGM-MDS) consensus proposals for thedefinition and enumeration of myeloblasts and ringsideroblasts. Haematologica. 2008;93:1712–7.
7. Haase D, Germing U, Schanz J, et al. New insights intothe prognostic impact of the karyotype in MDS andcorrelation with subtypes: evidence from a core datasetof 2124 patients. Blood. 2007;110:4385–95.
8. Della Porta MG, Malcovati L, Invernizzi R, et al. Flowcytometry evaluation of erythroid dysplasia in patientswith myelodysplastic syndrome. Leukemia. 2006;20:549 –55.
9. Ogata K, Della Porta MG, Malcovati L, et al. Diagnosticutility of flow cytometry in low-grade myelodysplasticsyndromes: a prospective validation study. Haemato-logica. 2009;94:1066–74.
0. van de Loosdrecht AA, Alhan C, Bene MC, et al. Standard-ization of flow cytometry in myelodysplastic syndromes:report from the first European LeukemiaNet working con-ference on flow cytometry in myelodysplastic syndromes.Haematologica. 2009;94:1124–34.
1. Della Porta MG, Malcovati L, Boveri E, et al. Clinicalrelevance of bone marrow fibrosis and CD34-positivecell clusters in primary myelodysplastic syndromes.J Clin Oncol. 2009;27:754 – 62.
2. Bennett JM, Orazi A. Diagnostic criteria to distinguishhypocellular acute myeloid leukemia from hypocellularmyelodysplastic syndromes and aplastic anemia: recom-mendations for a standardized approach. Haematologica.2009;94:264–8.
3. Bennett JM, Catovsky D, Daniel MT, et al. Proposals forthe classification of the myelodysplastic syndromes. Br JHaematol. 1982;51:189–99.
4. Cazzola M. Risk assessment in myelodysplastic syn-dromes and myelodysplastic/myeloproliferative neo-plasms. Haematologica. 2011;96:349–52.
5. Vardiman JW, Harris NL, Brunning RD. The World HealthOrganization (WHO) classification of the myeloid neo-plasms. Blood. 2002;100:2292–302.
6. Brunning RD, Orazi A, Germing U, et al. Myelodysplasticsyndromes/neoplasms, overview. In: Swerdlow SH,Campo E, Harris NL, et al eds. WHO classification oftumours of haematopoietic and lymphoid tissues. Lyon:IARC; 2008:88–93.
7. Malcovati L, Della Porta M, Pascutto C, et al. Prognosticfactors and life expectancy in myelodysplastic syndromesclassified according to WHO criteria. A basis for clinicaldecision-making. J Clin Oncol. 2005;23:7594–603.
8. Sanz GF, Sanz MA, Greenberg PL. Prognostic factors andscoring systems in myelodysplastic syndromes. Haema-tologica. 1998;83:358–68.
9. Greenberg P, Cox C, LeBeau MM, et al. Internationalscoring system for evaluating prognosis in myelodysplas-tic syndromes. Blood. 1997;89:2079–88.
0. Malcovati L, Germing U, Kuendgen A, et al. Time-depen-dent prognostic scoring system for predicting survivaland leukemic evolution in myelodysplastic syndromes.J Clin Oncol. 2007;25:3503–10.
1. Malcovati L, Della Porta MG, Strupp C, et al. Impact ofthe degree of anemia on the outcome of patients withmyelodysplastic syndrome and its integration into the
WHO classification-based Prognostic Scoring System
634 M. Cazzola et al
(WPSS). Haematologica. 2011 Jun 9. [Epub ahead ofprint].
22. Kantarjian H, O’Brien S, Ravandi F, et al. Proposal fora new risk model in myelodysplastic syndrome thataccounts for events not considered in the originalInternational Prognostic Scoring System. Cancer.2008;113:1351– 61.
23. Cazzola M, Malcovati L. Prognostic classification and riskassessment in myelodysplastic syndromes. Hematol On-col Clin North Am. 2010;24:459–68.
24. Alessandrino EP, Della Porta MG, Bacigalupo A, et al.WHO classification and WPSS predict posttransplanta-tion outcome in patients with myelodysplastic syn-drome: a study from the Gruppo Italiano Trapianto diMidollo Osseo (GITMO). Blood. 2008;112:895–902.
25. Zipperer E, Pelz D, Nachtkamp K, et al. The hemato-poietic stem cell transplantation comorbidity index isof prognostic relevance for patients with myelodys-
plastic syndrome. Haematologica. 2009;94:729 –32.26. Della Porta MG, Malcovati L. Clinical relevance of extra-hematologic comorbidity in the management of patientswith myelodysplastic syndrome. Haematologica. 2009;94:602–6.
27. Della Porta MG, Malcovati L, Strupp C, et al. Risk strati-fication based on both disease status and extra-hemato-logic comorbidities in patients with myelodysplastic syn-drome. Haematologica. 2011;96:441–9.
28. Naqvi K, Garcia-Manero G, Sardesai S, et al. Associationof comorbidities with overall survival in myelodysplasticsyndrome: development of a prognostic model. J ClinOncol. 2011;29:2240–6.
29. Piccirillo JF, Tierney RM, Costas I, Grove L, Spitznagel EL,Jr. Prognostic importance of comorbidity in a hospital-based cancer registry. JAMA. 2004;291:2441–7.
30. Bejar R, Stevenson K, Abdel-Wahab O, et al. Clinical effectof point mutations in myelodysplastic syndromes. N Engl
J Med. 2011;364:2496–506.