-
8/14/2019 CLAIRE GANTUANGCO01
1/13
CLAIRE GANTUANGCO 01-22-10
BSN-4C FPC MRS. ARENDAIN, RN,RM, MAN
Development
Main article: Prenatal development
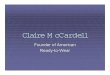
9 weeks of gestation: condition at start of fetal stage
Artist's depiction of fetus 11 weeks after fertilization. The
crown-rump length is 1.25
inches.[7]
The fetal stage commences at the beginning of the 9th week.[1]
At the start of the fetal
stage, the fetus is typically about 30 mm (1.2 inches) in length
from crown to rump, and
weighs about 8 grams.[1]The head makes up nearly half of the
fetus' size.[8] Breathing-like
movement of the fetus is necessary for stimulation of lung
development, rather than for
obtaining oxygen.[9]
The heart, hands, feet, brain and other organs are present, but
are onlyat the beginning of development and have minimal
operation.[10][11]
Fetuses are not capable of feeling pain at the beginning of the
fetal stage, and will not beable to feel pain until the third
trimester.[12] At this point in development, uncontrolled
movements and twitches occur as muscles, the brain and pathways
begin to develop.[13]
16 to 25 weeks after fertilization
A woman pregnant for the first time (i.e. a primiparous woman)
typically feels fetal
movements at about 21 weeks, whereas a woman who has already
given birth at least two
times (i.e. a multiparous woman) will typically feel movements
by 20 weeks.[14]
By theend of the fifth month, the fetus is about 20 cm (8
inches).
26 to 40 weeks of gestation
Artist's depiction of fetus at 40 weeks after fertilization,
about 20 inches (51 cm) head to
toe.
The amount of body fat rapidly increases. Lungs are not fully
mature. Thalamic brainconnections, which mediate sensory input,
form. Bones are fully developed, but are still
soft and pliable. Iron, calcium, and phosphorus become more
abundant. Fingernails reach
http://en.wikipedia.org/wiki/Prenatal_developmenthttp://en.wikipedia.org/wiki/Crown-rump_lengthhttp://en.wikipedia.org/wiki/Fetus#cite_note-6http://en.wikipedia.org/wiki/Fetus#cite_note-nursing-0http://en.wikipedia.org/wiki/Fetus#cite_note-nursing-0http://en.wikipedia.org/wiki/Fetus#cite_note-nursing-0http://en.wikipedia.org/wiki/Fetus#cite_note-itrfps-7http://en.wikipedia.org/wiki/Fetus#cite_note-8http://en.wikipedia.org/wiki/Fetus#cite_note-Columbia-9http://en.wikipedia.org/wiki/Fetus#cite_note-Columbia-9http://en.wikipedia.org/wiki/Fetus#cite_note-10http://en.wikipedia.org/wiki/Fetus#cite_note-JAMA-11http://en.wikipedia.org/wiki/Fetus#cite_note-Prechtl-12http://en.wikipedia.org/wiki/Fetus#cite_note-13http://en.wikipedia.org/wiki/Thalamushttp://en.wikipedia.org/wiki/Ironhttp://en.wikipedia.org/wiki/Calciumhttp://en.wikipedia.org/wiki/Phosphorushttp://en.wikipedia.org/wiki/File:40_weeks_pregnant.jpghttp://en.wikipedia.org/wiki/File:40_weeks_pregnant.jpghttp://en.wikipedia.org/wiki/File:10_weeks_pregnant.jpghttp://en.wikipedia.org/wiki/File:10_weeks_pregnant.jpghttp://en.wikipedia.org/wiki/Prenatal_developmenthttp://en.wikipedia.org/wiki/Crown-rump_lengthhttp://en.wikipedia.org/wiki/Fetus#cite_note-6http://en.wikipedia.org/wiki/Fetus#cite_note-nursing-0http://en.wikipedia.org/wiki/Fetus#cite_note-nursing-0http://en.wikipedia.org/wiki/Fetus#cite_note-itrfps-7http://en.wikipedia.org/wiki/Fetus#cite_note-8http://en.wikipedia.org/wiki/Fetus#cite_note-Columbia-9http://en.wikipedia.org/wiki/Fetus#cite_note-10http://en.wikipedia.org/wiki/Fetus#cite_note-JAMA-11http://en.wikipedia.org/wiki/Fetus#cite_note-Prechtl-12http://en.wikipedia.org/wiki/Fetus#cite_note-13http://en.wikipedia.org/wiki/Thalamushttp://en.wikipedia.org/wiki/Ironhttp://en.wikipedia.org/wiki/Calciumhttp://en.wikipedia.org/wiki/Phosphorus
-
8/14/2019 CLAIRE GANTUANGCO01
2/13
the end of the fingertips. The lanugo begins to disappear, until
it is gone except on the
upper arms and shoulders. Small breast buds are present on both
sexes. Head hair
becomes coarse and thicker. Birth is imminent and occurs around
the 40th week. Thefetus is considered full-term between weeks 35
and 40, [15] which means that the fetus is
considered sufficiently developed for life outside the
uterus.[16] It may be 48 to 53 cm (19
to 21 inches) in length, when born. Control of movement is
limited at birth, andpurposeful voluntary movements develop all the
way until puberty.[17][18]
Variation in growth
See also: Birth weight
There is much variation in the growth of the fetus. When fetal
size is less than expected,
that condition is known as intrauterine growth restriction
(IUGR) also called fetal growth
restriction (FGR); factors affecting fetal growth can be
maternal,placental, orfetal.[19]
Maternal factors include maternal weight, body mass index,
nutritional state, emotionalstress, toxin exposure (including
tobacco, alcohol, heroin, and other drugs which can also
harm the fetus in other ways), and uterineblood flow.
Placental factors include size, microstructure (densities and
architecture), umbilicalblood flow, transporters and binding
proteins, nutrient utilization and nutrient production.
Fetal factors include the fetus genome, nutrient production, and
hormone output. Also,
female fetuses tend to weigh less than males, at full
term.[19]
Fetal growth is often classified as follows: small for
gestational age (SGA), appropriate
for gestational age (AGA), and large for gestational age
(LGA).[20]
SGA can result in lowbirth weight, although premature birth can
also result in low birth weight. Low birth
weight increases risk for perinatal mortality (death shortly
after birth), asphyxia,
hypothermia, polycythemia, hypocalcemia, immune dysfunction,
neurologicabnormalities, and other long-term health problems. SGA
may be associated with growth
delay, or it may instead be associated with absolute stunting of
growth.
Viability
Main article: Viability (fetal)
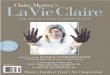
Stages inprenatal development, showing viability and point of
50% chance of survival at
bottom. Weeks and months numberedby gestation.
The lower limit of viability is approximately five months
gestational age, and usually
later.[21]
http://en.wikipedia.org/wiki/Breast_budhttp://en.wikipedia.org/wiki/Fetus#cite_note-14http://en.wikipedia.org/wiki/Fetus#cite_note-15http://en.wikipedia.org/wiki/Fetus#cite_note-16http://en.wikipedia.org/wiki/Fetus#cite_note-Becher-17http://en.wikipedia.org/wiki/Birth_weighthttp://en.wikipedia.org/wiki/Placentahttp://en.wikipedia.org/wiki/Fetus#cite_note-Holden-18http://en.wikipedia.org/wiki/Weighthttp://en.wikipedia.org/wiki/Body_mass_indexhttp://en.wikipedia.org/wiki/Stress_(medicine)http://en.wikipedia.org/wiki/Tobaccohttp://en.wikipedia.org/wiki/Alcoholhttp://en.wikipedia.org/wiki/Heroinhttp://en.wikipedia.org/wiki/Uterushttp://en.wikipedia.org/wiki/Bloodhttp://en.wikipedia.org/wiki/Umbilical_cordhttp://en.wikipedia.org/wiki/Hormonehttp://en.wikipedia.org/wiki/Fetus#cite_note-Holden-18http://en.wikipedia.org/wiki/Fetus#cite_note-19http://en.wikipedia.org/wiki/Deathhttp://en.wikipedia.org/wiki/Asphyxiahttp://en.wikipedia.org/wiki/Hypothermiahttp://en.wikipedia.org/wiki/Polycythemiahttp://en.wikipedia.org/wiki/Hypocalcemiahttp://en.wikipedia.org/wiki/Immune_dysfunctionhttp://en.wikipedia.org/wiki/Neurologichttp://en.wikipedia.org/wiki/Viability_(fetal)http://en.wikipedia.org/wiki/Prenatal_developmenthttp://en.wikipedia.org/wiki/Gestational_agehttp://en.wikipedia.org/wiki/Viabilityhttp://en.wikipedia.org/wiki/Gestational_agehttp://en.wikipedia.org/wiki/Fetus#cite_note-20http://en.wikipedia.org/wiki/File:Prenatal_development_table.svghttp://en.wikipedia.org/wiki/File:Prenatal_development_table.svghttp://en.wikipedia.org/wiki/Breast_budhttp://en.wikipedia.org/wiki/Fetus#cite_note-14http://en.wikipedia.org/wiki/Fetus#cite_note-15http://en.wikipedia.org/wiki/Fetus#cite_note-16http://en.wikipedia.org/wiki/Fetus#cite_note-Becher-17http://en.wikipedia.org/wiki/Birth_weighthttp://en.wikipedia.org/wiki/Placentahttp://en.wikipedia.org/wiki/Fetus#cite_note-Holden-18http://en.wikipedia.org/wiki/Weighthttp://en.wikipedia.org/wiki/Body_mass_indexhttp://en.wikipedia.org/wiki/Stress_(medicine)http://en.wikipedia.org/wiki/Tobaccohttp://en.wikipedia.org/wiki/Alcoholhttp://en.wikipedia.org/wiki/Heroinhttp://en.wikipedia.org/wiki/Uterushttp://en.wikipedia.org/wiki/Bloodhttp://en.wikipedia.org/wiki/Umbilical_cordhttp://en.wikipedia.org/wiki/Hormonehttp://en.wikipedia.org/wiki/Fetus#cite_note-Holden-18http://en.wikipedia.org/wiki/Fetus#cite_note-19http://en.wikipedia.org/wiki/Deathhttp://en.wikipedia.org/wiki/Asphyxiahttp://en.wikipedia.org/wiki/Hypothermiahttp://en.wikipedia.org/wiki/Polycythemiahttp://en.wikipedia.org/wiki/Hypocalcemiahttp://en.wikipedia.org/wiki/Immune_dysfunctionhttp://en.wikipedia.org/wiki/Neurologichttp://en.wikipedia.org/wiki/Viability_(fetal)http://en.wikipedia.org/wiki/Prenatal_developmenthttp://en.wikipedia.org/wiki/Gestational_agehttp://en.wikipedia.org/wiki/Viabilityhttp://en.wikipedia.org/wiki/Gestational_agehttp://en.wikipedia.org/wiki/Fetus#cite_note-20
-
8/14/2019 CLAIRE GANTUANGCO01
3/13
Human fetus, age unknown
There is no sharp limit of development, age, or weight at which
a fetus automaticallybecomes viable.[22] According to data years
2003-2005, 20 to 35 percent of babies born at
23 weeks of gestation survive, while 50 to 70 percent of babies
born at 24 to 25 weeks,
and more than 90 percent born at 26 to 27 weeks, survive. [23]
It is rare for a baby
weighing less than 500 gm to survive.[22]
When such babies are born, the main causes ofperinatal mortality
is that the respiratory
system and the central nervous system are not completely
differentiated.[22] If given
expert postnatal care, some fetuses weighing less than 500 gm
may survive, being arereferred to as extremely low birth
weightorimmature infants.[22]Preterm birth is the most
common cause of perinatal mortality, causing almost 30 percent
of neonatal deaths.[24]
Fetal pain
Main article: Fetal pain
Fetal pain, its existence, and its implications are debated
politically and academically.According to the conclusions of a
review published in 2005, "Evidence regarding the
capacity for fetal pain is limited but indicates that fetal
perception of pain is unlikely
before the third trimester."[12][25]However, there may be an
emerging consensus among
developmental neurobiologists that the establishment
ofthalamocortical connections" (atabout 26 weeks) is a critical
event with regard to fetal perception of pain. [26]
Nevertheless,
because pain can involve sensory, emotional and cognitive
factors, it is "impossible to
know" when painful experiences may become possible, even if it
is known whenthalamocortical connections are established.[26]
Whether a fetus has the ability to feel pain and to sufferis
part of the abortion debate.[27]
[28] For example, in the USA legislation has been proposed by
pro-life advocates thatabortion providers should be required to
tell a woman that the fetus may feel pain during
the abortion procedure, and require her to accept or decline
anesthesia for the fetus.[29]
http://en.wikipedia.org/wiki/Fetus#cite_note-developinghuman-21http://en.wikipedia.org/wiki/Fetus#cite_note-developinghuman-21http://en.wikipedia.org/wiki/Weeks_of_gestationhttp://en.wikipedia.org/wiki/Fetus#cite_note-22http://en.wikipedia.org/wiki/Fetus#cite_note-developinghuman-21http://en.wikipedia.org/wiki/Perinatal_mortalityhttp://en.wikipedia.org/wiki/Fetus#cite_note-developinghuman-21http://en.wikipedia.org/wiki/Fetus#cite_note-developinghuman-21http://en.wikipedia.org/wiki/Fetus#cite_note-developinghuman-21http://en.wikipedia.org/wiki/Preterm_birthhttp://en.wikipedia.org/wiki/Fetus#cite_note-23http://en.wikipedia.org/wiki/Fetal_painhttp://en.wikipedia.org/wiki/Fetus#cite_note-JAMA-11http://en.wikipedia.org/wiki/Fetus#cite_note-sskqke-24http://en.wikipedia.org/wiki/Fetus#cite_note-sskqke-24http://en.wikipedia.org/wiki/Neurobiologyhttp://en.wikipedia.org/wiki/Human_thalamushttp://en.wikipedia.org/wiki/Fetus#cite_note-Johnson-25http://en.wikipedia.org/wiki/Fetus#cite_note-Johnson-25http://en.wikipedia.org/wiki/Painhttp://en.wikipedia.org/wiki/Sufferinghttp://en.wikipedia.org/wiki/Abortion_debatehttp://en.wikipedia.org/wiki/Fetus#cite_note-26http://en.wikipedia.org/wiki/Fetus#cite_note-26http://en.wikipedia.org/wiki/Fetus#cite_note-27http://en.wikipedia.org/wiki/Pro-lifehttp://en.wikipedia.org/wiki/Fetus#cite_note-28http://en.wikipedia.org/wiki/File:Human_Fetus.jpghttp://en.wikipedia.org/wiki/File:Human_Fetus.jpghttp://en.wikipedia.org/wiki/Fetus#cite_note-developinghuman-21http://en.wikipedia.org/wiki/Weeks_of_gestationhttp://en.wikipedia.org/wiki/Fetus#cite_note-22http://en.wikipedia.org/wiki/Fetus#cite_note-developinghuman-21http://en.wikipedia.org/wiki/Perinatal_mortalityhttp://en.wikipedia.org/wiki/Fetus#cite_note-developinghuman-21http://en.wikipedia.org/wiki/Fetus#cite_note-developinghuman-21http://en.wikipedia.org/wiki/Preterm_birthhttp://en.wikipedia.org/wiki/Fetus#cite_note-23http://en.wikipedia.org/wiki/Fetal_painhttp://en.wikipedia.org/wiki/Fetus#cite_note-JAMA-11http://en.wikipedia.org/wiki/Fetus#cite_note-sskqke-24http://en.wikipedia.org/wiki/Neurobiologyhttp://en.wikipedia.org/wiki/Human_thalamushttp://en.wikipedia.org/wiki/Fetus#cite_note-Johnson-25http://en.wikipedia.org/wiki/Fetus#cite_note-Johnson-25http://en.wikipedia.org/wiki/Painhttp://en.wikipedia.org/wiki/Sufferinghttp://en.wikipedia.org/wiki/Abortion_debatehttp://en.wikipedia.org/wiki/Fetus#cite_note-26http://en.wikipedia.org/wiki/Fetus#cite_note-27http://en.wikipedia.org/wiki/Pro-lifehttp://en.wikipedia.org/wiki/Fetus#cite_note-28
-
8/14/2019 CLAIRE GANTUANGCO01
4/13
Circulatory system
Main article: Fetal circulation
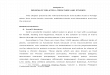
Diagram of the human fetal circulatory system.
The circulatory system of a human fetus works differently from
that of born humans,
mainly because the lungs are not in use: the fetus obtains
oxygen and nutrients from the
woman through theplacenta and the umbilical cord.[30]
Blood from the placenta is carried to the fetus by the umbilical
vein. About half of thisenters the fetal ductus venosus and is
carried to the inferior vena cava, while the other
half enters the liver proper from the inferior border of the
liver. The branch of the
umbilical vein that supplies the right lobe of the liver first
joins with the portal vein. Theblood then moves to the right atrium
of the heart. In the fetus, there is an opening
between the right and left atrium (theforamen ovale), and most
of the blood flows from
the right into the left atrium, thus bypassingpulmonary
circulation. The majority of bloodflow is into the left ventricle
from where it is pumped through the aorta into the body.
Some of the blood moves from the aorta through the internal
iliac arteries to the umbilical
arteries, and re-enters the placenta, where carbon dioxide and
other waste products fromthe fetus are taken up and enter the
woman's circulation.[30]
Some of the blood from the right atrium does not enter the left
atrium, but enters the right
ventricle and is pumped into the pulmonary artery. In the fetus,
there is a special
connection between the pulmonary artery and the aorta, called
the ductus arteriosus,
which directs most of this blood away from the lungs (which
aren't being used forrespiration at this point as the fetus is
suspended in amniotic fluid).[30]
Postnatal development
Main article: Adaptation to extrauterine life
With the first breath after birth, the system changes suddenly.
The pulmonary resistance
is dramatically reduced ("pulmo" is from the Latin for "lung").
More blood moves from
the right atrium to the right ventricle and into the pulmonary
arteries, and less flowsthrough theforamen ovale to the left
atrium. The blood from the lungs travels through the
pulmonary veins to the left atrium, increasing the pressure
there. The decreased right
http://en.wikipedia.org/wiki/Fetal_circulationhttp://en.wikipedia.org/wiki/Fetal_circulatory_systemhttp://en.wikipedia.org/wiki/Circulatory_systemhttp://en.wikipedia.org/wiki/Oxygenhttp://en.wikipedia.org/wiki/Placentahttp://en.wikipedia.org/wiki/Umbilical_cordhttp://en.wikipedia.org/wiki/Fetus#cite_note-Whitaker-29http://en.wikipedia.org/wiki/Umbilical_veinhttp://en.wikipedia.org/wiki/Ductus_venosushttp://en.wikipedia.org/wiki/Inferior_vena_cavahttp://en.wikipedia.org/wiki/Liverhttp://en.wikipedia.org/wiki/Portal_veinhttp://en.wikipedia.org/wiki/Hearthttp://en.wikipedia.org/wiki/Foramen_ovale_(heart)http://en.wikipedia.org/wiki/Foramen_ovale_(heart)http://en.wikipedia.org/wiki/Pulmonary_circulationhttp://en.wikipedia.org/wiki/Aortahttp://en.wikipedia.org/wiki/Carbon_dioxidehttp://en.wikipedia.org/wiki/Fetus#cite_note-Whitaker-29http://en.wikipedia.org/wiki/Pulmonary_arteryhttp://en.wikipedia.org/wiki/Ductus_arteriosushttp://en.wikipedia.org/wiki/Ductus_arteriosushttp://en.wikipedia.org/wiki/Amniotic_fluidhttp://en.wikipedia.org/wiki/Fetus#cite_note-Whitaker-29http://en.wikipedia.org/wiki/Adaptation_to_extrauterine_lifehttp://en.wikipedia.org/wiki/Lunghttp://en.wikipedia.org/wiki/Foramen_ovale_(heart)http://en.wikipedia.org/wiki/File:Fetal_circulation.pnghttp://en.wikipedia.org/wiki/File:Fetal_circulation.pnghttp://en.wikipedia.org/wiki/Fetal_circulationhttp://en.wikipedia.org/wiki/Fetal_circulatory_systemhttp://en.wikipedia.org/wiki/Circulatory_systemhttp://en.wikipedia.org/wiki/Oxygenhttp://en.wikipedia.org/wiki/Placentahttp://en.wikipedia.org/wiki/Umbilical_cordhttp://en.wikipedia.org/wiki/Fetus#cite_note-Whitaker-29http://en.wikipedia.org/wiki/Umbilical_veinhttp://en.wikipedia.org/wiki/Ductus_venosushttp://en.wikipedia.org/wiki/Inferior_vena_cavahttp://en.wikipedia.org/wiki/Liverhttp://en.wikipedia.org/wiki/Portal_veinhttp://en.wikipedia.org/wiki/Hearthttp://en.wikipedia.org/wiki/Foramen_ovale_(heart)http://en.wikipedia.org/wiki/Pulmonary_circulationhttp://en.wikipedia.org/wiki/Aortahttp://en.wikipedia.org/wiki/Carbon_dioxidehttp://en.wikipedia.org/wiki/Fetus#cite_note-Whitaker-29http://en.wikipedia.org/wiki/Pulmonary_arteryhttp://en.wikipedia.org/wiki/Ductus_arteriosushttp://en.wikipedia.org/wiki/Amniotic_fluidhttp://en.wikipedia.org/wiki/Fetus#cite_note-Whitaker-29http://en.wikipedia.org/wiki/Adaptation_to_extrauterine_lifehttp://en.wikipedia.org/wiki/Lunghttp://en.wikipedia.org/wiki/Foramen_ovale_(heart)
-
8/14/2019 CLAIRE GANTUANGCO01
5/13
atrial pressure and the increased left atrial pressure pushes
the septum primum against theseptum secundum, closing theforamen
ovale, which now becomes thefossa ovalis. This
completes the separation of the circulatory system into two
halves, the left and the right.
The ductus arteriosus normally closes off within one or two days
of birth, leaving behind
the ligamentum arteriosum. The umbilical vein and the ductus
venosus closes off withintwo to five days after birth, leaving
behind the ligamentum teres and the ligamentum
venosus of the liver respectively.
http://en.wikipedia.org/wiki/Ligamentum_tereshttp://en.wikipedia.org/wiki/Ligamentum_venosushttp://en.wikipedia.org/wiki/Ligamentum_venosushttp://en.wikipedia.org/wiki/Ligamentum_tereshttp://en.wikipedia.org/wiki/Ligamentum_venosushttp://en.wikipedia.org/wiki/Ligamentum_venosus
-
8/14/2019 CLAIRE GANTUANGCO01
6/13
There's a lot more to getting pregnantthan just having
intercourse sometime in the middle of yourcycle and hoping to see
that positive pregnancy test insteadof your period.
I learned this the hard way.
When I was trying to conceive, I found out that there was alot
that I didn't know. Which led me to making a lot of bigmistakes
which were actually preventing me from gettingpregnant.
For one thing, I had the timing all wrong. I thought Iovulated
14 days after the start of my period, but laterlearned that this is
a big mistake that many women make.For most women, ovulation does
not occur 14 days aftertheir period starts even though many women
think this istrue. That's because most women do not have a perfect
28day cycle.
And would you believe I was using lubrication that I laterfound
out can kill sperm!! That certainly wasn't helping meto get
pregnant, was it?
I also had my husband "save up" his sperm thinking thiswould
make him more fertile when my ovulation day came,and it turns out
this actually makes him less fertile, andreduces the chance of
pregnancy. Who knew??
Avoid Common Mistakes!Oh, I could go on and on about all the
mistakes I wasmaking.
Luckily, after spending months researching, I uncoveredmany
possible mistakes which can get in the
-
8/14/2019 CLAIRE GANTUANGCO01
7/13
way of getting pregnant, and I made a lot of changes basedon
what I learned.
And guess what, I conceived my two little "bundles of joy"
(not at the same time!) soon after I madesome changes!
I wrote a little report to inform other women about thecommon
mistakes I discovered which willreduce your chances of getting
pregnant. I bet you'll besurprised to find that you're making
atleast a few yourself!!
You can get your free copy of the "7 Mistakes Report" byclicking
here. Consider it my gift to you...
I sincerely hope it helps you have your own
little "bundle of joy."
Baby dust to you...
--Beth
http://www.personalpathtopregnancy.net/7MistakesReport.htmlhttp://www.personalpathtopregnancy.net/7MistakesReport.html
-
8/14/2019 CLAIRE GANTUANGCO01
8/13
GINA G. DALUMPINES 01-23-10
BSN-4C FPC MRS. ARENDAIN,RN, RM,MAN
OBSTETRICS & GYNECOLOGY
Maternal Physiology Changes During Pregnancy
The physiologic,biochemical,and anatomic changes that occur
during pregnancy areextensive and may be sistemic or
local..Teleologic alterations during pregnancy mantaina
healthy enviroment for the fetus without compromising the mother
shealth.Although,sometimes determine small disconfort to the
mother.
Gastrointestinal Tract
During pregnancy, nutritional requirements,including those for
vitamins and minerals, areincreased, and several maternal
alterations occur to meet this demand.The mother`s
appetite usually increases, so that food intake is greather,
some women have a decreased
appetite or experience nausea and vomiting.These symptoms may be
related to relative
levels of human chorionic gonadotrophin(hCG).
Oral Cavity
Salivation may seem to increase due to swallowing difficulty
associated with nausea
,and ,if the pH of the oral cavity decreases, tooth decay may
occur.Tooth decay duringpregnancy,however, is not due to lack of
calcium in the teeth.Indeed,dentalcalciumis
stable and not mobilized during pregnacy as is bone calcium.
The gums may become hipertrofic, hiperemic and friable;this
maybe due to increased
systemic estrogen. Vitamin Cdeficiency also can cause tenderness
and bleeding of the
gums.The gums shoud return tonormal in the early puerperium
Gastointestinal Motility
Gastrointestinal motility may be reduced during pregnancy due to
increased levels of
progesterone, which in turn decrease the production of motilin,
ahormonal peptide that is
known to stimulate smooth muscle in the gut.Transit time of food
throughout thegastrointestinal tract may be so much slower that
more water than normal is reabsorbed,
leading to constipation.
Stomach and Esophagus
Gastric production of hidrocloric acid is variable and sometimes
exaggrated, especiallyduring the first trimester. More commonly,
gastric acidity is reduced. Production of the
hormone gastin increases significantly, resulting in increased
sthomac volume and
decreased stomach pH. Gastric production of mucus may be
increased. Esophagealperistalses is deceased, accompanid by gastric
reflux because of the slower emptying
time and dilatation or relaxation of the cardiac sphincter.
Gastric reflux is more prvalent
in later pregnancy owing to elevation of the stomach by the
enlarged uterus.Besides
http://www.medstudents.com.br/gastro/gastro4.htmhttp://www.medstudents.com.br/gastro/gastro4.htm
-
8/14/2019 CLAIRE GANTUANGCO01
9/13
leading to heartburn, all of these alterations as well as lying
in the supine lithotomy
position, make the use of anesthesia more hazardous because of
the increased possibility
of regurgitation and aspiration.
Small and Large Bowel ann Appendix
The large and small bowel move upward and laterally,the appendix
is displaced
superiorly in the right flank area. These organs return to the
normal positions in the early
puerperium.
As noted previouly, motility is generally decreased an
gastrointestinal tone is decreased.
Gallblader
Gallblader function is also altered during pregnancy because of
the hypotonia of the
smooth muscle wall. Emptying time is slowed and often
incomplete. Bile can become
thick, and bile stasis may lead to gallstone formation.
Liver
There are no apparent morphologic changes in the liver during
normal pregnancy, but
there are functional alterations. Serum alkaline phosphatase
activity can double, probably
because of inceased placental alkaline phosphatase isoenzimes.
Thus, a decrease in the
albumin/globulin ratio occurs normally in pregnancy.
Kidneys and Urinary Tract
Renal Dilatation
During pregnancy , each kidney increases in leagth by 1-1,5cm,
with a concomitant
increase in weight.The renal pelvis is dilated.The ureters are
dilated above the brim of the
bony pelvis.The ureters also elongate, widen, and become more
curved.Thus there is anincrease in urinary stasis, this may lead to
infection and may make tests of renal function
difficult to interprete.
The absolute cause of hydonephrosis and hydroureter in pregnancy
is unknown, theremay be several contributing factors:1-Elevated
progesterone levels may contribute to
hypotonia of the smooth muscle in the ureter. 2-The ovarian vein
complex in the
suspensory ligament of the ovary may enlarge enough to compress
the ureter at the brimof the bony pelvis, thus causing dilatation
above that level. 3-Dextorotation of the uterusduring pregnancy,
may explain why the right ureter is usually more dilated than the
left.
4-Hyperplasia of smooth muscle in distal one-third of the ureter
may cause reduction in
the luminal size. Renal Function
The glomerular filtration rate(GFR) increases during pregnancy
by about 50% .The renalplasma flow rate increases by as much as
25-50%. Urinary flow and sodium excretion
rates in late pregnancy can be alterated by posture, being twice
as great in the lateral
recumbent position as in the supine position.
Even thought the GFR increased dramaticallyduring pregnancy, the
volume of the urinepassed each day is not increased. Thus, the
urinary system appears tobe even more
efficient during pregnancy.
With the increase inGFR, there is an incease in endogenous
clearence of creatinine.Theconcentration of creatinine in serum is
reduced in proportion to increase in GFR, and
concentration of blood urea nitrogen is similarly reduced.
-
8/14/2019 CLAIRE GANTUANGCO01
10/13
Glucosuria during pregnancy is not necessarily abnormal, may be
explained by the
increase in GFR with impairment of tubular reabsortion capacity
for filtered
glucose.Increased levels of urinary glucose also contribute
toincreased susceptibility ofpregnant women to urinary tract
infection.
Proteinuria changes litlle during pregnancy and if more than
500mg/24h is lost,a deseaseprocess shoud be suspected
Levels of the enzime renine, which is produced in kidney,
increase early in the firsttrimester, and continue toarise until
term. This enzime acts on its substrate
angiotensinogen, to first form angiotensin1 and then
angiotensin2, which acts as a
vasoconstrictor.Normal pregnant are resistent to the pressor
effect of elevated levels of
angiotensin2 but those suffering from preeclampsia are not
resistant, this is one of thesome theories to explain this
desease.
Blader As the uterus enlarges, the urinary blader is displaced
upward and flattened in the
anterior-posterior or diameter.Pressure from the uterus leads to
inceased in urinaryfrequency. Blader vascularity increases and
muscle tone decreases, incresin capacity up
to 1500ml.
Hematologic System
Blood Volume `
Perhaps the most striking maternal phisiologic alteration
occurring during pregnancy is
the increase in the blood volume. The magnitude of the increases
varies according to thesize of woman, the number of pregnancies she
has had, the number of infants she has
delivered, and whether there is one or multiple fetuses.The
increases in blood volumeprogress until term;the average increase
in volume at term is 45-50%. The increase is
needed for extra blood flow to the uterus, extra metabolic needs
of fetus, and increased perfusion of others organs, especially
kidneys. Extra volume also compensate for
maternal bllod loss delivery. The average blood loss with
vaginal delivery is 500-600ml,
and with cesarean section is 1000ml.
Red BloodCels The increase in red blood cel mass is about 33%.
Since plasma volume
increases early in pregnancy and faster than red blood cell
volume, the hematocrit falls
until the end of the second trimester, when the increase in the
red blood cells is
synchronized with the plasma volume increase. The hematocrit
then stabilizes or may
increase slightly near term.Iron
With the increase in red blood cells, the need for iron for the
production of
hemoglobin,naturally increases. If supplemental iron is not
added to the diet, irondeficiency anemia will result. Maternal
requiriments can reach 5-6mg/d in the latter half
of pregnancy. If iron is not readly available, the fetus uses
iron from maternal stores.
Thus, the production of fetal hemoglobin is usually adequate
even if the mother is serelyiron deficient. Therefore anemia in the
newborn is rarely a problem; instead, maternal
iron deficiency more commonly may cause preterm labour and late
spontaneus abortion,
incresing the incidence of infant wastage and morbidity.
White Blood Cells
The total blood leukocite count increases during pregnancy from
a prepregnancy level of
4300-4500/mL to 5000-12000/mL in the last trimester, althought
counts as hight as
16000/mL have been observed in the last trimester.Counts as
hight as 25000-30000/mL
have been noted in anormal patient during labor. Lymphocite and
monocyte numbers stay
-
8/14/2019 CLAIRE GANTUANGCO01
11/13
essencially the same throughout pregnancy; polymorphonuclear
leucocytes are the
primary contributors to the increase.
Clotting Factors
During pregnancy, levels of several essential coagulation
factors isincrease.Therearemarked increases in fibrinogen and
factor8. Factors VII, IX, X, and XII also increased but
to alesser extend.
Fibrinolytic activity is depressed during pregnancy and labor,
although the precise
mechanism is unkown. The placenta may be partially responsible
for this alteration infibrinolytic status.Plasminogen levels
increase concomitantly with fibrinogens levels,
causing an equilibrationof clotting and lysing activity.
Clearly, coagolation and fibrinolytic sistems undergo major
alterations during pregnancy.
Understanding these physiologic changes is necessary to manange
two of the more
serious problems of pregnancy: hemorrage and thromboembolic
desease, both caused bydisorders in the mechanism of
hemostasis.
Cardiovascular System
Position and Size of Heart
As the uterus enlarges and the diaphragm becomes elevated, the
heart is displaced
upward and somewhat to the left with rotation on its long axis,
so that the apex beat ismoved laterally. Cardiac capacity increases
by 70-80mL; this may be due to increased
volume or hyperthophy of cardiac muscle.The size of the heart
appears to increase by
about 12%
Cardiac Output
Cardiac output increases approximately 40% during pregnancy,
reaching its maximum at
20-24 weeks gestation and continuing at this level until term.
The increase in output can
be as much as1,5L/min over the non pregnant level. Cardiac
output is very sensitive tochanges in body position. This
sesitivity increases with leghthening gestation,
presumably because the uterus impinges upon the inferior vena
cava, thereby decreasing
blood return to the heart.
Blood Pressure
Systemic blood pressure declines slightly during pregnancy.
There is a little change insystolic blood pressure, but ddiastolic
pressure is reduced (5-10mmHg) from about 12-26
weeks.Diastolic pressure increases thereafter to prepregnancy
levels by about 36 weeks.
The obstruction posed by the uterus on the inferior vena cava
and the pressure of fetalpresentig part on the commom illiac vein
can result in decreased blood return to the heart.
This decreases cardiac output, leads to a fall in blood
pressure, and causes edema in the
lower extremities.
Peripheral Resistence Peripheral resistence equals blood
pressure divided by cardiacoutput. Because blood pressure either
decreases or remain the same during pregnancy and
cardiac output increases appreciably, there is good evidence
that peripheral resistence
declines markedly. The elevated venous pressure returns toward
normal if the woman lies
in the lateral recumbent position.
Effects of the Labor on the Cardiovascular System
-
8/14/2019 CLAIRE GANTUANGCO01
12/13
-
8/14/2019 CLAIRE GANTUANGCO01
13/13