Embed Size (px)
Citation preview

By Patwant Dhillon
CHRONIC KIDNEY DISEASE

• Presence of kidney damage, or a decreased level of kidney function, for a period of 3 months or more
• CKD can be divided into five stages, depending on how severe the damage is to the kidneys, or the level of decrease in kidney function
• There is no cure for kidney disease, but it is possible to prevent or delay the progression of CKD
WHAT IS CKD?
K/DOQI Clinical Practice Guidelines for chronic kidney disease: evaluation, classification and stratification. Am J Kidney Dis 2002; 39 [Supp 1]: S19

• Most diseases of the kidney attack the filtering units of the kidney, and damage their ability to remove wastes and excess fluids.
• 3 most common causes of CKD:
• Diabetes causing diabetic nephropathy
• Hypertension
• Glomerular disease such as glomerular nephritis
WHAT CAUSES CKD?

• Definition and staging depends on assessment of GFR, proteinuria, and other markers of kidney disease
• Estimates of GFR are the best overall indices of level of kidney function
- Equations: MDRD & Cockcroft-Gault
• Serum Creatinine alone should not be used to assess kidney function
• Spot urine samples are commonly used to detect/monitor proteinuria
• Patients with positive dipstick test should undergo confirmation of proteinuria within 3 months
CLINICAL ASSESSMENT OF CKD
K/DOQI Clinical Practice Guidelines for Chronic Kidney Disease: Evaluation, Classification and Stratification. Am J Kidney Dis 39:S1-S266, 2002

• Test of choice: random urine albumin-to-creatinine ratio
• Gold standard: 24-hour urine collection for protein/albumin
• Microalbuminuria: small amounts of albumin excretion, below detection level of urine dipstick
• Overt nephropathy: urinary albumin excretion sufficiently high to be detected
SCREENING FOR ALBUMINURIA
K/DOQI Clinical Practice Guidelines for Chronic Kidney Disease: Evaluation, Classification and Stratification. Am J Kidney Dis 39:S1-S266, 2002

• Common method of estimating renal function in Canada is eGFR using “Modification of Diet in Renal Disease” equation
• Should not be used in situations where kidney function is changing rapidly, such as dehydration
• Because renal function can be transiently depressed, a persistent reduction in eGFR is required before it is considered to be abnormal
ESTIMATION OF GFR
Alternatives to creatinine:
estimated GFR (eGFR) • eGFR is estimated from an equation developed in
studies of patients with significantly impaired renal function (GFR<60 ml/min)
GFR (mL/min/1.73 m2) = 186 x (0.742 if female) x (1.21 if African American)
(Scr)1.154 x (Age)0.203
• Online calculator:
http://www.kidney.org/professionals/kdoqi/gfr_calculator.cfm
K/DOQI Clinical Practice Guidelines for Chronic Kidney Disease: Evaluation, Classification and Stratification. Am J Kidney Dis 39:S1-S266, 2002

• The stage of disease is dependent on how severe the damage is, or the level of decrease in kidney function
• CKD starts slowly and progresses over a number of years
• Not everyone progresses from stage 1 to stage 5
STAGES OF CKD
Tanna, Gemini. Chronic Kidney Disease [unpublished lecture notes]. PHM 202, Leslie Dan Faculty of Pharmacy. Lecture given November 2013.

CURRENT CHRONIC KIDNEY DISEASE (CKD) NOMENCLATUREUSED BY KDIGO
CKD is defined as abnormalities of kidney structure or function, present for 43 months, with implications forhealth and CKD is classified based on cause, GFR category, and albuminuria category (CGA).
Persistent albuminuria categories Description and range
A1 A2 A3
Normal to mildly
increased
Moderately increased
Severely increased
<30 mg/g <3 mg/mmol
30-300 mg/g 3-30 mg/mmol
>300 mg/g >30 mg/mmol
GFR
cat
egor
ies
(ml/m
in/ 1
.73
m2 )
Des
crip
tion
and
rang
e
G1 Normal or high !90
G2 Mildly decreased 60-89
G3a Mildly to moderately decreased 45-59
G3b Moderately to severely decreased 30-44
G4 Severely decreased 15-29
G5 Kidney failure <15
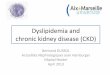
Prognosis of CKD by GFR and Albuminuria Categories:
KDIGO 2012
Prognosis of CKD by GFR and albuminuria category
Green: low risk (if no other markers of kidney disease, no CKD); Yellow: moderately increased risk;Orange: high risk; Red, very high risk.
http://www.kidney-international.org
& 2013 KDIGO
x Kidney International Supplements (2013) 3, x
Kidney International Supplements (2013) 3, xi

As patients progress to Stage 4/5 CKD, electrolyte/mineral abnormalities become common
Symptoms of CKD are often unnoticeable until about 75%
or more of kidney function is lost (stage 4)
SIGNS & SYMPTOMS
Tanna, Gemini. Chronic Kidney Disease [unpublished lecture notes]. PHM 202, Leslie Dan Faculty of Pharmacy. Lecture given November 2013.
Blood Level Normal Range
Hemoglobin 79 g/L 100-120 g/L
Calcium 2.05 mmol/L 2.20-2.60 mmol/L
Phosphate 1.96 mmol/L 0.87-1.52 mmol/L
PTH 68 pmol/L 1.4-7.6 pmol/L
An example of a patient’s blood work

• Cardiovascular
a. CAD
b. Hypertension
• Volume Overload • Bone and mineral metabolism
a. Hypocalcemia
b. Hyperphosphatemia
• Electrolyte abnormalities
a. Hyperkalemia
b. Metabolic acidosis
• Uremia
a. Nausea, vomiting
b. Pruritus • Anemia
CONSEQUENCES
Tanna, Gemini. Chronic Kidney Disease [unpublished lecture notes]. PHM 202, Leslie Dan Faculty of Pharmacy. Lecture given November 2013.

1. Consider using ACE Inhibitor or Angiotensin Receptor Blocker
2. Tight blood pressure control
a. <130/80 mmHg if diabetic
b. <140/90 mmHg if non-diabetic 3. Use of a statin in patients with dyslipidemia
a. High risk on Framingham Risk Score
b. LDL <2 mmol/L
TREATMENT

1. Smoking cessation 2. Avoid nephrotoxic medications
a. NSAIDs
b. COXIBs
c. Intravenous contrast 3. Optimization of glycemic control
a. A1C < 7%
b. Fasting PG 4-7 mmol/L
c. Post-Prandial PG 5-10 mmol/L
TREATMENT

1. Erythropoiesis Stimulating Agent to correct anemia
a. Eprex
b. Aranesp 2. Phosphate Binders to correct phosphate levels
a. Calcium supplementation
b. Sevelamer 3. Vitamin D3 supplementation to correct Parathyroid Hormone
Levels
a. Rocaltrol
TREATMENT

• Hypertension is both a cause and a complication of CKD
• More than 50% to 75% of patients with CKD have blood pressure >140/90 mm Hg
• Hypertension is a risk factor for progression of kidney disease and for CVD
• Blood vessels of the kidney become damaged as a result of high blood pressure
• The damaged blood vessels affect the kidney’s ability to filter
HYPERTENSION
K/DOQI clinical practice guidelines on hypertension and antihypertensive agents in chronic kidney disease. American Journal of Kidney Diseases, Volume 43, Issue null.

• Goals of Therapy:
• Antihypertensive therapy should be used to:
- Lower blood pressure
- Reduce the risk of CVD
- Slow progression of kidney disease
• Blood Pressure Goals:
- Diabetic: < 130/80 mmHg
- Non-Diabetic: < 140/90 mmHg
HYPERTENSION
K/DOQI clinical practice guidelines on hypertension and antihypertensive agents in chronic kidney disease. American Journal of Kidney Diseases, Volume 43, Issue null.

• Antihypertensives should be prescribed as follows:
• Preferred agents for CKD should be used first - ACE Inhibitors and ARBs
• Diuretics should be given to most patients - Daily or PRN use for volume control - Thiazides and Loop diuretics are commonly prescribed
• Choose additional agents based of CVD-specific indications to achieve blood
pressure targets - Non-dihydropyridine CCBs
ANTIHYPERTENSIVES
K/DOQI clinical practice guidelines on hypertension and antihypertensive agents in chronic kidney disease. American Journal of Kidney Diseases, Volume 43, Issue null.

ACE Inhibitors and ARBs:
• Slow progression of diabetic and non-diabetic CKD
• Reduce proteinuria by 35-40%, irrespective of the type of kidney disease
• Lower blood pressure
• Reduce CVD risk
• ACE Inhibitors and ARBs are prescribed for all CKD patients who have:
-Hypertension and/or
-Proteinuria • Monitor the patient for:
- Hypotension
- Decline in GFR
- Hyperkalemia
- Cough
- Angioedema
ACE INHIBITORS & ARBS
K/DOQI clinical practice guidelines on hypertension and antihypertensive agents in chronic kidney disease. American Journal of Kidney Diseases, Volume 43, Issue null.

• If response to ACE I/ARB does not achieve desired blood pressure, a diuretic is usually added as the second agent
• The dose is increased until: - The patient is euvolemic; - Target blood pressure is achieved, or - Adverse effects are noted
• Thiazide diuretics are preferred with GFR ≥30 mL/min
• Loop diuretics are preferred with GFR <30 mL/min, but may need to be given twice daily to achieve the desired natriuresis
• Potassium-sparing diuretics should be avoided in GFR <30 mL/min and in patients taking ACE inhibitors or ARBs
DIURETICS
American Journal of Kidney Diseases, Volume 43, Issue null.

• Patients with Stage 5 CKD, and kidney transplant recipients, on average have a 10-year cumulative risk of coronary heart disease of at least 20%, equivalent to risk in patients with previous CVD
• All adults and adolescents with CKD should be evaluated for dyslipidemias
• Patients with stage 5 CKD and LDL >100 mg/dL (>2.59 mmol/L), treatment should be considered to reduce LDL to <100 mg/dL
DYSLIPIDEMIA
American Journal of Kidney Diseases, Vol 41, No 4, Suppl 3 (April), 2003: pp S39-S58

• Patients with LDL 100-129 mg/dL (2.59-3.34 mmol/L), can attempt dietary changes for 2-3 months before beginning drug treatment
• In patients who cannot reduce LDL to <100 mg/dL by diet and exercise, a statin should be added
• Diet and exercise should be continued as an adjunct to a statin
• Substantial evidence is available stating that statins are safe and effective in reducing LDL in Stage 5 and kidney transplant recipients
DYSLIPIDEMIA
American Journal of Kidney Diseases, Vol 41, No 4, Suppl 3 (April), 2003: pp S39-S58

• Start at low dose and titrate up
• Although evidence is limited, reasonable to assume statins will reduce CHD events and all-cause mortality in CKD patients, similar to general population
• Monitor patient for side effects:
- Elevated hepatic transaminases. Baseline ALT & AST levels, although controversial
- Risk of myopathy increased by CKD. Baseline Creatinine Phosphokinase level. If patient develops muscle pain for tenderness, discontinue stating and measure CK level
STATINS
American Journal of Kidney Diseases, Vol 41, No 4, Suppl 3 (April), 2003: pp S39-S58

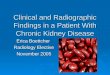
Why recommend smoking cessation
to CKD patients? • Smoking is an independent risk for
development/progression of CKD
Haroun M K et al. JASN 2003;14:2934-2941
Smoker
Non-smoker
Smoking is an independent risk factor for the development/progression of CKD
SMOKING CESSATION

• Erythropoeitin (EPO) produced by the kidneys prevents red blood cell progenitor apoptosis
• EPO is produced by peritublar fibroblasts in response to decrease in oxygen saturation
• Anemia is associated with adverse CV outcomes (LVH, mortality)
• Exogenous EPO (Eprex, Aranesp) is prescribed to correct anemia
ANEMIA
CKD and Anemia • Erythropoeitin (EPO) prevents red blood cell progenitor
apoptosis • EPO is produced by peritubular fibroblasts in response
to decrease in oxygen saturation
↓GFR ↓EPO production anemia
• Anemia is associated with adverse CV outcomes (LVH, mortality)
• Exogenous EPO (Eprex®, Aranesp®) is prescribed to correct anemia
American Journal of Kidney Diseases, Vol 47, No 5, Suppl 3 (May), 2006: pp S54-S57.
Tanna, Gemini. Chronic Kidney Disease [unpublished lecture notes]. PHM 202, Leslie Dan Faculty of Pharmacy. Lecture given November 2013.

• Starting dose:
a. 50-100 units/kg 3 times/week
• Route of administration:
a. IV preferred for patients on dialysis
b. Subcutaneous injection for non-
dialysis patients
• Side effects:
a. Hypertension
b. Headache
c. Nausea, vomiting
• Monitoring:
a. Hemoglobin Level: 100-120 g/L
b. Blood pressure: <130-140/80-90 mmHg
EPREX
e-CPS [Internet]. Ottawa (ON): Canadian Pharmacists Association; c2007 [cited 2013 Jun 10]. Available from: http://www.e-cps.ca. Also available in paper copy from the publisher.

• Patients with CKD almost always develop secondary hyperplasia of the parathyroid glands, resulting in elevated blood levels of parathyroid hormone (PTH)
• Abnormality due to:
- Hypocalcemia
- Deficiency of 1,25- dihydroxycholecalciferol [l,25(OH)2D3]
- Hyperphosphatemia
• Progressive loss of kidney function ! decrease in the number of vitamin D receptors (VDR) and calcium-sensing receptors (CaR) in the parathyroid glands occurs ! increasing resistance to the action of vitamin D and calcium.
• These events will allow secondary hyperparathyroidism to worsen.
BONE MINERAL METABOLISM
American Journal of Kidney Diseases, Vol 42, No 4, Suppl 3 (October), 2003: p S1

BONE MINERAL METABOLISM CKD and Bone Mineral Metabolism Secondary hyperparathyroidism
Skeletal Effects: CKD-MBD (Mineral and Bone Disorder) Osteitis fibrosa Demineralization Fractures Bone pain
Non-Skeletal Effects: Calcification of arteries, including coronary arteries Skin ulcers and soft tissue necrosis Pruritus
Tanna, Gemini. Chronic Kidney Disease [unpublished lecture notes]. PHM 202, Leslie Dan Faculty of Pharmacy. Lecture given November 2013.

• Calcium to Lower Serum Phosphate
• E.g. Tums Extra Strength 1 tab TID with first bite of meal
• Will bind to phosphate in gut preventing absorption
• Diet Low in Phosphate
• Limit dairy, whole wheat/multigrain, nuts, and beer/pop intake
• Rocaltrol to lower PTH
• 0.25 mcg po daily
• Monitor closely Ca, PO4, and PTH levels
• If PTH below target, Ca > 9.5 mg/ dL, PO4 > 4.6 mg/dL, hold calcitriol until levels return to normal
• Re-initiate at a lower dose
PREVENTING SKELETAL & NON-SKELETAL EFFECTS
• Parathyroid Hormone Level: 1.4-7.6 pmol/L • Calcium: 8.4-9.5 mg/dL • PO4: 3.5-5.5 mg/dL
e-CPS [Internet]. Ottawa (ON): Canadian Pharmacists Association; c2007 [cited 2013 Jun 10].
Lexicomp. [Internet]. Rocaltrol Monograph. [cited 2013 Jun 10].

• “The progressive increase in proteinuria in patients with longstanding diabetes, followed by declining function that eventually can lead to ESRD”
• Poor blood sugar control damages small blood vessels in kidneys, impairing kidneys' ability to filter blood
• Risk factors:
- Long duration of diabetes
- Poor glycemic control
- Hypertension
- Cigarette smoking
DIABETIC NEPHROPATHY
. McFarlane et al. / Can J Diabetes 37 (2013) S129eS136

• Screening for CKD should be conducted using a urine albumin-to-creatinine ratio & a serum creatinine converted to eGFR
• At diagnosis of Type 2 diabetes and 5 years after diagnosis in adults with Type 1 diabetes, and repeated yearly thereafter
• Diagnosis made if ACR >2.0 mg/mmol and/or eGFR <60 mL/min on at least 2 of 3 samples over 3-month period
SCREENING/DIAGNOSIS
. McFarlane et al. / Can J Diabetes 37 (2013) S129eS136

• Optimal glycemic control immediately after diagnosis will reduce the risk of diabetic nephropathy
• Goals of therapy:
• A1C < 7%
• Fasting Plasma Glucose 4-7 mmol/L
• Post-Prandial Plasma Glucose 5-10 mmol/L
DIABETIC NEPHROPATHY
. McFarlane et al. / Can J Diabetes 37 (2013) S129eS136

. McFarlane et al. / Can J Diabetes 37 (2013) S129eS136

• ACE Inhibitors and ARBs can reduce the risk, and slow the progression, of diabetic nephropathy independent of their effect on blood pressure
• ACE Inhibitors and ARBs decrease albuminuria and prevent worsening of nephropathy
• This effect occurs in albuminuric normotensive patients, and patients with hypertension
• All adults with diabetes and CKD with either hypertension or albuminuria should receive an ACE Inhibitor or an ARB
DIABETIC NEPHROPATHY
. McFarlane et al. / Can J Diabetes 37 (2013) S129eS136