Embed Size (px)
Citation preview

CKDGENERAL AND CLINICALEPIDEMIOLOGY 2
MP157 THE SOUTH AFRICAN RENAL REGISTRY: A FIRST REPORT
Mogamat Razeen Davids1,2, Nicola Marais2 and Julian Jacobs21Stellenbosch University and Tygerberg Hospital, Cape Town, South Africa,2South African Renal Society, Johannesburg, South Africa
Introduction and Aims: There have been no reliable data on end-stage renal diseaseand renal replacement therapy (RRT) in South Africa since 1994 when the SouthAfrican Dialysis and Transplant Registry published their last report and stoppedoperating due to resource limitations. Several years ago the South African Renal Societymandated a small team to re-establish a national renal registry for the purpose ofcollecting and publishing critical data concerning RRT in South Africa.Methods: An Internet-based system was developed which included a central serverhousing the database, with users around the country interfacing with the server via asmall, downloadable desktop application. Paper-based forms were provided to unitswho had difficulties using the online system. Assistance with data capture was offeredwhere there were serious human resource limitations. The Registry was registered as along-term observational study with ethics approval for country-wide data collectionand a waiver of individual informed consent was granted. In this first round of datacollection we focused only on the most important epidemiological data. The resultsdescribe the situation as on 31 December 2012.Results: A total of 8617 patients were receiving RRT in December 2012. With apopulation of 52.3 million people this translates into a prevalence of 165 patients permillion population (pmp). Mean age was 48.9 years. Most of the patients (62.6%) werebeing treated in the private healthcare sector, which caters for the approximately 17%of the population who have medical insurance. The remainder were being treated instate/public healthcare facilities and a small number in units which operate aspublic-private partnerships. The most common primary renal disease recorded wasCKD of unknown cause, followed by hypertensive renal disease, diabetic nephropathyand chronic nephritic syndromes. Haemodialysis was the most common treatmentmodality (70.7%), followed by transplantation (15.1%) and peritoneal dialysis (14.2%).Our results contrast with those from 1994 when the prevalence was 70 pmp, with55.5% of patients having functioning transplants, 29.8% being on haemodialysis and14.7% being on peritoneal dialysis.Conclusions: The treatment rate for patients with ESRD is low in South Africa whencompared with countries having a similar GNI per capita. There has been stronggrowth in haemodialysis patient numbers in the private sector but little growth in thenumbers of patients who are on peritoneal dialysis or who have been transplanted. Inthe state sector there has been little overall growth in the numbers of patients beingtreated despite a substantial increase in the total population.
MP158 A LONGITUDINAL ASSESSMENTOF THE NATURAL RATE OFDECLINE IN RENAL FUNCTIONWITH AGE
Eytan Cohen1, Irit Krause2, Elad Goldberg1, Moshe Garty1 and Ilan Krause11Rabin Medical Center, Petah Tiqva, Israel, 2Schneider’s Children Medical Centerof Israel, Petah Tiqva, Israel
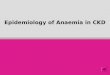
Introduction and Aims: Cross-sectional studies have long suggested that renalfunction declines with age. Longitudinal studies regarding this issue are limited. Wetherefore aimed to perform a longitudinal study, on a large population based cohort, tocalculate the natural rate of GFR decline with age.Methods:We retrospectively analyzed a database of subjects attending a screeningcenter in Israel between the years 2000-2012. Estimated GFR (eGFR) was calculatedusing the latest CKD-EPI equation. Only subjects with normal eGFR were included,eGFR was assessed consequently in at least 5 yearly visits. We estimated the rate of theannual decline in eGFR per subject using a linear regression model which regressed theeGFR against the year variable. The rate of decline in GFR with age was assessed inhealthy subjects and in subjects with co-morbidities.Results: The cohort included 2693 healthy subjects and 230 subjects with differentco-morbidities. The mean (± SE) annual rate of decline in eGFR in healthy subjectswas of 0.97± 0.02 mL/min/year/1.73m2. This decline increased significantly from 0.82± 0.22 at age group 20-30 years to 0.84 ± 0.08, 1.07 ± 0.08 and 1.15 ± 0.12 mL/min/year/1.73 m2 in age groups 31-40, 41-50 and 50 years and older respectively (p<0.001,Figure 1). No correlation was found between the annual decline in eGFR and bodymass index (Figure 2). In subjects with hypertension, diabetes mellitus, impairedfasting glucose or combined co-morbidity the decline in eGFR was 1.12 ± 0.12, 0.77 ±
0.16, 0.85 ± 0.17, 1.18 ± 0.26 mL/min/year/1.73 m2 respectively (Figure 3).Conclusions:• This large longitudinal study provides new data on the decrease in eGFR with age.• The rate of eGFR decline significantly increases with age.• Body mass index does not affect the rate of eGFR decline.
MP158 Figure 1: Annual rate of decline in eGFT (mL/min/year/1.73m2) in healthysubjects at different age groups.
MP158 Figure 2: Annual rate of decline in eGFR (mL/min/year/1.73m2) in relation todifferent BMI categories
MP158 Figure 3: Annual rate of decline in eGFR (mL/min/year/1.73m2) in healthysubjects and in subjects with co-morbidity
© The Author 2014. Published by Oxford University Press on behalf of ERA-EDTA. All rights reserved.
Nephrology Dialysis Transplantation 29 (Supplement 3): iii380–iii393, 2014doi:10.1093/ndt/gfu167
Downloaded from https://academic.oup.com/ndt/article-abstract/29/suppl_3/iii380/1882504by gueston 25 March 2018

• Accurate prediction of the natural rate of GFR decline might be used to distinguishbetween normally ageing kidneys and those with chronic disease. This approach couldavoid unnecessary diagnostic procedures in the former and provide appropriatetreatment in the latter.
MP159 DECREASED FETUIN-A AND INCREASED PENTRAXIN-3LEVELS ARE ASSOCIATEDWITH AORTIC STIFFNESS INDIABETIC AND NON-DIABETIC CHRONIC KIDNEY DISEASEPATIENTS
Belda Dursun1, Yasin Sahan1, Halil Tanriverdi1, Simin Rota1, Sukriye Uslu1 andHande Senol11Pamukkale University Medical School, Denizli, Turkey
Introduction and Aims: Vascular calcifications are a common phenomenon thatcontribute to arterial stiffening in chronic kidney disease (CKD) patients; however, itspathology is not very well understood. Vascular stiffness is associated with morbidityand mortality in this population. Fetuin-A is involved in mineral metabolism and actsas an endogenous inhibitor of calcification. Pentraxin-3 (PTX3) is a reliable marker ofinflammation in CKD. The study was conducted to investigate the associations offetuin-a, pentraxin-3 and aortic stiffness in diabetic and non-diabetic CKD patients.Methods: The study was performed on 40 diabetic stage 3-5 CKD patients, 40non-diabetic stage 3-5 CKD patients and 40 non-uremic non-diabetic controls whowere matched for age and gender. Exclusion criteria included any documentation ofcardiovascular event, malignancy, and active infection.Fetuin-A (Elisa), PTX3 (Elisa),hemoglobin, hematocrit, C-reactive protein (CRP), calcium, phosphate, alkalinephosphatase, parathyroid hormone (PTH), 25(OH)D vitamin, total cholesterol, LDL,HDL cholesterol, triglycerides, uric acid, albumin and fibrinogen levels weredetermined. By M-mode echocardiography and tissue doppler echocardiography,elastic properties of aorta was calculated and an aortic stiffness index was determined.Results: The mean aortic stiffness index was higher both in diabetic CKD (0.148±0.005) and non-diabetic CKD group (0.142±0.004) than the control group (0.102±0.004); p=0,0001, but did not statistically differ between diabetics and non-diabeticgroups. The mean fetuin-A levels (ng/ml) were lower in diabetic CKD (17.4±10.4) andnon-diabetic CKD (18.1±10.5) than controls (42.3±16.8); p=0,0001. The meanPentraxin-3 level (ng/ml) were higher in diabetic CKD (1.13±0.2) and non-diabeticCKD group (1.04 ±0.24) than the control group (0.33 ±0.39), p=0,0001; diabetics hadstatistically higher levels of PTX3 than non-diabetics (p=0.022). The mean 25(OH)Dlevels (pg/ml) were significantly lower in in diabetic CKD (25.7±9.3) and non-diabeticCKD (26.1±10.9) than controls (42.4±9.8); p=0.001.(Pentraxin-3 levels were positivelycorrelated with aortic stiffness (r=0.410, P=0.0001). Fetuin-A levels were negativelycorrelated with aortic stiffness (r=-0.283, P=0.002). Fetuin-A showed negativecorrelations with duration of CKD, blood glucose, HBA1c, PTH, serum phosphoruslevels. Fetuin-A levels were positively correlated with 25(OH)D vitamin levels. Aorticstiffness index showed negative correlations with serum albumin, body mass index, 25(OH)D3 vitamin, and diastolic blood pressure. Aortic stiffness index showed positivecorrelations with serum creatinine, fasting blood glucose, HbA1c, uric acid, CRP, PTH,pulse pressure and systolic blood pressure.Conclusions: Our findings demonstrate increased aortic stiffness in stage 3-5 diabeticand non-diabetic CKD patients. Serum fetuin-A levels negatively reflected whereaspentraxin-3 levels positively reflected an increase in aortic stiffness. Based on ourresults, fetuin-A and pentraxin-3 could be used as risk factors for progression of aorticstiffness and therefore may have prognostic value in the follow up of these patients withhigh cardiovascular morbidity and mortality.
MP160 PROGNOSIS OFWHITE COAT HYPERTENSION ANDMASKEDHYPERTENSION IN NON-DIALYSIS CKD PATIENTS
Roberto Minutolo1, Francis B Gabbai2, Rajiv Agarwal3, Paolo Chiodini4,Silvio Borrelli1, Giovanna Stanzione1, Felice Nappi5, Vincenzo Bellizzi6,Giuseppe Conte1 and Luca De Nicola1
1Nephrology, Second University of Naples, Naples, Italy, 2University of California atSan Diego, San Diego, CA, 3Indiana University, Indianapolis, IN, 4SecondUniversity of Naples, Naples, Italy, 5Nephrology, County Hospital, Nola, Italy,6Nephrology, University Hospital, Salerno, Italy
Introduction and Aims: In non-dialysis chronic kidney disease (CKD), the prognosticrole of white coat hypertension (WCH) and masked hypertension (MH) remainsill-defined. Therefore, we designed this multicenter prospective cohort study toevaluate the impact of various BP profiles (WCH, MH and sustained hypertension,SH) on the overall prognosis including fatal and non-fatal CV events, ESRD andall-cause mortality.Methods:We performed ambulatory blood pressure (ABP) and clinic blood pressure(CBP) measurements in 489 consecutive hypertensive CKD patients, recruited in threenephrology units in Italy. Goal ABP was defined as daytime and nighttime BP <135/85and <120/70 mmHg, respectively; CBP was considered at goal if <130/80 mmHg.Based on these thresholds, patients were classified into four groups: normotensive,NOR (CBP and ABP at goal after treatment), WCH (CBP above goal and ABP at goal),MH (CBP at goal and ABP above goal), SH (CBP and ABP above goal).Results:Mean age was 64.4±14.2 years, GFR 43.3±19.8 mL/min/1.73m2 andproteinuria 0.9±1.6 g/day. Women were 41%, 36% had diabetes and 30% had history ofCV disease, with no differences among groups. Combining CBP and ABP, 47 patients(9.6%, 95%CI 7.0-12.2) were classified as NOR, 143 (29.2%, 95%CI 25.2-33.3) asWCH, 30 (6.1%, 95%CI 4.0-8.3) as MH and 269 (55.0%, 95%CI 50.6-59.4) with SH. BPlevels and main therapeutic features are reported in the Table. Over 9 years offollow-up (median 5.2, IQR 3.1-7.1 yrs), we recorded 131 CV events and 214 renalevents (Table).Since patients with worst prognosis (MH and SH) differed from those atlower risk (normotensive and WCH) for the presence of ABP above the target, werepeated the Cox analysis by replacing the four groups with out-of-target CBP and ABPvariables. These additional analyses confirmed that the main predictor of adverseoutcome was the presence of ABP above goal while CBP ≥130/80 mmHg did notpredict either CV or renal endpoint. Finally, sensitivity analyses performed usingdifferent thresholds for defining groups (according to AASK study, Japanese CKDcohort, Spanish ABPM Registry and Veterans cohort), confirmed that, unlike WCH,MH was associated to an increased risk of CV and renal outcome.Conclusions: In non-dialysis CKD patients, WCH is a prevalent benign condition;whereas MH is less frequent, it associates with increased cardio-renal risk, that is,similar to that observed in patients with SH. These findings support the use of ABPMin all hypertensive patients with CKD to better stratify their cardio-renal risk and,likely, to optimize the treatment.
MP161 INCREASED UNDERSTANDING OF ATYPICAL HAEMOLYTICURAEMC SYNDROME (AHUS): CHARACTERISTICS OFPATIENTS RECRUITED INTO THE GLOBAL AHUS REGISTRY
Johan Van De Walle1, Sally Johnson2, Véronique Frémeaux-Bacchi3,Gianluigi Ardissino4, Gema Ariceta5, Jon Beauchamp6, David Cohen7, LarryA Greenbaum8, Masayo Ogawa9, Franz Schaefer10 and Christoph Licht111University Hospital Ghent, Ghent, Belgium, 2Great North Children’s Hospital,Newcastle upon Tyne, United Kingdom, 3Assistance Publique-Hôpitaux de Paris,Paris, France, 4Fondazione IRCCS Cà Granda, Ospedale Maggiore Policlinico,Milan, Italy, 5Hospital Vall D’ Hebron, Barcelona, Spain, 6Alexion PharmaceuticalsInternational, Lausanne, Switzerland, 7Columbia University, New York, NY, 8EmoryUniversity, Atlanta, GA, 9Alexion Pharmaceuticals, Cheshire, CT, 10HeidelbergUniversity Pediatric Nephrology Clinic, Heidelberg, Germany, 11The Hospital forSick Children, Toronto, ON, Canada
Introduction and Aims: Atypical haemolytic uraemic syndrome (aHUS) is a rare,genetic condition, with most cases caused by uncontrolled complement activation. Thedisease is severe with patients experiencing thrombotic microangiopathy leading toorgan ischemia and damage. To increase understanding of aHUS, current managementand provide data on the long-term safety and efficacy of eculizumab, a terminalcomplement inhibitor, the aHUS Registry (NCT01522183) has been established. Here,
MP160
NOR (n=47) WCH (n=143) MH (N=30) SH (N=269)
CBP (mmHg) 119±8/70±8 147±14/83±10 118±8/70±7 153±17*/85±11Daytime BP (mmHg) 112±9/68±8 118±9#/70±8 127±10/74±8 142±15†/80±11†Nighttime BP (mmHg) 103±8/59±6 106±8/59±6 121±10/68±8 133±18†/71±10Non dippers (%) 66.0 48.3 76.7 67.7BP lowering drugs (N) 2.4±1.2 2.4±1.3 2.0±1.1 2.8±1.6 †RAS inhibitors (%) 87.2 83.9 53.3 81.0CV/Renal events (N) 6/14 29/31 10/19 86/150Cox analysis [HR (95%CI)]CV outcome Ref. 1.73 (0.71-4.20) 4.44 (1.57-12.6) 3.31 (1.43-7.67)Renal outcome Ref. 1.41 (0.72-2.75) 4.94 (2.36-10.4) 3.36 (1.86-6.05)ESRD Ref. 1.86 (0.65-5.30) 5.94 (1.93-18.3) 5.65 (2.36-13.5)Death Ref. 1.13 (0.46-2.75) 3.68 (1.32-10.3) 2.31 (1.02-5.24)
* P<0.05 vs WCH; # P<0.05 vs NOR; † P<0.05 vs MH. Non dippers: night/day ratio of systolic ambulatory BP ≥0.9. Cox model adjusted for age, gender, BMI, diabetes, history of CVdisease, Hb, GFR, proteinuria, non dipping, RAS inhibitors and stratified for Center.
Nephrology Dialysis Transplantation Abstracts
Volume 29 | Supplement 3 | May 2014 doi:10.1093/ndt/gfu167 | iiiDownloaded from https://academic.oup.com/ndt/article-abstract/29/suppl_3/iii380/1882504by gueston 25 March 2018

we describe the baseline demographics and characteristics of patients recruited in thefirst 18 months.Methods: The aHUS registry is an observational, non-interventional, multicenter,global study. Patients are eligible for inclusion into the registry if they have received aclinical diagnosis of aHUS. Patients can be enrolled irrespective of their age ormanagement, and are not required to have an identified complement mutation oranti-complement factor antibodies. On enrolment, details relating to demographic andgeneral medical history are collected, together with information on management. Dataare then collected prospectively every 6 months thereafter. The data cut-off for thisanalysis was 18 September, 2013.Results: The first 211 patients recruited into the registry come from 12 countries inEurope, the USA and Australia. Half of the patients are female, Table 1 shows thebaseline data. Many individuals have experienced prior renal damage. Around half thepatients had received eculizumab (104/211 [49%]), and the mean (SD) age on startingthis treatment was 25 (21) years.Conclusions: Analyses of data from the aHUS Registry will help to advance ourunderstanding of the history and progression of aHUS, as well as increase ourknowledge on safety and efficacy of the use of eculizumab in such patients comparedwith other management. The global nature of the registry is intended to facilitatecollection of a suitable volume of data relating to a rare disease, and physicians areencouraged to enrol eligible patients. Table 1. Baseline characteristics of patientsenrolled in the aHUS Registry by 18 Sept 2013
MP162 CARDIAC PHENOTYPE IMPAIRMENT DUE TO UREMICSERUM
Elisa Scalzotto1, Federico Nalesso1, Tania Zaglia2, Valentina Corradi1, Mauro Neri3,Francesca Martino1, Monica Zanella1, Alessandra Brendolan1, Marco Mongillo4and Claudio Ronco31San Bortolo Hospital, Vicenza, Italy, 2Venetian Institute of MolecularMedicine-VIMM, Padua, Italy, 3San Bortolo Hospital, IRRIV-Department ofNephrology, Italy, 4Venetian Institute of Molecular Medicine-VIMM, Padova, Italy
Introduction and Aims: Traditional cardiovascular risk factors play an important rolein the incidence of cardiovascular mortality in Chronic Kidney Disease (CKD) patient(pts). The presence of cardiovascular disease is an important predictor of mortality inCKD stage V pts, as it is responsible for almost 50% of deaths. Uremic Serum (Ser)contains more factors playing an important role in the incidence of cardiovascularmorbidity and mortality. However, the molecular mechanism is still unclear. Wehypothesized that a circulating substances present in Ser contributes to cardiomyocytesdamage.Methods: The present study included CKD stage V pts on hemodialysis treatment(HD) and healthy volunteers as control samples characterized by the same gender. Serand ultrafiltrate (UF) samples were collected at the beginning of Renal ReplacementTherapy (RRT) after 20 min of Isolated Ultrafiltration (iUF). Cardiomyocytes fromneonatal rats hearts (NRC) were isolated and incubated with 10%, 30%, 60% of samplesconcentration. Cell count, morphology and apoptotic events were evaluated.Results: The proteins separation obtained by western blot analysis between Ser and UFsamples were similar. In particular, the ionic composition and the low molecularweight (MW) proteins were comparable. The effect of Ser and UF incubation weredifferent on NRC: the Ser caused increases of cell death and contraction in dosedependent manner, whereas UF, like control samples, did not have demostrable effectson any of the parameters examined. Moreover, cell atrophy, disarrangement ofsarcomers myofibrillar organization and the decrease of the NRC' nuclei total numberwere particularly evident already at 10% of Ser concentration.Conclusions: The phenotype observed after Ser incubation highlights that there aresubstances involved in the impairment of NRC death and sarcomere disarrangement.Our findings suggests the involvement of high MW proteins. Next steps will be toevaluate this protein profile into Ser versus UF also using several filters (in terms ofmembrane cut-off ) to explain the molecular mechanism involved, the cell adhesionproteins and autophagy pathway.
MP163 CHARACTERISATION OF FUNCTIONAL IMPAIRMENT OFURAEMIC CARDIOMYOPATHY
S Chinnappa1,2, A Mooney2, A M El Nahas1, Y K Tu3 and L B Tan21Sheffield Kidney Institute, Sheffield, United Kingdom, 2Leeds Teaching HospitalsNHS Trust, Leeds, United Kingdom, 3National Taiwan University, Taipei, Taiwan
Introduction and Aims: A large observational study has demonstrated that reducedrenal function is associated with cardiac structural abnormality but not with cardiacfunctional impairment [Park et al., JASN 23:1725]. Like many others, they measuredindices of resting cardiac performance but true cardiac dysfunction is better shownduring peak stress. KDIGO identified assessment of asymptomatic cardiac dysfunctionin chronic kidney disease (CKD) as a research priority, which can be addressed bymeasuring peak cardiac power output (CPOmax) [Chinnappa et al., Expert RevCardiovasc Ther 12(2):127], a direct representation of the integrated function of theorgan. We tested the hypothesis that asymptomatic CKD patients without any knownprimary cardiac diseases (CVD) or diabetes mellitus (DM) have cardiac impairmentcompared to healthy controls.Methods: In a cross sectional study of male subjects, 60 CKD patients [22 CKD stages2&3, 17 CKD 4 and 21 CKD 5 (pre-dialysis)] without any primary cardiac disease orDM were compared with 101 healthy male volunteers by undertakingsymptom-limited exercise testing to measure CPOmax. As a positive control, data from39 age- and gender-matched HF patients in NYHA class II & III were also obtained.CPOmax was obtained non-invasively during cardiopulmonary exercise test usingstandard CO2 rebreathing technique. Results are given as mean±SD and standardstatistical analysis methods applied.Results: All subjects performed exercise well above the anaerobic threshold with amean peak respiratory exchange ratio of 1.15±0.09. None of them had induciblecardiac ischaemia during the test. The mean eGFRs of CKD 2&3, CKD 4 and CKD 5groups were 55.7±17.5ml/min, 21.7±3.9ml/min and 12.3±2.4 ml/min respectively.Compared to healthy controls, the CKD patients showed a graded reduction in CPOmax
with 92.2±11.7% of predicted CPOmax in CKD 2&3 (P=0.03), 87.4±10% in CKD 4(P=0.0001) and 77.5%±13.5% in CKD 5 (P<10-6). These values were not as impaired asin HF patients who had 45.5±10.7% of predicted CPOmax (P<10
-6) (Fig 1).Conclusions: The results show a first clear evidence of asymptomatic cardiacdysfunction associated with reduced renal function even in the absence of primarycardiac disease and DM. Future such evaluations have potential applications incharacterising uraemic cardiomyopathy and finding therapeutic strategies to reverse it.
MP164 LOWDOSE ASPIRIN FOR PREVENTION OFCARDIOVASCULAR DISEASE IN PATIENTSWITH CHRONICKIDNEY DISEASE; A PROPENSITY-MATCHED STUDY
Ji Yong Jung1, Ae Jin Kim1, Han Ro1, Chungsik Lee2, Jae Hyun Chang1,Hyun Hee Lee1 and Wookyung Chung11Gachon University Gil Medical Center, Incheon, Republic of Korea,2Cheju Halla General Hospital, Jeju, Republic of Korea
Introduction and Aims: Chronic kidney disease (CKD) is a powerful risk factor fordevelopment of cardiovascular disease (CVD). Previous trials have investigated the
MP161
MP163
Abstracts Nephrology Dialysis Transplantation
iii | Abstracts Volume 29 | Supplement 3 | May 2014Downloaded from https://academic.oup.com/ndt/article-abstract/29/suppl_3/iii380/1882504by gueston 25 March 2018

effect of low dose aspirin on prevention of CVD in patients with diabetes but not inCKD patients. In addition, the role of aspirin in diabetics is controversial and theavailable literature is contradictory. Therefore, we studied whether low dose aspirinwould be beneficial in patients with chronic kidney disease (CKD) as high risk groupfor CVD.Methods: Using propensity score matching, 1884 low dose aspirin (100mg/day)recipients and 1884 non-recipients were 1:1 paired for analysis from 25340 patientswith CKD. The primary endpoint was atherosclerotic CVD including coronary arterialdisease, stroke, and peripheral arterial disease. Secondary endpoints included deathfrom any cause, bleeding events, doubling of serum creatinine and renal death.Results: Low dose aspirin was prescribed for 8.16% (2068 of 25340) of patients withCKD. The incidence of primary endpoint of any atherosclerotic CVD was significantlyhigher in the aspirin users than in the non-aspirin users (P<0.001). Secondaryendpoints including all-cause mortality, composite bleeding events were notsignificantly different between the aspirin and non-aspirin users. However, theoccurrence of a doubling of serum creatinine concentration (P=0.001) and renal death(P=0.042) were significantly associated with the use of aspirin.Conclusions: These results suggest that use of low-dose aspirin in patients with CKDhas a possible harmful effect on CVD and renal progression. Further randomizedclinical trials are warranted to confirm the effect of low dose aspirin therapy on thedevelopment of CVD in these patients.
MP165 PATIENT PERSPECTIVES AND READINESS TO CHANGE INCHRONIC KIDNEY DISEASE: EXERCISE AND PHYSICALACTIVITY BEHAVIOURS
Amy L Clarke1, Hannah ML Young1, Katherine L Hull1, Nicky Hudson2, JamesO Burton1 and Alice C Smith11University Hospitals of Leicester, Leicester, United Kingdom, 2De MontfortUniversity, Leicester, United Kingdom
Introduction and Aims: Chronic Kidney Disease (CKD) is associated with a widerange of physiological and psychological complications. Exercise is beneficial for CKDpatients but it is rarely integrated into the care plan and patients typically leadsedentary lifestyles. Physical inactivity is often related to low self-efficacy (SE) and lackof readiness to change, but the reasons underlying patient inactivity have not beenexplored in the UK CKD population. Here we present the findings of a two-part mixedmethods study. Part 1 aimed to investigate readiness to change physical activity andexercise self-efficacy in patients with CKD, using a survey. Part 2 aimed to explorepatient perceived motivators and barriers towards exercise and physical activity, usingqualitative methodology.Methods: In Part 1,399 patients with CKD Stage 1-5 pre-dialysis (223 male, age range16-93 years) completed a survey at routine outpatient clinic appointments. The surveyincluded two validated questionnaires: (1) Stage of Change (SOCQ), which identifies apatient’s readiness to change physical activity behaviour; and (2) Exercise Self-EfficacyQuestionnaire (SEQ), which explores confidence to exercise. In Part 2, a purposivesample of 36 patients with CKD Stage 1-5 pre-dialysis (20 male, age range 26-81 years)were recruited to participate in a qualitative exploration of patient-perceived barriersand motivators to exercise in CKD. 3 focus groups and 22 semi-structured interviewswere facilitated by researchers uninvolved in clinical care. Interviews and focus groupswere audio recorded, transcribed verbatim and translated where necessary, and weresubjected to thematic analysis.Results: In Part 1, the SOCQ showed that 54% of patients considered themselves toparticipate in some form of exercise behaviour, while 24% were contemplating exerciseand only 22% were pre-contemplation (no interest in exercise). Self-efficacy wassignificantly lower for patients who were in the pre-contemplation or contemplationstages compared to patients who were in the preparation, action or maintenance stages(Z=-4.81,P<0.005). Part 2 showed that patient-perceived barriers to physical activitymainly included other medical condition, old age, fear relating to injury, fatigue andlack of motivation. Themes for motivation included enjoyment, previously or currentlyexperienced physical benefits support provided by family, desired benefits and goalsetting.Conclusions: This study demonstrates that the majority of patients with CKD are opento the idea of increasing their physical activity levels. Low SE is an important factor in
changing exercise behaviour, and a number of patient-perceived barriers andmotivators to exercise were identified. This information is an important first stage inthe development of a CKD- specific exercise behaviour change intervention with afocus on improving SE and goal setting, and designed to assist in finding solutions tobarriers and utilising patient-reported motivators to exercise.
MP166 RESOURCE AND COST BURDEN OF CHRONIC KIDNEYDISEASE (CKD) STAGE 3-5 NOTON DIALYSIS (ND) IN THEUNITED KINGDOM (UK): TYPE 2 DIABETES (T2D) ANDWITHOUT DIABETES
Steven Marx1, Allison Petrilla2, Ivana Filipovic1 and Won Chan Lee21Abbvie, North Chicago, IL, 2IMS Health, Alexandria, VA
Introduction and Aims: To understand the economic implications of kidney functiondecline in the UK, in CKD patients with T2D, a known CKD risk factor, versus thosewithout diabetes.Methods: The study utilized IMS Disease Analyzer primary care EMR-EuropeanUnion data to identify UK patients between 2007-2011 with reduced kidney function.Patients were stratified by diagnosis of T2D (versus No Diabetes) and by estimatedglomerular filtrate rate < 60ml/min/m2 (CKD Stage 3a, 3b, 4 and 5ND), those receivingdialysis were excluded due to incomplete dialysis care records. The primary studyoutcome was per patient per year (PPPY) resources utilization and costs (2010 USD)for all-cause health care services beginning with the first observed CKD stage from theprimary care physician (PCP) perspective.Results:Conclusions: This study provides evidence of increase healthcare resource use andcosts with the progression of CKD from Stage 3a through Stage 5ND from a UK PCPperspective. CKD patients with T2D experienced higher resources and cost comparedto those without diabetes. Within this EMR dataset, inpatient utilization/costs are likelyunderreported and the true cost of CKD care may be higher.
MP167 SOLUBLE UROKINASE RECEPTOR (SUPAR) PREDICTSMORTALITY AND CARDIOVASCULAR DISEASE IN PATIENTSWITHMILD-TO-MODERATE CHRONIC KIDNEY DISEASE
Björn Meijers1, Ruben Poesen1, Markus Storr2, Kathleen Claes1, Dirk Kuypers1and Pieter Evenepoel11University Hospitals Leuven, Leuven, Belgium, 2Gambro Dialysatoren GmbH,Hechingen, Germany
Introduction and Aims: suPAR is linked to mortality and cardiovascular disease inpatients without chronic kidney disease (CKD). Studies evaluating the role of suPAR asFSGS biomarker observed an inverse association between eGFR and suPAR. WhethersuPAR accumulates in patients with CKD and whether accumulation of suPAR isassociated with mortality in CKD has not been studied to date.Methods:We measured suPAR concentrations in patients with CKD from the Leuvenmild-to-moderate CKD study (Clinical trials protocol NCT00441623) using the humanuPAR enzyme-linked immune sorbent assay (R&D systemsTM). Associations withoverall mortality and cardiovascular disease were explored using Kaplan-Meierestimates and multivariate Cox proportional hazards analyses.Results:We determined suPAR concentrations in 486 patients with known non-FSGSCKD patients. eGFR was the strongest determinant of suPAR concentrations (P <0.0001) and suPAR accumulated in patients at low eGFR. suPAR concentrations wereassociated with overall mortality (P < 0.0001) and cardiovascular events (P < 0.0001).These associations persisted after correction for age, sex, eGFR and C-reactive proteinconcentration, but for mortality was lost after correction for serum albumin. suPARremained associated with cardiovascular disease in multivariate analysis.Conclusions: suPAR accumulates in patients with CKD and is directly and graduallyassociated with overall mortality and cardiovascular events, independent of kidneyfunction. Given the versatile roles of uPAR as signaling orchestrator, accumulation ofsuPAR in patients at lower eGFR may be in the causal chain of extrarenalmanifestations of CKD.
MP166
T2D Patients versus Non-Diabetic Patients, Number PPPY (SD)
CKD 3a (n=4,982 vs 19,576) CKD 3b (n=3,583 vs n=11,090) CKD 4 (n=1,576 vs n=4,209) CKD 5ND (n=403 vs n=1,254)
Medications* 78.6(60) vs52.5(47.8) 93.8(69.3) vs68.5(59.2) 106(74.5) vs79.8(66.7) 91.1(72.7) vs71.6(86.2)Office Visits 18.8(17.9) vs15.7(17) 22.3(22.5) vs19.1(19.6) 25.7(20.1) vs23.6(23.3) 27.6(30.7) vs24.0(25.3)Hospitalizations 0.3(1.2) vs0.2(0.8) 0.4(1.6) vs0.4(1.5) 0.7(1.9) vs0.8(3) 1.1(3.4) vs0.8(3.1)T2D Patients versus Non-Diabetic Patients, Mean PPPY Costs USD (SD)Medications $1,135(1,312) vs $655(947) $1,338(1,585) vs $813(1,166) $1,690(2,101) vs $1,012(1,525) $1,760(1,903) vs $1,235(1,735)Office Visits $2,881(2,741) vs $2,413(2,605) $3,416(3,448) vs $2,923(3,013) $3,941(3,089) vs $3,619(3,569) $4,238(4,701) vs $3,685(3,877)Hospitalizations $1,126(5,271) vs $867(3,692) $1,920(7,179) vs $1,546(6,622) $3,107(8,144) vs $3,425(13,238) $4,760(14,853) vs $3,688(13,341)
SD = Standard Deviation, USD = United States Dollars, Medication* = Prescriptions written Multivariate analyses adjusting for age, gender, comorbidities, and pre-indexmedications demonstrated higher costs among T2D in CKD3 1.113, p=0.0156 and CKD4 1.354, p<0.0001.
Nephrology Dialysis Transplantation Abstracts
Volume 29 | Supplement 3 | May 2014 doi:10.1093/ndt/gfu167 | iiiDownloaded from https://academic.oup.com/ndt/article-abstract/29/suppl_3/iii380/1882504by gueston 25 March 2018

MP168 ETHNIC AND GENDER VARIATIONS IN SELF-REPORTEDFUNCTIONAL CAPACITY IN CHRONIC KIDNEY DISEASE
M Aukland1, A L Clarke1, K L Hull1, J O Burton1 and AC Smith11University Hospitals of Leicester, Leicester, United Kingdom
Introduction and Aims: Chronic kidney disease (CKD) is associated with high levelsof co-morbidity including accelerated cardiovascular disease, muscle wasting,functional decline and depression. In addition, patients frequently suffer fromweakness and fatigue which contribute to a sedentary lifestyle. There is increasingevidence that exercise can impact positively on these factors, yet its incorporation intoroutine care of CKD patients has been slow. For the effective development andimplementation of rehabilitation programmes, understanding the factors that influenceactivity levels and motivation in different cross sections of the population is required.The aim of this study is to investigate the impact of ethnicity and gender onself-reported functional capacity in patients with CKD.Methods: 515 patients (285 male) with CKD 1-5 pre-dialysis were recruited inoutpatient clinic waiting areas and completed the Duke Activity Status Index (DASI), avalidated measure of functional capacity. Of 438 of known ethnicity, 364 participantswere of British, Irish or other white background (208 male, 156 female, age range19-93, mean eGFR 34.8, range 6 to >90 ml/min/1.73m2). 91 patients were of black,Asian or other minority ethnic (BAME) origins (51 male, 40 female age range 17-81years, mean eGFR 30.7, range 5 to >90 mL/min/1.73m2). 74 (81%) of the BAME groupwere of Asian or of Asian British background.Results: The BAME patients were a significantly younger group than the white patients(BAME median age 52, range 17 to 81 years; White median age 66, range 19 to 93years, p>0.001) and therefore each group was divided into age quartiles. DASIfunctional capacity scores were significantly lower in the BAME group for all agequartiles except the youngest, as shown in the table below.As functional capacitydeclines with age, patients were divided into the same age quartiles to assess the impactof gender (Females median age 62, range 17-89 years; Male median age 61, range 16-93years). DASI scores were significantly lower in the female group in the two olderquartiles age groups as shown in the following table.Conclusions: Neither ethnicity nor gender influences functional capacity in youngerCKD patients. However, with increasing age, functional capacity drops more rapidly inthe BAME and female groups. This highlights the need to target them as a priority witheffective rehabilitation strategies.
As functional capacity declines with age, patients were divided into the same agequartiles to assess the impact of gender (Females median age 62, range 17-89 years;Male median age 61, range 16-93 years). DASI scores were significantly lower in thefemale group in the two older quartiles age groups as shown in the following table.
MP169 PREVALENCE OF SUBCLINICAL ATHEROMATOSIS ANDASSOCIATED RISK FACTORS IN CHRONIC KIDNEY DISEASETHE NEFRONA STUDY
Angels Betriu1, Montserrat Martinez-Alonso2, M Vittoria Arcidiacono2,Jorge Cannata-Andia3,4, Julio Pascual5,4, José Manuel Valdivielso2,4,1 andElvira Fernández-Giraldez1,2,41Udetma, Lleida, Spain, 2IRBLleida, Lleida, Spain, 3Hospital Universitario Central,Oviedo, Spain, 4RedinRen del ISCIII, Madrid, Spain, 5Hospital del Mar, Barcelona,Spain
Introduction and Aims: Background: The causes of the high cardiovascular mortalityobserved in chronic kidney disease (CKD), the presence of subclinical atheromatousdisease and their associated risk factors are unknown.Aim: Analyze the prevalence ofsublclinical atherosclerosis (atheromatous plaque) and the risk factors correlated to itin a cohort study of a Spanish population affected by different stages of CKD(NEFRONA study).Methods:We analysed 2445 patients with an estimated glomerular filtration rate(eGFR) below 60 ml/min (CKD3: 937; CKD4-5: 820; CKD5D: 688) and 559 non-CKD
subjects (eGFR >60 ml/min), 18 to 75 years old, without previous cardiovascularevents. An itinerant team of professionals performed carotid and femoral arterialultrasound to evaluate the presence of atheromatous plaque, defined as intima-mediathickness ≥1.5 mm. A stratified multivariate logistic analysis was used to associate therisk factors with the presence of plaque at any CKD stage.Results: The prevalence of plaque was high at any stage of CKD and positivelyassociated with the severity of CKD (CKD3:60%; CKD4-5:69% ;CKD5D:70%; p=.87).Multivariate logistic analysis showed that, at any CKD stage, age and being maleindependently associated with the presence of plaques (p<.001). In CKD3, there was asignificant interaction of the smoking status and triglycerides levels whichindependently associated with the presence of plaque (p<.001). Being diabetic alsoassociated with the presence of subclinical atherosclerosis (p<.001). In CKD4-5 therewas a significant association with smoking (p<.001), high phosphate (p=.01) and CRPlevels (p=.03). In diabetic dialysis patients (p=.02), low levels of 25(OH)-vitaminD3(p=.006) and smoking (p=.003) also showed a significant association with the presenceof plaque. Furthermore, the association of phosphate levels with the presence ofsubclinical atheromatosis showed a U shape curve.Conclusions: This analysis demonstrates the magnitude of subclinical atheromatousdisease in a large CKD population. The patient characteristics associated with thepresence of plaque differ in every CKD stage, indicating that it is necessary to treat therisk factors accordingly to the CKD stage
MP170 TOSCA - TUBEROUS SCLEROSIS REGISTRY TO INCREASEDISEASE AWARENESS
John C Kingswood1, Bernard Zonnenberg2, Matthias Sauter3 and ToscaConsortium1Royal Sussex County Hospital, Brighton, United Kingdom, 2University MedicalCenter, Utrecht, The Netherlands, 3Medizinische Klinik Und Poliklinik IV, KlinikumDer Universität München, Munich, Germany
Introduction and Aims: Tuberous sclerosis complex (TSC) is a rare genetic multisystemdisorder. The disease is characterised by growth of hamartomas in several organs, includingthe brain, lungs, heart, eyes, and skin. Kidney involvement is very common and significantlycontributes to morbidity andmortality in these patients. Renal angiomyolipomas areobserved in a majority of TSC patients. The TOSCA disease registry has been designed toaddress knowledge gaps in the natural history andmanagement of TSC.Methods: TOSCA is an international disease registry to assess manifestations, interventions,and outcomes in patients diagnosed with TSC. Patients of any age with a documented visitfor TSCwithin preceding 12 months or newly diagnosed individuals are eligible. Objectivesinclude mapping the course of TSCmanifestations and their prognostic role, identifyingpatients with rare symptoms and co-morbidities, recording interventions and theiroutcomes, contributing to creation of an evidence-base for disease assessment and therapy.TOSCA includes a core with general mandatory information on patients’ backgrounds andsubsections to collect additional data on disease manifestations. Estimated enrolment isapproximately 2000 patients in 31 countries worldwide. An initial enrolment period ofabout 24 months and a follow-up observation period of up to 5 years are planned. Interimanalyses are planned every year with data available starting from 2014. Data from the firstinterim analysis concerning renal involvement of TSCwill be presented.Results:As of 12 July 2013, baseline core data from 508 patients (pts) were entered in thedatabase (44.9%male). Median age was 16 years (range: 0-71 years), median age of TSCdiagnosis was 1 year (range: 0-67 years). Two hundred and seventy pts (53.1%) werediagnosed with a renal angiomyolipoma.Median age of renal angiomyolipoma diagnosiswas 18 years (range: 0- 63 years). Renal angiomyolipomas were multiple and bilateral in 135pts and caused symptoms in 35 pts, namely hemorrhage (13 pts, 4.8%), elevated bloodpressure (12 pts, 4.4%), pain (10 pts, 3.7%), impaired renal function (8 pts, 3.0%), hematuria(6 pts, 2.2%). The renal angiomyolipomawas treated in 75 pts (27.8%) with embolization(66.7%), mTOR inhibitor (28.0%), nephrectomy (20.0%), resection (4.0%). Further detailson renal manifestations available from the first interim analysis will be presented.Conclusions:Available data from the TOSCA first interim analysis underline the frequencyand clinical importance of kidney involvement in this disease. These will provide usefulinsights on diagnostics, interventional and treatment outcome factors of renalmanifestations of patients in the TOSCA database.
MP171 PROMOTING TIMELY REFERRALOF CHRONIC KIDNEYPATIENTS THROUGH A NURSE OPERATED PHONEANSWERING SYSTEM
Gabor Zakar1, Beata Biro1, Boglarka Besenczi1, Andrea Varga1 andPiroska Pekacs11BBraun Avitum Hungary, Szekesfehervar, Hungary
Introduction and Aims: Late referral of patients with chronic kidney disease (CKD) isa common problem interfering with timely initiaton of the renal replacement therapy.General practitioners and specialists in other medical fields (diabetology, cardiology,urology, hepatology etc.) often refer their patients to the nephrologist without anyurgency ranking and and the the timing of the appointment is done by a centralcoordinator of the hospital in the order of presentation. This way it can take even 2-3months to be seen by the nephrologist even for new patients in advanced stages ofCKD. To avoid dangerous delays of this kind we developed a locally operated phone
MP168
MP168
Abstracts Nephrology Dialysis Transplantation
iii | Abstracts Volume 29 | Supplement 3 | May 2014Downloaded from https://academic.oup.com/ndt/article-abstract/29/suppl_3/iii380/1882504by gueston 25 March 2018

answering system at our nephrology outpatient facility. In the presentation we reporton our experiences gained with the operation of the system.Methods: By the end of December 2009 a phone call answering machine was set up at thenephrology outpatient facility located in the building of the hemodialysis center, operated5 days a week with 30 contact medical hours by 4 nephrologists. After dialing the numbera standard message was given to the caller asking for the name, age, basic laboratory data(serum creatinine, eGFR) and and phone number, with the promise, that our assistant willcall back her/him with a suitable appointment date. Two nephrology nurses were trainedto receive and answer the messages. Upon calling back on the same day it was theresponsibility of the nurse to ask further questions (proteinuria, serum hemoglobin level)and make an individualized appointment date based on preset medical instructions.Results:After the introduction of the phone answering system monthly number of newlyregistered CKD patients grew by more than 20% (from 30-35 / month to 40-55)compared to the preceding two years (2007-2008). Waiting time for new patients to beseen by a nephrologist with an eGFR below 30 ml/min decreased from 64 to 45 days, withan urgency referreal time of within one week for those below 20 ml/min. Patients withheavy proteinuria and/or low serum hemoglobin levels were also called for an urgentreferreal within 2 weeks. As a result the number of planned dialysis starts increased by15% (from 20 to 35%) in the years 2010-2013, most planned patients choosing peritonealdialysis as their first treatment option.Conclusions: Based on patients opinions the independent phone call answering systemprovided reliable and safe acces for them to the nephrology care. The “call back”individualized approach was helpful in selecting those in need for an earlier or urgentneed of consultation and in reassuring those with “better” values not being endangeredthrough their longer waiting period. The “data based” appointment list contributed to abetter task-planning and problem oriented utilization of the nephrology team.
MP172 PHOSPHATE LOAD PER FUNCTIONING RENAL UNITPREDICTS ACCELERATED RENAL FUNCTION LOSSINDEPENDENTLY OF FGF23 AND OTHER RISK FACTORS INSTAGE 2-5 CKD PATIENTS
Patrizia Pizzini1, Anna Pisano1, Daniela Leonardis1, Vincenzo Panuccio1,Sebastiano Cutrupi1, Giovanni Tripepi1, Francesca Mallamaci1, Carmine Zoccali1and - On Behalf Of The MAUROWorking Group2
1CNR-IFC, Reggio Calabria, Italy, 2Mauro Working Group, Reggio Calabria, Italy
Introduction and Aims: Hyperphosphatemia is a predictor of accelerated renalfunction loss in patients with chronic kidney disease (CKD). This phenomenon couldbe interpreted as the trade-off of a counter-regulatory response aimed at maintainingglobal phosphate balance. The background hypothesis is that global phosphate balanceis maintained by raising phosphate excretion per functioning renal unit (fractionalphosphate excretion) and is possibly mediated by high FGF23. However, thishypothesis has never been formally tested in appropriate cohort studies.Methods:We studied 494 incident patients with stages 2-5 CKD (age 62±11 years, 60%males and 32% diabetics). The baseline eGFR in this cohort was 28.4±13.9 ml/min/1.73m2. The study end point was a composite renal outcome (i.e. eGFR reduction > 30%,dialysis or transplantation).Results: Fractional phosphate excretion (median: 41%, interquartile range 27-61%) wasabove the upper limit of the normal range (>20%) in the majority of CKD patients (83%).In unadjusted analyses, fractional phosphate excretion was related directly to urinaryprotein (rho=0.24, P<0.001), FGF-23 (r=0.25, P<0.001), male gender (r=0.13, P=0.003),smoking (r=0.13, P=0.004) and diastolic blood pressure (r=0.09, P=0.04) and inversely toeGFR (r=-0.44, P<0.001) and diabetes (r= -0.11, P=0.02). Fractional phosphate excretionwas largely unrelated to serum phosphate (r=-0.03, P=0.54). During the follow-up (mean:2.4 years), 165 renal events occurred. In a crude analysis, an increase in fractionalphosphate excretion of 5% was associated to a 6% increase in the hazard ratio (HR) ofrenal events (HR: 1.06, 95%: 1.03-1.09, P<0.001). Data adjustment for potentialconfounders (age, gender, smoking, diabetes, cholesterol, diastolic pressure, urinaryprotein, phosphate, anti-hypertensive treatment and FGF-23) did not affect the strength ofthe relationship between fractional phosphate excretion and renal outcomes (HR: 1.05,95% C: 1.02-1.07, P<0.001).Conclusions: Fractional phosphate excretion is a strong, independent predictor of incidentrenal events. The predictive power of this parameter is largely independent of other riskfactors, including serum phosphate and FGF23. Phosphate burden per functioning renalunit, predicts progression towards end-stage kidney disease through yet unknownmechanism(s). Biological pathways independent of FGF-23 most likely play a dominantrole in phosphate-related renal damage.
MP173 VARIATIONS IN THEMANAGEMENTOF CHRONIC KIDNEYDISEASE ACROSS THE UK: RESULTS OF A NATIONALSURVEY (CKMAPPS)
Julia Arnold1, Jyoti Baharani1 and Hugh Rayner11Heart of England NHS Foundation Trust, Birmingham, United Kingdom
Introduction and Aims: The number of patients in the UK with chronic kidneydisease (CKD) continues to grow. Several factors are implicated: increasing prevalenceof CKD and its associated diseases e.g. diabetes, hypertension and cardiovasculardisease, better recognition and diagnosis of CKD and an aging population. The UK age
adjusted prevalence of CKD stages 3-5 is 8.5% (10.6% female, 5.8% male).International models of care for patients with advanced CKD (stages 4-5) vary widely.The way CKD services are provided in the UK has evolved over the last two decadesaccording to local circumstances and initiatives. There has been a strong emphasis onmulti-professional working in the UK compared with other countries. We analyseddata from the Conservative Kidney Management Assessment of Practice Patterns Study(CKMAPPS) to look at variations in the organisation of care for advanced CKDpatients across the UK.Methods: The CKMAPPS survey was developed based on existing literature andconsultation with nephrologists and a renal nurse specialist. It included questionsabout the organisation of CKD services including the number of consultants in eachunit, the presence of a multi-skilled renal team to manage CKD patients, provision ofCKD clinics in neighbouring hospitals, provision of pre-dialysis clinics and pre-dialysiseducation and how consultants share responsibility for patients.Results: 67 out of 71 UK renal units completed the questionnaire (94% response rate).The mean full time equivalent (FTE) for consultants per unit is 7.13. 98.5% of unitsfeature a multi-skilled renal team (MSRT) and 87.9% hold regular meetings, of which47.7% meet weekly. MSRT meetings involve a variety of staff including consultantnephrologists (77.6%), renal nurses (76.1%), dieticians (68.7%), vascular accesscoordinators (62.7%) and social workers (40.3%).88.1% of units run CKD clinics forneighbouring hospitals. 83.6% of units run a pre-dialysis clinic or equivalent forpatients approaching the need for renal replacement therapy (RRT). 64 of the renalunits (95.5%) reported 76-100% of patients receive nurse-led pre-dialysis educationand 24 (35.8%) units reported 76-100% of patients are provided with home visits.86.6% of patients have pre-dialysis education with a consultant or registrar, 95.5%receive written material and 76.1% receive a group session with other pre-dialysispatients. 80.6% of centres hold a pre-dialysis education day. 26.9% of consultants shareresponsibility for patients, 28.4% work on a named-patient basis and 29.9% take a leadrole for individual patients.Conclusions: Our data suggests that care for advanced CKD in the UK is welldeveloped with geographical spread of specialist services adopting a ‘hub and spoke’model. There is widespread incorporation of multi-professional team working and themajority of units provide specialist pre-dialysis clinics, patient education activities andcontinuity of consultant care.
MP174 THE LIPID PROFILE AND TREATMENTOF CKD PATIENTS:ACOMMUNITY BASED COHORT STUDY
Beng H So1, Scott Blackwell1, Alan G Jardine2 and Mark S Macgregor11University Hospital Crosshouse, Kilmarnock, United Kingdom, 2University ofGlasgow, Glasgow, United Kingdom
Introduction and Aims: Chronic kidney disease is common, and associated withincreased morbidity and mortality, especially from cardiovascular disease.Lipid-regulating therapy is one of few evidence-based interventions available toimprove outcomes in these patients. There is a lack of population-level data describingthe typical lipid profile and lipid-regulating therapy of CKD patients. We aim todescribe this for all CKD patients within our health board’s population.Methods: Our catchment adult population from 1/4/11-31/3/12 was 313,739. Usinglaboratory data, we identified all prevalent patients with CKD stages 3-5 for that year.Community pharmacy dispensing data was obtained from the Prescribing InformationService for Scotland, and linked using the NHS Scotland unique patient identifier. LDLvalues were calculated using the Friedewald formula. Independent sample T-test wasused to calculate mean difference and 95% CI.Results: CKD prevalence was 5.6% of the adult population. Lipid profiles were tested in70.2% of CKD patients (Table 1). Age, gender and eGFR were similar in the tested anduntested populations. However, proportionally fewer females (54.1% females vs 63.4%males) received treatment (χ2, p<0.001). Lipid-regulating agents were dispensed to 57%of CKD patients, with simvastatin most commonly used in 66% (median dose 40 mg,IQR 20 mg), followed by atorvastatin in 23% (20mg IQR 30mg), pravastatin in 7.1%(20mg, IQR 20mg), rosuvastatin in 2.6% (10mg, IQR 13mg) and fluvastatin in 0.4%(40mg IQR 20mg). Ezetemibe was used in 274 patients (combined with simvastatin)
MP174 Table 1. Population demographics and mean lipid profile.
A&ACKD 2011/12n=17,590
Dispensed lipidtherapyn=10,096
Not dispensed lipidtherapyn=7,494
Mean difference(95% CI)
Median age(IQR) 77(12) 78(16)Mean age(SD) 75.4(9.6) 75.9(12.5) -0.5(-0.8,-0.2)Female(%) 61.0% 69.7% -1.44(-1.77,-1.12)Mean eGFR(SD) 47.15(11.24) 48.59(10.94) -1.44(-1.77,-1.12)Lipid profile
available(%)n=8,393(83.1%) n=3,960(52.8%)
Mean lipid profile(SD):
59.6% 67.3%
Cholesterol 4.30(1.03) 5.28(1.05) -0.98(-1.02,-0.94)HDL 1.30(0.40) 1.39(0.44) -0.09(-0.11,-0.07)Triglycerides 1.85(1.05) 1.70(0.95) 0.15(0.11,0.18)LDL 2.17(0.85) 3.12(0.86) -0.95(-0.99,-0.92)
Nephrology Dialysis Transplantation Abstracts
Volume 29 | Supplement 3 | May 2014 doi:10.1093/ndt/gfu167 | iiiDownloaded from https://academic.oup.com/ndt/article-abstract/29/suppl_3/iii380/1882504by gueston 25 March 2018

and 130 patients as monotherapy. Other lipid lowering therapies were used in 160patients.Conclusions: Despite being an evidence-based intervention in CKD, only 57% ofpatients were receiving lipid-regulating therapy with the majority receiving a Statin anda small number on alternative agents. Patients receiving lipid-regulating therapy had asimilar age and gender to those who did not, but females were less likely to be treated.Total and LDL cholesterol were significantly higher in the untreated population. Thereis a significant opportunity to improve the management of lipids in the CKDpopulation.
MP175 PREVALENCE AND RISK FACTORS FOR CHRONIC KIDNEYDISEASE AMONG HIV-INFECTED PATIENTS: RESULTSFROM A PORTUGUESE CENTER
Cátia Cunha1, Patrícia Barreto1, Susana Pereira1, Ana Ventura1, Margarida Mota1and Joaquim Seabra11Centro Hospitalar de Vila-Nova de Gaia, Vila-Nova de Gaia, Portugal
Introduction and Aims: As HIV-infected patients live longer with antiretroviraltherapy (ART), chronic kidney disease (CKD) becomes a more frequent reality in thesepatients. The aim of this study was to evaluate the prevalence and risk factors for CKDamong HIV-infected patients, followed in a specialized consultation in a Portuguesecentral hospital.Methods: In this retrospective study, glomerular filtration rate (GFR) was calculatedusing the Modification of Diet in Renal Disease (MDRD) equation. CKD was definedas GFR<60ml/min per 1,73m2 and/or proteinuria on urine dipstick on at least twoevaluations separated by a minimum of 3 months. Patients with CKD were selectedand data concerning risk factors of CKD was retrospectively collected from medicalrecords.Results: In a total of 837 patients, CKD was identified in 41 (5,8%), 39 males. Theywere followed for 7 years (±2,8) in average and all were infected by type 1 HIV. Theaverage age was 57 years (±12). Sixteen patients (39%) had estimated GFR < 60ml/min per 1,73m2, distributed as follows: 14 in stage 3 of CKD, one in stage 4 and onein stage 5, in haemodialysis. Proteinuria with normal renal function was found in 25patients (61%). All patients but one were on ART at the moment of analysis. Themedian of CD4+ cells count was 475/ul and plasma viral load was undetectable in71% of patients. HCV co-infection was present in 29% of cases and HBVco-infection only in 5%. Almost half of the patients were hypertensive (49%) and32% had known cardiovascular disease. More than half had dyslipidemia, 29% werediabetic and at least 22% were obese. Active smoking was present in 46% of patients.Metabolic syndrome, hypertension and cardiovascular disease were even moreprevalent when considering only patients with estimated GFR < 60ml/min per1,73m2.Conclusions: CKD is prevalent in this center. As HIV-infected patients live longer,important comorbidities as hypertension, dyslipidemia, obesity, cardiovasculardisease and diabetes become more frequent and, as in the general population, theybecome potential risk factors for renal disease. Screening and control of these riskfactors and routine screening for CKD are essential in these patients.
MP176 HOW LONG DOES IT TAKE FROMCKD ESTIMATED GFR10ML/MIN/1.73M2 TO THE INITIATION OF HAEMODIALYSIS?-THE COMPARISON OF DIABETIC NEPHROPATHY ANDOTHER CKDS
Toshifumi Sakaguchi1, Sou Kobayashi1, Takuro Yano1 and Wataru Yoshimoto11Rinku General Medical Center, Izumisano, Japan
Introduction and Aims: In ESRD, especially after CKD stage 5, it is important toknow the length to the initiation of haemodialysis in the context of preparation forrenal replacement therapy. It is plausible that diabetic nephropathy patients needhaemodialysis earlier than other CKD patients. However, no research clearly statedabout this issue so far. Therefore we try to make it clear.Methods:We compare the duration of the period from CKDeGFR10mL/min/1.73m2to the initiation of haemodialysis between diabetic nephropathy (Group 1) and otherCKDs (Group 2).One hundred seventy six patients were initiated haemodialysis in ourhospital for five years from 2009 to 2013. Necessary data were available for 122 patientsout of all the patients.Results: In Group 1 the number of patients was 67 including 38 men and 19 women.Their average age ± SD were 63.4 ± 11.8 and 72.7 ± 8.76 years old respectively. InGroup 2 the number of patients was 56 including 29 men and 27 women. Their averageage ± SD were 73.4 ± 13.3 and 69.8 ± 13.3 years old respectively. As for the length fromestimated eGFR 10mL/min/1.73m2 to the initiation of haemodialysis, the median was240 days, the 25th percentile was 111.5 days and the 75th percentile was 365 days inGroup 1. In Group 2, median was 341.5 days, the 25th percentile was 184 days, and the75th percentile was 557 days. There was significant difference between Group 1 andGroup 2 (Mann-Whitney U test, P<0.05)Conclusions: The duration was approximately 100 days longer in Group2 in median.This result may contribute for the preparation of haemodailysis. It may contributechoosing better timing of making AV-fistula, for example.
MP177 A POPULATION-BASED STUDYOF PREVALENCE ANDOUTCOMES OF CHRONIC KIDNEY DISEASE AMONG ADULTSIN CATALONIA
Ioana Bancu1, J. Bonal Bastons1, M. Cleries Escayola2, E. Vela Vallespin2,M. Bustins Poblet2, D. Magem Luque2 and M. Pastor Fabregas21Hospital Universitari Germans Trias I Pujol, Badalona, Spain, 2Servei Catala de LaSalut, Barcelona, Spain
Introduction and Aims: Chronic kidney disease (CKD) is a public health issue, withmajor clinical and economic impact, an independent predictor of mortality risk in thegeneral population, involving a high associated economic cost. Although CKDepidemiologic data is still partly lacking, efforts should be made to elaborateappropriate health strategies and plan resources.Therefore our aim is to offer acomplete updated report of CKD prevalence, clinical characteristics, mortality,pharmacologic treatment and estimate the cost among catalan population.Methods: Cross-sectional analysis of data from primary care, acute hospitals, mentalhealth institutions, Pharmacy Activity Register, including information andprescriptions of hospital outpatient dispensing medication and the date of deathcontained in the Central Register of Insured (CatSalut) at the end of 2012. Out of7.820.118 subjects contained in the database in 2012, we selected those with a codeCKD, a total of 152.711 patients.Results: The prevalence at 31 December 2012 was 1.776,6 per 100,000. The mean agein our population was 76.2, 92.7% of wich were previosly diagnosed with hypertension,36.9% with Diabetes Mellitus, and 59.1% with dyslipidemia. The overall mortality ratewas 9.8%, the rate of hospital admissions 59.5% and the average drug dispensing cost1,397.1€. As the renal function deteriorates, the use of specific drugs, such aserythropoietin (9.1% global, 63,4% HD), vitamin D (14.1% global, 50.0% HD), iron(30.1% global, 69.1% HD) and calcium (12.8% global, 36.2%HD) chelators increased.Conclusions: At the end of 2012, 2.3% of the total number of subjects (7.820.118)suffered from CKD. CKD was associated with a high mortality rate and considerablefinancial impact and differences were observed between different stages of the KDOQICKD classification.
MP178 ASSOCIATION OF INTERANKLE SYSTOLIC BLOODPRESSURE DIFFERENCEWITH PERIPHERALVASCULARDISEASE AND ECHOCARDIOGRAPHIC PARAMETERS INCKD
Jui-Hsin Chen1, Szu-Chia Chen1, Jer-Ming Chang2, Shang-Jyh Hwang3 andHung-Chun Chen31Kaohsiung Municipal Hsiao-Kang Hospital, Kaohsiung Medical University,Kaohsiung, Taiwan, 2Kaohsiung Municipal Hsiao-Kang Hospital, KaohsiungMedical University, KKaohsiung, Taiwan, 3Kaohsiung Medical University Hospital,Kaohsiung, Taiwan
Introduction and Aims: An interankle systolic blood pressure (SBP) difference hasbeen associated with overall and cardiovascular mortality in hemodialysis. Weinvestigated whether an association existed between this difference and ankle-brachialindex (ABI), brachial-ankle pulse wave velocity (baPWV), and echocardiographicparameters in patients with chronic kidney disease (CKD) stages 3-5.Methods: A total of 495 CKD patients referred for echocardiographic examinationwere included in the study. The four limb blood pressures were measuredsimultaneously by an ABI-form device.Results:We performed multivariate forward analysis for determining the factorsassociated with an interankle SBP difference ≧15 mmHg. The ABI < 0.9 (P < 0.001),high baPWV (P < 0.001) and increased left atrial volume index index (LAVI) (P =0.032) were associated with an interankle SBP difference ≧15 mmHg. Besides, theaddition of an interankle SBP difference ≧15 mmHg to a model of clinical featurescould significantly improve the value in predicting ABI < 0.9 (P < 0.001) and increasedLAVI (P = 0.034).Conclusions: Our study demonstrated that ABI < 0.9, high baPWV, and increasedLAVI were independently associated with an interankle SBP difference ≧15 mmHg.Besides, interankle SBP difference ≧15 mmHg could offer an extra benefit in predictingpatients with ABI < 0.9 and increased LAVI beyond conventional clinical features.Hence, calculation of interankle SBP difference may provide additional information inidentifying patients with peripheral vascular disease and increased LAVI in patientswith CKD stages 3-5.
MP179 AA AMYLOIDOSISWITH RENAL INVOLVEMENT:RETROSPECTIVE REVIEWOF 121 PATIENTS
Elbis Ahbap1, Ekrem Kara1, Taner Basturk1, Tuncay Sahutoglu1, Yener Koc1,Tamer Sakaci1, Mustafa Sevinc1, Cuneyt Akgol1, Ayse Aysim Ozagari1 andAbdulkadir Unsal11Sisli Etfal Educational and Research Hospital, Istanbul, Turkey
Introduction and Aims: AA amyloidosis is a multisystem, progressive and fataldisease, in which renal involvement occurs early. We aimed to investigate the clinicalfeatures of AA amyloidosis with renal involvement.
Abstracts Nephrology Dialysis Transplantation
iii | Abstracts Volume 29 | Supplement 3 | May 2014Downloaded from https://academic.oup.com/ndt/article-abstract/29/suppl_3/iii380/1882504by gueston 25 March 2018

Methods: One hundred and twenty-one patients (Male/Female: 84/37, mean age 42.6±14.4 years) were analyzed retrospectively between January of 2001-May of 2013.Clinical, laboratory and outcome data were obtained from follow up charts.
Results: Familial Mediterranean fever (37.2%) and tuberculosis (24.8%) were the mostfrequent causes of amyloidosis. Mean serum creatinine and proteinuria at diagnosiswere 2.3±2.1 mg/dl and 6.7±5.3 g/day, respectively. Stage I, II, III, IV and V renaldisease were present in 31.4%, 19.1%, 20.6%, 15.7%, and 13.2% of patients, respectively.Mean renal survival was 64.7±6.3 months. Sixty-eight (56.2%) of 121 patients requireddialysis. One, two and five year renal survival rates were 81.7%, 67.3% and 46.1%,respectively. Age, serum creatinine and albumin levels were the predictors of end stagerenal disease. Fifty patients (%41.3) died during follow up. Mean survival of patientswas 88.7±7.8 months (median: 63±13.9). One, two and five year patient survival rateswere 80.7%, 68.2% and 51.3%, respectively. Older age, male gender, lower BMI, GFR,serum albumin, Ca, and higher levels of P, iPTH and proteinuria were associated with ahigher mortality. Serum creatinine, albumin, dialysis requirement and short time todialysis were the predictors of mortality.Conclusions: The outcome of patients with AA amyloidosis and renal involvement ispoor, particularly in those who had massive proteinuria, severe hypoalbuminemia anddialysis requirement at the outset.
MP180 THE RENAL RESISTIVE INDEX IS ASSOCIATEDWITHCARDIOVASCULAR DISEASE IN PATIENTSWITHPREDIALYTIC CHRONIC KIDNEY DISEASE.
Satoshi Minami1, Atsushi Hesaka1, Satoshi Yamaguchi1, Eriko Iwahashi1,Shinsuke Sakai1, Taku Fujimoto1, Kouichi Sasaki1, Yoshimasa Fujita1 andKenji Yokoyama11Osaka Koseinenkin Hospital, Osaka-shi, Japan
Introduction and Aims: Recent studies have shown that the renal resistive index (RRI)is in relation to the systemic arteriosclerosis, but it is not clear that RRI is relevant toincident cardiovascular diseases (CVD). We studied retrospectively to elucidate theassociation of RRI with CVD incidence in patients with non-dialysis chronic kidneydisease (CKD).Methods: One hundred sixteen patients with CKD stage 4, 5 not on dialysis whounderwent Doppler ultrasound were retrospectively enrolled from a single departmentof nephrology as a hospital cohort from May 2008 to April 2013. For this study, weexcluded patients with malignancy (n=7), active infection (n=6), or renal arterystenosis (n=2) from enrollment. Analysis was based on the remaining 101 participants.ROC analysis was used to determine best cut-off value of RRI to predict CVDincidence, and patients were devided into 2 groups according to their RI values (Higroup; RI ≧0.75 and Lo group; RI < 0.75). In this study, CVD was deifined as theoccurence of stroke, of cardiac infarction, of angina pectoris and the hospitalization forheart failure. Survival analysis was performed using cumulative CVD event-freeKaplan-Meier curves and the curves were compared between the 2 groups by log-ranktest. Cox proportional hazard analysis was used to examine the association betweenvariables and cumulative incidence of CVD.Results: The median follow-up period was 32.4 months. Baseline median age was 64.0years old. Sixty-nine percents of total patients were men and 36% had diabetes mellitusand 35% had cardiovascular history. During the study period, CVD occurred in 29patients. The CVD incidence was significantly higher in patients with Hi group (HR =4.05, 95%CI =1.23 to 13.39) than with Lo group (reference) after the adjustment forage, gender, eGFR, urinary protein, and systolic pressure.Conclusions: These results suggest that the high value of RRI in patients with CKDstage 4, 5 not on dialysis was associated with the high CVD incidence.
MP181 DIFFERENCES IN COMORBIDITY BURDEN BETWEEN THOSEWITH CHRONIC KIDNEY DISEASE AND NORMAL RENALFUNCTION
Angharad Marks1, Nicholas Fluck1, Gordon Prescott1, Lynn Robertson1, WilliamC Smith1 and Corri Black11University of Aberdeen & NHS Grampian, Aberdeen, United Kingdom
Introduction and Aims: Chronic kidney disease (CKD) and renal replacement therapyare both associated with significant mortality and morbidity. Co-existing comorbidity
MP179
MP179
MP179
MP179
Nephrology Dialysis Transplantation Abstracts
Volume 29 | Supplement 3 | May 2014 doi:10.1093/ndt/gfu167 | iiiDownloaded from https://academic.oup.com/ndt/article-abstract/29/suppl_3/iii380/1882504by gueston 25 March 2018

is common. The degree to which the increased morbidity and mortality is a result ofthe CKD, and how much a result of the co-existing comorbidity is less clear. We aimedto describe the range of comorbidity at baseline in a population cohort containing allidentified within a healthcare region with CKD, those on RRT and a sample of 20,000individuals from the same population with normal renal function.Methods: The GLOMMS-II cohort contained all individuals with a low eGFR (<60)ml/min/1.73m2 measured in our healthcare region in 2003 (in 2/3 of these with “CKD”the low eGFR was present for at least 90 days, in 1/3 with “impaired eGFR” it was notpresent for at least 90 days); all those with raised PCR and ACR; all those receivingRRT and a 20,000 sample of those with only normal eGFR measurements in 2003.Data-linkage to hospital episode statistics in the five years prior gave information oncomorbidity in 2003. The prevalence of common comorbidities in the subgroups of thecohort is described. The odds of having each comorbidity at baseline with adjustmentfor age and sex are presented.Results: The prevalence of most comorbidities was higher in those with more advancedCKD (including RRT, as table). After correction for age and sex, vascular comorbidity,diabetes and haematological malignancy continued to be strongly associated with moreadvanced CKD. The association for other comorbidities was less marked, particularlyfor dementia. Impaired eGFR was also associated with many of these comorbiditiesConclusions:More advanced CKD was strongly associated with vascular comorbidityand diabetes even after correction for age. This association may in part be due to therole of these comorbidities in the aetiology of CKD, as well as a consequence. In theassessment of outcomes in CKD, the effect of these comorbidities on outcome over andabove that of CKD itself should be investigated further.
MP182 MORTALITY RATES OF DIALYSIS PATIENTS AND INCIDENCERATES OF ESRD INCREASED AFTER THE GREAT EASTJAPAN EARTHQUAKE AND TSUNAMI 2011
Masaki Ohsawa1, Tomoaki Fujioka2, So Omori2, Takashi Isurugi3, Kozo Tanno1,Toshiyuki Onoda1, Shinichi Omama2, Yasuhiro Ishibashi2, Shinji Makita2 andAkira Okayama41Iwate Medical University, Iwate Prefecture, Japan, 2Iwate Medical University,Morioka, Japan, 3Iwate Medical Association, Morioka, Japan, 4JpnAnti-Tuberculosis Assoc., Tokyo, Japan
Introduction and Aims: The Great East Japan Earthquake and Tsunami 2011 causedsignificant damage to people in Iwate Prefecture (North-east area in Japan). Patientswith end-stage renal disease (ESRD) are thought to be vulnerable for disasters andprolonged sedentary lifestyle during evacuation may contribute to worsening diabeticand hypertensive status of the refugees living in shelters. It is hypothesized thatmortality rates in patients with ESRD increased and incident rates of ESRD increasedin disaster area.Methods: The Iwate ESRD registry program based on inventory survey was initiated in2010 and this program has been continued to the present. We obtained data from thedatabase of Iwate ESRD registry program from Iwate Medical Association. We counttotal annual number of deaths in ESRD patients and total annual number of incidentESRD in Iwate Prefecture, respectively in 2010 and 2011 (disaster year) across the seacoast area (Tsunami disaster area) and inland region.Results: The results are shown in the table.
Conclusions:Mortality rates of ESRD patients and incidence rates of ESRD increasedafter The Great East Japan Earthquake and Tsunami 2011 in Tsunami-disaster area.
MP183 CAROTID ULTRASOUNDWITH PLAQUE QUANTIFICATION ISPREDICTIVE OF OCCLUSIVE CORONARY ARTERY DISEASEIN PATIENTSWITH ANDWITHOUT CKD
Jocelyn S Garland1, Christopher S Simpson1, Murray F Metangi1,Brendan Parfrey1 and Amer M Johri11Queen's University, Kingston, ON, Canada
Introduction and Aims: Coronary angiography is the clinical standard test to evaluatefor occlusive coronary disease, but can be nephrotoxic. Non-invasive methods to detectcoronary disease in chronic kidney disease (CKD) patients are desirable to enable riskstratification, cardiovascular disease (CVD) treatment and improved CVD morbidityand mortality in CKD. Quantification of maximal carotid artery plaque height is anemerging surrogate for coronary intimal atherosclerosis, and has been correlated withcoronary events in the general population. In CKD, maximal carotid artery plaqueheight has not been extensively evaluated. The primary objective of our study was todetermine if carotid artery disease quantified by carotid intimal media thickness(CIMT)and maximal carotid artery plaque height are predictive of occlusive coronaryartery disease in a population with and without CKD.Methods: 320 consecutive outpatients referred for clinically indicated coronaryangiography were recruited. Of these, 266 patients had data to estimate kidney function(MDRD eGFR) are were selected for this analysis. All patients had coronaryangiography and carotid ultrasound on the same day. Maximal carotid artery plaqueheight, and CIMT were measured by carotid ultrasound. CKD was defined as eGFR <60 ml/min/1.73 m2. Coronary artery disease was defined as at least 1 major epicardialcoronary artery with greater than 50% luminal narrowing as per coronary angiography.Results: Table 1 describes patient characteristics by the presence or absence of greaterthan 50% stenosis in at least one coronary artery by angiography. Patients withcoronary stenosis (es) had significantly increased maximal carotid artery plaque height(2.64 mm versus 1.81 mm; P<0.0001), whereas CIMT was not significantly differentbetween groups. By multivariable logistic regression adjusted for age, sex,hyperlipidemia , hypertension and CKD, maximal carotid plaque height was apredictor of coronary artery stenosis of 50% or more (Odds ratio 3.15; 95% confidenceinterval 1.99 to 4.98; P<0.0001). In considering only patients with renal disease (eGFR< 60; N=76) this relationship remained robust (Odds ratio 4.5; 95% confidence interval1.6 to 13; P=0.005).Conclusions: The maximal carotid plaque height, and not CIMT, was associated withclinically significant epicardial coronary artery stenosis in patients with and withoutCKD. Selecting which CKD patients could benefit from coronary angiography, despitethe potential nephrotoxicity, is important since CVD remains the most common causeof death in CKD. Carotid ultrasound with plaque quantification may serve to aid theselection of patients who would benefit from coronary angiography, and these resultsappear to be generalizable to the CKD population.
MP182 Number of prevalent ESRD, annual total number of deaths, annual total number of incident ESRD and th
2009/12/31 2010/1/1-12/31 2010/12/31 2011/1/1-2011-12/31
sea coastprevalent ESRD (/one million) 647 (3532) 697 (3842)annual No. of death (crude mortality) 36 (55.6/1000 pys) 69 (99.0/1000 pys)annual number of incident ESRD (crude incidence) 86 (0.47/1000 pys) 108 (0.60/1000 pys)inland areaprevalent ESRD 1952 (2142) 2043 (2249)annual No. of death (crude mortality) 189 (96.8/ 1000 pys) 214 (105/1000 pys)annual number of incident
ESRD (crude incidence)280 (0.31/1000 pys) 285 (0.31/1000 pys)
MP181
MP183 Comparison of patients with and without coronary stenosis
Variable Stenosis < 50% Stenosis > 50% P
Age 63.5 +/- 13 66.5 +/-11 0.07BMI 29.5 +/- 6 30.0 +/- 6 0.6eGFR 73.0 +/- 19 67.8 +/- 23 0.07smoker 13% 18% 0.44HTN 69% 74% 0.52Lipids 58% 80% 0.001Male 48% 75% 0.0001DM 26% 32% 0.43CIMT 0.84 +/- 0.2 mm 0.88 +/- 0.3 mm 0.18Plaq Ht 1.81 +/- 1 mm 2.64 +/- 0.9 mm 0.0001
Abstracts Nephrology Dialysis Transplantation
iii | Abstracts Volume 29 | Supplement 3 | May 2014Downloaded from https://academic.oup.com/ndt/article-abstract/29/suppl_3/iii380/1882504by gueston 25 March 2018

MP184 EXPERIENCE OF A SUPPORTIVE CARE CLINIC FORPATIENTSWITH ADVANCED CHRONIC KIDNEY DISEASE
Louise Sloan1, Jayne McAuley1, Ronan Cunningham1, Robert Mullan1,Michael Quinn1 and Camille Harron11Antrim Area Hospital, Antrim, United Kingdom
Introduction and Aims: Initiation of renal replacement therapy in patients withadvanced chronic kidney disease and significant other co-morbidities may not improvelife expectancy. In 2010, we established a supportive care clinic for patients withdeteriorating renal function who did not wish to pursue dialysis therapy. Patients arereferred to the supportive care clinic after they have chosen this option for ongoing careor where a joint decision has been made between patient and clinical team that dialysistherapy is unlikely to improve the quality or quantity of the patient's life. Patientsattending the clinic are assessed by a consultant nephrologist, consultant palliative carephysician, renal nurse specialist and a renal dietician. If patients are unfit to attend foroutpatient review, other arrangements are put in place for supportive care whichinclude virtual reviews, home visits and liason with community palliative care services.We wished to review the patient outcomes from this clinic.Methods:We have reviewed the records of patients who have attended the supportivecare clinic over a 4 year period from January 2010 until December 2013.We haveanalysed demographic details for the patients, renal function at the time of referral andultimate outcomes for the patients in terms of life expectancy and end-of-life care.Results: 39 patients have been referred to the supportive care clinic with all referralscoming from the Low Clearance (Pre-dialysis) Clinic. Average age at the time of referralwas 85 years (range 66 to 100 years). 51% of patients have been male. Average eGFR(estimated Glomerular Filtration Rate) at time of referral was 11.3ml/min with amedian of 8ml/min (range 3 to 42 ml/min).The current cohort of supportive carepatients is 14 which represents 7.2% of the patients attending for 'pre-dialysis' care andeducation. The median age of these patients is 88.5 years (range 78 to 96 years) with amedian eGFR of 14 ml/min (range 5 to 24 ml/min). 21% of these patients have becomeunfit to attend clinic and are under virtual review (electronic review of laboratoryresults and symptom assessment by telephone). Average length of follow-up is 66 dayswith longest follow-up 526 days.24 patients have died. The average length of follow-upbetween decision to pursue supportive care and death has been 95 days (range 14 to803 days). The largest proportion of these patients (45.5%) died in their usual place ofresidence with 33% dying in their own home and 12.5% dying in a nursing home. 42%of patients died as hospital inpatients with 12.5% dying in a specialist palliative careunit. For those patient who died as inpatients previous discussions from the supportivecare clinic were able to inform care at the end of life.Conclusions: Development of a supportive care renal clinic has improved the choice ofcare available to patients with advanced chronic kidney diease. The aim of the clinic isto optimise symptom control, focus on palliative care with a view to optimising qualityof life and to plan for end-of-life care when required. Ongoing studies will look at thedegree of comorbidity affecting these patients and life expectancy compared toage-matched patients who chose to pursue active plans for renal replacement therapy.
MP185 ADVANCING QUALITY IN PROVINCIAL END-OF-LIFE CAREFOR PATIENTSWITH KIDNEY DISEASE IN CANADA
Helen Chiu1, Donna Murphy-Burke1, Ronald Werb2, Beverly Jung2,Clifford Chan-Yan2, John Duncan2, Brian Forzley2, Robin Lowry2,Gaylene Hargrove2, Rachel Carson3, Adeera Levin2, Mohamud Karim2 and eSteering Committee On Behalf Of The British Columbia Renal End-Of-Lif1BC Provincial Renal Agency, Vancouver, BC, Canada, 2The University of BritishColumbia, Vancouver, BC, Canada, 3Nanaimo Regional General Hospital,Nanaimo, BC, Canada
Introduction and Aims: Acknowledging the needs and importance of deliveringquality end-of-life (EOL) care for renal patients, the British Columbia Provincial RenalAgency (BCPRA) developed a provincial EOL framework which articulated four pillarsof EOL care: Patient identification, advance care planning, symptom assessment &management and care of the dying patient & bereavement. As set out in theframework, the need to assess both processes and outcomes are essential to qualityimprovement in each of these four areas of EOL care. We aimed to develop andimplement an evaluative framework which will provide data for strategic planning andcontinuous quality improvement in EOL care for renal patients.Methods: An environmental scan was conducted to assess current state andperceptions of EOL care among care providers using a survey and interviews withindividual EOL champions in the Health Authority Renal Programs (HARPs).Literature review was carried out to identify tools for measuring the quality of dyingand death from various perspectives.Results: Implementation of the EOL framework varies across the HARPs with eachhaving formalized strategies to facilitate ongoing growth in EOL care. Specifically,prominent improvements were shown in symptom care & management and advancecare planning. The majority of survey respondents deemed standardizing agreed-uponmeasures (79%) and evaluating EOL care at a provincial level (93%) provincially as“very” and “moderately” important on a 5-point Likert scale. Key challenges identifiedinclude enabling the organizational culture, sustaining quality EOL care and continualimprovement.Conclusions: From the environmental scan, we were able to identify enablers, barriers
and opportunities in advancing EOL care provincially. Our next steps include selectionand testing of tools for measuring quality of death, establishing provinciallyagreed-upon outcome and process measures for population-based monitoring ofprogress for continual improvement in EOL care for renal patients, their families andcaregivers.
MP186 COMPARISON OF CREATININE-BASED EQUATIONS FORESTIMATION OF RENAL FUNCTION IN CHRONIC HEARTFAILURE PATIENTS
Elena Vl Reznik1 and Gennady I.V. Storozhakov11Russian National Research Medical University, Moscow, Russian Federation
Introduction and Aims: The renal dysfunction is common and related with the poorprognosis in the chronic heart failure (CHF). The glomerular filtration rate (GFR) has aparamount diagnostic role in the chronic kidney disease (CKD). Cystatin C improvesestimation of GFR over creatinine alone; however, the association between most of therisk factors and GFR is more accurate by GFR based on creatinine alone. The mostwidely used creatinine-based GFR formulas are the Cockcroft-Gault (CG),Modification of Diet in Renal Disease Study (MDRD) and Chronic Kidney DiseaseEpidemiology Collaboration (CKD-EPI) equations. The MDRD equation limitationsare imprecision and systematic underestimation of measured GFR at higher levels. TheCKD-EPI formula is more accurate than others in numerous populations, but it hasnot been studied well in CHF. Our aim was to compare nine different equations forestimation of renal function in CHF patients.Methods: 154 systolic CHF patients I-IV New York Heart Association (NYHA)functional class without primary renal, autoimmune and oncological diseases werestudied. Median (interquartile range) of age was 64.0 (56.0-69.0) years; left ventricularejection fraction (Simpson) was 30.4 (25.3-37.1)%, 86.4% were male. We calculated theglomerular filtration rate (eGFR) by CG, original 4-variable MDRD (4MDRD),2-variable MDRD (2MDRD), simplified MDRD (sMDRD), CKD-EPI, Jellife 1 and 2,Gates, Salazar-Corcoran equations and measured urinary albumin excretion (spot and24h UAE). All patients were stable on optimal medical therapy.Results: Serum creatinine was 103.0 (87.0-120.0) mcM, eGFR CKD-EPI 65.0(49.8-80.3) ml/min/1.73m2, spot UAE 20.3 (6.8-38.7) mg/ml, 24h UAE 43.8(31.6-71.0) mg/24h. eGFR CKD-EPI did not differ from eGFR 4MDRD [64.3(50.2-81.1) ml/min/1.73m2, p>0.05]. eGFR CKD-EPI was lower than eGFR CG [68.6(51.5-96.2) ml/min/1.73m2, p<0.001], eGFR 2MDRD [65.4 (50.0-79.7) ml/min/1.73m2, p<0.001], eGFR Jellife2 [76.9 (64.0-95.3) ml/min/1.73m2, p<0.001], eGFRGates [77.9 (61.4-95.3) ml/min/1.73m2, p<0.001], eGFR Salazar-Corcoran [79.1.0(61.9-102.4) ml/min/1.73m2, p<0.001]. eGFR CKD-EPI was higher than eGFRsMDRD [61.4 (47.4-74.7) ml/min/1.73m2, p<0.001], eGFR Jellife 1 [59.3 (45.9-72.3)ml/min/1.73m2, p<0.001]. eGFR CKD-EPI correlated with other eGFR: CG r=0.75,4MDRD r=0.97, 2MDRD r=0.99, sMDRD r=0.99, Jellife 1 r=0.97, Jellife2 r=0.96, Gatesr=0.96, Salazar-Corcoran r=0.93 (p<0.001 for all), spot UAE r=-0.24 (p=0.025), 24hUAE r=-0.27 (p=0.018). Based on eGFR CKD-EPI, there were 46.4%, 39.3% and 1.4%patients with CKD Stages 2-4, respectively. There were not significant differences inCKD stage estimated using CKD-EPI, 4MDRD and 2MDRD eqaitions (p>0.05). 10.7%of CHF patients were accurately reclassified into higher CKD classes with CKD-EPI incomparison with sMDRD, p<0.001. 32.7% of CHF patients were reclassified into lowerand 9.9% into higher CKD classes with CKD-EPI in comparison with CG equation,p<0.001. Limitations of our study are old age of patients, absence of racial and ethnicminorities, absence of measured GFR.Conclusions: The CKI-EPI equation and original 4-variable MDRD may be thepreferred creatinine-based GFR estimation method in chronic heart failure patients,particularly those with mild and moderate renal dysfunction.
MP187 EPIDEMIOLOGYOF NEPHROPATHIES IN IRREGULARIMMIGRANTS IN NORTHERN ITALY
Cristiana Rollino1, Michela Troiano1, Matteo Bagatella2, Chantal Liuzzo3,Francesco Quarello4 and Dario Roccatello11Division of Nephrology and Dialysis and Center of Immunopathology and RareDiseases, Coordinating Center of Rare Diseases of Piedmont and Aosta Valley, StGiovanni Bosco Hospital and University of Turin, Torino, Italy, 2ISI Center - ASL To2, Torino, Italy, 3ISI Center - ASL To 2, Torino, Italy, 4Nephrology - OspedaleS. G. Bosco, Torino, Italy
Introduction and Aims: Free movement within the European Union is granted by theSchengen Agreement. Transnational trips are expected to increase in 2014 with thepossible addition of Romania and Bulgaria to the Schengen area.The World HealthOrganization stated that ”there is a need to assess trends in migrants’ health byimproving country health information systems, which can help identify and fill gaps inservice delivery”. Data regarding the incidence of specific nephropathies in immigrantsare lacking.Aim of our study was to evaluate the prevalence of renal disease in irregularimmigrants in Turin, the main metropolitan area of north-western Italy bordering onFrance, which is strongly affected by irregular immigration.Methods: The study was sponsored by the Italian Society of Nephrology andconducted in the health reception facility for immigrants of our Hospital from January2012 to December 2012.A 7 language questionnaire-based survey was administered
Nephrology Dialysis Transplantation Abstracts
Volume 29 | Supplement 3 | May 2014 doi:10.1093/ndt/gfu167 | iiiDownloaded from https://academic.oup.com/ndt/article-abstract/29/suppl_3/iii380/1882504by gueston 25 March 2018

regarding signs, symptoms and familiarity for renal disease. The study also includeddirect assessment of GFR with EPI equation, urinalysis and blood pressuremeasurement.Results: Data regarding 494 irregular immigrants (287 women, 207 men), mean age36.9±12 years, 167 black, 11 Asians, and 316 Caucasians living in Italy for 6.2±5.8years, were examined.Four people reported familiarity for nephropathies (2 kidneystone diseases, 2 Autosomal Dominant Polycystic Disease).Arterial hypertension wasfound in 29 subjects (5.8%). Mean serum Creatinine (sCr) was 0.79±0.25 mg/dl (range0.6-3 mg/dl), GFR-EPI 109±23.7 ml/min/1.73mq. 13 patients (2.6%) presented renalfailure (RF), 10 of whom also had urinary abnormalities and/or hypertension.Hematuria was found in 55 subjects (11.1%), proteinuria in 67 (13.5%) and bothhematuria and proteinuria (without RF) in 15 (3%). Eight subjects had glycosuria, onedue to previously unknown diabetes and one to renal glycosuria. A case of urinary eggsof Schistosoma mansoni was detected. Four patients had kidney stones.99 patients(20%) were summoned (30 did not turn up): 41 needed nephrologic follow-up, butonly 8 showed up a second time.Conclusions: Signs of nephropathy were detected in 116 (23.4%) irregular immigrants,a figure much higher than the epidemiologic expectancy of 39 cases among the Italianpopulation residing in the same area.
MP188 WAIST TO HEIGHT RATIO IS INDEPENDENTLY ASSOCIATEDWITH CHRONIC KIDNEY DISEASE IN OVERWEIGHT TYPE 2DIABETIC PATIENTS
Kristina Blaslov1, Tomislav Bulum2, Ingrid PrkacIn1 and Lea Duvnjak11University Hospital Merkur, School of Medicine, University of Zagreb, Zagreb,Croatia, 2University Hospital Merkur, Zagreb, Croatia
Introduction and Aims: Chronic kidney disease (CKD) i.e. diabetic nephropathy isone of the most serious complications of central obesity-induced type 2 diabetesmellitus (T2DM). Body mass index (BMI), waist circumference (WC), and waist-to-hipratio (WHR) are traditional tools to detect obesity and higher risk of micro- andmacrovascular complications in T2DM. Waist-to-height ratio (WhtR) was also recentlyreported to be associated with CKD in non diabetic patients. The aim of our study wasto investigate the predictive power of BMI, WC, WHR and WHtR for CKD prevalencein overweight T2DM patients.Methods: Study included 125 overweight (BMI≥35 kg/m2) T2DM patients. Basicanthropometric measurements were performed on all study subjects by the samephysician. GFR was estimated using the Chronic Kidney Disease EpidemiologyCollaboration (CKD-EPI) formula. Urine albumin excretion (UAE) was measuredfrom at least two 24-h urine samples. CKD was defined as the presence of impairedeGFR (less than 60 mlmin-11.73m-2) and/or macroalbuminuria (UAE≥300 mg/24h).Validity of the each test was assesses by receiver operating characteristic (ROC curves;the area under the curves (AUCs) and calculated for each anthropometrical parameter(BMI, WC, WHR, WHtR) and risk condition (CKD).Results: Among the 125 T2DM patients 65 (52%) were male and 60 (48%) female,with median age of 58 years and 36 (29%) with CKD. The results from ROC analysis ofthe four anthropometric indices for CKD shows that AUCs for WHtR was significantlyhigher than AUC for WC with respect to CKD, while the AUCs for otheranthropometric parameters suggest that those predictors are not to be considered asvalidated tests. In the logistic regression models of the CKD in case of an increase ofone SD of the respective anthropometric parameter, only WHtR yielded the significantand great OR of 1.69 (CI 1.12-1.89, P<0.05) in association to nephropathy afteradjustment for age, gender, disease duration, HbA1c, dyslipidaemia, arterialhypertension and smoking status.Conclusions: Our study results indicate that WHtR might be of a greater importanceas a risk factor in CKD development than other anthropometric parameters thatindicate obesity in overweight T2DM patients. High sensitivity but low specificity ofWHtR in predicting CKD is clearly important because it might give a possibility toidentify the disease and could be used as a good screening test.
MP189 NEPHROLOGICAL AWARNESS AND DRUG ADHERENCE INPATIENTSWITH CHRONIC KIDNEY DISEASE (CKD).
Zbigniew Heleniak1, Magdalena Cieplinska1, Tomasz Szychlinski1,Magdalena Pryczkowska1, Ewa Bartosinska1, Hanna Wiatr1, Hanna Kotłowska1,Leszek Tylicki1 and BolesłAw Rutkowski11Nephrology, Transplantology and Internal Medicine Department MedicalUniversity of GdańSk, Gdańsk, Poland
Introduction and Aims: Awareness of CKD and medical adherence among patients islow. The aim of presented study was to assess the basic nephrological knowledge anddrugs adherence among persons with CKD in Gdańsk Nephrology Center in PolandMethods: A total of 888 adult participants of the cross-sectional study responded to aquestionnaire regarding their use of drugsResults: General characteristic of the study group is in the table 1.87,7% and 78,9% ofrespondents indicated as an indicator of renal injury the level of serum creatinine andproteinuria respectively. 70.8% knew the concept of eGFR.The most often drugs usedby our patients were: hypotensive agents (67,5%),vitamins (32,8%), statins (27,8%).The average number of drugs received per day was 5. The time from diagnosis of CKD
was connected with using higher number of drugs (p<0,05)72.4% of patients alwaysbuys drugs prescribed by a doctor. In case they didn’t make a purchase of drugs only68,4% of them informed the doctor about it. 86,9% of patients take drugs regularly.85.5% know the names of drugs they used.When patients change dosing of theirmedicines without doctor’s consultation, it is due to wit forgetfulness, side effects andlack of treatment effect in 56,6%, 25,6% and 13,2% respectivelyConclusions: Nephrological awareness in our CKD group was quite high. In contrast,drugs adherence was low. Patients with CKD use a large amount of drugs. It isnecessary to systematically repeat the patient’s education concerning the benefits ofregular using medication
MP190 B-TYPE NATRIURETIC PEPTIDE PREDICTS AN ISCHEMICETIOLOGYOF ACUTE HEART FAILURE IN PATIENTSWITHSTAGE 4-5 CHRONIC KIDNEY DISEASE
Young Rim Song1, Sung Gyun Kim Kim2, Hyung Jik Kim2 and Jung Woo Noh31Hallym University College of Medicine, Anyang-si, Republic of Korea, 2HallymUniversity Sacred Heart Hospital, Anyang-si, Republic of Korea, 3Hallym UniversityKangnam Sacred Heart Hospital, Seoul, Republic of Korea
Introduction and Aims: The non-invasive differentiation of ischemic andnon-ischemic acute heart failure (AHF) not resulting from acute myocardial infarctionis difficult and has therapeutic and prognostic implications. The aim of this study wasto assess whether serum B-type natriuretic peptide (BNP) can identify ischemicetiology in patients with stage 4-5 chronic kidney disease presenting with AHF.Methods:We prospectively analyzed 61 patients. The diagnosis of ischemic AHF wasconfirmed by coronary angiography or stress myocardial perfusion imaging. Plasmalevels of BNP were measured at admission (BNP1) and 48 h after admission (BNP2).Results: The mean age was 67 years; 70.5% had diabetes and 47.5% weredialysis-dependent CKD. Twenty-eight (45.9%) had an ischemic etiology and theconcentrations of BNP1 and BNP2 were significantly higher in patients with ischemicetiology than those without ischemia. The area under the receiver operatingcharacteristic curve was 0.755 (P = 0.001) for BNP1 and 0.868 (P < 0.001) for BNP2 todetect ischemic etiology of AHF. Serum BNP1 > 2907 ng/L (odds ratio [OR], 10.9; 95%confidence interval [CI] 2.5-48.4; P = 0.002) and BNP2 > 2322 ng/L (OR 93.1, 95% CI7.0-1238.7; P = 0.001) were independently associated with an ischemic etiology ofAHF.Conclusions: Plasma BNP may represent a clinically useful non-invasive tool foridentification of ischemic etiology of AHF in patients with stage 4-5 chronic kidneydisease
MP191 BELIEFS AND EXPERIENCES OF PREGNANCY INWOMENWITH CHRONIC KIDNEY DISEASE: SYSTEMATIC REVIEWOFQUALITATIVE STUDIES
Allison Tong1, Shilpanjali Jesudason2, Jonathan C Craig1 and WolfgangCWinkelmayer31The University of Sydney, Sydney, Australia, 2Royal Adelaide Hospital, Adelaide,Australia, 3Stanford University, Palo Alto, CA
Introduction and Aims: Achieving parenthood in women receiving renal replacementtherapy is challenging due to reduced fertility and the substantially higher risk ofadverse outcomes. Clinical decision-making and management involves weighing thepotential complications of accelerated decline in renal function, maternal morbidity,perinatal loss, pre-eclampsia, and poor fetal outcomes against the preferences andvalues of women with chronic kidney disease (CKD). We aimed to describe theperspectives and experiences of pregnancy in women across all stages of CKD.Methods:MEDLINE, Embase, PsycINFO, CINAHL, reference lists and PhDdissertations were searched to September 2013. We included any qualitative study thatexplored the perspectives of women with CKD on their knowledge, decisions, beliefs,and experiences of pregnancy. Studies were imported into HyperRESEARCH software,coded, and synthesized thematically.Results: Eleven studies involving 250 women with CKD (haemodialysis [n=72],peritoneal dialysis [n=16], kidney transplantation [n=45], unspecified modality[n=117]) were included. Six themes were identified. Pursuing motherhood was drivenby the need to fulfill their own or their partner’s desire to have a child, and a social role.Failure and blame described the responsibility and guilt of being unable to conceive
MP189 Table 1 General characteristic of the study participants
UNIT VALUE
Amount of participants 888Gender F/M 417/471Average age years 54,71Time of control in Nephrological Outpatients Clinic years 9,61Average time of chronic kidney disease years 13,9Average level of serum creatinine mg/dl 1,7Average level of eGFR (MDRD) ml/min 42,69
Abstracts Nephrology Dialysis Transplantation
iii | Abstracts Volume 29 | Supplement 3 | May 2014Downloaded from https://academic.oup.com/ndt/article-abstract/29/suppl_3/iii380/1882504by gueston 25 March 2018

which diminished their sense of self-worth and value. Fear of birth defects was mostlyattributed to the potential side effects of immunosuppression in kidney transplantation.Insecurity in decision making encompassed the uncertainties of prioritising pregnancyas this meant considerable sacrifices had to be made in the areas of family life and workto minimise their risk of pregnancy complications, and kidney transplant recipientswere concerned about the increased likelihood of graft loss. Also, for patients withautosomal dominant polycystic kidney disease, the possibility of genetic transmissioninfluenced their decisions about childbearing.Withholding emotional investment wasreported in some participants as a way of protecting themselves from thedisappointment and devastation of inability to conceive, miscarriage or stillbirth.Control and autonomy reflected their capacity to choose to accept the risks ofpregnancy, while some described feeling traumatised when their physician undulywarned against pregnancy.Conclusions: Inability to conceive caused a pervading sense of guilt, disappointmentand social devaluation in women with CKD. Also, decisions about pregnancy can beemotionally complicated by the threat to their own health, burden on their family, andthe perceived risk of delivering a malformed baby. Women can feel confronted whenadvised to avoid pregnancy. Shared and informed decision making about pregnancy inCKD may be enhanced by developing clinical decision aids that integrates evidence onpregnancy outcomes and patient’s preferences. Multidisciplinary care involvingnephrologists, reproductive and obstetrics specialists, and access to psychologicalsupport, are also suggested to help patients resolve decisional conflict and improvetheir confidence in managing pregnancy issues in CKD.
MP192 YOUNG STROKE PATIENTS ARE AT HIGH RISK FORSUBSEQUENT ESRD: A POPULATION-BASEDOBSERVATIONAL STUDY
Peir Haur Hung1,2, Yu Tung Huang3, Chih Yen Hsiao1, Pi Shan Sung4,5, HowRan Guo4,5 and Kuen Jer Tsai41Ditmanson Medical Foundation Chia-Yi Christian Hospital, Chia-yi City, Taiwan,2Chia-Nan University of Pharmacy and Science, Tainan City, Taiwan, 3ChangGung University of Science and Technology, Taoyuan County, Taiwan, 4NationalCheng Kung University, Tainan City, Taiwan, 5National Cheng Kung UniversityHospital, Tainan City, Taiwan
Introduction and Aims: An increased incidence of end stage renal disease (ESRD) instroke patients has not been confirmed. The aim of this population-based study was toexamine the risk of ESRD in stroke patients in Taiwan.Methods:We conducted a nationwide cohort study of 442355 patients newlydiagnosed with stroke, but without prior history of ESRD. Data were collected fromTaiwan’s National Health Insurance claims data during 2000-2008. Incidence andstandardized incidence ratio (SIR) of ESRD were calculated using the generalpopulation of Taiwan as the reference.Results: Among all stroke patients, 7813 (1.77%) developed ESRD with a meanfollow-up of 4.11 years. The SIR for ESRD was 2.78 (95% CI 2.72 to 2.84) among strokepatients of all ages and was 22.73 (95% CI 20.39 to 25.20) for patients aged 25-44 years.Male patients with stroke had a higher risk of ESRD (SIR 2.94, 95% CI 2.85 to 3.03)among stroke patients of all ages and it was 23.41 (95% CI 20.46 to 26.36) for malepatients aged 25-44 years.Conclusions: Increased risk of ESRD in stroke patients is confirmed in Taiwan, andmale patients between ages 25-44 years were at higher risk of ESRD compared withtheir counterparts in the general population. The clinical implication of our results is toclosely monitor renal function in stroke patients, particularly those of younger age.
MP193 RISK FACTORS FOR CHRONIC KIDNEY DISEASE INSPECIFIC HIGH RISK PATIENTSWITH DIABETESMELLITUSAND HYPERTENSION IN TAIWAN
Chia-Chao Wu1, Sui-Lung Su2, Sen-Yeong Kao2, Kuo-Cheng Lu3 andYuh-Feng Lin41Division of Nephrology, Department of Medicine, Tri-Service General Hospital,Taipei, Taiwan, 2School of Public Health, National Defense Medical Center, Taipei,Taiwan, 3Division of Nephrology, Department of Medicine, Cardinal Tien Hospital,School of Medicine, Fu Jen Catholic University, New Taipei City, Taiwan, 4Divisionof Nephrology, Department of Medicine, Shuang Ho Hospital, Graduate Institute ofClinical Medicine, Taipei Medical University, New Taipei City, Taiwan
Introduction and Aims: Taiwan has the highest prevalence and incidence of end stagerenal disease in the world. The majorities were due to diabetes mellitus (DM) orhypertension (HTN). However, the characteristic risk factors for the development ofchronic kidney disease (CKD) in each specific high risk population in Taiwan regionare still unclear. This study surveyed the most common risk factors and identified theireffects on CKD in general population or patients with HTN and/or DM in Taiwan.Methods: This study included 5328 cases and 5135 controls in CKD/HTN/DMoutpatient department and health center of 10 hospitals from 2008 to 2010. Forteencommon risk factors were surveyed (4 of demographic factors, 5 of isease factors and 5of lifestyle factors) and checked their impact on CKD evelopment. Variables withsignificant heterogeneity between patients with ifferent comorbidities were stratifiedanalysed.
Results:Male,aging, low incomes, hyperuricemia and no exercise hbits were riskfactors of CKD; and their impact on people with dfferent comorbidities were the same.Anemia also was a risk factor, and there ws an additive effect between anemia andhypertension on CKD. The association btween hyperlipidemia related factors and CKDwas moderated by HTN; it was a significant risk factor in people without HTN but notin patient with HTN. Based on the power of this study, we considered that hepatitis Bsmoking, alcohol intake and groundwater using might not the important risk factors ofCKD. The associations between hepatitis C/betelnut chewing and CKD wre notconclusive.Conclusions: Several risk factors in each specific high risk population had beenidentified in Taiwan. We considered that screening/preventing strategy on CKD in eachhigh risk patients might differ from health population. Further larger studies areneeded for more strong statistical power.
MP194 ACOMPARISON OF PROGNOSIS FACTORS BETWEENPATIENTS OF CHRONIC KIDNEY DISEASE STAGE 3WITHANDWITHOUTMETABOLIC SYNDROME
Wei-Hung Lin1, Hui-Mei Lee2, Meng-Fu Cheng3, Wei-Ming Wang4, Li-Yu Yang2
and Ming-Cheng Wang51National Cheng Kung University Hospital, Tainan, Taiwan, 2Department andGraduate Institute of Nursing, College of Medicine, Kaohsiung Medical University,Kaohsiung City, Taiwan, Kaohsiung, Taiwan, 3Institute of Clinical Medicine, Tainan,Taiwan, 4Biostatistics Consulting Center, National Cheng Kung University Hospital,Tainan, Taiwan, 5Division of Nephrology, Department of Internal Medicine, NationalCheng Kung University Hospital, College of Medicine, National Cheng KungUniversity, Tainan City, Taiwan, Tainan, Taiwan
Introduction and Aims: The 2011 United States Renal Disease Database (USRDS)showed the prevalence of end stage renal disease (ESRD) in Taiwan was second highestin the world. There is a trend of increasing rate in chronic kidney disease (CKD)combined with metabolic syndrome (MS) year by year. Previous studies revealed thatMS would worsen the decline of renal function. However, so far there is no studyfocusing on the association between self-care, population characteristics and riskfactors with prognosis among patients of CKD combined with MS. The goal of ourstudy is to predict the important factors associated with the prognosis of CKD, todevelop the prevention strategy which may slow the decline of renal function and todelay the entrance of ESRD.Methods: This was a retrospective cohort study. We enrolled total 465 patients in CKDstage 3 under the nationwide CKD Preventive Project with multidisciplinary careprogram at a tertiary medical center in Southern Taiwan. From chart review weinvestigated the association between self-care, population characteristics and riskfactors with prognosis among patients of CKD combined with or without MS.Furthermore, we found the main determining factors effecting outcome by statisticsanalysis including t-test, Chia-Square and Kaplan-Meier survival estimate.Results: The results showed CKD with MS, young aged, irregular blood pressure
MP194 Characteristics of CKD with or without MS
CKD with MS (N=291) CKD without MS (N=193) P Value
Male 213 (73.2%) 146 (75.6%) 0.61Religion 238 (81.8%) 153 (79.3%) 0.57Marriage 256 (88.7%) 178 (92.2%) 0.18Education 113 (38.8%) 96 (49.7%) 0.02*Compliance 262 (90.0%) 171 (88.6%) 0.73Exercise 144 (49.5%) 98 (50.8%) 0.85Sugar control 131 (45.0%) 124 (64.2%) <0.01*BP monitor 218 (76.8%) 144 (74.6%) 1.00Smoking 41 (14.1%) 26 (13.5%) 0.79Drinking 27 (9.5%) 11 (5.7%) 0.35Betel nut 5 (1.7%) 4 (2.1%) 0.14Analgesics 40 (13.7%) 27 (14.0%) 1.00
MP194
Nephrology Dialysis Transplantation Abstracts
Volume 29 | Supplement 3 | May 2014 doi:10.1093/ndt/gfu167 | iiiDownloaded from https://academic.oup.com/ndt/article-abstract/29/suppl_3/iii380/1882504by gueston 25 March 2018

monitor were significantly associated with outcome of ESRD. The hazard ratio forESRD among CKD with MS was 7.31 compared with CKD without MS.Conclusions: In conclusion, we should pay more attention to identify the risk factorsof MS among CKD patients and educate for the importance of home blood pressurecheck to improve the understanding, detection and management of CKD with MS.
MP195 IMMIGRANT STATUS IN A BALKAN AREAOF ENDEMICNEPHROPATHY IS A NEGATIVE PREDICTOR FOR PROXIMALTUBULE DAMAGE
Ivana Vukovic Lela1,2, Maja Sekoranja3, Tamara Poljicanin3, Sandra Karanovic1,2,Mirta Abramovic4, Vesna Matijevic5, Zelimir Stipancic6, Ninoslav Leko7,Ante Cvitkovic8, Zivka Dika1,2, Jelena Kos1, Mario Laganovic1,2, ArthurP. Grollman9 and Bojan Jelakovic1,21University Hospital Center Zagreb, Zagreb, Croatia, 2School of Medicine,University of Zagreb, Zagreb, Croatia, 3Croatian National Institute of Public Health,Zagreb, Croatia, 4Outpatient Clinic Bebrina, Bebrina, Croatia, 5Outpatient ClinicSlavonski Kobas, Slavonski Kobas, Croatia, 6Department for Nephrology andDialysis Orasje, General Hospital Odzak, Odzak, Bosnia and Herzegovina,7General Hospital "Dr Josip Bencevic", Slavonski Brod, Croatia, 8Institute forPublic Health Brodsko-Posavska County, Slavonski Brod, Croatia, 9Stony BrookUniversity, Stony Brook, NY
Introduction and Aims: Endemic nephropathy (EN) represents a form of aristolochicacid nephropathy (AAN) where AAwas ingested via contaminated bread.Improvement in agriculture that took place 20-30 years ago significantly decreasedcontamination of flour with AA. We hypothesized that a group of immigrants fromBosnian non-EN area who settled Croatian EN area in that period, due to the lack ofexposure, could not be at risk for developing EN.Methods: According to EN consensus criteria, we analysed proximal tubule damage(PTD) = α1microglobuline/creatinine (Alfa1CR)> 31.5 mg/g and renal function (CKD= eGFR <60ml/min/1.73m2) in 2 161 farming villagers who were divided into 3groups: autochthonous inhabitants of EN (N=1687) and non-EN villages (N=372), andimmigrants (N=102).Results: Diseased and suspect of having EN had higher alfa1CR values thanimmigrants (102vs.48vs.7.04; p0.05). Immigrants had significantly lower prevalence ofPTD (1.3% vs.3.0%vs.8.3%) and CKD (5.9% vs. 8.9% vs.15.8%) than non-EN and ENvillagers, respectively (for both p<0.001). No EN case was detected in immigrants.Immigrant status was found to be independent negative predictor of PTD (OR 0.35;95%CI 0.14-0.86;p=0.022), unlike positive family history for EN which was stronglypositive predictor (OR 2.31;95%CI 1.43-3.74;0.001). As we reported, 20 years agoimmigrants observed significantly less A.clematitis and their seeds, and less frequentlybaked bread compared to EN villagers (p<0.001).Conclusions: Due to improvements in agriculture exposure to AA, an environmentaltoxic agent for EN is decreasing. Our result on negative predictive value of immigrantstatus strongly confirms this presumption. Attenuation of exposure to AAwill probablylead to decrease in prevalence and subsequently disappearance of EN.
MP196 PREVALENCE OF CKD IN RANDOMLY SELECTED 20 CITIESALLOVER THE POLAND IS DEPENDENTON AGE
Teresa Dryl-Rydzynska1, Tomasz Prystacki1 and Jolanta Malyszko21FMC, Poznan, Poland, 2Med Univ, Bialystok, Poland
Introduction and Aims: Prevalence of chronic kidney disease is about 10-16%, mainlyin the elderly. According to guidelines glomerular filtration rate-GFR below 60 ml/minis associated with the increased risk of cardiovascular morbidity and mortality. Earlydetection of chronic kidney disease (CKD) is particularly important in patients withsuch risk factors as diabetes, hypertension and in the elderly. There are not so manypopulation studies assessing the prevalence of CKD, the only one Polish study on theepidemiology of CKD was PolNef regions of performed in 3 selected regions in
Pomerania in North Poland. Taking into consideration time elapsed after PolNef,educational activities of the working group of the Polish Society of Nephrology on theearly detection of CKD and changes introduced in the primary health system by thenational healthy fund (incorporating also cardiology and diabetology care into theduties of general practitioners), we designed the study to evaluate prevalence of CKD inrandomly selected 20 cities all over the Poland. We named the activity “Nefrotest” andgave the motto: “kidneys do not hurt, ignorance hurt”. The study was founded by theunrestricted educational grant form Fresenius Medical Care under the auspices ofPolish Society of Nephrology, national and regional consultants for nephrology.Methods:We employed two approaches: during World Kidney Day we organizekidney check-ups in the nephrology outpatient unit and in the public places likeschools, churches, shopping malls gave invitations for kidney check-ups in thenephrology outpatient units. We gathered the data from 13449 subjects. Kidneyfunction was assessed on the basis of serum creatinine and eGFR by MDRD asprovided by a laboratory.Results: In the first approach 8333 subjects appeared in the nephrology outpatientclinic for check-up and creatinine assessment. 767 subjects had abnormal results(9.24%), in 749 CKD stage 3 was diagnosed, and in 18 CKD stage 4 was diagnosed. Inthe second approach out of 32600 invitations, 5116 subjects appeared in nephrologyclinic for check-up and creatinine assessment. 530 subjects had abnormal results(11,34%), including 489 with stage 3 CKD, 36 with stage 4 CKD and 3 with stage 5CKD. In the whole population screened, over 10% of subjects had CKD, at least stage3. When we divided our population studied into age categories, we found that inpatients over 40 years of age prevalence of CKD was 9.2%, over 50 year of age 11.25%and over 60 years of age 13.38%. All the subjects with abnormal results were offered afast track visit in outpatient nephrology clinic.Conclusions: Concluding, in the screened population the prevalence of CKD is over10%, and increasing with age. Early detection of CKD and introduction ofnephroprotective therapies may slower the progression to the end-stage kidney disease.It is also important form the pharmacoeconomic perspective.
MP197 CHRONIC KIDNEY DISEASE REQUIRING HEALTHCARESERVICES: A NEWAPPROACH TO EVALUATEEPIDEMIOLOGYOF RENAL DISEASE
Gianluca Trifirò1, Janet Sultana1, Francesco Giorgianni1, Ylenia Ingrasciotta1,Marco Muscianisi1, Daniele Ugo Tari2, Margherita Perrotta2, Michele Buemi1,Valeria Canale1, Vincenzo Arcoraci1 and Domenico Santoro11University of Messina, Messina, Italy, 2Local Health Service Caserta, Caserta, Italy
Introduction and Aims: CKD estimates based on screening of general population donot provide a real insight into the impact of CKD on the use of healthcare resources inclinical practice.The aim of this study is to evaluate the epidemiology of “medicalized”CKD, i.e. CKD requiring healthcare services in outpatient setting.Methods: This is a retrospective, longitudinal population-based study which wasconducted in a large general practice of Southern Italy (Caserta) using a healthcaredatabase.Over the years 2006-2011, we identified all patients with CKD diagnosis, aseither indication of use associated to any drug prescription or cause of hospitaldischarge diagnoses/procedures using this database. The prevalence of “medicalized”CKD in the general population of Caserta by age, gender and calendar year wasestimated.Results: Overall, we identified 1,989 (1.3%) patients with a diagnosis of CKD duringthe years 2006-2011 in the Caserta general population. The one year prevalenceincreased from 0.9% in 2006 to 1.6% in 2011, which is much lower as compared toprevious screening-based studies. The prevalence was slightly higher in males andincreased significantly with advancing age (in 2011, 0.2% in ≤44 years old vs. 9.2%in>80 years old).Conclusions:We demonstrated that, in general population, the prevalence of CKDrequiring healthcare resources, i.e. “medicalized” CKD, is lower as compared to thescreening-based CKD prevalence.
MP198 A SYSTEMATIC LITERATURE REVIEWOF THE HUMANISTICBURDEN OF ANAEMIA ASSOCIATEDWITH CHRONICKIDNEY DISEASE
Maria Rizzo1, Ike Iheanacho1, Floortje E Van Nooten2 and David Goldsmith31Evidera, London, United Kingdom, 2Astellas, Leiden, The Netherlands, 3Guy'sHospital, London, United Kingdom
Introduction and Aims: The humanistic burden associated with anaemia in patientswith chronic kidney disease (CKD) and the instruments used to measure health-relatedquality of life (HRQoL) in this setting have not been explored recently using systematicliterature review (SLR) methods. Therefore, these important topics were investigatedusing such an approach.Methods: A systematic search was performed in MEDLINE- and EMBASE-indexedliterature on CKD-related anaemia from 2007 to 2012, for English-language HRQoLpublications from any country. Data were abstracted into a pre-designed template andsynthesised using qualitative methods.Results: The review identified 37 studies that had reported on HRQoL. In these, theShort Form (36) Health Survey (SF-36) was the most frequently employed measure of
MP194
Abstracts Nephrology Dialysis Transplantation
iii | Abstracts Volume 29 | Supplement 3 | May 2014Downloaded from https://academic.oup.com/ndt/article-abstract/29/suppl_3/iii380/1882504by gueston 25 March 2018

humanistic burden, used in 19 of the studies. Other measures of HRQoL were not oftenreported by more than one study. Two studies among non-dialysis patients withanemia of CKD (CKD-ND) found SF-36 scores to be lower among this group ofpatients, compared with the general US population, with the difference generally beingmore marked the lower the haemoglobin threshold used to define anaemia (Figures 1and 2). In seven cross-sectional studies, a correlation was reported between the severityof anaemia and HRQoL, in that, as Hb or hematocrit (Ht) levels decreased across agroup of patients, so did scores for both the mean physical component summary (PCS)and mental component summary (MCS) of the SF-36. Similarly, an additional fourstudies (two on CKD-ND and two on dialysis patients) found that groups of patientswith higher Hb or Ht levels had poorer HRQoL in terms of PCS or MCS scorescompared to those with lower levels. Also, a single study suggested that there may be anoptimal Hb threshold (10-11 g/dL) to target with erythropoietin-stimulating treatmentin order to maximise HRQoL benefits associated with anaemia management in CKD.Associations between Hb or Ht levels and either vitality or functional ability subscalesof the SF-36 were less consistently demonstrated.Conclusions: Anaemia of CKD is associated with a considerable humanistic burden.This highlights the need for appropriate management of anaemia in patients with CKDto improve their HRQoL outcomes.
MP199 BALNEOTHERAPY AND CHRONIC URINARY TRACTINFECTIONS, A BENEFIT OR A DANGER?
Barbara Grandtnerová1, Zuzana Beratšová1, Miroslava cErvenOvá1, Ján cErven1,Marian Markech1 and Anna Štefániková11Golden Spa, Turcianske Teplice, Slovakia
Introduction and Aims: In countries rich in thermal waters, balneotherapy is oftenused as a part of supportive therapy and rehabilitation process for chronic kidney andurinary tract infection. It is in a clear contradiction with nephrologistsrecommendations for patients in risk, to avoid bath tubs and whirpools as much aspossible, not to contract urinary tract infection. Unfortunately, publications concerningboth problems are very scarce.Aim: to assess the effect of the bath tubs and thewhirpools as a standard part of balneotherapy on the immediate risk of relapse/recurrence of the urinary infection in patients at increased risk for infection.Methods: In a retrospective manner, we evaluated 106 patients (87 women), medianage 58 years (30-87), treated for chronic cystitis (diagnosis N30.1, N30.2). Controlgroup consisted of 101 patients (87 women), median age 56 years (20-75), p = ns, witha vertebrogenic algic syndrome (VAS).All patients were treated in bath tubes andwhirpools for 15 minutes daily during 20-22 days of their stay in the spa. The numberof procedures in both groups was comparable. Water was thermal and low mineralised,soluts consisted mainly of bicarbonate, sulphate, magnesium, calcium and fluoride.Bathing was combined with other treatments, such as physical exercise, aquatic exercisein pool with thermal chlorinated water, mud packs, massages and electro- ormagnetotherapy.Results: Symptoms of the acute urinary tract infection arised in 11 patients (10.4%)treated for chronic cystitis and 0 patient treated for VAS, p = 0.0008, RR 2.063, 95% CI1.786 to 2.384. In women only, respective data were 11.5% vs 0%, p = 0.0015, RR 2.130,95% CI 1.810 to 2.506. All but one case were mild blader infections, well responding toperoral antibiotic therapy. Only in one patient, early discharge from spa was necessary.Conclusions: 1. Bath tubes and whirpools increased the risk of the acute cystitis inpredisposed patients, despite only 15 minutes of their duration.2. Notwithstanding this complication, all patients reported raised well-being at theirdismissal.3. This study was not designed to answer long term benefit of balneotherapy onchronic kidney and urinary tract infection.
MP200 RENAL CARE IN AN ISO(9001:2008)-CERTIFIEDPREDIALYSIS CLINIC
Wendy Engelen1, Monique Elseviers2,3, Eric Gheuens1,4, Conny Colson1,5,Ilse Muyshondt1,4 and Ronald Daelemans1,51Ziekenhuis Netwerk Antwerpen, Antwerpen, Belgium, 2Universiteit Antwerpen,Wilrijk, Belgium, 3UA University of Antwerp, Antwerp, Belgium, 4ZNA ZiekenhuisNetwerk Antwerpen, Antwerp, Belgium, 5ZNA Ziekenhuis Netwerk Antwerpen,Antwerp, United Kingdom
Introduction and Aims: In 2008 a multidisciplinary predialysis clinic (MPC) (acooperation between a renal nurse, a renal dietician, a social assistant and anephrologist) was started. In 2012 this predialysis clinic, was ISO(9001:2008)-certified,offering a protocol-driven approach, evaluated in PDCA-cycles (Plan-Do-Check-Act).Despite the possibility of this organized predialysis care, many patients were followedwith standard renal care (SRC), provided by the same team of nephrologists.Wecompared the influence of organized, multidisciplinary care in the predialysis period tostandard renal care, on the outcome after one year of dialysis.Methods: Of all patients, starting dialysis, patient characteristics were registered at startand after 1 year of renal replacement therapy, as well as dialysis access.Results: All patients received at least 3 months of predialysis renal care. Patientcharacteristics did not differ between patients followed in the MPC (n=69), andpatients with SRC (n=62). There was a trend to performing more renal biopsies inpatients followed in the MPC, versus with SRC (26.1% versus 15.1%, p=0.174).Patientsin the PMC needed significantly less urgent start of dialysis (23.5% versus 43.5%,p<0.015). More frequently an AV fistula was present at start (38.2% versus 19.4%,p<0.018). At the start of renal replacement therapy, there was a trend to shorterhospitalization in this population (13.4 days versus 17.3 days, p=0.349). The advantageof the predialysis care became more apparent after 1 year of dialysis. At that time therewas a highly significant difference in use of AV fistulas in favor of the patients followedin the MPC (58.8% versus 23.8%, p=0.002) and there was a trend to lower mortality at1 year of dialysis in the latter group (30.6% versus 41.9%, p=0.171).Conclusions: Follow up in a multidisciplinary predialysis clinic, with protocol-drivenhealthcare, offers advantages compared to standard renal care.
MP198 Figure 2: Mean SF-36 Scores in Patients with Anaemia and CKD Defined byDifferent Hb Thresholds Compared with the General US Population
MP198 Figure 1: Mean SF-36 Scores in Patients with Anaemia of CKD Comparedwith US General Population Norms
Nephrology Dialysis Transplantation Abstracts
Volume 29 | Supplement 3 | May 2014 doi:10.1093/ndt/gfu167 | iiiDownloaded from https://academic.oup.com/ndt/article-abstract/29/suppl_3/iii380/1882504by gueston 25 March 2018