Embed Size (px)
Citation preview

The journa l fo r re sp i ra to r y
hea l th p ro fes s iona l s in Canada
La revue des professionnels de la
santé respiratoire au Canada
Summer 2004, Volume 40 (3)
Features■■ New Funding
Opportunities 11
■■ Student Special InterestGroup 14
■■ CoARTE Update 19
■■ Treatment of LobarAtelectasis With SurfactantLavage in the Neonate 23
On Air■■ Honoraray Life Member
Terry G. Boone 5
■■ Forum Highlights 6
Sputum Cup Winners, Forum 2004Respiratory TherapyWeek Catalogue 15

Table of ContentsOn Air . . . . . . . . . . . . . . . . .5Honorary Life Member Terry G. Boone Forum 2004 HighlightsNuggets
President’s Message . . . . . .8
CSRT News . . . . . . . . . . . . . .11New Funding OpportunitiesThank you to the VolunteersStudent Special Interest GroupRespiratory Therapy Week Catalogue
Scientific News . . . . . . . . . .22AbstractsTreatment of Lobar Atelectasis WithSurfactant Lavage in the Neonate
Industry News . . . . . . . . . . .27Mobile Air Purification SystemFacial Protective EquipmentAsthma Research Funding
The CJRT acknowledges the financial support of the Government ofCanada, through the Publications Assistance Program (PAP), toward ourmailing costs.
Cover Photo The Michener Team Sputum cup winners:Nancy Brown, Paula Burns, Martha Williams, Andrea White-MarkhamPhoto by Craig Hillier.
Summer 2004 Canadian Journal of Respiratory Therapy — www.csrt.com 3
Contents ■ Table des matières
CSRT membership inquiries /Questions concernant l’adhésion à la SCTR :
102 – 1785 Alta Vista Dr.,Ottawa, Ontario, K1G [email protected]
Canadian Journal ofRespiratory Therapy
Revue canadienne dela thérapie respiratoire
Official Journal of the CSRTRevue officielle de la SCTR
CSRT Board Representative / Représentante duConseil d’administration de la SCTR Colya Kaminiaz, RRT
Managing Editor / Directrice de la rédactionRita Hansen
Consulting Editors / Rédacteurs-conseilMembers of the Scientific Review Committee
President. CSRT / Président, SCTRBrent Kitchen, RRT
The Canadian Journal of Respiratory Therapy (CJRT)(ISSN 1205-9838) is produced for RRT: The CanadianJournal of Respiratory Therapy, Inc., by the GraphicCommunications Department, Canadian PharmacistsAssociation and printed in Canada by Gilmore Printing.Publications mail registration no. 09846. CJRT is pub-lished 5 times a year (in February, May, July, October andDecember); one of these issues is a supplement pub-lished for the Annual Educational Forum of the CanadianSociety of Respiratory Therapists (CSRT).
La Revue canadienne de la thérapie respiratoire (RCTR)(ISSN 1205-9838) est produite pour le compte de RRT :The Canadian Journal of Respiratory Therapy, Inc., parCommunications graphiques de l’Association des phar-maciens du Canada et imprimée au Canada par HarmonyPrinting. Courrier de publications no 09846. La RCTRparaît cinq fois l’an (en février, mai, juillet, octobre etdécembre); un de ces numéros constitue un supplémentpublié pour le compte du Forum éducatif annuel de laSociété canadienne des thérapeutes respiratoires (SCTR).
Advertiser’s IndexSpiriva . . . . . . . . . . . . . . . . . . . . . . . . . . . 2, PI 29, 30
Beausejour . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
Capital Health . . . . . . . . . . . . . . . . . . . . . . . . . . OBC
On Air

4 Été 2004 Revue canadienne de la thérapie respiratoire — www.csrt.com
Welcome to the SummerEdition of the Journal.Recent changes in theCSRT/CJRT corporate struc-ture, will result in theJournal falling back underthe umbrella of the CSRT,instead of as a separatecorporate entity. With thisrestructuring, the position ofPresident of the CJRT hasbeen retired. I would like totake this opportunity tothank Allan Shemanko for his tireless work as President of the CJRT. Allan hassteadfastly kept the Journal on track, always looking foropportunities to improve and streamline production.Thank you Allan!
Issues involving the CJRT will now fall under themandate of Colya Kaminiarz, Director of MembershipServices. Along with Colya, I would also like towelcome Sue Jones, President Elect of the CSRT; Wrae Hill, Director of Professional Advocacy; Ray Hubble, Director of Education and ClinicalStandards, and Scott LeMessurier, Director of Nationaland Provincial Relations.
In this issue you will find a wrap of Forum 2004 as wellas information on Forum 2005. We have articles on theStudents Special Interest Group, CICF funding and ourScience paper on Treatment of Lobar Atelectasis.
RT Week is also around the corner! Check our RT catalogue for interesting items to help promoterespiratory therapy in your area. We look forward to the continued support of our membership.
Douglas Maynard BSc, RRT, MBAExecutive Director CSRT
Welcome from Doug
Design and production / Conception et productionCanadian Pharmacists Association / Association des pharmaciens du Canada
Marketing and Advertising Sales / Marketing et publicitéKeith Health Care Inc.Mississauga 905 278-6700, fax 905 278-4850Montréal 877 761-0447, fax 514 624-6707
Classified Advertising / Annonces classéesCSRT102 – 1785 prom. Alta Vista Dr.Ottawa ON K1G 3Y6800 267-3422 or fax 613-521-4314
Subscriptions / AbonnementsAnnual subscriptions are included in annual membership to theCSRT. Subscription rate for 2004 for other individuals and institutionswithin Canada is $44 and $44(US) for others outside Canada. AllCanadian orders are subject to 7% GST / 15% HST as applicable.Requests for subscriptions and changes of address: Member ServiceCentre, CSRT, 102 - 1785 Alta Vista Dr., Ottawa ON K1G 3Y6.
L’abonnement annuel est compris dans la cotisation des membres dela SCTR. Le tarif annuel d’abonnement pour les non-membres et lesétablissements au Canada est de 44$ et de 44$ US à l’étranger. LaTPS de 7% ou la TVH de 15% est ajoutée aux commandes canadi-ennes. Veuillez faire parvenir les demandes d’abonnement et leschangements d’adresse à l’adresse suivante: Centre des services auxmembres, SCTR, 102 - 1785 prom. Alta Vista, Ottawa ON K1G 3Y6.
Once published, an article becomes the permanent property of RRT:The Canadian Journal of Respiratory Therapy, Inc., and may not bepublished elsewhere, in whole or in part, without written permissionfrom the Canadian Society of Respiratory Therapists, 102 - 1785 AltaVista Dr., Ottawa ON K1G 3Y6. / Dès qu’un article est publié, ildevient propriété permanente de RRT: The Canadian Journal ofRespiratory Therapy, Inc., et ne peut être publié ailleurs, en totalitéou en partie, sans la permission de la Société canadienne desthérapeutes respiratoires, 102 - 1785 prom. Alta Vista, Ottawa ONK1G 3Y6.
All editorial matter in CJRT represents the opinions of the authorsand not necessarily those of RRT: The Canadian Journal ofRespiratory Therapy, Inc., the editors or the publisher of the journal,or the CSRT. / Tous les articles à caractère éditorial dans le RCTRreprésentent les opinions de leurs auteurs et n’engagent ni le RRT:The Canadian Journal of Respiratory Therapy, Inc., ni les rédacteursou l’éditeur de la revue, ni la SCTR.
RRT : The Canadian Journal of Respiratory Therapy Inc. assumes noresponsibility or liability for damages arising from any error or omis-sion of from the use of any information or advice contained in theCJRT including editorials, articles, reports, book and video reviewsletters and advertisements. / RRT : The Canadian Journal ofRespiratory Therapy, Inc. décline toute responsabilité civile ou autrequant à toute erreur ou omission, ou à l’usage de tout conseil ouinformation figurant dans le RCTR et les éditoriaux, articles, rapports,recensions de livres et de vidéos, lettres et publicités y paraissant.
All prescription drug advertisements have been cleared by thePharmaceutical Advertising Advisory Board. / Toutes les annonces demédicaments prescrits ont été approuvées par le Conseil consultatifde publicité pharmaceutique.
Doug Maynard
Welcome!

OnAir
Summer 2004 Canadian Journal of Respiratory Therapy — www.csrt.com 5
Honorary Life Membership —Terry G. Boone
When Terry was obliged to leave work in June2000 because of primary progressive MultipleSclerosis, he was the Dean of InformationTechnology, Health and Business Studies at New Brunswick Community College in Saint John,New Brunswick — with the only formal educationbehind him being his respiratory technologydiploma.
From the time he graduated from Victoria GeneralSchool of Respiratory Therapy in Halifax as a respi-ratory therapist in 1972, with the most outstand-ing student award, until he left work in 2000,Terry made continuous, dedicated, unselfish andidentifiable contributions to the profession ofrespiratory therapy.
He was a founding member of the CSRTEducation Committee, before there was a CBRC,as well as the New Brunswick member of theCBRC Examination Committee.
In September 1989 Terry set up the firstRespiratory Therapy program at NBCC. He partici-pated in many accreditation surveys throughoutCanada — medical laboratory, paramedicine andrespiratory therapy. Terry was Chair of the CSRTAccreditation Working Group, which led thedevelopment of CoARTE, respiratory therapy’sown accreditation process in Canada.
He was also a founding member and firstsecretary of the New Brunswick Association ofRespiratory Therapists, and President of the NewBrunswick Association of Respiratory Therapistsand a member of the CSRT Board of Directors.
From 1993 to 2001 Terry was Chair of the CSRTJudicial Committee. During this time he docu-mented the required process, provided recom-mendation for bylaws to enforce the requirementsand trained others on the process.
Terry was always involved in his profession,strongly supporting its advancement. His personalattributes made all this possible. Throughout theyears it has been his determination to steadfastlyand solidly, yet so diplomatically “plant his foot”when it was the right thing to do, even when itwas not popular to do so. Though there havebeen obstacles along the way, his perseverancehas been both appreciated and respected. Terry ismeticulous, a loyal friend, has a wonderful wit,and is a great storyteller — stories that willinclude many “Terryisms” sure to bring out ahearty laugh in all who are around.
Terry’s inspiration and dedication to the professionhas been recognized previously. Most recently in1999 — NBART “RT of the Year award and in2001 — CSRT Professional Achievement Award,now renamed the Robert Merry Memorial Award.
Respiratory therapists across this country owe somuch to Terry for his support and commitment. It gives my colleagues and I great pleasure to havenominated Terry Boone, for Honourary LifeMembership in the Canadian Society ofRespiratory Therapists. I only wish Terry, a mostcaring individual, could had been well enough tobe here to receive this award in person, to seeand feel the impact he has had on so many of our lives.
Cheryl Homuth, RRT
Terry Boone was awarded a CSRT Life Membership at the CSRT Educational Forum,
in Toronto, May 29, 2004, along with Robert Colyn and Ian Reid.

6 Été 2004 Revue canadienne de la thérapie respiratoire — www.csrt.com
OOnn Air Highlights from
CSRT Honorary Life Memberships were awarded to RobertColyn, left Ian Reid and Terry G. Boone not present.
Summit Award winner Robert Martell left and JimCosman, Summit Technologies President.Chair of Registration, Gail Lang, takes a well-deserved
breather after a long day of stuffing delegate bags
Fun Night included aSecond City comedyreview.

Summer 2004 Canadian Journal of Respiratory Therapy — www.csrt.com 7
OOnn Air CSRT Forum 2004
Thanks to Gail and her hard-working crew who made sure the Registration Desk ran like awell-oiled machine.
Left to right Ana MacPherson, RRT;Lisa Butcher, RRT (student); SophiaCabral, RRT;Gail Lang, RRT.
CSRT Gold Medal winner Salvatore Salamone, leftMichener Institute and Past-President Jim Winnick.
Bill Butler received the Robert Gerry Award, presentedby CSRT President-Elect Sue Jones.
Past-President Jim Winnickshows his true colors.

OOnn Air
ON AIR NUGGETS
▲▲
▲
Global AsthmaThe Global Burden of Asthma Report detailsthe prevalence, morbidity, and mortality ofasthma in 20 regions around the world,reveals a number of alarming facts about theburden of this chronic respiratory disease inthe world. The “Global Burden of Asthma”Report, Pocket Guide, Pediatric Guide andPatient Guide can be obtained atwww.ginasthma.com.
▲
Congratulations Ray Hubble!Ray Hubble, RRT, MMEd, the CSRT Directorof Education and Curriculum Standards wasrecently awarded the Excellence in TeachingAward from the Saint John campus of theNew Brunswick Community College.
An innovative teacher at the college, Mr. Hubble is widely known for his dedicationto respiratory therapy and his determinationto keep his students updated on the ever-changing world of technology. Mr. Hubble has been teaching respiratorytherapy for 14 years.▲
Award WinnersRobert Merry Memorial Award forProfessional Achievement William Butler
CSRT Honorary Lifetime Memberships Terrence BooneRobert ColynIan Reid
Summit Award In Respiratory ExcellenceRobert Martell
▲
Passport WinnerNancy Chan of Mississauga was the winner of our Passport draw. She will receive freeregistration to the CSRT Forum —“Compassion in Action” in Edmonton 2005along with three nights accommodation.
▲
CSRT Forum Poster WinnersCongratulations to our Forum 2004 Poster winners. Each will receive complimentaryregistration to Forum 2005 — “Compassion inAction” in Edmonton, Alberta
Best tudent Poster — Patrick Nellis, BSc, RRT“Review of Inhaled Nitric Oxide Therapy in HeartTransplantation” submitted as a student in theAnaesthesia Support Program of TMI.
Best Poster — Nancy Garvey, RRT “Asthma Care Map for Primary Care Providers”
Best Poster — Susan Dunington“Critical Thinking Competence in Respiratory Therapy”
▲
Edmonton 2005The CSRT Planning Committee for Forum2005 “Compassion in Action” is alreadyplanning sessions to be held at the ShawConference Centre in Edmonton, Alberta —June 3 – 5, 2005.
Streams will include Sleep Studies,Neonatal/Pediatric Care, Critical Care,Anesthesia and Community Care. Suggestionsand input are very welcome [email protected]

Summer 2004 Canadian Journal of Respiratory Therapy — www.csrt.com 9
At the CSRT Educational Forum in Toronto in May, I was asked to make a presentation describing thefuture of the CSRT. I sat down to consider what Ibelieve are the strengths and weaknesses of the CSRTand how well the organization is positioned for thefuture. A few key issues that I think are paramount tothe future success of the CSRT, and to the profession,jumped out at me.
Forty years ago, when the CSRT was formed, theprofession needed an organization to define what arespiratory therapist was. The CSRT RRT credential wascreated and eventually became based on the promotionof a common school curriculum, an accreditationprocess for schools, a national exam and a judiciaryprocess. The CSRT evolved into a society that alsoprovides other benefits to members including thejournal for sharing information, educational forums, aprofessional development program, promotion of theprofession, a national/international voice for RTs inCanada and much more. I believe that the success thatwe have achieved as a profession is largely based uponthe CSRT’s success in providing excellent programs andmoving the profession forward.
The needs of respiratory therapy are changing. At onetime the CSRT was the organization that defined what aRT was. Now legislation in various provinces has madethe definition of respiratory therapy provincial law.This is an important step forward for the profession,but provincial law (self-regulation) now gives thecolleges of respiratory therapy in each province theauthority to define what a RT is in their province.Although it has been essential for the development ofthe profession, the credentialling role of the CSRT isdiminishing. As more provinces become self-regulatedthe need for this role will lessen even further.
The new role for the CSRT is to provide services tomeet the needs of our profession that are not providedby regulatory bodies. They include maintaining nationalprocesses, advancing respiratory therapy practice byproviding best practice guidelines, promoting theprofession to the public and to governments, recruitinginto the profession, supporting respiratory therapyresearch, networking and collaborating with regulatorybodies. We need to guarantee that the voice of theprofession is heard when all decisions affecting us asprofessionals and our practice are being made.
The reality is that as a society we currently dedicatemore of our resources to credentialling than we do toproviding other services to our members. To meet theneeds of the profession we need resources. Ourresources come from our members. We need moremembers! Fewer and fewer RTs need credentiallingservices because their regulator performs that functionfor them. Part of self-regulation means that CSRTmembership is optional for the majority of RTs in this country. People need to experience the tangiblevalue of membership to remain or become members of the CSRT. The CSRT needs to refocus on being anorganization that primarily provides services andbenefits to its members.
We need to decide if the CSRT will continue to repre-sent only those fewer and fewer RTs that go throughour specific processes for the non-regulated provincesor if we will become a society that truly represents theentire profession in Canada. This means allowing thoseRTs defined as RTs by regulatory bodies to become fullmembers of our society. The Mutual RecognitionAgreement was signed between regulators and theCSRT because we identified evidence (the NationalCompetency Profile) that showed that all RTs practicing
continued page 10
Message from the President
Message from the President
Brent Kitchen
“The significant problems we face cannot be solved at the
same level of thinking we were at when we created them.”
— Albert Einstein

10 Été 2004 Revue canadienne de la thérapie respiratoire — www.csrt.com
in all provinces in Canada are more than 90% equiva-lent. We also expect that within the next few monthsevery school in Canada will use the same accreditationprocess, each school will teach to the same profile andall jurisdictions will examine graduates based on thesame profile. That should be enough for us to decidethat we can include all RTs in our society and trulyrepresent all RTs in Canada. We need to be inclusiverather than exclusive, while guaranteeing that ourstandards are high. This is the future of the CSRT.
In the coming months you will receive a mailout ballotasking for approval to change our bylaws to allow RTslicensed in the regulated provinces who meet therequirements of the Mutual Recognition Agreement tobecome full members of the CSRT. I believe this can bea turning point for our society and a point that we will
look back on one day and see as a key step to how we achieved new success. If we remain exclusive ratherthan inclusive, I believe that our society will stagnateand we will never reach our true potential, meaning we will not meet our true potential as respiratorytherapists. Please consider the information you receivewith your ballot carefully and consider the future,rather than the past, when you cast your vote.
Brent Kitchen, RRTPresident, CSRT
Message from the President
Message from the President continued from page 9
Gold Plus SponsorGold Plus Sponsor
Silver Sponsor
Bronze Sponsor
Gold Plus Sponsor
Gold SponsorSilver Sponsor
Silver SponsorBronze Sponsor
The CSRT thanks its sponsors for their generoussupport of the CSRT Educational Forum 2004.
Silver Sponsor

Summer 2004 Canadian Journal of Respiratory Therapy — www.csrt.com 11
CSRT NEWS
CSRT and Canadian Intensive
Care Foundation Join Hands to
Support Respiratory Therapists
In addition to the Canadian Society ofRespiratory Therapist, RTs can now turn to theCanadian Intensive Care Foundation (CICF) forprofessional support.
Leaders from the Canadian Society of RespiratoryTherapists (CSRT) and the CICF have agreed tocross-promote education, events and member-ship in order to increase awareness and supportfor critical care professionals, such as respiratorytherapists.
As a testament to their assistance, CICF leadersnow offer a new source of education funding forrespiratory therapists from intensive care unitsacross Canada.
The CICF has expanded research andeducational funding opportunities to include alldisciplines within the intensive care environment.The Foundation offers grants-in-aid of researchand education to qualified applicants who arepracticing critical care personnel: critical carephysicians, nurses, respiratory therapists andpharmacists.
For 2004, grant committee adjudicators for CICFexpect to release about $100,000 to support criti-cal care research and teaching. Foundation ChairCindy Hamielec, MD, FRCPC, said the CICFBoard redesigned the grant program last year toprovide broad coverage and benefit as manycaregivers as possible.
“The CSRT is very excited about the CICF nowoffering education funding for respiratory thera-pists from intensive care units. It’s a new part-nership that really benefits our profession. Formore information on how membership — or
involvement with a local CICF Chapter — canassist you with professional development go to the CICF website www.cicf.ca”, said BrentKitchen, CSRT President. ICU respiratory thera-pists can also contact CICF Executive DirectorWayne Peterson at the Foundation.
CICF leads the wayThe CICF continues to engage as members, RTs and other critical care professionals acrossthe country to gain support to fund new research— and now education — for patient care of thecritically ill and injured. The induction of moreChapters, and members, in Canadian centresmark the path.
“In the past year, we followed a course for suc-cess, prioritized tasks, introduced more fundrais-ing activities, and prepared to take advantage ofmore opportunities down the road”, Petersonsaid. “And as we grow, we never lose sight of our true purpose — to generate more fundsfor life-saving research and education.” TheFoundation released another $135,000 in 2003 to initiate studies by researchers in intensive careand related fields.
Recognition and awareness for the Foundationremains a major goal. “To that end, we continueto expand our profile and representation acrossthe country through Chapter development, agrowing membership and connection with healthcare professionals,” Peterson said. “We also con-tinue to attract more corporate sponsors anddonations, present more fundraising events, andimprove overall administration of theFoundation.”
CICF demographicThe CICF now has an affiliation with doctors andother intensive care staff at more than 000Canadian hospitals — the result of an assertivecampaign stimulated by the Foundation’s Board
continued on page 12
New Funding Opportunities

12 Été 2004 Revue canadienne de la thérapie respiratoire — www.csrt.com
CSRT News
continued from page 11of Directors in recent years. With generoussupport through the Coalition of Excellence bycorporate partners — Ortho Biotech, Bayer Inc.and GE Medical Systems — CICF leaders confi-dently set an aggressive business plan in 2003 toadvance the Foundation and raise more funds forresearch and education over several years.
Through CICF, respiratory therapists are connected with:
■ About 600 CICF members (doctors and otherhealth care staff, administrators, volunteers,patients and their families and business andcommunity leaders)
■ Three new CICF Chapters established inCanadian centres (Calgary, Halifax andHamilton) with Montreal, Toronto, Vancouverand Winnipeg in the development stage.
Foundation revenues grew to $560,000 by 2003.Grant and education allocations also increasedfrom $80,000 in 2001 to $135,000 in 2003. The fledgling organization has invested over$500,000 in grants since formation.
CICF growth todayBy June 2004, CICF leaders expect to achievebusiness plan key objectives of:
■ Three corporate partners and $85,000 in corpo-rate partnership revenue
■ 500 members and more than $12,000 in mem-bership revenue
■ Four new chapters across Canada (Calgary,Halifax, Hamilton and Montreal)
■ Six sources of alternative funds (e.g.,grants/endowments) at $45,000
■ $100,000 in grant and education allocations.
CICF growth tomorrowBy June 2007, the business plan projects keyobjectives of:
■ 10 corporate partners and about $300,000 in corporate partnership revenue
■ 1,700 members and about $42,000 in member-ship revenue
■ $100,000 from personal and communitydonations
■ 12 chapters across Canada (Calgary, Halifax,Hamilton, Montreal, Toronto, London,Winnipeg, Vancouver, Quebec City, Edmonton,Saskatoon/Regina, and Ottawa) as well asother non-teaching communities
■ About $600,000 (net) in fundraising activitiesfrom chapters
■ 11 sources of alternative funds (e.g., grants/endowments) at $95,000
■ $500,000 in grant and education allocations.
All-Can Medical Inc.
Cardinal Health
Care Stream Medical
London Scientific Limited
Methapharm Inc.
ProResp/ProHealth
Respan Products Inc.
Roxon-Universal Medical
Source Medical Corporation
Tyco Healthcare
VitalAire
The CSRT wishes to acknowledge the on-going support of our Corporate
Members. Sponsorship by ourCorporate Members helps the CSRT
maintain the current standards of excellence in the profession.
Thank you!
CSRTCorporate Members
2004 – 2005

Summer 2004 Canadian Journal of Respiratory Therapy — www.csrt.com 13
Darcy AndresMary BaylissD. BrooksNancy BrownLynn BeatonMelva BellefontaineSandra BiesheuvelChristopher BredesonCatherine Burke-TreblayHélène BurnetteLisa ButcherPaula BurnsSophia CabralThelma CashenPamela CoganR.H. CollinsMark CrowtherRick CulverKevin de JongGlenn DayDebbie DemizioMelanie DeremoShane DonaldsonTom DorvalCarmella DuchschererHelene DunaediSusan DuningtonNancy GarveyDiane GauvreauR..S. GoldsteinDon GranoskiLeanne GrantG.H. GuyattJan HaffnerChris HarmonyElenore HaywoodFran HillWrae HillCraig HillierRay HubbleCheryl HomuthGwynne Jones
Sue JonesColya KaminiarzThelma KashinMike KeimBrent KitchenCindy KellyGreg KinghornArnold KwokKathy KowalskiCarole LeblancScott LeMessurierGail LangEleanor LordDeborah LuschinskiSue MartinAna McPhersonJohn MinskiTodd MortimerGinny MyersM.L. NonoyamaHeather Jean NoyesAllison NykolaychukKathleen Olden-PowellMargaret OganowksiMarg PatellDemi PapapanagioutouDaniel ParéRick ParadisMarg PatellGraham PineoRobert ReidM. ReillyPhil RichardsonAngeline Robitaille-FilionMarc A. RodgerJason SallowsRichard SewardCliff SevilleDavid SheetsTracy SimcoeKathy SpurrDavid Sheets
Alan ShemankoDavid SwiftAngela TaylorJan TaylorKen TinNorm TiffinDavid ThompsonGil VergilioAndrea White MarkhamKen TinGil VergilioKathy WalkerBrenda WhatmoughPhilip S. WellsCynthia WeltonWade WheelerJim WinnickAndrea White-Markham
We endeavor to include all ourvolunteers. If you have beeninadvertently left off our list, weapologize. Please let us know!
Thank You Volunteers.We Couldn’t Do it Without You!
CSRT News

14 Été 2004 Revue canadienne de la thérapie respiratoire — www.csrt.com
CSRT News
Following a vote at this year’s AGM held inToronto, a Special Interest Group (SIG) has beenset up, dedicated to student members of theCSRT. I will be assuming the role of chairpersonfor this Special Interest Group, and look forwardto speaking with those of you interested inbecoming involved in this new project.
Allow me to first of all introduce myself. I amentering my third year of Respiratory Therapyand am working towards my Bachelor of HealthSciences degree at Dalhousie University inHalifax, Nova Scotia. I have been involved invarious community initiatives through differentnon-profit organizations supporting the work ofRespiratory Therapists, and look forward toengaging students in some new and exciting lev-els of Respiratory Therapy.
As outlined in my proposal made at the AGM,the main goals of the Student SIG will be to firstof all establish networks through which students,educators and general members can communi-cate different ideas that relate to respiratorytherapy education, student life, etc. Differentstudents and schools have become engaged in avariety of different projects that deserve to beshared, as they would no doubt benefit differentcommunities and schools throughout thecountry. It is my hope that by setting up services such as the ListServer e-mail service and by providing regular access to the CJRT forstudents, that we can begin to start sharing somevaluable information and resources of relevanceto students.
It is my hope that we can start to see studentrepresentation on different committees through-out the country, and this is something that I willbe promoting as part of my goals for this group.I want to keep the membership large but theactual structure of the SIG simple. The structure
of the group will require an additional person,the Co-Chairperson, to act alongside theChairperson. Due to the fact that there arecurrently no established Terms of Reference for the group, I feel that an appropriate measureis to announce that we will be acceptingapplications for the position from studentmembers of the CSRT. Contact information will be made available on the CSRT website andanyone interested is encouraged to check forinformation there.
I will be making contact with the differentschools throughout the country and intend toprovide you with information to share withstudents regarding what I hope to accomplish.The success of this group will rely heavily uponits promotion through both educators and thegeneral membership. The ultimate goal is toprovide students with further reasons to join the CSRT and in turn, hopefully secure moremembers upon graduation.
It is with sincere thanks that I submit this, thefirst report from the Student Special InterestGroup, to you - the members of the CanadianSociety of Respiratory Therapists — for yourcontinued support of Respiratory TherapyEducation and Respiratory Therapy Students inCanada. Your continued commitment to provid-ing students with excellent opportunities foradvancement in professional engagements iswhat makes our profession one that willcontinue to grow and advance for years to come.
Student Special Interest GroupJason Nickerson, BHSc (RSPT) StudentChairperson, CSRT Student Special Interest Group

THE CANADIAN SOCIETY OF RESPIRATORY THERAPISTS
LA SOCIÉTÉ CANADIENNE DES THÉRAPEUTES RESPIRATOIRES
RtWeekS E M A I N E D E L A T H É R A P I E R E S P I R A T O I R E
RReessppiirraattoorryy TThheerraappyy WWeeeekk“Our goal
is simple...”
NATIONAL RESPIRATORY THERAPY WEEK
Share the air
!
Thank you for not smoking
Share the air
!
Items are available year round
Les items sont disponibles pendant toute l’année
RT WEEK POSTERPoster “Semaine de laThérapie Respiratoire”Perfect to display inyour department, facilityor in the community.Item R97$4.00/ea Member$5.50/ea Non-member
THE CANADIAN SOCIETY OF RESPIRATORY THERAPISTS
LA SOCIÉTÉ CANADIENNE DES THÉRAPEUTES RESPIRATOIRES
THE CANADIAN SOCIETY OF RESPIRATORY THERAPISTS
LA SOCIÉTÉ CANADIENNE DES THÉRAPEUTES RESPIRATOIRES
THE CANADIAN SOCIETY OF RESPIRATORY THERAPISTS
LA SOCIÉTÉ CANADIENNE DES THÉRAPEUTES RESPIRATOIRESSSeemmaaiinnee ddee llaa TThhéérraappiiee RReessppiirraattooiirree“Notre but
est simple ...”
THE CANADIAN SOCIETY OF RESPIRATORY THERAPISTS
LA SOCIÉTÉ CANADIENNE DES THÉRAPEUTES RESPIRATOIRES
October 3 – 9, 2004
Partagez l’ai
r!
Merci de ne pas fumer
Partagez l’ai
r!
THE CANADIAN SOCIETY OF RESPIRATORY THERAPISTS
LA SOCIÉTÉ CANADIENNE DES THÉRAPEUTES RESPIRATOIRES
NO SMOKING POSTERA powerful message.Display it everywhere.Poster “Ne Pas Fumer”Item R97/7$4.00/ea Member$5.50/ea Non-member

CLIC PENWhite and blue pen, CSRT colour logo.Item R00/1 (10/pkg)$10.50/ pkg Member$13.50/pkg Non-member
CSRT PINSRed lapel pin with gold writing.Item R99/1 (5/pkg)$17.50/pkg Member$20.00/pkg Non-member
“MEET A RESPIRATORY THERAPIST” ACTIVITY SHEET
One-page puzzle sheet for children.Word search. Fill in the blanks.Colour by number.Gummed pads/50 sheets/padItem R01/1$6.00/each Member$8.00/each Non-member
CSRT DENIM SHIRTS-XXLCSRT Colour logo.Item R00/5$48.00 Member$60.00 Non-member
FLASHLIGHT KEYCHAINCSRT colour logo.Item R00/2 (5/pkg)$10.00/pkg Member$13.50/pkg Non-member
BROCHURE“What is a RespiratoryTherapist?”(10/pkg)One package free with a$25.00 order$10.00/pkg Member$15.00/pkg Non-member
FREE
Respiratory Therapists Inspire!
Respiratory Word Search
a s l w p n a s t h m a d t o a k t
g r u b r e a t h e e l y s b i t r
k r n e s g m i y s a a n j t r g a
e l g x o y s r c a t c r u e w f c
n j s e a x t a c n q u h t r a e h
r a t s n o r e w i n p e e r y g e
t o a c n k e g h y r l a b a i r a
asthma oxygen airway lungs breathe trachea snore heart
The Canadian Society of Respiratory TherapistsLa Société Canadienne des Thérapeutes Respiratoires
AAiir Breaatth
LLuunngs
WhaWhat is a Respirat is a Respirattorory Therapisy Therapist ?t ?Our lungs breathe in oxygen and breathe out carbon dioxide. Respiratory therapistsmake sure our lungs are doing their job.
■ They help babies, children and grown-ups who have trouble breathing.
■ They show people with asthma the right way to use inhalers.
■ They make sure patients stay sound asleep when they have operations.
■ They teach people who smoke cigarettes how to quit.
■ They help people sleep better by teaching them to stop snoring.
■ Respiratory therapists are breathing experts!
CCan yan you get the air throu get the air through theough thellunungs intgs into the bo the ballalloons?oons?
BRUSHED NICKEL BALL POINTPEN WITH ILLUMINATING TIPGreat for low-light writingNavy Blue, engraved CSRTItem R004/03$5.50/each Member$7.00/each Non-Member
CSRT POST-IT NOTES25 sheets per pad.Item R04/1 (5/pkg)$3.75/pkg Member$4.25/pkg Non-member
THE CANADIAN SOCIETY OF RESPIRATORY THERAPISTSLA SOCIÉTÉ CANADIENNE DES THÉRAPEUTES RESPIRATORIES
1-800-267-3422 WWW.CSRT.COM

TABLE TENTSMake a statement! Personalizewith activities you haveplanned for your facility.Item R8 (25/pkg)$12.50/pkg Member$15.00/pkg Non-member
MOUSE PADRemember our CSRT website address.Teal and White.Item R98/5 (2/pkg)$11.00/pkg Member$13.00/pkg Non-member
CSRT BUTTONSItem R97c/ (10/pkg)$ 8.00/pkg Member$10.00/pkg Non-Member
FRIDGE MAGNETS2"x2.5"Colour logo.Item R00/3 (10/pkg)$3.50/pkg Member$4.50/pkg Non-member
CSRT SCREWDRIVERWhite handle, colour logo.R00/4 (5/pkg)$6.50/pkg Member$8.50/pkg Non-member
CSRT CARABEENERSBlue laser engraved CSRT on the side.Item R002/1 $ 4.00/each Member$10.00/each Non-Member
“NEON” PENCILSColourful giveaway. “Neon” Pencils in bright yellow, green and orange.Item R98/4 (10/pkg)$6.00/pkg Member $7.50/pkg Non-member
CSRT TOTEHeavy, reinforced canvass. Side pocket with CSRT logo, navy or red.Item R004 $15.00/each or 2 for $25.00 Member$18.00/each or 2 for $35.00 Non-Member
NEW

Canadian Society of Respiratory Therapists / La Société Canadienne des Thérapeutes Respiratoires102 – 1785 Alta Vista Drive, Ottawa ON K1G 3Y6 TEL (613) 731-3164 or 800 267-3422 FAX (613) 521-4314 EMAIL [email protected] HOMEPAGE www.csrt.com
Order Form / Formulaire de Commande
THE CANADIAN SOCIETY OF RESPIRATORY THERAPISTS
LA SOCIÉTÉ CANADIENNE DES THÉRAPEUTES RESPIRATOIRES
Respiratory Therapy WeekSemaine de la thérapie respiratoire
Payment is due upon receipt ofinvoice (Please provide a purchaseorder number)
Paiement est due à la réception dela facture (Veuillez fournier unnuméro de bon d’achat)
CARD NUMBER | | | | | | | | | | | | | | | | | | | |
SIGNATURE
CONTACT PERSON / PERSONNE CONTACTE MEMBER NUMBER / NUMÉRO DE MEMBRE
ADDRESS / ADRESSE
TELEPHONE / TÉlÉPHONE FAX PURCHASE ORDER / BON D’ACHAT
DEPARTMENT / DÉPARTEMENT
POSTAL CODE / CODE POSTAL
NAME OF INSTITUTION / NOM DE L’INSTITUTION
Method of Payment / Méthode de paiement
We will accept your order by mail or faxNous accepterons vos commandes par la poste ou par télécopie
SHIP TO/ENVOYEZ À:
subtotal/sous-total
y a
EXPIRY DATE
Cheque or money order enclosed.Payable to the CSRT.
Inclure un chèque ou un mandatde poste. Faire votre paiement àl’ordre de la SCTR.
7% GST/TPS
15% HST/TVH
TOTAL
(NS, NF and NB only)
Minimum order $25.00 / Commande minimum 25,00 $Deadline for orders: September 24, 2004
Échéance pour commandes : 24 septembre 2004
Quantity/quantité Item # Description Price / Prix Total
shipping & handling $10.00

Summer 2004 Canadian Journal of Respiratory Therapy — www.csrt.com 19
CoARTE and the National Competency ProfileThe Council on Accreditation for RespiratoryTherapy Education (CoARTE), has based theiraccreditation standards on ISO principles and the cross referencing of the Respiratory Therapy Education program to the CSRTOccupational Profile.
In 2003, the Provincial Regulatory Bodies and the CSRT began the creation of a new profileentitled the “National Competency Profile” (NCP)which outlines the competencies for practicingand entry level therapists. The CSRT has been anequal partner in this process from the beginningand as such supports the implementation of thisdocument. CoARTE, as a council of the CSRTalso supports the proper implementation of thisdocument.
When the CSRT and the Alliance members feelall stakeholders are prepared for the implementa-tion of the NCP, CoARTE, as one of these stake-holders will also be prepared to use the NCP inits processes.
In order to assist the schools and CoARTE withthe implementation of the NCP, the CSRT ispreparing supporting documentation. Thissupporting documentation can be usedvoluntarily by the schools and CoARTE to help ensure the various curricula result in stu-dents that have achieved all of the competencieslisted in the NCP.
This is an exciting time for the RespiratoryTherapy profession. We are approaching a transi-tional period where respiratory therapy programsin Canadian when schools will implement allcompetencies in the new National CompetencyProfile. CoARTE is looking forward to a continu-ing collaborative partnership with the CSRT, theschools and the members of the National
Alliance in providing high quality educationalprograms, for entry-level Respiratory Therapist,in the interest of safe patient care.
CoARTE MembershipTom Dorval, Instructor at the University of theCariboo in Kamloops has now taken over RayHubble's position as the national representativefor didactic education on CoARTE. On behalf ofCoARTE and the CSRT, we welcome you andthank you for accepting the position.
Ray Hubble, Instructor at the New BrunswickCommunity College in Saint John, is now aMember of the CSRT's Board of Directors. He now holds the position of Director ofEducation and Clinical Standards and he will bea valuable resource to CoARTE on matters per-taining to the new National Competency Profile.
Upcoming Site VisitsAlgonquin College, La Cité collégiale andCanadore College in Ontraio are scheduled forsite visits in January, February and April 2005,respectively.
Would you like to get involved with CoARTE?CoARTE is always looking for volunteers to serve as program reviewers on teams for accreditationof respiratory therapy programs. Each team con-sists of respiratory therapists, a senior education-al administrator and a physician. Training work-shops are offered for individuals eligible to par-ticipate on program review teams.
If you would like more information on the next training workshop, please call MichelleKowlessar, Accreditation and Education Managerat 1-800-267-3422 x26 or e-mail [email protected]
CoARTE UpdateMichelle Kowlessar, Accreditation and Education Manager
CoARTE Update

20 Été 2004 Revue canadienne de la thérapie respiratoire — www.csrt.com
Canadian Healthcare Workers Report
The Report reviewed four years of data (2000 – 2003) and represents healthcare casesfrom across Canada.
Key findings of the Report suggest:
■ A growing number of hospital workers areaccessing Employee Assistance Programs(EAPS). EAP utilization increased over threeyears (3.96 % in 2000 to 5.36 % in 2002) andspiked in 2003 (6.59 %)
■ Hospital workers face high stress around issuesof respect and security, including workplaceclosure, employee termination and violence inthe workplace
■ The year of the SARS epidemic (2003) sawelevated symptoms of depression, anxiety,workplace stress and marital-relationshipdiscord among hospital workers
■ The largest single source of trauma for hospitalworkers in any one year was workplacetrauma, accounting for over 92 % of traumacounselling in 2003.
Trauma counselling for the death of an employeehas increased 4.5 times in the last three years(2.21 % in 2000 to 10 % in 2002).
The Canadian healthcare sector employs 824,600people or approximately five per cent of theemployed labour force.
The Canadian healthcare system has seendramatic changes in the last 15 years, especiallyin the hospital environment. Government cut-backs and downsizing in the sector have lead toa widespread shortage of hospital workers andlonger waits for healthcare.
For a copy of the Report:David Eisenstadt, Beth Merrick, Regina LevyLaura Macdonald
The Communications Group Inc.WarrenShepell (416) 696-9900 or (800)-267-4476(416) 961-0023 or (800)-461-9972
Healthcare Assistance Programs NeedImprovement
A Report released by the WarrenShepell Research Group which examined the
mental health of Canadian employees in the healthcare sector, indicates that hospital
organizations need to improve the wellbeing of workers to alleviate employee stress
and prevent future burnout.

Summer 2004 Canadian Journal of Respiratory Therapy — www.csrt.com 21
CALENDAR OF EVENTSAugust 20 – 22, 200413th Annual NationalNeurotrauma ConferenceLudhiana Indiawww.neurotrauma2004.com
September 4 – 8, 200414th European RespiratorySociety Annual CongressGlasgow, [email protected]
September 9 – 12, 20049th International Congress ofCardiothoracic and VascularAnesthesiaTokyo, Japanwww.jscva.org/iccva2004/index.html
September 11, 20042004 Obstetric AnesthesiaConferenceToronto, Ontariowww.mtsinai.on.ca/Seminars/Ce/Anesthesia/default.htm
September 15 – 18, 20047th Asia Pacific Conference on Tobacco or HealthGyeongju, Republic of Korea www.apact2004.org/
September 18 – 22, 200463rd National ScientificCongress of the AustralianSociety of AnaesthetistsSydney, Australiawww.asa2004.com/
October 7, 200415th Annual Meeting ofthe European Society forComputing and Technology in Anesthesia and Intensive CareToulouse, [email protected]
October 10 – 13, 200417th Annual Congress of the European Society of Intensive Care MedicineBerlin, Germanywww.esicm.org
October 18 – 19, 2004The 16th Annual EdmontonPalliative Care ConferenceCalgary, Albertawww.palliative.org
October 22 – 23, 2004RTSNS Fall ConferenceHalifax, Nova Scotiawww.rtsns.com
October 23 – 29, 2004Canadian Cardiovascular Congress 2004Calgary, Albertawww.ccs.ca/
October 23 – 30, 2004CHEST 2004 – AACP’s 70thAnnual International ScientificAssembly and the ClinicalWorld Congress on Diseases of the ChestSeattle, [email protected]
October 23 – 27, 2004Canadian CardiovascularCongressCalgary, Albertawww.ccs.ca/
October 25 – 26, 200414th Annual Canadian HomeCare Association Conference Halifax Nova Scotiawww.cdnhomecare.on.ca/
November 15 – 17, 2004Ontario Hospital AssociationHealthAchieve 2004Toronto, Ontariowww.oha.com/oha/ohawm.nsf?OpenDatabase
December 4 – 7, 200450th International RespiratoryCongressAmerican Association forRespiratory CareNew Orleans, [email protected]
Calendar of Events
Smoking Quitlines
71% of all smokers want to quit.The 2001 Canadian Tobacco UseMonitoring Survey found that 54% ofcurrent smokers aged 15 and overintended to quit smoking in the next sixmonths, and another 17% intended to quit in the next 30 days. This is a veryhigh proportion of smokers who arecontemplating quitting smoking.
Quitlines can helpIn recent years there has been increasinginterest in using telephone quitlines aspart of an integrated and steppedapproach to smoking cessation to helpsmokers successfully quit smoking. All Canadian provinces have operationalquitlines and options are being exploredfor service in the territories
A quitline is a free, confidential telephoneservice for all smokers, whether or notthey are interested in quitting and for theirfamily and friends who would like tohelp. A trained counsellor answers thecalls and offers information, advice andsupport in developing an individual quitplan. They also refer callers to communityservices and resources and provide callersand health care providers with promotion-al and educational materials.
Quitlines have the potential to provide anaccessible, high reach, low cost service.They can be both the point of entry forpeople into the smoking cessation systemand/or offer counselling services. A recent review found that long term (12–18 months) quit rates ranged from11% to 22% and that Canadian quitlinescurrently reach between .1 and 5% of the population.
For more information:http://www.cctc.ca/

22 Été 2004 Revue canadienne de la thérapie respiratoire — www.csrt.com
Can a Standardized Acupuncture Technique PalliateDisabling Breathlessness* A Single-Blind, Placebo-Controlled Crossover Study
George T. Lewith, MA, DM; Philip Prescott, BSc, PhDand Carol L. Davis, MBBS
* From the Complementary Medicine Research Unit (Dr. Lewith), Royal South Hants Hospital, Southampton, UK;Faculty of Mathematical Studies (Dr. Prescott), University ofSouthampton, Southampton, UK; and CountessMountbatten House (Dr. Davis), Southampton, UK. Correspondence to: George T. Lewith, MA, DM,Complementary Medicine Research Unit, Mail PointOPH, Royal South Hants Hospital, Southampton, SO140YG UK; e-mail: [email protected] Study objectives: The management of disablingbreathlessness is poor, and a standardized form ofacupuncture has been reported as offering benefit. This study was designed to evaluate the efficacy ofstandardized acupuncture treatment. Design: A single-blind, randomized, crossover study. Setting: This study was carried out on a domiciliarybasis in Southampton (UK). Interventions: This study evaluated a standardizedacupuncture technique vs an appropriately validatedplacebo/control (mock transcutaneous electrical nervestimulation [TENS]) for disabling, nonmalignant breath-lessness (largely COPD). The acupuncture was providedby an appropriately trained nurse acupuncturist. Eachpatient received six treatments in each phase of thestudy, with an intervening 2-week washout period. Measurements and results: The primary outcome wasworst breathlessness (visual analog scale, 0 to 100 mm),with the sample size based on an 80% power to detecta 10-mm difference between treatment means.Secondary outcomes included the St George’srespiratory questionnaire score and treatment credibility. Results: Thirty-six patients were entered into the study(33 with COPD), and 24 patients completed both treat-ment phases. The primary outcome improved signifi-cantly during the course of the study, but there were nosignificant treatment differences between acupunctureand the placebo/control of mock TENS for either primaryor secondary outcomes. The placebo was shown to be acredible control. There was no evidence of a carryovereffect from the first to second phase of the study. Conclusion: This standardized acupuncture techniquedoes not show specific efficacy in disabling nonmalig-nant breathlessness, but those entered into the studydid experience clinically significant benefit from bothtreatments. Key Words: acupuncture; disabling breathlessness;placebo/control; randomized controlled trial(Chest. 2004;125:1783-1790.)© 2004 American College of Chest Physicians
Protective Effects of Sphingosine 1-Phosphate in Murine Endotoxin-induced Inflammatory Lung Injury
Xinqi Peng, Paul M. Hassoun, Saad Sammani, Bryan J.McVerry, Melissa J. Burne, Hamid Rabb, David Pearse,Rubin M. Tuder and Joe G. N. Garcia
Department of Medicine, Divisions of Pulmonary andCritical Care Medicine and Nephrology; Department ofPathology; and the Center for Translational RespiratoryMedicine, Johns Hopkins University School of Medicine,Baltimore, Maryland
Correspondence: Correspondence and requests forreprints should be addressed to Joe G. N. Garcia, M.D.,Center for Translational Respiratory Medicine, Division of Pulmonary and Critical Care Medicine, 5501 HopkinsBayview Circle, Baltimore, MD 21224. E-mail:[email protected] Our prior in vitro studies indicate that sphingosine 1-phosphate (S1P), a phospholipid angiogenic factor,produces endothelial cell barrier enhancement throughligation of endothelial differentiation gene family recep-tors. We hypothesized that S1P may reduce the vascularleak associated with acute lung injury and found thatS1P infusion produced a rapid and significant reductionin lung weight gain (more than 50%) in the isolatedperfused murine lung. The effect of S1P was nextassessed in a murine model of LPS-mediated microvas-cular permeability and inflammation with markedincreases in parameters of lung injury at both 6 and 24 hours after intratracheal LPS. Each parameterassessed was significantly reduced by intravenous S1P (1 µM final) and in selected experiments by the S1P ana-logue FTY720 (0.1 mg/kg, intraperitoneally) delivered 1 hour after LPS. S1P produced an approximately40–50% reduction in LPS-mediated extravasation ofEvans blue dye albumin, bronchoalveolar lavage proteincontent, and lung tissue myeloperoxidase activity(reflecting phagocyte infiltration). Consistent with sys-temic barrier enhancement, S1P significantly decreasedEvans blue dye albumin extravasation and myeloperoxi-dase content in renal tissues of LPS-treated mice. Thesestudies indicate that S1P significantly decreases pul-monary/renal vascular leakage and inflammation in a murinemodel of LPS-mediated acute lung injury and mayrepresent a novel therapeutic strategy for vascularbarrier dysfunction. Key Words: permeability; inflammation; sphingolipids;acute respiratory distress syndromeAmerican Journal of Respiratory and Critical CareMedicine Vol 169. pp. 1245-1251, (2004)© 2004 American Thoracic Society
Abstracts
SCIENTIFIC NEWS

Summer 2004 Canadian Journal of Respiratory Therapy — www.csrt.com 23
Treatment of Lobar Atelectasis With SurfactantLavage in the Neonate
Case History38 year-old G2P1 mother is referred to the HighRisk Pregnancy Service at Mount Sinai Hospital.The prenatal diagnosis of hydrops fetalis is madein the presence of bilateral pleural effusions andmild ascites diagnosed at the 28-week ultra-sound. Bilateral in utero chest drains are insertedinto the fetus to relieve the effusions. Unfor-unalety premature labour ensues. A single doseof Celestone is given and an emergency caesare-an section is performed for fetal distress.
Baby M is born at 32 weeks gestation, a birthweight of 2230 grams and APGARs of 5 at oneminute, 7 at five minutes and 8 at ten minutes.Baby M is apneic at birth and requires positivepressure ventilation and intubation at 5 minutesof life. The in utero chest drains are clampedand removed. A right pneumothorax is diag-nosed and relieved by needle thoracentesis for40 ml of air. Subsequently a chest tube wasplaced on the right side. The left chest drain wasremoved and replaced with a left chest tube,which drained serous fluid. The patient is addi-tionally hypotensive and received three 10ml/kgboluses of normal saline and a dopamine infu-sion of 10 mcg/kg/min. The patient is stabilizedon synchronized intermittent mandatory ventila-tion (SIMV), respiratory rate (RR) of 36 breathsper minute (bpm), peak inspiratory pressures(PIP) of 20 cmH20, a positive end expiratorypressure (PEEP) of 5 cmH2O and a fraction ofinspired oxygen (FiO2) of 0.25 using the VIPGold Bird Ventilator. (Bird Products Corporation1100 Bird Center Drive, Palm Springs, CA.) The
patient subsequently required mechanical venti-lation for 8 weeks due to persistent bilateralpleural effusions secondary to hydops fetalis.
Clinical PresentationAt day 55 in the NICU (39 6/7 weeks correctedage) Baby M is extubated to nasal pharyngealtube (NPT) continuous positive airway pressure(CPAP). NPT CPAP is utilized to maintain anadequate functional residual capacity (FRC) inthe presence of bilateral pleural effusions. Thepatient tolerates extubation well and remains
Scientif ic News
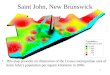
Figure 1
A/P Chest roentgenogram taken after Baby M presentedwith increased work of breathing. There is a focal rightupper and middle lobe atelectasis.
Craig Campbell, B.Sc, RRCP/RRT, Registered Respiratory Care Practitioner, Neonatal Intensive Care UnitMount Sinai Hospital, Toronto, Ontario
Dr. Kin Fan Young-Tai, MB.BS, FRCPC, MHSc, Directory of Nurseries, Department of Paediatrics, Mount Sinai Hospital, Toronto, Ontario

24 Été 2004 Revue canadienne de la thérapie respiratoire — www.csrt.com
Scientif ic News
stable for the next 36 hours on NPT CPAP of 10 cmH20 and FiO2 of 0.45 only requiring tran-sient increases in oxygen for handling. On day58 the patient is noted to have tachypnea andincreased work of breathing. The NPT waschanged and large amounts of yellowish secre-tions were noted in the tube. The patientimproved for 3 hours at which time increasedwork of breathing is again noted and a chestroentgenogram is ordered. The chestroentgenogram reveals a focal right upper andmiddle lobe atelectasis secondary to consolida-tion from an undiagnosed pneumonia. There is aright basal chest drain in situ and a small rightbasal pneumothorax is noted. (Figure 1.) Baby M is re-intubated at this point and mechan-ically ventilated with the following parameters:Assist Control, RR-20 bpm PIP-20 cmH20, PEEP-8cmH20 MAP-11.6 cmH20 and FiO2-0.75. Baby Mis positioned with the right chest elevated to facilitate drainage of the right upper lobe and frequent suctioning is undertaken to clear secretions. Arterial blood gas (ABG) after 2 hours pH-7.48, PaCO2-69 mmHg, PaO2-74 mmHg, HCO3-22.3 mEq. The PEEP isincreased to 9 cm H20 further increasing themean airway pressure in an attempt to recruit the atelectatic regions and facilitate better oxy-genation. This manifests in a decrease in theFiO2 from 0.75 to 0.55 however the atelectasispersisted. The patient is stable for the remainderof the day with the PIP weaned to 18 cmH20. Onday 4 the ETT blocked with secretions and isexchanged with the patient remaining on thesame ventilation with an FiO2 of 0.55. ETT aspi-rates revealed heavy growth of enterobacter cloa-cae, +/- pus cells, +/- epithelial cells. At chestroentgenogram at midday displays the persistentright upper lobe collapse. (Figure 2.) Baby M remains stable in an FiO2 of 0.55. By midafternoon with no improvement in oxy-genation and no resolution of the atelectasis after30 hours of intubation a decision is made to trya selective surfactant lavage of the right lung.The standard procedure in the neonatal intensivecare unit (NICU) at Mount Sinai Hospital is tocombine 2.5 mL/kg of Bovine Lipid ExtractSurfactant (BLES, 27 mg/mL phospholipid)
in a 1:4 ratio with 0.9% sodium chloride (NaCl).The solution is then administered in 2.0 mLaliquots followed with suctioning of theendotracheal tube after each aliquot. Suctionlevels are set at 100 mmHg and only one pass isperformed per instillation. Following the lavage adose of 2.5 mL/kg of BLES is administered bydirect instillation.
In this case a single lung is the target for thelavage and it is rationalized to use half of thenormal lavage dose. The solution to lavage theright lung consists of 1.25 mL/kg of BLES (33.75 mg phospholipid) diluted in a 1:4 ratiowith 0.9% NaCl. The patients weight was 3440grams so 4.5 mL of BLES was diluted with 18 mLof 0.9% NaCl for a total volume of 22.5 mL. BabyM is placed in the right lateral recumbent posi-tion for the lavage allowing gravity to assist indirecting the lavage solution into the right main-stem bronchus. A #5fr. feeding tube is inserteddown the ETT and extended 1.0 cm beyond thetip to facilitate right lung deposition of the lavagesolution. The solution was then instilled in 2.0mL aliquots and the patient is manually ventilat-ed to distribute to the solution. Pressures for
Figure 2
A/P Chest roentgenogram taken after 24 hours ofincreased PEEP and positioning with right sidedelevation. There is no resolution of the atelectasis.

Summer 2004 Canadian Journal of Respiratory Therapy — www.csrt.com 25
manual ventilation were maintained at a PIP of 20 cmH2O and a PEEP of 8–10 cmH20.Suctioning of the patient yields significantsecretions, which are thick and primarily whitein colour with slight blood tinge. Most of thesecretions are attained after the first 8–10 cyclesof instillation and suctioning. The procedure waswell tolerated by the patient. Vital signsremained stable throughout. Baby M continues tobe in the right lateral recumbent position on theventilator with the following settings: AC RR-20,PC-18, PEEP-9, It-0.40 and FiO2 0.40. The FiO2
decreases over the next four hours to 0.30. A follow-up chest roentgenogram (Figure 3) isdone at 2038, 4.5 hours after the procedure.There is significantly improved aeration of theright upper lobe. The patient's ventilation isweaned significantly the following day withcontinued improvement in oxygenation. Thepatient is subsequently extubated 36 hours afterthe lavage to NPT CPAP of 10 cmH20 and anFiO2 of 0.30.
DiscussionPersistent regional atelectasis presents the neona-tal clinician with limited management options.Bronchoscopy to improve atelectasis and consoli-dation is not an option due to the small ETTsize. Other procedures aim at the indirect treat-ment of the atelectasis through positioning,recruitment of lung tissue through increased ven-tilatory pressures, recruitment manoeuvres or fre-quent suctioning to clear secretions. Positioningthe patient with the atelectatic region superior tothe rest of the lung field can facilitate drainage ofthe affected region via gravity. This however isoften not sufficient when tenacious secretions arethe cause of the atelectasis. Lung recruitmentmay be achieved by increasing PIP and/or PEEPlevels over a period of time. One must be cau-tious however since ventilation may preferential-ly travel to the well inflated lung region awayfrom the atelectatic regions. The clinician mustbe aware that a portion of the lung is consolidat-ed and he/she is in essence ventilating a smallerlung. This can lead to over distension and stretchinjury in the ventilated regions. A tidal volume of 4–6 mL/kg that only travels to half of the lung is actually ventilating those regions with
8–12 mL/kg.1 The use of recruitment manoeuvreswhere by the lung is held inflated at an elevatedPEEP level for a period of time without inter-spersed breaths has received little study in theneonatal population. Recruitment manoeuvresare not utilized in this case due to the lack ofresearch and experience with them in our patientpopulation. Frequent suctioning will clear thelarge airways of secretions however the distal airways cannot be reached and may beunaffected by suctioning. Persistent suctioningcan also lead to airway trauma and derecruit-ment of lung regions.
Surfactant lavage is a relatively new procedurethat has been employed in neonates primarily formeconium aspiration syndrome (MAS). There islimited clinical research utilizing surfactant lavage in human trials for MAS. In a small studyLam et al demonstrated surfactant lavage to be a safe and effective procedure for treatmentof severe MAS when compared with historic
Scientif ic News
Figure 3
A/P Chest roentgenogram taken after 24 hours ofincreased PEEP and positioning with right sidedelevation. There is no resolution of the atelectasis.

26 Été 2004 Revue canadienne de la thérapie respiratoire — www.csrt.com
controls.2 Wiswell et al enrolled 22 infants with MAS into a study utilizing Surfaxin®(Lucinactant) and concluded the procedure to besafe and potentially effective.3 Dilute surfactantsolution has been shown through radioisotopelabelling to increase the dispersion of surfactantcompared with bolus surfactant administration.4
This may explain the ability of the lavage solu-tion to penetrate atelectatic regions forming aphospholipid monolayer and decreasing surfacetension. Surfactant will function as a detergent toincrease the mobilization of secretions andimprove oxygenation post procedure when com-pared with saline lavage.5,6 This was evident inthe large amount of secretions suctioned fromBaby M during the procedure relative to suction-ing undertaken previously with either dry passesor normal saline instillation. The recruited alveolimay then be stabilized with appropriate ventila-tion. Bacterial pneumonia has been shown toimpair the surfactant system by reducing theconstituents of surfactant.7,8 The surfactant lavageprocedure will deposit some residual surfactantin the affected area acting as replacement tolosses from a bacterial species. Surfactant lavagefor lobar atelectasis secondary to bacterial pneu-monia provides an effective and definitive treat-ment in this case study. Evidence supportingsuch therapies is lacking, however in theory thelavage fluid should be able to;
1. Penetrate regions of atelectasis and decreasesurface tension that in conjunction withappropriate ventilation strategies can stabilizealveolar regions
2. Detergent action of surfactant may facilitatesecretion clearance
3. Residual surfactant can replace innatesurfactant impaired by bacterial colonization.
Surfactant lavage is a safe procedure when per-formed by appropriate personnel with cardiores-piratory monitoring. Cases such as Baby M showpotential benefits to the procedure outside ofmeconium aspiration. Further study is requiredto ascertain the efficacy of surfactant lavage forvarious neonatal pathologies.
References1. Clark R, Gerstmann D, Jobe A, Moffitt S, Slutsky A,
Yoder B. Lung injury in neonates: causes, strategiesfor prevention, and long-term consequences.J Pediatr 2001; 139:478-86.
2. Lam B, Yeung C. Surfactant lavage for meconiumaspiration syndrome: a pilot study. Pediatrics 1999;103 (5):1014-18.
3. Wiswell T, Knight G, Finer N, Donn S, Desai H,Walsh W, et al. A multicenter, randomized, con-trolled trial comparing surfaxin (lucinactant) lavagewith standard care for treatment of Meconium aspi-ration syndrome. Pediatrics 2002; 109 (6): 1081-87.
4. Balaraman V, Sood S, Finn K, Hashiro G, Uyehara C,Easa D. Physiological response and lung distributionof lavage versus bolus Exosurf® in piglets with acutelung injury. Am J Respir Crit Care Med. 1996; 153:1838-43.
5. Lam B. Surfactant lavage for the management ofsevere meconium aspiration syndrome. Biol Neonate.1999; 76(suppl 1): 10-14.
6. Charles G, Cochrane S, Revak T, Allen M,Schraufstatter I, Robert C, et al. Bronchoalveolarlavage with KL4-Surfactant in models of meconiumaspiration syndrome. Pediatr Res. 1998; 44(5): 705-15.
7. Greenough A. Expanded use of surfactant replace-ment therapy. Eur J Pediatr. 2000; 159: 635-40.
8. Baughman R, Sternberg R, Hull W, Bushsbaum J,Whitsett J. Decreased surfactant protein A inpatients with bacterial pneumonia. Am Rev RespirDis. 1993; 147: 653-57.
Scientif ic News

Summer 2004 Canadian Journal of Respiratory Therapy — www.csrt.com 27
INDUSTRY NEWS
Airsonett is the marketing distribu-tor of a new Swedish mobile airpurification system. This system,the Airsonett Airshower, delivers“clean room” quality air directly tothe breathing zone of an individual.
A unique one-of-kind technology,the patented Airsonett Airshower is a self-contained mobile airpurifier based on the principle of non-turbulent displacement air flow. At least 99.95 % of airborne particles greater than 0.3 micron are removed such asviruses, bacteria, mite pollution andpollen. Previously only available toindustrial-type “clean room” facili-ties, this marks the first applicationof this proven technology to thehome health/medical markets.Users of the unit include individualasthma, allergy or upper respiratorysufferers, individuals with sleepdisorders, patients who need to beprotected from airborne infection,treatment for Chronic ObstructivePulmonary Disease (COPD) plusmany other applications.
The Airsonett Airshower will bemarketed to a sales distribution net-work throughout the U.S. andCanada as well as through medicaloutlets, allergists, immunologists,respiratory therapists, dentists,pulmonologists, hospitals, nursinghomes and sleep centers.
www.airsonett.com.
Swedish Mobile Air Purification System
Clean, slightly cooled air moves slowly downward and because of itssomewhat higher density displaces the conventional ambient air withnegible turbulence and mixing. This creates a zone of clean air qualityaround the head of the individual who is normally seated or lying down.

28 Été 2004 Revue canadienne de la thérapie respiratoire — www.csrt.com
Executive SummaryOn March 12, 2003, the World HealthOrganization (WHO) announced a global out-break of an atypical pneumonia that was quicklynamed Severe Acute Respiratory Syndrome (SARS)and shortly thereafter determined to be caused by a novel coronavirus. The virus spread interna-tionally along travel routes and caused the well-documented nosocomial outbreaks in the GreaterToronto Area, China, Hong Kong, Vietnam andSingapore. Contact, droplet and airborne precau-tions were reportedly instituted in affected hospi-tals; however, they were apparently incomplete,intermittently applied or only partially effective.
The Canadian outbreak resulted in 438 cases, 51% of these were health care workers (HCWs)with three related deaths. The objective of thisreport is to summarize our findings from an analy-sis of the key domains, as pertinent to improvingthe effectiveness of facial protective equipment(FPE) in preventing occupational-associated respi-ratory disease transmission in healthcare workers.
The report includes:
1. A review of the scientific literature dealing withbioaerosols, filtration and how this influencesthe design and performance of FPE
2. A review of the scientific literature of theorganizational, environmental and individualfactors that influence the effectiveness ofoccupational health and safety in general, andinfection control procedures, in particular
3. An analysis of these factors as identifiedthrough a series of 15 focus group discussionsinvolving front-line healthcare workers and
4. A framework for assigning priorities for furtherresearch and a list of priorities derived from thegaps identified in the literature review and thepriorities of front-line healthcare workers.
Facial Protective Equipment Report
The Change Foundation and OHA have released a report to help protect hospital and
healthcare staff from future outbreaks of infectious diseases. For the complete document
go to their website at www.changefoundation.com/
AstraZeneca IncreasesAsthma Research Funding
AstraZeneca has announced additional fund-ing of $2 million over five years to supportSt. Joseph’s Healthcare/McMaster University’sFirestone Institute. This new additional fund-ing will be used for investigator-initiatedrespiratory research.
Additionally, AstraZeneca will provide aminimum of $5 million over five years to the Canadian Masters Program; three worldclass symposiums directed by the FirestoneInstitute which will facilitate the establish-ment of a cooperative national network offuture Canadian leaders in both communitymedicine and academia, and provide oppor-tunities to examine and discuss advances infront line research with international leaders.
AstraZeneca Canada has also made an addi-tional contribution of $900,000, to support anendowed chair in asthma research at theUniversity of Alberta. AstraZeneca has nowdonated $3 million to support the chairhold-er's work. Researchers will intensify theirefforts to find answers to some of the yet-unanswered questions about the disease.
INDUSTRY NEWS

Summer 2004 Canadian Journal of Respiratory Therapy — www.csrt.com 31
Classif ied and Publice Service Announcements
La Régie régionale de la santé Beauséjour La Régie régionale de la santé Beauséjour, située àMoncton au Nouveau-Brunswick, est le plus vasteregroupement francophone de services de santédans la région de l’Atlantique. Elle regroupel’Hôpital régional Dr-Georges-L.-Dumont, l’HôpitalStella-Maris-de-Kent, le Centre médical régional deShediac, l’Unité de médecine familiale de Dieppe,le Programme extra-mural et le Centre de santédes anciens combattants. Nous sollicitons descandidatures pour les postes suivants:
THÉRAPEUTES RESPIRATOIRES(Temps comple, temps partiel et occasionnel)
Compétences requises :
■ Avoir complété avec succès un cours deformation en thérapie respiratoire;
■ Être membre en règle de l’Associationcanadienne des thérapeutes respiratoires(C.S.R.T.) et/ou de l’Ordre professionnel desthérapeutes respiratoires du Québec (O.P.I.Q.);
■ Maîtriser le français et avoir une connaissancefonctionnelle de l’anglais;
■ Avoir un bon dossier d’emploi et d'assiduité au travail;
■ Être physiquement en mesure de faire le travail assigné.
Pour de plus amples renseignements au sujet denos postes vacants et de la possibilité d’aide à larelocalisation, veuillez communiquer avec :
Monsieur Roger BasqueAgent de recrutementRégie régionale de la santé Beauséjour330, avenue Université Moncton NB E1C 2Z3Téléphone : 506-862-4250courriel : [email protected]
Mission LungFunction LaboratoryRespiratoryTherapist RequiredMission Lung Function LaboratoryRespiratory Therapist, with CARTAcredentials required to perform a varietyof functions including PFT’s, for a verybusy private laboratory in Calgary.Positions availability for the summermonths and to cover maternity leave.Training is provided.Fax resume to Helen (403) 258-3518 oremail [email protected].
Education and Research Days “CaringTogether” will be held October 18 and 19, 2004 at the Fantasyland Hotel, WestEdmonton Mall. Conference topics willcover the physical, psychosocial andspiritual care at the end of life, as well as caring for the caregivers.
For further information, please contactthe conference secretary at:
(780)482-8081; fax (780)450-7700
e-mail: [email protected]
or check the palliative website at
www.palliative.org for updates.
The 16th AnnualEdmonton PalliativeCare Conference
Caring Together

People who care. Work that matters.We welcome all inquiries and thank you for your interest.
To save a life, to get closer to a cure, to teach, to learn, to give someonea second chance and to make an impact…
This is why you chose a health care career. But to make the greatest impact, you need the best tools, the best resources
and the strength of a dedicated team on your side. With a reputation for innovation and excellence, Capital Health
has been recognized as a leading health system for five consecutive years by the Canadian Institute of Health Information.
Affiliated with the University of Alberta, Capital Health is one of Canada's largest academic-based, integrated heath
care regions. Our staff enjoys a vibrant and diverse setting, a strong local economy, high calibre training and,
most importantly, the opportunity to raise the bar.
Enjoy the challenges and rewards offered by a leader in health care.
Visit our website at www.capitalhealth.ca
Talk to us today!
Relocation assistance is available
Capital Health Regional RecruitmentToll-free: 1-877-488-4860 • Local: 408-5940E-mail: [email protected]
Just another reason we’re continuing to raise the bar.
Edmonton, Canada