Embed Size (px)
Citation preview

472
CIRRHOSIS OF THE LIVERSHEILA SHERLOCK, M.D.(EDIN.), M.R.C.P.
Lecturer in Medicine, Postgraduate Medical School of London
Hepatic cirrhosis is a term applied to chronicdiffuse liver disease of varied aetiology. All thedifferent forms of cirrhosis have a common back-ground of hepatic histology. All show disturbanceof the essential lobular architecture of the liver,with proliferation of connective tissue and de-generation, death and regeneration of hepaticcells. Cellular infiltrations, usually with lympho-cytes, and proliferation of bile ducts are nearlyalways present. This common hepatic histologicalpicture may be produced in many different ways.The more important will be discussed.
Aetiology and Pathology of Cirrhosis(i) Classic ' portal '-or Laennec's cirrhosis:
(a) Post-hepatitic.(b) Dietetic.(c) Alcoholic.(d) ' Banti's syndrome.'
(2) Cardiac cirrhosis, associated with congestiveheart failure.
(3) Haemochromatosis, a cirrhosis associatedwith disordered iron metabolism.
(4) Biliary cirrhosis associated with extra-hepatic or intra-hepatic biliary tractobstruction.
(5) Bilharzial cirrhosis associated with bilharzialinfection of the portal venous system.
(6) Hepatolenticular degeneration (Kinnier-Wilson's disease), a cirrhosis withassociated degenerative disease of thecentral nervous system.
(7) Other postulated causes of cirrhosis such aschemical poisons, syphilis and malaria.
(I) CLASSIC 'PORTAL' OR LAENNEC'S CIRRHOSIS(a) Post-Hepatitic CirrhosisAcute infective hepatitis is usually followed by
complete restoration of the liver to normal.However, long-term sequelae are not unknownand, in many instances, hepatic cirrhosis can bedirectly related to a preceding acute infectivehepatitis (Jones and Minot, 1923; Rennie, I945).In these patients serial aspiration liver biopsiesshow a destruction of the normal reticulin frame-work of the liver lobule with nodular regenerationof surviving liver cells and the development of atrue hepatic cirrhosis (Sherlock, I948). (Figs.I, 2, 3, 4.)
The exact importance of acute ' viral' hepatitisin the aetiology of cirrhosis remains uncertain.Ratnoff and Patek (1942) elicited a past history ofjaundice in only 6.5 per cent. of 356 patients withcirrhosis. Howard and Watson (1947), however,obtained a history of previous infective hepatitisin 17 per cent. of patients with cirrhosis con-trasted with 3 per cent. in a similar group withouthepatic disease. The absence of a history of pre-vious jaundice does not exclude acute hepatitis inthe past, for mild attacks may well be passed overas intercurrent infections, quickly forgotten, andnot related to the succeeding hepatic cirrhosis.Kelsall and his co-workers (0947) could find nodifference between the clinical and pathologicalfeatures of cirrhosis developing with no knowncause and those of cirrhosis preceded by hepatitis.There seems no doubt that post-hepatitis cirrhosisand ' classical' Laennec's cirrhosis can presentthe same clinical picture. Future analysis of theeffect of the great war-time epidemics of hepatitison the incidence of cirrhosis will enable theaetiological importance of hepatitis to be betterassessed.
(b) Dietetic CirrhosisInterest in the dietary production of liver lesions
was initiated in 1924 by the observation of Mac-Leod and his group in Toronto that pancreatec-tomized dogs, although maintained on insulin,developed fatty change in the liver. This lesioncould be prevented by choline. Later it wasshown particularly by Himsworth and Glynn(I944) that dietetic deficiencies could result intwo broad types of hepatic pathology. Deficiencyof lipotropic factors (e.g. choline) resulted in fattyinfiltration of the liver and later cirrhosis, whereasdeficiency of first-class protein led to massivehepatic necrosis and scarring, a condition perhapsanalogous to post-hepatitis cirrhosis. The con-stituents of first-class protein which preventsmassive hepatic necrosis were believed to besulphydryl group containing amino acids (e.g.cystine). Methionine which contains both thelipotropic labile methyl and sulphydryl groups willprevent both fatty infiltration and post-necroticscarring. The literature has been well reviewedby Witts (I947).
Application of these observations to disease in
by copyright. on M
arch 6, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.26.299.472 on 1 S
eptember 1950. D
ownloaded from
by copyright.
on March 6, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.26.299.472 on 1 Septem
ber 1950. Dow
nloaded from
by copyright. on M
arch 6, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.26.299.472 on 1 S
eptember 1950. D
ownloaded from
by copyright.
on March 6, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.26.299.472 on 1 Septem
ber 1950. Dow
nloaded from

September 1950 SHERLOCK: Cirrhosis of the Liver 473
J. ,4..
awa.1 .
.,.
A
K *1
. I
ve. '.
FIG. i.-Serum hepatitis, ioth day. Severe acutehepatitis with groups of liver cells surviving inwide areas of necrosis. Best's carmine stain X II 5.
4,
.
FIG. 2.-Serum hepatitis. Same field as in Fig. I,showing preservation of normal reticulin structure.Modified Foot's stain X i6o.
man is more difficult. There seems no doubt thatthe high incidence of liver disease in under-privileged peoples can be related to dietetic de-ficiencies. This is true, for instance, of the fattylivers and pigment cirrhosis of South Africanbabies (Gillman and Gillman, 1945), the malig-nant malnutrition (Kwashiorkor) of children in'Uganda (Trowell, I949), the fatty livers and cirr-hosis of West Indian infants (Waterlow, I947) andthe cirrhosis of the liver common among the poornatives of the Punjab (Hughes, 1933). Certaindiseases which interfere with the intake andmetabolism of amino acids may be associated withdietetic liver lesions. For instance, a fatty liver isa practically constant association with chronicdiarrhoea, particularly in ulcerative colitis, and thismay progress to cirrhosis (Pollard and Block,I948). Patients with amino acid loss in the urine,for instance the Fanconi syndrome, may show fattychange in the liver and cirrhosis. The relation of
ALI.~
FIG. 3.-Same patient 47th day. Fully developedhepatic cirrhosis. Best's carmine stain x I15.
di. J4i.
4...
"
FIG. 4.-Same field as in Fig. 3. Reticulin stains con-firm the destruction of the normal hepatic lobularpattern. Modified Foot's stain X i6o.
alcohol to hepatic cirrhosis will be discussed be-low. Apart from these considerations it seemsunlikely that the dietary intake of protein in thiscountry, even in the poorest groups, is so low as toresult in liver injury and cirrhosis.
(c) Alcoholic cirrhosisHepatic cirrhosis is 6.7 times as frequent in
inebriates as in the temperate population (Jolliffeand Jellinek, I941). However, alcohol poisoningalone will not lead to cirrhosis (Jolliffe and Jellinek,I94I; Best et al., I949), and the relation betweenalcoholism and cirrhosis is probably indirect.Most alcoholics take a poor general diet which isparticularly deficient in protein and lipotropicfactors. At the same time their caloric intake inthe form of alcohol is above normal. An Im-balance between caloric intake and the supply ofessential food factors results, and the consequentcirrhosis is dietetic and analogous to that described
by copyright. on M
arch 6, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.26.299.472 on 1 S
eptember 1950. D
ownloaded from

474 POSTGRADUATE MEDICAL JOURNAL September 1950
above in animals on experimental diets (Best et al.,I949). This type of cirrhosis could probably beprevented by ensuring that alcoholics took notonly adequate calories (alcohol) but also essentialamino acids and lipotropes (first-class protein).
(d) ' Banti's Syndrome' (congestive splenomegaly,splenic anaemia)
In I898 Banti described a primary splenicdisease which was later followed by hepaticcirrhosis. Three stages were recognized, a pre-ascitic in which the disease was confined to thespleen with leukopenia and microcytic hypo-chromic anaemia, an intermediate with enlarge-ment of the liver but with no hepatic symptomsand a third or ascitic stage with ascites, liverfailure and gastrointestinal haemorrhage. How-ever, this clinical history is very rare. In his wideexperience Eppinger (i920) saw only one possibleexample. McNee (I932) states that he never en-countered a case history really showing the se-quence of events originally described. There arenow grave doubts whether Banti's disease exists asa distinct entity. It seems probable that this syn-drome will result from a wide variety of conditions,the common denominator of which is portal venousobstruction. The lesion may be in the splenicveins, in the portal veins (thrombosis, congenitalocclusive bands, cystic dilatation, etc.) or in theliver itself (most varieties of cirrhosis). The leu-kopenia is not specific and occurs in practically allconditions where the spleen is hyperplastic. Theanaemia can usually be related to gastrointestinalhaemorrhage resulting from the portal hyper-
,i
j~jllip j
FIG. 5.-Cardiac cirrhosis. Congestion in the centri-lobular zones from which bands of fibrous tissuepass to adjoining central areas. A portal tract occupiesan apparently central position (reversed lobulation).H.E. X 90.
tension. Overactivity of the splenic pulp (hyper-splenism of Doan and Wright, I946) may alsocontribute to the anaemia.
In clinical medicine there is little useful purposeserved by retaining the term ' Banti's syndrome,'which should be replaced by ' portal venousobstruction ' together with its cause.
2. CARDIAC CIRRHOSISCardiac failure, unless acute and of short dura-
tion, usually results in some centrilobular dis-appearance of liver cells with resultant collapse ofthe reticulin framework at the centre of the hepaticlobule. Reticulin proliferation may follow, spread-ing outwards from the central hepatic vein towardsthe periphery of the lobule. Eventually connectivetissue from one central vein joins the connectivetissue from adjoining lobules (Figs. 5 and 6). Theportal tracts now apparently occupy a centralposition in the hepatic lobule surrounded by theconnective tissue running between the hepaticveins. This is described as reversed lobulation.The lesion is a frank cardiac cirrhosis. This se-quence of events occurs only when the cardiacfailure relapses and is of long duration (Sherlock,1950). It follows that although cardiac cirrhosiscan occur with every type of chronic heart failureit is most frequently associated with mitralvalvular stenosis.
3. HAEMOCHROMATOSISIncreased iron in the liver is distributed both in
the hepatic parenchyma and in the cells of thereticulo-endothelial system. If excessive, this
7.
4.
N' .
(-.
.1>. .\. .
--'
FIG. 6.-Reticulin stains show the condensation andproliferation around the central veins from whichbands pass to neighbouring central veins. Portaltracts normal. Modified Foot's stain x 8o.
by copyright. on M
arch 6, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.26.299.472 on 1 S
eptember 1950. D
ownloaded from

September 1950 SHERLOCK: Cirrhosis of the Liver 475
IL
FIG. 7.-Haemochromatosis. Iron pigment in livercells, Kupffer cells and macrophages of the portaltracts. Fibrosis and disturbance of the hepaticlobular architecture are also seen. Prussian bluestain for iron x I20.
leads to liver cell disintegration and to portaltract fibrosis. Increased haemolysis and hence allforms of haemolytic anaemia are the commonestcauses of hepatic siderosis. Multiple blood trans-fusions may also lead to increased iron in the liver(Schwartz and Blumenthal, I948). However innone of these conditions is the iron deposition ofsufficient extent to provoke such liver cell dis-integration and fibrosis as to warrant the termcirrhosis. In true haemochromatosis there are notonly coarse granules of iron in the liver andreticulo-endothelial cells, but also gross fibrosis,liver cell degeneration and disturbance of thelobular architecture (Fig. 7). Iron absorption fromthe intestines is normal (Fowler and Barer, 1937),and this condition is probably intracellular, inter-fering with the metabolism of the iron containingpigment cytochrome. An acquired form isdescribed in infantile pellagra (Gillman and Gill-man, 1945).
(4) BILIARY CIRRHOSISObstruction to the common bile duct leads to
centrilobular accumulation of bile pigment oftenwith bile-stained focal necrosis of liver cells. Theportal tracts show bile duct proliferation, fibrosisand scanty round-celled infiltration. As thebiliary obstruction continues the fibrosis extendsand increases, passing from portal tract to portaltract so that the lobule is surrounded by a band ofconnective tissue (Fig. 8). The essential lobulararchitecture, however, remains undisturbed andthe lesion is not a true hepatic cirrhosis. Livercell regeneration does not occur in the presence ofbiliary stasis (Mann, Fishbank, Gay and Green,1931). If the biliary obstruction is incomplete,intermittent or surgical relief is possible, then
,.
h--.-
-.
- r
4 4*
-4
FIG. 8.-Unrelieved bile duct obstruction. Bile ductproliferation and fibrosis in the portal tracts whichare becoming joined together. Bile pigment ac-cumulations at the lobular centre. Hepatic lobulararchitecture normal. H.E. x 90.
nodular hyperplasia of liver cells occurs and a truehepatic biliary cirrhosis results (Fig. 9). Gall-stones are the most frequent cause of intermittentbiliary obstruction and of biliary cirrhosis.The histological picture of biliary cirrhosis is
sometimes encountered in patients in whom thebile ducts are patent or even dilated (Dible, Mc-Michael and Sherlock, 1947). The clinicalfeatures and laboratory findings are usually iden-tical with those found in association with obstruc-tion to the extrahepatic bile ducts. This con-dition in the past has received many names,amongst them Hanot's cirrhosis, primary biliarycirrhosis, cholangiolitic biliary cirrhosis, or, wherethere are conspicuous cholesterol deposits in theskin, xanthomatous biliary cirrhosis. The lesionis an obliteration 'of the intrahepatic bile ductsand an infective aetiology seems most likely.
(5) BILHARZIAL CIRRHOSISThis condition is due to invasion of the liver by
the eggs of Bilharzia mansoni. The ova embolizein the portal vein from the intestines and aretrapped in the portal tracts of the liver lobules(Fig. io). A reaction is excited which includesfibrosis and inflammatory cell infiltration withnecrosis of adjoining liver cells. The lesion is atrue hepatic cirrhosis. Bilharzial cirrhosis is foundparticularly in Egypt, Central and West Africa andSouth America.
(6) HEPATO-LENTICULAR DEGENERATION (KINNIER-WILSON S DISEASE)
In I913 Kinnier-Wilson drew attention to theassociation of liver cirrhosis and degeneration ofthe central nervous system and, in particular, ofthe basal' ganglia. The hepatic lesion corres-
by copyright. on M
arch 6, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.26.299.472 on 1 S
eptember 1950. D
ownloaded from

476 POSTGRADUATE MEDICAL JOURNAL September 1950
2
. 4*
..
1.
FIG. 9.-Biliary cirrhosis due to intermittent bile ductdestruction. Note the disturbed hepatic lobulararchitecture. Bile thrombi are conspicuous andadjoin the fibrous bands. H.E. x 8o.
ponds to the general pattern of cirrhosis and his-tologically cannot be distinguished from the usual' portal' variety. The aetiology of the conditionis uncertain. In erythroblastosis foetalis there isa liver lesion and also bile staining of the basalganglia (kernicterus) and rhesus blood groupincompatibility has been cited as the cause ofWilson's disease, particularly as the condition isfamilial. Studies on a large group of patients,however, have failed to show any relationshipbetween the two diseases (Yannet and Lieberman,I946). More interesting is the recent report ofthe association of persistent aminoaciduria andWilson's disease (Uzman and Denny-Brown,1948). This would provide a link between Wil-son's disease and the dietetic cirrhoses.
(7) OTHER POSTULATED CAUSES OF CIRRHOSISChemical poisonsAcute carbon tetrachloride poisoning in man
and experimental animals produces fatty infiltra-tion of the liver. In rats and dogs repeatedadministration of carbon tetrachloride over longperiods is needed to result in hepatic cirrhosis(Bollman and Mann, I93 I; Cameron and Karun-aratne, I936). It might be thought that in man,also, prolonged exposure to the substance wouldlead to cirrhosis. However, this does not seemto be the case and prolonged industrial exposureto carbon tetrachloride appears to promoteresistance rather than susceptibility. Investigationof a large series of workers using carbon tetra-chloride failed to show a single case of cirrhosisdue to the vapour (Smyth and Smyth, I936). - Itappears that carbon tetrachloride is not an impor-tant aetiological factor in cirrhosis. This applies
A.. 1b. *
.PEF j.
I * . .4.f ,.
V. .e .t .d'.
.5
FIG. io.-Bilhazzial cirrhosis. An ovum of B. Mansonihas lodged in a portal tract which shows a cellularreaction. H.E. X 220.
also to the related substances, chloroform andtetrachlorethane.
Arsenical poisoning has been reported withcirrhosis in man but is a rarity and arsenic in-toxication is not an important cause of cirrhosis.The association of cirrhosis in syphilitics havinghad previous organic arsenical therapy is probablythrough a preceding serum hepatitis resultingfrom contaminated syringes.
SyphilisSyphilis was formerly considered an important
factor in the production of hepatic cirrhosis. Thisis apparently not so in adults, although in con-genital syphilitic infants, invasion of the liver bythe spirochaetes does result in pericellular fibrosisand cirrhosis. In adults the only lesion clearlyrelated to syphilis is the gumma, which on healingleaves a scar. These scars may result in a coarselynodular liver (hepar lobatum) but are never sowidespread as to merit the term cirrhosis. Itseems more likely that cirrhosis discovered inpreviously treated syphilitics is in fact related toa previous serum hepatitis. The opportunitiesfor syringe transmission of hepatitis in patientsattending venereal disease clinics is well known.
MalariaMalarial parasites cause a reaction in the reticulo-
endothelial system generally and hence prolifera-tions both of the Kupffer cells of the hepatic
by copyright. on M
arch 6, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.26.299.472 on 1 S
eptember 1950. D
ownloaded from

September 1950 SHERLOCK: Cirrhosis f theLiver 477
sinusoids and the large macrophages of the portaltracts. The destruction of red blood cells leads torelease of bilirubin which further stimulatesreticulo-endothelial proliferation. If severe, theanaemia and fever are associated with centii-lobular liver cell necrosis. These features, how-ever, do not result in chronic diffuse liver diseasewith fibrosis and destruction of the hepatic lobulararchitecture and malaria is of no importance in theaetiology of cirrhosis. The frequent occurrenceof malaria and cirrhosis in the same patient mustbe ascribed to malaria and conditions causingcirrhosis (e.g. bilharziasis, malnutrition) beingsimultaneously present in the community.
Clinical and Laboratory Features of CirrhosisAlthough the various types of cirrhosis have
certain individual characteristics the effects of thelesion are common and can be divided into twomain groups. Firstly there are those related toobstruction of the intrahepatic blood flow withconsequent portal venous hypertension. Thesecond group result from the functional in-adequacy of the hepatic cells. The clinical in-vestigation of a patient suffering from any type ofcirrhosis involves an assessment of the part playedby each of these major factors. The followingaccount refers to classic ' portal ' or Laennec'scirrhosis which is used as a type example. Thedifferential diagnostic features of the othervarieties of cirrhosis will be described later.
ASSESSMENT OF PORTAL VENOUS HYPERTENSIONIn hepatic cirrhosis the distortion of the hepatic
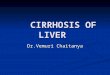
lobular architecture and the fibrosis result in greatdiminution of the intrahepatic vascular bed(McIndoe, I928). The portal venous blood flowis obstructed and the portal venous pressure rises(Whipple, 1945; Blakemore, I948; Davidson,Gibbons and Faloon, 1950). The portal blood isdeviated to channels anastomosing with thesystemic system and the majority of the portalblood may be recovered from these collateralsrather ,than the hepatic vein (Dock, I947). Theclinical diagnosis of portal venous obstruction ispresumptive and depends on the demonstration ofdilated portal-systemic collaterals (Fig. i i). Atten-tion should be paid in the clinical history tohaematemesis which may come not only fromoesophageal varicosities but also from dilated veinsin the stomach wall. Bleeding from haemorrhoidsmust also be noted. The anterior abdominal wallshould be carefully examined for distended veins.a' frank ' caput medusae ' is rare and usually onlyone or two veins are noted running from theumbilical region. The blood flow in these veins isradially away from the umbilicus (Fig. I2). Thisis in contra-distinction to collaterals occurring with
VEI
A ,
(jil/I
FIG. iI.-The effects of obstruction to the portalvenous system.
inferior vena caval obstruction in which the bloodflow is always upwards over the abdominal wall(Fig. I3). Tense ascites leads to functional ob-struction of the inferior vena cava and may causedifficulty in the interpretation of anterior ab-dominal wall veins. The use of infra-red photo-graphy to show up the veins more clearly is to berecommended. As a further diagnostic aid aglucose drink may be given and 30 minutes laterthe glucose content of the blood in the anteriorabdominal wall vein and in an antecubital veinestimated. A higher glucose content in the ab-dominal than in the antecubital vein confirms thatthe abdominal vein is a portal collateral (Sherlockamd Walshe, 1946). Occasionally in cirrhosis theanastomotic umbilical vein may be so dilated that avenous hum can be heard above and to the rightof the umbilicus (Cruveilhier-Baumgarten syn-drome). The size of the spleen in cirrhosis isanother good indication of the degree of portafhypertension. Portal obstruction is also one factorin the production of ascites and this will be dis-cussed later. Oesophageal varicosities can oftenbe demonstrated radiologically using a thickbarium emulsion. Oesophagoscopy is rarely in-dicated. Proctoscopy is used to visualize haemor-rhoids.
by copyright. on M
arch 6, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.26.299.472 on 1 S
eptember 1950. D
ownloaded from

POSTGRADUATE MEDICAL JOURNAL
ASSESSMENT OF HEPATIC CELLULAR FUNCTIONChanges in Bile Pigment Metabolism
Jaundice in a' cirrhotic patient means that therate of destruction of liver cells has exceeded thecapacity for regeneration and the lesion is a de-compensated one. It is therefore of serious con-sequence and considerably worsens the prognosis.Icterus is rarely deep, serum bilirubin values beingof the order of z to 5 mg./ioo ml. In generalthe deeper the jaundice the greater the inadequacyof the liver cell function. Sometimes icterus is pre-cipitated by an acute episode of liver damage suchas an alcoholic bout or an intercurrent infection.In these patients jaundice is not so serious and maywell disappear if the acute condition can be treated.An increase in the serum bilirubin value in cir-rhosis is by no means constant and many patientswith well compensated hepatic lesions have serumbilirubin values of less than i.o mg./ioo ml.The qualitative Van den Bergh reaction and the
proportions of the serum bilirubin acting ' dir-ectly ' and ' indirectly ' with the diazo reagent arenon-contributory in the clinical investigation ofcirrhosis.The bromsulphalein excretion test is a further
sensitive method of estimating liver cell function(Helm and Machella, I942). Bromsulphalein isprobably metabolised very similarly to bilirubinand its retention in the blood stream after intra-venous injection reflects an inability'of the liver toexcrete bile pigment. It is clearly of no value inpatients with raised serum bilirubin concentra-tions in whom there is already a clear indication ofinability to excrete naturally formed bilirubin.
Excess of urinary urobilinogen or its oxidationproduct, urobilin, further indicates failure of livercell function. Urobilinogen is normally absorbedfrom the intestines and re-excreted by the liverinto the bile. If liver cell function fails some ofthis urobilinogen is excreted by the kidneys intothe urine (Fig. I4). Qualitative tests are simplyperformed either for urobilinogen by Ehrlich'saldehyde reaction or for urobilin by Schlesinger'salcoholic zinc acetate method. Daily urine testingfor these substances often gives as good anevaluation of the state of the liver cells in cirrhosisas far more time-consuming laboratory procedures.Bilirubin appears in the urine only when thepatient is frankly jaundiced.
Changes in Protein MetabolismIt is generally accepted that the liver plays a
major role in the regeneration of the plasma pro-teins (Madden and Whipple, I940). This is par-ticularly true Qf the plasma albumin. Someplasma globulin may be formed elsewhere (Sabin,I939). Chronic diffuse liver disease, therefore,results in a diminished plasma albumin level and
V bA
.li +;-'i S :..X4 .i1-,iAti.
1IV..
.41
lJ AdEpc4; tz8,
~ airk i':-* - 4}t
'.+i!es ,7,.,se' . 2 i~ Nii'...Jtti'
4J
FIG.c 12.Diagram of distribution and direction of bloodflow in anterior abdominalI wall veins mn portalvenous obstruction.
this is partially compensated by an increase in theplasma globulin. In general, the lower the plasmaalbumin the greater the extent of hepatic cellnecrosis and the worse the prognosis (Sherlock,1946b).
In active cirrhosis, not only are the plasma Pro-teins quantitatively abnormal but there is a changein their constitution as shown by electrophoreticanalysis (Gray and Barron, 1943). This resultsin positive findings for various flocculation andprecipitation tests. The most useful proceduresare the thymol turbidity and the colloidal goldtests. A positive thymol turbidity (Maclagan,1944) probably indicates continuing inflammatorycell change in the liver. A positive colloidal goldreaction (Gray, 1940) may represent continuingliver cell degeneration, especially with fatty change.It follows that the thymol turbidity test should bemore often positive in post-hepatitis cirrhosis,whereas a positive colloidal gold reaction is'usually associated with nutritional alcoholic cir-rhosis. In practice, results for the two tests incirrhosis usually run in parallel.
478 PSeptemb~er 19[50by copyright.
on March 6, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.26.299.472 on 1 Septem
ber 1950. Dow
nloaded from

SHERLOCK: Cirrhosis of the Liver
FIG. 13.-Diagram of distribution and direction of bloodflow in anterior abdominal wall veins in inferiorvena caval obstruction.
Estimation of the plasma albumin and plasmaglobulin values and performance of the two pre-cipitation tests are useful adjuncts in the diagnosisof cirrhosis and in assessing the progress of thepatient. It should be emphasized, however, thatnormal results for all these procedures are foundin the patient with a well-compensated lesionand should not exclude a diagnosis of cirrhosis(Sherlock, 1946).
Ascites in CirrhosisExperimentally it is clear that portal venous
hypertension per se will not necessarily lea-i toascites (Volwiler, Grindlay and Bollman, 1950).This is also true of such scanty observations asare available in man (Davidson et al., I950; Patti-son, i949). Reduction of the colloid osmoticpressure of the plasma consequent upon thefailure of the liver to maintain the plasma albuminconcentration assists transudation of fluid fromthe capillaries into the peritoneal cavity, but it isdoubtful whether this factor alone ever initiates
ascites in cirrhosis. There is also evidence thatthe peritoneum in patients with cirrhosis andascites is unduly permeable to albumin (Pateket al., 1948). Additional factors may be involved.The urine of cirrhotics with ascites may containan antidiuretic factor perhaps originating fromthe posterior lobe of the pituitary and not in-activated by a damaged liver (Ralli, et al., 1945).Sodium and water retention by the kidney may beanother factor in the maintenance of ascites incirrhosis (Farnsworth, I948). Moreover, onceascites is present the diminished renal blood flowresulting from the increased intra-abdominalpressure (Bradley and Bradley, 1947) furthertends to retain fluid in the tissues.The aetiology of ascites in cirrhosis is therefore
complex. Its presence implies that factorsadditional to portal hypertension are operatingand, in general, is indicative of liver cellinadequacy.
Changes in Carbohydrate MetabolismThe liver is the keystone of carbohydrate meta-
bolism. Ingested glucose reaches the liver by theportal vein and is there stored to be released tothe blood stream as required for the maintenanceof the blood glucose concentration. The liveralso converts the monosaccharides fructose andgalactose to glucose. Abnormalities in the glucose,laevulose and galactose tolerance tests might beexpected in patients with cirrhosis. However thereserve power of the liver with respect to carbo-hydrate metabolism is so great that very severeliver cell damage is necessary before these testsbecome positive and carbohydrate tolerance testsare of little practical importance in the study. ofcirrhosis. Similarly the cirrhotic liver might notbe able to maintain a normal blood glucose value.Hypoglycaemic episodes do occur in the cirrhoticpatient but are infrequent.
Changes in Cholesterol MetabolismThe liver excretes cholesterol in the bile and
obstructive lesions of the biliary passages may beassociated with a raised total serum cholesterolconcentration. The hepatic parenchyma alsoesterifies cholesterol with fatty acids. The seraof active cirrhotics show a diminished proportionof esterified to free cholesterol and this ratio isan excellent index of hepatic cellular function.Unfortunately the use of this procedure is usuallyimpracticable because of the tedious nature of thechemical estimation. The serum lipids in liverdisease have recently been discussed by Man andher co-workers (I945).
Haematologwcal ChangesMost textbooks describe a macrocytic anaemia
September 1950 479
by copyright. on M
arch 6, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.26.299.472 on 1 S
eptember 1950. D
ownloaded from

POSTGRADUATE MEDICAL JOURNAL
sT~~~~.:j' F:'v''ca
FI 1 4 The mechansm of urbliui in hepti
t~~~E..MWi.7Pr
cirroi. Stercobilinogenj an urblioe AareHf
chemicallyh;idenia as ae thir oiatio pr-oductsCZs:ercobi;in andurobLili A.
FIG. I14.-The mechanism of urobilinuria in hepaticcirrhosis. Stercobilinogen and urobilinogen arechemically identical as are their oxidation productsstercobilin and urobilin.
associated with cirrhosis. This is related to failureof the liver to synthesize and store the anti-pernicious anaemia principle. However, recentbone marrow studies do not support this conceptas erythropoiesis is usually macronormoblasticand not megaloblastic (Berman et al., 1949). Theanaemia is probably relative and is due to amarked increase in total blood volume with arelatively greater increase in plasma than circu-lating red cell mass; this suggests a more severeanaemia than actually exists (Bateman, Shorr andElgvin, I949). Anaemia in cirrhosis also resultsfrom alimentary tract blood loss related to portalvenous hypertension, iron deficiency from poordietary habits and disturbed haemoglobin meta-bolism from failure of proper protein synthesis inthe liver.The bleeding tendency in cirrhosis is usually
attributed to inadequate prothrombin manufactureby the diseased liver and in general a prolongedprothrombin time in cirrhosis as a good reflectionof severe liver cell damage. Thrombocytopeniamay contribute to the bleeding tendency (Mor-lock and Hall, 1943).
Detoxication ChangesPoisons enter the body through the gastro-
intestinal tract and pass via the portal system to theliver. A cirrhotic liver detoxicates poisons lesswell than normal and this leads among other thingsto poor tolerance for morphia and barbituratedrugs which should be exhibited cautiously. Thisapplies particularly to the short-acting barbiturateanaesthetics which are safe only in small dosesand-should only be used for inducing anaesthesia.Some liver function tests are based on the de-
toxicating power of the liver. The most popularutilizes the conjugation by the liver of benzoicacid with glycine to form hippuric acid. Patientswith active cirrhosis usually show an impairedhippuric acid synthesis test but this test has provedof little practical value as it is so often positive innon-hepatic conditions and bears little relation tounderlying changes in the liver (Sherlock, 1945).The liver is the essential organ for the inactiva--
tion of oestrogens and other steroids and this maybe the explanation of certain endocrine changes incirrhosis. These are well reviewed by Lloyd andWilliams '(1948). In males loss of body hair,.
480 September I1950by copyright.
on March 6, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.26.299.472 on 1 Septem
ber 1950. Dow
nloaded from

SHERLOCK: Cirrhosis of the Liver
gynaecomastia and tesitcular atrophy may occur.In females changes in the menstrual pattern, inbody hair and atrophy of breasts and uterusoccur. Certain cutaneous lesions which occurboth in cirrhotics and in pregnant women areattributed to excess of circulatory oestrogens.These include vascular spiders and palmar ery-thema. Cutaneous arterial spiders are found onlyin the vascular territory of the superior vena cava.Thcy consist of a central point, which may beraised, and in which pulsation is sometimes seen.Branching vessels radiate from the centre. Pressureof the centre with a pin head leads to blanching ofthe entire lesion (Bean, I945). The palmarerythema is seen over the pads of the fingers andover the thenar and hypothenar eminences. Thesurface is red and mottled, with increased tem-perature. The soles of the feet may be similarlyaffected. All these evidences of endocrine in-balance indicate inadequacy of liver cell function.
Aspiration Liver Biopsy in CirrhosisThe patient presenting the full picture of de-
compensated liver disease does not require anaspiration liver biopsy to confirm the diagnosis.However a high proportion of patients with cir-rhosis remain compensated and have equivocalclinical features and normal biochemical tests.Scrutiny of the last 50 case histories of patientswith cirrhosis seen at the Postgraduate MedicalSgchool shows that in 25 there was doubt in theclinical diagnosis. In all these patients liver func-tion tests were non-contributory but in 24 a correctdiagnosis could be made with the aid of the aspira-tion liver biopsy sections. There are certain draw-backs to the use of this technique in the cirrhoticsubject. If ascites is present the liver may be' ballottable ' and difficult to fix; paracentesisshould be performed before the puncture is at-tempted. Failure may also result if the liver isvery tough and difficult to pierce; a few livercells may then be extracted leaving the fibrousframework behind (Sherlock, I946a). Particularcare should also be taken if it is suspected that theliver has greatly contracted as there is chance ofthe biopsy trocar missing the liver and perforatinga hollow viscus such as the gall bladder. How-ever, suspected cirrhosis still remains one of theimportant indications for aspiration liver biopsyand in the great proportion of cases gives anaccurate diagnosis and enables the activity of thelesion to be assessed. Serial aspiration hepaticbiopsies may be used to follow progress and toevaluate therapy instituted.
DIAGNOSIS OF THE TYPE OF CIRRHOSISAs has already been indicated the investigation
of all patients suspected of suffering from cirrhosis
involves an evaluation of the liver cellular functionand the degree of portal venous hypertension.The cirrhosis associated with different aetiologicalfactors may present more diagnostic features.
Classic ' portal ' or Laennec's cirrhosis has beenused as the type example and has been discussedfully above. The importance of alcoholism and ofinfective hepatitis in the preceding history mayagain be emphasized. A suggested outline of theminimum investigation of a suspected case ofportal cirrhosis is shown in Table i.
Wilson's disease or hepato-lenticular degenera-tion is recognized by its familial nature and by theassociated neurological signs of basal ganglia de-generation. Slit lamp studies may show thecharacteristic golden yellow pigment rings in thecornea (Kayser Fleischer rings). Liver cell failureor portal hypertension are rare.
TABLE I
OUTLINE OF THE INVESTIGATION OF A PATIENT WITHHEPATIC (PORTAL) CIRRHOSIS
Occupation, Age and Sex:Clinical History:
Digestive disturbance- anorexia and flatulentdyspepsia.
Abdominal pain.Jaundice. Colour of urine and faeces.Swelling of abdomen and legs.Haemorrhage-nose, skin, alimentary tract.Weight loss.
Past Health:Jaundice.
Social:Heredity, alcohol consumption, Forces service in
hepatitis epidemics.Examination:
Nutrition and evidences of vitamin deficiencies.Jaundice.Vascular spiders, palmar erythema, gynaecomastia.Finger clubbing. Distribution of body hair.Abdomen: Ascites, abdominal wall veins, liver,
spleen.Oedema.
Investigations:Proctoscopy for piles.Barium swallow X-ray for oesophageal varices.Infra-red photograph of anterior abdominal wall for
superficial veins.
Biochemical:Serum bilirubin concentration.Bromsulphalein excretion test (if serum bilirubin value
less than I mg./Ioo ml.).Urinary urobilin (ogen) daily (qualitative test).Serum alkaline phosphatase concentration.Serum albumin. Concentratim.Serum globulin. Concentratim.Serum thymol turbidity test.Serum colloidal gold test.
Aspiration Liver Biopsy if diagnosis is still uncertain.
S-eptember I 950 48iby copyright.
on March 6, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.26.299.472 on 1 Septem
ber 1950. Dow
nloaded from

POSTGRADUATE MEDICAL JOURNAL
Patients with haemochromatosis may have skinpigmentation and endocrine disturbances, par-ticularly gonadal atrophy and diabetes. Exactdiagnosis involves the demonstration of excessiron in the tissues. In the skin it is shown bybiopsy or the ferricyanide intradermal test (Beard-wood and Rouse, I944), in the liver by aspirationbiopsy (Fig. 7) or in the urine by iron staining ofthe centrifuged deposit. The liver lesion inhaemochromatosis is usually compensated andportal hypertension, jaundice and ascites are rare.
Cardiac cirrhosis usually has no specific clinicalor biochemical associations. It does not produceportal venous hypertension, and jaundice inpatients with heart failure does not necessarilyindicate cardiac cirrhosis (Sherlock, 1950). Cardiaccirrhosis can occur with all the aetiological formsof heart failure, but is most frequent in patientswith mitral stenosis and tricupsid valvular in-competence in whom congestive failure is inter-mittent and prolonged.
Bilharzial cirrhosis is recognized by its geo-graphical distribution. It results in portal hyper-tension without much hepatic parenchymal dys-function. Aspiration liver biopsy may demonstratethe ova of the parasite in the portal tracts (Fig. io).
Biliary cirrhosis is usually associated with clinicalmanifestations of the causative lesion. This isfrequently gallstones and there is usually somesystemic infection with mild fever, leucocytosisand raised erythrocyte sedimentation rate. Jaun-dice is fluctuant. Ascites and portal hypertensionare terminal. The biochemical findings are thoseof obstructive jaundice with an increased serumalkaline phosphatase and cholesterol and normalplasma proteins and flocculation tests. Aspirationliver biopsy may be diagnostic, but in a phasewhere jaundice is minimal and intrahepatic bilepigment retention slight, the histological appear-ances can be very difficult to distinguish fromthose of ' portal ' cirrhosis.
Treatment of CirrhosisThe treatment of cirrhosis with liver cell
failure is very disappointing. The best resultsoccur when the failure has a very clear precipitat-ing cause. Thus an acute infection may respondto antibiotics, and the anaemia of a gastrointestinalhaemorrhage be relieved by blood transfusion,with consequent liver cell regeneration and a returnto a compensated state. If the liver cell failure isrelated to an acute alcoholic episode, recovery offunction may follow abstinence and, in general,all patients with cirrhosis should become totalabstainers. Where there is no apparent cause forthe failure or when the cause has been treated,the management of the patient must be on moregeneral lines.
Bed rest is essential and should be continuedwhile improvement 'continues. The work ofPatek and his group (I94I) showing the advantagesof a nutritious diet in the treatment of cirrhosiswas a landmark in this field. Their present regimeincludes a 3,500 calorie diet containing I40 gm.protein, 175 gm. fat and 365 gm. carbohydrate with50 gm. powdered brewer's yeast (Patek et al.,I948). It may be difficult to persuade the patientto take such a liberal diet, moreover this may notbe necessary. Good results are recorded with abasic caloric and protein intake, provided bed restis emphasized and alcohol forbidden (Buck, 1948;Klatskin and Yesner, 1949). The addition ofmethionine and choline is said to be of value(Franklin, Salk, Steigmann and Popper, 1948;Kinsell et al., 1948) as is intravenous ' crude'liver extract (Ralli et al., 1949). These reportsusually have either inadequate control groups orthe controls are taken from a time when thera-peutic measures such as chemotherapy and bloodtransfusion were not so generally available as theyare at present. Moreover, excess amino acidsgiven to a patient with active liver disease mayfurther strain hepatic metabolism and be injurious.It is therefore difficult to assess the value of thesevarious therapeutic agents. A reasonable regimeseems to be a diet containing about 2,500 calorieswith ioo gm. protein. Fat need not be restrictedwithin the caloric total. Fresh brewer's yeast, iftolerated, can be given in one dessertspoon dosesstirred in milk three times a day. This providesadditional first-class protein and also the vitaminB complex. Further dietetic supplements are notnecessary.
Ascites modifies the treatment. Paracentesisabdominis is only palliative and results in greatloss of body protein. Measures must be taken toprevent the fluid reaccumulating and of these themost helpful is the restriction- of sodium chlorideintake (Eisenmenger et al., I949). A cirrhoticpatient who is accumulating ascites can, by bothrenal and extrarenal channels, excrete only I.5 g.sodium chloride daily. Every gram of sodiumchloride taken above this amount means that iooml. water will be retained in the tissues. Sodiumchloride intake should therefore not exceed igram daily. It may be difficult to maintain theprotein content of such a diet without the use oflow salt content bread and low sodium milkpowder. Mercurial diuretics may also be usefulin the prevention of further ascites. Human salt-poor albumin infusions have been used to raise theserum colloidal osmotic pressure but are of onlytransitory value and untoward reactions to themhave been reported (Faloon et al., I949).The treatment of portal venous hypertension is
largely surgical and is chiefly concerned With
482 September I 950by copyright.
on March 6, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.26.299.472 on 1 Septem
ber 1950. Dow
nloaded from

September 1950 SHERLOCK: Cirrhosis of the Liver 483
anastomosis of the portal and systemic venoussystems. In cirrhosis there is already intra-hepatic obstruction to the portal vascular bed andfurther diversion of portal blood into the systemicveins is not attended by any serious effects on theliver cells. Most patients with ' alcoholic' cir-rhosis have disturbed liver cell function andcandidates for porto-caval anastomoses are usuallyfound in the group of younger subjects with post-hepatitis cirrhosis. In these patients normal livercell function may exist with gross portal venoushypertension.The treatment of bleeding oesophageal varices
depends on the severity of the haemorrhage. Asmall ooze may stop spontaneously with or withoutblood transfusion. Severe haemorrhage can
sometimes be checked by the introduction of aballoon into the stomach which, after inflation, isdrawn up against the cardia by means of tractionon the rubber tube to which the balloon is attached(Rowntree et al., I947). Porto-caval anastomosesperformed as a surgical emergency to relieveportal pressure and stop haemorrhage are fraughtwith considerable hazard (Linton, I949). The in-jection of oesophageal varicosities through anoesophagoscope is rarely attempted nowadays.The danger of full doses of morphine to cir-rhotic patients with bleeding oesophageal vari-cosities must again be emphasized.
I am indebted to Mr. E. V. Willmott for themicrophotographs and to Miss Patricia Burrowsfor the diagrams.
BIBLIOGRAPHYALLAN, F. N., BOWIE, D. J., MAcLEOD, J. J. R., and ROBIN-
SON, W. L. (1924), Brit. J. exp. Path., 5, 75.BANTI, G. (I898), Beitr. path. Anat., 24, 2I.BATEMAN, J. C., SHORR, H. M., and ELGVIN, T. (1949),
J. clin. Invest., 28, 539. eBEAN, W. B. (I945), Medicine, 24, 243.BEARDWOOD. J. T., JUN., and ROUSE, G. P., JUN. (I944),
Clinics, 3, 25I.BERMAN, L.. AXELROD, A. R., HORAN, T. N., JACOBSON,
S. D., SHARP, E. A., and VONDER HEIDE, E. C. (x949),Blood, 4, 51 '.
BEST, C. H., HARTROFT, W. S., LUCAS, C. C., and RIDOUT,J. H. (I949), Brit. med. -7., 2, IOOI.
BLAKEMORE, A. H. (I948), Ann. Surg., I28, 825.BOLLMAN, J. L., and MANN, F. C. (193i), Ann. intern. Med.,
S, 699.BRADLEY, S. E., and BRADLEY, G. P. (1947), Y. clin. Invest., 26,
1010.BUCK, R. E. (1948), Y. Lao. clin. Med., 33, 555.CAMERON, G. R., and KARUNARATNE, W. A. E. (1936), 7.
Path. Bact., 42, I.DAVIDSON, C. S.. GIBBONS, T. B., and FALOON, W. W.
(1950), Y. Lab. clin. Med., 35, i8i.DIBLE, J. H., McMICHAEL, J., and SHERLOCK, S. (1947),
Gastroenterology, 9, 736.DOAN, C. A., and WRIGHT, C. S. (1946), Blood, I, IO.DOCK, W. (I947), New Engl. Y. Med., 236, 773.EISENMENGER, W. J., AHRENS, E. J., JUN., BLONDHEIM,
S. H., and KUNKEL, H. G. (1949), Y. Lab. clin. Med., 34,I029.
EPPINGER, H. (I920), 'Die Hepato-Lienalen Erkrankungen,'Berlin.
FALOON, W. W., ECKHARDT, R. D., MURPHY, T. L.,COOPER, A. M., and DAVIDSON, C. S. (d949)Y. clin.Invest., 28, 583.
FARNSWORTH, E. B. (I948), Amer. Y. Med., 4, 338.FOWLER, W. M., and BARER, A. P. (I937), J. Lab. clin. Med.,
23, 47.FRANKLIN, M., SALK, M. R., STEIGMANN, F., and POPPER,
H. (1948), Amer. J. clin. Path., I8, 273.GILLMAN, J., and GILLMAN, T. (1945), Arch. Path.,'40, 239.GRAY, S. J. (1940), Arch. intern. Med., 65, 524.GRAY, S. J., and BARRON, E. S. G. (I943),J. clin. Invest., 22, 191.HELM, J. D., and MACHELLA, T. E. (1942), Amer. Y. digest.
Dis., 9, I4I.HIMSWORTH, H. P., and GLYNN, L. E. (I944), Clin. Sci., 5,
93-HOWARD, R., and WATSON, C. J. (I947), Arch. intern. Med.,
8o, i.HUGHES, T. A. (I933), Indian 7. med. Res., 25, 353.JOLLIFFE, N., and JELLINEK, E. M. (I94I), Quart. Y. Stud.
Alcohol, 2, 544.JONES, C. M., and MINOT, G. R. (1923), Boston med. surg. J.,
189, 53I.KELSALL, A. R., STEWART, A., and WITTS, L. J. (1947),
Lancet, 2, 195.KINSELL, L. W., MICHAELS, G. D., BARTON, H. C., and
WEISS, H. A. (1948), Ann. intern. Med., 29, 88i.
KLATSKIN, G., and YESNER, R. (I949), J. dlin. Invest., 28, 723.LINTON, R. R. (I949), Ann. intern. Med., 31, 794.LLOYD, C. W., and WILLIAMS, R. H. (1948), Amer. J. Med.,
4, 315.McINDOE, A. H. (g928), Arch. Path., 5, 23.MACLAGAN, N. F. (I944), Brit. J. exp. Path., 25, 234.McNEE, J. W. (1932), Brit. med. J7., I, I I Ii.MADDEN, S. C., and WHIPPLE, G. H. (1940), Physiol. Rev.,
20, 194.MAN, E. B., KARTIN, B. L., DURLACHER, S. H., and
PETERS, J. P. (I945), Y. clin. Invest., 24, 623.MANN, F. C., FISHBANK, F. C., GAY, J. G., and GREEN,
G. F. (093i), Arch. Path., 12, 797.MORLOCK, C. G., and HALL, B. E. (I943), Arch. intern. Med.,
72, 69.PATEK, A. T., JUN., MANKIN, H., COLCHER, H., LOWELL
A., and EARLE, D. P., JUN. (1948), J. clin. Invest., 27, 135.PATEK, A. J., JUN., and POST, J. (I941), J. clin. Invest., 20, 48i.PATEK, A. J., JUN., POST, J., RATNOFF, 0. D., MANKIN,
H., and HILLMAN, R. W. (1948), J. Amer. med. Ass., 138,541.
PATTISON, A. C. (1949), Arch. Surg., 58, 590.POLLARD, H. M., and BLOCK, M. (1948), Arch. intern. Med.,
82, 159.
RALLI, E. P.. LESLIE, S. H., STUECK, G. H., JUN., SHORR,H. E.. ROBSON, J. S., CLARKE, D. H., and LAKEN, B.(i94 9) Medicine, 28, 30 I .
RALLI, E. P., ROBSON, J. S., CLARKE, D. H., and HOAG-LAND, C. L. (I945), J. clin. Invest., 24, 3i6.
RATNOFF, 0. D., and PATEK, A. J., JUN. (1942), Medicine, 21,207.
RENNIE, J. B. (1945), Amer. ). med. Sci., 210, i8.ROWNTREE, L. G., ZIMMERMAN, E. F., TODD, M. H., and
AJAC, J. (1947), J. Amer. med. Ass., 135, 630.SABIN, F. R. (1939), J. exp. Med., 70, 67.SCHWARTZ, S. O., and BLUMENTHAL, S. A. (1948), Blood,
3, 617.SHELDON, J. H. (I935), ' Haemochromatosis,' London.SHERLOCK, S. (1945), Lancet, 2, 397.SHERLOCK, S. (1946a), Lan.tet, x, I59.SHERLOCK, S. (I946b), J. Path. Bact., 58, 523.SHERLOCK, S. (1948), Lancet, I, 817.SHERLOCK, S. (i950), Brit. Heart J. (In the press).SHERLOCK, S., and WALSHE, V. (1946), Clin. Sic., 6, 113.SMYTH, H. F., and SMYTH, H. F., JUN. (1936), J. Amer. med.
Ass., 107, I683.TROWELL, H. C. (I949), Trans. R. Soc. trop. Med. Hyg., 42, 417.UZMAN, L., and DENNY-BROWN, D. (1948), Amer. J. med.
Sci., 215, 599.VOLWILER, W., GRINDLAY, J. H., and BOLLMAN, J. L.
(i950), Gastroenterology, 14, 40.WATERLOW, J. C. (I947), Proc. R. So-. Med., 40, 347.WHIPPLE, A. O. (1945), Ann. Surg., 122, 449.WILSON, S. A. K. (I9I2), Brain, 34, 295.WITTS, L. J. (I947), Brit. med. J7., I, 45.YANNET, H., and LIEBERMAN, R. (1946), 7. Amer. med. Ass.,
130, 335.
by copyright. on M
arch 6, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.26.299.472 on 1 S
eptember 1950. D
ownloaded from

572 POSTGRADUATE MEDICAL JOURNAL November i950
certainly possible to improve the results of medicaltreatment in our present state of knowledge. Firstthe diagnosis of ulcer should be established as earlyas possible after symptoms begin and thoroughtreatment with bed rest should be given at theonset; how rarely does one see a patient in ahospital bed with an ulcer history of less than ayear? It is in this respect that our professionalcolleagues so often have the advantage over thehospital patient.
Secondly, the diet prescribed should be palat-able; in spite of dietitians how many hospitalscan be said to provide this? Moreover, some at-tempt should be made to instruct not only thepatients themselves but also their wives in themethods of preparation of such a diet.
Finally, the social circumstances of the patientmust be considered and every help given to en-able him to adjust himself to the difficulties andresponsibilities of his daily life.
The Editor much regrets the omission of the full caption to Fig. ii
in Dr. Sherlock's important article on ' Cirrhosis of the Liver ' in ourSeptember issue. The illustration is. reproduced in full on page 595 inthe present issue.
ANNOTATION
The Milk DripSince Winkelstein (I932) first introduced the
continuous alkalinized milk drip for the treatmentof peptic ulcer, this method of therapy, withcertain modifications, has enjoyed increasingpopularity. Not only has it been widely adopted inthe management of the dyspepsias, but also as ameans of feeding in certain cases of injury ordisease of the mouth or pharynx. In a number ofconditions of nervous origin as well as in ceitainforms of renal disease it has proved a life-savingmeasure.The basis for Winkelstein's introduction of the
milk drip in the treatment of peptic ulcer restedupon his observation that night sampling of theresting gastric contents in cases of gastric andduodenal ulcer showed abnormally high curves forboth free and total acid. In duodenal ulcer,especially, a high continuous curve was obtained.He subsequently showed the absence of free hydro-chloric acid in such cases during milk drip treat-ment and concluded that the method is a logical
and practical means of producing constantachlorhydria.
Subsequent experience has proved the value ofWinkelstein's method of treatment, but in recentyears more concentrated modified milk mixturesfulfilling calorie, vitamin and electrolyte require-ments have been devised. Details of five suchdiets will be found elsewhere in this issue. Themain advantage of these fortified milk mixtures isthat a completely balanced diet can be administeredin a volume of 3 or 4 pints and that patients may befed by continuous intragastric drip for an in-definite period.The original alkalinized milk drip had certain
disadvantages, namely that it was difficult toachieve a gain in the weight without giving hugequantities; that a vitamin deficiency-especiallyof ascorbic acid, so important in the healing ofulcers-and an anaemia were prone to develop;and, finally, that the large intake of alkali was notwithout risk.The apparatus consists of a suitable container
with rubber tubing, an adjustable clip and a bloodtransfusion drip chamber. The clip is adjusted todeliver about 30 drops a minute. A Ryle's tube is

November 1950 GLAZEBROOK and WRIGLEY: The Relief of Pain 595
BIBLIOGRAPHY
BERGEL, F., and MORRISON, A. L. (1948), Quart. Rev. Chem.SOc., ii, No. 4, 349.
B.I.O.S. FINAL REPORT (I945), iI6, No. 24, 52.COMMISSION ON NARCOTIC DRUGS (1948), Extract from
'Report to the Economic and Social Council on the SecondSession of the Commission.'
DAVIES, 0. L., RAVENTOS, J., and WALPOLE, A. L. (1946),Brit. J. Pharmacol., I, 255.
EISLEB, O., and SCHAUMANN, 0. (I939), Dtsch. med. Wschr.,65s,967.
ELLIOTT, H. W. (I947), Fed. Proc., 6, Part ii, 327.FOURNEAU (I938), Chim. et Ind., 39, 1043.GLAZEBROOK, A. J. (I949), Edinb. Med. J., 56, 206.GLAZEBROOK, A. J., and BRANWOOD, A. W. (1945), Lancet,
H, 528.GLAZEBROOK, A. J., and COOKSON, B. (I947), Edinb. med. J.,
44, 193.HARDY, J. D., WOLFF, H. G., and GOODELL, H. (1940),
J. clin. Invest., I9, 649.HEWER, A. J. H., and KEELE, C. A. (i948), Lancet, ii, 683.MAcLAGAN, T. J. (1876), Lancet, L, 383.
PARKER, C. S., and WRIGLEY, F. (I947), Lancet ii, 223.PARKER, C. S., and WRIGLEY, F. (I950), J. ment. Sci., 96, 276.PERLSTEIN, M. A. (I947), Y. Amer. Med. Ass., 135, 633.POLONIO, P. (I947), Lancet, i, S92.PRESCOTT, F., et al. (I949), Lancet, 1, 340.ROBSON, J. M., and KEELE, C. A. (I950), 'Recent Advances in
Pharmacology,' Churchill.SAHLI, H. (I909), Therapeutische Monatshefte Jgg., 23, H I, S I-6.SCOTT, C. C., ROBINS, E. B., and CHEN, K. K. (1946), Science,
I04, 587.SERTURNER (i8o6),J. d. Pharm. f. Aerzte. Apoth. u. Chem., 14, 49.STRAUB (i9xiI), Dtsch. med. Wschr., 37, I462.WILLIAMS, E. M. V., and STREETEN, D. H. P. (ig5o), Lancet
ii, 213.WILSON, W. M., and HUNTER, R. B. (1948), Brit. Med. J7.,
ii, 553.WREN, SIR C., and BOYLE, R. (1656), Quoted from ' History of
Medicine,' Garrison, 4th edition, 1945, p. 273.WRIGLEY, F. (1948), West London Hospital, Dept. of Rheum. Dis.,
Annual Report, p. 28.ZAGER, L. L., ft al. (1949),J. Lab. clin. Med., 34, 1530.
Dr. SHEILA SHERLOCK: Cirrhosis- of the ILm4er
-e-
FIG. I i.-The effects of obstruction to the portal venous system.
Site of Obstruction Clinical EffectsA Splenomegaly.B Splenomegaly, haemorrhoids.C Splenomegaly, haemorrhoids, flatulent dyspepsia, delayed water absorption from
the intestines.D Splenomegaly, haemorrhoids, flatulent dyspepsia, delayed water absorption,
gastric and oesophageal varices.E Splenomegaly, haemorrhoids, flatulent dyspepsia, delayed water absorption,
gastric and oesophageal varices, engorgement of the anterior abdominal wallveins around the umbilicus.