Embed Size (px)
Citation preview

Cirrhosis
18 November 2009
Thomas C Sodeman MDAssociate Professor of Medicine
Chief, Division of Gastroenterology

Cirrhosis
• Definition
• Diagnosis
• Pathogenesis
• Treatment
• Outlook

Cirrhosis
• Definition– Distortion of hepatic architecture by fibrosis
and attempted regeneration that leads to loss of function, portal hypertension, and potential hepatocellular malignancy.

Cirrhosis
http://www.hivandhepatitis.com/2006icr/ddw/images/cirrhosis-liver.jpg

Cirrhosis
http://www.pathology.vcu.edu/education/gi/images/3.3h-b.jpg

Cirrhosis
• Causes– Alcohol– NASH– HBC, HCV, HDV– Iron, copper– Autoimmune– PSC, PBC, SSC– Vascular– 1-AT– Drugs– ?

Cirrhosis
• Diagnosis– Clinical– Laboratory– Radiologic

Cirrhosis
• Diagnosis– Clinical
• Silent• Ascites• Encephalopathy• Sleep-wake reversals• Variceal bleeding• Muscle wasting• Gynecomastia• Spiders
Cirrhosis

Cirrhosis
http://www.hepatitis.cl/images/varices.jpg

Cirrhosis
http://www.medscape.com/content/2000/00/40/55/405535/art-mgi7381.lang.Fig2.jpg

Cirrhosis
http://content.answers.com/main/content/wp/en/thumb/9/91/200px-IGV1.jpg

Cirrhosis
• Diagnosis– Laboratory
• Synthetic defect– Albumen, INR
• Thrombocytopenia• Ammonia• Bilirubin• AST / ALT• FP

Cirrhosis
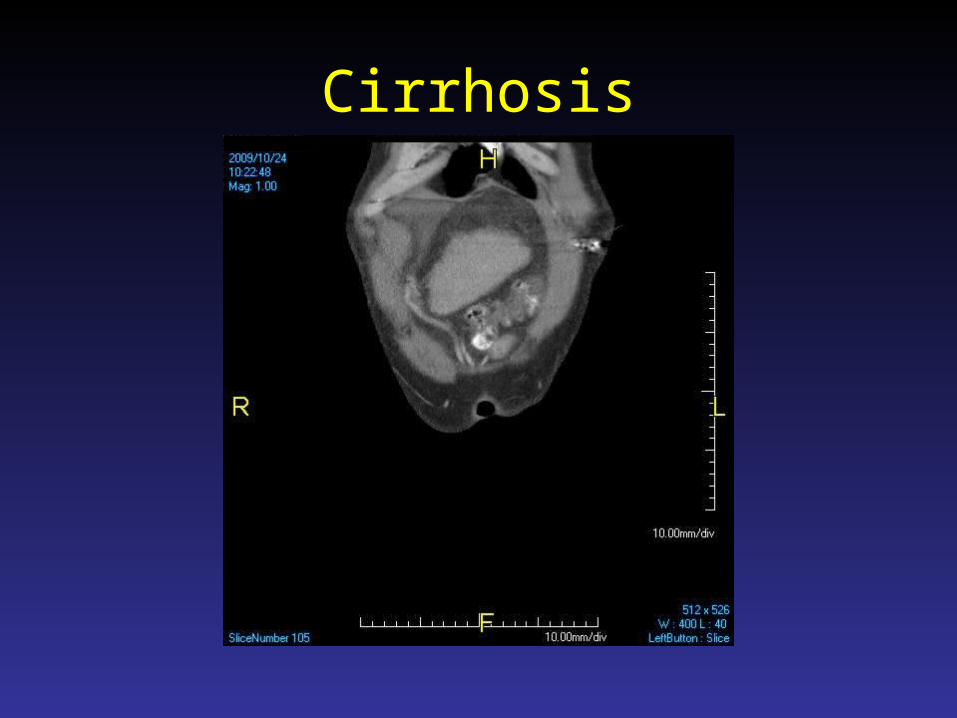
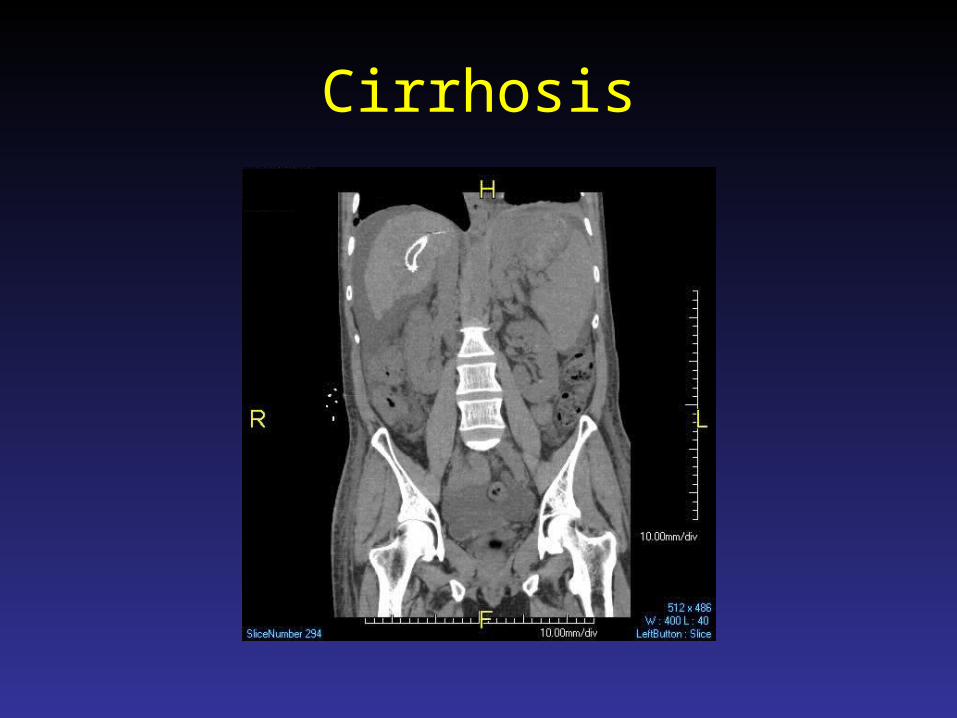
• Diagnosis– Radiologic– Can rule in but not rule out– Sensitivity and specificity of 80%– Splenomegaly, varices, ascites

Cirrhosis

Cirrhosis

Cirrhosis

Cirrhosis

Cirrhosis
Cirrhosis

Cirrhosis

Cirrhosis
• Diagnosis– Biopsy
• 1% risk of complications• Often understages• Misdiagnosed in 10-30%• Optimal biopsy 40 mm• Average 16 mm

Cirrhosis
• Diagnosis– Noninvasive
• Fibroscan• Fibrosure• Actitest• AST/platelet ratio
( AST / ULN)/PLT (109/L)×100.

Cirrhosis
• Pathogenesis

Cirrhosis

Cirrhosis
• Treatment– Treat underlying disease– Treat manifestations– Screen for problems
• Varices• HCC
– Transplantation

Cirrhosis
• Treatment– Treat underlying disease– HBV/HCV – slow progression– HHC – slow progression– AIH – slow progression– EtOH – slow progression

Cirrhosis
• Treatment– Treat manifestations
• Ascites• Encephalopathy• Varices
Cirrhosis

Cirrhosis
• Treatment– Treat manifestations
• Ascites– Tap– SAAG >1.1– Culture– Cytology– Albumen
• Lasix / aldactone• Salt restriction 2g/day• Tap / TIPS

Cirrhosis
• Treatment– Treat manifestations
• Ascites– SAAG– >1.1 Cirrhosis, CHF, Mets, FHF, Budd-Chiari– <1.1 Peritoneal Ca, TB, bile leak, nephrotic syndrome

Cirrhosis
• Treatment– Treat manifestations
• Ascites– Tap– 1100 LVP– INR 8.7– Plt 19– No major complications
Hepatology 2004: 40:484-488
Cirrhosis
• Treatment– Treat manifestations
• Ascites– “Failure”– High salt diet– IV fluids– NSAIDS
Hepatology 2004: 40:484-488

Cirrhosis
• Treatment– Treat manifestations
• Ascites– SBP– >250 PMN– Cefotaxime– Quinolones
Hepatology 2004: 40:484-488

Cirrhosis
• Treatment– Treat manifestations
• Hepatorenal syndrome• GFR>1.5 or CrCl <40• No shock, infection, etc• Urine protein <500 mg/day
Hepatology 2004: 40:484-488

Cirrhosis
• Treatment– Treat manifestations
• Hepatorenal syndrome• Current treatment
– Preventive– Transplant– Midodrine / octreotide
Hepatology 2004: 40:484-488

Cirrhosis
• Treatment– Treat manifestations
• Varices– Predict with thrombocytopenia– Grading I-IV– Bleeding risk with III IV– Screen
» Repeat in 1-2 years if grade I or II» Repeat in 6 months if III IV

Cirrhosis
• Treatment– Treat manifestations
• Varices– Bleeding carries up to 50% mortality– Transfusion to Hb 8– Octreotide– Intubation– Endoscopy– blockers– Antibiotics for SBP

Cirrhosis
• Outlook– Bad– Mortality
• Compensated• Decompensated
– Variceal bleed 20%– Ascites 50% 2 year

Cirrhosis
• Outlook– Hepatocellular carcinoma
• Risk 1-5%/year• Increased with:
– Male– Iron– HBV– 1AT

Cirrhosis
• Outlook– Transplantation
• HCV/alcohol• NASH• HCC• PBC/PSC

Cirrhosis
• Outlook– Transplantation
• MELD score• MELD Score = 10 {0.957 Ln(Scr) + 0.378 Ln(Tbil)
+ 1.12 Ln(INR) + 0.643}

Cirrhosis
• Key points– Diagnosis
• Anything fixable?
– Management of manifestations– Screening for problems– Transplantation












![Scrotal Edema in a Patient with Liver Cirrhosis › gastroenterology › fulltext › downl… · The incidence of acute scrotal swellings is up to 20% in childhood [1]. The major](https://img.pdfslide.us/doc/110x75/5f2501575c9ddf4907735589/scrotal-edema-in-a-patient-with-liver-cirrhosis-a-gastroenterology-a-fulltext.jpg)