Embed Size (px)
Citation preview
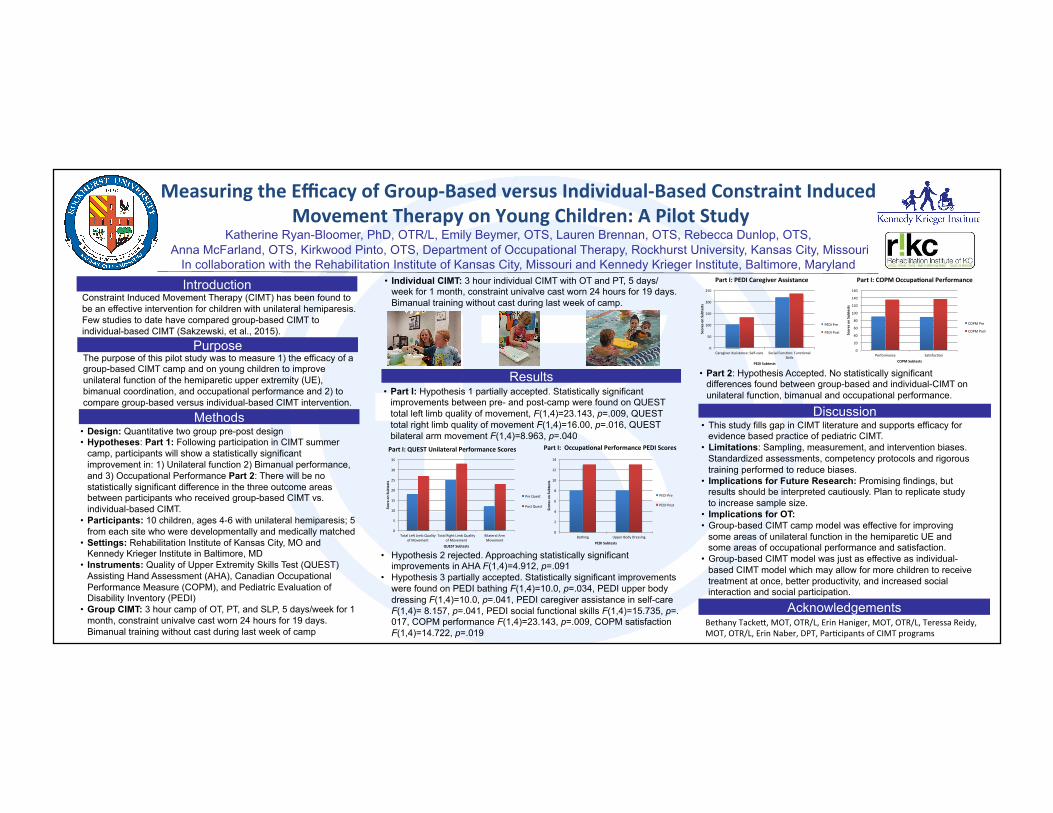
MeasuringtheEfficacyofGroup-BasedversusIndividual-BasedConstraintInducedMovementTherapyonYoungChildren:APilotStudy
Katherine Ryan-Bloomer, PhD, OTR/L, Emily Beymer, OTS, Lauren Brennan, OTS, Rebecca Dunlop, OTS, Anna McFarland, OTS, Kirkwood Pinto, OTS, Department of Occupational Therapy, Rockhurst University, Kansas City, Missouri
In collaboration with the Rehabilitation Institute of Kansas City, Missouri and Kennedy Krieger Institute, Baltimore, Maryland
Constraint Induced Movement Therapy (CIMT) has been found to be an effective intervention for children with unilateral hemiparesis. Few studies to date have compared group-based CIMT to individual-based CIMT (Sakzewski, et al., 2015).
• Part 2: Hypothesis Accepted. No statistically significant differences found between group-based and individual-CIMT on unilateral function, bimanual and occupational performance.
Introduction
Methods Discussion
Acknowledgements
Results
Purpose The purpose of this pilot study was to measure 1) the efficacy of a group-based CIMT camp and on young children to improve unilateral function of the hemiparetic upper extremity (UE), bimanual coordination, and occupational performance and 2) to compare group-based versus individual-based CIMT intervention.
• Individual CIMT: 3 hour individual CIMT with OT and PT, 5 days/week for 1 month, constraint univalve cast worn 24 hours for 19 days. Bimanual training without cast during last week of camp.
• This study fills gap in CIMT literature and supports efficacy for evidence based practice of pediatric CIMT.
• Limitations: Sampling, measurement, and intervention biases. Standardized assessments, competency protocols and rigorous training performed to reduce biases.
• Implications for Future Research: Promising findings, but results should be interpreted cautiously. Plan to replicate study to increase sample size.
• Implications for OT: • Group-based CIMT camp model was effective for improving
some areas of unilateral function in the hemiparetic UE and some areas of occupational performance and satisfaction.
• Group-based CIMT model was just as effective as individual-based CIMT model which may allow for more children to receive treatment at once, better productivity, and increased social interaction and social participation.
• Design: Quantitative two group pre-post design • Hypotheses: Part 1: Following participation in CIMT summer
camp, participants will show a statistically significant improvement in: 1) Unilateral function 2) Bimanual performance, and 3) Occupational Performance Part 2: There will be no statistically significant difference in the three outcome areas between participants who received group-based CIMT vs. individual-based CIMT.
• Participants: 10 children, ages 4-6 with unilateral hemiparesis; 5 from each site who were developmentally and medically matched
• Settings: Rehabilitation Institute of Kansas City, MO and Kennedy Krieger Institute in Baltimore, MD
• Instruments: Quality of Upper Extremity Skills Test (QUEST) Assisting Hand Assessment (AHA), Canadian Occupational Performance Measure (COPM), and Pediatric Evaluation of Disability Inventory (PEDI)
• Group CIMT: 3 hour camp of OT, PT, and SLP, 5 days/week for 1 month, constraint univalve cast worn 24 hours for 19 days. Bimanual training without cast during last week of camp
• Part I: Hypothesis 1 partially accepted. Statistically significant improvements between pre- and post-camp were found on QUEST total left limb quality of movement, F(1,4)=23.143, p=.009, QUEST total right limb quality of movement F(1,4)=16.00, p=.016, QUEST bilateral arm movement F(1,4)=8.963, p=.040
0
5
10
15
20
25
30
35
TotalLe.LimbQualityofMovement
TotalRightLimbQualityofMovement
BilateralArmMovement
Scoreon
Sub
tests
QUESTSubtests
PreQuest
PostQuest
PartI:QUESTUnilateralPerformanceScores
0
2
4
6
8
10
12
14
Bathing UpperBodyDressing
ScoresonSubtests
PEDISubtests
PEDIPre
PEDIPost
PartI:OccupaHonalPerformancePEDIScores
BethanyTackeL,MOT,OTR/L,ErinHaniger,MOT,OTR/L,TeressaReidy,MOT,OTR/L,ErinNaber,DPT,ParRcipantsofCIMTprograms
0
20
40
60
80
100
120
140
160
Performance SaRsfacRon
ScoresonSubtests
COPMSubtests
COPMPre
COPMPost
PartI:PEDICaregiverAssistance PartI:COPMOccupaHonalPerformance
• Hypothesis 2 rejected. Approaching statistically significant improvements in AHA F(1,4)=4.912, p=.091
• Hypothesis 3 partially accepted. Statistically significant improvements were found on PEDI bathing F(1,4)=10.0, p=.034, PEDI upper body dressing F(1,4)=10.0, p=.041, PEDI caregiver assistance in self-care F(1,4)= 8.157, p=.041, PEDI social functional skills F(1,4)=15.735, p=.017, COPM performance F(1,4)=23.143, p=.009, COPM satisfaction F(1,4)=14.722, p=.019
0
50
100
150
200
250
CaregiverAssistance:Self-care SocialFuncRon:FuncRonalSkills
ScoresonSubtests
PEDISubtests
PEDIPre
PEDIPost