Embed Size (px)
Citation preview
F1-08
830563 10/11 F1-0892151
This Patient Charge Schedule lists the benefits of the Dental Plan including covered procedures and patient charges.
Important Highlights
Cigna Dental Care® (*DHMO)Patient Charge Schedule
• ThisPatientChargeScheduleappliesonlywhencovereddentalservicesareperformedbyyourNetworkDentist,unlessotherwiseauthorizedbyCignaDentalasdescribedinyourplandocuments.NotallNetworkDentistsperformalllistedservicesanditissuggestedtocheckwithyourNetworkDentistinadvanceofreceiving services.
• ThisPatientChargeScheduleappliestoSpecialtyCarewhenanappropriatereferralismadetoaNetworkSpecialtyPeriodontist,OrthodontistorOralSurgeon.YoumustverifywiththeNetworkSpecialtyDentistthatyourtreatmentplanhasbeenauthorizedforpaymentbyCignaDental.PriorauthorizationisnotrequiredforspecialtyreferralsforPediatricandEndodonticservices.YoumayselectaNetworkPediatricDentistforyourchildundertheageof7bycallingCustomerServiceat1.800.Cigna24togetalistofNetworkPediatricDentistsinyourarea.CoveragefortreatmentbyaPediatricDentistendsonyourchild’s7thbirthday;however,exceptionsformedicalreasonsmaybeconsideredonanindividualbasis.YourNetworkGeneralDentistwillprovidecareuponyourchild’s7thbirthday.
• Procedures NOT listed on this Patient Charge Schedule are NOT covered and are the patient’s responsibility at the dentist’s usual fees.
• TheadministrationofIVsedation,generalanesthesia,and/orNitrousOxideisnotcoveredexceptasspecificallylistedonthisPatientChargeSchedule.Theapplicationoflocalanestheticiscoveredaspartofyourdentaltreatment.
• CignaDentalconsidersinfectioncontroland/orsterilizationtobeincidentaltoandpartofthechargesforservicesprovidedandnotseparatelychargeable.
• ThisPatientChargeScheduleissubjecttoannualchangeinaccordancewiththeterms of the group agreement.
• ProcedureslistedonthePatientChargeSchedulearesubjecttotheplanlimitationsandexclusionsdescribedinyourplanbook/certificateofcoverageand/orgroupcontract.
Cigna Dental Care®Patient Charge Schedule (F1-08)
-2-
Code Procedure Description Patient Charge
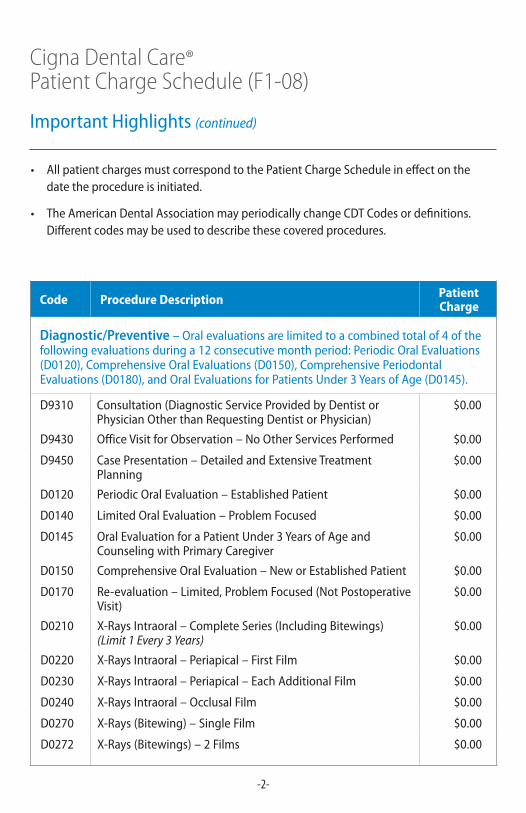
Diagnostic/Preventive –Oralevaluationsarelimitedtoacombinedtotalof4ofthefollowingevaluationsduringa12consecutivemonthperiod:PeriodicOralEvaluations(D0120),ComprehensiveOralEvaluations(D0150),ComprehensivePeriodontalEvaluations(D0180),andOralEvaluationsforPatientsUnder3YearsofAge(D0145).
D9310 Consultation(DiagnosticServiceProvidedbyDentistorPhysicianOtherthanRequestingDentistorPhysician)
$0.00
D9430 OfficeVisitforObservation–NoOtherServicesPerformed $0.00
D9450 CasePresentation–DetailedandExtensiveTreatmentPlanning
$0.00
D0120 PeriodicOralEvaluation–EstablishedPatient $0.00
D0140 LimitedOralEvaluation–ProblemFocused $0.00
D0145 OralEvaluationforaPatientUnder3YearsofAgeandCounselingwithPrimaryCaregiver
$0.00
D0150 ComprehensiveOralEvaluation–NeworEstablishedPatient $0.00
D0170 Re-evaluation–Limited,ProblemFocused(NotPostoperativeVisit)
$0.00
D0210 X-RaysIntraoral–CompleteSeries(IncludingBitewings)(Limit 1 Every 3 Years)
$0.00
D0220 X-RaysIntraoral–Periapical–FirstFilm $0.00
D0230 X-RaysIntraoral–Periapical–EachAdditionalFilm $0.00
D0240 X-RaysIntraoral–OcclusalFilm $0.00
D0270 X-Rays(Bitewing)–SingleFilm $0.00
D0272 X-Rays(Bitewings)–2Films $0.00
• AllpatientchargesmustcorrespondtothePatientChargeScheduleineffectonthedate the procedure is initiated.
• TheAmericanDentalAssociationmayperiodicallychangeCDTCodesordefinitions.Differentcodesmaybeusedtodescribethesecoveredprocedures.
Important Highlights (continued)
Cigna Dental Care®Patient Charge Schedule (F1-08)
-3-
Code Procedure Description Patient Charge
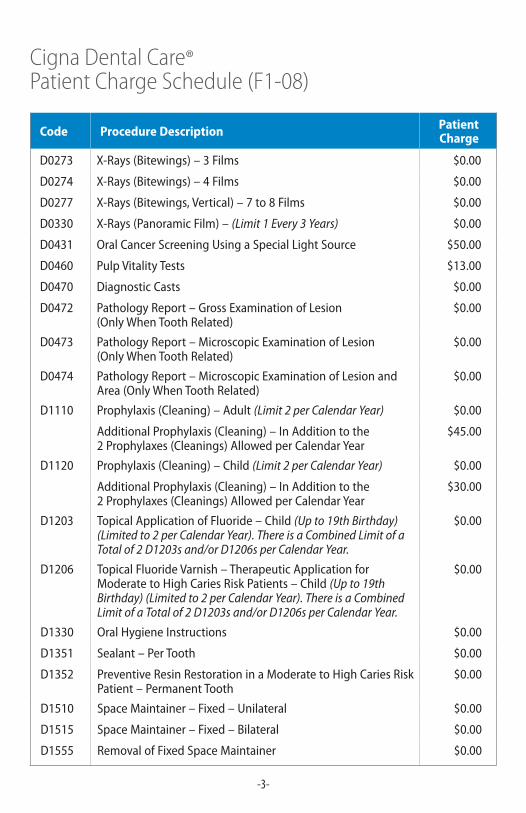
D0273 X-Rays(Bitewings)–3Films $0.00
D0274 X-Rays(Bitewings)–4Films $0.00
D0277 X-Rays(Bitewings,Vertical)–7to8Films $0.00
D0330 X-Rays(PanoramicFilm)–(Limit 1 Every 3 Years) $0.00
D0431 OralCancerScreeningUsingaSpecialLightSource $50.00
D0460 PulpVitalityTests $13.00
D0470 Diagnostic Casts $0.00
D0472 PathologyReport–GrossExaminationofLesion (OnlyWhenToothRelated)
$0.00
D0473 PathologyReport–MicroscopicExaminationofLesion (OnlyWhenToothRelated)
$0.00
D0474 PathologyReport–MicroscopicExaminationofLesionandArea(OnlyWhenToothRelated)
$0.00
D1110 Prophylaxis(Cleaning)–Adult(Limit 2 per Calendar Year) $0.00
AdditionalProphylaxis(Cleaning)–InAdditiontothe 2Prophylaxes(Cleanings)AllowedperCalendarYear
$45.00
D1120 Prophylaxis(Cleaning)–Child(Limit 2 per Calendar Year) $0.00
AdditionalProphylaxis(Cleaning)–InAdditiontothe 2Prophylaxes(Cleanings)AllowedperCalendarYear
$30.00
D1203 TopicalApplicationofFluoride–Child(Up to 19th Birthday) (Limited to 2 per Calendar Year). There is a Combined Limit of a Total of 2 D1203s and/or D1206s per Calendar Year.
$0.00
D1206 TopicalFluorideVarnish–TherapeuticApplicationforModeratetoHighCariesRiskPatients–Child(Up to 19th Birthday) (Limited to 2 per Calendar Year). There is a Combined Limit of a Total of 2 D1203s and/or D1206s per Calendar Year.
$0.00
D1330 OralHygieneInstructions $0.00
D1351 Sealant – Per Tooth $0.00
D1352 PreventiveResinRestorationinaModeratetoHighCariesRiskPatient – Permanent Tooth
$0.00
D1510 SpaceMaintainer–Fixed–Unilateral $0.00
D1515 SpaceMaintainer–Fixed–Bilateral $0.00
D1555 RemovalofFixedSpaceMaintainer $0.00
Cigna Dental Care®Patient Charge Schedule (F1-08)
-4-
Code Procedure Description Patient Charge
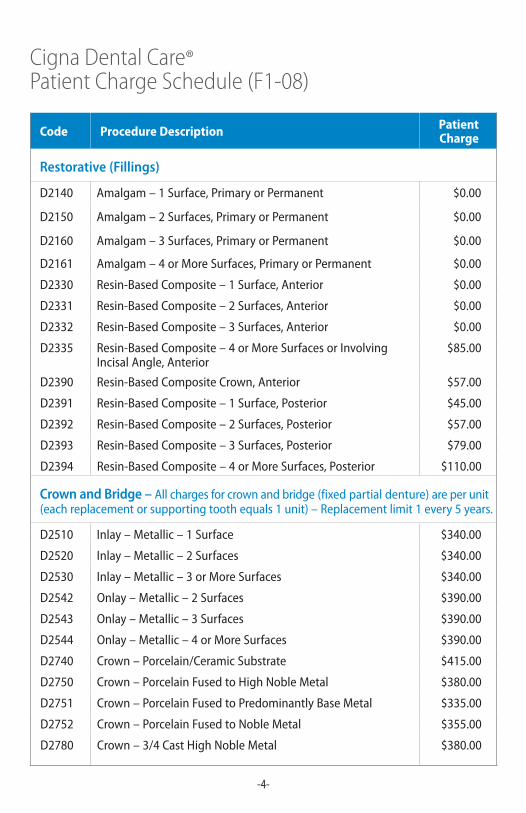
Restorative (Fillings)
D2140 Amalgam–1Surface,PrimaryorPermanent $0.00
D2150 Amalgam–2Surfaces,PrimaryorPermanent $0.00
D2160 Amalgam–3Surfaces,PrimaryorPermanent $0.00
D2161 Amalgam–4orMoreSurfaces,PrimaryorPermanent $0.00
D2330 Resin-BasedComposite–1Surface,Anterior $0.00
D2331 Resin-BasedComposite–2Surfaces,Anterior $0.00
D2332 Resin-BasedComposite–3Surfaces,Anterior $0.00
D2335 Resin-BasedComposite–4orMoreSurfacesorInvolvingIncisalAngle,Anterior
$85.00
D2390 Resin-BasedCompositeCrown,Anterior $57.00
D2391 Resin-BasedComposite–1Surface,Posterior $45.00
D2392 Resin-BasedComposite–2Surfaces,Posterior $57.00
D2393 Resin-BasedComposite–3Surfaces,Posterior $79.00
D2394 Resin-BasedComposite–4orMoreSurfaces,Posterior $110.00
Crown and Bridge – Allchargesforcrownandbridge(fixedpartialdenture)areperunit(eachreplacementorsupportingtoothequals1unit)–Replacementlimit1every5years.
D2510 Inlay–Metallic–1Surface $340.00
D2520 Inlay–Metallic–2Surfaces $340.00
D2530 Inlay–Metallic–3orMoreSurfaces $340.00
D2542 Onlay–Metallic–2Surfaces $390.00
D2543 Onlay–Metallic–3Surfaces $390.00
D2544 Onlay–Metallic–4orMoreSurfaces $390.00
D2740 Crown–Porcelain/CeramicSubstrate $415.00
D2750 Crown–PorcelainFusedtoHighNobleMetal $380.00
D2751 Crown–PorcelainFusedtoPredominantlyBaseMetal $335.00
D2752 Crown–PorcelainFusedtoNobleMetal $355.00
D2780 Crown–3/4CastHighNobleMetal $380.00
Cigna Dental Care®Patient Charge Schedule (F1-08)
-5-
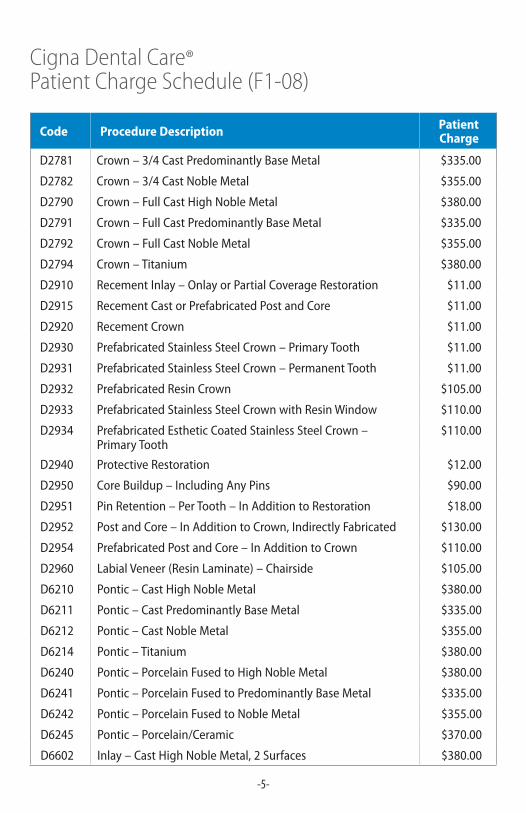
Code Procedure Description Patient Charge
D2781 Crown–3/4CastPredominantlyBaseMetal $335.00
D2782 Crown–3/4CastNobleMetal $355.00
D2790 Crown–FullCastHighNobleMetal $380.00
D2791 Crown–FullCastPredominantlyBaseMetal $335.00
D2792 Crown–FullCastNobleMetal $355.00
D2794 Crown–Titanium $380.00
D2910 RecementInlay–OnlayorPartialCoverageRestoration $11.00
D2915 RecementCastorPrefabricatedPostandCore $11.00
D2920 RecementCrown $11.00
D2930 PrefabricatedStainlessSteelCrown–PrimaryTooth $11.00
D2931 PrefabricatedStainlessSteelCrown–PermanentTooth $11.00
D2932 PrefabricatedResinCrown $105.00
D2933 PrefabricatedStainlessSteelCrownwithResinWindow $110.00
D2934 PrefabricatedEstheticCoatedStainlessSteelCrown– PrimaryTooth
$110.00
D2940 ProtectiveRestoration $12.00
D2950 CoreBuildup–IncludingAnyPins $90.00
D2951 PinRetention–PerTooth–InAdditiontoRestoration $18.00
D2952 PostandCore–InAdditiontoCrown,IndirectlyFabricated $130.00
D2954 PrefabricatedPostandCore–InAdditiontoCrown $110.00
D2960 LabialVeneer(ResinLaminate)–Chairside $105.00
D6210 Pontic–CastHighNobleMetal $380.00
D6211 Pontic–CastPredominantlyBaseMetal $335.00
D6212 Pontic–CastNobleMetal $355.00
D6214 Pontic – Titanium $380.00
D6240 Pontic–PorcelainFusedtoHighNobleMetal $380.00
D6241 Pontic–PorcelainFusedtoPredominantlyBaseMetal $335.00
D6242 Pontic–PorcelainFusedtoNobleMetal $355.00
D6245 Pontic–Porcelain/Ceramic $370.00
D6602 Inlay–CastHighNobleMetal,2Surfaces $380.00
Cigna Dental Care®Patient Charge Schedule (F1-08)
-6-
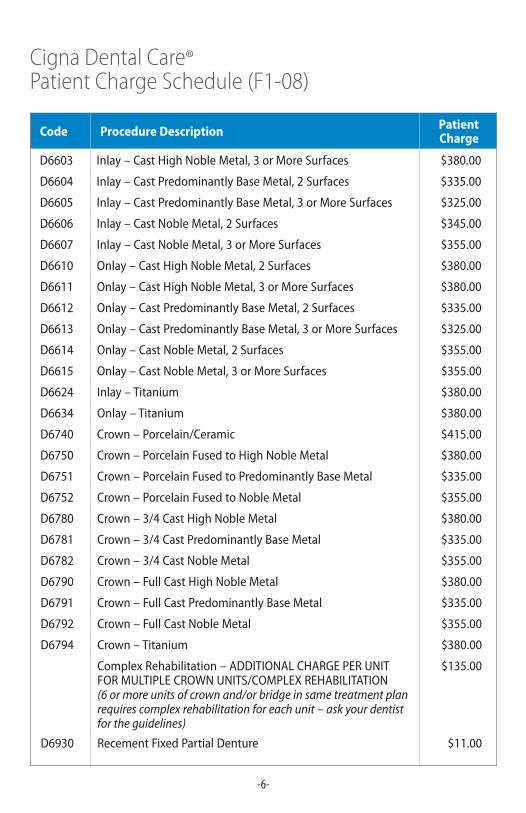
Code Procedure Description Patient Charge
D6603 Inlay–CastHighNobleMetal,3orMoreSurfaces $380.00
D6604 Inlay–CastPredominantlyBaseMetal,2Surfaces $335.00
D6605 Inlay–CastPredominantlyBaseMetal,3orMoreSurfaces $325.00
D6606 Inlay–CastNobleMetal,2Surfaces $345.00
D6607 Inlay–CastNobleMetal,3orMoreSurfaces $355.00
D6610 Onlay–CastHighNobleMetal,2Surfaces $380.00
D6611 Onlay–CastHighNobleMetal,3orMoreSurfaces $380.00
D6612 Onlay–CastPredominantlyBaseMetal,2Surfaces $335.00
D6613 Onlay–CastPredominantlyBaseMetal,3orMoreSurfaces $325.00
D6614 Onlay–CastNobleMetal,2Surfaces $355.00
D6615 Onlay–CastNobleMetal,3orMoreSurfaces $355.00
D6624 Inlay–Titanium $380.00
D6634 Onlay–Titanium $380.00
D6740 Crown–Porcelain/Ceramic $415.00
D6750 Crown–PorcelainFusedtoHighNobleMetal $380.00
D6751 Crown–PorcelainFusedtoPredominantlyBaseMetal $335.00
D6752 Crown–PorcelainFusedtoNobleMetal $355.00
D6780 Crown–3/4CastHighNobleMetal $380.00
D6781 Crown–3/4CastPredominantlyBaseMetal $335.00
D6782 Crown–3/4CastNobleMetal $355.00
D6790 Crown–FullCastHighNobleMetal $380.00
D6791 Crown–FullCastPredominantlyBaseMetal $335.00
D6792 Crown–FullCastNobleMetal $355.00
D6794 Crown–Titanium $380.00
ComplexRehabilitation–ADDITIONALCHARGEPERUNIT FORMULTIPLECROWNUNITS/COMPLEXREHABILITATION(6 or more units of crown and/or bridge in same treatment plan requires complex rehabilitation for each unit – ask your dentist for the guidelines)
$135.00
D6930 RecementFixedPartialDenture $11.00

Cigna Dental Care®Patient Charge Schedule (F1-08)
-7-
Code Procedure Description Patient Charge
Implant Supported Prosthetics – Allchargesforcrownandbridge(fixedpartialdenture)areperunit(eachreplacementonasupportingimplant(s)equals1unit)–Replacementlimit1every5years.Allchargesforanimplantsupporteddenturearelimitedtoreplacementof1every5years.
D6053 Implant/AbutmentSupportedRemovableDentureforCompletelyEdentulousArch
$800.00
D6054 Implant/AbutmentSupportedRemovableDentureforPartiallyEdentulousArch
$875.00
D6058 AbutmentSupportedPorcelain/CeramicCrown $715.00
D6059 AbutmentSupportedPorcelainFusedtoMetalCrown(HighNobleMetal)
$680.00
D6060 AbutmentSupportedPorcelainFusedtoMetalCrown(PredominantlyBaseMetal)
$635.00
D6061 AbutmentSupportedPorcelainFusedtoMetalCrown(NobleMetal)
$655.00
D6062 AbutmentSupportedCastMetalCrown(HighNobleMetal) $680.00
D6063 AbutmentSupportedCastMetalCrown(PredominantlyBaseMetal)
$635.00
D6064 AbutmentSupportedCastMetalCrown(NobleMetal) $655.00
D6065 ImplantSupportedPorcelain/CeramicCrown $715.00
D6066 ImplantSupportedPorcelainFusedtoMetalCrown(Titanium,TitaniumAlloy,HighNobleMetal)
$680.00
D6067 ImplantSupportedMetalCrown(Titanium,TitaniumAlloy,HighNobleMetal)
$680.00
D6068 AbutmentSupportedRetainerforPorcelain/CeramicFixedPartial Denture
$715.00
D6069 AbutmentSupportedRetainerforPorcelainFusedtoMetalFixedPartialDenture(HighNobleMetal)
$680.00
D6070 AbutmentSupportedRetainerforPorcelainFusedtoMetalFixedPartialDenture(PredominantlyBaseMetal)
$635.00
D6071 AbutmentSupportedRetainerforPorcelainFusedtoMetalFixedPartialDenture(NobleMetal)
$655.00
D6072 AbutmentSupportedRetainerforCastMetalFixedPartialDenture(HighNobleMetal)
$680.00
Cigna Dental Care®Patient Charge Schedule (F1-08)
-8-
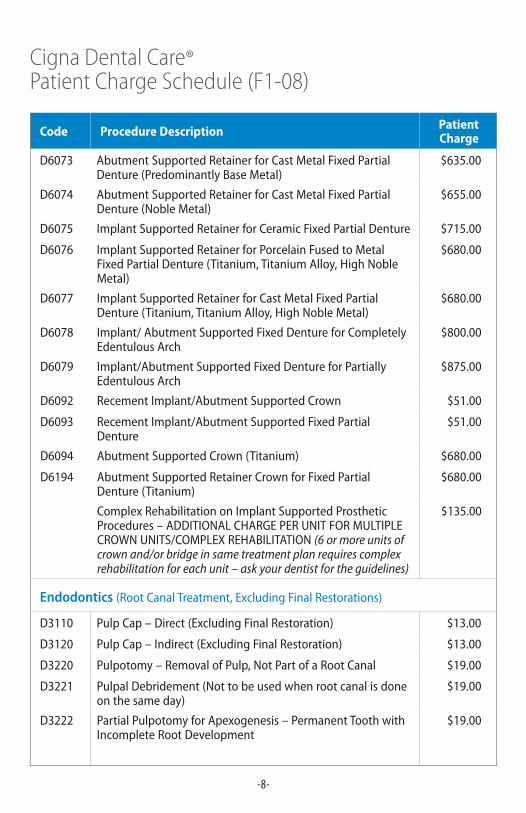
Code Procedure Description Patient Charge
D6073 AbutmentSupportedRetainerforCastMetalFixedPartialDenture(PredominantlyBaseMetal)
$635.00
D6074 AbutmentSupportedRetainerforCastMetalFixedPartialDenture(NobleMetal)
$655.00
D6075 ImplantSupportedRetainerforCeramicFixedPartialDenture $715.00
D6076 ImplantSupportedRetainerforPorcelainFusedtoMetalFixedPartialDenture(Titanium,TitaniumAlloy,HighNobleMetal)
$680.00
D6077 ImplantSupportedRetainerforCastMetalFixedPartialDenture(Titanium,TitaniumAlloy,HighNobleMetal)
$680.00
D6078 Implant/AbutmentSupportedFixedDentureforCompletelyEdentulousArch
$800.00
D6079 Implant/AbutmentSupportedFixedDentureforPartiallyEdentulousArch
$875.00
D6092 RecementImplant/AbutmentSupportedCrown $51.00
D6093 RecementImplant/AbutmentSupportedFixedPartialDenture
$51.00
D6094 AbutmentSupportedCrown(Titanium) $680.00
D6194 AbutmentSupportedRetainerCrownforFixedPartialDenture (Titanium)
$680.00
ComplexRehabilitationonImplantSupportedProstheticProcedures–ADDITIONALCHARGEPERUNITFORMULTIPLECROWNUNITS/COMPLEXREHABILITATION(6 or more units of crown and/or bridge in same treatment plan requires complex rehabilitation for each unit – ask your dentist for the guidelines)
$135.00
Endodontics (RootCanalTreatment,ExcludingFinalRestorations)
D3110 PulpCap–Direct(ExcludingFinalRestoration) $13.00
D3120 PulpCap–Indirect(ExcludingFinalRestoration) $13.00
D3220 Pulpotomy–RemovalofPulp,NotPartofaRootCanal $19.00
D3221 PulpalDebridement(Nottobeusedwhenrootcanalisdoneonthesameday)
$19.00
D3222 PartialPulpotomyforApexogenesis–PermanentToothwithIncompleteRootDevelopment
$19.00
Cigna Dental Care®Patient Charge Schedule (F1-08)
-9-
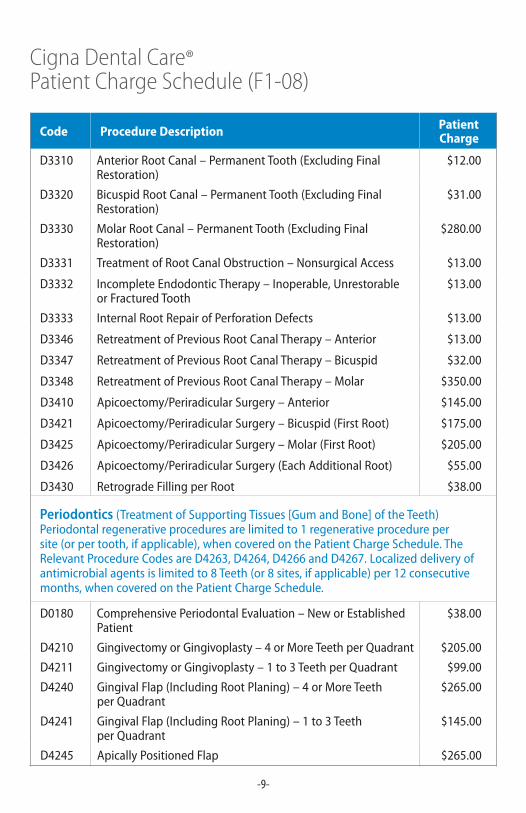
Code Procedure Description Patient Charge
D3310 AnteriorRootCanal–PermanentTooth(ExcludingFinalRestoration)
$12.00
D3320 BicuspidRootCanal–PermanentTooth(ExcludingFinalRestoration)
$31.00
D3330 MolarRootCanal–PermanentTooth(ExcludingFinalRestoration)
$280.00
D3331 TreatmentofRootCanalObstruction–NonsurgicalAccess $13.00
D3332 IncompleteEndodonticTherapy–Inoperable,UnrestorableorFracturedTooth
$13.00
D3333 InternalRootRepairofPerforationDefects $13.00
D3346 RetreatmentofPreviousRootCanalTherapy–Anterior $13.00
D3347 RetreatmentofPreviousRootCanalTherapy–Bicuspid $32.00
D3348 RetreatmentofPreviousRootCanalTherapy–Molar $350.00
D3410 Apicoectomy/PeriradicularSurgery–Anterior $145.00
D3421 Apicoectomy/PeriradicularSurgery–Bicuspid(FirstRoot) $175.00
D3425 Apicoectomy/PeriradicularSurgery–Molar(FirstRoot) $205.00
D3426 Apicoectomy/PeriradicularSurgery(EachAdditionalRoot) $55.00
D3430 RetrogradeFillingperRoot $38.00
Periodontics(TreatmentofSupportingTissues[GumandBone]oftheTeeth) Periodontal regenerative procedures are limited to 1 regenerative procedure per site(orpertooth,ifapplicable),whencoveredonthePatientChargeSchedule.TheRelevantProcedureCodesareD4263,D4264,D4266andD4267.Localizeddeliveryofantimicrobialagentsislimitedto8Teeth(or8sites,ifapplicable)per12consecutivemonths,whencoveredonthePatientChargeSchedule.
D0180 ComprehensivePeriodontalEvaluation–NeworEstablishedPatient
$38.00
D4210 GingivectomyorGingivoplasty–4orMoreTeethperQuadrant $205.00
D4211 GingivectomyorGingivoplasty–1to3TeethperQuadrant $99.00
D4240 GingivalFlap(IncludingRootPlaning)–4orMoreTeeth perQuadrant
$265.00
D4241 GingivalFlap(IncludingRootPlaning)–1to3Teeth perQuadrant
$145.00
D4245 ApicallyPositionedFlap $265.00
Cigna Dental Care®Patient Charge Schedule (F1-08)
-10-
Code Procedure Description Patient Charge
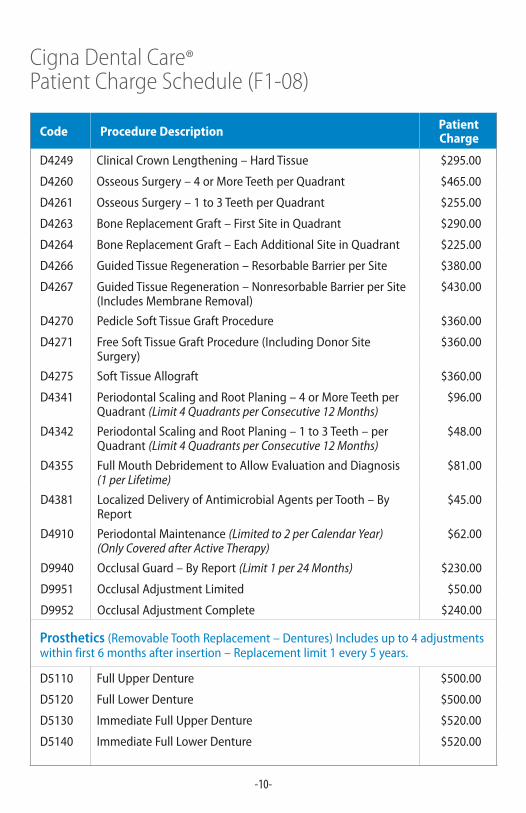
D4249 ClinicalCrownLengthening–HardTissue $295.00
D4260 OsseousSurgery–4orMoreTeethperQuadrant $465.00
D4261 OsseousSurgery–1to3TeethperQuadrant $255.00
D4263 BoneReplacementGraft–FirstSiteinQuadrant $290.00
D4264 BoneReplacementGraft–EachAdditionalSiteinQuadrant $225.00
D4266 GuidedTissueRegeneration–ResorbableBarrierperSite $380.00
D4267 GuidedTissueRegeneration–NonresorbableBarrierperSite(IncludesMembraneRemoval)
$430.00
D4270 PedicleSoftTissueGraftProcedure $360.00
D4271 FreeSoftTissueGraftProcedure(IncludingDonorSiteSurgery)
$360.00
D4275 SoftTissueAllograft $360.00
D4341 PeriodontalScalingandRootPlaning–4orMoreTeethperQuadrant(Limit 4 Quadrants per Consecutive 12 Months)
$96.00
D4342 PeriodontalScalingandRootPlaning–1to3Teeth–perQuadrant(Limit 4 Quadrants per Consecutive 12 Months)
$48.00
D4355 FullMouthDebridementtoAllowEvaluationandDiagnosis (1 per Lifetime)
$81.00
D4381 LocalizedDeliveryofAntimicrobialAgentsperTooth–ByReport
$45.00
D4910 PeriodontalMaintenance(Limited to 2 per Calendar Year) (Only Covered after Active Therapy)
$62.00
D9940 OcclusalGuard–ByReport(Limit 1 per 24 Months) $230.00
D9951 OcclusalAdjustmentLimited $50.00
D9952 OcclusalAdjustmentComplete $240.00
Prosthetics(RemovableToothReplacement–Dentures)Includesupto4adjustmentswithinfirst6monthsafterinsertion–Replacementlimit1every5years.
D5110 FullUpperDenture $500.00
D5120 FullLowerDenture $500.00
D5130 ImmediateFullUpperDenture $520.00
D5140 ImmediateFullLowerDenture $520.00
Cigna Dental Care®Patient Charge Schedule (F1-08)
-11-
Code Procedure Description Patient Charge
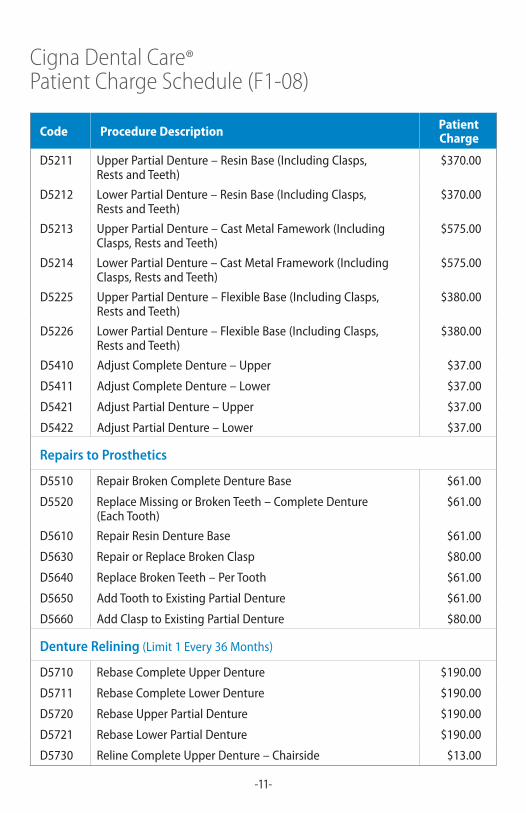
D5211 UpperPartialDenture–ResinBase(IncludingClasps, RestsandTeeth)
$370.00
D5212 LowerPartialDenture–ResinBase(IncludingClasps, RestsandTeeth)
$370.00
D5213 UpperPartialDenture–CastMetalFamework(IncludingClasps,RestsandTeeth)
$575.00
D5214 LowerPartialDenture–CastMetalFramework(IncludingClasps,RestsandTeeth)
$575.00
D5225 UpperPartialDenture–FlexibleBase(IncludingClasps, RestsandTeeth)
$380.00
D5226 LowerPartialDenture–FlexibleBase(IncludingClasps, RestsandTeeth)
$380.00
D5410 AdjustCompleteDenture–Upper $37.00
D5411 AdjustCompleteDenture–Lower $37.00
D5421 AdjustPartialDenture–Upper $37.00
D5422 AdjustPartialDenture–Lower $37.00
Repairs to Prosthetics
D5510 RepairBrokenCompleteDentureBase $61.00
D5520 ReplaceMissingorBrokenTeeth–CompleteDenture (EachTooth)
$61.00
D5610 RepairResinDentureBase $61.00
D5630 RepairorReplaceBrokenClasp $80.00
D5640 ReplaceBrokenTeeth–PerTooth $61.00
D5650 AddToothtoExistingPartialDenture $61.00
D5660 AddClasptoExistingPartialDenture $80.00
Denture Relining(Limit1Every36Months)
D5710 RebaseCompleteUpperDenture $190.00
D5711 RebaseCompleteLowerDenture $190.00
D5720 RebaseUpperPartialDenture $190.00
D5721 RebaseLowerPartialDenture $190.00
D5730 RelineCompleteUpperDenture–Chairside $13.00
Cigna Dental Care®Patient Charge Schedule (F1-08)
-12-
Code Procedure Description Patient Charge
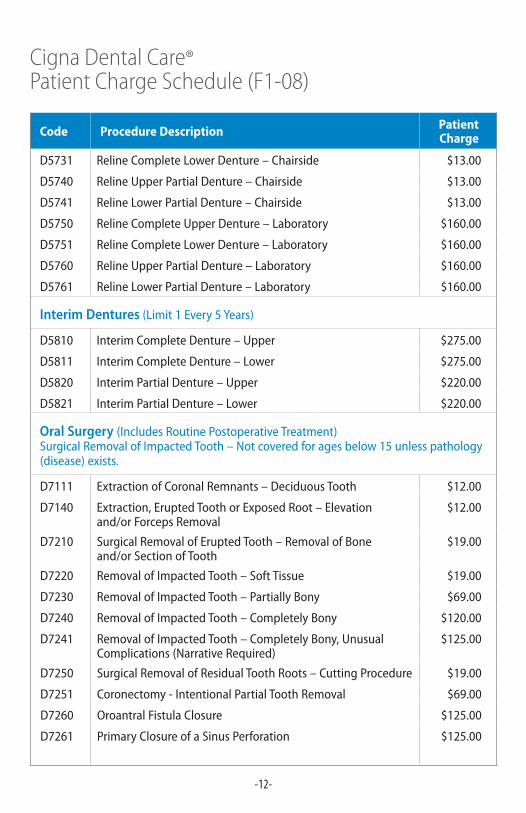
D5731 RelineCompleteLowerDenture–Chairside $13.00
D5740 RelineUpperPartialDenture–Chairside $13.00
D5741 RelineLowerPartialDenture–Chairside $13.00
D5750 RelineCompleteUpperDenture–Laboratory $160.00
D5751 RelineCompleteLowerDenture–Laboratory $160.00
D5760 RelineUpperPartialDenture–Laboratory $160.00
D5761 RelineLowerPartialDenture–Laboratory $160.00
Interim Dentures(Limit1Every5Years)
D5810 InterimCompleteDenture–Upper $275.00
D5811 InterimCompleteDenture–Lower $275.00
D5820 InterimPartialDenture–Upper $220.00
D5821 InterimPartialDenture–Lower $220.00
Oral Surgery (IncludesRoutinePostoperativeTreatment)SurgicalRemovalofImpactedTooth–Notcoveredforagesbelow15unlesspathology(disease) exists.
D7111 ExtractionofCoronalRemnants–DeciduousTooth $12.00
D7140 Extraction,EruptedToothorExposedRoot–Elevation and/orForcepsRemoval
$12.00
D7210 SurgicalRemovalofEruptedTooth–RemovalofBone and/orSectionofTooth
$19.00
D7220 RemovalofImpactedTooth–SoftTissue $19.00
D7230 RemovalofImpactedTooth–PartiallyBony $69.00
D7240 RemovalofImpactedTooth–CompletelyBony $120.00
D7241 RemovalofImpactedTooth–CompletelyBony,UnusualComplications(NarrativeRequired)
$125.00
D7250 SurgicalRemovalofResidualToothRoots–CuttingProcedure $19.00
D7251 Coronectomy-IntentionalPartialToothRemoval $69.00
D7260 OroantralFistulaClosure $125.00
D7261 PrimaryClosureofaSinusPerforation $125.00

Cigna Dental Care®Patient Charge Schedule (F1-08)
-13-
Code Procedure Description Patient Charge
D7270 ToothStabilizationofAccidentallyEvulsedorDisplacedTooth $13.00
D7280 SurgicalAccessofanUneruptedTooth(Excluding Wisdom Teeth)
$13.00
D7283 PlacementofDevicetoFacilitateEruptionofImpactedTooth $7.00
D7285 BiopsyofOralTissue–Hard(Bone,Tooth)(Tooth Related – Not allowed when in conjunction with another surgical procedure)
$86.00
D7286 BiopsyofOralTissue–Soft(AllOthers)(Tooth Related – Not allowed when in conjunction with another surgical procedure)
$74.00
D7287 ExfoliativeCytologicalSampleCollection $74.00
D7288 BrushBiopsy–TransepithelialSampleCollection $74.00
D7310 AlveoloplastyinConjunctionwithExtractions– 4orMoreTeethorToothSpacesperQuadrant
$13.00
D7311 AlveoloplastyinConjunctionwithExtractions– 1to3TeethorToothSpacesperQuadrant
$7.00
D7320 AlveoloplastyNotinConjunctionwithExtractions– 4orMoreTeethorToothSpacesperQuadrant
$13.00
D7321 AlveoloplastyNotinConjunctionwithExtractions– 1to3TeethorToothSpacesperQuadrant
$7.00
D7450 RemovalofBenignOdontogenicCystorTumor– Upto1.25cm
$13.00
D7451 RemovalofBenignOdontogenicCystorTumor– Greaterthan1.25cm
$13.00
D7471 RemovalofLateralExostosis–MaxillaorMandible $13.00
D7472 RemovalofTorusPalatinus $13.00
D7473 RemovalofTorusMandibularis $13.00
D7485 SurgicalReductionofOsseousTuberosity $13.00
D7510 IncisionandDrainageofAbscess–IntraoralSoftTissue $13.00
D7511 IncisionandDrainageofAbscess–IntraoralSoftTissueComplicated
$19.00
D7960 Frenulectomy–AlsoKnownasFrenectomyorFrenotomy–SeparateProcedureNotIncidentaltoAnother
$13.00
D7963 Frenuloplasty $19.00
Cigna Dental Care®Patient Charge Schedule (F1-08)
-14-
Code Procedure Description Patient Charge
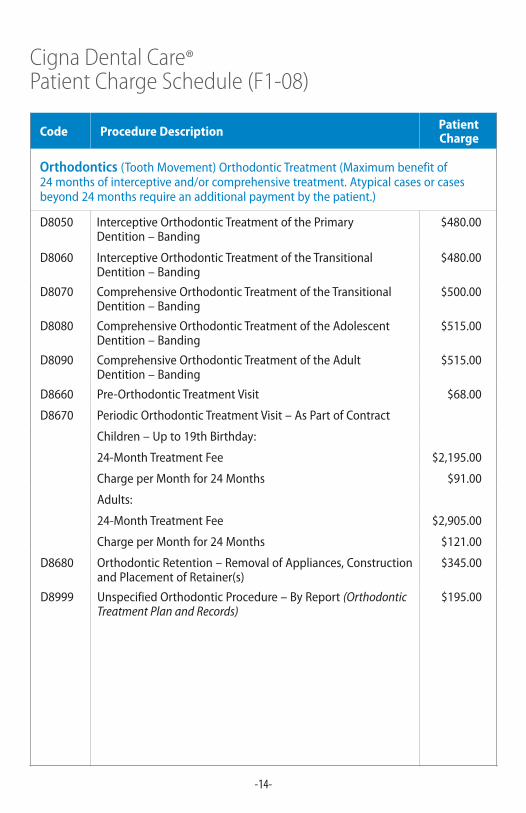
Orthodontics (ToothMovement)OrthodonticTreatment(Maximumbenefitof24monthsofinterceptiveand/orcomprehensivetreatment.Atypicalcasesorcasesbeyond24monthsrequireanadditionalpaymentbythepatient.)
D8050 InterceptiveOrthodonticTreatmentofthePrimary Dentition–Banding
$480.00
D8060 InterceptiveOrthodonticTreatmentoftheTransitionalDentition–Banding
$480.00
D8070 ComprehensiveOrthodonticTreatmentoftheTransitionalDentition–Banding
$500.00
D8080 ComprehensiveOrthodonticTreatmentoftheAdolescentDentition–Banding
$515.00
D8090 ComprehensiveOrthodonticTreatmentoftheAdult Dentition–Banding
$515.00
D8660 Pre-OrthodonticTreatmentVisit $68.00
D8670 PeriodicOrthodonticTreatmentVisit–AsPartofContract
Children–Upto19thBirthday:
24-MonthTreatmentFee $2,195.00
ChargeperMonthfor24Months $91.00
Adults:
24-MonthTreatmentFee $2,905.00
ChargeperMonthfor24Months $121.00
D8680 OrthodonticRetention–RemovalofAppliances,ConstructionandPlacementofRetainer(s)
$345.00
D8999 UnspecifiedOrthodonticProcedure–ByReport(Orthodontic Treatment Plan and Records)
$195.00
Cigna Dental Care®Patient Charge Schedule (F1-08)
-15-
Code Procedure Description Patient Charge
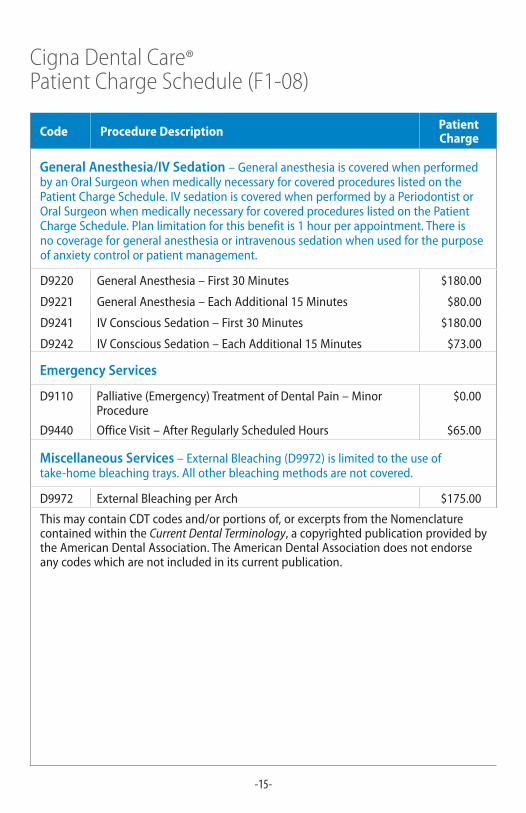
General Anesthesia/IV Sedation –GeneralanesthesiaiscoveredwhenperformedbyanOralSurgeonwhenmedicallynecessaryforcoveredprocedureslistedonthePatientChargeSchedule.IVsedationiscoveredwhenperformedbyaPeriodontistorOralSurgeonwhenmedicallynecessaryforcoveredprocedureslistedonthePatientCharge Schedule. Plan limitation for this benefit is 1 hour per appointment. There is nocoverageforgeneralanesthesiaorintravenoussedationwhenusedforthepurposeofanxietycontrolorpatientmanagement.
D9220 GeneralAnesthesia–First30Minutes $180.00
D9221 GeneralAnesthesia–EachAdditional15Minutes $80.00
D9241 IVConsciousSedation–First30Minutes $180.00
D9242 IVConsciousSedation–EachAdditional15Minutes $73.00
Emergency Services
D9110 Palliative(Emergency)TreatmentofDentalPain–MinorProcedure
$0.00
D9440 OfficeVisit–AfterRegularlyScheduledHours $65.00
Miscellaneous Services–ExternalBleaching(D9972)islimitedtotheuseoftake-homebleachingtrays.Allotherbleachingmethodsarenotcovered.
D9972 ExternalBleachingperArch $175.00
ThismaycontainCDTcodesand/orportionsof,orexcerptsfromtheNomenclaturecontainedwithintheCurrent Dental Terminology,acopyrightedpublicationprovidedbytheAmericanDentalAssociation.TheAmericanDentalAssociationdoesnotendorseanycodeswhicharenotincludedinitscurrentpublication.
* The term “DHMO” is used to refer to product designs that may differ by state of residence of enrollee, including but not limited to, prepaid plans, managed care plans, and plans with open access features.
“Cigna” and “Cigna Dental” are registered service marks and the “Tree of Life” logo is a service mark of Cigna Intellectual Property, Inc., licensed for use by Cigna Corporation and its operating subsidiaries. All products and services are provided exclusively by such operating subsidiaries, including Connecticut General Life Insurance Company (“CGLIC”), Cigna Health and Life Insurance Company (“CHLIC”), Cigna HealthCare of Connecticut, Inc., and Cigna Dental Health, Inc. (“CDHI”) and its subsidiaries, and not by Cigna Corporation. The Cigna Dental Care plan is provided by Cigna Dental Health Plan of Arizona, Inc.; Cigna Dental Health of California, Inc.; Cigna Dental Health of Colorado, Inc.; Cigna Dental Health of Delaware, Inc.; Cigna Dental Health of Florida, Inc., a Prepaid Limited Health Services Organization licensed under Chapter 636, Florida Statutes; Cigna Dental Health of Kansas, Inc. (Kansas and Nebraska); Cigna Dental Health of Kentucky, Inc.; Cigna Dental Health of Maryland, Inc.; Cigna Dental Health of Missouri, Inc.; Cigna Dental Health of New Jersey, Inc.; Cigna Dental Health of North Carolina, Inc.; Cigna Dental Health of Ohio, Inc.; Cigna Dental Health of Pennsylvania, Inc.; Cigna Dental Health of Texas, Inc.; and Cigna Dental Health of Virginia, Inc. In other states, the Cigna Dental Care plan is underwritten by CGLIC, CHLIC, or Cigna HealthCare of Connecticut, Inc., and administered by CDHI.
830563 10/11 © 2011 Cigna
Afteryourenrollmentiseffective:CallthedentalofficeidentifiedinyourWelcomeKit.Ifyouwishtochangedentaloffices,atransfercanbearrangedatnochargebycallingCignaDentalatthetoll-freenumberlistedonyourIDcardorplanmaterials.
Multiplewaystolocatea*DHMONetworkGeneralDentist:
• Onlineproviderdirectoryatwww.Cigna.com
• OnlineproviderdirectoryonmyCigna.com
• CallthenumberlocatedonyourIDcardto:
– UsetheDentalOfficeLocatorviaSpeechRecognition
– SpeaktoaCustomerServiceRepresentative
EMERGENCY:Ifyouhaveadentalemergencyasdefinedinyourgroup’splandocuments,contactyourNetworkGeneralDentistassoonaspossible.IfyouareoutofyourserviceareaorunabletocontactyourNetworkOffice,emergencycarecanberenderedbyanylicenseddentist.Definitivetreatment(e.g.,rootcanal)isnotconsideredemergencycareandshouldbeperformedorreferredbyyourNetworkGeneralDentist.Consultyourgroup’splandocumentsforacompletedefinitionofdentalemergency,youremergencybenefitandalistingofExclusionsandLimitations.





























