Embed Size (px)
Citation preview

1
MANAGEMENT OF CHRONIC PAIN IN OLDER ADULTS
LEANNE R. CIANFRINI, PHD
Clinical Psychologist
Program Director
The Doleys Clinic
OVERVIEW OF TOPICS
We’ll discuss:
• How important effective pain management is for older
adults
• Unique physiological and psychosocial factors that
influence chronic pain perception and response to
treatment modalities in older adults
• Practical methods for assessing and managing pain
• Nonpharmacological
• Pharmacological
• Guidelines
THE PREVALENCE AND NATURE OF PAIN IN OLDER ADULTS (1 OF 2)
• High prevalence of pain in general American
population
• As much as 50% of the older adult population
report chronic pain.
• Studies show up to 80% of nursing home residents
have clinically significant pain.
• Older adults more likely to be affected by joint
pain and other forms of musculoskeletal pain.

2
Diseases associated with chronic pain in later life, by system or specialty
• Dermatology — pressure or ischemic ulcers, burns, scleroderma
• Gastrointestinal — constipation, diverticulitis, IBD
• Cardiovascular — advanced heart disease, peripheral vascular disease
• Pulmonary — advanced COPD, pleurisy
• Rheumatology — OA, RA, gout, polymyalgia rheumatica, spinal stenosis
and other low back syndromes, myofascial syndromes, osteoporotic
related fractures
• Endocrine — diabetic neuropathy
• Nephrology — chronic cystitis, end stage renal disease
• Immune — herpes zoster, post-herpetic neuralgia, HIV/AIDs
neuropathy
• Neurology — headache, peripheral neuropathies, compressive
neuropathies, radiculopathies, Parkinson’s disease, post-stroke pain
• Oncology — cancer
• Miscellaneous — depression, tendonitis, bursitis
THE PREVALENCE AND NATURE OF PAIN IN OLDER ADULTS (2 OF 2)
•We have an aging population.
•Pain is still under-recognized and under-treated
in older adults.
WHY IS THIS IMPORTANT?
• Undertreated pain is associated with:• Sleep disturbance
• Functional decline
• Risks associated with polypharmacy
• Malnutrition
• Prolonged hospital stay
• Challenging behaviors
• Cognitive decline
• Increased healthcare utilization
• Lawsuits
• Impact on family
• Impact on society
“I must die. But must I die groaning?” -- Epictetus, 135 AD

3
CHRONIC PAIN BASICS (1 OF 3)
DEFINITIONS:
• IASP: “An unpleasant sensory and emotional experience…”
• McCaffery: “Whatever the experiencing person says it is, existing whenever the experiencing person says it does.” --SUBJECTIVE
• A disease in its own right.Chapman, Tuckett, Song. J Pain, 2008; 9 (2): 122-45
ACUTE VS. CHRONIC
• Acute pain: Makes sense to focus on location, sensory aspects for rehabilitation purposes
• Chronic pain: Danger of too much focus on peripheral “generators”
CHRONIC PAIN BASICS (2 OF 3)
Sensory-Discriminative
Cognitive-Evaluative
Affective-Motivational
Sensory-Discriminative
Cognitive-Evaluative
Affective-Motivational
WHO ‘GETS’ THE DISEASE OF CHRONIC PAIN?
From Birth• Genetics, female sex, ethnicity,
congenital disorders, prematurity• Parental anxiety, irregular feeding and
sleeping• Parents’ pain exposure and reactions• Temperament and personality
Childhood• Physical/sexual abuse and other
traumatic events• Low SES• Emotional, conduct, and peer
problems• Hyperactivity
Adolescence• Changes of puberty, gender roles• Educational level, learning
(behavioral reactions to pain)• Injuries• Obesity• Low fitness levels
Adulthood• Vivid recall of childhood trauma• Lack of social support; accum. stress• Surgery• Overuse of joints and muscles• Occupational exposures, job
dissatisfaction, low work status• Development of chronic disease• Aging
Relieving Pain in America. Institute of Medicine. National Academic Press. Washington, D.C. 2011

4
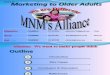
Woolf C. Ann Intern Med. 2004;140:441-451.
Central Pain Amplification
Abnormal pain processing by CNS
(ie, Fibromyalgia)
Nociceptive Pain
Noxious stimuli
(ie, Burn)
Inflammatory Pain
Inflammation
(ie, Rheumatoid arthritis)
Neuropathic Pain
Neuronal damage
(ie, Herpes zoster)
CHRONIC PAIN BASICS (3 OF 3)
CONSIDER A “MECHANISTIC-BASED” APPROACH TO PAIN ASSESSMENT AND TREATMENT
Neuroanatomy of Nociception
AGE-RELATED CHANGES IN PAIN PROCESSING AND PRESENTATION
• Pain modulatory imbalance• Bio:
• Systemic inflammation (increased “inflamm-aging”)• Changes in structure of peripheral nerves that transmit pain
signals• Studies of pain threshold
• Brain structure and function changes (reduction in gray matter in certain regions of the brain)
• Psychosocial: • Cope with pain differently? E.g., under-reporting• Present with more behavioral expressions• Late life depression in OA (risk factor)• Social (isolation is more likely)

5
ASSESSMENT
“TO HEAR ABOUT PAIN IS TO HAVE DOUBT;
TO EXPERIENCE PAIN IS TO HAVE CERTAINTY”.
-ELAINE SCARRY, THE BODY IN PAIN: THE MAKING AND UNMAKING OF THE WORLD

6
IS PAIN PRESENT?
• Ask about the presence of pain in regular and frequent
intervals:• Upon admission
• During periodic scheduled assessments
• Whenever a change occurs in patient’s condition
• Considerations:
• Simply ask the patient!
• Myth – pain is a normal part of aging
• Assume pain if patient has conditions or procedures that are
typically painful
• Involve family, staff
• In nonverbal patients, may need to use observation – at rest and
during activity (e.g., repositioning)
BEHAVIORAL OBSERVATIONSINDICATIVE OF CHRONIC PAIN
• Facial expressions: grimacing, fearful expression, grinding of teeth
• Vocalizations: crying, moaning, groaning, sighing, breathing heavily
• Body movements: bracing, guarding, rubbing
• Change in movement: rigid posture, limping, resistance to motion during care, fidgeting/restlessness
• Change in interpersonal interactions: combative, resistant, withdrawm
• Change in mental status: confusion, irritability, agitation, crying
• Change in usual activity: refusing food/appetite change, increased wandering, change in sleep habits Loss of function
OBSERVATIONAL PAIN TOOLS
• 2006 BMC Geriatrics systematic review
• Compared psychometric qualities and criteria
for 12 observational tools
• Concluded that PACSLAC & DOLOPLUS2 most
appropriate scales
• The APS recommends ABBEY or PAINAD.

7

8
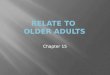
PAIN CHARACTERISTICS
• Pain Intensity: VAS, NRS, Facial Pain Scales, Pain Thermometer
• Location: pain map
• Explore different descriptive words, such as “aching,” “burning,” “stabbing”
• Distinguishes muscular, nerve, inflammatory pain and can guide treatment
• E.g., McGill Pain Questionnaire
• Basic sensory questions:• Please tell me all of the places you experience pain or discomfort.
What does it feel like? What words come to mind?
• Is your pain or discomfort with you all of the time or does it come and go? How long has it been present? What makes it better, what makes it worse?
Faces Pain Scale
Horizontal Visual Analogue Scale
Iowa Pain Thermometer McGill Pain Questionnaire

9
DETERMINE CAUSES OF PAIN
• Physical exam
• Musculoskeletal, neurologic
• Performance-based measures
• Rule out: Is it something as basic as toileting needs?
• Laboratory, radiologic, and other diagnostic tests as appropriate
• Can be overused, does not “prove” presence or absence of pain
• Consultation if needed
BIOPSYCHOSOCIAL PERSPECTIVE –EFFECT ON FUNCTIONING
• Functional impact:• Has pain affected your ability to do every day activities?
To do things you enjoy?
• How about relating with others? If so, how?
• Emotional impact:• Has pain affected your mood, sense of wellbeing, energy
level?
• Are you worried about your pain or what may be causing
it?
• Consider PHQ9 or PHQ2
• Other psychosocial factors:• History of mood disorders or mental illness?• History of addiction?• Family involvement?
• Is there anyone at home or in the community that you can turn to for help and support when your pain is really bad?
• Does patient act differently around family members?
• Do family members seem insistent on a particular treatment?
BIOPSYCHOSOCIAL PERSPECTIVE –PSYCHOSOCIAL HISTORY

10
• Attitudes and beliefs• Do you have any thoughts or opinions about experiencing pain at this point in
your life that you believe would be important for me to know?
• Do you have any thoughts or opinions about specific pain treatments that you
believe would be important for me to know?
• Coping styles• What things do you do to help you cope with your pain? This could be listening
to your favorite music, praying, sitting still, or isolating yourself from others
• Treatment expectations and goals• What do you think is likely to happen with the treatment I have recommended?
• What are the most important things you hope will happen as a result of the
treatment?
BIOPSYCHOSOCIAL PERSPECTIVE –OTHER QUESTIONS
TREATMENT
“If we know that pain and suffering can be alleviated, and we do nothing about it, then
we ourselves become the tormentors.”
- Primo Levi
MULTIMODAL APPROACHTO PAIN MANAGEMENT
Treatment Approaches
Pharmacotherapy Physical Therapy
Complementaryand Alternative
Medicine
Psychological Support
Exercise
Interventional
Approaches

11
NON-PHARMACOLOGICAL: INTERVENTIONAL TECHNIQUES
Degenerative conditions precipitating spinal stenosis, herniated discs, foraminal stenosis, compression fractures, or degenerative joint disease
• Spinal surgical techniques
• Kyphoplasty
• Epidural steroids
• Facet joint injections
• Cortisone injections
• Trigger point injections
• Radiofrequency ablation
NON-PHARMACOLOGICAL: PHYSICAL AND CBT TECHNIQUES
Physical Modalities:• Heat & cold, TENS, massage
• Moderate exercise – active vs. passive
• Occupational therapy
Cognitive-Behavioral Approaches:• Self-management (e.g., moderation/modification, pacing)
• Biofeedback, relaxation
• Setting realistic expectations
Other general health strategies:• Anti-inflammatory diet, bowel health, and weight management
• Sleep hygiene
• Increasing social engagement
WHO 3-STEP ANALGESIC LADDER

12
GENERAL PHARMACOLOGIC CONSIDERATIONS
• Tailor to type of pain
• Does benefit outweigh the risk?• All meds have risk (not just opioids)
• Medications must be monitored closely to avoid over- or under-medicating
• What are goals?• Disease management• Quality of life• Improve or maintain functional status• Comfort near end of life
SPECIAL PHARMACOLOGIC CONSIDERATIONS FOR OLDER ADULTS
(1 OF 3)
• Older adults are at increased risk for adverse drug reactions
• Pharmacokinetics vs. pharmacodynamics
• Drug-Drug interactions -- Polypharmacy
• Drug-Disease interactions
• Drug-Food and Drug-Herb interactions
• Smaller body size/different body composition
SPECIAL PHARMACOLOGIC CONSIDERATIONS FOR OLDER ADULTS
(2 OF 3)
• Increased risk for adverse drug reactions (continued)
• Increased sensitivity to anticholingeric effects
• Decreased blood-pressure maintaining ability
• Decreased temperature compensation
• Inadequate testing of drugs in older adults before FDA approval
• Problems with vision, hearing or memory

13
• Decreased ability of the
kidneys to clear drugs
out of the body
• Decreased ability of the
liver to process drugs
• Decreased liver mass and
variable blood flow
• Metabolism through the
Cytochrome P450 system
decreases with age
SPECIAL PHARMACOLOGIC CONSIDERATIONS FOR OLDER ADULTS
(3 OF 3)
RENAL CHANGES IN OLDER ADULTS
HEPATIC CHANGES IN OLDER ADULTS
MEDICATIONS TO AVOID
• Meperidine (Demerol)
• Ketorolac (Toradol)
• Mixed agonist-antagonists like Talwin (pentazocine-naloxone)
• Tramadol
• Caution with muscle relaxants, amitriptyline, NSAIDs
• Products containing diphenhydramine (e.g., Tylenol PM)
Check the Beers criteria

14
NON-OPIOID MEDICATION OPTIONS
• Acetaminophen
• NSAIDs • Use judiciously due to increased risk of GI bleeding and
renal toxic side effects; not for chronic, prolonged use
• Cox-2 inhibitors • Celebrex contraindicated in pts with sulfa sensitivity
• Topicals• OTC vs. RX/compounded
For neuropathic pain: • Anticonvulsants• Antidepressants (SSRIs > SNRIs)
OPIOID BASICS
• Bind to one or more of the mu, kappa, delta mu receptors (in periphery, DRG, PAG, midbrain, gut)
• Long-acting/extended-release vs. short-acting/immediate-release
• Need for continuous vs. intermittent dosing• “Breakthrough” vs. incident pain
• MEDD
• Risk stratification
• Route of administration (e.g., IV, transdermal, PO)
• Dependence vs. Addiction
• START LOW AND GO SLOW
OPIOID OPTIONS
• Codeine
• Tramadol
• Tapentadol
• Hydrocodone
• Morphine
• Buprenorphine
• Oxycodone
• Hydromorphone
• Fentanyl
• Oxymorphone
• Methadone

15
SIDE EFFECTS OF OPIOIDS
• Constipation• Never resolves
• Prevent with scheduled softeners plus stimulants
• Avoid bulking agents (eg, Metamucil) (dehydration + fiber = worse)
• Nausea and vomiting
• Sedation and delirium
• Respiratory depression (unintentional overdose)
• Concomitant use of opioids/benzos
• Prone to respiratory issues (COPD, sleep apnea, URIs)
• Others: endocrine dysfunction with long-term use; dry mouth
(avoid anticholinergics); urinary retention; fall risk; immune
system suppression
AT FACILITIES: INVEST IN THE SYSTEM AND THE INDIVIDUAL (1 OF 2)
• Arrange presentations on Nature of Pain, Evaluation
Tools, and Treatment Modalities
• Arrange easily accessible printed materials for review
and use
• Assign a “point person” or expert in Pain Management
who can consult/assist as needed on challenging cases
• Provide and seek prompt feedback for specific cases,
and overall progress
AT FACILITIES: INVEST IN THE SYSTEM AND THE INDIVIDUAL (2 OF 2)
• Evaluation of systemic approach ongoing
• What tools are cumbersome/not working
• Is inter-team communication working?
• Is documentation adequate?
• Evaluation of Personal Approach as well…
• Knowledge Deficits
• Past Personal Experience vs. “Expert” Opinion
• Personal Biases re: Pain
• Fear of Negative Consequences

16
OTHER RESOURCES
• 2009 AGS Panel on Pharmacological
Management of Persistent Pain in Older Persons
• Summary in handouts
• JAGS AUGUST 2009–VOL. 57, NO. 8
• PAINAD
• Example in handouts
THANK YOU
QUESTIONS?