Embed Size (px)
Citation preview

Original paper
Changes in lower limb muscle functionand muscle mass following exercise-basedinterventions in patients with chronicobstructive pulmonary disease: A reviewof the English-language literature
Jana De Brandt1, Martijn A Spruit1,2,3, Dominique Hansen1,Frits ME Franssen2, Wim Derave4, Maurice JH Sillen2
and Chris Burtin1
AbstractChronic obstructive pulmonary disease (COPD) patients often experience lower limb muscle dysfunction andwasting. Exercise-based training has potential to improve muscle function and mass, but literature on this topic isextensive and heterogeneous including numerous interventions and outcome measures. This review uses a detailedsystematic approach to investigate the effect of this wide range of exercise-based interventions on muscle functionand mass. PUBMED and PEDro databases were searched. In all, 70 studies (n ¼ 2504 COPD patients) thatimplemented an exercise-based intervention and reported muscle strength, endurance, or mass in clinicallystable COPD patients were critically appraised. Aerobic and/or resistance training, high-intensity interval training,electrical or magnetic muscle stimulation, whole-body vibration, and water-based training were investigated. Musclestrength increased in 78%, muscle endurance in 92%, and muscle mass in 88% of the cases where that specificoutcome was measured. Despite large heterogeneity in exercise-based interventions and outcome measuresused, most exercise-based trials showed improvements in muscle strength, endurance, and mass in COPDpatients. Which intervention(s) is (are) best for which subgroup of patients remains currently unknown.Furthermore, this literature review identifies gaps in the current knowledge and generates recommendationsfor future research to enhance our knowledge on exercise-based interventions in COPD patients.
KeywordsCOPD, pulmonary rehabilitation, exercise training, lower limb, muscle function, muscle mass
Date received: 26 September 2016; accepted: 29 March 2017
IntroductionChronic obstructive pulmonary disease (COPD) is alung disease characterized by persistent airflow lim-itation.1 Nevertheless, many patients with COPD alsocommonly experience systemic features, such asimpaired lower limb muscle function and musclewasting.2 Cross-sectional research has reported thatquadriceps strength is reduced by 20–30% in patientswith COPD.2 This observed decrease in strength isproportional to the decrease in muscle mass in the
1 REVAL - Rehabilitation Research Center, BIOMED - BiomedicalResearch Institute, Faculty of Medicine and Life Sciences, HasseltUniversity, Diepenbeek, Belgium2 Department of Research and Education, CIRO, Center ofExpertise for Chronic Organ Failure, Horn, the Netherlands3 Department of Respiratory Medicine, Maastricht UniversityMedical Centre, NUTRIM School of Nutrition and TranslationalResearch in Metabolism, Maastricht, the Netherlands4 Department of Movement and Sports Sciences, GhentUniversity, Ghent, Belgium
Corresponding author:Jana De Brandt, REVAL, Hasselt University, Agoralaan Gebouw A,3590 Diepenbeek, Belgium.Email: [email protected]
Chronic Respiratory Disease1–39ª The Author(s) 2017Reprints and permission:sagepub.co.uk/journalsPermissions.navDOI: 10.1177/1479972317709642journals.sagepub.com/home/crd
Creative Commons CC BY-NC: This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 License (http://www.creativecommons.org/licenses/by-nc/4.0/) which permits non-commercial use, reproduction
and distribution of the work without further permission provided the original work is attributed as specified on the SAGE and Open Access pages(https://us.sagepub.com/en-us/nam/open-access-at-sage).

majority of patients with COPD, suggesting the onsetof disuse-related muscle atrophy instead ofmyopathy-related muscle atrophy.3 In line with thisreasoning, patients with COPD generally are less phy-sically active compared to healthy peers,4,5 which isdirectly related to lower limb muscle dysfunction.6 Adecreased quadriceps endurance has also been estab-lished in COPD but is more variable across studiesbecause of differences in test procedures.2 This lowerlimb muscle dysfunction clearly contributes to theobserved exercise intolerance and exercise-inducedsymptoms of dyspnea and fatigue in patients withCOPD.7 Moreover, lower limb muscle dysfunctionhas been associated with a worse health status, morehospitalizations, and worse survival.2
In turn, exercise-based interventions have the poten-tial to reverse or at least stabilize lower limb muscularchanges in patients with COPD.2,8 Exercise-based pul-monary rehabilitation programs are a cornerstone ofthe comprehensive care of patients with COPD.9
Indeed, international guidelines state that exercisetraining is the best available nonpharmacological ther-apy to improve lower limb muscle function and musclemass in these patients.9,10 The comprehensive Ameri-can Thoracic Society/European Respiratory Society(ATS/ERS) statement provides only a short overviewof the effects of exercise-based therapies on musclefunction and muscle mass in patients with COPD,2
whereas actually the literature about this topic is exten-sive and heterogeneous including numerous interven-tions and outcome measures. A critically appraisedand detailed overview of the impact of this widerange of exercise-based therapies on lower limbmuscle function and muscle mass in patients withCOPD is presented in this narrative review.
MethodsInclusion and exclusion criteriaThe included studies investigated the effects of anyexercise training intervention on lower limb musclestrength, endurance, and mass in clinically stablepatients with COPD. Studies investigating the muscleresponse to a single exercise test or a single exercisesession were excluded. Studies that specifically inves-tigated the effect of an additional intervention on topof exercise training were also excluded. The selectedstudies needed to include original data, but there wereno restrictions regarding study design or musclestrength, endurance, and mass assessment used. Onlystudies published in English were included.
Search methodsElectronic databases PUBMED and PEDro weresearched for articles published from inception untilMarch 7, 2016. In PUBMED, the following searchstrategy was used: COPD AND (exercise OR exercisetraining OR rehabilitation OR pulmonary rehabilitationOR physical activity OR aerobic training OR endur-ance training OR resistance training OR strength train-ing OR cycling OR walking OR neuromuscularelectrical stimulation OR NMES OR magnetic stimu-lation). The search strategy was adapted to “COPD”alone when searching in PEDro to identify all relevantarticles. Corresponding authors were contacted to pro-vide full texts when not accessible via electronic data-bases. Reference screening of available reviews in thesame field of research was also performed to expandthe search for eligible articles.
Selection of studiesTwo reviewers (JDB and CB) performed the studyscreening based on the listed inclusion and exclusioncriteria. In the first phase, both reviewers conducted apart of the title screening in a conservative manner,excluding only titles that undoubtedly did not fulfillthe criteria. Next, both reviewers screened all remain-ing abstracts independently. Results were compared,discrepancies between reviewers were discussed, anda consensus-based decision was taken. Finally, full-textscreening was performed in a similar way.
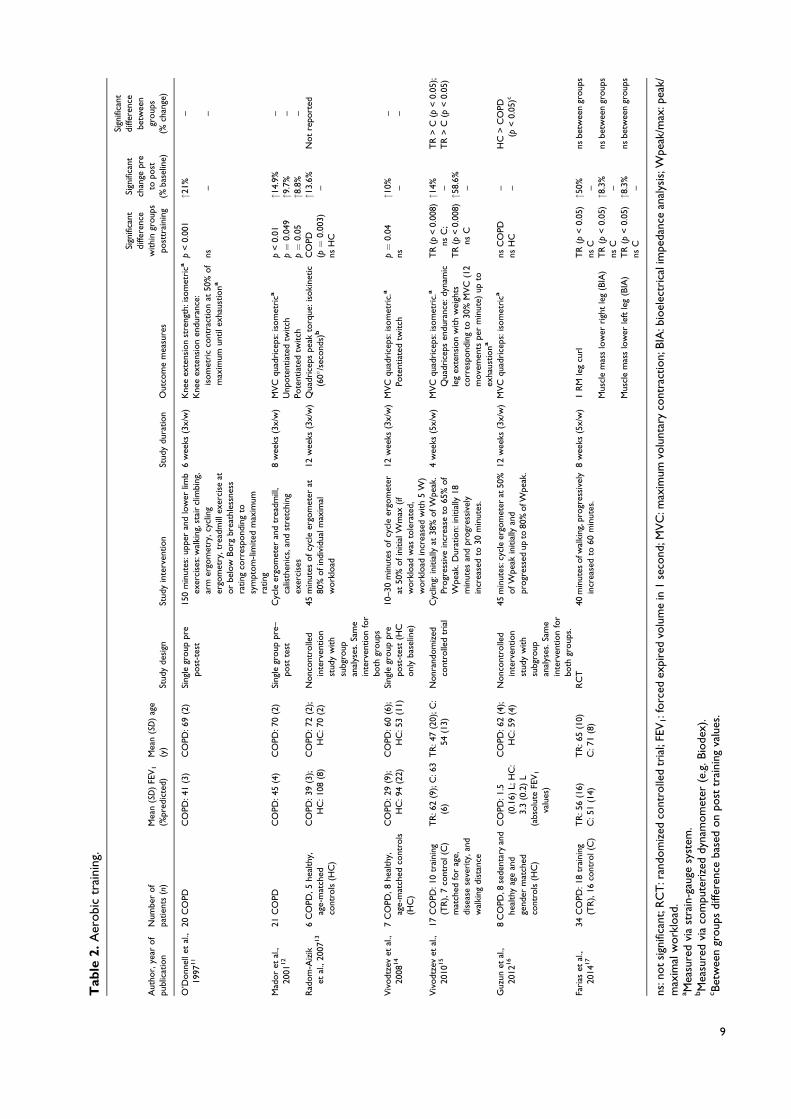
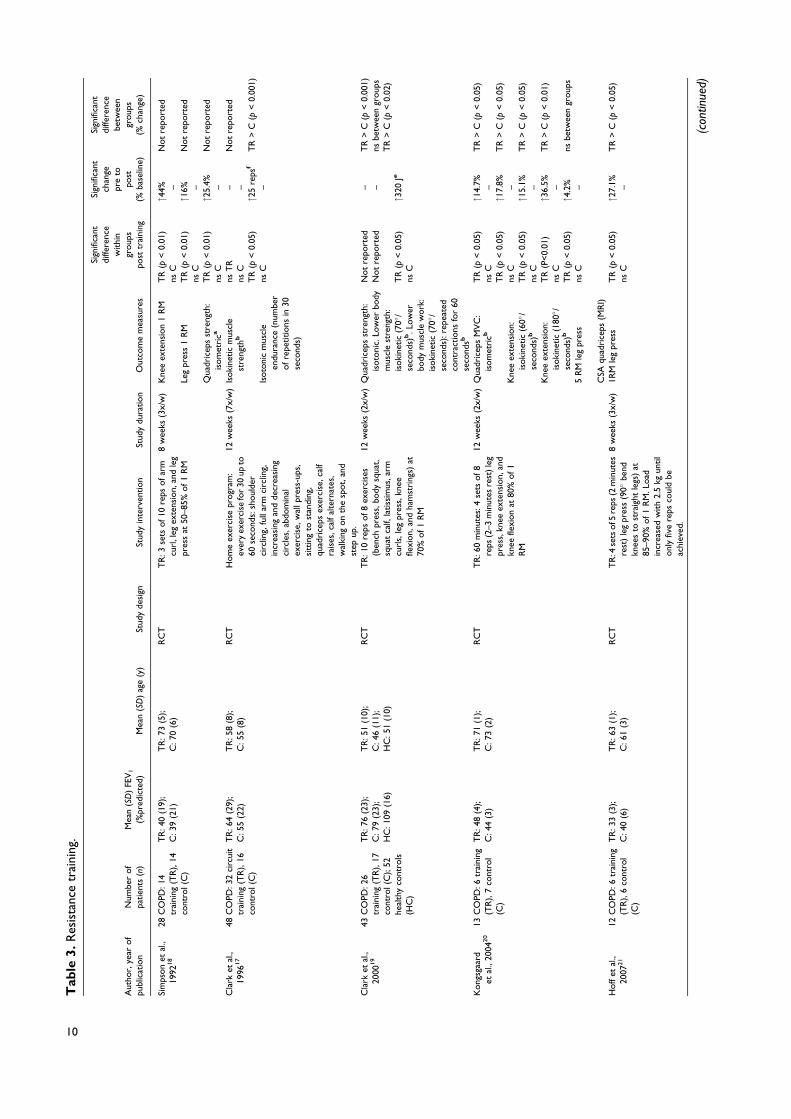
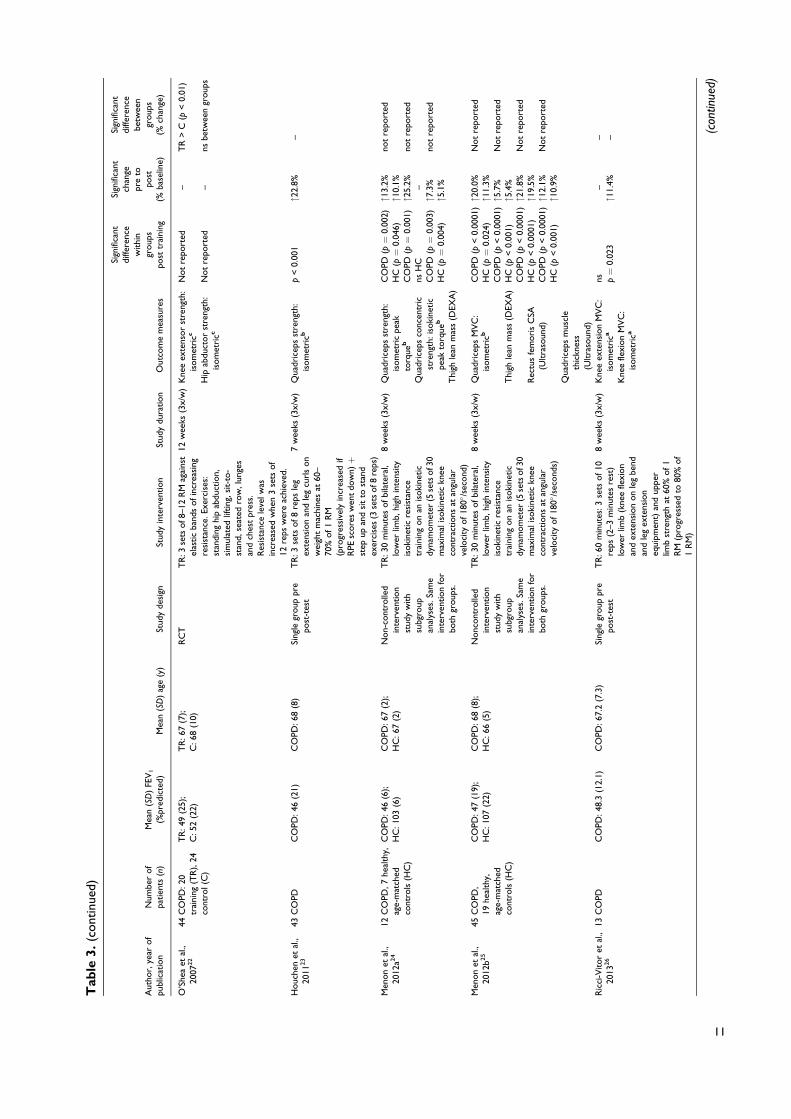
Data extractionInformation on sample size, study design (for studiescomparing COPD with other disease states, only thedata from patients with COPD is shown and thedesign described as single group pre post-test), base-line forced expiratory volume at first second (FEV1),age, exercise training parameters (frequency, inten-sity, modality, session and program duration), assess-ment modality, and relevant outcome measures ofmuscle strength, muscle endurance, and muscle masswere extracted from the articles. Mean relativechange (percentages of baseline) between pre- andpostmeasurements were extracted. If mean relativechange (expressed as percentage of baseline) was notavailable, pre- and postvalues were used to manuallycalculate mean relative change as percentage of base-line: ([post – pre]/pre x 100). All extracted data arepresented in Tables 2–7 (according to training mod-ality) and Figures 1–7. For Figure 4, a weighted mean
2 Chronic Respiratory Disease
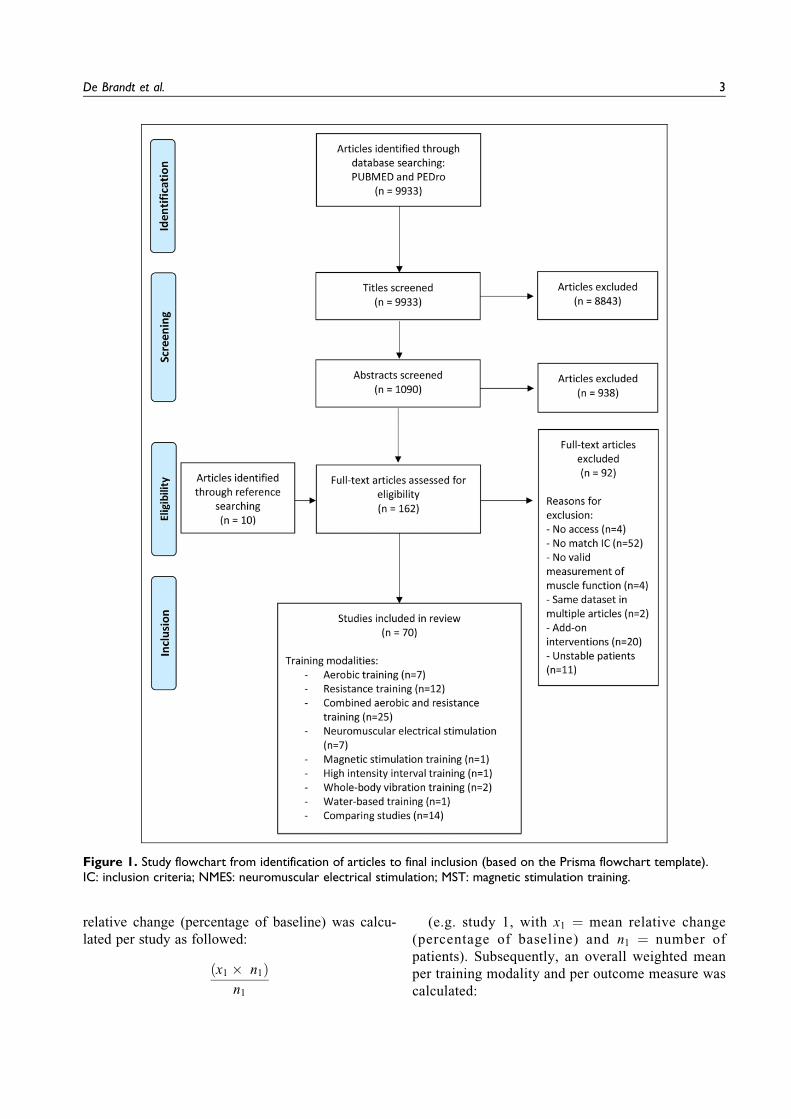
relative change (percentage of baseline) was calcu-lated per study as followed:
ðx1 # n1Þn1
(e.g. study 1, with x1 ¼ mean relative change(percentage of baseline) and n1 ¼ number ofpatients). Subsequently, an overall weighted meanper training modality and per outcome measure wascalculated:
Figure 1. Study flowchart from identification of articles to final inclusion (based on the Prisma flowchart template).IC: inclusion criteria; NMES: neuromuscular electrical stimulation; MST: magnetic stimulation training.
De Brandt et al. 3
ðx1 # n1 þ x2 # n2 þ x3 # n3 þ . . . þ xn # nnÞðn1 þ n2 þ n3 þ . . . þ nnÞ
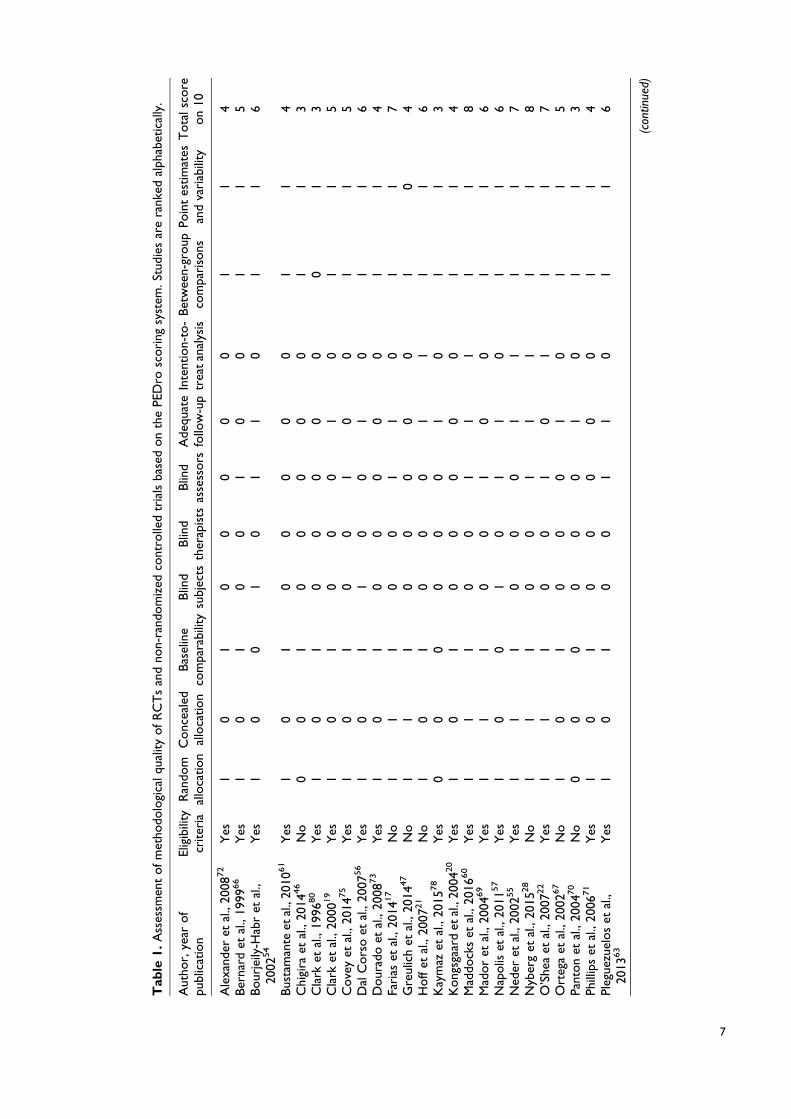
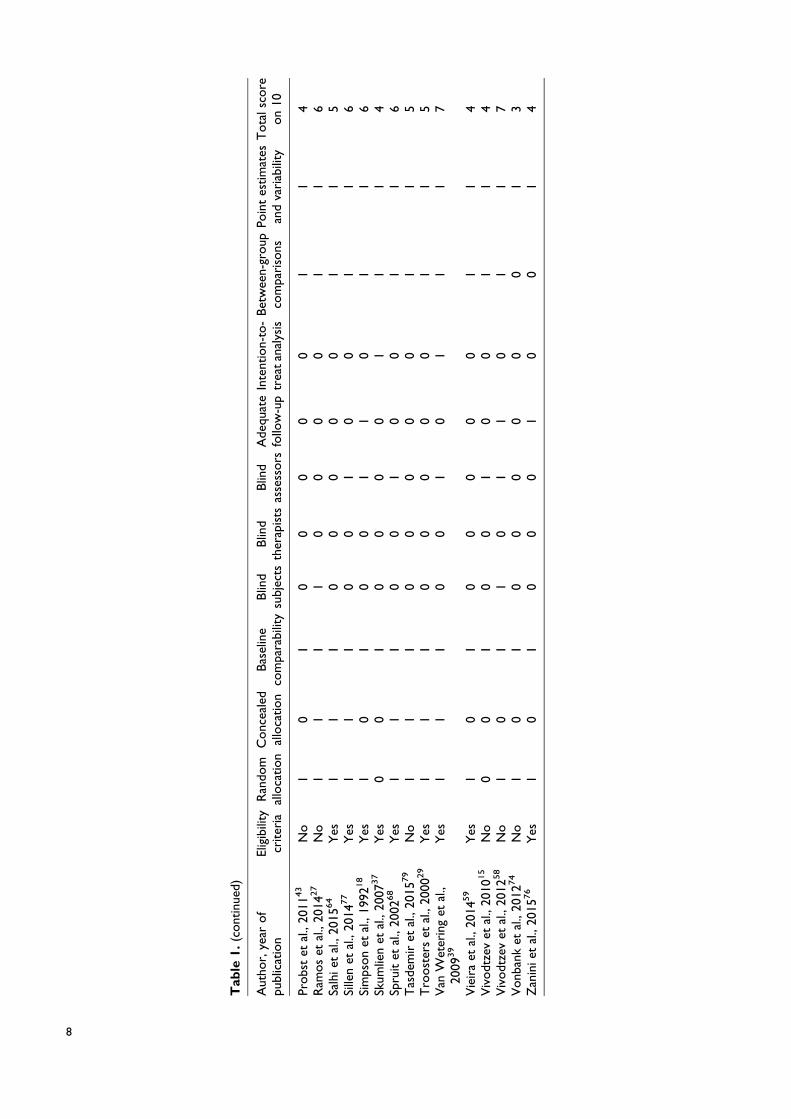
Quality assessmentMethodological quality of randomized controlled trials(RCT) or nonrandomized controlled trials wereassessed (Table 1). The PEDro scale, based on theDelphi list and “expert consensus,” was used as a tool
to assess the quality of the studies.81,82 PEDro scoreswere obtained from the PEDro database. If a study wasnot found in the PEDro database, PEDro scores werecalculated for that study by two reviewers (JDB andCB). Eleven quality criteria received a “yes” or “no”answer and were summed (criteria 1 is not used in thecalculation) to a maximum score of 10 points.82 Stud-ies were considered of “good” to “excellent” qualitywhen scoring &6 points on the PEDro scale. Studiesscoring '5 points were defined as “low” to “fair”
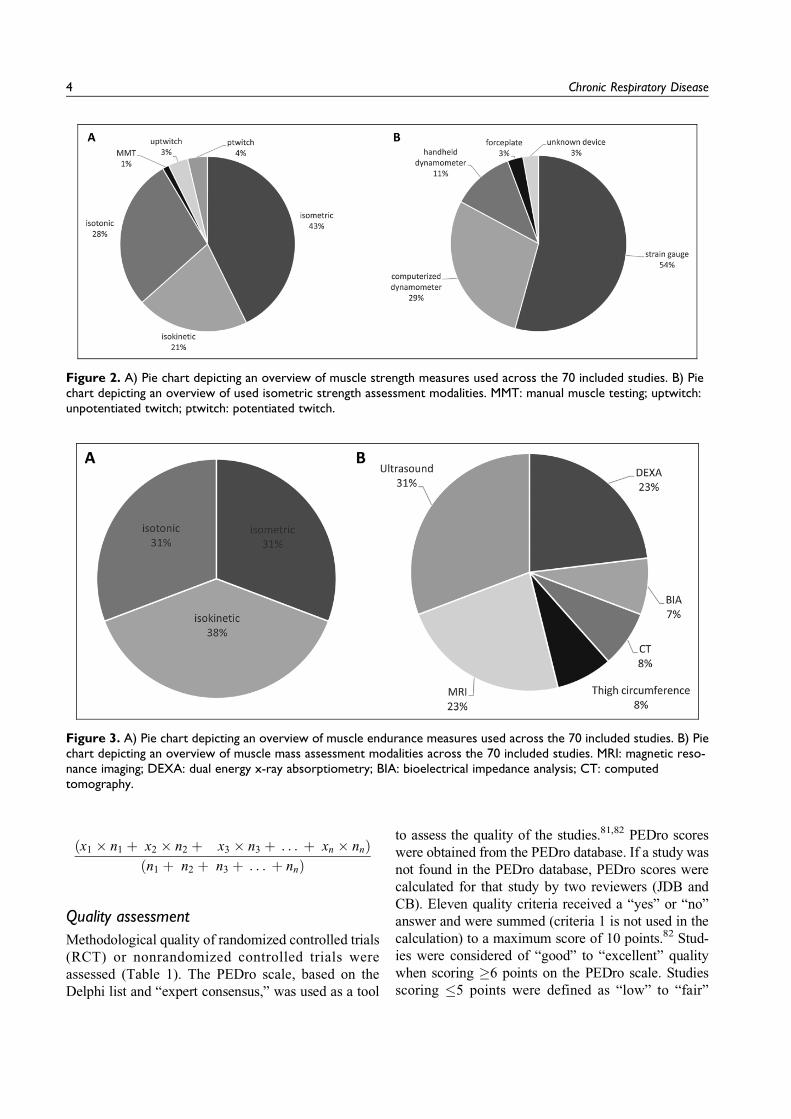
Figure 2. A) Pie chart depicting an overview of muscle strength measures used across the 70 included studies. B) Piechart depicting an overview of used isometric strength assessment modalities. MMT: manual muscle testing; uptwitch:unpotentiated twitch; ptwitch: potentiated twitch.
Figure 3. A) Pie chart depicting an overview of muscle endurance measures used across the 70 included studies. B) Piechart depicting an overview of muscle mass assessment modalities across the 70 included studies. MRI: magnetic reso-nance imaging; DEXA: dual energy x-ray absorptiometry; BIA: bioelectrical impedance analysis; CT: computedtomography.
4 Chronic Respiratory Disease

Figure 4. Effect of aerobic, resistance, combined aerobic and resistance training and NMES on various measures ofquadriceps strength in patients with COPD expressed as weighted means of relative change (percentage of baseline).Values on top of the bars are the number of patients with COPD. NMES: neuromuscular electrical stimulation.
Figure 5. Effect of different exercise interventions on quadriceps endurance in patients with COPD expressed as meanof relative change (percentage of baseline). NMES: neuromuscular electrical stimulation; HF: high-frequency NMES; LF:low-frequency NMES; HIIT: high-intensity interval training. #Significant change from baseline (within group effect: P < 0.05).
De Brandt et al. 5

Figure 6. Effect of different exercise interventions on muscle mass in patients with COPD expressed as mean of relativechange (percentage of baseline). T: thigh; LL: lower-limb; Q: quadriceps; RF: rectus femoris; IT: individualized training; NIT:non-individualized training; NMES: neuromuscular electrical stimulation; HIIT: high-intensity interval training; DEXA: dualenergy x-ray absorptiometry; MRI: magnetic resonance imaging; CT: computed tomography; BIA: bioelectrical impedanceanalysis. #Significant change from baseline (within group effect: P < 0.05).
Figure 7. Effect of different exercise interventions on isotonic quadriceps strength in patients with COPD expressed asmean of relative change (percentage of baseline). §Significantly different with aerobic training (P < 0.05 - between groupeffect).
6 Chronic Respiratory Disease
Tab
le1.
Ass
essm
ent
ofm
etho
dolo
gica
lqua
lity
ofR
CT
san
dno
n-ra
ndom
ized
cont
rolle
dtr
ials
base
don
the
PED
rosc
ori
ngsy
stem
.Stu
dies
are
rank
edal
phab
etic
ally
.
Aut
hor,
year
of
publ
icat
ion
Elig
ibili
tycr
iter
iaR
ando
mal
loca
tion
Conc
eale
dal
loca
tion
Bas
elin
eco
mpa
rabi
lity
Blin
dsu
bjec
tsB
lind
ther
apis
tsB
lind
asse
ssors
Ade
quat
efo
llow
-up
Inte
ntio
n-to
-tr
eat
anal
ysis
Bet
wee
n-gr
oup
com
pari
sons
Poin
tes
tim
ates
and
vari
abili
tyT
ota
lsco
reon
10
Ale
xand
eret
al.,
2008
72
Yes
10
10
00
00
11
4B
erna
rdet
al.,
1999
66
Yes
10
10
01
00
11
5B
our
jeily
-Hab
ret
al.,
2002
54
Yes
10
01
01
10
11
6
Bus
tam
ante
etal
.,20
1061
Yes
10
10
00
00
11
4C
higi
raet
al.,
2014
46
No
00
10
00
00
11
3C
lark
etal
.,19
9680
Yes
10
10
00
00
01
3C
lark
etal
.,20
0019
Yes
10
10
00
10
11
5C
ove
yet
al.,
2014
75
Yes
10
10
01
00
11
5D
alC
ors
oet
al.,
2007
56
Yes
10
11
00
10
11
6D
our
ado
etal
.,20
0873
Yes
10
10
00
00
11
4Fa
rias
etal
.,20
1417
No
11
10
01
10
11
7G
reul
ich
etal
.,20
1447
No
11
10
00
00
10
4H
off
etal
.,20
0721
No
10
10
00
11
11
6K
aym
azet
al.,
2015
78
Yes
00
00
00
10
11
3K
ong
sgaa
rdet
al.,
2004
20
Yes
10
10
00
00
11
4M
addo
cks
etal
.,20
1660
Yes
11
10
01
11
11
8M
ador
etal
.,20
0469
Yes
11
10
01
00
11
6N
apolis
etal
.,20
1157
Yes
10
01
01
10
11
6N
eder
etal
.,20
0255
Yes
11
10
00
11
11
7N
yber
get
al.,
2015
28
No
11
10
01
11
11
8O
’She
aet
al.,
2007
22
Yes
11
10
01
01
11
7O
rteg
aet
al.,
2002
67
No
10
10
00
10
11
5Pa
nton
etal
.,20
0470
No
00
00
00
10
11
3Ph
illip
set
al.,
2006
71
Yes
10
10
00
00
11
4Pl
egue
zuel
os
etal
.,20
1363
Yes
10
10
01
10
11
6
(con
tinue
d)
7
Tab
le1.
(cont
inue
d)
Aut
hor,
year
of
publ
icat
ion
Elig
ibili
tycr
iter
iaR
ando
mal
loca
tion
Conc
eale
dal
loca
tion
Bas
elin
eco
mpa
rabi
lity
Blin
dsu
bjec
tsB
lind
ther
apis
tsB
lind
asse
ssors
Ade
quat
efo
llow
-up
Inte
ntio
n-to
-tr
eat
anal
ysis
Bet
wee
n-gr
oup
com
pari
sons
Poin
tes
tim
ates
and
vari
abili
tyT
ota
lsco
reon
10
Probs
tet
al.,
2011
43
No
10
10
00
00
11
4R
amos
etal
.,20
1427
No
11
11
00
00
11
6Sa
lhie
tal
.,20
1564
Yes
11
10
00
00
11
5Si
llen
etal
.,20
1477
Yes
11
10
01
00
11
6Si
mps
on
etal
.,19
9218
Yes
10
10
01
10
11
6Sk
umlie
net
al.,
2007
37
Yes
00
10
00
01
11
4Sp
ruit
etal
.,20
0268
Yes
11
10
01
00
11
6T
asde
mir
etal
.,20
1579
No
11
10
00
00
11
5T
roost
ers
etal
.,20
0029
Yes
11
10
00
00
11
5V
anW
eter
ing
etal
.,20
0939
Yes
11
10
01
01
11
7
Vie
ira
etal
.,20
1459
Yes
10
10
00
00
11
4V
ivodt
zev
etal
.,20
1015
No
00
10
01
00
11
4V
ivodt
zev
etal
.,20
1258
No
10
11
01
10
11
7V
onb
ank
etal
.,20
1274
No
10
10
00
00
01
3Z
anin
iet
al.,
2015
76
Yes
10
10
00
10
01
4
8
Tab
le2.
Aer
obi
ctr
aini
ng.
Aut
hor,
year
of
publ
icat
ion
Num
ber
of
patien
ts(n
)M
ean
(SD
)FE
V1
(%pr
edic
ted)
Mea
n(S
D)
age
(y)
Stud
yde
sign
Stud
yin
terv
ention
Stud
ydu
ration
Out
com
em
easu
res
Sign
ifica
ntdi
ffere
nce
withi
ngr
oup
spo
sttr
aini
ng
Sign
ifica
ntch
ange
pre
topo
st(%
base
line)
Sign
ifica
ntdi
ffere
nce
betw
een
group
s(%
chan
ge)
O’D
onn
elle
tal
.,19
9711
20C
OPD
CO
PD:41
(3)
CO
PD:6
9(2
)Si
ngle
group
pre
post
-tes
t15
0m
inut
es:u
pper
and
low
erlim
bex
erci
ses:
wal
king
,sta
ircl
imbi
ng,
arm
ergo
met
ry,c
yclin
ger
gom
etry
,tre
adm
illex
erci
seat
or
belo
wB
org
brea
thle
ssne
ssra
ting
corr
espo
ndin
gto
sym
ptom
-lim
ited
max
imum
rating
6w
eeks
(3x/
w)
Kne
eex
tens
ion
stre
ngth
:iso
met
rica
Kne
eex
tens
ion
endu
ranc
e:is
om
etri
cco
ntra
ctio
nat
50%
of
max
imum
untile
xhau
stio
na
p<
0.00
1
ns
"21% –
– –
Mad
or
etal
.,20
0112
21C
OPD
CO
PD:45
(4)
CO
PD:7
0(2
)Si
ngle
group
pre–
post
test
Cyc
leer
gom
eter
and
trea
dmill
,ca
listh
enic
s,an
dst
retc
hing
exer
cise
s
8w
eeks
(3x/
w)
MV
Cqu
adri
ceps
:iso
met
rica
Unp
ote
ntia
ted
twitch
Pote
ntia
ted
twitch
p<
0.01
p¼
0.04
9p¼
0.05
"14.
9%"9
.7%
"8.8
%
– – –R
adom
-Aiz
iket
al.,
2007
13
6C
OPD
,5he
alth
y,ag
e-m
atch
edco
ntro
ls(H
C)
CO
PD:39
(3);
HC
:108
(8)
CO
PD:7
2(2
);H
C:7
0(2
)N
onc
ont
rolle
din
terv
ention
stud
yw
ith
subg
roup
anal
yses
.Sam
ein
terv
ention
for
both
group
s
45m
inut
esofcy
cle
ergo
met
erat
80%
ofin
divi
dual
max
imal
work
load
12w
eeks
(3x/
w)
Qua
dric
eps
peak
torq
ue:i
soki
netic
(60(
/sec
ond
s)b
CO
PD(p¼
0.00
3)ns
HC
"13.
6%–
Not
repo
rted
Viv
odt
zev
etal
.,20
0814
7C
OPD
,8he
alth
y,ag
e-m
atch
edco
ntro
ls(H
C)
CO
PD:29
(9);
HC
:94
(22)
CO
PD:6
0(6
);H
C:5
3(1
1)Si
ngle
group
pre
post
-tes
t(H
Conl
yba
selin
e)
10–3
0m
inut
esofcy
cle
ergo
met
erat
50%
ofin
itia
lWm
ax(if
work
load
was
tole
rate
d,w
ork
load
incr
ease
dw
ith
5W
)
12w
eeks
(3x/
w)
MV
Cqu
adri
ceps
:iso
met
ric.
a
Pote
ntia
ted
twitch
p¼
0.04
ns"1
0% –– –
Viv
odt
zev
etal
.,20
1015
17C
OPD
:10
trai
ning
(TR
),7
cont
rol(
C)
mat
ched
for
age,
dise
ase
seve
rity
,and
wal
king
dist
ance
TR
:62
(9);
C:6
3(6
)T
R:4
7(2
0);C
:54
(13)
Nonr
ando
miz
edco
ntro
lled
tria
lC
yclin
g:in
itia
llyat
38%
ofW
peak
.Pr
ogr
essi
vein
crea
seto
65%
of
Wpe
ak.D
urat
ion:
initia
lly18
min
utes
and
progr
essi
vely
incr
ease
dto
30m
inut
es.
4w
eeks
(5x/
w)
MV
Cqu
adri
ceps
:iso
met
ric.
a
Qua
dric
eps
endu
ranc
e:dy
nam
icle
gex
tens
ion
with
wei
ghts
corr
espo
ndin
gto
30%
MV
C(1
2m
ove
men
tspe
rm
inut
e)up
toex
haus
tiona
TR
(p<
0.00
8)ns
C;
TR
(p<
0.00
8)ns
C
"14% –"5
8.6%
–
TR
>C
(p<
0.05
);T
R>
C(p
<0.
05)
Guz
unet
al.,
2012
16
8C
OPD
,8se
dent
ary
and
heal
thy
age
and
gend
erm
atch
edco
ntro
ls(H
C)
CO
PD:1.
5(0
.16)
L;H
C:
3.3
(0.2
)L
(abs
olu
teFE
V1
valu
es)
CO
PD:6
2(4
);H
C:5
9(4
)N
onc
ont
rolle
din
terv
ention
stud
yw
ith
subg
roup
anal
yses
.Sam
ein
terv
ention
for
both
group
s.
45m
inut
es:c
ycle
ergo
met
erat
50%
ofW
peak
initia
llyan
dpr
ogr
esse
dup
to80
%ofW
peak
.
12w
eeks
(3x/
w)
MV
Cqu
adri
ceps
:iso
met
rica
nsC
OPD
nsH
C– –
HC
>C
OPD
(p<
0.05
)c
Fari
aset
al.,
2014
17
34C
OPD
:18
trai
ning
(TR
),16
cont
rol(
C)
TR
:56
(16)
C:5
1(1
4)T
R:6
5(1
0)C
:71
(8)
RC
T40
min
utes
ofw
alki
ng,p
rogr
essi
vely
incr
ease
dto
60m
inut
es.
8w
eeks
(5x/
w)
1R
Mle
gcu
rl
Mus
cle
mas
slo
wer
righ
tle
g(B
IA)
Mus
cle
mas
slo
wer
left
leg
(BIA
)
TR
(p<
0.05
)ns
CT
R(p
<0.
05)
nsC
TR
(p<
0.05
)ns
C
"50% –"8
.3%
–"8
.3%
–
nsbe
twee
ngr
oup
s
nsbe
twee
ngr
oup
s
nsbe
twee
ngr
oup
s
ns:n
ot
sign
ifica
nt;R
CT
:ran
dom
ized
cont
rolle
dtr
ial;
FEV
1:f
orc
edex
pire
dvo
lum
ein
1se
cond
;MV
C:m
axim
umvo
lunt
ary
cont
ract
ion;
BIA
:bio
elec
tric
alim
peda
nce
anal
ysis
;Wpe
ak/m
ax:p
eak/
max
imal
work
load
.a M
easu
red
via
stra
in-g
auge
syst
em.
bM
easu
red
via
com
pute
rize
ddy
nam
om
eter
(e.g
.Bio
dex)
.c B
etw
een
group
sdi
ffere
nce
base
don
post
trai
ning
valu
es.
9
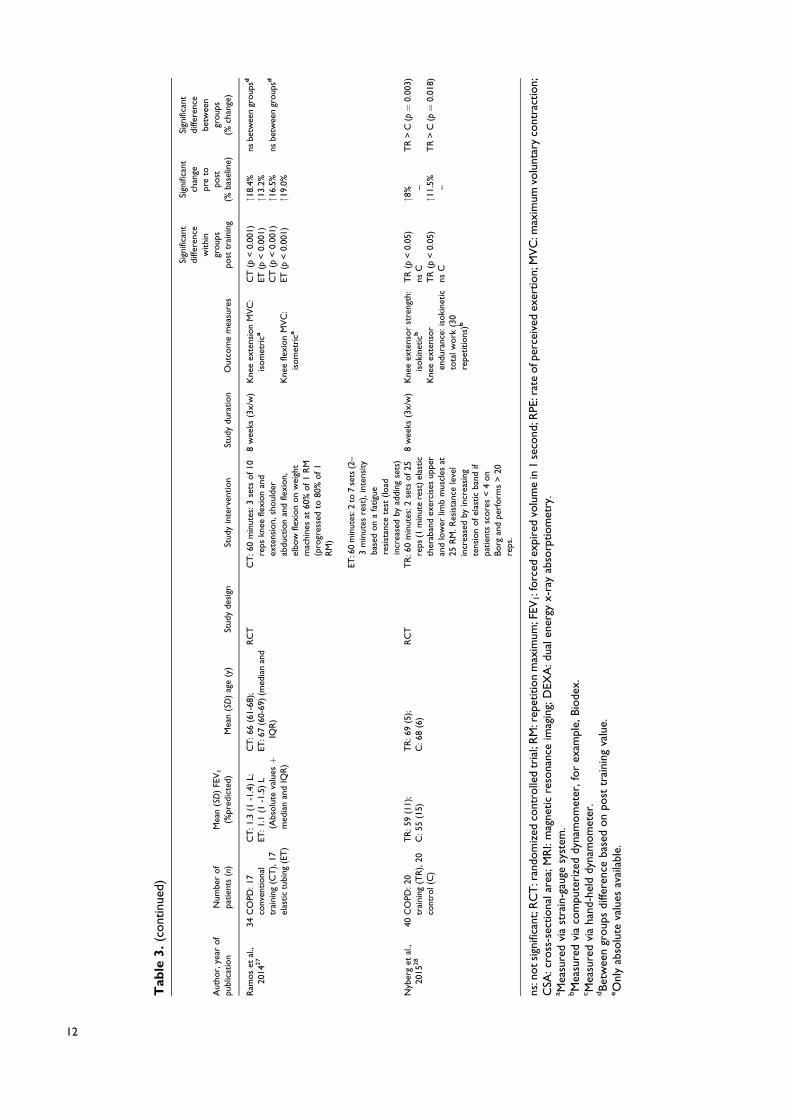
Tab
le3.
Res
ista
nce
trai
ning
.
Aut
hor,
year
of
publ
icat
ion
Num
ber
of
patien
ts(n
)M
ean
(SD
)FE
V1
(%pr
edic
ted)
Mea
n(S
D)
age
(y)
Stud
yde
sign
Stud
yin
terv
ention
Stud
ydu
ration
Out
com
em
easu
res
Sign
ifica
ntdi
ffere
nce
withi
ngr
oup
spo
sttr
aini
ng
Sign
ifica
ntch
ange
pre
topo
st(%
base
line)
Sign
ifica
ntdi
ffere
nce
betw
een
group
s(%
chan
ge)
Sim
pson
etal
.,19
9218
28C
OPD
:14
trai
ning
(TR
),14
cont
rol(
C)
TR
:40
(19)
;C
:39
(21)
TR
:73
(5);
C:7
0(6
)R
CT
TR
:3se
tsof10
reps
ofar
mcu
rl,l
egex
tens
ion,
and
leg
pres
sat
50–8
5%of1
RM
8w
eeks
(3x/
w)
Kne
eex
tens
ion
1R
M
Leg
pres
s1
RM
Qua
dric
eps
stre
ngth
:is
om
etri
ca
TR
(p<
0.01
)ns
CT
R(p
<0.
01)
nsC
TR
(p<
0.01
)ns
C
"44% –
"16% –
"25.
4% –
Not
repo
rted
Not
repo
rted
Not
repo
rted
Cla
rket
al.,
1996
17
48C
OPD
:32
circ
uit
trai
ning
(TR
),16
cont
rol(
C)
TR
:64
(29)
;C
:55
(22)
TR
:58
(8);
C:5
5(8
)R
CT
Hom
eex
erci
sepr
ogr
am:
ever
yex
erci
sefo
r30
upto
60se
cond
s:sh
oul
der
circ
ling,
full
arm
circ
ling,
incr
easi
ngan
dde
crea
sing
circ
les,
abdo
min
alex
erci
se,w
allp
ress
-ups
,si
ttin
gto
stan
ding
,qu
adri
ceps
exer
cise
,cal
fra
ises
,cal
fal
tern
ates
,w
alki
ngon
the
spot,
and
step
up.
12w
eeks
(7x/
w)
Isoki
netic
mus
cle
stre
ngth
b
Isoto
nic
mus
cle
endu
ranc
e(n
umbe
rofre
petitions
in30
seco
nds)
nsT
Rns
CT
R(p
<0.
05)
nsC
– –"2
5re
psf
–
Not
repo
rted
TR
>C
(p<
0.00
1)
Cla
rket
al.,
2000
19
43C
OPD
:26
trai
ning
(TR
),17
cont
rol(
C);
52he
alth
yco
ntro
ls(H
C)
TR
:76
(23)
;C
:79
(23)
;H
C:1
09(1
6)
TR
:51
(10)
;C
:46
(11)
;H
C:5
1(1
0)
RC
TT
R:1
0re
psof8
exer
cise
s(b
ench
pres
s,bo
dysq
uat,
squa
tca
lf,la
tiss
imus
,arm
curl
s,le
gpr
ess,
knee
flexi
on,
and
ham
stri
ngs)
at70
%of1
RM
12w
eeks
(2x/
w)
Qua
dric
eps
stre
ngth
:is
oto
nic.
Low
erbo
dym
uscl
est
reng
th:
isoki
netic
(70(
/se
cond
s)b.L
ow
erbo
dym
uscl
ew
ork
:is
oki
netic
(70(
/se
cond
s):r
epea
ted
cont
ract
ions
for
60se
cond
sb
Not
repo
rted
Not
repo
rted
TR
(p<
0.05
)ns
C
– –
"320
Je
TR
>C
(p<
0.00
1)ns
betw
een
group
sT
R>
C(p
<0.
02)
Kong
sgaa
rdet
al.,
2004
20
13C
OPD
:6tr
aini
ng(T
R),
7co
ntro
l(C
)
TR
:48
(4);
C:4
4(3
)T
R:7
1(1
);C
:73
(2)
RC
TT
R:6
0m
inut
es:4
sets
of8
reps
(2–3
min
utes
rest
)le
gpr
ess,
knee
exte
nsio
n,an
dkn
eefle
xion
at80
%of1
RM
12w
eeks
(2x/
w)
Qua
dric
eps
MV
C:
isom
etri
cb
Kne
eex
tens
ion:
isoki
netic
(60(
/se
cond
s)b
Kne
eex
tens
ion:
isoki
netic
(180( /
seco
nds)
b
5R
Mle
gpr
ess
CSA
quad
rice
ps(M
RI)
TR
(p<
0.05
)ns
CT
R(p
<0.
05)
nsC
TR
(p<
0.05
)ns
CT
R(P
<0.
01)
nsC
TR
(p<
0.05
)ns
C
"14.
7% –"1
7.8% –
"15.
1% –"3
6.5% –
"4.2
% –
TR
>C
(p<
0.05
)
TR
>C
(p<
0.05
)
TR
>C
(p<
0.05
)
TR
>C
(p<
0.01
)
nsbe
twee
ngr
oup
s
Hoff
etal
.,20
0721
12C
OPD
:6tr
aini
ng(T
R),
6co
ntro
l(C
)
TR
:33
(3);
C:4
0(6
)T
R:6
3(1
);C
:61
(3)
RC
TT
R:4
sets
of5
reps
(2m
inut
esre
st)
leg
pres
s(9
0(be
ndkn
ees
tost
raig
htle
gs)
at85
–90%
of1
RM
.Load
incr
ease
dw
ith
2.5
kgun
til
onl
yfiv
ere
psco
uld
beac
hiev
ed.
8w
eeks
(3x/
w)
1RM
leg
pres
sT
R(p
<0.
05)
nsC
"27.
1% –T
R>
C(p
<0.
05)
(con
tinue
d)
10
Tab
le3.
(cont
inue
d)
Aut
hor,
year
of
publ
icat
ion
Num
ber
of
patien
ts(n
)M
ean
(SD
)FE
V1
(%pr
edic
ted)
Mea
n(S
D)
age
(y)
Stud
yde
sign
Stud
yin
terv
ention
Stud
ydu
ration
Out
com
em
easu
res
Sign
ifica
ntdi
ffere
nce
withi
ngr
oup
spo
sttr
aini
ng
Sign
ifica
ntch
ange
pre
topo
st(%
base
line)
Sign
ifica
ntdi
ffere
nce
betw
een
group
s(%
chan
ge)
O’S
hea
etal
.,20
0722
44C
OPD
:20
trai
ning
(TR
),24
cont
rol(
C)
TR
:49
(25)
;C
:52
(22)
TR
:67
(7);
C:6
8(1
0)R
CT
TR
:3se
tsof8
–12
RM
agai
nst
elas
tic
band
sofin
crea
sing
resi
stan
ce.E
xerc
ises
:st
andi
nghi
pab
duct
ion,
sim
ulat
edlif
ting
,sit-t
o-
stan
d,se
ated
row
,lun
ges
and
ches
tpr
ess.
Res
ista
nce
leve
lwas
incr
ease
dw
hen
3se
tsof
12re
psw
ere
achi
eved
.
12w
eeks
(3x/
w)
Kne
eex
tens
or
stre
ngth
:is
om
etri
cc
Hip
abdu
ctor
stre
ngth
:is
om
etri
cc
Not
repo
rted
Not
repo
rted
– –
TR
>C
(p<
0.01
)
nsbe
twee
ngr
oup
s
Houc
hen
etal
.,20
1123
43C
OPD
CO
PD:46
(21)
CO
PD:6
8(8
)Si
ngle
group
pre
post
-tes
tT
R:3
sets
of8
reps
leg
exte
nsio
nan
dle
gcu
rls
on
wei
ght
mac
hine
sat
60–
70%
of1
RM
(pro
gres
sive
lyin
crea
sed
ifR
PEsc
ore
sw
ent
dow
n)þ
step
upan
dsi
tto
stan
dex
erci
ses
(3se
tsof8
reps
)
7w
eeks
(3x/
w)
Qua
dric
eps
stre
ngth
:is
om
etri
cbp
<0.
001
"22.
8%–
Men
on
etal
.,20
12a2
412
CO
PD,7
heal
thy,
age-
mat
ched
cont
rols
(HC
)
CO
PD:46
(6);
HC
:103
(6)
CO
PD:6
7(2
);H
C:6
7(2
)N
on-
cont
rolle
din
terv
ention
stud
yw
ith
subg
roup
anal
yses
.Sam
ein
terv
ention
for
both
group
s.
TR
:30
min
utes
ofbi
late
ral,
low
erlim
b,hi
ghin
tens
ity
isoki
netic
resi
stan
cetr
aini
ngon
anis
oki
netic
dyna
mom
eter
(5se
tsof3
0m
axim
alis
oki
netic
knee
cont
ract
ions
atan
gula
rve
loci
tyof18
0(/s
econd
)
8w
eeks
(3x/
w)
Qua
dric
eps
stre
ngth
:is
om
etri
cpe
akto
rque
b
Qua
dric
eps
conc
entr
icst
reng
th:is
oki
netic
peak
torq
ueb
Thi
ghle
anm
ass
(DEX
A)
CO
PD(p¼
0.00
2)H
C(p¼
0.04
6)C
OPD
(p¼
0.00
1)ns
HC
CO
PD(p¼
0.00
3)H
C(p¼
0.00
4)
"13.
2%"1
0.1%
"25.
2% –"7
.3%
"5.1
%
not
repo
rted
not
repo
rted
not
repo
rted
Men
on
etal
.,20
12b2
545
CO
PD,
19he
alth
y,ag
e-m
atch
edco
ntro
ls(H
C)
CO
PD:47
(19)
;H
C:1
07(2
2)C
OPD
:68
(8);
HC
:66
(5)
Nonc
ont
rolle
din
terv
ention
stud
yw
ith
subg
roup
anal
yses
.Sam
ein
terv
ention
for
both
group
s.
TR
:30
min
utes
ofbi
late
ral,
low
erlim
b,hi
ghin
tens
ity
isoki
netic
resi
stan
cetr
aini
ngon
anis
oki
netic
dyna
mom
eter
(5se
tsof3
0m
axim
alis
oki
netic
knee
cont
ract
ions
atan
gula
rve
loci
tyof18
0(/s
econd
s)
8w
eeks
(3x/
w)
Qua
dric
eps
MV
C:
isom
etri
cb
Thi
ghle
anm
ass
(DEX
A)
Rec
tus
fem
ori
sC
SA(U
ltra
soun
d)
Qua
dric
eps
mus
cle
thic
knes
s(U
ltra
soun
d)
CO
PD(p
<0.
0001
)H
C(p¼
0.02
4)C
OPD
(p<
0.00
01)
HC
(p<
0.00
1)C
OPD
(p<
0.00
01)
HC
(p<
0.00
01)
CO
PD(p
<0.
0001
)H
C(p
<0.
001)
"20.
0%"1
1.3%
"5.7
%"5
.4%
"21.
8%"1
9.5%
"12.
1%"1
0.9%
Not
repo
rted
Not
repo
rted
Not
repo
rted
Not
repo
rted
Ric
ci-V
itor
etal
.,20
1326
13C
OPD
CO
PD:48
.3(1
2.1)
CO
PD:6
7.2
(7.3
)Si
ngle
group
pre
post
-tes
tT
R:6
0m
inut
es:3
sets
of10
reps
(2–3
min
utes
rest
)lo
wer
limb
(kne
efle
xion
and
exte
nsio
non
leg
bend
and
leg
exte
nsio
neq
uipm
ent)
and
uppe
rlim
bst
reng
that
60%
of1
RM
(pro
gres
sed
to80
%of
1R
M)
8w
eeks
(3x/
w)
Kne
eex
tens
ion
MV
C:
isom
etri
ca
Kne
efle
xion
MV
C:
isom
etri
ca
ns p¼
0.02
3–
"11.
4%– –
(con
tinue
d)
11
Tab
le3.
(cont
inue
d)
Aut
hor,
year
of
publ
icat
ion
Num
ber
of
patien
ts(n
)M
ean
(SD
)FE
V1
(%pr
edic
ted)
Mea
n(S
D)
age
(y)
Stud
yde
sign
Stud
yin
terv
ention
Stud
ydu
ration
Out
com
em
easu
res
Sign
ifica
ntdi
ffere
nce
withi
ngr
oup
spo
sttr
aini
ng
Sign
ifica
ntch
ange
pre
topo
st(%
base
line)
Sign
ifica
ntdi
ffere
nce
betw
een
group
s(%
chan
ge)
Ram
os
etal
.,20
1427
34C
OPD
:17
conv
entiona
ltr
aini
ng(C
T),
17el
astic
tubi
ng(E
T)
CT
:1.3
(1-1
.4)
L;ET
:1.1
(1-1
.5)
L(A
bsolu
teva
luesþ
med
ian
and
IQR
)
CT
:66
(61-
68);
ET:6
7(6
0-69
)(m
edia
nan
dIQ
R)
RC
TC
T:6
0m
inut
es:3
sets
of10
reps
knee
flexi
on
and
exte
nsio
n,sh
oul
der
abdu
ctio
nan
dfle
xion,
elbo
wfle
xion
on
wei
ght
mac
hine
sat
60%
of1
RM
(pro
gres
sed
to80
%of1
RM
)
ET:6
0m
inut
es:2
to7
sets
(2–
3m
inut
esre
st),
inte
nsity
base
don
afa
tigu
ere
sist
ance
test
(load
incr
ease
dby
addi
ngse
ts)
8w
eeks
(3x/
w)
Kne
eex
tens
ion
MV
C:
isom
etri
ca
Kne
efle
xion
MV
C:
isom
etri
ca
CT
(p<
0.00
1)ET
(p<
0.00
1)C
T(p
<0.
001)
ET(p
<0.
001)
"18.
4%"1
3.2%
"16.
5%"1
9.0%
nsbe
twee
ngr
oup
sd
nsbe
twee
ngr
oup
sd
Nyb
erg
etal
.,20
1528
40C
OPD
:20
trai
ning
(TR
),20
cont
rol(
C)
TR
:59
(11)
;C
:55
(15)
TR
:69
(5);
C:6
8(6
)R
CT
TR
:60
min
utes
:2se
tsof25
reps
(1m
inut
ere
st)el
astic
ther
aban
dex
erci
ses
uppe
ran
dlo
wer
limb
mus
cles
at25
RM
.Res
ista
nce
leve
lin
crea
sed
byin
crea
sing
tens
ion
ofel
astic
band
ifpa
tien
tssc
ore
s<
4on
Borg
and
perf
orm
s>
20re
ps.
8w
eeks
(3x/
w)
Kne
eex
tens
or
stre
ngth
:is
oki
neticb
Kne
eex
tens
or
endu
ranc
e:is
oki
netic
tota
lwork
(30
repe
titions
)b
TR
(p<
0.05
)ns
CT
R(p
<0.
05)
nsC
"8% –
"11.
5% –
TR
>C
(p¼
0.00
3)
TR
>C
(p¼
0.01
8)
ns:n
otsi
gnifi
cant
;RC
T:r
ando
miz
edco
ntro
lled
tria
l;R
M:r
epet
itio
nm
axim
um;F
EV1:f
orc
edex
pire
dvo
lum
ein
1se
cond
;RPE
:rat
eofp
erce
ived
exer
tion;
MV
C:m
axim
umvo
lunt
ary
cont
ract
ion;
CSA
:cro
ss-s
ectiona
lare
a;M
RI:
mag
netic
reso
nanc
eim
agin
g;D
EXA
:dua
lene
rgy
x-ra
yab
sorp
tiom
etry
.a M
easu
red
via
stra
in-g
auge
syst
em.
bM
easu
red
via
com
pute
rize
ddy
nam
om
eter
,fo
rex
ampl
e,Bio
dex.
c Mea
sure
dvi
aha
nd-h
eld
dyna
mom
eter
.dBet
wee
ngr
oup
sdi
ffere
nce
base
don
post
trai
ning
valu
e.eO
nly
abso
lute
valu
esav
aila
ble.
12
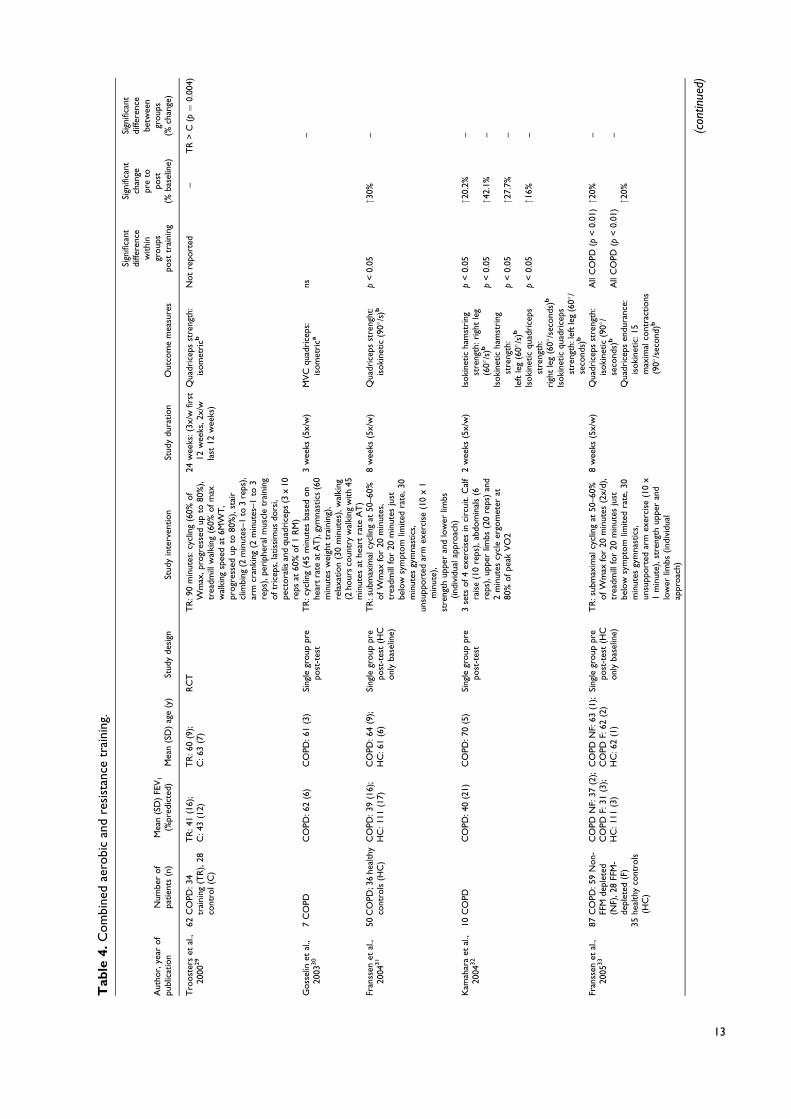
Tab
le4.
Com
bine
dae
robi
can
dre
sist
ance
trai
ning
.
Aut
hor,
year
of
publ
icat
ion
Num
ber
of
patien
ts(n
)M
ean
(SD
)FE
V1
(%pr
edic
ted)
Mea
n(S
D)
age
(y)
Stud
yde
sign
Stud
yin
terv
ention
Stud
ydu
ration
Out
com
em
easu
res
Sign
ifica
ntdi
ffere
nce
withi
ngr
oup
spo
sttr
aini
ng
Sign
ifica
ntch
ange
pre
topo
st(%
base
line)
Sign
ifica
ntdi
ffere
nce
betw
een
group
s(%
chan
ge)
Tro
ost
ers
etal
.,20
0029
62C
OPD
:34
trai
ning
(TR
),28
cont
rol(
C)
TR
:41
(16)
;C
:43
(12)
TR
:60
(9);
C:6
3(7
)R
CT
TR
:90
min
utes
:cyc
ling
(60%
of
Wm
ax,p
rogr
esse
dup
to80
%),
trea
dmill
wal
king
(60%
ofm
axw
alki
ngsp
eed
at6M
WT
,pr
ogr
esse
dup
to80
%),
stai
rcl
imbi
ng(2
min
utes
–1to
3re
ps),
arm
cran
king
(2m
inut
es–1
to3
reps
),pe
riph
eral
mus
cle
trai
ning
oftr
icep
s,la
tiss
imus
dors
i,pe
ctora
lisan
dqu
adri
ceps
(3x
10re
psat
60%
of1
RM
)
24w
eeks
:(3x
/wfir
st12
wee
ks,2
x/w
last
12w
eeks
)
Qua
dric
eps
stre
ngth
:is
om
etri
cbN
ot
repo
rted
–T
R>
C(p¼
0.00
4)
Goss
elin
etal
.,20
0330
7C
OPD
CO
PD:62
(6)
CO
PD:61
(3)
Sing
legr
oup
pre
post
-tes
tT
R:c
yclin
g(4
5m
inut
esba
sed
on
hear
tra
teat
AT
),gy
mna
stic
s(6
0m
inut
esw
eigh
ttr
aini
ng),
rela
xation
(30
min
utes
),w
alki
ng(2
hour
sco
untr
yw
alki
ngw
ith
45m
inut
esat
hear
tra
teA
T)
3w
eeks
(5x/
w)
MV
Cqu
adri
ceps
:is
om
etri
cans
–
Fran
ssen
etal
.,20
0431
50C
OPD
;36
heal
thy
cont
rols
(HC
)C
OPD
:39
(16)
;H
C:1
11(1
7)C
OPD
:64
(9);
HC
:61
(6)
Sing
legr
oup
pre
post
-tes
t(H
Conl
yba
selin
e)
TR
:sub
max
imal
cycl
ing
at50
–60%
ofW
max
for
20m
inut
es,
trea
dmill
for
20m
inut
esju
stbe
low
sym
ptom
limited
rate
,30
min
utes
gym
nast
ics,
unsu
pport
edar
mex
erci
se(1
0x
1m
inut
e),
stre
ngth
uppe
ran
dlo
wer
limbs
(ind
ivid
uala
ppro
ach)
8w
eeks
(5x/
w)
Qua
dric
eps
stre
nght
:is
oki
netic
(90(
/s)b
p<
0.05
"30%
–
Kam
ahar
aet
al.,
2004
32
10C
OPD
CO
PD:40
(21)
CO
PD:70
(5)
Sing
legr
oup
pre
post
-tes
t3
sets
of4
exer
cise
sin
circ
uit.
Cal
fra
ise
(10
reps
),ab
dom
inal
s(6
reps
),up
per
limbs
(20
reps
)an
d2
min
utes
cycl
eer
gom
eter
at80
%ofpe
akV
O2
2w
eeks
(5x/
w)
Isoki
netic
ham
stri
ngst
reng
th:ri
ght
leg
(60(
/s)b
Isoki
netic
ham
stri
ngst
reng
th:
left
leg
(60(
/s)b
Isoki
netic
quad
rice
psst
reng
th:
righ
tle
g(6
0(/s
econd
s)b
Isoki
netic
quad
rice
psst
reng
th:l
eft
leg
(60(
/se
cond
s)b
p<
0.05
p<
0.05
p<
0.05
p<
0.05
"20.
2%
"42.
1%
"27.
7%
"16%
– – – –
Fran
ssen
etal
.,20
0533
87C
OPD
:59
Non-
FFM
depl
eted
(NF)
,28
FFM
-de
plet
ed(F
)35
heal
thy
cont
rols
(HC
)
CO
PDN
F:37
(2);
CO
PDF:
31(3
);H
C:1
11(3
)
CO
PDN
F:63
(1);
CO
PDF:
62(2
)H
C:6
2(1
)
Sing
legr
oup
pre
post
-tes
t(H
Conl
yba
selin
e)
TR
:sub
max
imal
cycl
ing
at50
–60%
ofW
max
for
20m
inut
es(2
x/d)
,tr
eadm
illfo
r20
min
utes
just
belo
wsy
mpt
om
limited
rate
,30
min
utes
gym
nast
ics,
unsu
pport
edar
mex
erci
se(1
0x
1m
inut
e),st
reng
thup
per
and
low
erlim
bs(ind
ivid
ual
appr
oac
h)
8w
eeks
(5x/
w)
Qua
dric
eps
stre
ngth
:is
oki
netic
(90(
/se
cond
s)b
Qua
dric
eps
endu
ranc
e:is
oki
netic:
15m
axim
alco
ntra
ctio
ns(9
0(/s
econd
)b
All
CO
PD(p
<0.
01)
All
CO
PD(p
<0.
01)
"20%
"20%
– – (con
tinue
d)
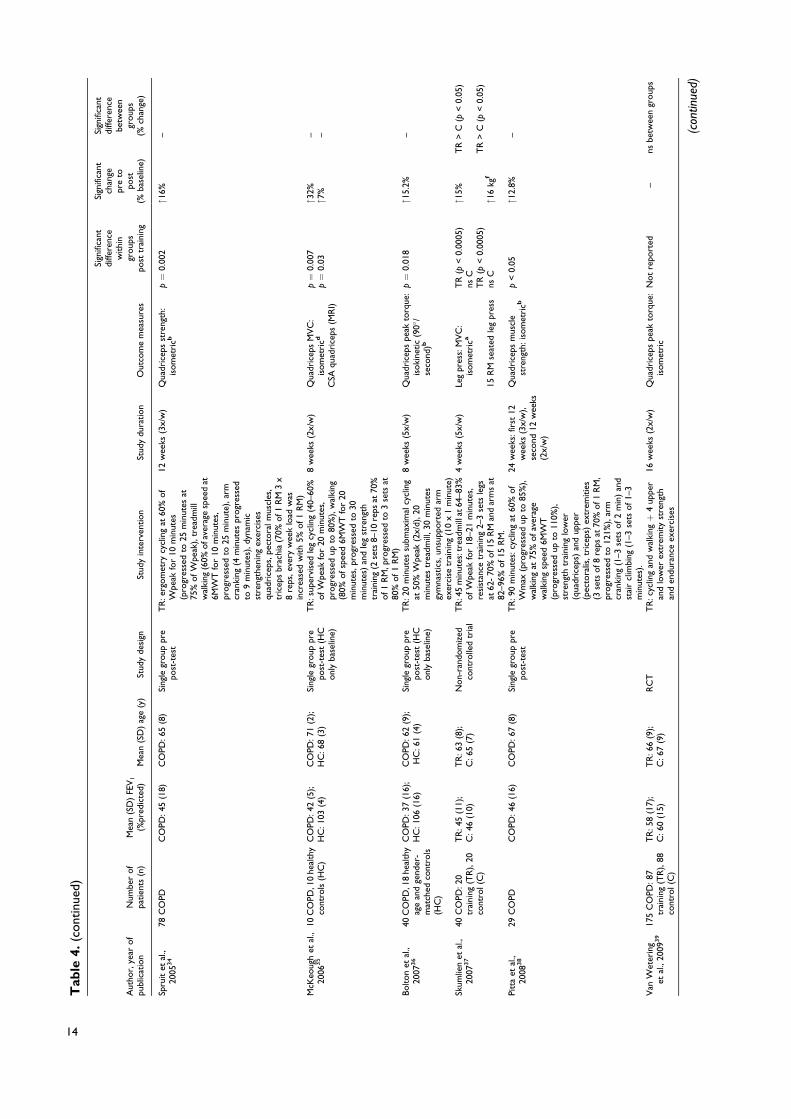
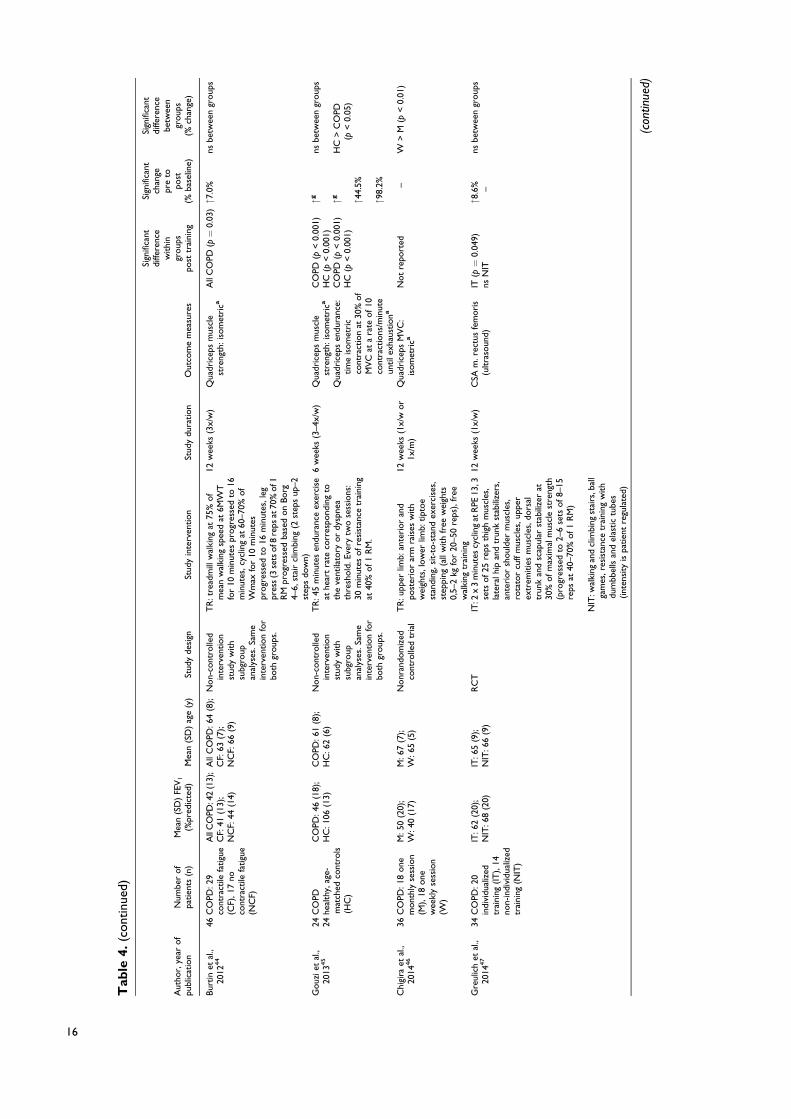
13
Tab
le4.
(cont
inue
d)
Aut
hor,
year
of
publ
icat
ion
Num
ber
of
patien
ts(n
)M
ean
(SD
)FE
V1
(%pr
edic
ted)
Mea
n(S
D)
age
(y)
Stud
yde
sign
Stud
yin
terv
ention
Stud
ydu
ration
Out
com
em
easu
res
Sign
ifica
ntdi
ffere
nce
withi
ngr
oup
spo
sttr
aini
ng
Sign
ifica
ntch
ange
pre
topo
st(%
base
line)
Sign
ifica
ntdi
ffere
nce
betw
een
group
s(%
chan
ge)
Spru
itet
al.,
2005
34
78C
OPD
CO
PD:45
(18)
CO
PD:65
(8)
Sing
legr
oup
pre
post
-tes
tT
R:e
rgom
etry
cycl
ing
at60
%of
Wpe
akfo
r10
min
utes
(pro
gres
sed
to25
min
utes
at75
%ofW
peak
),tr
eadm
illw
alki
ng(6
0%ofa
vera
gesp
eed
at6M
WT
for
10m
inut
es,
progr
esse
dto
25m
inut
e),ar
mcr
anki
ng(4
min
utes
progr
esse
dto
9m
inut
es),
dyna
mic
stre
ngth
enin
gex
erci
ses
quad
rice
ps,p
ecto
ralm
uscl
es,
tric
eps
brac
hia
(70%
of1
RM
3x
8re
ps,e
very
wee
klo
adw
asin
crea
sed
with
5%of1
RM
)
12w
eeks
(3x/
w)
Qua
dric
eps
stre
ngth
:is
om
etri
cbp¼
0.00
2"1
6%–
McK
eoug
het
al.,
2006
35
10C
OPD
,10
heal
thy
cont
rols
(HC
)C
OPD
:42
(5);
HC
:103
(4)
CO
PD:71
(2);
HC
:68
(3)
Sing
legr
oup
pre
post
-tes
t(H
Conl
yba
selin
e)
TR
:sup
ervi
sed
leg
cycl
ing
(40–
60%
ofW
peak
for
20m
inut
es,
progr
esse
dup
to80
%),
wal
king
(80%
ofsp
eed
6MW
Tfo
r20
min
utes
,pro
gres
sed
to30
min
utes
)an
dle
gst
reng
thtr
aini
ng(2
sets
8–10
reps
at70
%of1
RM
,pro
gres
sed
to3
sets
at80
%of1
RM
)
8w
eeks
(2x/
w)
Qua
dric
eps
MV
C:
isom
etri
cd
CSA
quad
rice
ps(M
RI)
p¼
0.00
7p¼
0.03
"32%
"7%
– –
Bolton
etal
.,20
0736
40C
OPD
,18
heal
thy
age
and
gend
er-
mat
ched
cont
rols
(HC
)
CO
PD:37
(16)
;H
C:1
06(1
6)C
OPD
:62
(9);
HC
:61
(4)
Sing
legr
oup
pre
post
-tes
t(H
Conl
yba
selin
e)
TR
:20
min
utes
subm
axim
alcy
clin
gat
50%
Wpe
ak(2
x/d)
,20
min
utes
trea
dmill
,30
min
utes
gym
nast
ics,
unsu
pport
edar
mex
erci
setr
aini
ng(1
0x
1m
inut
e)
8w
eeks
(5x/
w)
Qua
dric
eps
peak
torq
ue:
isoki
netic
(90(
/se
cond
)b
p¼
0.01
8"1
5.2%
–
Skum
lien
etal
.,20
0737
40C
OPD
:20
trai
ning
(TR
),20
cont
rol(
C)
TR
:45
(11)
;C
:46
(10)
TR
:63
(8);
C:6
5(7
)N
on-
rand
om
ized
cont
rolle
dtr
ial
TR
:45
min
utes
:tre
adm
illat
64–8
3%ofW
peak
for
18–2
1m
inut
es,
resi
stan
cetr
aini
ng2–
3se
tsle
gsat
62-
70%
of1
5R
Man
dar
ms
at82
–96%
of15
RM
.
4w
eeks
(5x/
w)
Leg
pres
s:M
VC
:is
om
etri
ca
15R
Mse
ated
leg
pres
s
TR
(p<
0.00
05)
nsC
TR
(p<
0.00
05)
nsC
"15%
"16
kgf
TR
>C
(p<
0.05
)
TR
>C
(p<
0.05
)
Pitt
aet
al.,
2008
38
29C
OPD
CO
PD:46
(16)
CO
PD:67
(8)
Sing
legr
oup
pre
post
-tes
tT
R:9
0m
inut
es:c
yclin
gat
60%
of
Wm
ax(p
rogr
esse
dup
to85
%),
wal
king
at75
%ofav
erag
ew
alki
ngsp
eed
6MW
T(p
rogr
esse
dup
to11
0%),
stre
ngth
trai
ning
low
er(q
uadr
icep
s)an
dup
per
(pec
tora
lis,t
rice
ps)
extr
emitie
s(3
sets
of8
reps
at70
%of1
RM
,pr
ogr
esse
dto
121%
),ar
mcr
anki
ng(1
–3se
tsof2
min
)an
dst
air
clim
bing
(1–3
sets
of1–
3m
inut
es).
24w
eeks
:fir
st12
wee
ks(3
x/w
),se
cond
12w
eeks
(2x/
w)
Qua
dric
eps
mus
cle
stre
ngth
:is
om
etri
cbp
<0.
05"1
2.8%
–
Van
Wet
erin
get
al.,
2009
39
175
CO
PD:8
7tr
aini
ng(T
R),
88co
ntro
l(C
)
TR
:58
(17)
;C
:60
(15)
TR
:66
(9);
C:6
7(9
)R
CT
TR
:cyc
ling
and
wal
kingþ
4up
per
and
low
erex
trem
ity
stre
ngth
and
endu
ranc
eex
erci
ses
16w
eeks
(2x/
w)
Qua
dric
eps
peak
torq
ue:
isom
etri
cN
ot
repo
rted
–ns
betw
een
group
s
(con
tinue
d)
14

Tab
le4.
(cont
inue
d)
Aut
hor,
year
of
publ
icat
ion
Num
ber
of
patien
ts(n
)M
ean
(SD
)FE
V1
(%pr
edic
ted)
Mea
n(S
D)
age
(y)
Stud
yde
sign
Stud
yin
terv
ention
Stud
ydu
ration
Out
com
em
easu
res
Sign
ifica
ntdi
ffere
nce
withi
ngr
oup
spo
sttr
aini
ng
Sign
ifica
ntch
ange
pre
topo
st(%
base
line)
Sign
ifica
ntdi
ffere
nce
betw
een
group
s(%
chan
ge)
Evan
set
al.,
2010
40
44C
OPD
CO
PD:43
(15)
CO
PD:69
(8)
Sing
legr
oup
pre
post
-tes
tT
R:1
20m
inut
es:w
alki
ngat
85%
of
VO
2pe
akofIS
WT
(pro
gres
sed
base
don
Borg
3–6)
,per
iphe
ral
mus
cle
exer
cise
sup
per
and
low
erlim
bs(8
exer
cise
s:10
reps
)
7w
eeks
(2x/
ww
alki
ng,3
x/w
stre
ngth
)
Qua
dric
eps
peak
torq
ue:
isom
etri
cbns
––
Ari
zono
etal
.,20
1141
57C
OPD
CO
PD:44
(16)
CO
PD:63
(8)
Sing
legr
oup
pre
post
-tes
tT
R:6
0m
inut
essu
perv
ised
:cyc
leer
gom
eter
for
20m
inut
esat
80%
ofW
peak
,str
engt
htr
aini
ngup
per
and
low
erbo
dy(1
1ex
erci
ses:
step
-ups
,sit-t
o-s
tand
,le
gpr
ess,
knee
exte
nsio
ns,t
runk
flexi
on,
trun
kro
tation,
pelv
ictilt,
lyin
gtr
icep
sex
tens
ion,
dum
bbel
lbe
nch
pres
s,du
mbb
ellf
ly,
shoul
der
shru
gs)
Uns
uper
vise
d:w
alki
ng(2
0m
inut
esat
Borg
dysp
nea
inte
nsity
4an
d5)
10w
eeks
(2x/
wsu
perv
ised
,3x/
wun
supe
rvis
ed)
Kne
eex
tens
ion
stre
ngth
:is
oki
neticb
p<
0.01
"8.3
%–
Kozu
etal
.,20
1142
45C
OPD
CO
PD:45
(12)
CO
PD:67
(5)
Sing
legr
oup
pre
post
-tes
tT
R:4
0–50
min
utes
:cyc
ling
at50
%of
Wpe
akfo
r5–
10m
inut
espr
ogr
esse
dto
20m
inut
es,
repe
titive
bila
tera
lsho
ulde
rfle
xion
and
abdu
ctio
nw
ith
light
wei
ghts
(2m
inut
es),
stre
ngth
trai
ning
:fre
ew
eigh
ts,1
set
of1
0re
pspr
ogr
esse
dto
3se
ts.
8w
eeks
(2x/
w)
Qua
dric
eps
stre
ngth
:is
om
etri
cc
Qua
dric
eps
stre
ngth
(%bo
dyw
eigh
t)c
p<
0.01
p<
0.01
"23.
5%
"23.
3%
– –
Probs
tet
al.,
2011
43
40C
OPD
:20
low
inte
nsity
(L),
20hi
ghin
tens
ity
(H)
L:39
(14)
;H
:40
(13)
L:65
(10)
;H
:67
(7)
RC
TL:
60m
inut
es:5
sets
ofex
erci
ses:
brea
thin
gex
erci
ses,
stre
ngth
enin
gofth
eab
dom
inal
mus
cles
,cal
isth
enic
s(1
set¼
12di
ffere
ntex
erci
ses,
15re
ps).
Incr
ease
inte
nsity
bym
ore
diffi
cult
exec
utio
nofex
erci
ses
H:6
0m
inut
es:c
yclin
gat
60%
of
Wm
ax,w
alki
ngat
75%
of
aver
age
wal
king
spee
dba
sed
on
6MW
T(p
rogr
essi
on
base
don
Borg
4–6)
and
stre
ngth
trai
ning
ofq
uadr
icep
s,bi
ceps
and
tric
eps
at70
%of1
RM
12w
eeks
(3x/
w)
1R
Mqu
adri
ceps
:leg
exte
nsio
nns
LH
(p¼
0.02
)–
"33.
9%H
>L
(p¼
0.04
)
(con
tinue
d)
15
Tab
le4.
(cont
inue
d)
Aut
hor,
year
of
publ
icat
ion
Num
ber
of
patien
ts(n
)M
ean
(SD
)FE
V1
(%pr
edic
ted)
Mea
n(S
D)
age
(y)
Stud
yde
sign
Stud
yin
terv
ention
Stud
ydu
ration
Out
com
em
easu
res
Sign
ifica
ntdi
ffere
nce
withi
ngr
oup
spo
sttr
aini
ng
Sign
ifica
ntch
ange
pre
topo
st(%
base
line)
Sign
ifica
ntdi
ffere
nce
betw
een
group
s(%
chan
ge)
Bur
tin
etal
.,20
1244
46C
OPD
:29
cont
ract
ilefa
tigu
e(C
F),1
7no
cont
ract
ilefa
tigu
e(N
CF)
All
CO
PD:4
2(1
3);
CF:
41(1
3);
NC
F:44
(14)
All
CO
PD:6
4(8
);C
F:63
(7);
NC
F:66
(9)
Non-
cont
rolle
din
terv
ention
stud
yw
ith
subg
roup
anal
yses
.Sam
ein
terv
ention
for
both
group
s.
TR
:tre
adm
illw
alki
ngat
75%
of
mea
nw
alki
ngsp
eed
at6M
WT
for
10m
inut
espr
ogr
esse
dto
16m
inut
es,c
yclin
gat
60–7
0%of
Wm
axfo
r10
min
utes
progr
esse
dto
16m
inut
es,l
egpr
ess
(3se
tsof8
reps
at70
%of1
RM
progr
esse
dba
sed
on
Borg
4–6,
stai
rcl
imbi
ng(2
step
sup
–2st
eps
dow
n)
12w
eeks
(3x/
w)
Qua
dric
eps
mus
cle
stre
ngth
:is
om
etri
caA
llC
OPD
(p¼
0.03
)"7
.0%
nsbe
twee
ngr
oup
s
Gouz
iet
al.,
2013
45
24C
OPD
24he
alth
y,ag
e-m
atch
edco
ntro
ls(H
C)
CO
PD:46
(18)
;H
C:1
06(1
3)C
OPD
:61
(8);
HC
:62
(6)
Non-
cont
rolle
din
terv
ention
stud
yw
ith
subg
roup
anal
yses
.Sam
ein
terv
ention
for
both
group
s.
TR
:45
min
utes
endu
ranc
eex
erci
seat
hear
tra
teco
rres
pond
ing
toth
eve
ntila
tory
or
dysp
nea
thre
shold
.Eve
rytw
ose
ssio
ns:
30m
inut
esofre
sist
ance
trai
ning
at40
%of1
RM
.
6w
eeks
(3–4
x/w
)Q
uadr
icep
sm
uscl
est
reng
th:is
om
etri
ca
Qua
dric
eps
endu
ranc
e:tim
eis
om
etri
cco
ntra
ctio
nat
30%
of
MV
Cat
ara
teof10
cont
ract
ions
/min
ute
untile
xhau
stio
na
CO
PD(p
<0.
001)
HC
(p<
0.00
1)C
OPD
(p<
0.00
1)H
C(p
<0.
001)
"g "g "44.
5%
"98.
2%
nsbe
twee
ngr
oup
s
HC
>C
OPD
(p<
0.05
)
Chi
gira
etal
.,20
1446
36C
OPD
:18
one
mont
hly
sess
ion
(M),
18one
wee
kly
sess
ion
(W)
M:5
0(2
0);
W:4
0(1
7)M
:67
(7);
W:6
5(5
)N
onr
ando
miz
edco
ntro
lled
tria
lT
R:u
pper
limb:
ante
rior
and
post
erio
rar
mra
ises
with
wei
ghts
,low
erlim
b:tipt
oe
stan
ding
,sit-t
o-s
tand
exer
cise
s,st
eppi
ng(a
llw
ith
free
wei
ghts
0,5–
2kg
for
20–5
0re
ps),
free
wal
king
trai
ning
12w
eeks
(1x/
wor
1x/m
)Q
uadr
icep
sM
VC
:is
om
etri
caN
ot
repo
rted
–W
>M
(p<
0.01
)
Gre
ulic
het
al.,
2014
47
34C
OPD
:20
indi
vidu
aliz
edtr
aini
ng(I
T),
14no
n-in
divi
dual
ized
trai
ning
(NIT
)
IT:6
2(2
0);
NIT
:68
(20)
IT:6
5(9
);N
IT:6
6(9
)R
CT
IT:2
x3
min
utes
cycl
ing
atR
PE13
,3se
tsof25
reps
thig
hm
uscl
es,
late
ralh
ipan
dtr
unk
stab
ilize
rs,
ante
rior
shoul
der
mus
cles
,ro
tato
rcu
ffm
uscl
es,u
pper
extr
emitie
sm
uscl
es,d
ors
altr
unk
and
scap
ular
stab
ilize
rat
30%
ofm
axim
alm
uscl
est
reng
th(p
rogr
esse
dto
2–6
sets
of8–
15re
psat
40–7
0%of1
RM
)
NIT
:wal
king
and
clim
bing
stai
rs,b
all
gam
es,r
esis
tanc
etr
aini
ngw
ith
dum
bbel
lsan
del
astic
tube
s(int
ensi
tyis
patien
tre
gula
ted)
12w
eeks
(1x/
w)
CSA
m.r
ectu
sfe
mori
s(u
ltra
soun
d)IT
(p¼
0.04
9)ns
NIT
"8.6
% –ns
betw
een
group
s
(con
tinue
d)
16
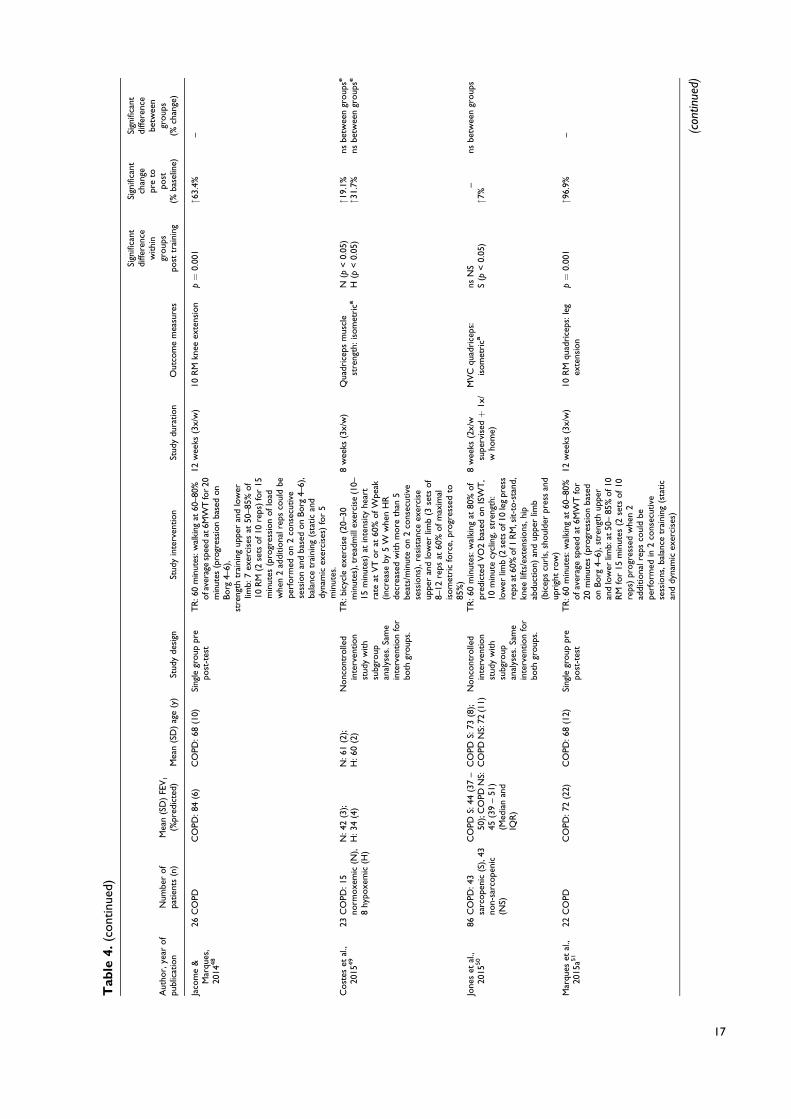
Tab
le4.
(cont
inue
d)
Aut
hor,
year
of
publ
icat
ion
Num
ber
of
patien
ts(n
)M
ean
(SD
)FE
V1
(%pr
edic
ted)
Mea
n(S
D)
age
(y)
Stud
yde
sign
Stud
yin
terv
ention
Stud
ydu
ration
Out
com
em
easu
res
Sign
ifica
ntdi
ffere
nce
withi
ngr
oup
spo
sttr
aini
ng
Sign
ifica
ntch
ange
pre
topo
st(%
base
line)
Sign
ifica
ntdi
ffere
nce
betw
een
group
s(%
chan
ge)
Jaco
me
&M
arqu
es,
2014
48
26C
OPD
CO
PD:84
(6)
CO
PD:68
(10)
Sing
legr
oup
pre
post
-tes
tT
R:6
0m
inut
es:w
alki
ngat
60–8
0%ofa
vera
gesp
eed
at6M
WT
for
20m
inut
es(p
rogr
essi
on
base
don
Borg
4–6)
,st
reng
thtr
aini
ngup
per
and
low
erlim
b:7
exer
cise
sat
50–8
5%of
10R
M(2
sets
of1
0re
ps)
for
15m
inut
es(p
rogr
essi
on
oflo
adw
hen
2ad
ditiona
lrep
sco
uld
bepe
rform
edon
2co
nsec
utiv
ese
ssio
nan
dba
sed
on
Borg
4–6)
,ba
lanc
etr
aini
ng(s
tatic
and
dyna
mic
exer
cise
s)fo
r5
min
utes
.
12w
eeks
(3x/
w)
10R
Mkn
eeex
tens
ion
p¼
0.00
1"6
3.4%
–
Cost
eset
al.,
2015
49
23C
OPD
:15
norm
oxe
mic
(N),
8hy
poxe
mic
(H)
N:4
2(3
);H
:34
(4)
N:6
1(2
);H
:60
(2)
Nonc
ont
rolle
din
terv
ention
stud
yw
ith
subg
roup
anal
yses
.Sam
ein
terv
ention
for
both
group
s.
TR
:bic
ycle
exer
cise
(20–
30m
inut
es),
trea
dmill
exer
cise
(10–
15m
inut
es)
atin
tens
ity
hear
tra
teat
VT
or
at60
%ofW
peak
(inc
reas
eby
5W
whe
nH
Rde
crea
sed
with
more
than
5be
ats/
min
ute
on
2co
nsec
utiv
ese
ssio
ns),
resi
stan
ceex
erci
seup
per
and
low
erlim
b(3
sets
of
8–12
reps
at60
%ofm
axim
alis
om
etri
cfo
rce,
progr
esse
dto
85%
)
8w
eeks
(3x/
w)
Qua
dric
eps
mus
cle
stre
ngth
:is
om
etri
caN
(p<
0.05
)H
(p<
0.05
)"1
9.1%
"31.
7%ns
betw
een
group
se
nsbe
twee
ngr
oup
se
Jone
set
al.,
2015
50
86C
OPD
:43
sarc
ope
nic
(S),
43no
n-sa
rcope
nic
(NS)
CO
PDS:
44(3
7–
50);
CO
PDN
S:45
(39
–51
)(M
edia
nan
dIQ
R)
CO
PDS:
73(8
);C
OPD
NS:
72(1
1)N
onc
ont
rolle
din
terv
ention
stud
yw
ith
subg
roup
anal
yses
.Sam
ein
terv
ention
for
both
group
s.
TR
:60
min
utes
:wal
king
at80
%of
pred
icte
dV
O2
base
don
ISW
T,
10m
inut
ecy
clin
g,st
reng
th:
low
erlim
b(2
sets
of1
0le
gpr
ess
reps
at60
%of1
RM
,sit-t
o-s
tand
,kn
eelif
ts/e
xten
sions
,hi
pab
duct
ion)
and
uppe
rlim
b(b
icep
scu
rls,
shoul
der
pres
san
dup
righ
tro
w)
8w
eeks
(2x/
wsu
perv
isedþ
1x/
who
me)
MV
Cqu
adri
ceps
:is
om
etri
cans
NS
S(p
<0.
05)
–"7
%ns
betw
een
group
s
Mar
ques
etal
.,20
15a5
122
CO
PDC
OPD
:72
(22)
CO
PD:68
(12)
Sing
legr
oup
pre
post
-tes
tT
R:6
0m
inut
es:w
alki
ngat
60–8
0%ofav
erag
esp
eed
at6M
WT
for
20m
inut
es(p
rogr
essi
on
base
don
Borg
4–6)
,st
reng
thup
per
and
low
erlim
b:at
50–
85%
of1
0R
Mfo
r15
min
utes
(2se
tsof10
reps
)pr
ogr
esse
dw
hen
2ad
ditiona
lrep
sco
uld
bepe
rform
edin
2co
nsec
utiv
ese
ssio
ns,b
alan
cetr
aini
ng(s
tatic
and
dyna
mic
exer
cise
s)
12w
eeks
(3x/
w)
10R
Mqu
adri
ceps
:le
gex
tens
ion
p¼
0.00
1"9
6.9%
– (con
tinue
d)
17

Tab
le4.
(cont
inue
d)
Aut
hor,
year
of
publ
icat
ion
Num
ber
of
patien
ts(n
)M
ean
(SD
)FE
V1
(%pr
edic
ted)
Mea
n(S
D)
age
(y)
Stud
yde
sign
Stud
yin
terv
ention
Stud
ydu
ration
Out
com
em
easu
res
Sign
ifica
ntdi
ffere
nce
withi
ngr
oup
spo
sttr
aini
ng
Sign
ifica
ntch
ange
pre
topo
st(%
base
line)
Sign
ifica
ntdi
ffere
nce
betw
een
group
s(%
chan
ge)
Mar
ques
etal
.,20
15b5
29
CO
PDC
OPD
:69
(25)
CO
PD:70
(8)
Sing
legr
oup
pre
post
-tes
tT
R:6
0m
inut
es:2
0m
inut
esw
alki
ngat
60–8
0%ofav
erag
esp
eed
at6W
MT
,res
ista
nce
trai
ning
:15
min
utes
ofe
last
icba
nds
and
free
wei
ghts
(7ex
erci
ses
uppe
ran
dlo
wer
limbs
,2
sets
of10
reps
at50
–85%
of10
RM
),5
min
utes
bala
nce
trai
ning
12w
eeks
(3x/
w)
10R
Mqu
adri
ceps
:le
gex
tens
ion
p¼
0.00
2"9
1.2%
–
Poth
irat
etal
.,20
1553
30C
OPD
CO
PD:45
(11)
CO
PD:69
(9)
Sing
legr
oup
pre
post
-tes
tT
R:3
5–40
min
ute:
3se
tsat
100%
of
10R
Mofup
per
and
low
erlim
bs(n
otsp
ecifi
ed)u
sing
wei
ghtlif
ting
and
resi
stiv
elo
adin
g(p
rogr
esse
dw
ith
10re
psan
d2
sets
),w
alki
ngat
40–4
5%ofhe
art
rate
rese
rve
witho
utex
ceed
ing
Borg
6fo
r15
–20
min
utes
progr
esse
dup
to35
–40
min
.
8w
eeks
(2x/
w)
10R
Mqu
adri
ceps
p<
0.00
1"7
1.0%
–
ns:n
otsi
gnifi
cant
;RC
T:r
ando
miz
edco
ntro
lled
tria
l;R
M:r
epet
itio
nm
axim
um;F
EV1:f
orc
edex
pire
dvo
lum
ein
1se
cond
;FFM
:fat
free
mas
s;IS
WT
;inc
rem
enta
lshu
ttle
wal
kte
st;M
VC
:max
imum
volu
ntar
yco
ntra
ctio
n;W
peak
/max
:pe
ak/m
axim
alw
ork
load
;6M
WT
:6-
min
ute
wal
king
test
;M
RI:
mag
netic
reso
nanc
eim
agin
g;A
T/V
T:an
aero
bic/
vent
ilato
ryth
resh
old
;C
SA:cr
oss
-sec
tiona
lar
ea;R
PE:r
ate
ofpe
rcei
ved
exer
tion.
a Mea
sure
dvi
ast
rain
-gau
gesy
stem
.bM
easu
red
via
com
pute
rize
ddy
nam
om
eter
,for
exam
ple,
Bio
dex.
c Mea
sure
dvi
aha
nd-h
eld
dyna
mom
eter
.dM
easu
red
via
push
ing
agai
nst
forc
epl
atfo
rm.
eBet
wee
ngr
oup
diffe
renc
eba
sed
on
post
trai
ning
valu
e.f O
nly
abso
lute
valu
esav
aila
ble.
g Dat
ano
tre
port
ed.
18
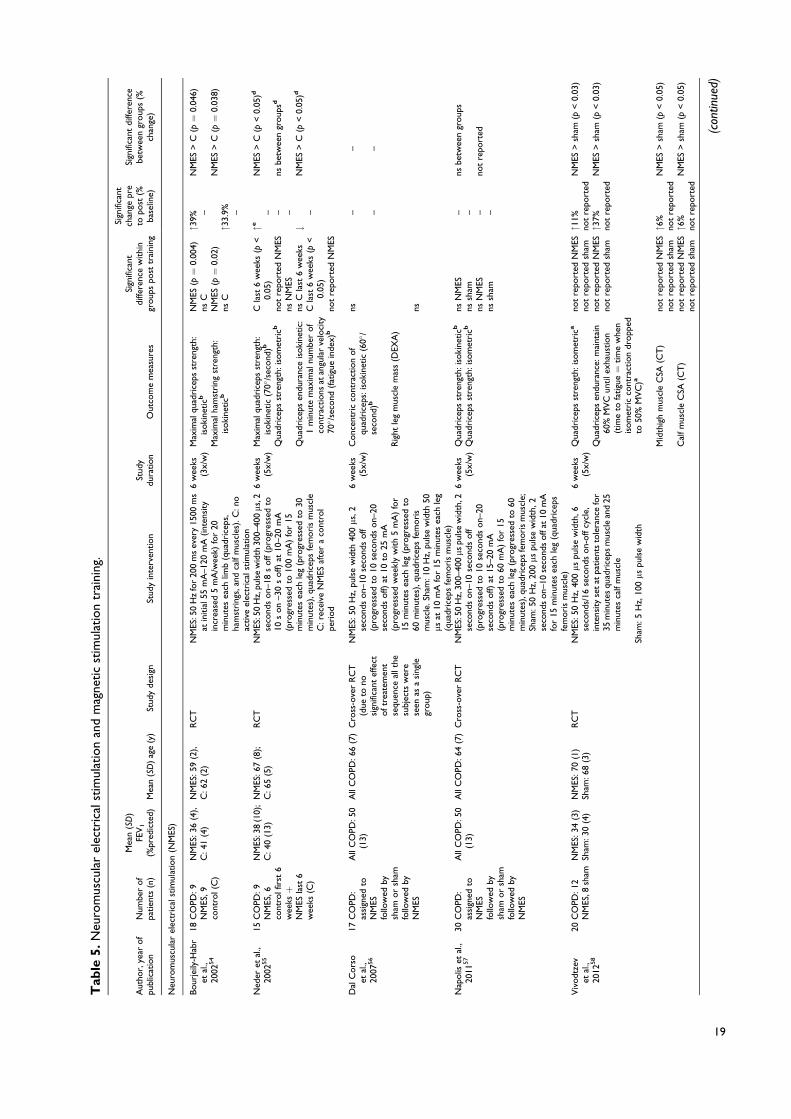
Tab
le5.
Neu
rom
uscu
lar
elec
tric
alst
imul
atio
nan
dm
agne
tic
stim
ulat
ion
trai
ning
.
Aut
hor,
year
of
publ
icat
ion
Num
ber
of
patien
ts(n
)
Mea
n(S
D)
FEV
1
(%pr
edic
ted)
Mea
n(S
D)
age
(y)
Stud
yde
sign
Stud
yin
terv
ention
Stud
ydu
ration
Out
com
em
easu
res
Sign
ifica
ntdi
ffere
nce
withi
ngr
oup
spo
sttr
aini
ng
Sign
ifica
ntch
ange
pre
topo
st(%
base
line)
Sign
ifica
ntdi
ffere
nce
betw
een
group
s(%
chan
ge)
Neu
rom
uscu
lar
elec
tric
alst
imul
atio
n(N
MES
)
Bour
jeily
-Hab
ret
al.,
2002
54
18C
OPD
:9
NM
ES,9
cont
rol(
C)
NM
ES:3
6(4
),C
:41
(4)
NM
ES:5
9(2
),C
:62
(2)
RC
TN
MES
:50
Hz
for
200
ms
ever
y15
00m
sat
initia
l55
mA
–120
mA
(int
ensi
tyin
crea
sed
5m
A/w
eek)
for
20m
inut
esea
chlim
b(q
uadr
icep
s,ha
mst
ring
s,an
dca
lfm
uscl
es).
C:n
oac
tive
elec
tric
alst
imul
atio
n
6w
eeks
(3x/
w)
Max
imal
quad
rice
psst
reng
th:
isoki
neticb
Max
imal
ham
stri
ngst
reng
th:
isoki
neticb
NM
ES(p¼
0.00
4)ns
CN
MES
(p¼
0.02
)ns
C
"39%
–
"33.
9% –
NM
ES>
C(p¼
0.04
6)
NM
ES>
C(p¼
0.03
8)
Ned
eret
al.,
2002
55
15C
OPD
:9
NM
ES,6
cont
rolf
irst
6w
eeksþ
NM
ESla
st6
wee
ks(C
)
NM
ES:3
8(1
0);
C:4
0(1
3)N
MES
:67
(8);
C:6
5(5
)R
CT
NM
ES:5
0H
z,pu
lse
wid
th30
0–40
0ms
,2se
cond
son–
18s
off
(pro
gres
sed
to10
son
–30
soff)
at10
–20
mA
(pro
gres
sed
to10
0m
A)
for
15m
inut
esea
chle
g(p
rogr
esse
dto
30m
inut
es),
quad
rice
psfe
mori
sm
uscl
eC
:rec
eive
NM
ESaf
ter
aco
ntro
lpe
riod
6w
eeks
(5x/
w)
Max
imal
quad
rice
psst
reng
th:
isoki
netic
(70(
/sec
ond
)b
Qua
dric
eps
stre
ngth
:iso
met
ricb
Qua
dric
eps
endu
ranc
eis
oki
netic:
1m
inut
em
axim
alnu
mbe
rof
cont
ract
ions
atan
gula
rve
loci
ty70( /
seco
nd(f
atig
uein
dex)
b
Cla
st6
wee
ks(p
<0.
05)
not
repo
rted
NM
ESns
NM
ESns
Cla
st6
wee
ksC
last
6w
eeks
(p<
0.05
)no
tre
port
edN
MES
"e– – –
#–
NM
ES>
C(p
<0.
05)d
nsbe
twee
ngr
oup
sd
NM
ES>
C(p
<0.
05)d
Dal
Cors
oet
al.,
2007
56
17C
OPD
:as
sign
edto
NM
ESfo
llow
edby
sham
or
sham
follo
wed
byN
MES
All
CO
PD:5
0(1
3)A
llC
OPD
:66
(7)
Cro
ss-o
ver
RC
T(d
ueto
nosi
gnifi
cant
effe
ctoftr
eate
men
tse
quen
ceal
lth
esu
bjec
tsw
ere
seen
asa
sing
legr
oup
)
NM
ES:5
0H
z,pu
lse
wid
th40
0ms
,2se
cond
son–
10se
cond
soff
(pro
gres
sed
to10
seco
nds
on–
20se
cond
soff)
at10
to25
mA
(pro
gres
sed
wee
kly
with
5m
A)
for
15m
inut
esea
chle
g(p
rogr
esse
dto
60m
inut
es),
quad
rice
psfe
mori
sm
uscl
e.Sh
am:1
0H
z,pu
lse
wid
th50
msat
10m
Afo
r15
min
utes
each
leg
(qua
dric
eps
fem
ori
sm
uscl
e)
6w
eeks
(5x/
w)
Conc
entr
icco
ntra
ctio
nof
quad
rice
ps:i
soki
netic
(60(
/se
cond
)b
Rig
htle
gm
uscl
em
ass
(DEX
A)
ns ns
– –
– –
Nap
olis
etal
.,20
1157
30C
OPD
:as
sign
edto
NM
ESfo
llow
edby
sham
or
sham
follo
wed
byN
MES
All
CO
PD:5
0(1
3)A
llC
OPD
:64
(7)
Cro
ss-o
ver
RC
TN
MES
:50
Hz,
300–
400ms
puls
ew
idth
,2se
cond
son–
10se
cond
soff
(pro
gres
sed
to10
seco
nds
on–
20se
cond
soff)
at15
–20
mA
(pro
gres
sed
to60
mA
)fo
r15
min
utes
each
leg
(pro
gres
sed
to60
min
utes
),qu
adri
ceps
fem
ori
sm
uscl
e;Sh
am:5
0H
z,20
0ms
puls
ew
idth
,2
seco
nds
on–
10se
cond
soff
at10
mA
for
15m
inut
esea
chle
g(q
uadr
icep
sfe
mori
sm
uscl
e)
6w
eeks
(5x/
w)
Qua
dric
eps
stre
ngth
:iso
kine
ticb
Qua
dric
eps
stre
ngth
:iso
met
ricb
nsN
MES
nssh
amns
NM
ESns
sham
– – – –
nsbe
twee
ngr
oup
s
not
repo
rted
Viv
odt
zev
etal
.,20
1258
20C
OPD
:12
NM
ES,8
sham
NM
ES:3
4(3
)Sh
am:3
0(4
)N
MES
:70
(1)
Sham
:68
(3)
RC
TN
MES
:50
Hz,
400ms
puls
ew
idth
,6se
cond
s/16
seco
nds
on-
off
cycl
e,in
tens
ity
set
atpa
tien
tsto
lera
nce
for
35m
inut
esqu
adri
ceps
mus
cle
and
25m
inut
esca
lfm
uscl
e
Sham
:5H
z,10
0ms
puls
ew
idth
6w
eeks
(5x/
w)
Qua
dric
eps
stre
ngth
:iso
met
rica
Qua
dric
eps
endu
ranc
e:m
aint
ain
60%
MV
Cun
tile
xhau
stio
n(t
ime
tofa
tigu
e¼
tim
ew
hen
isom
etri
cco
ntra
ctio
ndr
opp
edto
50%
MV
C)a
Mid
thig
hm
uscl
eC
SA(C
T)
Cal
fm
uscl
eC
SA(C
T)
not
repo
rted
NM
ESno
tre
port
edsh
amno
tre
port
edN
MES
not
repo
rted
sham
not
repo
rted
NM
ESno
tre
port
edsh
amno
tre
port
edN
MES
not
repo
rted
sham
"11%
not
repo
rted
"37%
not
repo
rted
"6%
not
repo
rted
"6%
not
repo
rted
NM
ES>
sham
(p<
0.03
)
NM
ES>
sham
(p<
0.03
)
NM
ES>
sham
(p<
0.05
)
NM
ES>
sham
(p<
0.05
)
(con
tinue
d)
19
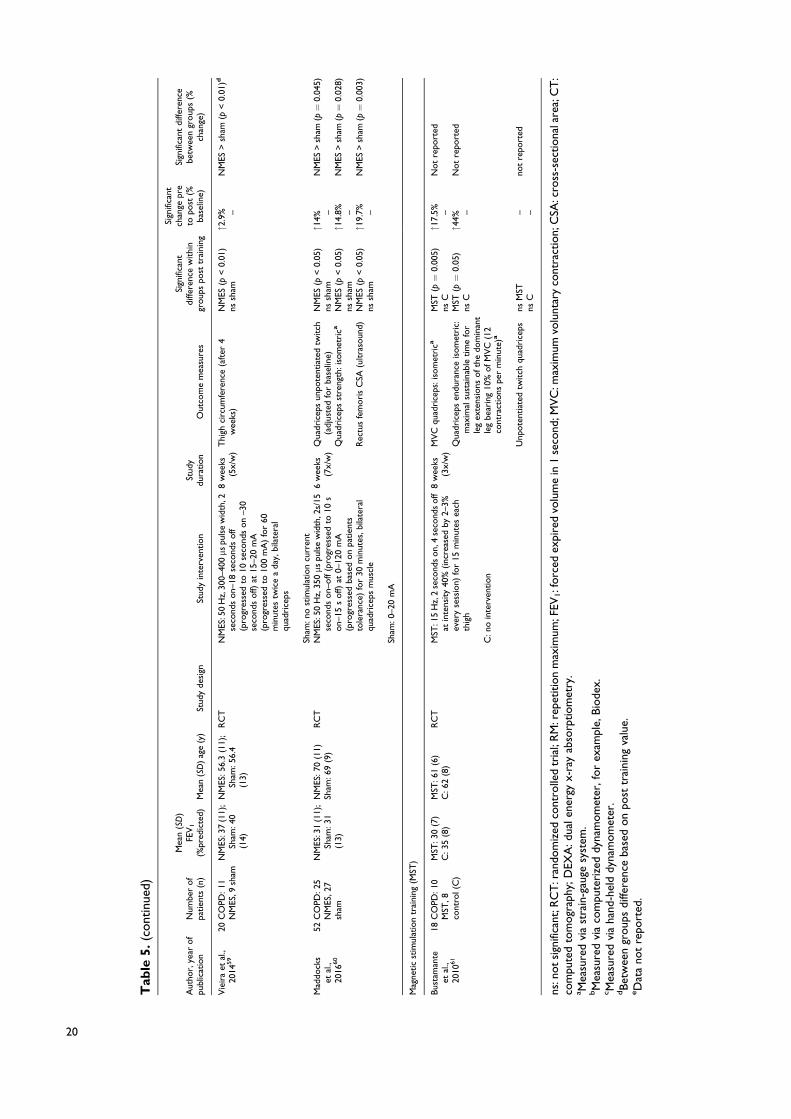
Tab
le5.
(cont
inue
d)
Aut
hor,
year
of
publ
icat
ion
Num
ber
of
patien
ts(n
)
Mea
n(S
D)
FEV
1
(%pr
edic
ted)
Mea
n(S
D)
age
(y)
Stud
yde
sign
Stud
yin
terv
ention
Stud
ydu
ration
Out
com
em
easu
res
Sign
ifica
ntdi
ffere
nce
withi
ngr
oup
spo
sttr
aini
ng
Sign
ifica
ntch
ange
pre
topo
st(%
base
line)
Sign
ifica
ntdi
ffere
nce
betw
een
group
s(%
chan
ge)
Vie
ira
etal
.,20
1459
20C
OPD
:11
NM
ES,9
sham
NM
ES:3
7(1
1);
Sham
:40
(14)
NM
ES:5
6.3
(11)
;Sh
am:5
6.4
(13)
RC
TN
MES
:50
Hz,
300–
400ms
puls
ew
idth
,2se
cond
son–
18se
cond
soff
(pro
gres
sed
to10
seco
nds
on
–30
seco
nds
off)
at15
–20
mA
(pro
gres
sed
to10
0m
A)
for
60m
inut
estw
ice
ada
y,bi
late
ral
quad
rice
ps
Sham
:no
stim
ulat
ion
curr
ent
8w
eeks
(5x/
w)
Thi
ghci
rcum
fere
nce
(aft
er4
wee
ks)
NM
ES(p
<0.
01)
nssh
am"2
.9% –
NM
ES>
sham
(p<
0.01
)d
Mad
dock
set
al.,
2016
60
52C
OPD
:25
NM
ES,2
7sh
am
NM
ES:3
1(1
1);
Sham
:31
(13)
NM
ES:7
0(1
1)Sh
am:6
9(9
)R
CT
NM
ES:5
0H
z,35
0ms
puls
ew
idth
,2s/
15se
cond
son–
off
(pro
gres
sed
to10
son–
15s
off)
at0–
120
mA
(pro
gres
sed
base
don
patien
tsto
lera
nce)
for
30m
inut
es,b
ilate
ral
quad
rice
psm
uscl
e
Sham
:0–2
0m
A
6w
eeks
(7x/
w)
Qua
dric
eps
unpo
tent
iate
dtw
itch
(adj
uste
dfo
rba
selin
e)Q
uadr
icep
sst
reng
th:i
som
etri
ca
Rec
tus
fem
ori
sC
SA(u
ltra
soun
d)
NM
ES(p
<0.
05)
nssh
amN
MES
(p<
0.05
)ns
sham
NM
ES(p
<0.
05)
nssh
am
"14%
–"1
4.8% –
"19.
7% –
NM
ES>
sham
(p¼
0.04
5)
NM
ES>
sham
(p¼
0.02
8)
NM
ES>
sham
(p¼
0.00
3)
Mag
netic
stim
ulat
ion
trai
ning
(MST
)
Bus
tam
ante
etal
.,20
1061
18C
OPD
:10
MST
,8co
ntro
l(C
)
MST
:30
(7)
C:3
5(8
)M
ST:6
1(6
)C
:62
(8)
RC
TM
ST:1
5H
z,2
seco
nds
on,
4se
cond
soff
atin
tens
ity
40%
(inc
reas
edby
2–3%
ever
yse
ssio
n)fo
r15
min
utes
each
thig
h
C:n
oin
terv
ention
8w
eeks
(3x/
w)
MV
Cqu
adri
ceps
:iso
met
rica
Qua
dric
eps
endu
ranc
eis
om
etri
c:m
axim
alsu
stai
nabl
etim
efo
rle
gex
tens
ions
ofth
edo
min
ant
leg
bear
ing
10%
ofM
VC
(12
cont
ract
ions
per
min
ute)
a
Unp
ote
ntia
ted
twitch
quad
rice
ps
MST
(p¼
0.00
5)ns
CM
ST(p¼
0.05
)ns
C
nsM
STns
C
"17.
5% –"4
4%– – –
Not
repo
rted
Not
repo
rted
not
repo
rted
ns:n
ot
sign
ifica
nt;R
CT
:ran
dom
ized
cont
rolle
dtr
ial;
RM
:rep
etitio
nm
axim
um;F
EV1:f
orc
edex
pire
dvo
lum
ein
1se
cond
;MV
C:m
axim
umvo
lunt
ary
cont
ract
ion;
CSA
:cro
ss-s
ectiona
lare
a;C
T:
com
pute
dto
mogr
aphy
;DEX
A:d
uale
nerg
yx-
ray
abso
rptiom
etry
.a M
easu
red
via
stra
in-g
auge
syst
em.
bM
easu
red
via
com
pute
rize
ddy
nam
om
eter
,fo
rex
ampl
e,Bio
dex.
c Mea
sure
dvi
aha
nd-h
eld
dyna
mom
eter
.dBet
wee
ngr
oup
sdi
ffere
nce
base
don
post
trai
ning
valu
e.eD
ata
not
repo
rted
.
20

Tab
le6.
Oth
ertr
aini
ngm
oda
litie
s.
Aut
hor,
year
ofpu
blic
atio
nN
umbe
rof
patien
ts(n
)M
ean
(SD
)FE
V1
(%pr
edic
ted)
Mea
n(S
D)
age
(y)
Stud
yde
sign
Stud
yin
terv
ention
Stud
ydu
ration
Out
com
em
easu
res
Sign
ifica
ntdi
ffere
nce
withi
ngr
oup
spo
sttr
aini
ng
Sign
ifica
ntch
ange
pre
topo
st(%
base
line)
Sign
ifica
ntdi
ffere
nce
betw
een
group
s(%
chan
ge)
Hig
h-in
tens
ity
inte
rval
trai
ning
(HIIT
)
Bro
nsta
det
al.,
2012
62
7C
OPD
5he
alth
y,ag
e-m
atch
edco
ntro
ls(H
C)
CO
PD:4
6(1
0);
HC
:93
(14)
CO
PD:6
8(7
);H
C:7
0(5
)Si
ngle
group
pre
post
-tes
t(H
Conl
yba
selin
e)
Kne
e-ex
tens
or
proto
col:
5m
inut
esw
arm
upw
itho
utlo
ad,4
inte
rval
sof4
min
utes
at90
%ofpe
akW
R,2
min
utes
active
unlo
aded
kick
ing
(60
kick
sa
min
ute)
.Leg
str
aine
dse
para
tely
.
6w
eeks
(3x/
w)
Qua
dric
eps
endu
ranc
e:pe
akw
ork
e
Qua
dric
eps
mus
cle
mas
s(M
RI)
p<
0.00
1
ns
"37%
–
– –
Who
le-b
ody
vibr
atio
ntr
aini
ng
Pleg
uezu
elos
etal
.,20
1363
51C
OPD
:26
who
lebo
dyvi
brat
ion
trai
ning
(WB
VT
),25
cont
rol(
C)
WB
VT
:37
(12)
;C
:32
(7)
WB
VT
:68
(9);
C:7
1(8
)R
CT
WB
VT
:squ
atting
posi
tion
(30(
hip
flexi
on,
55(
knee
flexi
on)
,6se
ries
of4
x30
-sre
petitions
atfr
eque
ncy
35H
zan
dam
plitud
e2
mm
with
60se
cond
sre
stin
betw
een
sets
.Int
ensi
tyse
tvi
aB
org
scal
e.
6w
eeks
(3x/
w)
Rig
htle
g:is
oki
netic
knee
exte
nsio
n(6
0(/s
)b
Rig
htle
g:is
oki
netic
knee
exte
nsio
n(1
80( /
s)b
Rig
htle
g:is
oki
netic
knee
flexi
on
(60(
/s)b
Rig
htle
g:is
oki
netic
knee
flexi
on
(180( /
s)b
Left
leg:
isoki
netic
knee
exte
nsio
n(6
0(/s
)b
Left
leg:
isoki
netic
knee
exte
nsio
n(1
80( /
s)b
Left
leg:
isoki
netic
knee
flexi
on
(60(
/s)b
Left
leg:
isoki
netic
knee
flexi
on
(180( /
s)b
nsbo
thgr
oup
s
nsbo
thgr
oup
s
nsbo
thgr
oup
s
nsbo
thgr
oup
s
nsbo
thgr
oup
s
nsbo
thgr
oup
s
nsbo
thgr
oup
s
nsbo
thgr
oup
s
– – – – – – – –
nsbe
twee
ngr
oup
s
nsbe
twee
ngr
oup
s
nsbe
twee
ngr
oup
s
nsbe
twee
ngr
oup
s
nsbe
twee
ngr
oup
s
nsbe
twee
ngr
oup
s
nsbe
twee
ngr
oup
s
nsbe
twee
ngr
oup
s
Salh
iet
al.,
2015
64
51C
OPD
:26
who
le-
body
vibr
atio
ntr
aini
ng(W
BV
T),
25re
sist
ance
trai
ning
(RT
)
WB
VT
:38
(28–
45);
RT
:39
(29–
45)
(Med
ian
and
IQR
)
WB
VT
:58
(55–
73)
RT
:63
(57–
68)
(Med
ian
and
IQR
)
RC
TW
BV
T:2
7hz
,pea
k-to
-pea
kam
p(2
mm
),30
seco
nds–
1m
inut
e,re
ps1–
3,4
low
erbo
dyex
(hig
hsq
uat,
deep
squa
t,w
ide-
stan
cesq
uat
and
lung
e),4
uppe
rbo
dyex
(fro
ntra
ise,
bent
ove
rla
tera
l,bi
ceps
curl
and
cross
-ove
r)þ
15m
inut
esae
robi
cex
erci
seR
T:3
sets
of10
reps
quad
rice
ps,
ham
stri
ngs,
deltoid
,bic
eps
brac
hii,
tric
eps
brac
hii,
pect
ora
lmus
cles
at70
%of1
RM
(pro
gres
sed
base
don
Borg
4-6)þ
15m
inut
esae
robi
cex
erci
se(A
fter
6w:d
ynam
icst
reng
thex
erci
ses)
12w
eeks
(3x/
w)
Kne
eex
tens
ion
stre
ngth
:is
om
etri
ccns
WB
VT
RT
(p¼
0.00
9)–
10.5
%ns
betw
een
group
se
(con
tinue
d)
21
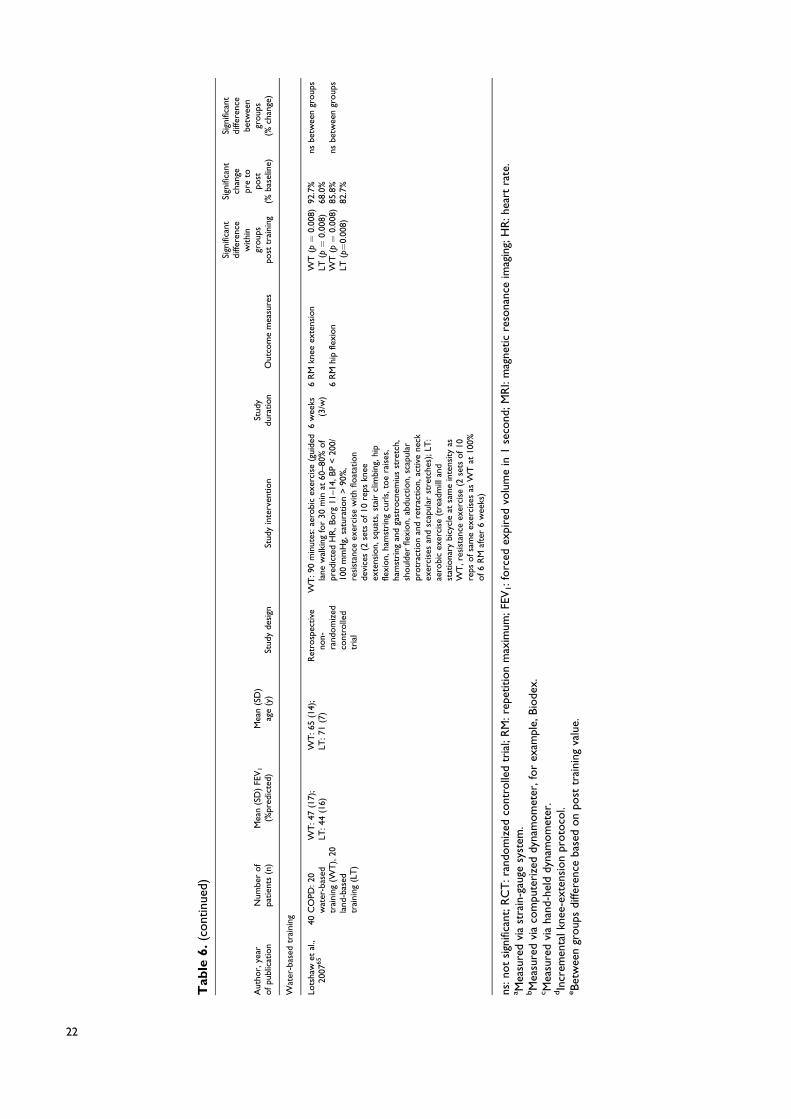
Tab
le6.
(cont
inue
d)
Aut
hor,
year
ofpu
blic
atio
nN
umbe
rof
patien
ts(n
)M
ean
(SD
)FE
V1
(%pr
edic
ted)
Mea
n(S
D)
age
(y)
Stud
yde
sign
Stud
yin
terv
ention
Stud
ydu
ration
Out
com
em
easu
res
Sign
ifica
ntdi
ffere
nce
withi
ngr
oup
spo
sttr
aini
ng
Sign
ifica
ntch
ange
pre
topo
st(%
base
line)
Sign
ifica
ntdi
ffere
nce
betw
een
group
s(%
chan
ge)
Wat
er-b
ased
trai
ning
Lots
haw
etal
.,20
0765
40C
OPD
:20
wat
er-b
ased
trai
ning
(WT
),20
land
-bas
edtr
aini
ng(L
T)
WT
:47
(17)
;LT
:44
(16)
WT
:65
(14)
;LT
:71
(7)
Ret
rosp
ective
non-
rand
om
ized
cont
rolle
dtr
ial
WT
:90
min
utes
:aer
obi
cex
erci
se(g
uide
dla
new
alki
ngfo
r30
min
at60
–80%
of
pred
icte
dH
R,B
org
11–1
4,B
P<
200/
100
mm
Hg,
satu
ration
>90
%,
resi
stan
ceex
erci
sew
ith
float
atio
nde
vice
s(2
sets
of10
reps
knee
exte
nsio
n,sq
uats
,st
air
clim
bing
,hip
flexi
on,
ham
stri
ngcu
rls,
toe
rais
es,
ham
stri
ngan
dga
stro
cnem
ius
stre
tch,
shoul
der
flexi
on,
abdu
ctio
n,sc
apul
arpr
otr
action
and
retr
action,
active
neck
exer
cise
san
dsc
apul
arst
retc
hes)
;LT
:ae
robi
cex
erci
se(t
read
mill
and
stat
iona
rybi
cycl
eat
sam
ein
tens
ity
asW
T,r
esis
tanc
eex
erci
se(2
sets
of10
reps
ofsa
me
exer
cise
sas
WT
at10
0%of6
RM
afte
r6
wee
ks)
6w
eeks
(3/w
)6
RM
knee
exte
nsio
n
6R
Mhi
pfle
xion
WT
(p¼
0.00
8)LT
(p¼
0.00
8)W
T(p¼
0.00
8)LT
(p¼
0.00
8)
92.7
%68
.0%
85.8
%82
.7%
nsbe
twee
ngr
oup
s
nsbe
twee
ngr
oup
s
ns:n
ot
sign
ifica
nt;R
CT
:ran
dom
ized
cont
rolle
dtr
ial;
RM
:rep
etitio
nm
axim
um;F
EV1:f
orc
edex
pire
dvo
lum
ein
1se
cond
;MR
I:m
agne
tic
reso
nanc
eim
agin
g;H
R:h
eart
rate
.a M
easu
red
via
stra
in-g
auge
syst
em.
bM
easu
red
via
com
pute
rize
ddy
nam
om
eter
,fo
rex
ampl
e,Bio
dex.
c Mea
sure
dvi
aha
nd-h
eld
dyna
mom
eter
.dIn
crem
enta
lkne
e-ex
tens
ion
proto
col.
eBet
wee
ngr
oup
sdi
ffere
nce
base
don
post
trai
ning
valu
e.
22
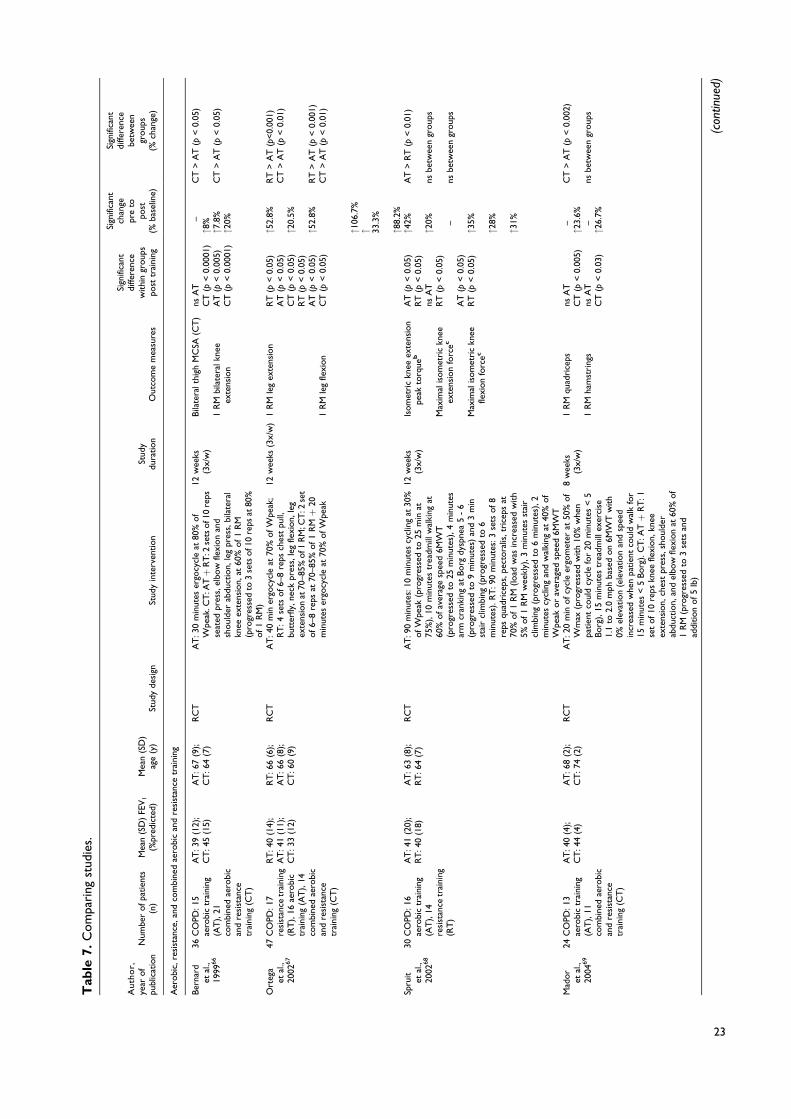
Tab
le7.
Com
pari
ngst
udie
s.
Auth
or,
year
of
publ
icat
ion
Num
ber
ofpa
tien
ts(n
)M
ean
(SD
)FE
V1
(%pr
edic
ted)
Mea
n(S
D)
age
(y)
Stud
yde
sign
Stud
yin
terv
ention
Stud
ydu
ration
Out
com
em
easu
res
Sign
ifica
ntdi
ffere
nce
withi
ngr
oup
spo
sttr
aini
ng
Sign
ifica
ntch
ange
pre
topo
st(%
base
line)
Sign
ifica
ntdi
ffere
nce
betw
een
group
s(%
chan
ge)
Aer
obi
c,re
sist
ance
,and
com
bine
dae
robi
can
dre
sist
ance
trai
ning
Ber
nard
etal
.,19
9966
36C
OPD
:15
aero
bic
trai
ning
(AT
),21
com
bine
dae
robi
can
dre
sist
ance
trai
ning
(CT
)
AT
:39
(12)
;C
T:4
5(1
5)A
T:6
7(9
);C
T:6
4(7
)R
CT
AT
:30
min
utes
ergo
cycl
eat
80%
of
Wpe
ak.C
T:A
Tþ
RT
:2se
tsof1
0re
psse
ated
pres
s,el
bow
flexi
on
and
shoul
der
abdu
ctio
n,le
gpr
ess,
bila
tera
lkn
eeex
tens
ion,
at60
%of1
RM
(pro
gres
sed
to3
sets
of1
0re
psat
80%
of1
RM
)
12w
eeks
(3x/
w)
Bila
tera
lthi
ghM
CSA
(CT
)
1R
Mbi
late
ralk
nee
exte
nsio
n
nsA
TC
T(p
<0.
0001
)A
T(p
<0.
005)
CT
(p<
0.00
01)
–"8
%"7
.8%
"20%
CT
>A
T(p
<0.
05)
CT
>A
T(p
<0.
05)
Ort
ega
etal
.,20
0267
47C
OPD
:17
resi
stan
cetr
aini
ng(R
T),
16ae
robi
ctr
aini
ng(A
T),
14co
mbi
ned
aero
bic
and
resi
stan
cetr
aini
ng(C
T)
RT
:40
(14)
;A
T:4
1(1
1);
CT
:33
(12)
RT
:66
(6);
AT
:66
(8);
CT
:60
(9)
RC
TA
T:4
0m
iner
gocy
cle
at70
%ofW
peak
;R
T:4
sets
of6–
8re
psch
est
pull,
butt
erfly
,nec
kpr
ess,
leg
flexi
on,
leg
exte
nsio
nat
70–8
5%of1
RM
;CT
:2se
tof6–
8re
psat
70–8
5%of1
RMþ
20m
inut
eser
gocy
cle
at70
%ofW
peak
12w
eeks
(3x/
w)
1R
Mle
gex
tens
ion
1R
Mle
gfle
xion
RT
(p<
0.05
)A
T(p
<0.
05)
CT
(p<
0.05
)R
T(p
<0.
05)
AT
(p<
0.05
)C
T(p
<0.
05)
"52.
8%
"20.
5%
"52.
8%
"106
.7%
" 33.3
%
"88.
2%
RT
>A
T(p
<0.
001)
CT
>A
T(p
<0.
01)
RT
>A
T(p
<0.
001)
CT
>A
T(p
<0.
01)
Spru
itet
al.,
2002
68
30C
OPD
:16
aero
bic
trai
ning
(AT
),14
resi
stan
cetr
aini
ng(R
T)
AT
:41
(20)
;R
T:4
0(1
8)A
T:6
3(8
);R
T:6
4(7
)R
CT
AT
:90
min
utes
:10
min
utes
cycl
ing
at30
%ofW
peak
(pro
gres
sed
to25
min
at75
%),
10m
inut
estr
eadm
illw
alki
ngat
60%
ofav
erag
esp
eed
6MW
T(p
rogr
esse
dto
25m
inut
es),
4m
inut
esar
mcr
anki
ngat
Borg
dysp
nea
5-
6(p
rogr
esse
dto
9m
inut
es)
and
3m
inst
air
clim
bing
(pro
gres
sed
to6
min
utes
).R
T:9
0m
inut
es:3
sets
of8
reps
quad
rice
ps,p
ecto
ralis
,tr
icep
sat
70%
of1
RM
(load
was
incr
ease
dw
ith
5%of1
RM
wee
kly)
,3
min
utes
stai
rcl
imbi
ng(p
rogr
esse
dto
6m
inut
es),
2m
inut
escy
clin
gan
dw
alki
ngat
40%
of
Wpe
akor
aver
aged
spee
d6M
WT
12w
eeks
(3x/
w)
Isom
etri
ckn
eeex
tens
ion
peak
torq
ueb
Max
imal
isom
etri
ckn
eeex
tens
ion
forc
ec
Max
imal
isom
etri
ckn
eefle
xion
forc
ec
AT
(p<
0.05
)R
T(p
<0.
05)
nsA
TR
T(p
<0.
05)
AT
(p<
0.05
)R
T(p
<0.
05)
"42%
"20% –
"35%
"28%
"31%
AT
>R
T(p
<0.
01)
nsbe
twee
ngr
oup
s
nsbe
twee
ngr
oup
s
Mad
or
etal
.,20
0469
24C
OPD
:13
aero
bic
trai
ning
(AT
),11
com
bine
dae
robi
can
dre
sist
ance
trai
ning
(CT
)
AT
:40
(4);
CT
:44
(4)
AT
:68
(2);
CT
:74
(2)
RC
TA
T:2
0m
inofcy
cle
ergo
met
erat
50%
of
Wm
ax(p
rogr
esse
dw
ith
10%
whe
npa
tien
tco
uld
cycl
efo
r20
min
utes
<5
Borg
),15
min
utes
trea
dmill
exer
cise
1.1
to2.
0m
phba
sed
on
6MW
Tw
ith
0%el
evat
ion
(ele
vation
and
spee
din
crea
sed
whe
npa
tien
tco
uld
wal
kfo
r15
min
utes
<5
Borg
).C
T:A
Tþ
RT
:1se
tof10
reps
knee
flexi
on,
knee
exte
nsio
n,ch
est
pres
s,sh
oul
der
abdu
ctio
n,an
del
bow
flexi
on
at60
%of
1R
M(p
rogr
esse
dto
3se
tsan
dad
dition
of5
lb)
8w
eeks
(3x/
w)
1R
Mqu
adri
ceps
1R
Mha
mst
ring
s
nsA
TC
T(p
<0.
005)
nsA
TC
T(p
<0.
03)
–"2
3.6%
–"2
6.7%
CT
>A
T(p
<0.
002)
nsbe
twee
ngr
oup
s
(con
tinue
d)
23

Tab
le7.
(cont
inue
d)
Auth
or,
year
of
publ
icat
ion
Num
ber
ofpa
tien
ts(n
)M
ean
(SD
)FE
V1
(%pr
edic
ted)
Mea
n(S
D)
age
(y)
Stud
yde
sign
Stud
yin
terv
ention
Stud
ydu
ration
Out
com
em
easu
res
Sign
ifica
ntdi
ffere
nce
withi
ngr
oup
spo
sttr
aini
ng
Sign
ifica
ntch
ange
pre
topo
st(%
base
line)
Sign
ifica
ntdi
ffere
nce
betw
een
group
s(%
chan
ge)
Pant
on
etal
.,20
0470
17C
OPD
:8
aero
bic
trai
ning
(AT
),9
com
bine
dae
robi
can
dre
sist
ance
trai
ning
(CT
)
AT
:40
(32)
;C
T:4
2(1
6)A
T:6
3(8
);C
T:6
1(7
)N
on-
rand
om
ized
cont
rolle
dtr
ial
AT
:30
min
utes
ofar
mer
gom
eter
,cyc
leer
gom
eter
,A
irdy
necy
clin
g,tr
eadm
ill,
indo
or
trac
kw
alki
ngþ
30m
inut
esch
air
aero
bics
.Eve
ryth
ing
at50
–70%
of
HR
R.C
T:A
Tþ
RT
:45–
60m
inut
es:3
sets
of10
–12
reps
leg
pres
s,ca
lfpr
ess,
seat
edle
gcu
rl,l
egex
tens
ion,
ches
tpr
ess,
pull
dow
n,sh
oul
der
pres
s,se
ated
row
,cru
nch,
back
exte
nsio
n,bi
ceps
curl
,and
tric
eps
exte
nsio
n(w
hen
12re
psco
uld
beco
mpl
eted
,re
sist
ance
was
incr
ease
d).
AT
:12
wee
ks(2
x/w
);C
T:1
2w
eeks
(4x/
w)
1R
Mle
gex
tens
ion
nsA
TC
T(p
<0.
05)
–"3
6.5%
CT
>A
T(p
<0.
05)d
Phill
ips
etal
.,20
0671
19C
OPD
,9
aero
bic
trai
ning
(AT
),10
com
bine
dae
robi
can
dre
sist
ance
trai
ning
(CT
)
AT
:33
(6);
CT
:42
(3)
AT
:70
(2);
CT
:71
(1)
RC
TA
T:2
0–
40m
inut
esar
mer
gom
eter
,tr
eadm
ill,cy
cle
and
step
per
(all
at3
MET
,RPE
<13
and
satu
ration&
90%
),lo
win
tens
ity
resi
stan
cetr
aini
ngw
ith
2or
3lb
hand
held
dum
bbel
ls(8
–10
reps
arm
curl
,lat
eral
tors
obe
nd,l
ater
alar
mra
ise,
wri
stcu
rl,s
tand
ing
tric
eps
exte
nsio
n,an
dsh
oul
der
abdu
ctio
nw
ith
arm
sfle
xed)
.Pro
gres
sion:
incr
ease
with
2–3
reps
each
sess
ion
base
don
RPE
<13
,load
incr
ease
dw
hen
patien
tco
uld
com
plet
e16
–18
reps
..C
T:A
Tþ
RT
:che
stpr
ess,
leg
pres
s,la
tpu
lldow
n,ca
ble
tric
eps
push
dow
n,ca
ble
tric
eps
curl
at50
%of1
RM
(load
incr
ease
dw
ith
5–10
%af
ter
com
plet
ion
of10
reps
)
8w
eeks
(2x/
w)
1R
Mle
gpr
ess
nsA
TC
T(p
<0.
05)
–"9
%C
T>
AT
(p<
0.05
)
Ale
xand
eret
al.,
2008
72
20C
OPD
:10
aero
bic
trai
ning
(AT
),10
com
bine
dae
robi
can
dre
sist
ance
trai
ning
(CT
)
AT
:39
(15)
;C
T:3
0(1
3)A
T:7
3(9
);C
T:6
5(8
)R
CT
AT
:20–
40m
inut
es:u
pper
(arm
ergo
met
er)
and
low
erlim
b(t
read
mill
,cy
cle
ergo
met
er,a
ndst
eppe
r)at
20–4
0bp
mab
ove
HR
rest
,bre
athl
essn
ess
score
1–5,
RPE
11–1
3an
d3
MET
s,up
per
arm
stre
ngth
trai
ning
atlo
win
tens
ity
usin
gha
ndhe
lddu
mbb
ells
(1se
tof8–
15re
psar
mcu
rl,l
ater
alto
rso
bend
,lat
eral
arm
rais
e,w
rist
curl
,tr
icep
sex
tens
ion,
upri
ght
row
with
1–10
lbs)
.Pr
ogr
essi
on:
dura
tion
was
incr
ease
dbe
fore
inte
nsity.
CT
:ATþ
RT
:one
set
of1
2re
psbe
nch
pres
s,le
gpr
ess,
pull
dow
n,ca
ble
tric
eps
push
dow
n,ca
ble
bice
pscu
rlat
RPE
:11
–13
and
50%
of1
RM
.Pro
gres
sion:
load
sin
crea
sed
with
3–5
lbaf
ter
com
plet
ion
>12
reps
for
2co
nsec
utiv
ese
ssio
ns
8w
eeks
(2x/
w)
1R
Mle
gpr
ess
nsbo
thgr
oup
s–
nsbe
twee
ngr
oup
s
(con
tinue
d)
24
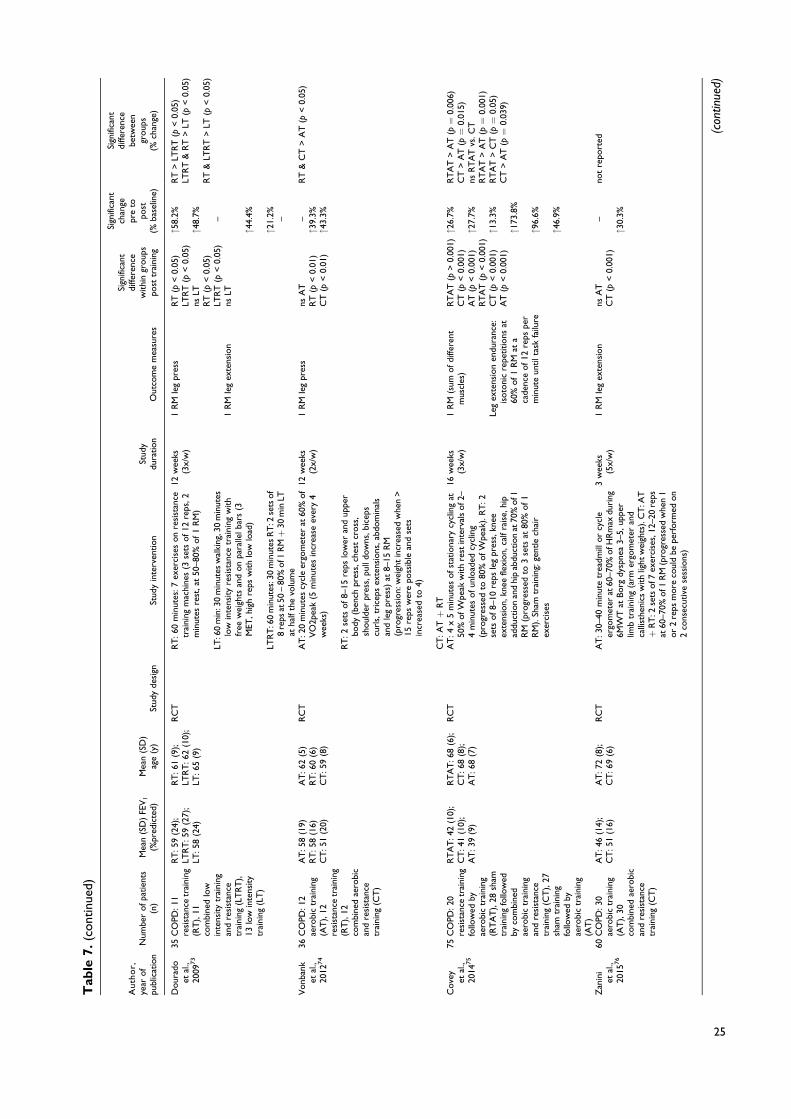
Tab
le7.
(cont
inue
d)
Auth
or,
year
of
publ
icat
ion
Num
ber
ofpa
tien
ts(n
)M
ean
(SD
)FE
V1
(%pr
edic
ted)
Mea
n(S
D)
age
(y)
Stud
yde
sign
Stud
yin
terv
ention
Stud
ydu
ration
Out
com
em
easu
res
Sign
ifica
ntdi
ffere
nce
withi
ngr
oup
spo
sttr
aini
ng
Sign
ifica
ntch
ange
pre
topo
st(%
base
line)
Sign
ifica
ntdi
ffere
nce
betw
een
group
s(%
chan
ge)
Dour
ado
etal
.,20
0973
35C
OPD
:11
resi
stan
cetr
aini
ng(R
T),
11co
mbi
ned
low
inte
nsity
trai
ning
and
resi
stan
cetr
aini
ng(L
TR
T),
13lo
win
tens
ity
trai
ning
(LT
)
RT
:59
(24)
;LT
RT
:59
(27)
;LT
:58
(24)
RT
:61
(9);
LTR
T:6
2(1
0);
LT:6
5(9
)
RC
TR
T:6
0m
inut
es:7
exer
cise
son
resi
stan
cetr
aini
ngm
achi
nes
(3se
tsof12
reps
,2m
inut
esre
st,a
t50
–80%
of1
RM
)
LT:6
0m
in:3
0m
inut
esw
alki
ng,3
0m
inut
eslo
win
tens
ity
resi
stan
cetr
aini
ngw
ith
free
wei
ghts
and
on
para
llelb
ars
(3M
ET,h
igh
reps
with
low
load
)
LTR
T:6
0m
inut
es:3
0m
inut
esR
T:2
sets
of
8re
psat
50–
80%
of1
RMþ
30m
inLT
atha
lfth
evo
lum
e
12w
eeks
(3x/
w)
1R
Mle
gpr
ess
1R
Mle
gex
tens
ion
RT
(p<
0.05
)LT
RT
(p<
0.05
)ns
LTR
T(p
<0.
05)
LTR
T(p
<0.
05)
nsLT
"58.
2%
"48.
7% –
"44.
4%
"21.
2% –
RT
>LT
RT
(p<
0.05
)LT
RT
&R
T>
LT(p
<0.
05)
RT
<
RT
>LT
(p<
0.05
)
Vonb
ank
etal
.,20
1274
36C
OPD
:12
aero
bic
trai
ning
(AT
),12
resi
stan
cetr
aini
ng(R
T),
12co
mbi
ned
aero
bic
and
resi
stan
cetr
aini
ng(C
T)
AT
:58
(19)
RT
:58
(16)
CT
:51
(20)
AT
:62
(5)
RT
:60
(6)
CT
:59
(8)
RC
TA
T:2
0m
inut
escy
cle
ergo
met
erat
60%
of
VO
2pea
k(5
min
utes
incr
ease
ever
y4
wee
ks)
RT
:2se
tsof8–
15re
pslo
wer
and
uppe
rbo
dy(b
ench
pres
s,ch
est
cross
,sh
oul
der
pres
s,pu
lldo
wns
,bic
eps
curl
s,tr
icep
sex
tens
ions
,abd
om
inal
san
dle
gpr
ess)
at8–
15R
M(p
rogr
essi
on:
wei
ght
incr
ease
dw
hen
>15
reps
wer
epo
ssib
lean
dse
tsin
crea
sed
to4)
CT
:ATþ
RT
12w
eeks
(2x/
w)
1R
Mle
gpr
ess
nsA
TR
T(p
<0.
01)
CT
(p<
0.01
)
–"3
9.3%
"43.
3%
RT
&C
T>
AT
(p<
0.05
)
Cove
yet
al.,
2014
75
75C
OPD
:20
resi
stan
cetr
aini
ngfo
llow
edby
aero
bic
trai
ning
(RT
AT
),28
sham
trai
ning
follo
wed
byco
mbi
ned
aero
bic
trai
ning
and
resi
stan
cetr
aini
ng(C
T),
27sh
amtr
aini
ngfo
llow
edby
aero
bic
trai
ning
(AT
)
RT
AT
:42
(10)
;C
T:4
1(1
0);
AT
:39
(9)
RT
AT
:68
(6);
CT
:68
(8);
AT
:68
(7)
RC
TA
T:4
x5
min
utes
ofst
atio
nary
cycl
ing
at50
%ofW
peak
with
rest
inte
rval
sof2
–4
min
utes
ofun
load
edcy
clin
g(p
rogr
esse
dto
80%
ofW
peak
).R
T:2
sets
of8–
10re
psle
gpr
ess,
knee
exte
nsio
n,kn
eefle
xion,
calf
rais
e,hi
pad
duct
ion
and
hip
abdu
ctio
nat
70%
of1
RM
(pro
gres
sed
to3
sets
at80
%of1
RM
).Sh
amtr
aini
ng:ge
ntle
chai
rex
erci
ses
16w
eeks
(3x/
w)
1R
M(s
umofdi
ffere
ntm
uscl
es)
Leg
exte
nsio
nen
dura
nce:
isoto
nic
repe
titions
at60
%of1
RM
ata
cade
nce
of12
reps
per
min
ute
untilt
ask
failu
re
RT
AT
(p>
0.00
1)C
T(p
<0.
001)
AT
(p<
0.00
1)R
TA
T(p
<0.
001)
CT
(p<
0.00
1)A
T(p
<0.
001)
"26.
7%
"27.
7%
"13.
3%
"173
.8%
"96.
6%
"46.
9%
RT
AT
>A
T(p¼
0.00
6)C
T>
AT
(p¼
0.01
5)ns
RT
AT
vs.C
TR
TA
T>
AT
(p¼
0.00
1)R
TA
T>
CT
(p¼
0.05
)C
T>
AT
(p¼
0.03
9)
Zan
ini
etal
.,20
1576
60C
OPD
:30
aero
bic
trai
ning
(AT
),30
com
bine
dae
robi
can
dre
sist
ance
trai
ning
(CT
)
AT
:46
(14)
;C
T:5
1(1
6)A
T:7
2(8
);C
T:6
9(6
)R
CT
AT
:30–
40m
inut
etr
eadm
illor
cycl
eer
gom
eter
at60
–70%
ofH
Rm
axdu
ring
6MW
Tat
Borg
dysp
nea
3–5,
uppe
rlim
btr
aini
ng(a
rmer
gom
eter
and
calli
sthe
nics
with
light
wei
ghts
).C
T:A
Tþ
RT
:2se
tsof7
exer
cise
s,12
–20
reps
at60
–70%
of1
RM
(pro
gres
sed
whe
n1
or
2re
psm
ore
coul
dbe
perf
orm
edon
2co
nsec
utiv
ese
ssio
ns)
3w
eeks
(5x/
w)
1R
Mle
gex
tens
ion
nsA
TC
T(p
<0.
001)
–
"30.
3%
not
repo
rted
(con
tinue
d)
25
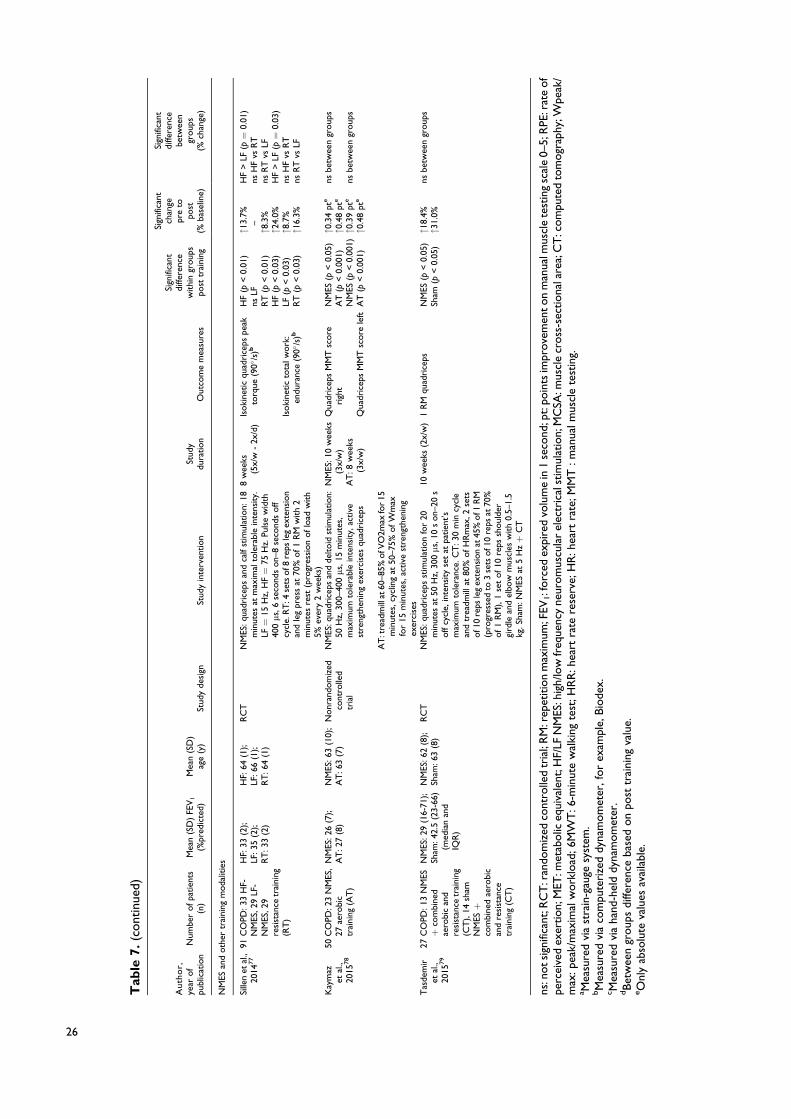
Tab
le7.
(cont
inue
d)
Auth
or,
year
of
publ
icat
ion
Num
ber
ofpa
tien
ts(n
)M
ean
(SD
)FE
V1
(%pr
edic
ted)
Mea
n(S
D)
age
(y)
Stud
yde
sign
Stud
yin
terv
ention
Stud
ydu
ration
Out
com
em
easu
res
Sign
ifica
ntdi
ffere
nce
withi
ngr
oup
spo
sttr
aini
ng
Sign
ifica
ntch
ange
pre
topo
st(%
base
line)
Sign
ifica
ntdi
ffere
nce
betw
een
group
s(%
chan
ge)
NM
ESan
doth
ertr
aini
ngm
oda
litie
s
Sille
net
al.,
2014
77
91C
OPD
:33
HF-
NM
ES,2
9LF
-N
MES
,29
resi
stan
cetr
aini
ng(R
T)
HF:
33(2
);LF
:35
(2);
RT
:33
(2)
HF:
64(1
);LF
:66
(1);
RT
:64
(1)
RC
TN
MES
:qua
dric
eps
and
calf
stim
ulat
ion:
18m
inut
esat
max
imal
tole
rabl
ein
tens
ity.
LF¼
15H
z,H
F¼
75H
z.Pu
lse
wid
th40
0ms
,6se
cond
son–
8se
cond
soff
cycl
e.R
T:4
sets
of8
reps
leg
exte
nsio
nan
dle
gpr
ess
at70
%of1
RM
with
2m
inut
esre
st(p
rogr
essi
on
oflo
adw
ith
5%ev
ery
2w
eeks
)
8w
eeks
(5x/
w-
2x/d
)Is
oki
netic
quad
rice
pspe
akto
rque
(90(
/s)b
Isoki
netic
tota
lwork
:en
dura
nce
(90(
/s)b
HF
(p<
0.01
)ns
LFR
T(p
<0.
01)
HF
(p<
0.03
)LF
(p<
0.03
)R
T(p
<0.
03)
"13.
7%–"8
.3%
"24.
0%"8
.7%
"16.
3%
HF
>LF
(p¼
0.01
)ns
HF
vsR
Tns
RT
vsLF
HF
>LF
(p¼
0.03
)ns
HF
vsR
Tns
RT
vsLF
Kay
maz
etal
.,20
1578
50C
OPD
:23
NM
ES,
27ae
robi
ctr
aini
ng(A
T)
NM
ES:2
6(7
);A
T:2
7(8
)N
MES
:63
(10)
;A
T:6
3(7
)N
onr
ando
miz
edco
ntro
lled
tria
l
NM
ES:q
uadr
icep
san
dde
ltoid
stim
ulat
ion:
50H
z,30
0–40
0ms
,15
min
utes
,m
axim
umto
lera
ble
inte
nsity,
active
stre
ngth
enin
gex
erci
ses
quad
rice
ps
AT
:tre
adm
illat
60–8
5%ofV
O2m
axfo
r15
min
utes
,cyc
ling
at50
–75%
ofW
max
for
15m
inut
es,a
ctiv
est
reng
then
ing
exer
cise
s
NM
ES:1
0w
eeks
(3x/
w)
AT
:8w
eeks
(3x/
w)
Qua
dric
eps
MM
Tsc
ore
righ
t
Qua
dric
eps
MM
Tsc
ore
left
NM
ES(p
<0.
05)
AT
(p<
0.00
1)N
MES
(p<
0.00
1)A
T(p
<0.
001)
"0.3
4pt
e
"0.4
8pt
e
"0.3
9pt
e
"0.4
8pt
e
nsbe
twee
ngr
oup
s
nsbe
twee
ngr
oup
s
Tas
dem
iret
al.,
2015
79
27C
OPD
:13
NM
ESþ
com
bine
dae
robi
can
dre
sist
ance
trai
ning
(CT
),14
sham
NM
ESþ
com
bine
dae
robi
can
dre
sist
ance
trai
ning
(CT
)
NM
ES:2
9(1
6-71
);Sh
am:4
2.5
(23-
66)
(med
ian
and
IQR
)
NM
ES:6
2(8
);Sh
am:6
3(8
)R
CT
NM
ES:q
uadr
icep
sst
imul
atio
nfo
r20
min
utes
at50
Hz,
300ms
,10
son–
20s
off
cycl
e,in
tens
ity
set
atpa
tien
t’s
max
imum
tole
ranc
e.C
T:3
0m
incy
cle
and
trea
dmill
at80
%ofH
Rm
ax,2
sets
of1
0re
psle
gex
tens
ion
at45
%of1
RM
(pro
gres
sed
to3
sets
of1
0re
psat
70%
of1
RM
),1
set
of10
reps
shoul
der
gird
lean
del
bow
mus
cles
with
0.5–
1.5
kg.S
ham
:NM
ESat
5H
zþ
CT
10w
eeks
(2x/
w)
1R
Mqu
adri
ceps
NM
ES(p
<0.
05)
Sham
(p<
0.05
)"1
8.4%
"31.
0%ns
betw
een
group
s
ns:n
otsi
gnifi
cant
;RC
T:r
ando
miz
edco
ntro
lled
tria
l;R
M:r
epet
itio
nm
axim
um;F
EV1:f
orc
edex
pire
dvo
lum
ein
1se
cond
;pt:
poin
tsim
prove
men
ton
man
ualm
uscl
ete
stin
gsc
ale
0–5;
RPE
:rat
eof
perc
eive
dex
ertion;
MET
:met
abolic
equi
vale
nt;H
F/LF
NM
ES:h
igh/
low
freq
uenc
yne
urom
uscu
lar
elec
tric
alst
imul
atio
n;M
CSA
:mus
cle
cross
-sec
tiona
lare
a;C
T:c
om
pute
dto
mogr
aphy
;Wpe
ak/
max
:pea
k/m
axim
alw
ork
load
;6M
WT
:6-m
inut
ew
alki
ngte
st;H
RR
:hea
rtra
tere
serv
e;H
R:h
eart
rate
;MM
T:m
anua
lmus
cle
test
ing.
a Mea
sure
dvi
ast
rain
-gau
gesy
stem
.bM
easu
red
via
com
pute
rize
ddy
nam
om
eter
,fo
rex
ampl
e,Bio
dex.
c Mea
sure
dvi
aha
nd-h
eld
dyna
mom
eter
.dBet
wee
ngr
oup
sdi
ffere
nce
base
don
post
trai
ning
valu
e.eO
nly
abso
lute
valu
esav
aila
ble.
26

quality studies.83 Studies using a single group designwith or without a healthy control group following asimilar intervention were not assessed.
ResultsSearch resultsThe study selection process is outlined in Figure 1. Weidentified 9933 articles with our search strategy. Aftertitle screening, 8843 articles were excluded, resulting in1090 remaining articles for abstract screening. Refer-ence screening of review papers delivered 10 more eli-gible articles. Finally, 162 full-text articles werescreened, of which 92 articles were excluded. Theremaining 70 articles (n ¼ 2504 patients with COPD;n¼ 2124 exercise training, n¼ 380 control) were estab-lished as eligible to be used in our review.
Quality assessmentPedro scores of RCTs and non-RCTs are given inTable 1. Of the 40 assessed studies, 17 studies scoredbetween 6 and 8 points and are considered to bestudies of “good” quality. In all, 23 studies scored' 5 points, with 18 studies scoring 4 or 5 points(“fair” quality), and 5 studies ' 3 points which isconsidered “low” quality. The criteria of concealedallocation, blinding of assessors, adequate follow-up, and intention-to-treat analysis were often notfulfilled. One non-RCT was not assessed becauseof its retrospective nature.65 The other 29 studiesused a single group design with (n ¼ 4) or without(n¼ 25) a healthy control group that followed a similarintervention (Table 1).
Results per outcome measureOutcome measures. Muscle strength can be categor-ized into voluntary strength, that is, isometric, isoki-netic, and isotonic strength, and involuntary strength.Isometric strength is defined as a static contractionwithout a change in muscle length. Isokinetic strengthis determined as dynamic strength while maintaininga constant speed. Isotonic strength is defined asdynamic strength with maintaining constant forcewhile changing the length of the muscle. Involuntarystrength is assessed by electrically or magneticallystimulating a peripheral nerve, resulting in an unpo-tentiated twitch (rest) or potentiated twitch (per-formed seconds after a maximum voluntarycontraction). An overview of muscle strength mea-sures used across the 70 included studies is given in
Figure 2 (A). Isometric strength measures were usedmost frequently (43%), followed by isotonic (28%),and isokinetic (21%) strength measures. Manual mus-cle testing and involuntary strength measures wererarely used. Isometric strength assessment modalitiesare depicted in Figure 2 (B) and were dominantlyperformed by strain gauge, followed by computerizeddynamometer, handheld dynamometer, force plate, oran unknown device. Used measures of muscle endur-ance and assessment modalities of muscle mass variedstrongly and are depicted in Figure 3.
Results per outcome measure. All studies wherein per-centage change from baseline was available or wherepercentage change from baseline was calculated bythe reviewers are presented per outcome measure inFigures 4–7. Weighted means for changes from base-line for isometric, isokinetic, and isotonic strength aredepicted for aerobic, resistance, combined aerobicand resistance training, and neuromuscular electricalstimulation (NMES) in Figure 4. Overall, isometricquadriceps strength increased with 15%, isokineticquadriceps strength with 17%, and isotonic lowerlimb strength with 34% (Figure 4). Quadriceps endur-ance improved with 8.7–96.6% (Figure 5) and quad-riceps muscle mass with 4.2–12.1% (Figure 6).Comparisons in isotonic lower limb strength betweenaerobic, resistance and combined aerobic, and resis-tance training are presented in Figure 7.
Results per training modalityDifferent exercise training modalities were used toinvestigate the effect of exercise-based therapy on mus-cle function and muscle mass (Figure 1). A detailedoverview is given in the following sections. More infor-mation on the characteristics of the different studiesgrouped per training modality are given in Tables 2–7.
Aerobic training (Table 2)Muscle strength
Isometric strength: Four studies showed an increaseof 10–21% in isometric quadriceps strength aftertraining.11,12,14,15 In contrast, one study reportedno significant change in isometric quadricepsstrength.16 Significant between-group differ-ences in the change in isometric quadricepsstrength were reported in favor of the traininggroup compared to the nonexercising COPDcontrol group.15
De Brandt et al. 27

Isokinetic strength: One study measured isokineticquadriceps strength which increased with 13.6%after training in patients.13
Isotonic strength: Isotonic hamstring musclestrength was measured by 1RM leg curl andincreased with 50% after training, while in theCOPD control group no significant change wasreported.17 The difference between groups washowever not significant.17
Involuntary strength: Involuntary contraction of thequadriceps muscle produced by magnetic stimu-lation of the nervus femoralis and measured aspotentiated and unpotentiated twitch showed asignificant increase of 8.8% and 9.7% after train-ing, respectively.12 In contrast, another studyreported a nonsignificant increase in potentiatedtwitch after training.14
Muscle endurance
Isometric endurance: A study showed a nonsignificantincrease in isometric knee extension endurance,measured as holding an isometric contraction at50% of maximum until exhaustion.11
Isokinetic endurance: An increase of 58.6% inquadriceps muscle endurance, measured asdynamic repeated leg extension with weightscorresponding to 30% MVC until exhaustion,was reported in one study. This change was sig-nificantly greater compared to the nonexercisingcontrol group.15
Muscle mass
A significant increase of 8.3% in muscle mass,measured via bioelectrical impedance analysis,was reported of both lower limbs after aerobictraining but not in the nonexercising COPD con-trol group.17 Differences between groups werehowever not significant.17
Resistance training (Table 3)Muscle strength
Isometric strength: Six studies showed a significantincrease of 13.2–25.4% in isometric quadricepsstrength after resistance training.17,18,20,23–25,27
Two studies also reported a significant differ-ence in isometric quadriceps strength betweentraining group and control group in favor of
training.20,22 One study, however, did not reporta significant increase in isometric quadricepsmuscle strength after training.26 Two studiesmeasured isometric hamstrings muscle strength,all showing a significant increase of 11.4–19.0%.27,26 Isometric hip abductor strength wasnot significantly different after training betweenthe training group and the control group22. Thestudy of Ramos et al. did not report a significantdifference in isometric strength of knee flexorsand knee extensors between 8 weeks of conven-tional resistance training and elastic tube resis-tance training.27
Isokinetic strength: Three studies showed a signifi-cant increase of 8.0–25.2% in isokinetic peak tor-que (Nm) after training.24,20,28 One study,however, reported no significant increase in iso-kinetic peak torque.80 Significant between-groupdifferences in isokinetic peak torque were in favorof training compared to control in two stud-ies.20,28 In one study, however, no significant dif-ference between training and control group wasreported in isokinetic peak torque.19
Isotonic strength: Isotonic quadriceps strengthmeasured by 1RM leg press showed an increaseof 16.0–27.1% after training.18,21 Between groupdifferences were also significant in favor oftraining compared to control.18,21 A 5RM legpress was also measured in one study andincreased with 34.5% after training, which wassignificantly different compared to control.20 A1RM leg extension increased with 44% afterresistance training in patients with COPD, whichwas significantly different compared to controlin favor of training.18
Muscle endurance
Isokinetic endurance: Isokinetic total work during30 consecutive knee extension repetitions wassignificantly increased with 11.5%, which wassignificantly different with controls.28 Anotherstudy reported a significant increase of 320 J inisokinetic total work during 60 seconds of kneeextension repetitions in patients with COPDafter training which was also significantly dif-ferent with controls.19
Isotonic endurance: Isotonic muscle endurance ofthe lower limbs with external loading increasedwith 25 repetitions performed in 30 seconds in thetraining group compared to the control group.80
28 Chronic Respiratory Disease

Muscle mass. One study reported a significant 4.2%increase in cross-sectional area (CSA) of the quadri-ceps, measured by magnetic resonance imaging(MRI), which was not different compared to nonexer-cising COPD controls.20 Two other studies measuredthigh lean mass with dual-energy x-ray absorptiome-triy (DEXA) and reported a 5.7–7.3% increase afterresistance training.24,25 Menon et al. also measured anincrease of 21.8% in m. rectus femoris CSA and12.1% in quadriceps thickness via ultrasound aftertraining.25
Combined aerobic and resistance training (Table 4)Muscle strength
Isometric strength—A significant increase of 7.0–32.0% in isometric quadriceps strength after train-ing was reported in seven studies,34,35,37,38,42,44,49
with one study only stating significant improve-ment without showing data.45 Two studiesreported no significant change in isometric quad-riceps strength after training.30,40 Three studiesreported significant differences between thetraining and the control group in favor oftraining,37,29,46 while one other study reported nosignificant difference between training and controlgroup.39 Nonsignificant differences were alsoreported between sarcopenic and nonsarcopenicpatients,50 between patients with or without con-tractile muscle fatigue,44 between trained patientswith COPD and trained healthy controls,45 andbetween hypoxemic and normoxemic patients.49
Isokinetic strength: Five studies measured isoki-netic quadriceps strength after training showinga 8.3–30% increase in peak torque.31–33,36,41
One study also measured isokinetic hamstringstrength of the right and the left leg whichincreased with 20.2% and 42.1%, respectively.32
Isotonic strength: One study measured isotonicstrength as 1RM after training, showing a33.9% increase in leg extension 1RM afterhigh-intensity training which was significantlydifferent with low-intensity training.43 Nosignificant change was established after low-intensity training.43 Four studies measured iso-tonic quadriceps strength via 10RM, with threestudies showing a 63.4–96.9% increase in 10RMleg extension,48,51,52 while another studyreported a 71.0% increase in 10RM weightliftingafter training.53 A 15RM leg press was measured
in one study, with a mean change of 16 kgreported after training, which was significantlydifferent with controls whom did not show asignificant change.37
Muscle endurance
Isokinetic endurance: Quadriceps fatigue as a pro-portional decline of isokinetic peak torques dur-ing 15 sequential voluntary maximal contractionsat an angular velocity of 90(/second was mea-sured and improved with 20% after training.33
Isotonic endurance: A study measured an increaseof 44.5% in time to exhaustion during dynamiccontractions at 30% maximal voluntary contrac-tion (MVC) at a rate of 10 movements per min-ute after training.45
Muscle mass. Quadriceps CSA, measured via MRI,was reported to increase with 7% after combinedaerobic and resistance training.35 Another studycompared CSA of m. rectus femoris, measured viaultrasound, between a nonindividualized low-intensity and individualized training group. Musclemass improved significantly with 8.6% after indivi-dualized training but not after nonindividualizedlow-intensity training. Between group differenceswere however not significant.47
Neuromuscular electrical stimulationand magnetic stimulation training (Table 5)Muscle strength
Isometric strength: Two studies reported an 11–14.8% increase in isometric quadriceps strengthafter NMES,58,60 which was significantly differ-ent between NMES and sham after 6 weeks infavor of NMES.58,60 Two other studies did notreport a significant increase after NMES,55,57
with one study also reporting no significant dif-ferences between NMES and control after thetraining protocol.55 Magnetic stimulation train-ing (MST) increased isometric quadricepsstrength with 17.5%.61
Isokinetic strength: Peak torque increased and wassignificantly different with controls in favor ofNMES after the training protocol,55,54 whereinone study with 39.0%54 while the other study didnot report significant data.55 Two studies did notreport a significant increase after NMES56,57
De Brandt et al. 29

with also no significant difference betweenNMES and sham after the training protocol.57
Hamstrings peak torque showed a 33.9%increase after NMES which was significantlydifferent with controls in favor of NMES.54
Involuntary strength: Unpotentiated twitch afterNMES was reported to be significantly increasedwith 14% which was significantly differentbetween NMES and sham after 6 weeks in favorof NMES after adjustment for baseline.60 Unpo-tentiated twitch after MST showed no significantincrease in both the intervention and the controlgroup.61
Muscle endurance
Isometric endurance: A NMES study measuredtime to exhaustion after an endurance test (iso-metric contraction at 60% MVC) and reported a37% increase in time to exhaustion after NMES,which was significantly different with the con-trol group58. After MST, quadriceps muscleendurance was increased with 44%. Muscleendurance was measured as time to exhaustionfor isometric leg extensions at 10% MVC with12 contractions per minute.61
Isokinetic endurance: The fatigue index after aquadriceps muscle endurance isokinetic test(maximal number of contractions in 1 minute)was reported to be decreased which was signif-icantly different between NMES and controls infavor of NMES.55
Muscle mass. A 6% increase in mid-thigh and calfmuscle mass was reported, which was significantlydifferent between NMES and sham in favor of NMES,measured by computed tomography (CT).58 In con-trast, another study reported no increase in leg musclemass, measured by DEXA, after NMES.56 A thirdstudy measured thigh circumference and reported asignificant 2.9% increase, which was significantlyhigher compared to the control group.59 Anotherrecent study measured rectus femoris CSA via ultra-sound after NMES and reported a significant increaseof 19.7%, which was significantly different betweenNMES and sham in favor of NMES.60 (Table 6)
Other training modalities (Table 6)High-intensity interval training. One study performedhigh-intensity interval knee-extensor training in
patients with COPD (Table 6). Muscle endurance ofthe quadriceps, measured as peak work during anincremental knee-extensor protocol with 2 W incre-ments every 3 minutes, increased with 37.0% aftertraining.62 Muscle mass, measured with MRI, did notincrease significantly after HIIT of the kneeextensors.62
Whole-body vibration training. Two studies implemen-ted whole-body vibration training (WBVT) as theirtraining stimulus (Table 6)63,64. In one 6-week WBVTstudy, isokinetic strength of the quadriceps and ham-strings did not increase significantly after WBVT andwas not significantly different between WBVT andcontrol group after the intervention.63 Another 12-week study implemented WBVT or resistance train-ing. Only the resistance training group increased theirisometric quadriceps strength significantly with10.5%. However, no significant differences betweenWBVT and resistance training were established afterthe intervention (Table 6).64
Water-based training. One study compared water-based with land-based pulmonary rehabilitation65
(Table 6). Aerobic and resistance components oftraining were similar for both water and land-basedtraining. The 6RM knee extension (92.7% and 68.0%)and 6RM hip flexion (85.8% and 82.7%) increasedsignificantly after both water- and land-based train-ing, respectively. Between group differences were notsignificant (Table 6).65
Comparing aerobic, resistance and combined aerobic andresistance training (Table 7)Aerobic versus resistance training. Isometric knee exten-sion peak torque was compared after 12 weeks aero-bic versus resistance training and increasedsignificantly with 42% versus 20% respectively,which was significantly different between the twotraining modalities.68 Isometric knee flexion forceincreased 28% versus 31%, respectively,68 while iso-metric knee extension force only increased signifi-cantly (35%) after resistance training.68
Aerobic versus combined aerobic and resistance training.Significant increases were found after combined aero-bic and resistance training (20%) and aerobic trainingalone (7.8%) in isotonic quadriceps strength in favor ofcombined aerobic and resistance training.66 In contrast,isotonic quadriceps strength did not increase signifi-cantly after aerobic training compared to a significant9–36.5% increase after combined aerobic and resistance
30 Chronic Respiratory Disease

training in four other studies.69–71,76 A similar phenom-enon was reported for isotonic hamstring strength.69
One study, however, reported no significant increasesin isotonic quadriceps strength after both aerobic andcombined aerobic and resistance training.72 Solely onestudy compared muscle mass between different trainingmodalities and reported a significantly increased bilat-eral thigh MCSA, measured by CT, with 8% after com-bined aerobic and resistance training but not afteraerobic training alone.66 Between group differenceswere significant and in favor of combined aerobic andresistance training.66
Aerobic versus resistance versus combined aerobic andresistance training. A study reported a significantincrease of 20.5%, 52.8%, and 52.8% in isotonicquadriceps strength after both aerobic, resistance, andcombined aerobic and resistance training, respec-tively.67 Isotonic hamstring strength also showed sig-nificant increases after all three training modalities.67
Significant between group differences identified agreater increase in quadriceps and hamstring strengthafter resistance training and combined aerobic andresistance training compared to aerobic training.67
Similar significant between group differences werereported in the study of Vonbank et al., where theaerobic training group did not improve its isotonicquadriceps strength significantly.74
Training modality sequence. One study investigated thesequence of training modalities and reported that 8weeks of resistance training followed by 8 weeks ofaerobic training increased the sum of 1RM of lowerlimb exercises with 26.7%. Comparable significantresults were found after 8 weeks of combined aerobicand resistance training which increased the 1RM sumwith 27.7%, while 8 weeks of aerobic training onlyincreased the 1RM sum with 13.3%.75 Isotonic mus-cle endurance, measured by repeated leg extensions at60% of 1RM (12 repetitions per minute) until exhaus-tion, increased significantly after resistance trainingfollowed by aerobic training (þ 173.8%) but also aftercombined aerobic and resistance training (þ96.6%)and after aerobic training (þ46.9%).75 Both resistancetraining followed by aerobic training and combinedaerobic and resistance training increased muscleendurance significantly more compared to the aerobictraining group.75
Resistance training versus low-intensity training. Resis-tance training increased leg press and leg extension1RM with 58.2% and 44.4% compared to no
significant changes after low-intensity training. Resis-tance training combined with low-intensity trainingincreased leg press and leg extension with 48.7% and21.2%, respectively.73 Between group differencesestablished that adding resistance training signifi-cantly increases strength more compared to low-intensity training alone.73
Comparing NMES with other training modalities(Table 7)NMES versus aerobic training. Ten weeks of high-frequency NMES (HF-NMES) (50 Hz) versus 8weeks of aerobic training (treadmill walking andcycling) in patients with severe COPD78 increased thequadriceps manual muscle testing (MMT) score sig-nificantly in both groups with no significant differ-ences between the groups.78
NMES versus resistance training. Sillen et al. comparedresistance training (4 sets of 8 reps leg extension andleg press at 70% of 1RM) to low-frequency NMES(LF-NMES) (15 Hz) and HF-NMES (75 Hz)77 andreported significant increases in isokinetic quadricepspeak torque after HF-NMES (13.7%) and resistancetraining (8.3%). Isokinetic quadriceps peak torquewas significantly different between HF-NMES andLF-NMES with the latter showing no significantchanges.77 Quadriceps endurance was measured astotal work (J) during an isokinetic test, whichincreased significantly after HF-NMES (24.0%),LF-NMES, (8.7%) and resistance training (16.3%).Total work after HF-NMES was however signifi-cantly higher compared to total work after LF-NMES.77
NMES as add-on intervention. One other study inves-tigated the effect of adding HF-NMES (50 Hz) to a10-week combined aerobic and resistance trainingprogram.79 Quadriceps strength, measured with a1RM test, significantly increased with 18.4% and31.0% in the NMES group and the sham NMESgroup, respectively. No differences in quadricepsstrength were reported between the addition of NMESor sham NMES to combined aerobic and resistancetraining in patients with COPD.79
DiscussionThis is the first review of the English-language, peer-reviewed literature that summarizes in detail thechanges in lower limb muscle function and muscle
De Brandt et al. 31

mass after exercise-based training interventions inpatients with clinically stable COPD. Despite thelarge heterogeneity in exercise training interventionsand outcome measures used, most exercise-basedtrials showed improvements in lower limb musclestrength, muscle endurance, and muscle mass inpatients with COPD, which proves again the utterimportance of exercise training during pulmonaryrehabilitation.
Methodological considerationsGenerally, lower limb muscle function and massimproved in patients with COPD following theexercise-based interventions. Nevertheless, multiplemethodological considerations need to be discussed.
Large variation in exercise-based interventions. In total,70 articles were identified describing a variety ofexercise-based interventions. Indeed, the impact oftreadmill or outdoor walking, stationary cycling,resistance training, elastic tube training, HIIT, NMES,MST, WBVT, water-based training, or a combinationthereof on lower limb muscle function and mass haveall been assessed in patients with COPD. Which inter-vention(s) is (are) best for which subgroup of patientsremains currently unknown. To date, only a limitednumber of studies that assessed effects of exercise-based interventions on muscle function/mass havespecifically recruited patients with COPD based onthe degree of lower limb muscle dysfunction/atro-phy.68,77 For example, resistance training and NMESare safe and very effective in COPD patients withsevere dyspnea and lower limb muscle weakness atthe start of the program.84,85 The low burden on theimpaired ventilatory system may be another reason toselect NMES or resistance training to improve limbmuscle function/mass in severely dyspneic COPDpatients.86,87 The purposes of resistance training andNMES also reach the acute care setting and both train-ing modalities seem viable and effective in increasingmuscle function and mass in unstable patients that arehospitalized due to a severe COPD exacerbation.88–94
This evokes physiotherapists to implement theseexercise-based interventions during and after hospita-lization to counteract muscle weakness and wasting.
If the aim is to increase lower limb muscle func-tion/mass, resistance training may be a better train-ing modality than aerobic training.67,74 This fits withan important training principle: specificity, whichmeans that both acute exercise responses and
training adaptations are highly specific to the typeof activity and to the volume and intensity of theexercise performed.95 It is especially importantwhen aiming to achieve a specific goal, for example,increased muscle strength.95 Interestingly, increasesin lower limb muscle function (Figures 4 and 5) andmass (Figure 6) also occurred after walking/cyclingtraining in patients with COPD.3,11–15,17,67,68,73,75,78
These cross-over training effects have also beenobserved in healthy elderly96,97 and patients withchronic heart failure.98,99 It can be hypothesized thathigh-intensity (whole-body and local) aerobic exer-cises are sufficient to induce significant morpholo-gical (e.g. it can counteract skeletal muscle atrophy)and functional changes related to the force generat-ing capacity of the skeletal muscles in healthyelderly subjects and in patients with COPD or con-gestive heart failure. Nevertheless, it should be notedthat aerobic training combined with resistance train-ing resulted in significantly greater improvements inskeletal muscle force and in muscle CSA of the mid-thigh compared to aerobic training alone in patientswith COPD (Figure 7). 3,67,69,70,71,74,75 Thus, whenpatients with COPD are able to perform combinedaerobic and resistance training, this may be the pre-ferred choice of exercise training modality.
Another popular training modality in healthy adults,but still less used in patients with COPD is HIIT.Whole body HIIT (e.g. cycling) has been shown toimprove muscle fiber proportion (type I and IIAincrease, type IIB decrease), fiber size, and capillaryto fiber ratio in lower limb muscle regardless of GOLDstage and presence/absence of cachexia.8,100–103 Localmuscle HIIT induced improvements in quadricepsendurance, citrate synthase activity, and mitochondrialrespiration capacity.62 Muscle mass, however, did notincrease after local muscle HIIT.62 Measurements ofmuscle strength have not yet been performed inpatients with COPD after HIIT. It seems likely thatHIIT training will mostly affect the aerobic capacity,but in light of the cross-training effects on musclestrength seen after aerobic training it seems worth toinvestigate the effect of HIIT on muscle strength.
All studies reported a rather large variation in themuscle response to the various interventions. In light ofthis, in 17%, 87%, and 13% of cases where quadricepsstrength, quadriceps endurance, and lower-limb mass,respectively, were measured, a nonsignificant increasecompared to baseline values was reported. This sug-gests that not all patients may benefit to the same extentfrom a similar exercise-based intervention, and/or
32 Chronic Respiratory Disease

patients perform the exercise-based intervention to adifferent extent, which, in turn will give a differentresponse in change in muscle function and musclemass. This variation in response is also reported inhealthy elderly.104 A similar phenomenon is also seenin the combined aerobic and resistance training studyof Jones et al., where sarcopenic patients increasedsignificantly their quadriceps strength while nonsarco-penic patients did not.50 It is however specifically strik-ing for NMES interventions because NMES protocolsdid not differ greatly compared to the other NMES stud-ies with significant results. Whether this is a variation inindividual response to NMES dependent on diseaseseverity or attributed to poor compliance to the treat-ment in the home setting remains to be elucidated. Ingeneral, for all exercise-based therapies, to date in-depth analyses of responders and nonresponders in mus-cle function/mass following an exercise-based interven-tion have not been performed in patients with COPD.Only then statements can be made about which under-lying mechanisms (e.g. genetics, training intensity,training duration, disease severity, degree of sarcopenia,compliance, etc.) are responsible for this nonresponse.
Large variation in the methodology used to assess lowerlimb muscle function and mass. Lower limb musclefunction can be assessed using various methodolo-gies, using different outcomes. Some are effort depen-dent (isometric, isokinetic, and isotonic testing) andothers are not (n. femoralis magnetic stimulation).Even within a specific muscle testing approach, forexample, isokinetic muscle endurance testing, differ-ent protocols exist. Robles et al. also stipulate thatstandardization is necessary to acquire reliable andvalid muscle function measures.105 Indeed, to enablebenchmarking between studies/centers and to performa meta-analysis, standardization of the muscle testingmethodology needs to take place. The Official ATS/ERS statement on limb muscle dysfunction in COPDproposes to use a strain gauge to measure isometricquadriceps peak torque.2 Indeed this method is com-monly used in the research setting, but whether and towhat extent this method has been implemented indaily clinical practice remains currently unknown.Furthermore, without standardization of testing pro-cedures, it is difficult to make conclusions aboutwhich increase in muscle function/mass is actuallyclinically relevant. To the authors’ knowledge, thereis no minimal clinically important difference (MCID)developed for evaluating the relevance of musclefunction/mass increments.106
Envisioning Figure 4, the different muscle strengthoutcomes seem to respond differently to exercise train-ing, with isotonic strength clearly being more respon-sive to the effects of exercise training in comparisonwith the other strength outcomes. This is in line with astudy from Frontera et al., where knee extensor andflexor strength gains were 10 times greater measuredvia 1RM (isotonic) compared to Cybex (isokinetic),107
and a recent meta-analysis in healthy elderly reportingthat resistance training had large size effects on upperand lower limb 1RM (isotonic strength) while onlymedium size effects on lower-limb MVC (isometricstrength).108 The training principle of specificity mostprobably plays a large role in explaining this phenom-enon. During resistance training sessions, patients per-form their movements on the same device and in thesame motor pattern as during the 1RM testing method,while this is not the case when other strength tests (i.e.computerized and/or handheld dynamometry) are per-formed. Thus, neural adaptations specific to the type oftraining are suggested to explain this phenomenon,resulting in more pronounced increases in strengthwhen mimicking the training movements duringstrength test procedures.109,110 Also, the strength–velo-city relationship comes into play, suggesting thatincreases in slow contractions are gained after slow-velocity resistance training and increases in fast con-tractions after high-velocity exercise training.111 Thus,velocity and characteristics of the movements duringtraining are important factors to take into account wheninterpreting strength tests.107
Recommendations for future researchand practiceSeveral studies have implemented exercise trainingprograms that focus on short-term efficacy. Still, thecurrently available evidence did not enable the devel-opment and validation of a clinical decision tree insetting up an exercise-based pulmonary rehabilitationprogram, including setting, training modality/modal-ities, intensity, frequency, and duration. Such a clin-ical decision tree, already in development forcardiovascular disease,112 would support health-careprofessionals to choose the most optimal trainingapproach, taking multiple outcome measures, thebaseline characteristics of patients with COPD andtheir personal care needs into consideration. Interest-ingly, a reduced muscle function/mass can occur dueto a variety of reasons.2 Whether and to what extentexercise-based therapies can also reverse the impact
De Brandt et al. 33

of other underlying causes of muscle weakness/atro-phy (i.e. low-grade systemic inflammation, oxidativestress, accelerated aging, smoking, endocrinologicaldisturbances, etc.) remains to be determined but maypartially explain the lack of response to exercise-based therapies in individual patients. Therefore,future research may also want to take these covariatesinto consideration.
Obviously, consensus needs to be reached amongclinicians and researchers on how to assess musclefunction and mass before and after an exercise-basedintervention. At least, the chosen tests should besafe, reproducible, valid, and accurate. The clinicaldecision tree together with standardization of themethodology of muscle function and mass testingwill reduce the heterogeneity in the future trialresults. Indeed, this will also allow us to betterunderstand which patients will respond poorly to ourexercise-based treatments. In fact, exercise trainingalso fails to have a positive response in all healthysubjects.113–116
Additionally, in those patients with a beneficialshort-term response to exercise training, longitudinaleffects need to be studied. Indeed, maintaining thebenefits on a long-term basis seems difficult.117 Onlya few studies have shown that it is possible to main-tain muscle function improvements after a long-termfollow-up of 6–18 months in patients withCOPD.23,29,118 Therefore, focus should also be placedon educational interventions and behavior change.9
The behavior change interventions may also enablethe development of exercise maintenance strategiesfor patients to adopt a physically active and morehealthy lifestyle. In addition to exercise training,nutritional support also needs to be taken into consid-eration to optimize maintenance or increments inmuscle function and mass.
Methodologically, more research with a high levelof evidence is required to address future research rec-ommendations. After analyzing the study designs usedin the included studies in this review, 40 (57%) of 70studies were designed as (non)-randomized controlledtrials, with only 17 studies providing “good” qualityresearch. On the other hand, 29 (41%) of 70 identifiedstudies used a single group design with (n ¼ 5) orwithout (n ¼ 24) a healthy control group that followeda similar intervention. The lack of trials with a non-exercising COPD control group might be due to the“unethical” aspect of denying patients access to ahighly effective evidence-based intervention. A cross-over of the initial nonexercising COPD control group
after a waiting period might be a possible solution.Concerning sample size, 20 (29%) of the 70 studiesused a small sample size (defined as n' 10 per group).Hence, regarding future research, it seems advised tolift the current level of evidence by setting up moreRCTs or crossover RCTs with large sample sizes.
Acknowledgments
We would like to thank all colleagues in the field ofresearch that provided us with extra information about theirincluded work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interestwith respect to the research, authorship, and/or publicationof this article.
Funding
The author(s) disclosed receipt of the following financialsupport for the research, authorship, and/or publication of thisarticle: This work was supported by the Bijzonder Onder-zoeksfonds (BOF) of Hasselt University (15DOC12BOF).
References
1. Vestbo J, Hurd SS, Agusti AG, et al. Global strategy
for the diagnosis, management, and prevention of
chronic obstructive pulmonary disease: GOLD execu-
tive summary. Am J Respir Crit Care Med 2013; 187:
347–365.
2. Maltais F, Decramer M, Casaburi R, et al. An official
American thoracic society/european respiratory soci-
ety statement: update on limb muscle dysfunction in
chronic obstructive pulmonary disease. Am J Respir
Crit Care Med 2014; 189: e15–62.
3. Bernard S, LeBlanc P, Whittom F, et al. Peripheral
muscle weakness in patients with chronic obstructive
pulmonary disease. Am J Respir Crit Care Med 1998;
158: 629–634.
4. Troosters T, Sciurba F, Battaglia S, et al. Physical
inactivity in patients with COPD, a controlled
multi-center pilot-study. Respir Med. 2010; 104:
1005–1011.
5. Waschki B, Spruit MA, Watz H, et al. Physical activity
monitoring in COPD: compliance and associations
with clinical characteristics in a multicenter study.
Respir Med 2012; 106: 522–530.
6. Osthoff AK, Taeymans J, Kool J, et al. Association
between peripheral muscle strength and daily physical
activity in patients with COPD: a systematic literature
review and meta-analysis. J Cardiopulm Rehabil Prev
2013; 33: 351–359.
34 Chronic Respiratory Disease
7. Gosselink R, Troosters T, and Decramer M. Peripheral
muscle weakness contributes to exercise limitation in
COPD. Am J Respir Crit Care Med 1996; 153:
976–980.
8. De Brandt J, Spruit MA, Derave W, et al. Changes in
structural and metabolic muscle characteristics follow-
ing exercise-based interventions in patients with
COPD: a systematic review. Expert Rev Respir Med
2016; 10: 521–545.
9. Spruit MA, Singh SJ, Garvey C, et al. An official
american thoracic society/european respiratory society
statement: key concepts and advances in pulmonary
rehabilitation. Am J Respir Crit Care Med 2013; 188:
e13–64.
10. Ries AL, Bauldoff GS, Carlin BW, et al. Pulmonary
rehabilitation: joint ACCP/AACVPR evidence-based
clinical practice guidelines. Chest 2007; 131: 4S–42 S.
11. O’Donnell DE, McGuire M, Samis L, et al. General
exercise training improves ventilatory and peripheral
muscle strength and endurance in chronic airflow limita-
tion. Am J Respir Crit Care Med 1998; 157: 1489–1497.
12. Mador MJ, Kufel TJ, Pineda LA, et al. Effect of pul-
monary rehabilitation on quadriceps fatiguability dur-
ing exercise. Am J Respir Crit Care Med 2001; 163:
930–935.
13. Radom-Aizik S, Kaminski N, Hayek S, et al. Effects of
exercise training on quadriceps muscle gene expres-
sion in chronic obstructive pulmonary disease. J Appl
Physiol (1985) 2007; 102: 1976–1984.
14. Vivodtzev I, Flore P, Levy P, et al. Voluntary activa-
tion during knee extensions in severely deconditioned
patients with chronic obstructive pulmonary disease:
benefit of endurance training. Muscle Nerve 2008;
37: 27–35.
15. Vivodtzev I, Minet C, Wuyam B, et al. Significant
improvement in arterial stiffness after endurance train-
ing in patients with COPD. Chest 2010; 137: 585–592.
16. Guzun R, Aguilaniu B, Wuyam B, et al. Effects of
training at mild exercise intensities on quadriceps mus-
cle energy metabolism in patients with chronic
obstructive pulmonary disease. Acta Physiol (Oxf)
2012; 205: 236–246.
17. Farias CC, Resqueti V, Dias FA, et al. Costs and ben-
efits of pulmonary rehabilitation in chronic obstructive
pulmonary disease: a randomized controlled trial. Braz
J Phys Ther 2014; 18: 165–173.
18. Simpson K, Killian K, McCartney N, et al. Randomised
controlled trial of weightlifting exercise in patients with
chronic airflow limitation. Thorax 1992; 47: 70–75.
19. Clark CJ, Cochrane LM, Mackay E, et al. Skeletal
muscle strength and endurance in patients with mild
COPD and the effects of weight training. Eur Respir J
2000; 15: 92–97.
20. Kongsgaard M, Backer V, Jorgensen K, et al. Heavy
resistance training increases muscle size, strength and
physical function in elderly male COPD-patients–a
pilot study. Respir Med 2004; 98: 1000–1007.
21. Hoff J, Tjonna AE, Steinshamn S, et al. Maximal
strength training of the legs in COPD: a therapy for
mechanical inefficiency. Med Sci Sports Exerc 2007;
39: 220–226.
22. O’Shea SD, Taylor NF, and Paratz JD. A predomi-
nantly home-based progressive resistance exercise pro-
gram increases knee extensor strength in the short-term
in people with chronic obstructive pulmonary disease:
a randomised controlled trial. Aust J Physiother 2007;
53: 229–237.
23. Houchen L, Deacon S, Sandland C, et al. Preservation
of lower limb strength after a short course of pulmon-
ary rehabilitation with no maintenance: a 6-month
follow-up study. Physiotherapy 2011; 97: 264–266.
24. Menon MK, Houchen L, Singh SJ, et al. Inflammatory
and satellite cells in the quadriceps of patients with
COPD and response to resistance training. Chest
2012; 142: 1134–1142.
25. Menon MK, Houchen L, Harrison S, et al. Ultrasound
assessment of lower limb muscle mass in response to
resistance training in COPD. Respir Res 2012; 13: 119.
26. Ricci-Vitor AL, Bonfim R, Fosco LC, et al. Influence
of the resistance training on heart rate variability, func-
tional capacity and muscle strength in the chronic
obstructive pulmonary disease. Eur J Phys Rehabil
Med 2013; 49: 793–801.
27. Ramos EM, de Toledo-Arruda AC, Fosco LC, et al.
The effects of elastic tubing-based resistance training
compared with conventional resistance training in
patients with moderate chronic obstructive pulmonary
disease: a randomized clinical trial. Clin Rehabil 2014;
28: 1096–1106.
28. Nyberg A, Lindstrom B, Rickenlund A, et al. Low-
load/high-repetition elastic band resistance training in
patients with COPD: a randomized, controlled, multi-
center trial. Clin Respir J 2015; 9: 278–288.
29. Troosters T, Gosselink R, and Decramer M. Short- and
long-term effects of outpatient rehabilitation in
patients with chronic obstructive pulmonary disease:
a randomized trial. Am J Med 2000; 109: 207–212.
30. Gosselin N, Lambert K, Poulain M, et al. Endurance
training improves skeletal muscle electrical activity in
active COPD patients. Muscle Nerve 2003; 28: 744–753.
31. Franssen FM, Broekhuizen R, Janssen PP, et al. Effects
of whole-body exercise training on body composition
De Brandt et al. 35

and functional capacity in normal-weight patients with
COPD. Chest 2004; 125: 2021–2028.
32. Kamahara K, Homma T, Naito A, et al. Circuit training
for elderly patients with chronic obstructive pulmonary
disease: a preliminary study. Arch Gerontol Geriatr
2004; 39: 103–110.
33. Franssen FM, Broekhuizen R, Janssen PP, et al. Limb
muscle dysfunction in COPD: effects of muscle wast-
ing and exercise training. Med Sci Sports Exerc 2005;
37: 2–9.
34. Spruit MA, Gosselink R, Troosters T, et al. Low-grade
systemic inflammation and the response to exercise
training in patients with advanced COPD. Chest
2005; 128: 3183–3190.
35. McKeough ZJ, Alison JA, Bye PT, et al. Exercise
capacity and quadriceps muscle metabolism following
training in subjects with COPD. Respir Med 2006;
100: 1817–1825.
36. Bolton CE, Broekhuizen R, Ionescu AA, et al. Cellular
protein breakdown and systemic inflammation are
unaffected by pulmonary rehabilitation in COPD.
Thorax 2007; 62: 109–114.
37. Skumlien S, Skogedal EA, Bjortuft O, et al. Four
weeks’ intensive rehabilitation generates significant
health effects in COPD patients. Chron Respir Dis
2007; 4: 5–13.
38. Pitta F, Troosters T, Probst VS, et al. Are patients with
COPD more active after pulmonary rehabilitation?
Chest 2008; 134: 273–280.
39. van Wetering CR, Hoogendoorn M, Mol SJ, et al.
Short- and long-term efficacy of a community-based
COPD management programme in less advanced
COPD: a randomised controlled trial. Thorax 2010;
65: 7–13.
40. Evans RA, Singh SJ, Collier R, et al. Generic, symp-
tom based, exercise rehabilitation; integrating patients
with COPD and heart failure. Respir Med 2010; 104:
1473–1481.
41. Arizono S, Taniguchi H, Nishiyama O, et al. Improve-
ments in quadriceps force and work efficiency are
related to improvements in endurance capacity follow-
ing pulmonary rehabilitation in COPD patients. Intern
Med 2011; 50: 2533–2539.
42. Kozu R, Senjyu H, Jenkins SC, et al. Differences in
response to pulmonary rehabilitation in idiopathic pul-
monary fibrosis and chronic obstructive pulmonary
disease. Respiration 2011; 81: 196–205.
43. Probst VS, Kovelis D, Hernandes NA, et al. Effects of
2 exercise training programs on physical activity in
daily life in patients with COPD. Respir Care 2011;
56: 1799–1807.
44. Burtin C, Saey D, Saglam M, et al. Effectiveness of
exercise training in patients with COPD: the role of
muscle fatigue. Eur Respir J 2012; 40: 338–344.
45. Gouzi F, Prefaut C, Abdellaoui A, et al. Blunted muscle
angiogenic training-response in COPD patients versus
sedentary controls. Eur Respir J 2013; 41: 806–814.
46. Chigira Y, Takai T, Oda T, et al. Difference in the
effect of outpatient pulmonary rehabilitation due to
variation in the intervention frequency: intervention
centering on home-based exercise. J Phys Ther Sci
2014; 26: 1041–1044.
47. Greulich T, Kehr K, Nell C, et al. A randomized
clinical trial to assess the influence of a three months
training program (gym-based individualized vs.
calisthenics-based non-invidualized) in COPD-pati-
ents. Respir Res 2014; 15: 36.
48. Jacome C and Marques A. Impact of pulmonary reha-
bilitation in subjects with mild COPD. Respir Care
2014; 59: 1577–1582.
49. Costes F, Gosker H, Feasson L, et al. Impaired exercise
training-induced muscle fiber hypertrophy and Akt/
mTOR pathway activation in hypoxemic patients with
COPD. J Appl Physiol (1985) 2015; 118: 1040–1049.
50. Jones SE, Maddocks M, Kon SS, et al. Sarcopenia in
COPD: prevalence, clinical correlates and response to
pulmonary rehabilitation. Thorax 2015; 70: 213–218.
51. Marques A, Jacome C, Cruz J, et al. Effects of a pul-
monary rehabilitation program with balance training
on patients with COPD. J Cardiopulm Rehabil Prev
2015; 35: 154–158.
52. Marques A, Gabriel R, Jacome C, et al. Development
of a family-based pulmonary rehabilitation pro-
gramme: an exploratory study. Disabil Rehabil 2015;
37: 1340–1346.
53. Pothirat C, Chaiwong W, and Phetsuk N. Efficacy of a
simple and inexpensive exercise training program for
advanced chronic obstructive pulmonary disease
patients in community hospitals. J Thorac Dis 2015;
7: 637–643.
54. Bourjeily-Habr G, Rochester CL, Palermo F, et al.
Randomised controlled trial of transcutaneous electri-
cal muscle stimulation of the lower extremities in
patients with chronic obstructive pulmonary disease.
Thorax 2002; 57: 1045–1049.
55. Neder JA, Sword D, Ward SA, et al. Home based
neuromuscular electrical stimulation as a new rehabi-
litative strategy for severely disabled patients with
chronic obstructive pulmonary disease (COPD).
Thorax 2002; 57: 333–337.
56. Dal Corso S, Napolis L, Malaguti C, et al. Skeletal
muscle structure and function in response to electrical
36 Chronic Respiratory Disease
stimulation in moderately impaired COPD patients.
Respir Med 2007; 101: 1236–1243.
57. Napolis LM, Dal Corso S, Neder JA, et al. Neuromus-
cular electrical stimulation improves exercise toler-
ance in chronic obstructive pulmonary disease
patients with better preserved fat-free mass. Clinics
(Sao Paulo) 2011; 66: 401–406.
58. Vivodtzev I, Debigare R, Gagnon P, et al. Functional
and muscular effects of neuromuscular electrical sti-
mulation in patients with severe COPD: a randomized
clinical trial. Chest 2012; 141: 716–725.
59. Vieira PJ, Chiappa AM, Cipriano G Jr, et al. Neuro-
muscular electrical stimulation improves clinical and
physiological function in COPD patients. Respir Med
2014; 108: 609–620.
60. Maddocks M, Nolan CM, Man WD, et al. Neuromus-
cular electrical stimulation to improve exercise capac-
ity in patients with severe COPD: a randomised
double-blind, placebo-controlled trial. Lancet Respir
Med 2016; 4: 27–36.
61. Bustamante V, de Santa Maria EL, Gorostiza A, et al.
Muscle training with repetitive magnetic stimulation of
the quadriceps in severe COPD patients. Respir Med
2010; 104: 237–245.
62. Bronstad E, Rognmo O, Tjonna AE, et al.
High-intensity knee extensor training restores skeletal
muscle function in COPD patients. Eur Respir J 2012;
40: 1130–1136.
63. Pleguezuelos E, Perez ME, Guirao L, et al. Effects of
whole body vibration training in patients with severe
chronic obstructive pulmonary disease. Respirology
2013; 18: 1028–1034.
64. Salhi B, Malfait TJ, Van Maele G, et al. Effects of
whole body vibration in patients with COPD. COPD
2015; 12: 525–532.
65. Lotshaw AM, Thompson M, Sadowsky HS, et al.
Quality of life and physical performance in land- and
water-based pulmonary rehabilitation. J Cardiopulm
Rehabil Prev 2007; 27: 247–251.
66. Bernard S, Whittom F, Leblanc P, et al. Aerobic and
strength training in patients with chronic obstructive
pulmonary disease. Am J Respir Crit Care Med 1999;
159: 896–901.
67. Ortega F, Toral J, Cejudo P, et al. Comparison of
effects of strength and endurance training in patients
with chronic obstructive pulmonary disease. Am J
Respir Crit Care Med 2002; 166: 669–674.
68. Spruit MA, Gosselink R, Troosters T, et al. Resistance
versus endurance training in patients with COPD and
peripheral muscle weakness. Eur Respir J 2002; 19:
1072–1078.
69. Mador MJ, Bozkanat E, Aggarwal A, et al. Endurance
and strength training in patients with COPD. Chest
2004; 125: 2036–2045.
70. Panton LB, Golden J, Broeder CE, et al. The effects of
resistance training on functional outcomes in patients
with chronic obstructive pulmonary disease. Eur J
Appl Physiol 2004; 91: 443–449.
71. Phillips WT, Benton MJ, Wagner CL, et al. The effect
of single set resistance training on strength and func-
tional fitness in pulmonary rehabilitation patients. J
Cardiopulm Rehabil 2006; 26: 330–337.
72. Alexander JL, Phillips WT, and Wagner CL. The
effect of strength training on functional fitness in older
patients with chronic lung disease enrolled in pulmon-
ary rehabilitation. Rehabil Nurs 2008; 33: 91–97.
73. Dourado VZ, Tanni SE, Antunes LC, et al. Effect of
three exercise programs on patients with chronic
obstructive pulmonary disease. Braz J Med Biol Res
2009; 42: 263–271.
74. Vonbank K, Strasser B, Mondrzyk J, et al. Strength
training increases maximum working capacity in
patients with COPD–randomized clinical trial compar-
ing three training modalities. Respir Med 2012; 106:
557–563.
75. Covey MK, Collins EG, Reynertson SI, et al. Resis-
tance training as a preconditioning strategy for enhan-
cing aerobic exercise training outcomes in COPD.
Respir Med 2014; 108: 1141–1152.
76. Zanini A, Aiello M, Cherubino F, et al. The one
repetition maximum test and the sit-to-stand test in
the assessment of a specific pulmonary rehabilita-
tion program on peripheral muscle strength in
COPD patients. Int J Chron Obstruct Pulmon Dis
2015; 10: 2423–2430.
77. Sillen MJ, Franssen FM, Delbressine JM, et al. Effi-
cacy of lower-limb muscle training modalities in
severely dyspnoeic individuals with COPD and quad-
riceps muscle weakness: results from the DICES trial.
Thorax 2014; 69: 525–531.
78. Kaymaz D, Ergun P, Demirci E, et al. Comparison of
the effects of neuromuscular electrical stimulation and
endurance training in patients with severe chronic
obstructive pulmonary disease. Tuberk Toraks 2015;
63: 1–7.
79. Tasdemir F, Inal-Ince D, Ergun P, et al. Neuromuscu-
lar electrical stimulation as an adjunct to endurance
and resistance training during pulmonary rehabilitation
in stable chronic obstructive pulmonary disease.
Expert Rev Respir Med 2015; 9: 493–502.
80. Clark CJ, Cochrane L, and Mackay E. Low intensity
peripheral muscle conditioning improves exercise
De Brandt et al. 37

tolerance and breathlessness in COPD. Eur Respir J
1996; 9: 2590–2596.
81. Verhagen AP, de Vet HC, de Bie RA, et al. The Delphi
list: a criteria list for quality assessment of randomized
clinical trials for conducting systematic reviews devel-
oped by Delphi consensus. J Clin Epidemiol 1998; 51:
1235–1241.
82. Sherrington C, Herbert RD, Maher CG, et al.
PEDro. A database of randomized trials and sys-
tematic reviews in physiotherapy. Man Ther 2000;
5: 223–226.
83. Foley NC, Bhogal SK, Teasell RW, et al. Estimates of
quality and reliability with the physiotherapy
evidence-based database scale to assess the methodol-
ogy of randomized controlled trials of pharmacological
and nonpharmacological interventions. Phys Ther
2006; 86: 817–824.
84. O’Shea SD, Taylor NF, and Paratz JD. Progressive
resistance exercise improves muscle strength and may
improve elements of performance of daily activities for
people with COPD: a systematic review. Chest 2009;
136: 1269–1283.
85. Sillen MJ, Speksnijder CM, Eterman RM, et al. Effects
of neuromuscular electrical stimulation of muscles of
ambulation in patients with chronic heart failure or
COPD: a systematic review of the English-language
literature. Chest 2009; 136: 44–61.
86. Probst VS, Troosters T, Pitta F, et al. Cardiopulmonary
stress during exercise training in patients with COPD.
Eur Respir J 2006; 27: 1110–1118.
87. Sillen MJ, Franssen FM, Vaes AW, et al. Metabolic
load during strength training or NMES in individuals
with COPD: results from the DICES trial. BMC Pulm
Med 2014; 14: 146.
88. Troosters T, Probst VS, Crul T, et al. Resistance train-
ing prevents deterioration in quadriceps muscle func-
tion during acute exacerbations of chronic obstructive
pulmonary disease. Am J Respir Crit Care Med 2010;
181: 1072–1077.
89. Borges RC and Carvalho CR. Impact of resistance
training in chronic obstructive pulmonary disease
patients during periods of acute exacerbation. Arch
Phys Med Rehabil 2014; 95: 1638–1645.
90. Torres-Sanchez I, Valenza MC, Saez-Roca G, et al.
Results of a multimodal program during hospitaliza-
tion in obese COPD exacerbated patients. COPD 2016;
13(1): 19–25.
91. Zanotti E, Felicetti G, Maini M, et al. Peripheral mus-
cle strength training in bed-bound patients with COPD
receiving mechanical ventilation: effect of electrical
stimulation. Chest 2003; 124: 292–296.
92. Vivodtzev I, Pepin JL, Vottero G, et al. Improvement
in quadriceps strength and dyspnea in daily tasks after
1 month of electrical stimulation in severely decondi-
tioned and malnourished COPD. Chest 2006; 129:
1540–1548.
93. Abdellaoui A, Prefaut C, Gouzi F, et al. Skeletal
muscle effects of electrostimulation after COPD
exacerbation: a pilot study. Eur Respir J 2011; 38:
781–788.
94. Giavedoni S, Deans A, McCaughey P, et al. Neuro-
muscular electrical stimulation prevents muscle func-
tion deterioration in exacerbated COPD: a pilot study.
Respir Med 2012; 106: 1429–1434.
95. Wilmore JH. DLCKWL. Principles of exercise train-
ing. In: Bahrke MS, Garrett L, Schwarzentraub M, et al.
(eds) Physiology of Sport and Exercise. Champaign:
Human Kinetics, 2008, pp. 186–201.
96. Lovell DI, Cuneo R, and Gass GC. Can aerobic train-
ing improve muscle strength and power in older men?
J Aging Phys Act 2010; 18: 14–26.
97. Wood RH, Reyes R, Welsch MA, et al. Concurrent
cardiovascular and resistance training in healthy older
adults. Med Sci Sports Exerc 2001; 33: 1751–1758.
98. Delagardelle C, Feiereisen P, Autier P, et al. Strength/
endurance training versus endurance training in con-
gestive heart failure. Med Sci Sports Exerc 2002; 34:
1868–1872.
99. Tyni-Lenne R, Jansson E, and Sylven C.
Female-related skeletal muscle phenotype in patients
with moderate chronic heart failure before and after
dynamic exercise training. Cardiovasc Res 1999; 42:
99–103.
100. Vogiatzis I, Terzis G, Nanas S, et al. Skeletal muscle
adaptations to interval training in patients with
advanced COPD. Chest 2005; 128: 3838–3845.
101. Vogiatzis I, Stratakos G, Simoes DC, et al. Effects of
rehabilitative exercise on peripheral muscle TNFal-
pha, IL-6, IGF-I and MyoD expression in patients
with COPD. Thorax 2007; 62: 950–956.
102. Vogiatzis I, Simoes DC, Stratakos G, et al. Effect of
pulmonary rehabilitation on muscle remodelling in
cachectic patients with COPD. Eur Respir J 2010;
36: 301–310.
103. Vogiatzis I, Terzis G, Stratakos G, et al. Effect of
pulmonary rehabilitation on peripheral muscle fiber
remodeling in patients with COPD in GOLD stages II
to IV. Chest 2011; 140: 744–752.
104. Churchward-Venne TA, Tieland M, Verdijk LB, et al.
There are no nonresponders to resistance-type exer-
cise training in older men and women. J Am Med Dir
Assoc 2015; 16: 400–411.
38 Chronic Respiratory Disease
105. Robles PG, Mathur S, Janaudis-Fereira T, et al. Mea-
surement of peripheral muscle strength in individuals
with chronic obstructive pulmonary disease: a sys-
tematic review. J Cardiopulm Rehabil Prev 2011;
31: 11–24.
106. Wouters EF. Minimal clinically important differences
in COPD: body mass index and muscle strength.
COPD 2005; 2: 149–155.
107. Frontera WR, Meredith CN, O’Reilly KP, et al.
Strength conditioning in older men: skeletal muscle
hypertrophy and improved function. J Appl Physiol
(1985) 1988; 64: 1038–1044.
108. Borde R, Hortobagyi T, and Granacher U.
Dose-response relationships of resistance training
in healthy old adults: a systematic review and
meta-analysis. Sports Med 2015; 45: 1693–1720.
109. Dons B, Bollerup K, Bonde-Petersen F, et al. The
effect of weight-lifting exercise related to muscle
fiber composition and muscle cross-sectional area in
humans. Eur J Appl Physiol Occup Physiol 1979; 40:
95–106.
110. Coyle EF, Feiring DC, Rotkis TC, et al. Specificity of
power improvements through slow and fast isokinetic
training. J Appl Physiol Respir Environ Exerc Physiol
1981; 51: 1437–1442.
111. Caiozzo VJ, Perrine JJ, and Edgerton VR.
Training-induced alterations of the in vivo force-
velocity relationship of human muscle. J Appl Physiol
Respir Environ Exerc Physiol 1981; 51: 750–754.
112. Hansen D, Dendale P, Coninx K, et al. The European
Association of Preventive Cardiology Exercise
Prescription in Everyday Practice and Rehabilita-
tive Training (EXPERT) tool: A digital training
and decision support system for optimized exercise
prescription in cardiovascular disease. Concept,
definitions and construction methodology. Eur J
Prev Cardiol 2017. Epub ahead of print 1 January
2017. DOI: 10.1177/2047487317702042.
113. Karavirta L, Hakkinen K, Kauhanen A, et al. Individ-
ual responses to combined endurance and strength
training in older adults. Med Sci Sports Exerc 2011;
43: 484–490.
114. Bouchard C, An P, Rice T, et al. Familial aggregation
of VO(2max) response to exercise training: results
from the HERITAGE family study. J Appl Physiol
(1985) 1999; 87: 1003–1008.
115. Timmons JA. Variability in training-induced skeletal
muscle adaptation. J Appl Physiol (1985) 2011; 110:
846–853.
116. Chmelo EA, Crotts CI, Newman JC, et al. Heteroge-
neity of physical function responses to exercise train-
ing in older adults. J Am Geriatr Soc 2015; 63:
462–469.
117. Spruit MA, Troosters T, Trappenburg JC, et al. Exer-
cise training during rehabilitation of patients with
COPD: a current perspective. Patient Educ Couns
2004; 52: 243–248.
118. Cruz J, Brooks D, and Marques A. Walk2Bactive: a
randomised controlled trial of a physical
activity-focused behavioural intervention beyond
pulmonary rehabilitation in chronic obstructive pul-
monary disease. Chron Respir Dis 2016; 13: 57–66.
De Brandt et al. 39