Embed Size (px)
Citation preview
Guit Festschrift, 1989, 71-74
Chronic lymphocytic gastritis and protein losinggastropathyJ R CRAMPTON, J 0 HUNTER, G NEALE, AND D G D WIGHT
Chronic lymphocytic gastritis (CLG) is a recentlydescribed histopathological entity characterised bythe presence of lymphocytes in the surface andfoveolar epithelium of the gastric mucosa. Previousaccounts'- have paid attention to both the endoscopicand histological features of the condition but thepresenting features and clinical correlates of thepathology have not been clearly characterised. In thisreport we describe a new clinical association which issupported by a second case with similar features ofprotein loss. This is also the first report of CLG inwhich lymphocytic infiltration has also been shown inthe duodenal mucosa.
Case 1The patient, D M, a 34 year old solicitor, presented tohis general practitioner with slow recovery from a flulike illness. Although his own symptoms were few hiswife volunteered her concern over his lifestyle offrenetic activity, running and cycling over 10 milesper day, eating very little and having lost 7 kg inweight over the previous six months. On examinationhe was clearly wasted and thin, weight 50 kg withabsent body fat, muscle wasting and mild ankleoedema. He was thought to be suffering fromanorexia nervosa and was referred for a hospitalopinion.
Initial investigations showed that he had a haemo-globin of 11t8 g/dl (NR 12 5-17 5 g/dl), mean cellvolume 102 fl (NR 76-100 fl), leucocyte count 3 0x109/l (NR 4-11x109/l), lymphocyte count 1ix101/l(NR 1-5-4x109/l) and platelet count 205x109/l (NR150-450x 10"/1)). Erythrocyte sedimentation ratewas 58 mm/h. There was no folate, B12 or irondeficiency. Serum biochemical measurements re-vealed normal liver function tests (alkaline phos-phatase 48 U/l (NR 30-135 U/I), ALT 48(NR 7-40 U/I), bilirubin 7 ,umol/l (NR 2-17 Ftmol/l))but he was consistently hypoproteinaemic with a totalprotein concentration varying between 41-46 g/l (NR63-83 g/l) and albumin concentrations ranging from18-24 g/l (NR 30-51 g/l). Immunoglobulin levelswere low normal. Concentrations of calcium,magnesium and zinc were normal corrected forserum albumin. The urine contained no protein andrenal function and plasma electrolytes were alsonormal.
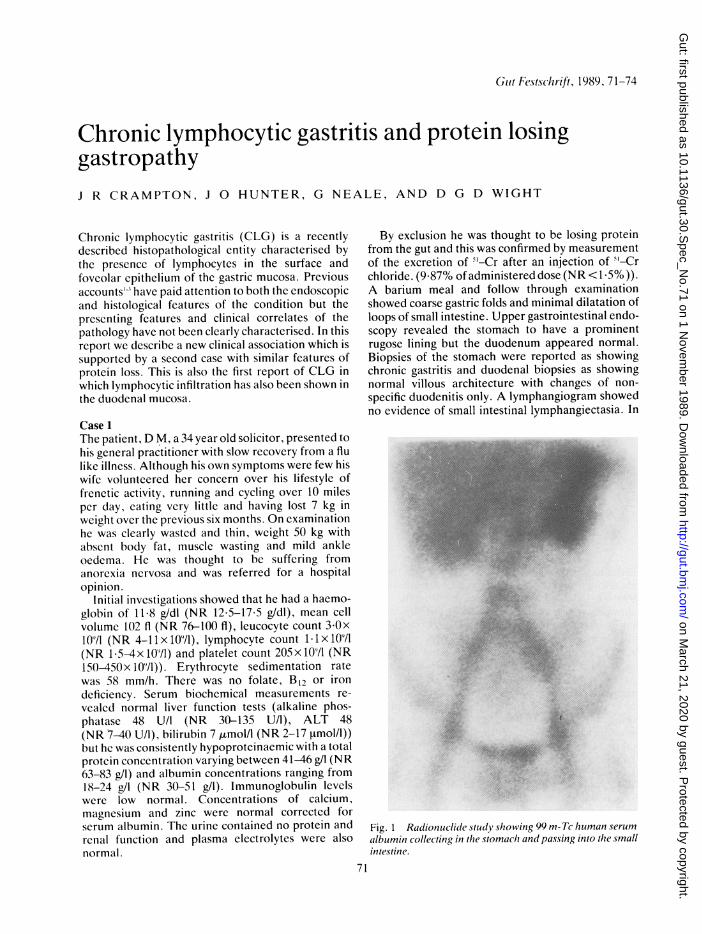
By exclusion he was thought to be losing proteinfrom the gut and this was confirmed by measurementof the excretion of >'-Cr after an injection of '-Crchloride. (9.87% of administered dose (NR < 1.5%)).A barium meal and follow through examinationshowed coarse gastric folds and minimal dilatation ofloops of small intestine. Upper gastrointestinal endo-scopy revealed the stomach to have a prominentrugose lining but the duodenum appeared normal.Biopsies of the stomach were reported as showingchronic gastritis and duodenal biopsies as showingnormal villous architecture with changes of non-specific duodenitis only. A lymphangiogram showedno evidence of small intestinal lymphangiectasia. In
Fig. 1 Radionuclide study showing 99 m- Tc human serumalbumin collecting in tlhe stomaclh and passing into the smallintestine.
71
on March 21, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.30.S
pec_No.71 on 1 N
ovember 1989. D
ownloaded from
72Cranipton, Hluniter, Neale, antii1 Wiglt
M t s i l *'ie sum?
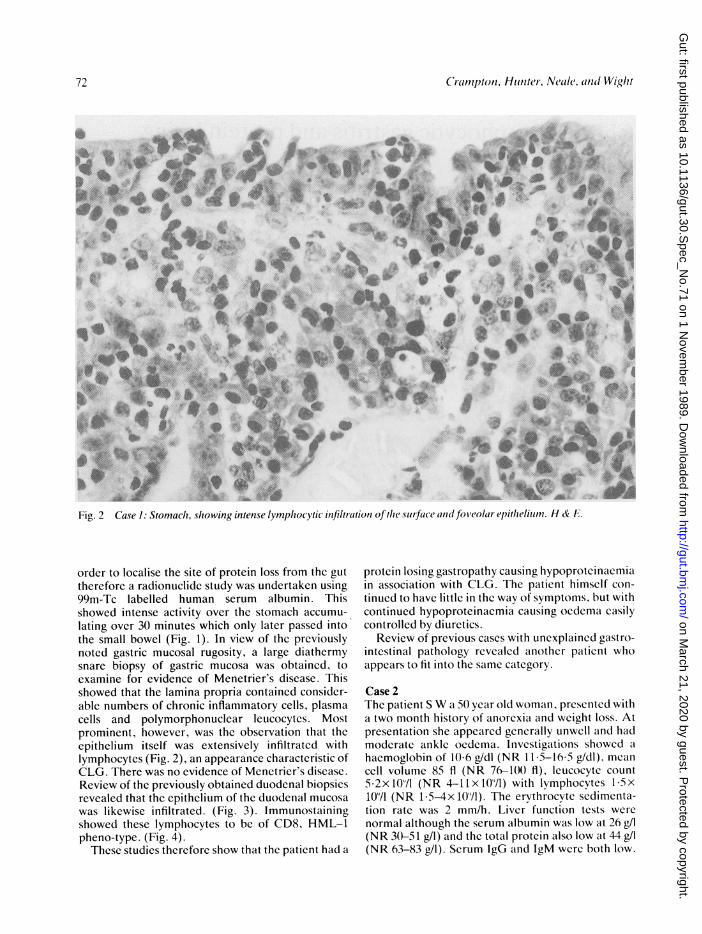
Fig. 2 Case 1: Stomach, showing intense lymphlocytic infiltration of t/ic .surface and lfolear(l ep)itlheliutn. H & F .
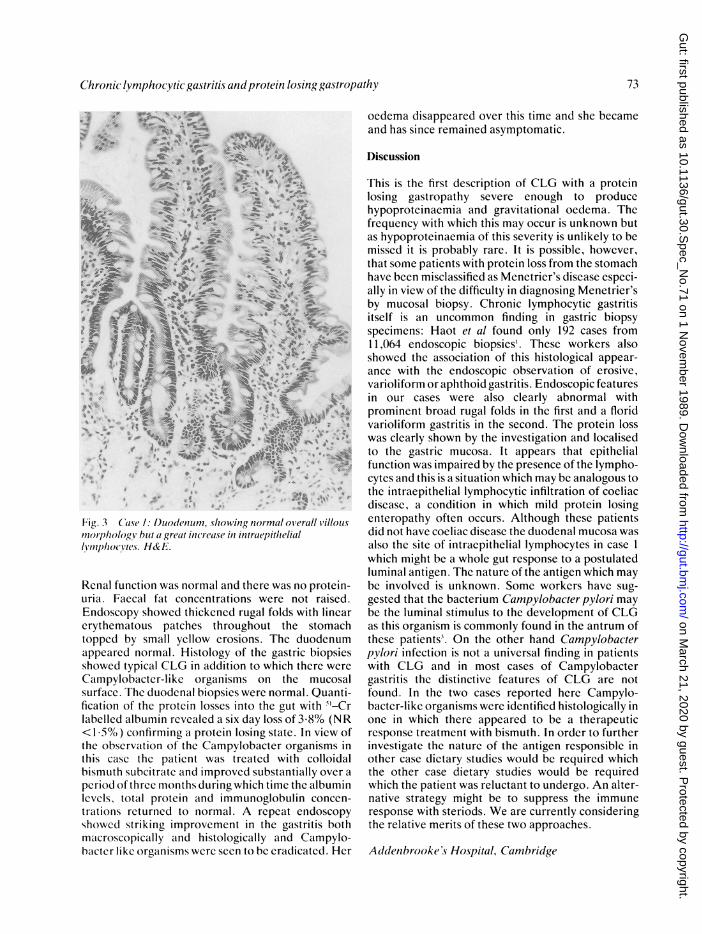
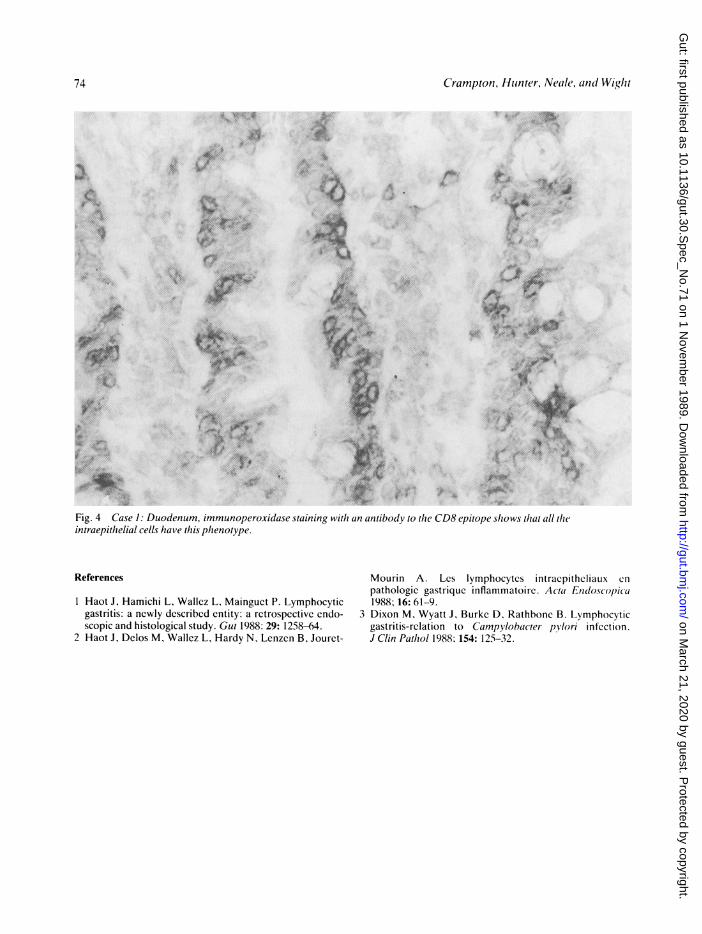
order to localise the site of protein loss from the guttherefore a radionuclide study was undertaken using99m-Tc labelled human serum albumin. Thisshowed intense activity over the stomach accumu-lating over 30 minutes which only later passed intothe small bowel (Fig. 1). In view of the previouslynoted gastric mucosal rugosity, a large diathermysnare biopsy of gastric mucosa was obtained, toexamine for evidence of Menetrier's disease. Thisshowed that the lamina propria contained consider-able numbers of chronic inflammatory cells, plasmacells and polymorphonuclear leucocytes. Mostprominent, however, was the observation that theepithelium itself was extensively infiltrated withlymphocytes (Fig. 2), an appearance characteristic ofCLG. There was no evidence of Menetrier's disease.Review of the previously obtained duodenal biopsiesrevealed that the epithelium of the duodenal mucosawas likewise infiltrated. (Fig. 3). Immunostainingshowed these lymphocytes to be of CD8, HML-1pheno-type. (Fig. 4).These studies therefore show that the patient had a
protein losing gastropathy causing hypoproteinaemiain association with CLG. The patient himself con-tinued to have little in the way of symptoms, but withcontinued hypoproteinaemia causing oedema easilycontrolled by diuretics.
Review of previous cases with unexplained gastro-intestinal pathology revealed another patient whoappears to fit into the same category.
Case 2The patient S W a 50 year old woman, presented witha two month history of anorexia and weight loss. Atpresentation she appeared generally unwell and hadmoderate ankle oedema. Investigations showed ahaemoglobin of 10-6 g/dl (NR 11 5-16-5 g/dl), meanccll volume 85 fl (NR 76-10() fl), leucocyte count5 2x109/l (NR 4-11xlO"/l) with lvmphocvtes 15x1071 (NR 1-5-4xlO"/l). The ervthrocyte sedimenta-tion rate was 2 mm/h. Liver function tests werenormal although the serum albumin was low at 26 g/l(NR 3(0-51 g/l) and the total protein also low at 44 g/l(NR 63-83 g/l). Serum IgG and IgM were both low.
72
on March 21, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.30.S
pec_No.71 on 1 N
ovember 1989. D
ownloaded from
Chronic lymphocytic gastritis andprotein losing gastropathy
S:
.4~~~~~~~~~~~~~
*t ?2 ; ^ *
Fig. 3 (atIs : ljuodeniun,s, owing nor-mal ooverallliilloulsmorphology 1)11t a greal itic'rcease in intraepitheliallWnpho(Y'tes. H& F.
Renal function was normal and there was no protein-uria. Faccal fat concentrations were not raised.Endoscopy showed thickened rugal folds with linearerythematous patches throughout the stomachtopped by small yellow erosions. The duodenumappeared normal. Histology of the gastric biopsiesshowed typical CLG in addition to which there were
Campylobacter-like organisms on the mucosalsurface. The duodenal biopsies were normal. Quanti-fication of the protein losses into the gut with 5'-Crlabelled albumin revealed a six day loss of 3 8% (NR< I 55%) confirming a protein losing state. In view ofthe observation of the Campylobacter organisms inthis case the patient was treated with colloidalbismuth subcitrate and improved substantially over a
period of three months during which time the albuminlevels, total protein and immunoglobulin concen-trations returned to normal. A repeat endoscopyshowed striking improvement in the gastritis bothmacroscopically and histologically and Campylo-bacter like organisms were seen to be eradicated. Her
oedema disappeared over this time and she becameand has since remained asymptomatic.
Discussion
This is the first description of CLG with a proteinlosing gastropathy severe enough to producehypoproteinaemia and gravitational oedema. Thefrequency with which this may occur is unknown butas hypoproteinaemia of this severity is unlikely to bemissed it is probably rare. It is possible, however,that some patients with protein loss from the stomachhave been misclassified as Menetrier's disease especi-ally in view of the difficulty in diagnosing Menetrier'sby mucosal biopsy. Chronic lymphocytic gastritisitself is an uncommon finding in gastric biopsyspecimens: Haot et al found only 192 cases from11,064 endoscopic biopsies'. These workers alsoshowed the association of this histological appear-ance with the endoscopic observation of erosive,varioliform or aphthoid gastritis. Endoscopic featuresin our cases were also clearly abnormal withprominent broad rugal folds in the first and a floridvarioliform gastritis in the second. The protein losswas clearly shown by the investigation and localisedto the gastric mucosa. It appears that epithelialfunction was impaired by the presence of the lympho-cytes and this is a situation which may be analogous tothe intraepithelial lymphocytic infiltration of coeliacdisease, a condition in which mild protein losingenteropathy often occurs. Although these patientsdid not have coeliac disease the duodenal mucosa wasalso the site of intraepithelial lymphocytes in case 1which might be a whole gut response to a postulatedluminal antigen. The nature of the antigen which maybe involved is unknown. Some workers have sug-gested that the bacterium Campylobacterpylori maybe the luminal stimulus to the development of CLGas this organism is commonly found in the antrum ofthese patients. On the other hand Campylobacterpylori infection is not a universal finding in patientswith CLG and in most cases of Campylobactergastritis the distinctive features of CLG are notfound. In the two cases reported here Campylo-bacter-like organisms were identified histologically inone in which there appeared to be a therapeuticresponse treatment with bismuth. In order to furtherinvestigate the nature of the antigen responsible inother case dietary studies would be required whichthe other case dietary studies would be requiredwhich the patient was reluctant to undergo. An alter-native strategy might be to suppress the immuneresponse with steriods. We are currently consideringthe relative merits of these two approaches.
Addenbrooke 's Hospital, Cambridge
73
on March 21, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.30.S
pec_No.71 on 1 N
ovember 1989. D
ownloaded from
74 Crampton, Hunter, Neale, and Wight
7XF -Ait~~
I~~~~~~~~~~~~~~~~~~~~~~~~~~~~~I
Fig. 4 Case 1: Duodenum, immunoperoxidase staining with an antibody to the CD8 epitope shows that all theintraepithelial cells have this phenotype.
References
1 Haot J, Hamichi L, Wallez L, Mainguet P. Lymphocyticgastritis: a newly described entity: a retrospective endo-scopic and histological study. Gut 1988: 29: 1258-64.
2 Haot J, Delos M, Wallez L, Hardy N, Lenzen B, Jouret-
Mourin A. Lcs lymphocytes intraepitheliaux cnpathologic gastrique inflammatoire. Acta Endoscopfica1988; 16: 61-9.
3 Dixon M, Wyatt J, Burke D, Rathbone B. Lymphocyticgastritis-relation to Campylobacter pylori infection.J Clin Pathol 1988; 154: 125-32.
on March 21, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.30.S
pec_No.71 on 1 N
ovember 1989. D
ownloaded from

















![Review Article Current Perspectives in NSAID-Induced ... · reducing the NSAID-induced gastropathy [ ].... Acid Suppressants. Acid increases NSAID-induced mucosal injury and gastric](https://img.pdfslide.us/doc/110x75/60b703eed9b43379f63b197c/review-article-current-perspectives-in-nsaid-induced-reducing-the-nsaid-induced.jpg)










