Embed Size (px)
Citation preview
CHRONIC LYMPHOCYTIC LEUKEMIA (CLL)
Curs an IV – limba engleza
2012-2013
04/19/23 2
CLL - Definition
• CLL is a neoplastic disease characterized by proliferation and accumulation (blood, marrow and lymphoid organs) of morphologically mature but immunologically dysfunctional lymphocytes
CLL - Definition
• Clonal B cell malignancy.
• Progressive accumulation of long lived mature lymphocytes.
• Increase in anti-apoptotic protein bcl-2.
• In most cases, the cells are monoclonal B lymphocytes that are CD5+
• Intermediate stage between pre-B and mature B-cell.
• T cell CLL can occur rarely
Cancer statastics 2000; CA J Clin 2000; 50:7-33
CLL - Epidemiology
• Most common leukemia of Western world.
• Less frequent in Asia and Latin America.
• Male to female ratio is 2:1.
• Median age at diagnosis is 65-70 years.
• Uncommon (10%) in patients under 50 years
• In US population incidence is similar in different races.
CLL - Etiology (1)
• The cause of CLL is unknown
• There is increased incidence in farmers, rubber manufacturing workers, asbestos workers, and tire repair workers
• Genetic factors have been postulated to play a role in high incidence of CLL in some families
CLL - Etiology (2)
• Cytogenetics– clonal chromosomal abnormalities are detected in
approximately 50% of CLL patients – the most common clonal abnormalities are:
• trisomy 12• structural abnormalities of chromosomes 13, 14 and 11
– patients with abnormal karyotypes have a worse prognosis
• Oncogenes– in most cases of CLL is overexpressed the proto-
oncogene c-fgr 9a member of the src gene family of tyrosine kinases
CLL – Initial symptoms
• Approximately 40% are asymptomatic at diagnosis – discovered by a CBC
• In symptomatic cases the most common complaint is fatigue
• Well’s syndrome – increase sensitivity to insects bites
• B symptoms – fever, sweats, weight loss
• Less often the initial complaint are enlarged nodes or the development of an infection (bacterial)
CLL - Clinical findings• Most symptomatic patients have enlarged lymph nodes
(more commonly cervical and supraclavicular) and splenomegaly
• The lymph nodes are usually discrete, freely movable, and nontender
• Hepatomegaly may occure• Less common manifestation are infiltration of tonsils,
mesenteric or retroperitoneal lymphadenopathy, and skin infiltration
• Patients rarely present with features of anemia, and bruising or bleeding
CLL – Lab findings a) Blood test lymphocytosis ≥ 5G/l (4 weeks)
b) Morphology monoconal population of small mature lymphocyte
c) B-cell CLL phenotype clonal CD5+/CD19+ population of lymphocyte
d) Markers of clonality κ/λ light chain restriction; cytogenetical abnormalities
e) Bone marrow infiltrate > 30% of nuceated cells on aspirate
f) Lymph node diffuse infiltrate of small lymphocye
CLL - Laboratory findings (1)
• The blood lymphocyte count above 5.000/mmc
• Leukemic cells have the morphologic appearance of
normal small lymphocytes
• In the blood smears are commonly seen ruptured
lymphocytes (“basket” or “smudge” cells)
• Careful examination of the blood smear can usually
differentiate CLL, and the diagnosis can be confirmed
by immunophenotyping
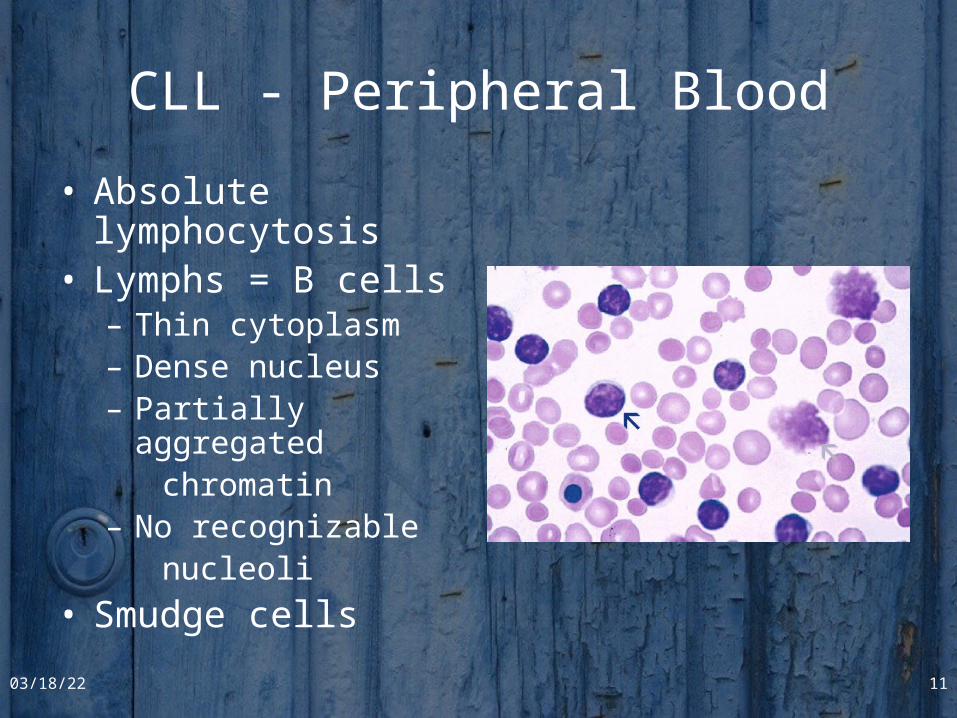
CLL - Peripheral Blood
• Absolute lymphocytosis• Lymphs = B cells
– Thin cytoplasm– Dense nucleus – Partially aggregated chromatin– No recognizable nucleoli
• Smudge cells
04/19/23 11
CLL - Laboratory findings (2)
• Clonal expansion of B (99%) or T(1%) lymphocyte– In B-cell CLL clonality is confirmed by
• the expression of either or light chains on the cell surface membrane
• the presence of unique idiotypic specificities on the immunoglobulins produced by CLL cells
• by immunoglobulin gene rearrangements• typical B-cell CLL are unique in being CD19+ and CD5+
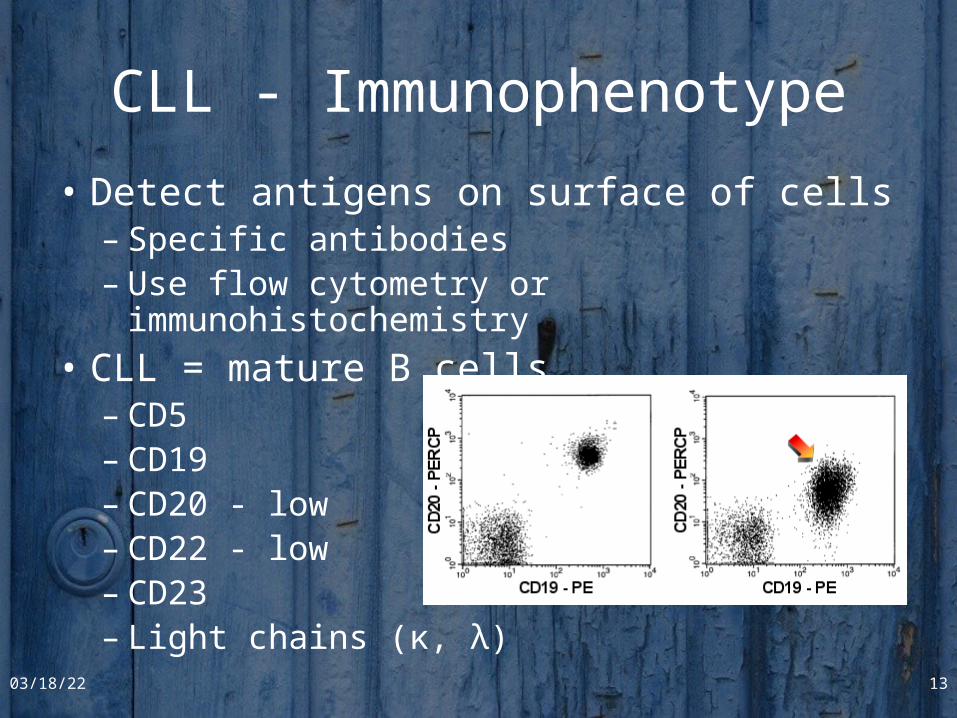
CLL - Immunophenotype
• Detect antigens on surface of cells – Specific antibodies– Use flow cytometry or immunohistochemistry
• CLL = mature B cells– CD5– CD19– CD20 - low– CD22 - low– CD23– Light chains (κ, λ)
04/19/23 13
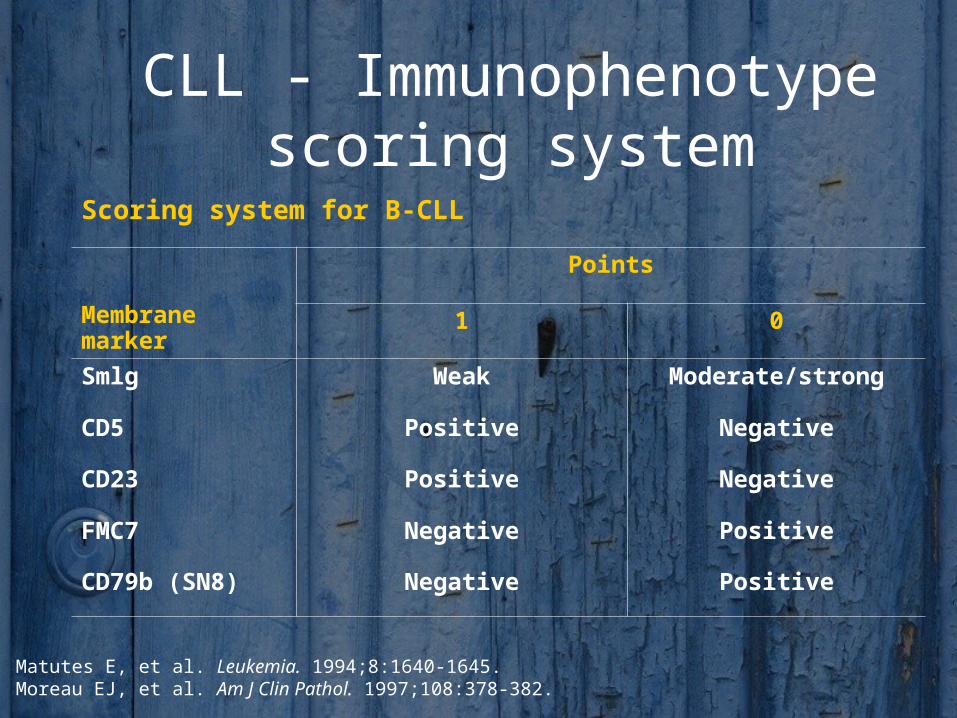
CLL - Immunophenotype scoring system
Scoring system for B-CLL
Membrane marker
Points
1 0
Smlg Weak Moderate/strong
CD5 Positive Negative
CD23 Positive Negative
FMC7 Negative Positive
CD79b (SN8) Negative Positive
1. Matutes E, et al. Leukemia. 1994;8:1640-1645.2. Moreau EJ, et al. Am J Clin Pathol. 1997;108:378-382.
CLL – Other lab tests
• Hypogammaglobulinemia or agamma-globulinemia are often observed
• 10 - 25% of patients with CLL develop autoimmune hemolytic anemia, with a positive direct Coombs’ test
• The marrow aspirates shows greater than 30% of the nucleated cells as being lymphoid
04/19/23 15
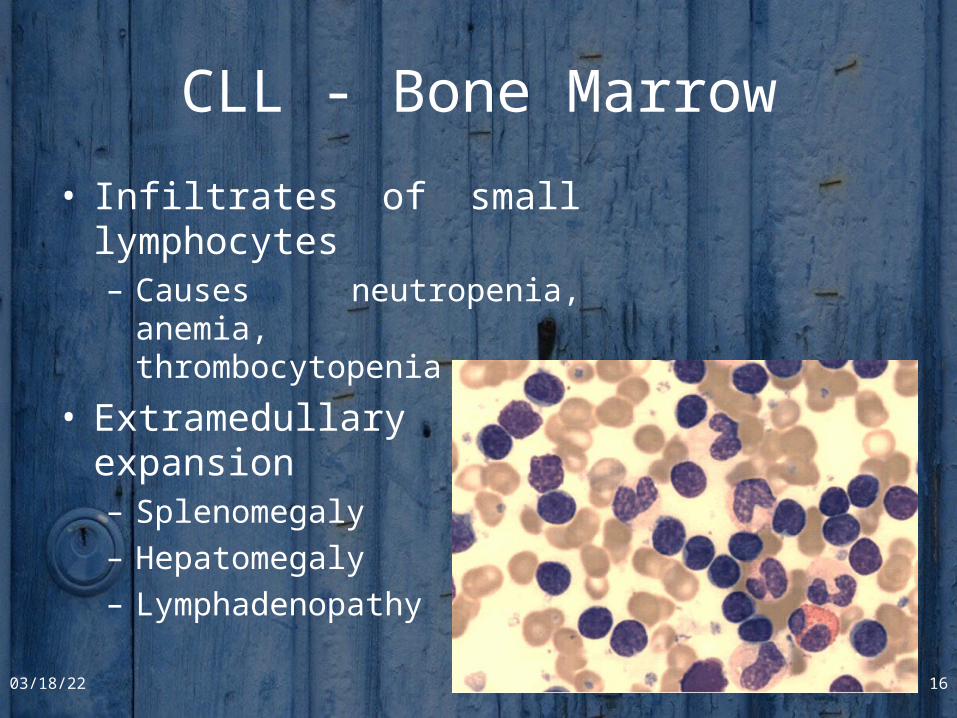
CLL - Bone Marrow
• Infiltrates of small lymphocytes– Causes neutropenia, anemia,
thrombocytopenia
• Extramedullary expansion– Splenomegaly
– Hepatomegaly
– Lymphadenopathy
04/19/23 16
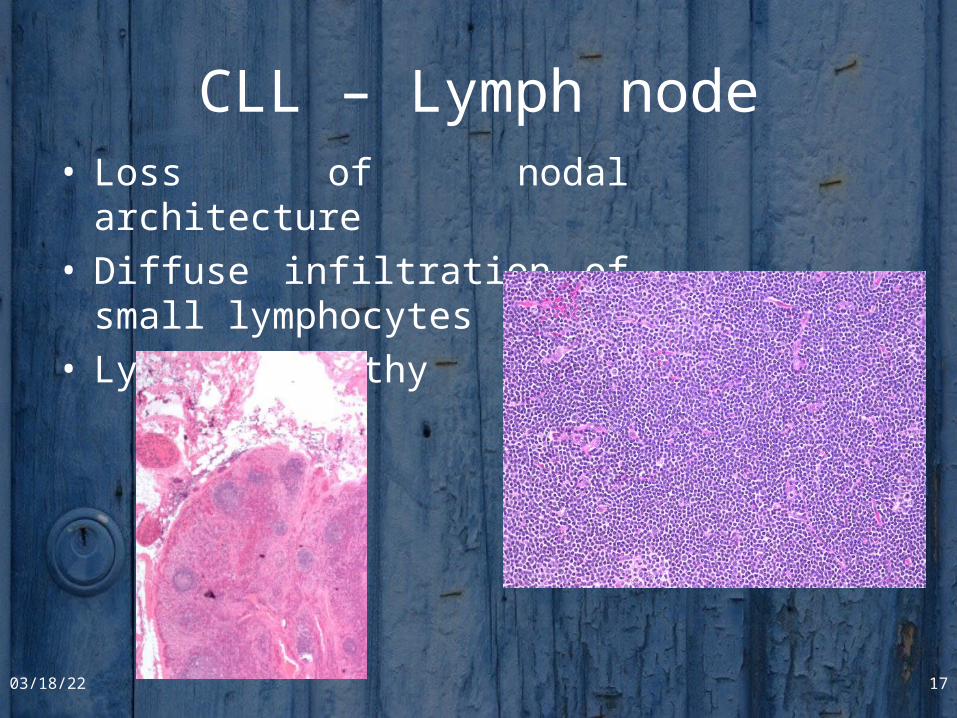
CLL – Lymph node• Loss of nodal architecture• Diffuse infiltration of small
lymphocytes• Lymphadenopathy
04/19/23 17
CLL - diagnostic criteria
1) A peripheral blood lymphocyte count of greater than 5 G/L, with less than 55% of the cells being atypical
2) The cell should have the presence of Bcell-specific differentiation antigens (CD19, CD20, and CD24) and be CD5(+)
3) A bone marrow aspirates showing greater than 30% lymphocytes
CLL - Differential diagnosis
• Infectious causes– bacterial (tuberculosis)– viral (mononucleosis)
• Malignant causes– B-cell– T-cell
• leukemic phase of non-Hodgkin lymphomas
• Hairy-cell leukemia
• Waldenstrom macroglobulinemia
• large granular lymphocytic leukemia
Investigations
• Pretreatment studies of patients with CLL should include examination of:– complete blood count– peripheral blood smear– reticulocyte count– Coomb’s test– renal and liver function tests – serum protein electrophoresis– immunoglobulin levels– plasma 2 microglobulin level
• If available immunophenotyping should be carried out to confirm the diagnosis
• Bone marrow biopsy and cytogenetic analysis is not routinely performed in CLL
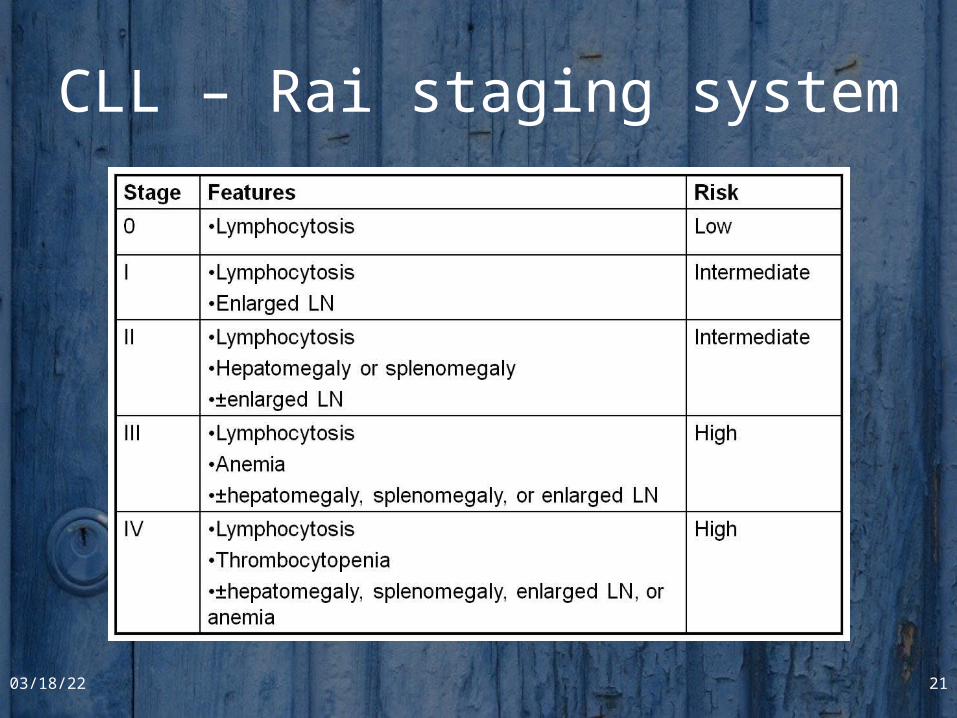
CLL – Rai staging system
04/19/23 21
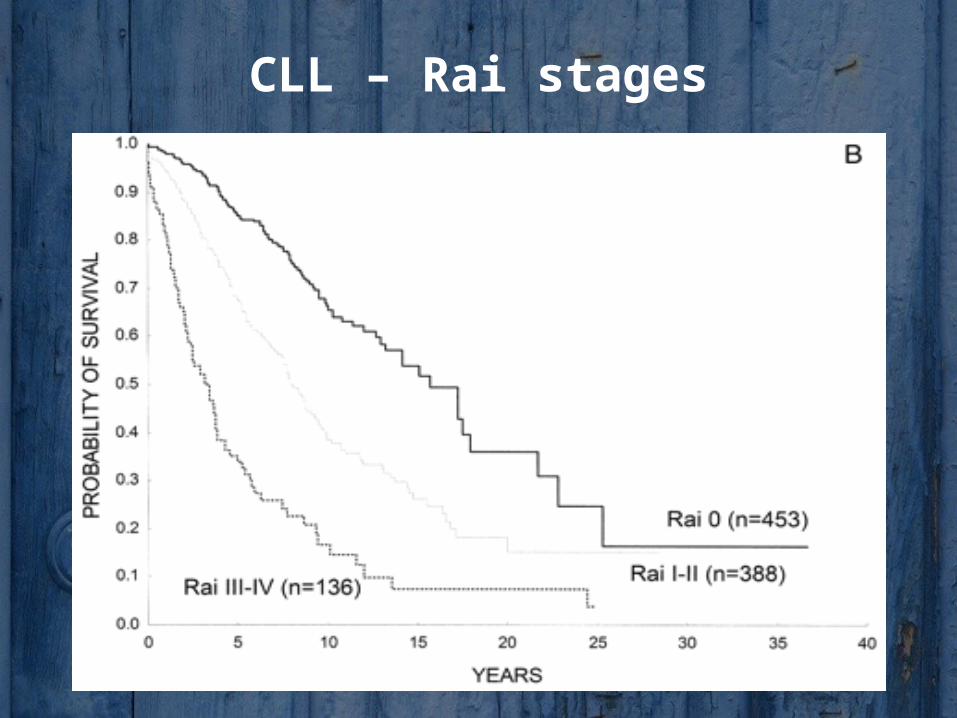
CLL – Rai stages
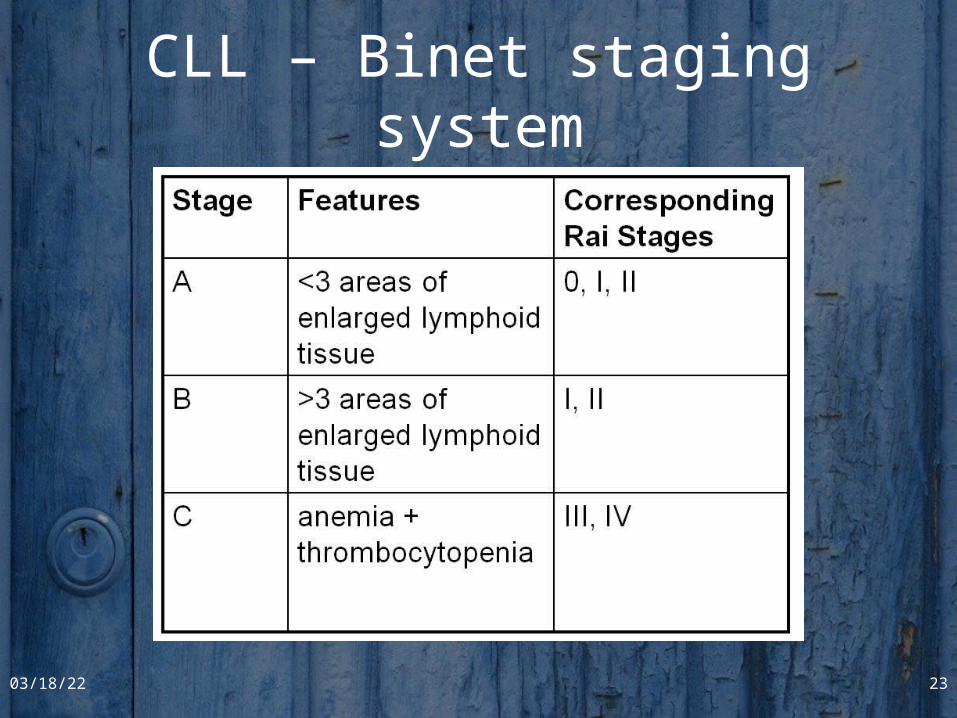
CLL – Binet staging system
04/19/23 23
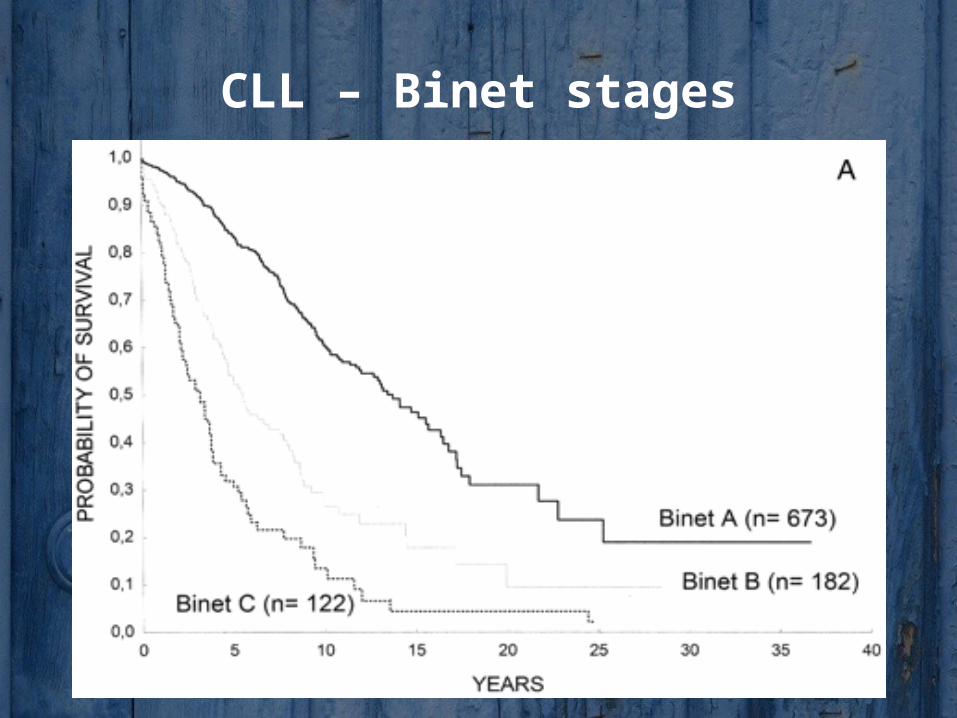
CLL – Binet stages
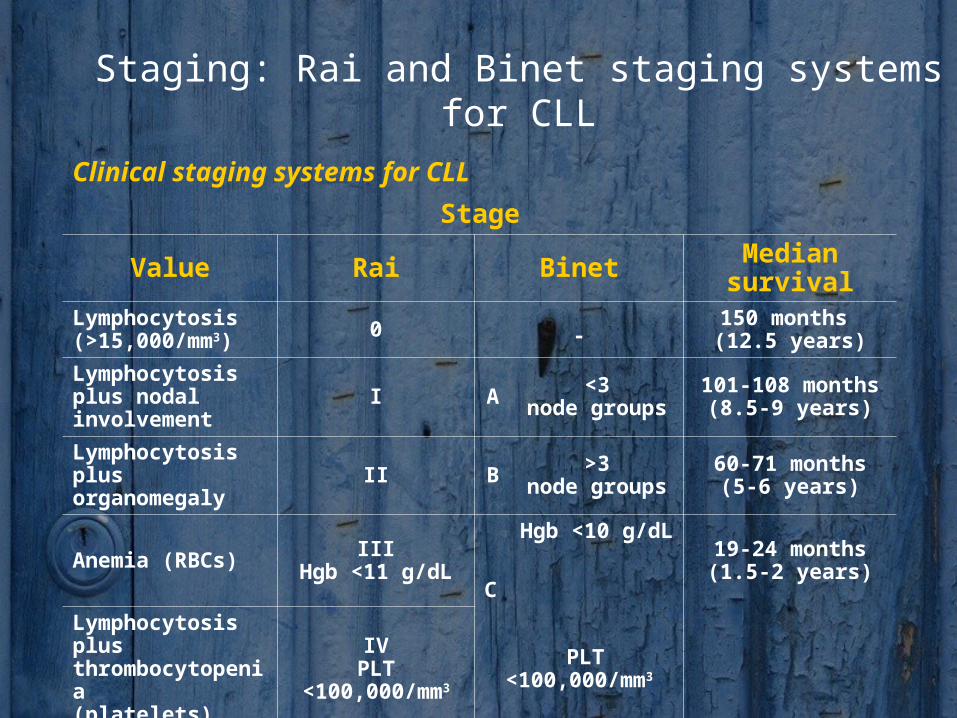
Staging: Rai and Binet staging systems for CLL
Clinical staging systems for CLL
Stage
Value Rai Binet Median survivalLymphocytosis (>15,000/mm3) 0 -
150 months (12.5 years)
Lymphocytosis plus nodal involvement I A <3
node groups101-108 months
(8.5-9 years)
Lymphocytosis plus organomegaly II B >3
node groups60-71 months
(5-6 years)
Anemia (RBCs) IIIHgb <11 g/dL
C
Hgb <10 g/dL 19-24 months
(1.5-2 years)
Lymphocytosis plus thrombocytopenia(platelets)
IVPLT <100,000/mm3 PLT <100,000/mm3
CLL - Markers of poor prognosis
• Advanced Rai or Binet stage
• Peripheral lymphocyte doubling time <12 months
• Diffuse marrow histology
• Increased number of prolymphocytes or cleaved cells
• Poor response to chemotherapy• High 2- microglobulin level
• Abnormal karyotyping
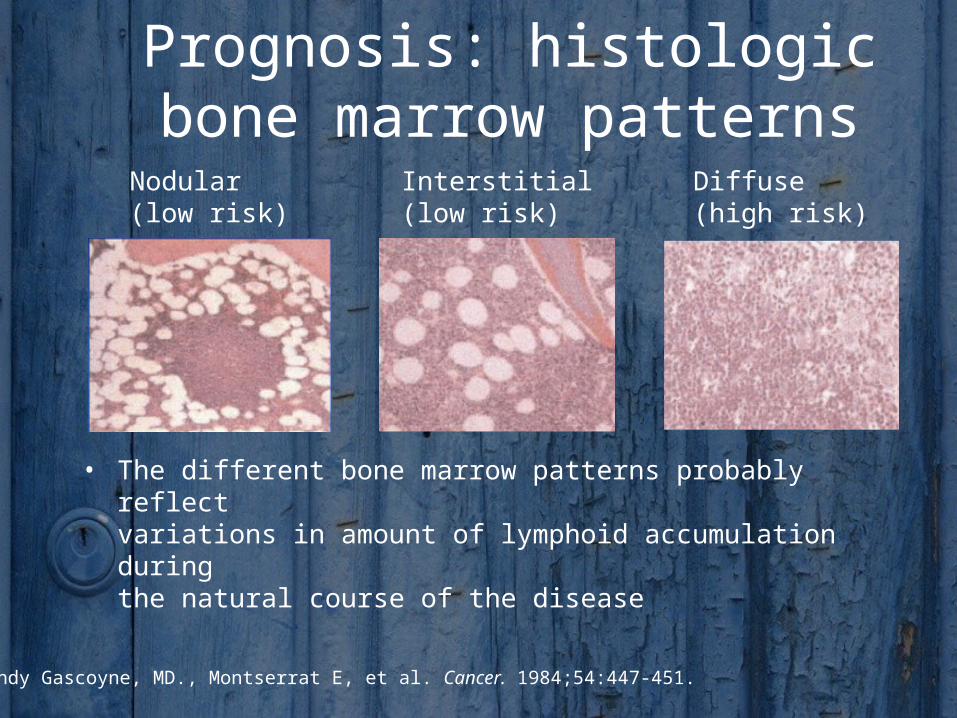
Prognosis: histologic bone marrow patterns
• The different bone marrow patterns probably reflectvariations in amount of lymphoid accumulation duringthe natural course of the disease
Interstitial(low risk)
Diffuse(high risk)
Nodular(low risk)
Randy Gascoyne, MD., Montserrat E, et al. Cancer. 1984;54:447-451.
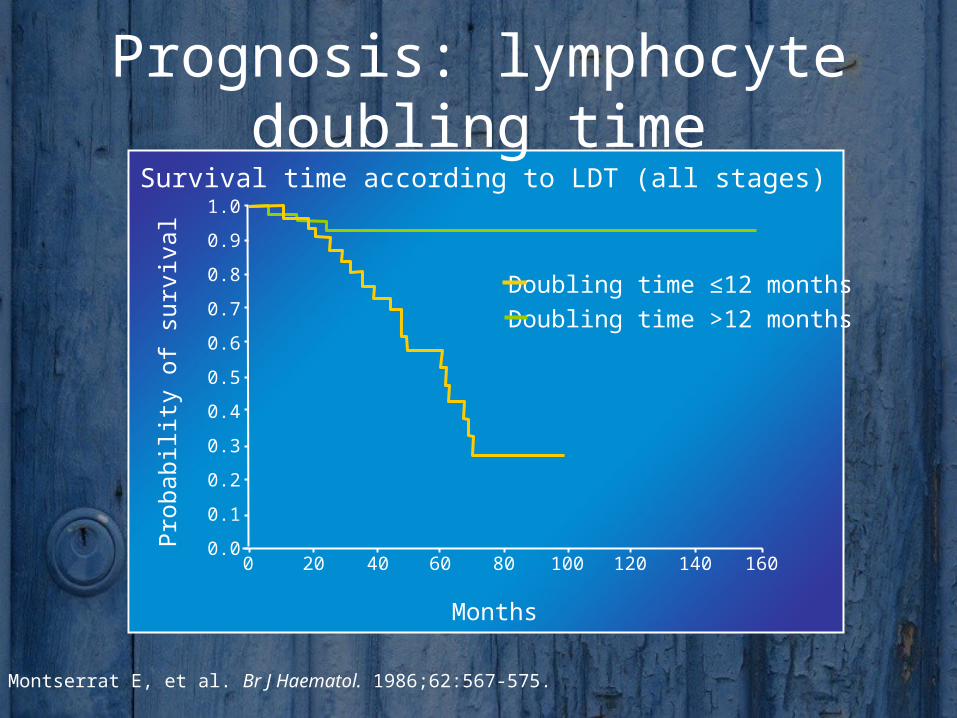
Prognosis: lymphocyte doubling time
Survival time according to LDT (all stages)
Months
Pro
babili
ty o
f su
rviv
al
1600 20 40 60 80 100 120 140
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
Doubling time ≤12 monthsDoubling time >12 months
1. Montserrat E, et al. Br J Haematol. 1986;62:567-575.
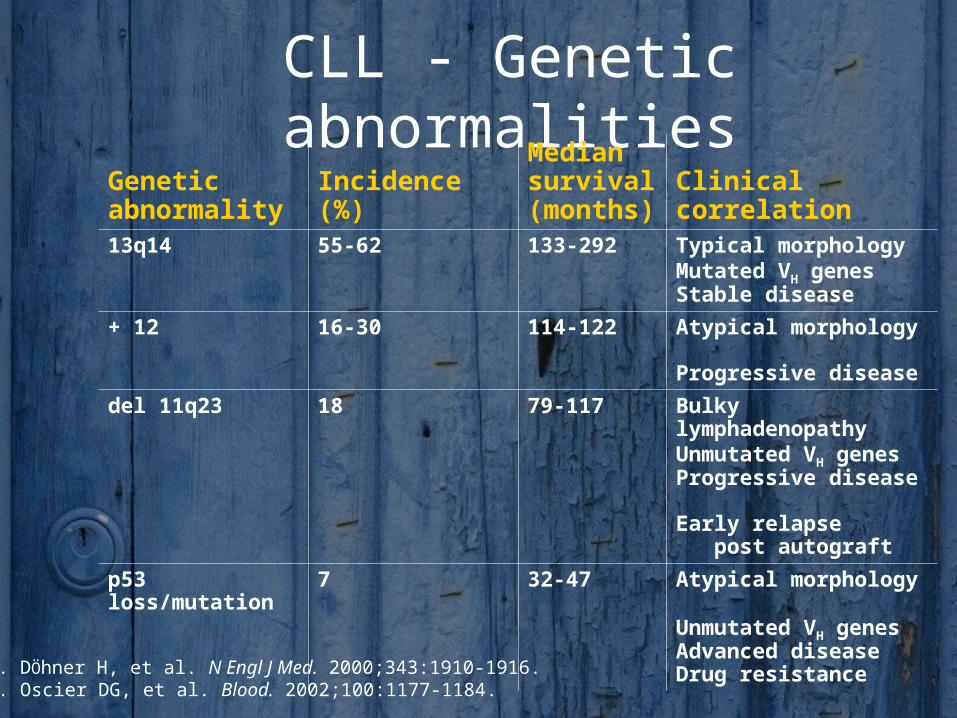
CLL - Genetic abnormalities
Genetic abnormality
Incidence (%)
Median survival (months)
Clinical correlation
13q14 55-62 133-292 Typical morphology Mutated VH genes Stable disease
+ 12 16-30 114-122 Atypical morphology
Progressive disease
del 11q23 18 79-117 Bulky lymphadenopathy Unmutated VH genes
Progressive disease Early relapse post autograft
p53loss/mutation
7 32-47 Atypical morphology
Unmutated VH genes
Advanced disease Drug resistance
1. DÖhner H, et al. N Engl J Med. 2000;343:1910-1916.2. Oscier DG, et al. Blood. 2002;100:1177-1184.
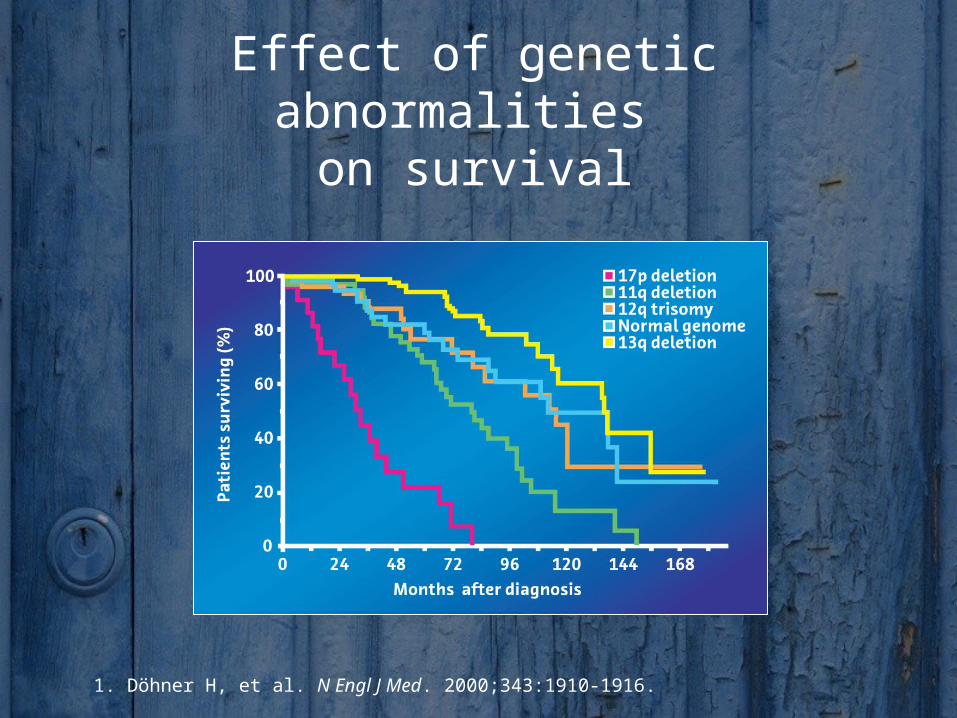
Effect of genetic abnormalities on survival
1. Döhner H, et al. N Engl J Med. 2000;343:1910-1916.
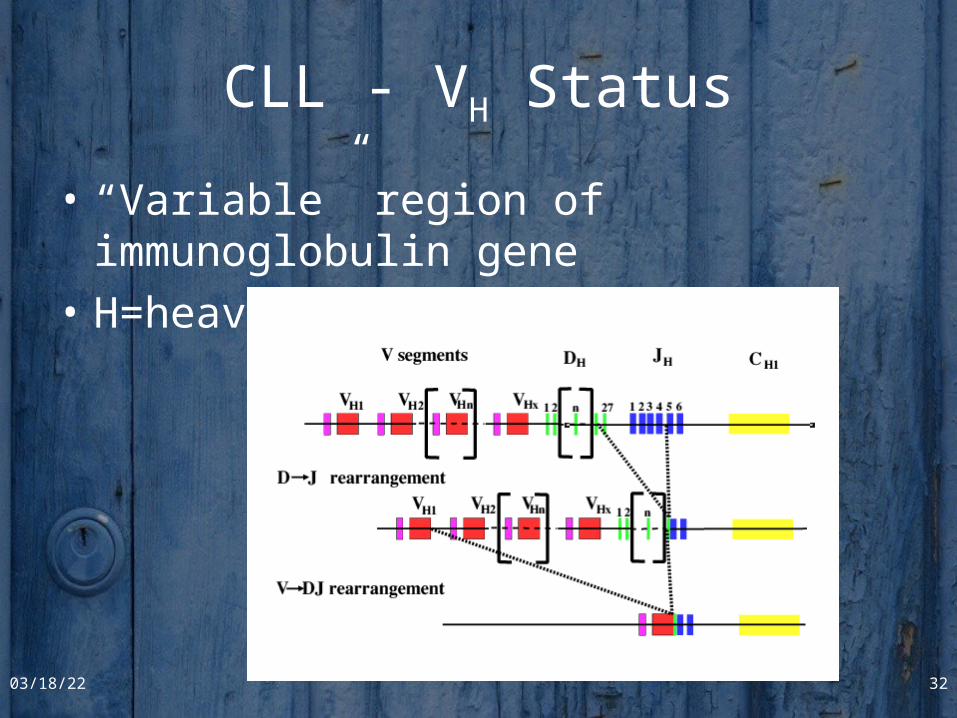
CLL - VH Status
• “Variable” region of immunoglobulin gene
• H=heavy chain
04/19/23 32
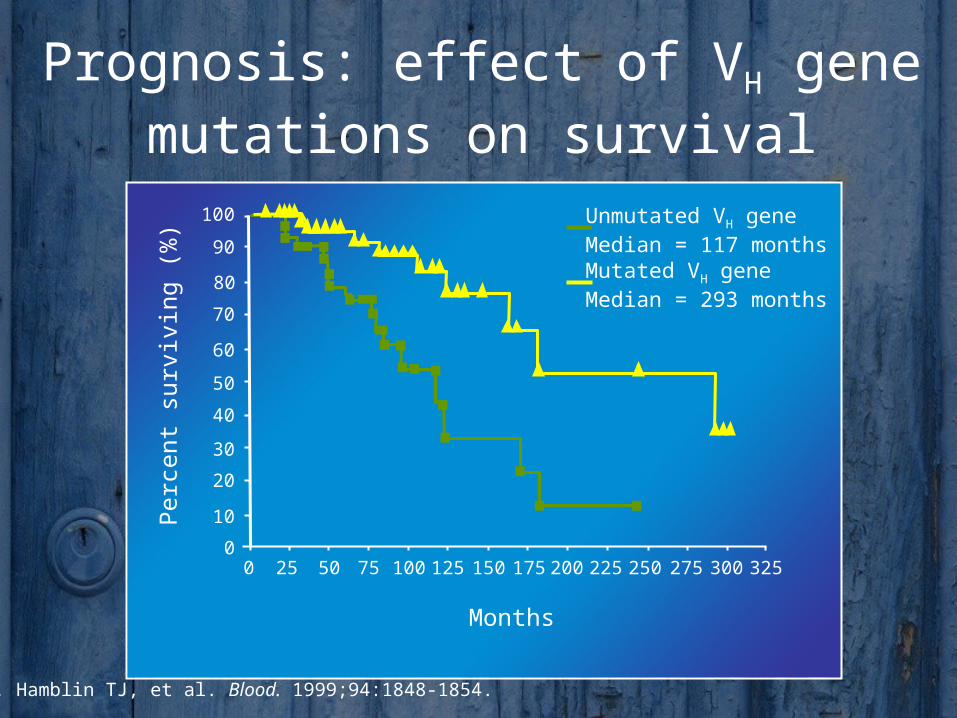
CLL - VH Mutation
• Naïve B cells have unmutated V regions– Make initial IgM and IgG that bind Ag poorly
• Somatic hypermutation of V region creates memory B cells– Make Ab with higher affinity for Ag
CLL progression is dependent on mutation status of B cells– Unmutated VH = rapid progression, short survival– Mutated VH = slow progression, long survival
04/19/23 33
CLL - VH Mutation
Naïve B cellsUnmutated VH
CLLFast progressionShort survival
Memory B cellsMutated VH
CLLSlow ProgressionLong Survival
90
225 3000 50 100 150 200 25025 75 125 175 275
100
80
60
40
0
20
70
50
30
10
Unmutated VH geneMedian = 117 monthsMutated VH geneMedian = 293 months
325
1. Hamblin TJ, et al. Blood. 1999;94:1848-1854.
Perc
ent
surv
ivin
g (
%)
Months
Prognosis: effect of VH gene mutations on survival
Clinical Course of CLL• Disease has a variable course; however, it often progresses
from an indolent lymphocytosis without other evident disease to one of generalized lymphatic enlargement with concomitant pancytopenia
• Progression: bone marrow impairment, susceptibility to infection
• Complications of pancytopenia, including hemorrhage and infection, represent a major cause of death in these patients
CLL - Immunologic Complications • Autoimmune hemolytic anemia
– Coombs’ positive– Clinical hemolysis
• Pure red cell aplasia• Immune-mediated thrombocytopenia• Depressed immunoglobin levels• Granulocytopenia• Hypogammaglobulinemia with advanced disease• Long-term complications: autoimmune phenomena,
Richter’s transformation
CLL - Complications
• Severe systemic infections
• Bleeding
• Richter’s transformation
• Prolymphocytoid transformation
• Secondary malignancies
• Acute myeloid leukemia
Transforming the way we approach CLL therapy
• Traditional treatment goal: Palliation– Age is a factor
– Treat to relieve symptoms
– Continuous/intermittent treatment
– No survival advantage for any tested treatment to date
• New advances may allow treatment for remissionand survival– Treat to complete remission (CR)
– Eliminate minimal residual disease
– Response predicts for survival: More CRs
CLL – treatment (1)
• Watch and wait• Monotherapy
– glucocorticoids– alkylating agents (Chlorambucil, Cyclophosphamide)– purine analogues (Fludarabine, Cladribine, Pentostatin)
• Combination chemotherapy– Chlorambucil/ Cyclophosphamide + Prednisone– Fludarabine + Cyclophosphamide +/- Mitoxantrone– CVP, CHOP
• Monoclonal antibodies (monotherapy and in combination)– Alemtuzumab (anti-CD52)– Rituximab (anti-CD20)
• Splenectomy• Radiotherapy
CLL – treatment (2)
• Hematopoietic stem cell transplantation– allogeneic with reduced intesity conditioning
– autologous
• New and novel agents– Oblimersen – bcl2-directed antisense oligonucleotide
– Lenalidomide
– Flavopiridol
– Anti-CD23
– Anti-CD40
• Vaccine strategies
• Supportive therapy (allopurinol, G-CSF, blood and platelet transfusion, immunoglobulins, antibiotics)
NCI-WG: Indications to Initiate Treatment for CLL
• Constitutional symptoms referable to CLL (B-symptoms)
• Progressive marrow failure• Autoimmune anemia and/or thrombocytopenia
poorlyresponsive to corticosteroids
• Massive or progressive splenomegaly• Massive or progressive lymphadenopathy• Rapid lymphocyte doubling time
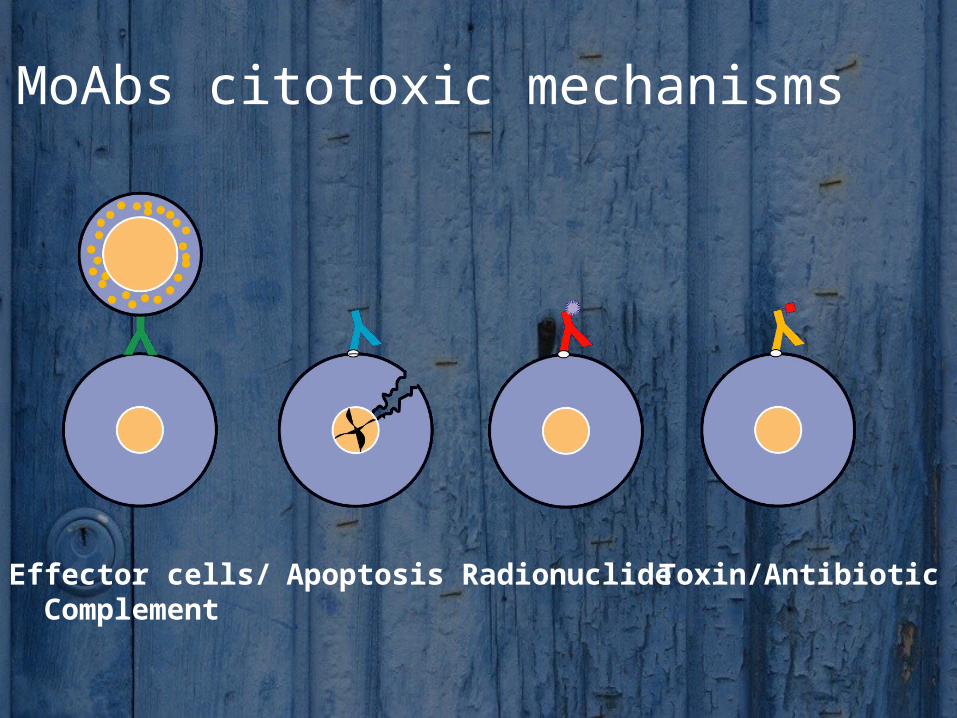
MoAbs citotoxic mechanisms
Effector cells/Complement
Apoptosis Radionuclide Toxin/Antibiotic
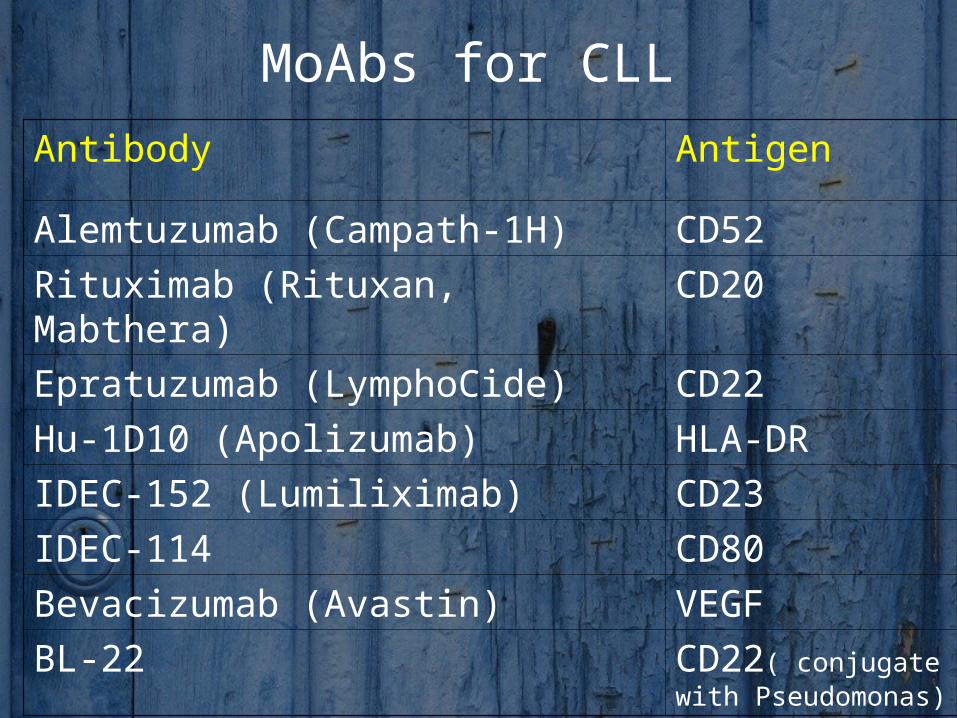
MoAbs for CLL
Antibody Antigen
Alemtuzumab (Campath-1H) CD52
Rituximab (Rituxan, Mabthera) CD20
Epratuzumab (LymphoCide) CD22
Hu-1D10 (Apolizumab) HLA-DR
IDEC-152 (Lumiliximab) CD23
IDEC-114 CD80
Bevacizumab (Avastin) VEGF
BL-22 CD22( conjugate with Pseudomonas)
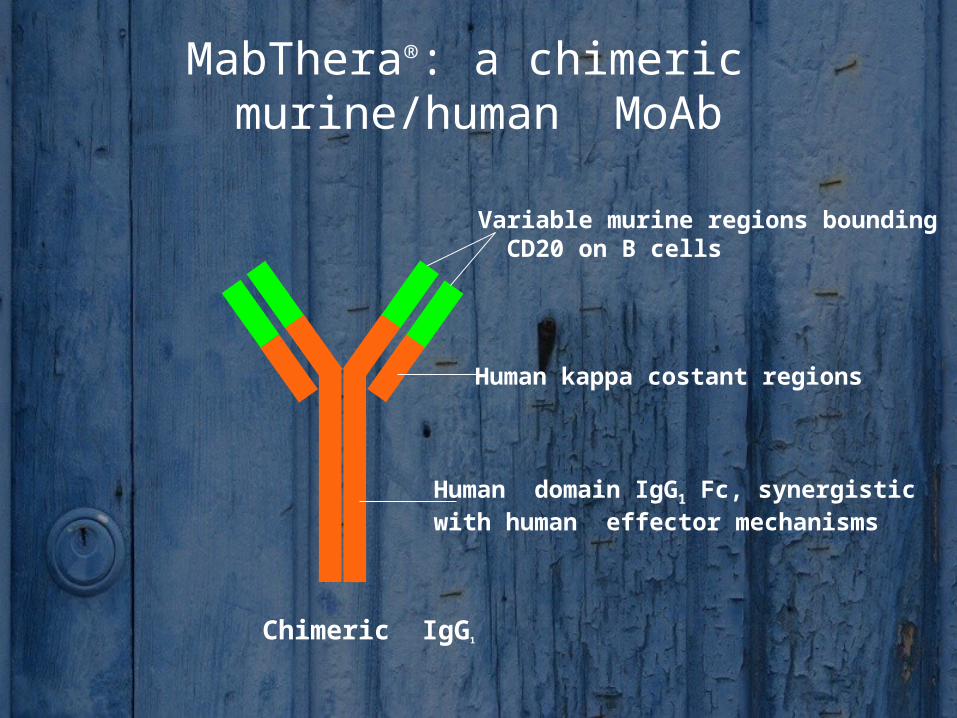
MabThera®: a chimeric murine/human MoAb
Variable murine regions bounding CD20 on B cells
Human kappa costant regions
Human domain IgG1 Fc, synergistic with human effector mechanisms
Chimeric IgG1
Rituximab as part of first-line therapy for CLL: Rationale
• Rituximab monotherapy is moderately active in CLL1,2
– Activity is dose dependent (between 500–2250 mg/m2)1
• Rituximab acts synergistically with other cytotoxic agents in vitro– Increases fludarabine activity in NHL cell lines3
– Increases activity of bendamustine, mitoxantrone and other chemotherapeutic agents in CLL cells4
• Rituximab combination therapies (e.g. R-F, R-FC, R-PC, R-FCM,R-Bendamustine, R-Chlorambucil) are now being assessed
Alemtuzumab (anti-CD52) antibody
IgG1 humanised antibody:Low immunogenicity
CD52 antigen: Highly expressed on
all lymphocytes monocytes and macrophages spermatozoa eosinophils
Not expressed on haemopoietic stem cells
Does not modulate/shed Also expressed on the majority of
malignant lymphocytes
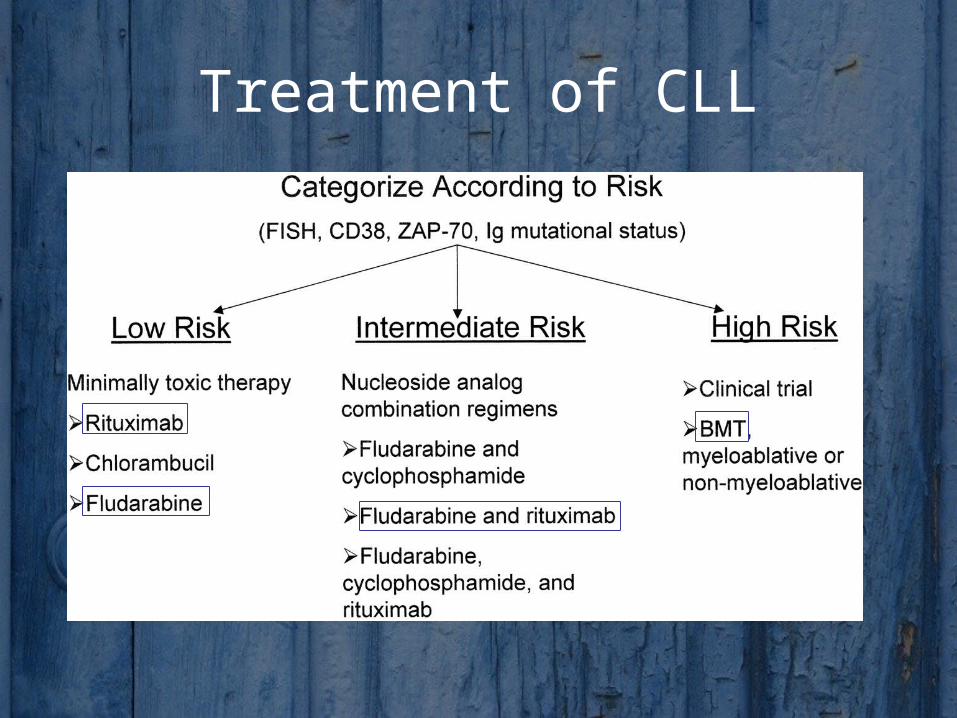
Treatment of CLL
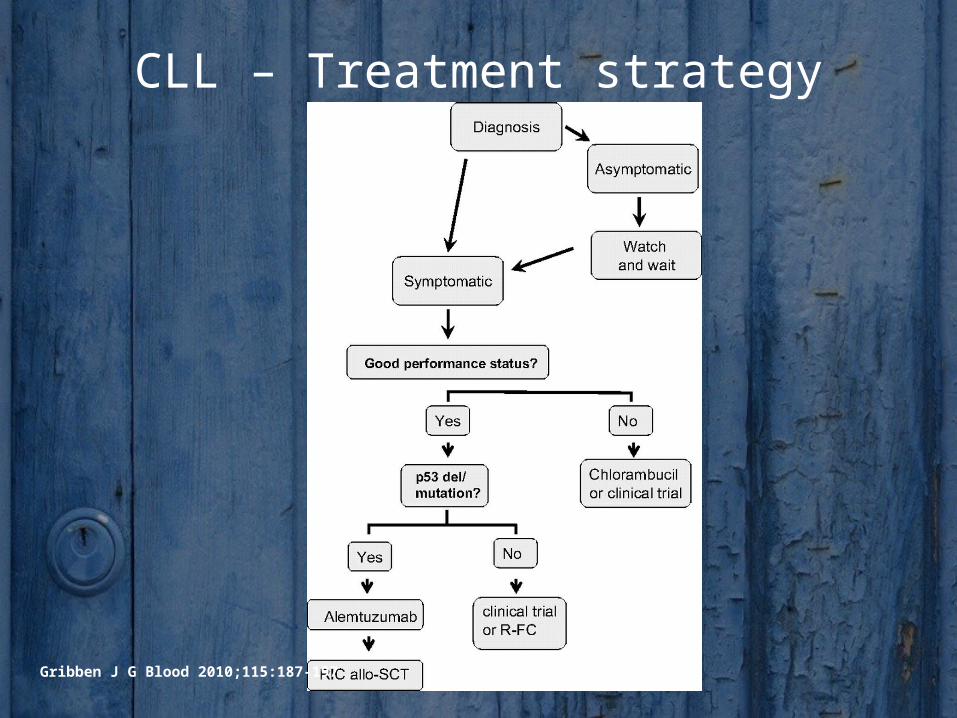
CLL – Treatment strategy
Gribben J G Blood 2010;115:187-197