Embed Size (px)
Citation preview

51
Initiation Progression Complication
hsCRP, MCP-1 OPG, IL-6
TNF-alpha, IL-10
ICAM-1, VCAM-1 E-Selectin, P-Selectin Insulin, Adiponectin
D-dimer
Inflammation Endothelial dysfunction
Insulin resistance Hypercoagulability
Chronic inflamation Immuneactivation/senescence
CD38+HLA-DR+CD8 T cells CD28-CD57+ CD8 T cells, resit. to apoptosis, shortened telomers

Switching strategies (monotherapy & double therapy) in suppressed patients usually consist on:
In the past and now: Replacing 2NRTI+1IP/r by
LPV/r monotherapy (OKT4, PIVOT) DRV/r monotherapy (MONET, MONOI, PROTEA, PIVOT)
LPV/r+3TC (OLE)
ATV/r+3TC (SALT)
DRV/r+3TC (DUAL) DTG +3TC (DOLAM,…..)

A. The HIV infected individual B. The pandemic C. In summary….
Approaches to HIV management: Horizon 2020

B. The pandemic Towards an AIDS free generation ….
in 2030 …… ?
Approaches to HIV management: Horizon 2020


clinicaloptions.com/hiv Starting Antiretroviral Therapy in 2012: A Compendium of Interactive Cases
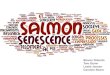
HPTN 052: HIV Transmission Reduced by 96% in Serodiscordant Couples
Single transmission in patient in immediate HAART arm believed to have occurred close to time therapy began and prior to suppression of genital tract HIV
Total HIV-1 Transmission Events: 39 (4 in immediate arm and
35 in delayed arm; P < .001)
Linked Transmissions: 28
Unlinked or TBD Transmissions: 11
P < .001
Immediate Arm: 1
Delayed Arm: 27
Cohen MS, et al. N Engl J Med. 2011;365:493-505.

• “Modelling by UNAIDS indicates that the world has a brief, five-‐year window of opportunity to lay the founda?on to end the AIDS epidemic as a public health threat.”


Cascade of HIV care – Switzerland 2012
81% 80% 79% 71% 68%
0%
20%
40%
60%
80%
100%
HIV Posi?ve People Diagnosed Linked to care Retained in Care On ART Viral Supression <200 copies/ml
12,700 12,300
10,700 11,200
15,700
12,600
Breakpoint 1 Breakpoint
2
Cascade of HIV care, Switzerland 2012

Slide 60 of 44
SIVES, Catalunya june 2013
20% Lack of adherence to general health recommendations
7% Lack of adherence to prescribed ART
25% Lack of diagnosis

61
individuals in care required antiretroviral therapy, but !27%
declined or failed to initiate therapy [47]. We estimate that 80%
of in-care HIV-infected individuals in the United States should
be receiving antiretroviral therapy but that 25% of these in-
dividuals are not receiving therapy. Recent guidelines recom-
mend considering antiretroviral therapy initiation when CD4
cell counts decrease to ,500 cells/lL, which would increase the
proportion of in-care individuals eligible for treatment [48, 49].
Persistence with Antiretroviral TherapyNonpersistence occurs when therapy is halted prematurely.
Patients may stop their medications as a result of medication
adverse effects or competing priorities [50, 51], and providers
may recommend cessation of therapy in response to clinical or
laboratory adverse events or barriers to adherence [52, 53]. In 3
large cohort studies, 4%–6% of individuals who remained in
care discontinued their antiretroviral regimen each year [52, 54,
55].
Adherence to Antiretroviral TherapyA meta-analysis of 31 North American adherence studies found
that 55% of HIV-infected individuals achieve adequate adher-
ence [56]. Because antiretroviral therapy has become more po-
tent, better treatment outcomes can be achieved despite lower
adherence. With modern initial antiretroviral regimens, 70%–
80% adherence leads to durable viral suppression in most
individuals [57, 58]. In 2 recent studies from large North
American cohorts, 60%–80% of individuals achieved adequate
levels of adherence by this new standard [59, 60]. As a consequence
of successful viral suppression at lower levels of adherence, the
population effectiveness of antiretroviral therapy has increased.
Two recent studies found that 78%–87% of individuals receiving
antiretroviral therapy, including individuals receiving initial and
subsequent regimens, had an undetectable viral load [1, 2].
Resistance to Antiretroviral MedicationsAntiretroviral resistance accumulates during virological failure.
Antiretroviral resistance also contributes to the failure of anti-
retroviral therapy. The contribution of antiretroviral medication
resistance to regimen failure is unclear but appears to be small,
particularly with the advent of new antiretroviral medications
and classes. On a population level, rates of transmitted and
prevalent resistance are stable or decreasing in some resource-
rich settings [1, 61, 62]. This is likely attributable to the high
genetic barrier to resistance and/or high potency of the most
frequently used regimens [63]. In a large US study from 2006,
15% of individuals with newly diagnosed HIV infection had
transmitted antiretroviral resistance—a slightly higher percent-
age than in prior studies [64].
Nonpersistence, nonadherence, and antiretroviral resistance
are barriers to effective antiretroviral therapy, contributing to
detectable HIV viremia in 15%–25% of individuals receiving
therapy. However, the majority of individuals receiving anti-
retroviral therapy in 2010 have undetectable viral loads. Thus,
most HIV-infected individuals receiving therapy are at low risk
for clinical progression and low risk to transmit HIV to others.
The Spectrum of Engagement in Care: By the
Numbers
In Figures 2 and 3a, we synthesize these findings to estimate the
spectrum of engagement in HIV care in the United States and
the proportion of the HIV-infected population who have an
HIV load ,50 copies/mL. Approximately 79% of HIV-infected
individuals are aware of their HIV infection, but !50% are not
adequately engaged in HIV care. Thus, 60% of HIV-infected
individuals in the United States are not receiving regular HIV
care because of deficits in diagnosis of HIV infection, linkage to
care, or retention in care. Of the remaining 40% of individuals,
!80% require antiretroviral therapy, 75% of whom receive it.
Finally, !80% of treated individuals have an undetectable viral
load (defined as , 50 copies/mL). These 210,000 HIV-infected
individuals with undetectable viral loads constitute just 19% of
the HIV-infected population in the United States. With .80%
of HIV-infected individuals in the United States having detect-
able HIV viremia, it is not surprising that the incidence of HIV
infection has not decreased in the United States despite almost
15 years of widespread access to combination antiretroviral
therapy. The model in Figure 2 is simplistic, but we are unaware
of data from cohorts of individuals tracked over the engage-
ment-in-care continuum that can more precisely determine the
true proportion of HIV-infected individuals in the United States
with an undetectable HIV load.
These estimates can be used to explore the potential impact of
interventions to improve engagement in care on the proportion
of HIV-infected individuals with an undetectable HIV load.
These simple simulations will also help demonstrate the impact
of uncertainty in our engagement-in-care estimates on the
projected proportion of HIV-infected individuals in the United
States with undetectable HIV loads.
Test-and-Treat Implications
Although there is now a burgeoning interest in the impact of
widespread antiretroviral therapy on HIV prevention, this is not
new. Approximately 10 years ago, mathematical models were
first published to suggest that widespread use of antiretroviral
therapy in HIV-infected individuals could reduce the incidence
of HIV infection [65–67]. Since that time, epidemiological data
have suggested that antiretroviral therapy reduces the risk of
HIV transmission in heterosexual sero-discordant couples by
92%–98% [7, 8, 68, 69]. In addition, ecological data have
revealed that the incidence of HIV infection may be decreasing
HIV/AIDS d CID 2011:52 (15 March) d 795
by guest on March 8, 2012
http://cid.oxfordjournals.org/Downloaded from
19%
↵80%
20%

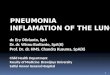
EECA: 90-‐90-‐90
881 149
90%
90%
90%
235 670?
Estimated PLHIV PLHIV who knowtheir status
On ART 2013 VL = 0
1 673 500
PLHIV do not knowtheir status
47%
PLHIVwho know their status
are not on ART
73%
86%
Estimated PLHIV are not on ART
Figure 2. Lack of access to key services for PLHIV in EECA
Source: See Annex 1
PLHIV do not know their status
1 673 500Estimated PLHIV
881 149PLHIV who know
their status
235 670On ART 2013
Figure 2. Lack of access to key services for PLHIV in EECA
Source: See Annex 1
PLHIV who know their status are not on ART
Estimated PLHIV are not on ART
47%
86%
73%

Source: UNAIDS

Source: UNAIDS

KM Estimates of Time to HIV-1 Infection (mITT Population)
Mean follow-up of 13 months: 16 subjects infected 14 in placebo arm (incidence: 6.6 per 100 PY), 2 in TDF/FTC arm (incidence: 0.94 per 100 PY)
86% relative reduction in the incidence of HIV-1 (95% CI: 40-99, p=0.002) NNT for one year to prevent one infection : 18
CROI 2015, Seattle, WA. #23LB.

A. The HIV infected individual B. The pandemic C. In summary….
Facing the challenge of the HIV patient in the near future / co-morbidities

In summary…. For HIV infected individuals …
- Ultimate goal of ART is an ajusted life expectancy close/identical to the general population. This would require managing the non-AIDS co-morbidities
- Achieving an sustaining an undetectable plasma VL is mandatory. II´s like Dolutegravir have an important role
- Objectives beyond undetectable plasma viral load should be considered
- The situation of many stable & suppressed patients can be potentially improved (including lowering the costs) without increasing the risk of loosing the virological suppression
- Functional cure may be an achievable goal

In summary…. For the AIDS pandemic
- Ultimate goal is an AIDS free generation in 2030…..?
- A combination of preventive strategies will be required including:
Classical prevention approaches More testing and more treating Likely PrEP (intermittent ?) in selected settings Possibly a preventative vaccine (even one only partially
effective)

Clinical Group JL Blanco M Laguno C Cáceres M López-Diéguez P Callau J Mallolas M Calvo C Manzardo S Corral D Martínez F Etcheverri E Martínez E Fernández M Martínez JM Gatell C Mensa F García A Milinkovic M Larrousse JM Miró E Lazzari A Moreno A León I Pérez M Loncà L Zamora
Virology Lab M Arnedo N Boulanger T Escribá C García M García C Gil C Hurtado S Lyonnais A Merino G Mirambeau L Muñoz
Immunology Lab C Alvarez L Miralles N Climent M Plana R Fernández C Rovira T Gallart S Sánchez A García V Sánchez J Joseph N Saubí MJ Maleno S Varea
E Yuste
Clinical Trials Coordination JA Arnaiz X Carné A Cruceta J Pich M Sarasa S Varea
Clinical Institute of Medicine & Dermatology Infectious Diseases & AIDS Division
External Colaborators J Alcamí B Autran M Lederman D Nixon G Pantaleo B Walker
ISCIII
Pharma companies

Infectious Diseases & AIDS Units. Hospital Clinic. Barcelona. Spain




www.escofetzamora.com

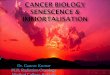
Attachment
Fusion
CD4
Chemokine co-receptor
Reverse transcription
Viral DNA Human genomic DNA
Integration (strand transfer) Transcription
Translation
Accessory viral proteins
Gag Pol Gag
Assembly/ cleavage
Release
Maturation
gp120
Budding
The need for novel drugs and novel classes
1. Dau et al. Drugs 2009;1:31–50. 2. Andrieux-Meyer et al. J Int AIDS Soc 2012;15:17986.
New drugs targeting different stages of the HIV-1 life cycle are needed to1,2
Improve tolerability and
toxicity
Reduce pill burden
Provide options for treatment-
experienced and -naive patients
Reduce drug–drug interactions
Provide novel formulations/
delivery systems
Figure from Lataillade et al. CROI 2015, Abstract 114LB.