Embed Size (px)
Citation preview

Chronic Family Economic Hardship, Family Processes and Progression of Physical and
Mental Health Problems in Adolescent Years
by
TAE KYOUNG LEE
(Under the Direction of K. A. S. Wickrama)
ABSTRACT
The purpose of the present study are to address the unique effects of chronic family
economic hardship as they influence marital conflict, supportive parenting, and adolescents’
anxiety, depressive symptoms, and physical complaints. To find unique pathways, the current
study also added the direct and indirect influence by using an SEM framework. The current study
analyzed data from a longitudinal sample of mothers, fathers, and target adolescents (N= 404-
451) to assess theoretical pathways. Findings generally supported the hypothesized model.
Chronic family economic hardship contributed to mental and physical health of adolescents. This
influence was largely mediated through supportive parenting. Moreover, supportive parenting
buffered marital conflict on depressive symptoms of adolescents. Adolescent females are more
vulnerable to health problems such as anxiety, depressive symptoms, and physical complaints in
several time points. The study demonstrates key mediating pathways based on family stress
model and also highlights the importance of improving health resources for adolescents.
INDEX WORDS: Chronic family economic hardships, Marital conflicts, Supportive parenting,
Adolescents, Anxiety, Depressive Symptoms, Physical Complaints and
Longitudinal data.

Chronic Family Economic Hardship, Family Processes and Progression of Physical and
Mental Health Problems in Adolescent Years
by
TAE KYOUNG LEE
B.S., CATHOLIC UNIVERSITY OF DAEGU, S. KOREA, 2004
M.A., SUNKYUNKWAN UNIVERSITY, S.KOREA, 2006
A Thesis Submitted to the Graduate Faculty of The University of Georgia in Partial Fulfillment
of the Requirements for the Degree
MASTER OF SCIENCE
ATHENS, GEORGIA
2011

© 2011
Tae Kyoung Lee
All Rights Reserved

Chronic Family Economic Hardship, Family Processes and Progression
of Physical and Mental Health Problems in Adolescent Years
by
TAE KYOUNG LEE
Major Professor: K.A.S. Wickrama
Committee: Lesile Gordon Simons Ronald L Simons Electronic Version Approved: Maureen Grasso Dean of the Graduate School The University of Georgia August 2011

iv
DEDICATION
This is dedicated to my wife who always pushed me to do my best. I am so thankful to
have had such a strong and loving my wife supporting me along the way.

v
ACKNOWLEDGEMENTS
With grateful heart, I would like to express my sincerest thanks to my major professor,
Dr. K. A. S. Wickrama, whose expert guidance, mentorship, inspiration, and encouragement
have given me the utmost support I needed to complete my degree. The experiences of working,
learning, and discussing with him across the years of my master training have made my graduate
education a meaningful and an enjoyable journey. Thank you for the unwavering mentorship,
thoughtful feedbacks, encouragement, and support. I also wish to thank my POS committee
members: Dr. Leslie Gordon Simons, Dr. Ronald Simons, who provided constructive insights
and time for this thesis.
For my friends in Athens, in other part of U.S., and abroad, thank you for listening and
updating me with life outside the academia. Most importantly, none of this would have been
possible without the love, support, patience, and continuous encouragement from my wonderful
wife, Ji-yeong Lee, and parents, Chang-gi Lee and Yeon-hee Kim, to whom I dedicate this
dissertation.
vi
TABLE OF CONTENTS
Page
ACKNOWLEDGEMENTS .............................................................................................................v
LIST OF TABLES ......................................................................................................................... ix
LIST OF FIGURES .........................................................................................................................x
CHAPTER
1 INTRODUCTION ........................................................................................................1
Indirect Influence of Chronic Family Economic Hardships on Adolescents’
Mental Health through Marital Conflict ....................................................2
Indirect Influence of Chronic Family Economic Hardship on Adolescents’ Mental
Health Problems through Supportive Parenting .........................................3
Indirect Influence of Marital Conflict on Adolescents’ Mental Health Problems
through Supportive Parenting ....................................................................4
Indirect Influence of Chronic Family Economic Hardship on Adolescents’
Physical Complaints through Marital Conflict ..........................................5
Indirect Influence of Chronic Family Economic Hardship on Adolescents’
Physical Complaints through Supportive Parenting ..................................6
Indirect Influence of Marital Conflict on Adolescents’ Physical Complaints
through Supportive Parenting ....................................................................6
Associations among Adolescents’ Anxiety, Depression, and Physical Complaints
over Time ...................................................................................................7

vii
Moderating Influence of Chronic Family Economic Hardship on Adolescents’
Health Problems through Supportive Parenting .........................................8
Moderating Influence of Supportive Parenting on the Association between Marital
Conflict and Adolescent’s Health Problems ..............................................9
Gender Differences ..........................................................................................................10
Control Variables .............................................................................................................10
Study Objectives ..............................................................................................................11
2 LITERATURE REVIEW ...........................................................................................12
The Theoretical Model ..........................................................................................12
The Association between Chronic Family Economic Hardship and Adolescents’
Health Problems .......................................................................................12
The Associations among Chronic Family Economic Hardship, Marital conflict,
and Adolescents’ Health Problems ..........................................................14
The Associations among Chronic Family Economic Hardship, Supportive
Parenting, and Adolescents’ Health Problems .........................................14
The Associations among Marital Conflicts, Supportive Parenting, and
Adolescents’ Health Problems ................................................................15
The Associations among Anxiety, Depressive Symptom, and Physical Complaints
over Time ................................................................................................16
Moderating Effect of Supportive Parenting on the Association between Chronic
Family Economic Hardship and Adolescents’ Health Problems .............20
Moderating Effect of Supportive Parenting on the Association between Marital
Conflicts and Adolescents’ Health Problems ...........................................20

viii
Gender Moderation on the Associations among Chronic Family Economic
Hardships, Marital Conflicts, Supportive Parenting, and Adolescents’ Health
Problems ................................................................................................................21
Study Control .......................................................................................................23
Specific Study Hypotheses ....................................................................................23
3 METHOD AND MEASUREMENTS ........................................................................25
Sample ...................................................................................................................25
Procedure ..............................................................................................................26
Measures ................................................................................................................27
Analytical Plan ......................................................................................................30
4 RESULTS ...................................................................................................................36
Descriptive Statistics of Study Variables ..............................................................36
Correlations among Study Variables .....................................................................37
Testing Specific Hypotheses ..................................................................................38
5 DISCUSSION ..............................................................................................................51
Summary and Understanding the Research Findings ...........................................51
Implications of the Current Study .........................................................................57
Limitations and Future Works for Current Study .................................................58
REFERENCES ..............................................................................................................................81

ix
LIST OF TABLES
Page
Table 1: Descriptive Statistics of Study Samples ..........................................................................61
Table 2: Mean Differences between Male and Female among Health Problems ..........................62
Table 3: Correlations among Study Variables ..............................................................................63
Table 4: Moderating Effects of Supportive Parenting ..................................................................64
Table 5: Gender Difference of Health Problems ...........................................................................65
Table 6: Gender Difference of the Hypothesized Path Model ......................................................66
Table 7: Univariate Growth Curves Model ..................................................................................67

x
LIST OF FIGURES
Page
Figure 1: Theoretical Model .........................................................................................................68
Figure 2: Operationalized Model ..................................................................................................69
Figure 3: Basic Mediational Structure for Sobel Test ..................................................................70
Figure 4: Direct Influence of Chronic Family Economic Hardship on Adolescents’ Health
Problems .....................................................................................................................71
Figure 5: Indirect Influence of Chronic Family Economic Hardship on Adolescents’ Health
Problems through Marital Conflict ...............................................................................72
Figure 6: Indirect Influence of Chronic Family Economic Hardship on Adolescents’ Health
Problems through Supportive Parenting ......................................................................73
Figure 7: Indirect Influence of Marital Conflict on Adolescents’ Health Problems through
Supportive Parenting ....................................................................................................74
Figure 8: The Operationalized Associations of the Current Study ...............................................75
Figure 9: Supportive Parenting Moderation of Marital Conflict on Adolescents’ Depression .....76
Figure 10: Moderating Effect of Gender Difference on Adolescents’ Health Problems ...............77
Figure 11: Gender Difference on the Associations among Chronic Family Economic Hardship,
Marital Conflicts, Supportive Parenting, and Adolescents’ Health Problems .............78
Figure 12: Gender Difference of Chronic Family Economic Hardship on Depression ................79
Figure 13: Hypothesized Interlocking Model ...............................................................................80

1
CHAPTER 1
INTRODUCTION
Poverty creates enormous challenges for families and living in poverty is associated with
adverse outcomes for adolescents. Living in poverty produces a “conglomeration of stressful
conditions and events” (McLoyd, 1990, p. 314) causing chronic financial hardship. Numerous
studies have been identified that explain the negative effects of economic hardship on children
and adolescents. For example, Adolescents who grow up poor are at heightened risk for a wide
range of psychological problems (e.g., McLoyd, 1998), physical health problems (Wickrama,
Conger, & Abraham, 2005), academic problems (Conger & Donnellan, 2007), alcohol use
(Conger, Lorenz, Elder, Melby, Simons, & Conger, 1991), and vandalism (Moffitt, 1993;
Patterson et al., 1989).
Previous psychological research suggests that anxiety, depression, and physical
complaints are serious health problems among youth (Jacques & Mash, 2004; Simeonsson,
McMillen, & Huntington, 2002; Wittchen, Kessler, Pfister, & Lieb, 2000). In the case of
adolescents’ psychological problems, Beck and Steer (1987) advance depression is associated
with ‘perceived loss’; whereas, anxiety is associated with ‘perceived threat’. However, such
mediating psychological constructs have rarely been used to characterize adolescents’ adverse
family experiences, or to link such experiences specifically with depression and anxiety.
Therefore, this study proposes that adolescents may perceive family economic problems as a loss
in terms of access to material needs, and an ability to develop friendships and close relationships,
which may result in feelings of depression. Also, adolescents may perceive family economic

2
problems as a threat anxiety to successfully transition to adulthood, due to excessive working
hours to earn money, and the possibility of truncating their education. Also, adolescents may
experience threatening family and community events, and circumstances associated with their
family’s adverse economic conditions. Thus, this study suspects that family economic hardship
may directly generate feelings of threat, independent of feelings of depression.
In addition, family economic hardship influences adolescent physical health through a
lack of accessibility and availability of health resources, such as health insurance, medication,
food, and clothing. Also, poor families often live in sub-standard housing and hazardous
environments (Miech, Caspi, Moffit, Wright, & Silva, 1999). In addition, family economic
hardship as a chronic stressor disrupts physiological functions (Lynch, Kaplan, & Shema, 1997).
Thus, consistent with these findings, this study will examine the direct influence of chronic
family economic hardships on adolescents’ health problems (i.e., anxiety, depression, and
physical complaints).
Indirect Influence of Chronic Family Economic Hardships on Adolescents’ Mental Health
through Marital Conflict
Some investigators suggest that socioeconomic factors may impact marital quality
(Piotrkowski, Rapoport, & Rapoport, 1987). For example, Atkinson, Liem, and Liem(1986)
found a significant inverse association between duration of unemployment and marital quality.
Larson (1984) found mean differences between groups of employed and unemployed spouses for
total dyadic adjustment, but not for the satisfaction, affection, or cohesion subscales of the
dyadic adjustment scale. Consistent with these ideas, research evidence continues to accumulate,
suggesting that economic hardship has an adverse influence on the quality of marital
relationships (Brody, Stoneman, Flor, McCrary, Hastings, & Conyers, 1994; Conger et al., 1990).

3
Furthermore, earlier studies have provided evidence for the association between parents’
marital problems and adolescent maladjustment. Exposure to high levels of marital conflict of
parents is associated with the development of a wide variety of difficulties for adolescents’
mental problems, such as anxiety and depressive symptoms (e.g., Cummings & Davies, 1994;
Gottman & Notarius, 2000). Many studies have demonstrated that adolescents’ mental problems
are most likely to occur when a marital relationship is intense and openly hostile (Buehler,
Krishnakumar, Stone, Anthony, Pemberton, & Gerard, 1998; Jenkins, 2000). With these ideas in
mind, the current study examines whether economic hardship influences adolescents’ depressive
symptoms and anxiety indirectly through their parents’ marital conflicts.
Indirect Influence of Chronic Family Economic Hardship on Adolescents’ Mental Health
Problems through Supportive Parenting
Previous research has shown that family economic hardship has a consistent impact on
parenting practices (Conger, Ge, Elder, Lorenz, & Simons, 1994; McLoyd, 1990; Simons,
Lorenz, Conger, & Wu, 1992). In particular, the frustration produced by economic hardship
fosters an irritable, aggressive psychological state in parents that operates to decrease warmth
displayed toward others, including their children (Simon et al., 1990). Also, research reports that
a low level of supportive parenting was judged by their adolescents to be more authoritarian in
their exercise of authority within the home (Buri, Cooper, Ricktsmeier, & Komer, 1991; Simons
et al., 1992).
Several studies have shown that retrospectively reported adverse threatening events and
circumstances associated with family adversity, such as family disruptions, were related to
anxiety disorders (Schwarts, Snidman, & Kagan, 1999; Rapee & Heimberg, 1997). However,
less has been written about the family precursors of anxiety than depression in mental health

4
problems. Specifically, there is a paucity of research on anxiety associated with family adversity.
In addition, most adolescent research on anxiety is also limited by either clinical or cross-
sectional samples. Therefore, this study will examine chronic economic hardship influences
adolescents’ depressive symptoms, as well as anxiety through supportive parenting.
Indirect Influence of Marital Conflict on Adolescents’ Mental Health Problems
through Supportive Parenting
Many studies suggest marital conflict influences adolescent mental problem through
parenting (Conger et al., 1992, 1993; Conger, Ge, Elder, Lorenz, & Simons, 1994; Kitzmann,
2000). For example, Caspi and Elder (1988) found that marital conflict influenced adolescent
mental problems indirectly through its effect on parenting practices. In addition, evidence for the
mediating role of parenting has also been provided by Conger and his colleagues (Conger, Ge,
Elder, Lorenz, & Simons, 1994). In particular, Harold and Conger (1997) found that marital
conflict indirectly predicted increases in adolescents’ internalizing problems through a low level
of supportive parenting.
Most of these previous studies are consistent with the “disrupted discipline hypothesis”
(Emery, 1982), which proposes that conflict and distress in the marital relationship lead to
negative behaviors in parenting, such as inconsistency, rejection, hostility, and harsh discipline.
However, these studies have primarily focused on the negative dimensions of parenting and did
not examine the positive dimensions of parenting behavior. The “loss of love” hypothesis
(Emery & O’Leary, 1982) proposes that parents’ marital problems reduce their warm and
supportive parenting behavior, which, in turn, leads to adjustment problems for children and
adolescents. Therefore, the present study will examine marital conflict influences adolescents’
mental problems through supportive parenting.

5
Indirect Influence of Chronic Family Economic Hardship on Adolescents’ Physical
Complaints through Marital Conflict
Previous studies showed that adolescents who live in families characterized by high
levels of inter-parental conflict have been found at increased risk of adolescents’ negative
adjustment outcomes (see Cummings & Davies, 1994) and physical problems (Nicolotti, El-
Sheikh, &Whitson, 2003). There is evidence that children’s physical health is negatively affected
by marital conflict (Campbell & Lewandowski, 1997; Wadsworth, 1997). Children exposed to
parental problems, such as marital conflict, have more health problems, including mild ailments
and more serious conditions, than children from intact homes (Mauldon, 1990).
Stressful family circumstances, such as parents’ marital conflicts, can contribute to the
physical complaints of adolescents through physiological mechanisms (Bradley & Corwyn,
2002). In detail, Dowd and Goldman (2006) reported that chronic stressors disrupt the body’s
physiological functions because they involve an allostatic load, defined as the cumulative wear
and tear on the body’s systems owing to repeated adaptations to stressors, such as family
economic hardship. This stress-ill health physiological connection may be attributed to hormonal
responses resulting in adverse health outcomes, including high blood pressure, high heart rate,
glucose intolerance, abdominal obesity, elevated low-density lipoprotein (LDL) cholesterol, and
lowered high-density lipoprotein (HDL) cholesterol. These health problems may underlie
adolescents’ physical complaints.
By identifying an association between family economic hardship and physical health
problems, the research focus has shifted to consider the processes underlying this relationship
with particular attention to possible mediating role of parents’ marital conflicts (Frosch &

6
Mangelsdorf, 2001). Thus, this study will examine whether family economic hardship can
influence adolescents’ physical complaints indirectly through marital conflict.
Indirect Influence of Chronic Family Economic Hardship on Adolescents’ Physical
Complaints through Supportive Parenting
Physical complaints are influenced by parenting style (e.g., Eiser & Havermans, 1992;
Hamlett, Pellegrini, & Katz, 1992). In fact, one of the most reliable predictors of adolescents’
adjustment to physical complaints is parenting behaviors (Elliott & Mullins, 2004). Furthermore,
parenting behaviors have been hypothesized to influence physical complaints by the adverse
effects of stressful family events (Wickrama, Conger, & Lorez, 1995).
Although previous developmental studies imply associations among adolescents’
physical complaints, parenting, and family economic hardships, there is very little empirical
research on these associations, including supportive parenting as social support (Vilhjalmsson,
1994). With these ideas in mind, this study examines family economic hardship can influence
adolescents’ physical complaints through supportive parenting.
Indirect Influence of Marital Conflict on Adolescents’ Physical Complaints
through Supportive Parenting
Mechanisms identified as mediating the effects of marital conflict on adolescents’
adjustment include adolescents’ appraisals for parenting (e.g., Harold, & Conger, 1997).
Especially, in the context of marital conflict, previous research found a significant association
between parental support and adolescent reports of physical complaints or well-being. In
particular, parental support reduced physical health problems during adolescence (Wickrama,
Lorenz, Conger, & Elder, 1997; Rogers & Holmbeck, 1997). Moreover, Radovanovic (1993)

7
suggested that positive social support, such as parental support, was negatively related to
adolescent health problems in conflicted families.
Although previous studies imply associations among marital conflict, supportive
parenting, and adolescent’s physical complaints, most of these studies have empirically tended
towards the influence on mental health outcomes (Conger, & Elder, 1994). Although mental
health outcomes may be associated with physical health status (Vilhjalmsson, & Thorlindsson,
1998), there are few empirical studies that focus on physical health over the adolescent years.
Hence, this study examines whether marital conflict influences adolescents’ physical complaints
through supportive parenting.
Associations among Adolescents’ Anxiety, Depression, and Physical Complaints over Time
According to the National Comorbidity Survey (Kessler & Walters, 1998), the lifetime
prevalence rate of depression in adolescents aged 15 to 18 years is 14%, and an estimated 20% of
these adolescents will have had a depressive disorder by the time they are 18 years old. Anxiety
disorders have a lifetime prevalence rate of approximately 20% and exhibit a significant degree
of stability across a lifespan (Costello, Edelbrock, & Costello, 2005). Adolescents with either
major depression or anxiety symptoms are at risk for a variety of negative outcomes, including
academic achievement (Boivin, Hymel, & Hodges 2001; Juvonen, Nishina, & Graham, 2000),
self-esteem (Muris, Schmidt, Lambrichs, & Meesters, 2001), substance abuse (O'Neil, Conner, &
Kendall, 2011), and relationship problems (Cole & Carpentieri, 1993).
Furthermore, adolescent depression and anxiety disorders highly co-occur as well as with
other psychiatric disorders (Angold, Costello, Farmer, Burns, & Erkanli, 1999). Research has
shown the odds ratio of co-occurring anxiety given a depressive disorder are as high as 30.0.
Also, depression and anxiety disorders are more likely to co-occur rather than with other

8
psychiatric disorders, such as attention-deficit hyperactivity disorder, disruptive behavior
disorders, or substance use disorders (Messer, Angold, Costello, & Burns, 2003).
One of the most important issues in the psychological development of adolescents is
associated with physical health problems (Simeonsson et al., 2002). Conversely, poor physical
health can also involve an array of psychological problems (Lewinsohn, Rohde, Seeley, & Fisher,
1993). Studies conducted over the last few decades have consistently shown that children and
youth with physical health problems are at an increased risk for developing psychological
problems (McDougall, King, de Wit, Miller, Hong, Offord, Laporta, & Meyer, 2004; Newacheck,
McManus, & Fox, 1991). A meta-analytic review of 87 studies revealed that youth with physical
health problems are significantly more likely to exhibit symptoms of psychological problems,
such as depression and anxiety. (Boekaerts & Roeder, 1999).
Given the significantly high prevalence, recurrence, and co-occurrence of depressive
symptoms, as well as anxiety and physical health problems during adolescence, it is important to
understand the inter-related health processes involving the three different health domains in
adolescents over this period. However, most research has focused on a single health domain of
adolescents—depression, physical health problems, but rarely anxiety. Therefore, this study
focuses on how depression, anxiety, and physical complaints mutually influence one another
over time, as an inter-related health process.
Moderating Influence of Chronic Family Economic Hardship on Adolescents’ Health
Problems through Supportive Parenting
The influence of economic hardship on adolescents’ health problems may vary,
depending on the level of supportive parenting. Consistent with the risk-resource perspective,
family economic hardships can be considered a factor that places adolescents at risk for mental

9
and physical health problems, while supportive parenting can be considered a resource factor
which protects and moderates the risk of family economic hardships. Rogers and White (1998)
reported that effective parenting is a buffer for children’s maladjustments, since attentive parents
take the time to reason and help their children develop effective problem-solving skills. Such
moderating effects are deemed important in the developmental literature on adolescents’ health
problems. However, they are still understudied and are infrequently found in the literature on
adolescents’ health problems (Luthar, Cicchetti, & Becker, 2000; Masten, 2001). To address this
need, the moderating effect of supportive parenting on the association between family economic
hardships and adolescents’ health problems (i.e., anxiety, depressive symptom, and physical
complaints) will be examined in this study.
Moderating Influence of Supportive Parenting on the Association between Marital Conflict
and Adolescent’s Health Problems
Prior studies suggest parenting behavior might moderate the association between marital
conflict and adolescents’ health problems. Gordis, Margolin, and John (1997) reported the
interaction between marital problems and parental behavior toward a child accounted for a
significant variance in adolescent’s maladjustment. Frosch and Mangelsdorf (2001) also found
that a mother’s supportive parenting moderated the association between marital conflict and
children’s problems. However, they did not find this moderating effect for adolescent health
problems, such as depressive symptoms, anxiety, and physical complaints. Given these findings
in the literature regarding the moderating effects of supportive parenting, the present study
examines whether the association between marital problems and adolescent health problems is
moderated by supportive parenting.

10
Gender Differences
In addition, Phillips and Diaz (1997) reported that gender difference is an important
marker to understand adolescents’ mental health problems, such as depressive symptoms and
anxiety. In their study, female’s comorbidity of depressive symptoms and anxiety was usually
higher than male’s comorbidity of these mental health problems. Moreover, Silverstein and
Lynch (1998) found evidence the high prevalence of clinical and subclinical depression that
arises among females is of the anxious somatic depression type, involving depression coupled
with anxiety and physical complaints (e.g. coughs, headaches, and fatigue). Therefore, this study
will examine potential gender differences on the association among depressive symptoms,
anxiety, and physical complaints.
Moreover, previous research suggests that economic stress may affect males and females
differently (Bolger, Patterson, & Kupersmidt, 1995; Conger et al., 1993; Elder & Caspi, 1988).
In general, prior work indicates that young males may be more vulnerable to family economic
stress than females (Bolger, Patterson, & Kupersmidt, 1995; Patterson, Vaden, Griesler, &
Kupersmidt, 1991). Therefore, the present study will also examine how gender moderates the
association among family economic hardship, supportive parenting, marital conflict, and
adolescents’ health problems (i.e., depressive symptoms, anxiety, and physical complaints).
Control Variables
Additionally, many previous studies support the view that the parental level of education
can significantly predict adolescents’ mental problems, such as anxiety and depressive symptoms,
as well as physical health problems, such as physical complaints (Donohue, Romero, & Hill,
2006; Wickrama, Conger, Lorenz, & Elder, 1998). Moreover, the research has shown that
parental depression can negatively influence their children’s health problems (Mustillo et al.,

11
2009). Therefore, this study will use parental education and parental depression as a control
variable to assess the uniqueness of the association among depressive symptoms, anxiety,
physical complaints, family economic hardship, and supportive parenting.
Study Objectives
The current study’s objectives are as follows:
1. To investigate the direct influence of family economic hardships on each—depression,
anxiety, and physical complaints.
2. To investigate the indirect influence of chronic family economic hardships on
depression, anxiety, and physical complaints through supportive parenting.
3. To investigate the indirect influence of chronic family economic hardships on
depression, anxiety, and physical complaints through marital conflicts.
4. To investigate the indirect influence of marital conflicts on depression, anxiety, and
physical complaints through supportive parenting.
5. To investigate the longitudinal mutual influences among depression, anxiety, and
physical complaints over the adolescent years.
6. To investigate the moderating effect of supportive parenting on the associations
among family economic hardships and adolescents’ health problems.
7. To investigate the moderating effect of supportive parenting on the associations
among marital conflicts and adolescents’ health problems
8. To investigate the gender difference in associations among adolescents’ health
problems.
9. To investigate the gender difference in pathways among family economic hardship,
marital conflicts, supportive parenting, and adolescents’ health problems.

12
CHAPTER 2
LITERATURE REVIEW
The Theoretical Model
Figure 1 shows the theoretical model for the current study. The theoretical model depicts
family economic hardships directly and indirectly influences adolescents’ anxiety, the levels of
depressive symptoms, and physical health problems through marital conflicts and supportive
parenting. Anxiety, depression, and physical complaints are contemporaneously associated with
each other. Cross-lagged paths depict the influence of early health problems in one domain on
change in health problems in another domain over time. The paragraphs that follow will discuss
all of the constructs and hypothesized associations for this model.
The Association between Chronic Family Economic Hardship
and Adolescents’ Health Problems
Socioeconomic health disparities appear to have increased in recent decades, due to
widening socioeconomic inequalities (Kahn & Fazio, 2005; Pappas, Queen, Hadden, & Fisher,
1993). Hence, the relationship between family-of-origin adversity and youth mental health is
vital to understand the progression of mental and physical health across a lifespan (Repetti,
Taylor, & Seeman, 2002; Wickrama et al., 2008b). Existing research suggests that family
socioeconomic adversity contributes to many domains associated with adolescent’s mental health
problems, such as anxiety and depressive symptoms (Conger et al., 1993). Adolescents become
more susceptible to family disadvantages during adolescence, due to dramatic increases in the
salience of family economic resources (Halpern-Felsher et al., 1997). In addition, adolescents

13
experience normative stressful circumstances during this period, including physical changes (e.g.,
puberty) and changes in social-family relationships (Conger & Ge, 1999). Therefore, a family’s
stressful circumstances may contribute to diminished psychological resources, an increased sense
of continuing entrapment, feelings of anger, hopelessness, frustration, and other negative
emotions among youth. In addition, parents with low-incomes are more likely to experience
mental health problems and chaotic lifestyles, which may transmit directly to their children
(Wickrama, Conger, Wallace, & Elder, 1999; Lempers, Clark-Lempers, & Simons, 1989).
Moreover, Pless and Nolan (1991), in their review of maladjustment for children and youth with
chronic physical health problems, suggest that socioeconomic status may play an important role
in their physical health problems. McDougall et al. (2004) also reported that children and youth
with chronic physical health problems are at increased risk of living in families that receive
welfare income or who are below the poverty level and, at the same time, are also shown to be at
increased risk for emotional problems.
Pless and Nolan (1991), in their review of maladjustment for children and youth with
chronic physical health problems, suggest that socioeconomic status may play an important role
in their physical health problems. Moreover, as I discussed previously in case of marital conflict,
chronic family economic hardship may also disrupt the body’s physiological functions and
results in negative physical health outcomes because it involve allostatic load. McDougall et al.
(2004) also reported that children and youth with chronic physical health problems are at
increased risk of living in families that receive welfare income or who are below the poverty
level and, at the same time, are also shown to be at increased risk for emotional problems.
Therefore, this study proposes that economic hardship would also have a direct effect on
adolescents' mental and physical complaints.

14
The Associations among Chronic Family Economic Hardship, Marital Conflicts, and
Adolescents’ Health Problems
Although there is some evidence that chronic economic stress has a direct impact on
adolescents’ health problems (McLoyd, 1990), adverse financial circumstances could affect
adolescents’ health problems through the quality of family interactions primarily through
emotions and cognitions that reflect their awareness of and responses to economic difficulties.
Considerable research notes that economic factors play an important role in the dynamics of
parents’ marital relationships, and children’s mental and physical problems (Conger & Conger,
2002; Conger et al., 1994, 2002). For example, research suggests the marital dyad is a critical
point of entry for adverse economic influences that eventually affect physical complaints (El-
Sheikh, Harger, & Whitson, 2001) and mental problems (Elder & Caspi, 1988). However, there
is very little empirical research on the relationships among these variables for adolescents.
Therefore, this study proposes that family economic hardships indirectly influence adolescents’
health problems through parents’ marital conflict.
The Associations among Chronic Family Economic Hardship, Supportive Parenting,
and Adolescents’ Health Problems
Previous research suggests that economic pressure is linked to adolescent adjustment
through parental behavior. For example, Patterson et al. (1989) argued that stressful family
circumstances have their greatest impact on children and adolescents through disruptions in
parent-child relations and effective parenting behaviors. Supportive parenting can have positive
effects on various aspects of adolescents’ health (Amlund, Hagen, Myers, & Mackintosh, 2005;
Leinonen, Solantaus, & Punamaki, 2003). For example, supportive parenting can reduce
adolescents’ mental health (Petersen, Sarigiani, & Kennedy, 1991) and physical health problems
15
(Wicrama, Lorenz, & Conger, 1997). Piko (2000) also reported that a low level of parental
support increased the risk of children’s maladjustment. Moreover, according to Robila and
Krishnakumar (2005), financial strain is associated with lowered social support. Financial
problems, as stated by Ge, Conger, Lorenz, and Simons (1994), are related to disruptive
parenting practices. Parental unemployment, as a possible source of stress and financial strain,
can thus negatively influence the amount of support provided to adolescents by their parents.
Taken together, previous studies provide support for the pathway from family economic
hardships, through supportive parenting to adolescents’ health problems. Thus, this study
proposes that chronic family economic hardships influence adolescents’ health problems
through supportive parenting.
The Associations among Marital Conflicts, Supportive Parenting,
and Adolescents’ Health Problems
Several researchers have suggested the relationship between marital conflict and youth
maladjustment may be mediated by parenting behaviors (Bray & Hetherington, 1993; Gable,
Belsky, & Crnic, 1992). Research has documented a significant association between parents and
selected parenting behaviors. Parenting behaviors and youth maladjustment are also related
(Gable et al., 1992). Specifically, marital conflict is associated negatively with parental support
(Conger et al., 1993; Fauber et al., 1990). In turn, parental support and responsiveness are
associated with psychological problems (Melby, Conger, Conger, & Lorenz, 1993) and physical
complaints (Katz & Gottman, 1997).
Although there has been some conflicting evidence on this association (Peterson & Zill,
1986), most studies have found that much of the relationship between marital conflict and youth
maladjustment is mediated by parenting behaviors (Bray & Hetherington, 1993; Cole &

16
McPherson, 1993). Therefore, the current study proposes the association between marital
conflict and adolescents’ health problems can be mediated by supportive parenting.
The Associations among Anxiety, Depressive Symptom, and Physical Complaints
over Time
Recently, the existing base of empirical evidence has established that depressive
symptom (Gutman & Sameroff, 2004; Lewinsohn et al., 1993), anxiety (Barnow, Lucht, &
Freyherger, 2005; Moffitt, 1993), and physical complaints (Ajdacic-Gross et al., 2006) show a
significant increase in both prevalence and incidence during adolescence. The time-related
developmental patterning raises questions about the relationships among anxiety, depressive
symptoms, and physical complaints during adolescence (Katon, Elizabeth, Lin, & Kroenke,
2007). Previous research focused on late childhood and adolescence suggests that constructs for
child anxiety and depressive symptoms are distinguishable and covary at dimensional and
categorical levels (Lonigan, Phillips, & Hooe, 2003). Additionally, many studies have reported
heterotypic continuity of psychiatric problems in childhood and adolescence. For example,
Lewinsohn, Klein, and Seeley (1995) found that anxiety symptoms precede and predict
subsequent depressive symptoms. Moreover, other research in the Christchurch Health and
Development Study shows that levels of ‘anxious and withdrawn’ behaviors at age 8 predicted
risk for major depression in late adolescence and early adulthood (Goodwin et al., 2004).
Reinherz et al. (1989) also found that self-reported symptoms of anxiety at age 9 predicted self-
reported symptoms of depression at age 15. Indeed, early symptoms of anxiety more than
doubled the likelihood of later depressive symptoms. Similar results emerged between ages 15
and 18 at a later stage of the same study (Reinherz et al., 1993). Snyder et al. (2009) indicated
that earlier anxiety symptoms facilitate subsequent depressive symptoms. However, other studies
have shown that early depressive symptoms predict changes in anxiety. In a study of consecutive

17
adolescent referrals to psychiatric clinics, Sanford et al. (1995) noted that depression at outcome
(1 year later) was significantly predicted by prior symptoms of anxiety. Conversely, almost half
of the teenagers with major depressive disorder at Time 1 manifested an anxiety disorder 1 year
later. In a review, Wittchen et al. (2000) concluded that anxiety disorders typically precede the
onset of depression when the two co-occur, and the number and type of anxiety disorders present
influence the risk for later depression.
However, research on the developmental ontogeny of depression and anxiety is critical to
this debate. For example, if depressive disorders are nearly always preceded by anxiety, then it is
possible the two symptom groups may be better thought of as a syndrome that begins with
anxiety and emerges as depression or comorbid depression and anxiety. The Dunedin Study is
one of the few studies which the relative predictive utility of anxiety versus depression to later
disorders was tested (Moffitt et al., 2007). Their results demonstrated that anxiety and major
depression had a reciprocal relation such that one preceded the onset of the other relatively
equally from ages 11 to 32 years (Moffitt et al., 2007). Similar findings of reciprocal relations
between anxiety and depression were reported in the Great Smoky Mountains Study, in which
testing of heterotypic and homotypic patterns of stability in anxiety and depression was carried
out using a much narrower age range from 9–16 (Costello, Mustillo, Erkanli, Keeler, & Angold,
2003).
Moreover, consistent with Beck and Streer (1987), I argue that adolescents may perceive
depressive symptoms as a loss in regard of limited resources that can aid school success and
access to material needs, which may precede a late-onset of feeling of anxiety. Also, adolescents
may perceive anxiety as a threat, due to the possibility of truncating their education and
excessive working hours to earn money, which, in turn, may precede late-onset of depressive
18
symptoms. Thus, the current study hypothesizes that anxiety and depression are mutually
influenced over time.
Mental health problems may lead to physical health problems. For instance, mental
disorders, such as depression, may directly lead to physical complaints by weakening and/or
altering the immune response. There is extensive evidence suggesting that stress can lead to
decreased immune functioning (Miller, Chen, & Zhou, 2007) and mental health problems, such
as depression, have been linked to changes in cellular immunity (Cohen & Herbert, 1996), often
resulting in reduced immune response. These changes may lead to an increase in physical
complaints, including fatigue and the common cold (Takkouche, Regueira, & Gestal-Otero,
2001).
In addition, individuals with depressive symptoms may be more likely to engage in
behaviors that lead to physical complaints. For instance, depressive symptoms are associated
with poor self-care (Katon, & Sullivan, 1990), and individuals who are depressed often sleep less
and exercise less than those who are not depressed (Herbert, & Cohen, 1993). Finally, depression
symptoms have been linked to poor eating habits and a lack of exercise, leading to elevated
weight status maintained from childhood into adulthood (Anderson, Cohen, Naumova, & Must,
2006).
While most previous research on the link between mental and physical health has focused
on depression, some evidence suggests that anxiety increases the risk of physical complaints as
well. Several recent studies report that anxiety disorders are associated with back pain and
headaches (Culpepper, 2009; Simon & Fischmann, 2005). Explanations for the association
between anxiety and physical complaints include dysregulation of the stress-response system
(Culpepper, 2009; Roy-Byrne et al., 2008).

19
In contrast, Lavigne and Faier-Routman (1993) reported that physical illness has
influenced psychological problems. They stated the results of their analysis indicated that
children with physical health problems are at an increased risk for psychological symptoms
compared to children without health problems, with internalizing symptoms being more likely
than externalizing symptoms.
Physical health problems may also predict mental health problems in psychosocial
mechanisms. First, internalized problems such as depression and anxiety, may be caused
physiologically by physical illness or through side effects resulting from medications used to
treat a disease (Eiser, 1990; Wallander & Varni, 1998). Second, previous studies suggest that
physical complaints may contribute to mental health problems through unhappiness about having
to heal with the ailment, physical complaints, or body pain or limitations, change in physical
appearance (Lewinshon, et al., 1995), and a limited socioeconomic attainment (Wickrama, et al.,
2005).
For the most part, the many studies that have examined the relationships between
physical health problems and psychological functioning in children and youth have been cross-
sectional or clinic-based, and have involved small, condition-specific samples (Barnett, Manly,
& Cicchetti, 1993). Few studies have followed a sizable cohort prospectively or have used
population-based samples. Moreover, given the paucity of longitudinal studies of comorbid
mental and physical health problems in adolescents from community populations, this study
examines the associations of mental and physical health problems in a sample of youth served in
community settings. Thus, the current study uses community-based longitudinal data. Also, this
study proposes that depression, anxiety, and physical complaints can influence each other over
time.

20
Moderating Effect of Supportive Parenting on the Association between Chronic Family
Economic Hardships, and Adolescents’ Health Problems
Systems theory emphasizes the family context of the adolescent as the critical factor
influencing the processes of coping and long-term adaptation (Mott, James, & Spherac, 1990).
Research has indicated that warm, supportive, and non-coercive parental practices buffer
children’s physical health problems from some of the adverse consequences of economic
hardships (Hanson, McLanahan, & Thomson, 1997). Conversely, Lempers et al. (1989) have
argued that hostile parenting might be expected to amplify adolescents’ mental health problems
against the disruptive threats posed by economic hardships. That is, supportive parenting may
moderate the association between economic hardships and adolescent mental and physical
problems. Thus, this study investigates the moderating influence of supportive parenting on the
association between family economic hardships and adolescents’ health problems.
Moderating Effects of Supportive Parenting on the Association between Marital Conflicts,
and Adolescents’ Health Problems
Previous research suggests that parent-child relationships may moderate the associations
between marital conflicts and adolescent health, such that relationships characterized by high
affective quality buffer adolescents from the negative consequences of marital conflict. For
instance, in keeping with the family systems theory principle of wholism, Grych and Fincham
(1990) argue that children interpret marital conflicts within the context of parent-child relations.
Therefore, marital conflicts that occur in the context of close, warm, and supportive parenting
will be perceived as less negative and threatening than marital conflicts that occur in the context
of less positive parenting. Similarly, Davies and Cummings (1994) argued that positive and
effective parenting protects and enhances children’s feelings of emotional security, which defend

21
children against the negative consequences of marital conflict exposure. Similar arguments for
the buffering role of parent-child relationships are found in chronic stress and early adversity
literature, in which high quality parent-child relationships are viewed as a mechanism by which
children are protected from negative consequences of early adversity (e.g., Bugental, 2004).
Viewing parenting practices as a moderator suggests that rather than playing a causal role in the
pathway between marital conflicts and child outcomes, there are individual differences in the
levels of parenting; supportive parenting is protective against the negative consequences of
marital conflict exposure. Therefore, consonant with this idea, this study proposes the
association between marital conflicts and adolescents’ health problems is moderated by
supportive parenting.
Gender Moderation on the Associations among Chronic Family Economic Hardships,
Marital Conflicts, Supportive Parenting, and Adolescents’ Health Problems
Gender differences in mental and physical health are well documented. Research on
gender differences in mental health has clearly established that women have higher rates of so-
called “internalizing” disorders, including depression and anxiety disorders (Kessler et al., 2005).
Research on gender differences in physical health has demonstrated that patterns of physical
complaints are gendered as well. The evidence suggests that women are more likely to have
chronic debilitating conditions, such as fatigues and headaches (Bird & Rieker, 2008; Verbrugge,
1985). Furthermore, Furnham and Kirkcaldy (1997) reported significant gender differences in
the frequency of physical ailments of individuals over six months: women reported an average of
3.4 complaints in contrast to 2.6 complaints for males. Females were more likely to report
headaches, general fatigue, and constipation compared to males. Moreover, in the case of adults,
women reported physical complaints consistently more frequently than men in longitudinal
22
research (Ajdacic-Gross et al., 2006). Also, the studies by both Garber et al. (2002) and Ge et al.
(2001) showed that females generally had more depressive symptoms at an earlier onset.
Also, evidence for differences in psychobiological processes between genders was
observed by Egger, Costello, Erkanli, and Angold (1999). They found that among 9-16 year olds,
physical complaints were strongly associated with emotional disorders in females. Also, there is
a study on gender differences on the comorbidity of mental health problems and physical
complaints. In Silverstein and Lynch’s study (1998), for both the genders, musculoskeletal pains
were related to depression. However, it was reported that females more often self-reported
anxious somatic depression, but not pure depression.
Although many studies imply that gender differences in mental and physical health are
widely acknowledged, it is unclear whether there are gender differences in the association
between mental health (i.e., depression and anxiety) and physical complaints. Thus, the current
study is an attempt to explore how the gender difference for adolescents’ health problems occurs
over adolescent years.
In addition to gender issues impacting adolescents’ health problems, some support for
testing gender moderation derives from work showing the mediating path through ineffective
parenting is stronger for sons than daughters (Buehler & Gerard, 2002). Moreover, prior research
proposes that economic stress may also influence males and females differently (Bolger et al.,
1995; Elder & Caspi, 1988). Also, child gender can moderate the association between marital
conflict and their health problems, including emotional problems and physical complaints
(Baviskar, 2010). Thus, this study extends this work by addressing gender differences on the
association between family economic hardships, marital conflicts, supportive parenting, and
adolescent’s health problems (i.e., depression, anxiety, and physical complaints).

23
Study Control
Demographic characteristics may influence contemporaneous and cumulative mental
health, as well as physical health consequences in adolescents. To further isolate the independent
influence of family economic hardships on self-assessed health problems through marital
conflicts and supportive parenting, this study controls for parental education and parental
depression. This is not only because, to a significant degree, adolescent health is an outcome of
the direct investment of parental knowledge and available resources (Becker, 1993), but also
because parental depression can influence their children’s outcome (Goodman & Gotlib, 2002;
Jaser et al., 2005).
Specific Study Hypotheses
This study simultaneously examines factors among individuals, parents, and family
economics for the development of youth’s anxiety, depression, and their physical complaints
during adolescence. The purpose of this study is to begin to address the specific issue of how
family circumstances (i.e., family economic hardships, and marital conflicts, and supportive
parenting) influence adolescents’ depression, anxiety, and physical complaints. Moreover, this
study examines how anxiety, depression, and physical complaints mutually influence one
another over time. Figure 2 depicts the specific hypotheses for this research.
Hypothesis 1. Chronic family adversity (i.e., economic hardships) directly influences
adolescents’ health problems (i.e., anxiety, depressive symptoms, and physical
complaints), controlling for parental education and parental depression.
Hypothesis 2. Chronic family adversity indirectly influences adolescents’ health problems
through marital conflicts, controlling for parental education and parental
depression. (Mediating effect.)

24
Hypothesis 3. Chronic family adversity indirectly influences adolescents’ health problems
through supportive parenting, controlling for parental education and parental
depression. (Mediating effect.)
Hypothesis 4. Marital conflicts indirectly influences adolescents’ health problems through
supportive parenting, controlling for parental education and parental depression.
(Mediating effect.)
Hypothesis 5. Adolescents’ anxiety, depression, and physical complaints mutually influence
one another over time, controlling for parental education and parental depression
(cross-lagged effect).
Hypothesis 6. The association between chronic family economic hardships and adolescents’
health problems is moderated by supportive parenting (moderating effect).
Hypothesis 7. The association between marital conflicts and adolescents’ health problems is
moderated by supportive parenting (moderating effect).
Hypothesis 8. Gender moderates the associations among adolescents’ health problems over the
years.
Hypothesis 9. Gender moderates the associations among family economic hardships,
supportive parenting, marital conflicts, and adolescents’ health problems.

25
CHAPTER 3
METHODS AND MEASUREMENTS
Sample
This study sampled 424 adolescents, who participated in the Iowa Youth Project (IYFP)
and Family Transitions Project (FTP). The IYFP began in 1989 and involved 451 families in 8
counties in Iowa. The site for the research was determined by an interest in rural economic stress
and well-being. Because many of the outcomes and processes considered in the overall study
were concerned with adolescent development, the families selected had at least two adolescents.
Beginning in 1994, the IYFP samples were combined with the FTP.
Data for the current study’s analyses originated from Wave 1 (N= 451), Wave 2 (N= 424),
Wave 3(N= 407), Wave 4(N= 404) of the IYFP, and Wave 6(N= 424) for the FTP longitudinal
study. Predictor variables of chronic family economic hardships were gathered through target
self-reported measures from Wave 1 (1989) to Wave 3 (1991). Supportive parenting was
assessed through parents’ self-report at Wave 2. This variable consisted of perceived father’s
support and mother’s support. The adolescents were in 7th grade and in the age range of 12-14
years of age when information on the predictor variables was collected in 1989. The longitudinal
IYFP study at Wave 3, Wave 4, and Wave 6 produced information on the outcome variables—
anxiety, depression, and physical complaints. At the time of the initial wave in 1989, 34% of the
families lived on a farm, around 12% lived in rural areas but not specifically on a farm, and 54%
of the families lived in rural communities with a population less than 6,500 (Conger et al., 1992).
The median family income of the previous year of the study (1988) was $33,000 and 11% of the

26
families in the IYFP data set had a median income that fell below the federal poverty line
(Conger et al., 1992). The median number of years of education was 13 years for fathers and
mothers, and the median age for fathers was 39 years and 37 years for mothers (Conger et al.,
1992). The average number of family members for the IYFP sample in 1989 was 4.95 children
(Conger et al., 1992). Around 53% of the targeted adolescents were female and 47% were male.
Procedure
Families were contacted prior to participation and information regarding participation
was obtained through letters in the mail and telephone-based interactions. Around 78% of the
participants who were contacted agreed to participate in the current study.
Data for this study originated through home visit methodologies (Conger et al., 1992).
For each wave, families were interviewed two different times. During the first visit, each of the
four family members was asked demographics, family economic circumstances, family
characteristics, and self-reports on behavior and cognitions/attitudes through surveys (Conger et
al., 1992). The second home visit, within 2 weeks of the first visit, consisted of the family
completing a structured task to assess interactions within the families. Coders were trained using
the Iowa Families Interactions Rating Scales (IFIRS) developed by Janet Melby and colleagues
at the Institute for Social and Behavioral Research at Iowa State University (Melby et al., 1999).
Coders were required to have a minimum of a bachelor’s degree in science, humanities, literature,
or education (Melby & Conger, 2001) and work no more than 20 hours a week, due to the high
intensity of the job. Coders were trained for 10-12 weeks at 20 hours per week to achieve a high
level of agreement (Melby & Conger, 2001).

27
Data from the current study only utilized the first home visit in which survey information
was collected. This current study did not utilize information collected during the second home
visit in which observational data were collected on a structured task.
Measures
Anxiety In 1991, 1992, and 1994, target adolescents reported their feelings on how much anxiety
they felt during a week. Anxiety in the current study was assessed from 10 sub-items from the
Symptoms Checklist (SCL-90-R; see Derogatis & Melisaratos, 1983). First, the target
adolescents were asked to report on anxiety on a scale from 1 (not at all) to 5 (extremely),
regarding “During the past week, how much were you distressed or bothered by ‘nervousness or
shakiness inside’, ‘trembling’, ‘suddenly scared for no reason’, ‘feeling fearful’, ‘heart pounding
or racing’, ‘feeling tense or keyed up’, ‘spells of terror or panic’, ‘feeling so restless you couldn’t
sit still’, ‘the feeling that something bad is going to happen to you’, and ’thoughts and images of
a frightening nature’.” Scores on these items were then summed in which higher levels of the
summed score reflect higher levels of anxiety. The internal consistency (Cronbach’s alpha) for
the scale equaled .83, .85, and .90 for 1991, 1992, and 1994, respectively, for the target
adolescents.
Depressive symptoms In 1991, 1992, and 1994, target adolescents reported their feelings of
distress using the 12-item depressive symptomology subscale of the Symptoms Checklist (SCL-
90-R; see Derogatis and Melisaratos, 1983). Respondents used a 5-point Likert-type scale
anchored with ‘not at all’ (1) and ‘extremely’ (5), regarding “how often during the past week
they were bothered by ‘feeling low in energy or slowed down’, ‘thoughts of ending your life’,
‘crying easily’, ‘feelings of being trapped or caught’, ‘blaming yourself for things’, ‘feeling
lonely’, ‘feeling blue’, ‘worrying too much about things’, ‘feeling no interest in things’, ‘feeling

28
hopeless about the future’, ‘feeling everything is an effort’, and ‘feelings of worthlessness’,”
Scores on these items were then summed in which higher levels of the summed score reflect
higher levels of depression. Internal consistency (Cronbach’s alpha) equaled .89, .91, and .92 for
1991, 1992, and 1994, respectively.
Physical complaints In 1991, 1992, and 1994, target adolescents reported their feelings of
physical condition using 12 common physical complaints. These complaints included headaches,
coughs, sore throats, muscular aches, stomach aches, congested nose, constipation, vomiting,
skin rashes, diarrhea, allergies, and bad acne or pimples experienced during the past three
months (Mechanic & Hansell, 1987). Respondents used a 4-point scale anchored with ‘never’ (1)
and ‘always’ (4) to indicate how often during the past three months they were bothered by
symptoms of physical complaints. Scores on the items were then summed in which higher levels
of the summed score reflect higher levels of physical complaints. Internal consistency
(Cronbach’s alpha) equaled .76, .74 and .77, for 1991, 1992, and 1994, respectively.
Marital conflict In 1991, marital conflict was measured by asking both father and mother to
report, on a five-point scale from “never” (0) to “all of the time” (4), how often you and your
spouse disagree or get upset about “Money,” “Discipline/ raising children,” “Time along
together,” “Tobacco,” “Alcohol,” “Drugs,” “Outside activities,” “Work schedules,” “Church,”
“Vacation time,” “Intimate times,” “Household chores,” “Relative/In-laws,” “Family time
together,” “Transportation,” and “Attitudes.” The rating for each item was summed to create a
score of marital conflict for each parent. Internal consistency (Cronbach’s alpha) equaled .87 for
father and .84 for mother.
Supportive Parenting In 1991, supportive parenting was measured by asking both father and
mother to report on a five-point Likert-type scale from “always” (1) to “never” (5), “I really trust

29
target child,” “I experience strong feelings of love for target child,” “How often do you talk with
the target child about what is going on in his or her life?,” “When you and the target child have a
problem, how often can the two of you figure out how to deal with it?,” “How often odes the
target child talk to you about things that bother him or her?,” “How often do you ask the target
child what he or she thinks before deciding on family matters that involve him or her?,” “How
often do you give reasons to the target child for your decisions?,” “ How often do you ask the
target child what he or she thinks before making decisions that affect him or her?,” “When the
target child has done something you like or approve of, how often do you let him or her know
you are pleased about it?”. The lists of supportive parenting were adapted from the supportive
parenting scale (Simons, Lorenz, Conger, & Wu, 1992). The rating for each item was reverse
coded so that a high score indicated high support. The supportive parenting scale was
constructed by summing the score for both parents. Internal consistency (Cronbach’s alpha)
equaled .87 for father’s supportiveness, and .84 for mother’s supportiveness.
Chronic Family economic hardships The lists of economic problems were adapted from Conger
(1988). The measure of family economic hardships was created by a 5-point Likert-type scale
anchored with ‘always’ (1), and ‘never’ (5). The targets responded to four items in1989, 1990,
and 1991, that indicated economic problems experienced by the family. The list of economic
problems included items, such as “How often do you have enough money for things like clothes,
school activities, or other things you need?,” “How often do you have enough money for doing
things you and friends like to do, such as going to movies, eating pizza, etc.?,” “How often do
you argue with your parents about not having enough money?,” and “How often do your parents
argue with each other about not having enough money?”. Two items were reverse-coded. Scores
on these items were then summed in which higher levels of the summed score reflect higher

30
levels of family economic hardships. The internal consistency (Cronbach’s alpha) of the scale
equaled .67, .70, and .67 for 1989, 1990, and 1991, respectively.
Parental depressive symptoms (control variable) Participants reported their feelings of distress
using the 13-item depressive symptomology subscale of the Symptoms Checklist (SCL-90-R;
see Derogatis and Melisaratos, 1983). Respondents used a 5-point Likert-type scale anchored
with ‘not at all’ (1) and ‘extremely’ (5) regarding how often during the past week they were
bothered by ‘loss of sexual interest or pleasure’, ‘feeling low in energy or slowed down’,
‘thoughts of ending our life’, ‘ crying easily’, ‘feelings of being trapped or caught’, ‘blaming
yourself for things’, ‘feeling lonely’, ‘feeling blue’, ‘worrying too much about things’, ‘feeling
no interest in things’, ‘feeling hopeless about the future’, ‘feeling everything is an effort’, and
‘feelings of worthlessness’. Scores on these items were then summed in which higher levels of
the summed score reflect higher levels of depressive symptoms. Internal consistency
(Cronbach’s alpha) equaled .92 for both father and mother.
Parental education (control variable) Parental education was measured by the number of years
of formal education and constructed by summing scores for both parents reported in 1991. The
mean score for father and mother is 13.54 and 13.35 years, respectively.
Gender (moderate variable) This current study also assessed the gender of the adolescent
through self-reported items. Gender was coded as 0 for females and 1 for males.
Analytical Plan
Prior to testing the hypotheses, descriptive statistics will be calculated for all this study’s
measures. Descriptive statistics include means, ranges, standard deviations, skewness, and
Cronbach’s alpha. Table 1 displays descriptive statistics, and Table 2 displays the mean
difference between males and females on study’s variables. Table 3 displays the correlations of

31
this study’s variables. The current study uses Structural Equation Modeling (SEM) to assess the
hypothesized longitudinal path model. SEM in the current study was employed to reduce the
impact of measurement error and analyze three repeated measures of health outcomes on the
succinct causal model. The latent construct of family economic hardships is captured by three
multiple indicators measured in 1989, 1990, and 1991, respectively. Moreover, the latent
construct of marital conflict is also calculated using two multiple indicators, which include
father’s and mother’s reports in 1991. The latent construct of supportive parenting is also
calculated using two multiple indicators, which include father’s and mother’s report in 1991. The
constructs of anxiety, depression, and physical complaints are measured directly by self-reported
measures. These observed measures were constructed by summing scores of individual items and
dividing the total of the items by the number of items to achieve a mean score.
Computer software program, AMOS 18.0, will be utilized to estimate standardized and
unstandardized coefficients for all paths in the SEM model. The default missing data program in
AMOS version 18.0 will use FIML (full-information maximum likelihood) to impute missing
data for all missing values. Also, model fit information will be calculated using absolute fit index
such as Chi-Squared and goodness of fit indices such as Root Mean Squared Error
Approximation (RMSEA), Comparative Fit Indices (CFI), and Tucker Lewis Index (TLI). For
good model fit, Hu and Bentler (1999) suggested that RMSEA values be close to .06 or below,
and CFI and TLI values be close to .95 or greater for model fit. However, for acceptable model
fit, Browne and Cudeck (1993) proposed that RMSEA values less than .07 and CFI and/or TLI
values in the range of .90 - .95 suggest an acceptable model fit.
The SEM framework will allow for the current study to test Hypotheses 1. This is the
direct pathways in the SEM framework.

32
Meditational Hypotheses
Three mediation effects are assessed using the two approaches in the Structural Equation
Modeling. The first approach for testing the mediating effect is the nested modeling approach in
the SEM framework (Baron & Kenny, 1986). According to this approach, mediation is said to
occur when the causal effect of an independent variable (X) on a dependent variable (Y) is
transmitted by a mediator (M). “Indirect effects” estimate the magnitude of mediation. In other
words, X affects Y because X affects M, and M, in turn, affects Y.
For example, to examine the mediating effect of marital conflicts and supportive
parenting on the association between chronic family economic hardships and adolescents’ health
problems, the first step in this analysis is to employ an SEM model in which the latent constructs
of chronic family economic hardships directly influence each of the outcome variables (i.e.,
anxiety, depression, and physical complaints) (M 1). The second step in the mediation analysis is
to create a model in the SEM framework in which the latent constructs of chronic family
economic hardships directly influence each outcome variable, as well as chronic family
economic hardships indirectly influencing each of the outcome variables through marital
conflicts (M 2), supportive parenting (M 3), and both marital conflicts and supportive parenting
(M4), respectively. The final step is to compare the direct path model (M 1) with the mediation
models (M 2, M 3, and M4). These models will be compared and discussed in the results section
to address hypotheses 2, 3, and 4. If direct paths become non-significant and meditational paths
are significant in meditational model (M 2, M 3, and M4), according to Baron and Kenny (1986),
supportive parenting and marital conflicts mediated the influence of chronic family economic
hardships on health problems.

33
For the second approach, the mediating effects of the current study are assessed using a
mediation test proposed by Sobel (1982). According to this test, the amount of mediation which
can be tested by the z-test is defined as the reduction of the effect of the initial variation on the
outcome or c – c’. This difference in coefficients is equal to the product of the effect of X on M
times the effect of M on Y or ab and so:
ab = c – c’ .
If this indirect effect on the second step of the nested modeling approach is statistically
significant, it follows there necessarily is a reduction in the effect of X on Y. One method to test
the null hypothesis (i.e., indirect effect) that ab = 0 is to test if both a and b are zero. Baron and
Kenny (1986) provide a direct test of ab, which is a modification of a test originally proposed by
Sobel (1982). This requires the standard error of a or Sa (which equals a/ta where ta is the t-test of
coefficient a) and the standard error of b or Sb (See Figure 3).
The standard error of ab equals
SEab = .
Therefore, under the null hypothesis that ab equals zero, the following,
,
is approximately distributed as z. In most cases, however, the term is insignificantly small
and can be safely omitted, yielding:
SEab = .
Hence, following the recommendation from MacKinnon, Warsi, and Dwyer (1995), the
significance of the indirect paths can be assessed using the modified Sobel test of indirect
effects:

34
z – value = .
To test the significance of the indirect effect, it was calculated by hand because this test is
not available in AMOS. A significant Sobel test suggests the level of mediation is meaningful.
The significance of the indirect paths can be assessed using the modified Sobel test of indirect
effects. According to the z-test, the mediating effect of hypotheses 2 – 4 will be assessed.
Cross-lagged hypothesis
The current study will examine a cross-lagged model to strengthen the hypothesized
associations of the theoretical path model using AMOS 18.0. Using a cross-lagged design, the
reciprocal relationship between mental problems and physical complaints will be explored in
greater detail. The benefit of this design is that it offers insight into the relative strengths of two
or more time-varying covariates on each other (Lorenz, Wickrama, & Conger, 2004). To
examine the health progression of adolescents, the “cross-lagged model” will be tested for
Hypothesis 5.
Moderational hypotheses
Moderation effects will be assessed through a stacked model approach using two groups
for the low and high levels of supportive parenting (Wickrama et al., 1995). In this approach, the
path coefficients are allowed to be different in one model for the low and the high groups, based
on one standard deviation from a mean of the grouping variable (i.e., unconstrained model). A
second model will be analyzed in which the path coefficients are held constant for the low and
high groups (i.e., constrained model). According to Bentler and Bonett (1980), a 2 difference
can be calculated for the constrained model subtracted from the unconstrained model. The 2
difference will have degrees of freedom equal to the degrees of freedom of the constrained

35
model minus the unconstrained model, and will be normally distributed. This 2 difference test
will allow for the test of significance for any significant interactions or moderations between
high and low groups for hypotheses 6 and 7.
Gender moderational hypotheses
Finally, to investigate the hypothesized gender difference, the model shown will estimate
the cross-lagged model and path model separately for males and females; these results will be
presented . The model allows comparison of male’s paths with corresponding female’s paths
using the equality constraint test (Wickrama et al., 1995). In these tests, the two theoretically-
relevant paths are constrained as equal in the model to determine whether this procedure would
significantly reduce the model fit. The change in chi-squared for one degree of freedom for each
paired comparison will be used to test whether two paths are significantly different for
hypotheses 8 and 9. Also, for Hypothesis 8, the group’s mean between male and female will be
estimated to report on whether group means among anxiety, depressive symptoms, and physical
complaints change for 1991, 1992, and 1994.
Supplement Growth Curve Analysis
Moreover, as a supplementary analysis, latent growth curve (LGC) analysis will be
performed using AMOS 18.0. The LGC model estimates individual change parameters, as well
as their differences across individuals, and systematically relates these differences to the
differences in time-invariant and/or time-varying predictors and in Sequence across individuals
(Karney & Bradbury, 1995; Wickrama, Beiser, & Kaspar, 2002). For example, this study will
relate growth parameters for depression, anxiety, and physical complaints to marital conflicts,
supportive parenting, and economic hardships, and then take the associations among growth
parameters into account.

36
CHAPTER 4
RESULTS
Descriptive Statistics of Study Variables
Table 1 presents of the descriptive statistics of the study variables for the current research.
The mean scores for anxiety showed no significant change over time; 1.40, 1.37, and 1.39, for
1991, 1992, and 1994, respectively (F(2, 752)=1.18, p>.05). However, the mean scores for
depression showed a significant increase; 1.51, 1.57, and 1.62, for 1991, 1992, and 1994,
respectively (F(2, 752)=4.99, p<.01). Also, the mean scores for physical complaints showed a
significant increase; 1.92, 2.03, and 2.01, for 1991, 1992, and 1994 (F(2, 696)=12.43, p<.001).
The mean scores for family economic hardships indicated a significant difference over time; 2.11,
2.08, and 2.20 for 1989, 1990, and 1991, respectively (F(2, 804)=9.40, p<.001). The mean scores
for marital conflicts showed no significant difference; 1.13, and 1.10, for father and mother
respectively (F(1, 396)=1.60, p>.05). Supportiveness for fathers and mothers indicated
significant differences, 3.79 and 4.02 in 1991, respectively (F(1, 405)= 92.92, p<.001). The
mean scores for parental depression indicated a significant difference in 1991, 1.32 for father and
1.50 for mother, respectively (F(1, 405)= 30.18, p<.001). Finally, mean scores for fathers and
mothers’ education were 13.54 and 13.35 years in 1991, respectively.
For the most part, skewness is not an issue for the distribution of the current study’s
variables. Father’s depression in 1991 was the most skewed variable among predictors. However,
this skewness is to be expected, based on the nature of the study variables and the self-report
measurement technique, which is subject to a potential bias in the answers.

37
Mean difference in health problems between males and females are provided in table 2.
Females report higher mean levels of depression, anxiety, and physical complaints in several
time points.
Correlations among Study Variables
Table 3 presents bivariate correlations among study variables. All outcome variables
were correlated in the expected direction. Significant correlations were observed among repeated
measures of anxiety symptoms in 1991, 1992, and 1994 (p<.01). Significant positive correlations
were also observed among repeated measures for depressive symptoms in the same period
(p<.01). Furthermore, significant positive correlations were observed among repeated measures
for physical complaints in the same period (p<.01). Also, significant contemporaneous and
longitudinal positive correlations were observed among different health domain variables;
anxiety and depressive symptoms (p<.01), between depression and physical complaints (p<.01),
and between anxiety and physical complaints (p<.01) (See Table 2).
For predicted variables, as expected, a significant correlation was observed among family
economic hardships in 1998, 1990, and 1991. The correlations ranged from .41 to .51 (p<.01). In
addition, these variables showed significant correlations with adolescents’ health problems (i.e.,
anxiety, depression, and physical complaints). The correlation coefficient ranged from .10 to .29
(p<.05) Moreover, a moderate correlation was observed between father’s marital conflicts and
mother’s marital conflicts measures. The correlation was .38 (p<.01). These variables were also
significantly correlated with most health problems during the same time period. The correlations
ranged from .11 to .15 (p<.05). However, marital conflicts for both father and mother were not
correlated with depression in 1992 and 1994. Additionally, marital conflicts measures for both
parents were significantly correlated with family economic hardships in 1989, 1990, and 1991.

38
The correlations ranged from .10 to .27 (p<.05). Furthermore, a significant correlation was
observed between fathers’ supportive and mothers’ supportive parenting. The correlation was .31
(p<.05). In addition, these variables were negatively correlated with anxiety and depression in
1991, 1992, and 1994. The correlation coefficients ranged from -.21 to -.12 (p<.05). However,
parental support for both parents was not significantly correlated with physical complaints in the
same time period. Nevertheless, parental support for both father and mother was significantly
correlated with marital conflicts and family economic hardships. The correlation between marital
conflicts and supportive parenting for both parents ranged from -.22 to -.11 (p<.05).
Testing Specific Hypotheses
Direct Path Model (Hypothesis 1)
The first hypothesis of the current study was that chronic family economic hardships
directly influence adolescents’ anxiety, depression, and physical complaints, controlling for
parental depression and education. The results can be seen in Figure 4. For anxiety, the chronic
family economic hardships directly influences anxiety in 1991 (β= .21, t=3.53). For depression,
the family economic hardships directly influence depression in 1991 (β= .29, t=4.84). Moreover,
for physical complaints, the family economic hardships directly influence adolescents’ physical
complaints in 1991 (β= .29, t=4.73). Thus, the first hypothesis of the current study was supported
by data.
Mediations of the Current Study (Hypothesis 2, 3, and 4)
Testing mediational hypothesis for marital conflicts on the association between chronic family
economic hardships and adolescents’ health problems (Hypothesis 2)
Figure 4 presents a simple SEM model in which the chronic family economic hardships
directly influence adolescent health problems. Figure 5 presents an SEM model in which the

39
chronic family economic hardship indirectly influences adolescents’ health problems through
marital conflicts (MC).
The model in Figure 4 can be compared to Figure 5 to assess the meditational effects of
marital conflicts on the association between the family economic hardships and adolescents’
health problems. The model in Figure 5 adds marital conflicts to the model in Figure 4. The
model in Figure 5 found a direct pathway between family economic hardships and adolescents’
health problems. In Figure 5, the pathway between family economic hardships and adolescents’
health problems was still significant (β=.20, t=2.96 for anxiety; β=.25, t=3.70 for depression, and
β=.28, t=4.05 for physical complaints). Moreover, the pathway between family economic
hardships and marital conflicts was significant in the model for Figure 5 (β=.38, t=4.32). The
pathways for family economic hardships and adolescents’ health problems shown in Figure 4 are
still significant in the model, as shown in Figure 5. The pathway between family economic
hardships and marital conflicts was significant. However, the pathways among marital conflicts
and all of health problems of adolescents were not significant, as shown in Figure 5. Thus, the
Sobel test cannot be used because indirect effect between chronic family economic hardships and
adolescents’ health problems is not statistically significant. Accordingly, the current study
suggests the association between chronic family economic hardships and adolescents’ health
problems is not mediated by marital conflicts, based on the mediating tests proposed by Baron
and Kenny (1986) and modified Sobel test (1995). Thus, the second hypothesis of the current
study was not supported by data.
Testing mediational hypothesis for supportive parenting on the association between chronic
family economic hardships and adolescents’ health problems (Hypothesis 3)

40
Another mediation to examine is whether supportive parenting mediates the association
between chronic family economic hardships and adolescents’ health problems. To examine this,
the current study compares the model shown in Figure 4 with the model shown in Figure 6. In
the hypothesized model of the current study shown in Figure 6, a significant association was
observed between chronic family economic hardships and supportive parenting (β= -.37, t=-3.99).
A significant association was also observed between supportive parenting and anxiety (β= -.28,
t= -2.95). However, a significant association was not observed between chronic family economic
hardships and anxiety as found for the model in Figure 6 (β=.11, t=1.67). This demonstrates the
association between chronic family economic hardships and anxiety is mediated by supportive
parenting. For depressive symptoms of adolescents, Figure 6, a significant association was
observed between supportive parenting and depression (β= -.26, t= -2.83). Also, a significant
association was still observed between chronic economic hardships and depression (β= .19, t=
2.81). However, when this model is compared with the model in Figure 4, the standardized
regression coefficient in the association was diminished from .28 (4.84) to .19 (2.81). According
to analysis of mediation hypotheses presented by Baron and Kenny (1986), to establish
supportive parenting completely mediates the association between chronic economic hardships
and depression, the effect of chronic economic hardships on depression of adolescents
controlling for supportive parenting should not be significant. However, although the direct
effect is reduced in the association between chronic family economic hardships and depression in
the current hypothesized model, the direct influence of chronic family economic hardships on
depression is still significant when controlling for supportive parenting. Therefore, partial
mediation on the association between chronic economic hardships and depressive symptoms of
adolescents is indicated. For physical complaints, a significant association was not observed

41
between supportive parenting and physical complaints (β= .07, t= .91) shown in Figure 6.
However, a direct pathway was significantly observed between chronic family economic
hardships and physical complaints (β=.31, t=4.46). Therefore, the relationship between chronic
family economic hardships and adolescents’ physical complaints is not mediated by supportive
parenting.
Moreover, to test the significance of the indirect effect, the recommendations by
MacKinnon, Warsi, and Dwyer (1995) are followed. For anxiety, the indirect effect using the
modified Sobel test is statistically significant (z = 2.35, p<.01); for depression, the indirect effect
is also significant (z = 2.23, p<.05). However, for physical complaints, the z-value for the Sobel
test was not calculated, because the indirect effect of the nested modeling approach is not met
(e.g., step 2 of the nested modeling approach).
In summary, supportive parenting mediates the association between chronic family
economic hardships and anxiety of adolescents, and partially mediates the association between
chronic family economic hardships and depression of adolescents. However, supportive
parenting did not mediate the association between chronic family economic hardships and
physical complaints. Thus, the third hypothesis of the current study was partially supported by
data.
Indirect effect of marital conflicts on adolescents’ health problems through supportive parenting
(Hypothesis 4)
The other mediation to examine is whether supportive parenting mediates the association
between marital conflicts and adolescents’ health problems. In the hypothesized model of the
current study shown in Figure 7 for anxiety and depression, a significant association was
observed between marital conflicts and supportive parenting (β= -.41, t= -3.26). A significant

42
association was also observed between supportive parenting and anxiety (β= -.31, t= -2.75), and
between supportive parenting and depression (β= -.26, t= -2.49), respectively. However, a
significant direct effect was not observed between marital conflicts and anxiety (β= -.07, t= -.72)
and between marital conflicts and depression anxiety (β=.01, t=.04) shown in Figure 7. Thus,
this suggests the association between marital conflicts and anxiety is mediated by supportive
parenting. The association between marital conflicts and depression is also mediated by
supportive parenting. For physical complaints, a significant association was not observed
between supportive parenting and physical complaints (β= .10, t= 1.00), as well as between
marital conflicts and physical complaints anxiety (β= .07, t=.79) shown in Figure 7. Therefore,
the results show the association between marital conflicts and physical complaints of adolescents
is not mediated by marital complaints (MC).
In addition, the z-values for the modified Sobel test were calculated to assess the
significance of the indirect effect. For anxiety, the indirect effect using the modified Sobel test is
statistically significant (z = 2.25, p<.05); for depression, the indirect effect is also significant (z =
2.18, p<.05). However, for physical complaints, the z-value for the Sobel test was not calculated,
because the indirect effect of the nested modeling approach is not met (e.g., step 2 of the nested
modeling approach).
In summary, supportive parenting mediates the association between marital conflicts
and anxiety and depression of adolescents. However, supportive parenting does not mediate the
association between marital conflicts and physical complaints. Thus, the fourth hypothesis of the
current study was partially supported by data.
The Operationalized SEM Model
43
Figure 8 presents the results for the comprehensive model. The factor loadings for the
study variables for the full operationalized model are presented in Figure 8. Three repeated
measures of family economic hardships significantly loaded on the latent construct of family
economic hardships (β= .66, .73, and .65, p< .001). Father’s marital conflicts (β= .65) and
mother’s marital conflicts (β= .59) also significantly loaded on the latent construct of marital
conflicts (p< .001). In addition, Father’s supportive parenting (β= .59) and mother’s supportive
parenting (β= .52) significantly loaded on the latent construct of marital conflicts (p< .001). The
operationalized model had a χ2 of 262.28 with 123 degrees of freedom. The ratio of χ2 divided by
the degrees of freedom equaled 2.13. According to Carmines and McIver (1981), a χ2 divided by
a degrees of freedom ratio of less than 3.00 suggests an acceptable fit, thus confirming this
model fits the data very well. Also, other model fit indices, such as CFI and TLI, indicate the
model fits the data very well.
For the control variables, contrary to expectations, parental education and depressive
symptoms fail to significantly predict anxiety, depressive symptoms, and physical complaints in
1991, 1992, and 1994.
Cross-Lagged Hypotheses (Hypothesis 5)
The fifth hypothesis of the current study is that adolescents’ anxiety, depression, and
physical complaints mutually influence one another over time, controlling for parental education
and depression. This hypothesis was partially confirmed in the current study as the several
significant associations among anxiety, depression, and physical complaints were observed. As
seen in Figure 8, for the association between anxiety and depression, depression in 1991
significantly predicts anxiety in 1992 (β=.14, t=2.18), and anxiety in 1992 significantly predicts
depression in 1994 (β=.15, t=2.01). Moreover, for the association between depression and

44
physical complaints, physical complaints in 1991 significantly predict depression in 1992 (β=.14,
t=3.28) and physical complaints in 1992 moderately predict depression in 1994 (β=.09, t=1.85).
Also, for the association between anxiety and physical complaints, the results indicate physical
complaints in 1991 significantly predict anxiety in 1992 (β=.10, t=2.17) and physical complaints
in 1992 significantly predict anxiety in 1994 (β=.12, t=2.34). However, the results show
depression in 1991 and 1992 does not predict physical complaints in 1992 and 1994. Anxiety in
1991 and 1992 also failed to influence physical complaints in 1992 and 1994. Consequently, the
fifth hypothesis of the current study was partially supported by data.
Moderation of the Current Study (Hypotheses 6 and 7)
Supportive parenting moderating hypotheses
Descriptive statistics show the measures for marital conflicts, supportive parenting, and
adolescents’ outcomes were all normally distributed. Therefore, the present study proceeded to
test the moderating effects (McClelland & Judd, 1993). Hypotheses 6 and 7 test the moderation
effects of supportive parenting on the association between chronic family economic hardships
and adolescents’ health problems, and between marital conflicts and adolescents’ health
problems using a stacked model approach (Wickrama, Conger, Lorenz, & Matthews, 1995).
According to this approach, the same structural model is estimated, using these two groups
simultaneously. Multiple group analysis is useful to test for differences using the “parameter
invariance” method of structural equation modeling.
In accordance with the guidelines set forth by Brookmeyer, Henrich, and Schwab-Stone
(2005), as a first step in the analysis, two groups (i.e., high vs. low supportive parenting group)
were selected from the sample in the following order (without replacement). First selected was
the low supportive parenting group—the low group whose score on supportive parenting in 1991

45
was equal to or less than one standard deviation (.34) away from the mean score (3.91) of
supportive parenting. Second, from the remaining parents, the high supportive parenting group
was selected—the high group whose score was equal to or more than one standard deviation
from the mean score of supportive parenting.
The current study followed the procedure for a stacked models approach used by
Wickrama et al. (1995) to test for moderations of study variables. According to this approach, for
the moderation effect on supportive parenting on the association between chronic family
economic hardships and adolescents’ health problems, a first model was analyzed in which the
all paths were freed across the two models. The second model was analyzed in which the path of
interest was constrained to be equal.
The fit between the model with equally constrained paths and the model with freed paths
can then be compared using a χ2 difference test (Bentler & Bonett, 1980; Wickrama et al.,
1995). For all model comparisons, a χ2 difference of 3.83 with a 1 degree of freedom is deemed
a significant moderation effect. The stacked models address hypotheses 6 and 7. Table 4
provides a summary of standardized coefficients (β), associated standard errors, intercepts, and
the differences in χ2 between low and high groups.
The first series of moderations to examine involve Hypothesis 6. This hypothesis states
the relationship between chronic family economic hardships and adolescents’ health problems is
moderated by the level of supportive parenting. For anxiety, A non-significant moderation effect
of supportive parenting on the association between chronic family economic hardships and
anxiety ( χ2= .01, df=1) was observed. For depressive symptoms, a non-significant moderation
effect of the level of a supportive parenting on the association between chronic family economic
hardships and depression ( χ2= .03, df=1) was observed. Moreover, for physical complaints, a

46
non-significant moderation effect of the level of a supportive parenting on the association
between chronic family economic hardships and physical complaints ( χ2= .18, df=1) was
observed.
In summary, there was no significant moderation in the level of supportive parenting on
the association between chronic family economic hardships and adolescents’ health problems.
Therefore, Hypothesis 6 was not supported by data.
The second series of moderations to examine involve Hypothesis 7. This hypothesis
states the association between marital conflicts and adolescents’ health problems is moderated by
the level of supportive parenting. For anxiety, a non-significant moderation effect of supportive
parenting on the association between marital conflicts and anxiety ( χ2= .26, df=1) was observed.
However, for depressive symptoms, a significant moderation effect of supportive parenting on
the association between marital conflicts and depression ( χ2= 4.13, df=1) was observed. Figure
9 illustrates the moderating effect of supportive parenting on the association between marital
conflicts and adolescents’ depressive symptoms. The graph clearly shows the interpretation for
the results of moderation. As shown in Figure 9, low level of supportive parenting had lower
average levels of depressive symptoms (M=1.71, SD=.66) than the higher level of supportive
parenting (M=1.35, SD=.40). Also, this mean difference was statistically significant (t=3.94, p
<.001). More importantly, the influence of marital conflicts on depressive symptoms was
stronger for low-level supportive parenting group than for high-level supportive parenting group.
However, for physical complaints, a non-significant moderation effect of supportive parenting on
the association between marital conflicts and physical complaints ( χ2= 1.58, df=1) was
observed.

47
Consequently, Hypothesis 7 was partially confirmed in the current study. There was only
a significant moderation of supportive parenting on the association between marital conflicts
and depressive symptoms.
Gender Difference of the Current Study (Hypotheses 8 and 9)
As in the case of supportive parenting effect, the two theoretically relevant paths are
constrained to be equal across male and female models to determine whether this procedure
would significantly reduce the model fit compared to the unconstrained model. The change in
chi-squared for one degree of freedom for each paired comparison is used to test whether two
paths are significantly different across male and female groups. Through 2 difference testing, a
model constraining path coefficient was analyzed for males and females.
Figure 10 presents the comprehensive model for gender difference on adolescents’ health
probles from 1991 to 1994. Among the 27 interaction effects, only one significant moderating
mechanism was seen in Table 5. For intra-domain continuity (i.e., homotypic continuity), the
stability coefficient of depressive symptoms in 1992 on depressive symptoms in 1994 was only
significantly different for males and females ( χ2= 5.00, df=1). Thus, Hypothesis 8 was partially
supported by data.
The other series of gender differences to examine involve Hypotheses 9. This hypothesis
states that gender moderates the associations among the family economic hardships, supportive
parenting, marital conflicts, and adolescents’ health problems. The moderating effects of gender
for the hypothesized path model can be seen in Figure 11. Through χ2 difference testing, a model
constraining all paths coefficients was analyzed for male and female. The result was a 2
difference of 40.06 with 19 degrees of freedom. This is statistically significant. In other words,
there is significantly different between males and females on the association among anxiety,

48
depression, and physical complaints over time. In detail, Table 6 presents the summary of
standardized coefficients, associated standard errors, and the difference in 2 between the
constrained model and the unconstrained model for each path for both the male and female
groups.
Among the 12 paths, two significant moderating mechanisms were seen in Table 6. For
depressive symptoms, gender of the adolescent moderates the association between chronic
family economic hardships and depressive symptoms ( 2 = 5.10, df=1). Also, gender of the
adolescent moderates the association between chronic family economic hardships and marital
conflicts ( χ2= 8.46, df=1). That is, females are more vulnerable to chronic family economic
hardships for both depressive symptoms, (β= .29, t=1.93) and marital conflicts (β= .35, t= 7.00).
Moreover, to examine the moderating effect of gender on the association between chronic
family economic hardships and depressive symptoms in 1991, the graph depicts the moderation.
As shown in Figure 12, males had lower average levels of depressive symptoms (M=1.36,
SD=.39) than females (M=1.63, SD=.53). Also, this mean difference was statistically significant
(t=4.95, p <.001). However, the influence of depressive symptoms on chronic family economic
hardships was greater among females than among males.
Also, in case of marital conflicts, the result of this moderation is quite similar to gender
moderation on association between chronic family economic hardships and depressive symptoms.
The males had lower average levels of marital conflicts (M=1.08, SD=.36) than females (M=1.14,
SD=.37). Although, this mean difference was not statistically significant (t=1.51, p >.05), the
influence of marital conflicts on chronic family economic hardships was greater among females
than among males.

49
In summary, gender of adolescents moderates the association between chronic family
economic hardships and depressive symptoms, and between chronic family economic hardships
and marital conflicts. Although gender marginally influences the association between chronic
family economic hardships and physical complaints, other associations among anxiety, marital
conflicts, and supportive parenting were not impacted by gender. Therefore, Hypothesis 9 was
partially supported by data.
Latent Growth Curve Analysis (Supplementary analysis)
As a supplementary analysis, latent growth curve (LGC) analysis using AMOS 18.0 was
estimated. The LGC model estimates individual change parameters as well as their differences
across individuals, and systematically relates these differences to the differences in time-
invariant and/or time-varying predictors, and in sequence across individuals (Karney & Bradbury,
1995; Wickrama, Beiser, & Kaspar, 2002). Consequently, through this analysis, growth
parameters of depression, anxiety, and physical complaints were related to marital conflicts,
supportive parenting, and chronic family economic hardships, and then the associations among
growth parameters were taken into account. The interlocking LGC model estimates are shown in
Figure 13.
For the current data, the results from fitting linear growth curves to three waves of
anxiety, depressive symptoms, and physical complaints (1991, 1992, and 1994) are summarized
in Table 7. As shown in Table 7, each univariate growth curve model for anxiety, depressive
symptoms, and physical complaints of adolescents showed a respectable fit with the data—a chi-
squared of 2.59, 1df; a chi-squared of .26, 1df; and a chi-squared of 18.88, 1df, respectively. Fit
indies (CFI) for the models also exceeded .90. In Table 7, significant slope shows linear trends in

50
depressive symptoms and physical complaints. More importantly, significant slope variances
show inter-individual variations in the rate of change in health problems.
The three univariate growth curves and exogenous variables were modeled together in an
interlocking trajectory model so that chronic family economic hardships, marital conflicts, and
parenting behaviors predict the adolescents’ health growth model. The interlocking trajectories
model is shown in Figure 13. The model fit indices indicate a good model fit. As expected,
exogenous variables predict the initial level of each health problem (i.e., anxiety, depressive
symptoms, and physical complaints). However, they did not predict the level of change at all. In
addition, Contrary to this researcher’s expectations, several path coefficients showed a negative
impact level of change. According to Conger, Lorenz, and Wickrama (2004), the growth curve
model, in contrast with the autoregressive model, may provide different results based on
correlation coefficients among repeated measures.

51
CHAPTER 5
DISCUSSION
Summary and Understanding the Research Findings
Although a considerable body of empirical research has established the importance of
family context, few studies have examined the unique influences of family factors and their
multiplicative influences on a range of adolescents’ health problems (Wickrama, Conger &
Abraham, 2008). The goals of the current research were to address the unique influences of
chronic family economic hardships as they influence marital conflicts, supportive parenting, and
adolescents’ health problems (i.e., anxiety, depressive symptoms, and physical complaints). To
find unique pathways, the current study also added to the direct and indirect influence by using
an SEM framework. The current research analyzed data from a longitudinal sample of mothers,
fathers, and target adolescents (N= 404-451) to assess theoretical pathways.
The Direct Influences of Chronic Family Economic Hardships
The family stress model posits that cumulative health disadvantages over the life course
by positing that stress proliferation takes a long-term toll on health through a process that places
people already facing serious adversity at risk for continued exposure to further adverse
circumstances (Pearlin, Schieman, Fazio, & Meersman, 2005). According to stress-process
theory, this study demonstrated family mechanisms, which influence risks for developing
adolescents’ health problems over time. The current study also provides support to previous
research (Conger et al., 1992; O’Rand & Hamil-Luker, 2005; Wickrama, Conger, & Abraham,

52
2005). As expected, the current study determined chronic family economic hardships directly
influence anxiety, depressive symptoms, and physical complaints of adolescents.
The Mediating Effect of Marital Conflicts
According to Wadsworth and Compas (2002), parental conflicts partially mediated the
relationship between economic strain and adolescent adjustment. However, the current study
failed to determine the significant mediating effect of marital conflicts on the association
between chronic family economic hardships and adolescents’ health problems (i.e., anxiety,
depressive symptoms, and physical complaints). Moreover, the findings indicated that chronic
family economic hardships still have a direct influence on each of the adolescents’ health
problems after controlling for marital conflicts.
This non-significant direct influence of marital conflicts on adolescents’ health problems
is similar with recent studies. For example, Crockbenberg and Langrock (2001) reported that
marital behavior continued to only predict females' external problems, but not internal problems
such as anger, fear, and depressive symptoms. Moreover, the amount of variance accounted for
by effects was too small (i.e., 5% or less). Furthermore, in Frosch and Mangelsdorf’s study
(2001), they observed marital behaviors were not associated with child functioning.
This pathway between marital behavior and adolescents’ health problems can be inferred
from evidence that correlated parenting behaviors partially explains associations between marital
conflicts and adolescents’ health problems. Consistent with the family process model (Conger et
al., 1992), it appears that marital conflicts primarily influence inefficient parenting, which, in
turn, negatively influences their children (Conger et al., 1992).
Moreover, this association between marital conflicts and adolescents’ outcomes may be
explained by the cognitive contextual framework (Grych & Fincham, 1990), the emotional

53
security hypothesis (Cummings & Davies, 1994), and the specific emotions model (Crockenberg
& Forgays, 1996; Crockenberg & Langrock, 2001). In the cognitive-contextual framework,
emotions are conceptualized as primary responses to parental conflicts, which then influence
secondary, cognitive, processing of the event. Through its relation to cognitions, affect is thus
viewed as a mediator of the relationship between parental conflicts and adolescents’ adjustment.
The emotional security hypothesis conceptualizes affect as an additional index of emotional
security, which is ultimately related to child adjustment (Cummings & Davies, 1994). Last, the
specific emotions model posits that adolescents’ evaluations of marital conflicts lead to affective
reactions, based on adolescents’ expectations of specific goal attainment. These affective
reactions are then theorized to relate to adolescents’ internalizing and externalizing behavior
problems (Crockenberg & Langrock, 2001).
The Mediating Effect of Supportive Parenting
The current study found the association between chronic family economic hardships and
anxiety and depressive symptoms is mediated by supportive parenting. Additionally, supportive
parenting mediated the association between marital conflicts and anxiety and depressive
symptoms of adolescents. These findings are consistent with previous studies. For example,
Wicrama, Lorenz, and Conger (1997) found that through adolescent perception of parental
support, parental supportive behavior is connected with changes in adolescent health problems.
Lempers et al. (1989) also reported that the indirect effects of parental nurturance on the
association economic strain and adolescent depressive symptoms.
Moreover, in case of mediating effects on the association between marital conflicts and
adolescents’ health problems, the current study determined the association between marital
conflicts and adolescents’ mental health problems, such as anxiety and depressive symptoms, is

54
mediated by supportive parenting. This conclusion is similar with research on mediating effect of
parenting on the association between marital conflicts and child adjustment (Kaczynski, Lindahl,
Malik, & Laurenceau, 2006).
However, the current study failed to support the hypothesis that the associations between
martial conflicts and physical complaints and between chronic family economic hardships and
physical complaints are mediated by supportive parenting. These findings are similar with the
findings from previous studies. According to Wickrama et al. (1997), observed parental behavior
do not directly affect physical health status. This means that parental behavior does not have an
independent contemporaneous direct effect on adolescents-reported physical complaints in the
same fashion as perceived parental support does. Because the scale of supportive parenting in the
current study is parent-self reported, the non-significant pathway of supportive parenting on
physical complaints implies that parental supports, which adolescents think is different from the
parental supports which parents think.
In the context of the family process model, chronic family economic hardships impact
their children’s distress through other family factors, such as inefficient parenting (Conger et al.,
1997), parental depressive symptoms (Liber et al., 2008), and marital conflicts (Nicolotti et al.,
2003). In the case of physical complaints, of special interest is the finding that chronic family
economic hardships still significantly influence physical complaints after controlling for marital
conflicts and supportive parenting. This may be due to the fact that chronic family economic
hardships influence adolescent health problems through structural constraints and limitations,
such as lack of food, clothing, proper housing, leisure, and other health resources. Additionally,
recent clinical studies support the evidence that chronic stressful conditions are linked with other
negative physical complaints (Stoney, Niaura, Bausserman, & Matacin, 1999).

55
The Association among Anxiety, Depressive symptoms, and Physical Complaints over time
The results of the cross-lagged model provided evidence that anxiety and depressive
symptoms have mutual influence on one another over the adolescent years. This finding is the
same result as the Dunedin study (Moffitt et al., 2007). According to this study, anxiety and
depressive symptoms have a reciprocal relationship, based on a longitudinal study. Moreover,
the current study tested homotypic continuity of anxiety and depressive symptoms. The results
indicated all stability coefficients of anxiety and depressive symptoms are statistically significant.
This means early anxiety predicts late anxiety, and early depressive symptoms also predict late
depressive symptoms.
However, in the case of physical complaints, although the current study indicated
homotypic continuity of physical complaints, for heterotypic continuity, the study indicates early
physical complaints only predict late depressive symptoms and anxiety, but not vice versa.
In the case for comorbidity, all comorbidities occur over time. Especially, the study
showed that comorbidities between anxiety and depressive symptoms have higher rates than
comorbidity between depressive symptoms and physical complaints, and between anxiety and
physical complaints. This result is consistent with previous studies (Silberg, Rutter, & Eaves,
2001). However, the current research showed that comorbidity among anxiety, depressive
symptoms and physical complaints decreased over adolescence. This result implies that
adolescents consider anxiety, depressive symptoms, and physical complaints respectively over
time.
The Moderating Effect of Supportive Parenting
For the moderating effect, the current study indicated that supportive parenting as a
resilience factor moderated the association between marital conflicts and depressive symptoms

56
of adolescents. This result is consistent with the findings of previous studies (Gordis et al., 1997;
Frosch & Mangelsdorf, 2001). It seems that high-level supportive parenting breaks down
cognitive and emotional mechanisms that link parents’ marital conflicts with generation of
adolescents’ depressive symptoms.
However, supportive parenting did not moderate the association between chronic family
economic hardships and adolescents’ health problems. Moreover, supportive parenting did not
moderate the associations between marital conflicts and anxiety and physical complaints.
Gender Differences
For homotypic continuity, males have a higher stability coefficient for depressive symptoms
than females during 1992-1994. This means that depressive symptoms for males have stronger
homotypic continuity than females over time. Also, in the case of mean differences, females’
health problems (i.e., anxiety, depressive symptoms, and physical complaints) are higher than
males over time. It seems that severity of health problems is greater for females than for males.
This finding is consistent with previous research (Kessler et al., 2005). Furthermore, over the
three years, only males showed decreasing anxiety and increasing depression during the same
period. However, for females, only physical complaints significantly increased.
Furthermore, as can be seen in figure 11, chronic family economic hardship is stronger
associated with depressive symptoms in females. This finding is also consistent with previous
study (Lempers et al., 1989). Additionally, in the present study, females perceived more inter-
parental conflicts in relation to chronic family economic hardships than males. Earlier study may
support this finding. For example, Gottman (1990) suggested that female is largely responsible
for the emotional work in family relationships. Based on this study, adolescents female may be
more sensitive about family adversities such as financial problems and inter-parental conflicts.

57
Implications for the Current Study
The purpose of this study was to explore the mechanisms through which family
economic stressors may positively impact inter-parental conflicts and undermine effective
parenting skills, which, in turn, influence adolescents’ mental and physical health problems.
According to the family stress paradigm, negative stressors, such as economic stress and
negative life events, lead to poor mental health in parents—negatively impacting the marital
relationship and undermining effective parenting. In turn, poor parental mental health, marital
distress, and ineffective parenting are expected to have a cumulative negative impact on
adolescents’ well-being.
Specifically, this study explored whether effective parenting significantly buffered the
negative effects of economic stress and marital conflicts. The implications of such findings
would be that the benefits of positive parental supports may be limited to married couples
because this result may be difficult to apply to divorced parents or single parents. However,
according to previous research on co-parenting (Lengua, Wolchick, & Braver, 1995), research
suggests that maintaining a stable relationship with both parents, even if they are separated or
divorced, is very important for their children to keep a healthy adjustment. Hence, the long-term
outlooks on well-being and parenting effectiveness of divorced single parents does not
necessarily have to be as bleak as many make it out to be.
Managing both mental and physical health problems leads to the need to negotiate
multiple health care systems, particularly among youths in the often complex community health
care system. It is important that youths with co-occurring problems understand the separate
systems and linkages between them. However, systems can also enact policies, structures, and
processes to support service access. For example, a study by Hurlburt et al. (2004) suggests that

58
linkages between child welfare and mental health agencies lead to stronger associations between
mental health needs and mental health service use. A similar theoretical approach could be
applied to the investigation of the impact of linkages between medical and mental health systems
on adolescents with comorbid physical and mental health problems seen in community mental
health settings.
Limitations and Future Works for the Current Study
The continuity of change
The traditional regression method for analyzing change in psychiatric research typically
includes regressing the final measurement of symptoms on predictors after controlling for the
initial level of symptoms. This is known as ‘residualized scores’ or autoregression (or cross-
lagged models in the SEM framework) because covariates are used to predict residualized scores
of the final measurement after removing the effect of the initial measurement. This method
entails several limitations. First, the non-dynamic nature of these models views psychopathology
as a status rather than a process that unfolds over time (Coyn & Downy, 1991). Second, when
individual change follows a non-linear trajectory, regression methods are unlikely to reveal
intricacies of such change (Willet & Sayer, 1994). Moreover, “Ignoring the continuous nature of
change process, traditional methods prevent empirical researchers from engaging a richer,
broader spectrum of research questions, questions that deal with the nature of individual
development” (Willet, 1988, p. 347). In the context of changing continuity, the current study
showed univariate growth curve modeling for each health problem to show how each changed
over time to preserve the continuity of change for adolescents’ health problems, such as anxiety,
depressive symptoms, and physical complaints. The latent growth curve modeling approach is
needed to show individual change over time. However, the current study failed to demonstrate

59
how each of these changes is mutually related. Additionally, to identify homogeneous
subpopulations within the larger heterogeneous population and for the identification of
meaningful groups or classes of individuals, the use of latent class growth analysis (LCGA) and
general mixture modeling (GMM) approaches have recently grown in popularity in family
research, but were not covered in the current study. Thus, future research should investigate
‘interlocking’ trajectories within the context of the ‘latent growth class modeling approach’ for
adolescents’ health problems.
The gender moderating of parents
In the current study, the hypothesized mediating effects of marital conflicts on
adolescents’ health problems were not observed. However, there may be gender differences for
parents in terms of the amount of distress caused by financial events. This explanation is
consistent with a previous study demonstrating that husbands and wives respond differently to
undesirable life events (Conger et al., 1993). The results of the present study also showed an
insight of gender difference on the associations among financial strains, marital conflicts, and
adolescents’ health problems. For example, chronic family economic hardships were stronger
associated with marital conflicts for females. Moreover, females are more vulnerable to
depressive symptoms in response to financial stress. Based on the findings of the present study,
marital conflicts of fathers and mothers may differently influence the association between
chronic family economic hardship stress and adolescents’ health problems. However, marital
conflicts indicators were combined to form a latent factor in this study. Thus, it is not possible to
tease apart the differential outcomes using the current models. However, future studies could
certainly explore these differential outcomes in greater detail.
The sample size of current study

60
Another limitation is the sample size in the current study. The current study used Wave 1,
Wave 2, Wave 3, and Wave 4 of the IYFP study. The sample size for the four waves ranged from
404 to 451. Missing data were not a problem for the current study and the sample size was
adequate for the hypothesized associations. However, the sample was derived from a rural area
consisting of 100% Caucasian parents and adolescents. Information on adolescents living in an
urban setting was not assessed. Future research should incorporate a more diverse sample
population from various ethnic backgrounds to improve the generalizations made in the current
study. Future research should also assess adolescents living in a rural setting and an urban setting
to improve the findings and generalizations made in the current study.

61
Table 1. Descriptive Statistics of Study Samples (N=404 - 451)
Variables M SD Range(Max-Min) Skewness Alpha
Anxiety(91) 1.40 .46 1.00 – 3.90 1.93 .83
Anxiety(92) 1.37 .51 1.00 – 5.00 2.64 .85
Anxiety(94) 1.39 .52 1.00 – 4.43 1.98 .90
Depression(91) 1.51 .55 1.00 – 4.27 1.82 .89
Depression(92) 1.57 .60 1.00 – 5.00 1.83 .91
Depression(94) 1,62 .63 1.00 – 4.55 1.43 .92
Physical Complaints(91) 1.92 .39 1.00 – 3.17 .27 .76
Physical Complaints(92) 2.03 .42 1.00 – 3.25 .25 .74
Physical Complaints(94) 2.01 .41 1.00 – 3.33 .12 .77
Perceived FEH(89) 2.11 .63 1.00 – 4.67 .34 .67
Perceived FEH(90) 2.08 .59 1.00 – 3.75 .12 .70
Perceived FEH(91) 2.20 .66 1.00 – 4.50 .35 .67
Father’s Marital Conflicts(91) 1.13 .44 0.00 – 2.56 .03 .87
Mother’s Marital Conflicts(91) 1.10 .44 0.00 – 2.94 .43 .84
Father’s Supportiveness(91) 3.79 .43 2.00 – 5.00 -.24 .79
Mother’s Supportiveness(91) 4.02 .42 2.67 – 5.00 -.21 .80
Father’s Depression(91) 1.32 .45 1.00 – 4.77 3.14 .92
Mother’s Depression(91) 1.50 .57 1.00 – 4.38 2.30 .92
Father’s education(years) 13.54 2.14 8.00 – 20.00 .83
Mother’s education(years) 13.35 1.66 9.00 – 18.00 .74
Note. FEH= Family Economic Hardship; Max= Maximum; Min = Minimum.

62
Table 2. Mean Differences between Male and Female of the Health Problems
Variables (year) Male Mean
Female Mean t-value Male’s mean
change over time Female’s mean
change over time
Anxiety (1991) 1.33(.40) 1.45(.50) 2.60**
2.50+ .08 Anxiety (1992) 1.27(.41) 1.45(.57) 3.64***
Anxiety (1994) 1.29(.44) 1.45(.54) 3.17**
Total mean of Anxiety 1.30(.34) 1.45(.43) 4.06***
Depression (1991) 1.36(.39) 1.63(.53) 4.95***
4.53* 2.04 Depression (1992) 1.39(.46) 1.72(.67) 5.84***
Depression (1994) 1.46(.55) 1.73(.64) 4.45***
Total mean of Depression 1.40(.38) 1.69(.51) 6.56***
Physical complaints (1991) 1.90(.38) 1.95(.40) 1.30
.76 16.48*** Physical complaints (1992) 1.96(.41) 2.09(.43) 3.05**
Physical complaints (1994) 1.94(.41) 2.07(.41) 3.18***
Total mean of Physical Complaints 1.93(.33) 2.03(.35) 3.25***
Note. n = 189 (Males), and 218 (Females). Standard Deviations are in the parentheses +p<.10; **p<.01; ***p<.001

63
Table 3. Correlations among Study Variables
Note. *p < .05, **p < .01
Measures (Year) 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
1 Anxiety(91) ____
2 Anxiety(92) .60** ____
3 Anxiety(94) .40** .48** ____
4 Depression(91) .75** .48** .38** ____
5 Depression(92) .49** .77** .40** .60** ____
6 Depression(94) .31** .39** .72** .38** .43** ____
7 Physical complaints(91) .37** .30** .26** .36** .33** .18** ____
8 Physical complaints(92) .30** .42** .31** .29** .44** .27** .59** ____
9 Physical complaints(94) .23** .32** .39** .21** .30** .36** .45** .55** ____
10 Father’s marital conflicts(91) .11* .14** .09 .12* .10 .01 .11* .09 .05 ____
11 Mother’s marital conflicts(91) .09 .11* .10 .14** .09 .06 .07 .14** .15** .38** ____
12 Father’s supportiveness(91) -.19** -.09 -.13* -.18** -.03 -.02 .02 -.02 -.02 -.22** -.14** ____
13 Mother’s supportiveness(91) -.19** -.14** -.07 -.21** -.12* -.08 -.09 -.08 -.13* -.11* -.21** .31** ____
14 Family Economic Hardship(89) .17** .11** .16** .18** .13** .10* .12* .11* .17** .20** .27** -.14** -.12* ____
15 Family Economic Hardship(90) .13** .21** .19** .16** .17** .13* .20** .23** .23** .14** .19** -.16** -.12* .51** ____
16 Family Economic Hardship(91) .18** .14** .22** .29** .13* .14** .27** .22** .23** .10* .17** -.14* -.17** .41** .47** ____

64
Table 4. Moderating Effects of Supportive Parenting
Note. L= the low group (n = 62); H= the high group (n = 69). Unstandardized coefficient in parentheses. *p<.05; **p<.01
Grouping Predictors Outcomes Standardized Coefficient
Standard Error Intercept χ2
difference
Supportive Parenting –L
Family Economic Hardship
Anxiety .20 (.37) .29 1.63
.01
Supportive Parenting – H
Family Economic Hardship
Anxiety .42** (.35) .12 1.28
Supportive Parenting –L
Family Economic Hardship
Depression .26* (.47) .28 1.73
.03
Supportive Parenting – H
Family Economic Hardship
Depression .45** (.52) .17 1.36
Supportive Parenting –L
Family Economic Hardship
Physical Complaints .08 (.09) .17 1.96
.18
Supportive Parenting – H
Family Economic Hardship
Physical Complaints .20 (.18) .13 1.83
Supportive Parenting –L
Marital Conflicts Anxiety .07 (.10) .19 1.63
.26 Supportive
Parenting – H Marital
Conflicts Anxiety -.01 (-.01) .09 1.28
Supportive Parenting –L
Marital Conflicts Depression .25* (.42) .22 1.19
4.13* Supportive
Parenting – H Marital
Conflicts Depression -.10 (-.12) .15 1.47
Supportive Parenting –L
Marital Conflicts
Physical Complaints .15 (.13) .12 1.96
1.58 Supportive
Parenting – H Marital
Conflicts Physical
Complaints -.08 (-.07) .10 1.83

65
Table 5.Gender Difference of Health Problems
Note. Group: Male (n= 189), Female (n = 218). Unstandardized coefficient in parentheses *p<.05; ***p<.001
Domain Predictors (year)
Outcomes (year) Grouping Standardized
Coefficient Intercept χ2 difference
Intra-domain
Continuity (Homotypic Continuity)
Depression (1992)
Depression (1994)
Male .47*** (.57) .55
5.00*
Female .22* (.21) .82

66
Table 6. Gender Difference of the Hypothesized Path Model
Predictors (year) Outcomes (year) Grouping Standardized coefficients
Standard errors
χ2 difference
Chronic Family Economic Hardship
(1989-1991)
Anxiety(1991) Male .09 .10
.42 Female .15 .11
Depression(1991) Male .06 .10
5.10* Female .29 .15
Physical Complaints(1991)
Male .17 .09 2.11
Female .35 .10
Marital conflicts(1991)
Male .08 .03 8.46**
Female .32 .05
Supportive Parenting(1991)
Male -.40 .07 .45
Female -.17 .10
Marital Conflicts (1991)
Anxiety (1991) Male -.02 .26
.03 Female .01 .20
Depression(1991) Male -.02 .18
.01 Female -.03 .24
Physical complaints(1991)
Male .03 .24 .05
Female .08 .15
Supportive parenting(1991)
Male -.25 .21 .01
Female -.26 .17
Supportive parenting (1991)
Anxiety(1991) Male -.32 .30
.38 Female -.25 .19
Depression(1991) Male -.36 .30
.51 Female -.20 .21
Physical complaints(1991)
Male -.07 .25 .75
Female .16 .13 Note. *p<.05;**p<.01

67
Table 7. Univariate Growth Curves Model
Note. t-ratios in parentheses. **p<.01; ***p<.001
Variables Intercept Slope Chi-Square (df) CFI
Mean Variance Mean Variance
Anxiety (1991-1994) 1.39*** (62.96) .15*** (8.64) -.01(-.12) .02*** (3.36) 2.59(1) .99
Depression (1991-1994) 1.52*** (57.14) .23***(9.17) .03*** (3.30) .02***(3.17) .26(1) 1.00
Physical Complaints (1991-1994)
1.95*** (104.27) .10*** (8.81) .03*** (3.44) .01**(3.20) 18.18(1) .94

68
Early Depression (t1)
Early Anxiety (t1)
Moderating variable - Gender, Supportive Parenting Control variable - Parental Depression - Parental Education
Figure 1. Theoretical Model Note. Double arrows depict hypothesized moderating effects
Early Physical Complaints (t1)
Physical Complaints (t2)
Depression (t2)
Anxiety (t2)
Marital Conflict
Chronic Family
Economic Hardship
Supportive Parenting

69
Figure 2. Operationalized Model Note. DEP=Depression; ANX=Anxiety; Double arrows depict moderating effects of supportive parenting
Father Mother Father 1990 1991 Mother
: Intra-domain continuity (Homotypic continuity) : Cross-domain continuity (Heterotypic continuity) : Comorbidity
Cross-lagged Model Moderating variable - Supportive parenting, Gender Control variable - Parental Education - Parental Depression
Supportive Parenting
Marital
Conflicts
Chronic Family
Economic Hardship
ANX (1991)
DEP (1991)
Physical Complaints
(1991)
ANX (1992)
DEP (1992)
Physical Complaints
(1992)
ANX (1994)
DEP (1994)
Physical Complaints
(1994)
1989
The Study Time Line
3 WAVES (1991 – 1994) 1991 1989 - 1991

70
Direct effect: c’ Indirect effect: ab Total effect(c): ab + c’ a (Sa) b (Sb)
c (c’) X
M
Figure 3. Basic Mediational Structure for Sobel Test Note. a, b, and c= unstandardized regression coefficient; c’= unstandardized regression efficient after controlling for M; Sa, and Sb = standard error of a and b
Y

71
.29***(4.73)
.28***(4.84)
.21***(3.53)
.72***
.28***
.33***
Figure 4. Direct Influence of Chronic Family Economic Hardship on Adolescents’ Health Problems Note. Standardized regression coefficients, t-values in the parentheses; CFEH = Chronic Family Economic Hardship; *p<.05; **p<.01; ***p<.001
Anxiety (1991)
Depression
(1991)
Physical
Complaints (1991)
CFEH (89-91)
Control variable - Parental Depression - Parental Education
CFI= .95 RMSEA= .05 TLI= .90

72
.73***
.28***
.33***
.25***(3.70)
.20**(2.96)
.28***(4.05)
.10(1.30)
.04(.53)
.03(.37)
.38***(4.32)
Figure 5. Indirect Influence of Chronic Family Economic Hardship on Adolescents’ Health Problems through Marital Conflict Note. Standardized regression coefficient; t-values in the parentheses; CFEH = Chronic Family Economic Hardship; MC = Marital Conflict;**p<.01; ***p<.001
Anxiety (1991)
Depression
(1991)
Physical
Complaints (1991)
CFEH (89-91)
MC (1991)
CFI= .90 RMSEA= .06 TLI= .90
Control variable - Parental Depression - Parental Education

73
.07(.91)
-.37***(-3.99) -.26**(-2.83)
.11(1.67)
.31***(4.46)
-.28**(-2.95)
.19**(2.81) .73***
.28***
.33***
Figure 6. Indirect Influence of Chronic Family Economic Hardship on Adolescents’ Health Problems through Supportive Parenting. Note. Standardized regression coefficient; t-values in the parentheses; CFEH = Chronic Family Economic Hardship; SP = Supportive Parenting; **p<.01; ***p<.001
Anxiety (1991)
Depression
(1991)
Physical
Complaints (1991)
CFEH (89-91)
SP (1991)
CFI= .93 RMSEA= .05 TLI= .94
Control variable - Parental Depression - Parental Education
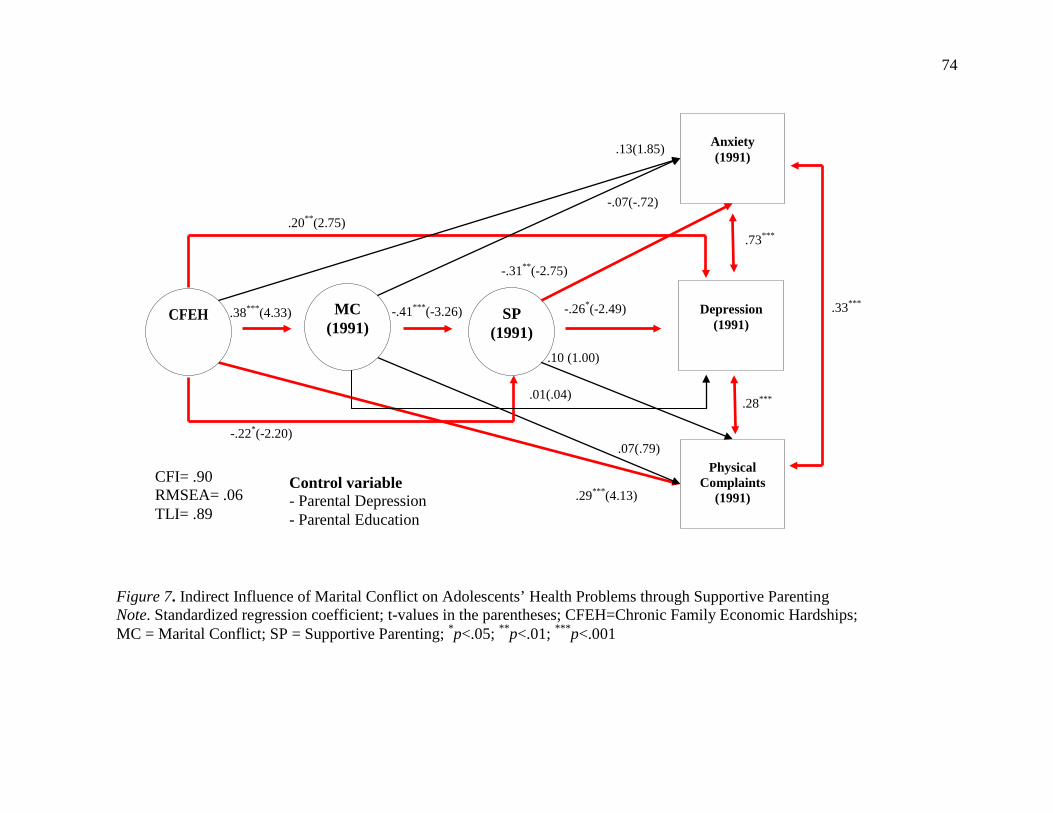
74
-.31**(-2.75)
-.22*(-2.20)
-.26*(-2.49)
.10 (1.00)
.73***
.33***
.28***
.29***(4.13)
.13(1.85)
-.07(-.72)
-.41***(-3.26)
.07(.79)
.38***(4.33)
.20**(2.75)
Figure 7. Indirect Influence of Marital Conflict on Adolescents’ Health Problems through Supportive Parenting Note. Standardized regression coefficient; t-values in the parentheses; CFEH=Chronic Family Economic Hardships; MC = Marital Conflict; SP = Supportive Parenting; *p<.05; **p<.01; ***p<.001
Anxiety (1991)
Depression
(1991)
Physical
Complaints (1991)
CFEH MC (1991)
CFI= .90 RMSEA= .06 TLI= .89
Control variable - Parental Depression - Parental Education
SP (1991)
.01(.04)

75
.38*** -.41***
-.31**
-.28**
.10
-.07
.07
+.13
.20**
.29***
.42*** .39***
.28*** .51***
.54*** .50***
.25***
.69*** .70*** .71***
.32*** .31***
.25*** .36*** .06 .14*
.15* .05
.09
.12*
.14***
.02
.10 .09+
-.02 .10*
.67 .73 .65 .62 .59 .60 .52
χ2(123)=262.28 CFI= .94 RMSEA= .05 TLI= .90
Father Mother 1989 1990 1991
Figure 8. The Operationalized Associations of the Current Study Note. Standardized regression coefficient; DEP=Depression; ANX=Anxiety; +p<.10; *p<.05; **p<.01; ***p<.001
ANX (1991)
DEP
(1991)
Physical
Complaints (1991)
ANX
(1992)
DEP
(1992)
Physical
Complaints (1992)
ANX (1994)
DEP
(1994)
Physical
Complaints (1994)
Father Mother
Chronic Family
Economic Hardship
Marital
Conflicts (1991)
Parental Support (1991)
-.22*
.28***
.01
Control variable - Parental Depression - Parental Education

76
High-level Supportive
parenting group
-.12
.42
Marital Conflicts
Depressive sym
ptoms
1.71
1.35
.97 1.23
Low-level Supportive
parenting group
Figure 9. Supportive Parenting Moderation of Marital Conflict on Adolescents’ Depression Note. Unstandardized coefficient

77
Figure 10. Moderating Effect of Gender Difference on Adolescents’ Health Problems Note. Standardized regression coefficients, Female in the parentheses. All comorbidities are significant at the .001 level
+p<.10; *p<.05; **p<.01; ***p<.001
: Intra-domain continuity (Homotypic Continuity) : Cross-domain influence (Heterotypic Continuity) : Comorbidity
.35*** (.50***) .47*** (.22*)
.54*** (.57***) .41*** (.58***)
.49***(.43***) .50*** (.46***)
Female (n=218) ² (9) = 27.20
CFI = .98 TLI = .90
Male (n=189) ² (9) = 17.13
CFI = .99 TLI = .95
.16*(.09) .11(.17**) .09(.14*)
.11(-.10)
-.01(.12) .18+(-.05)
.05(.02) .07(.10)
.06(.09)
.16+(.04) -.02(.17+)
.01(.08)
.68(.61) .71(.68)
.32(.36) .27(.29) .17(.27)
.30(.27) .75(.75)
.35(.38) .24(.29)
Anxiety (1991)
Anxiety (1992)
Anxiety (1994)
Depression (1991)
Physical complaints
(1991)
Depression (1992)
Physical complaints
(1992)
Depression (1994)
Physical complaints
(1994)
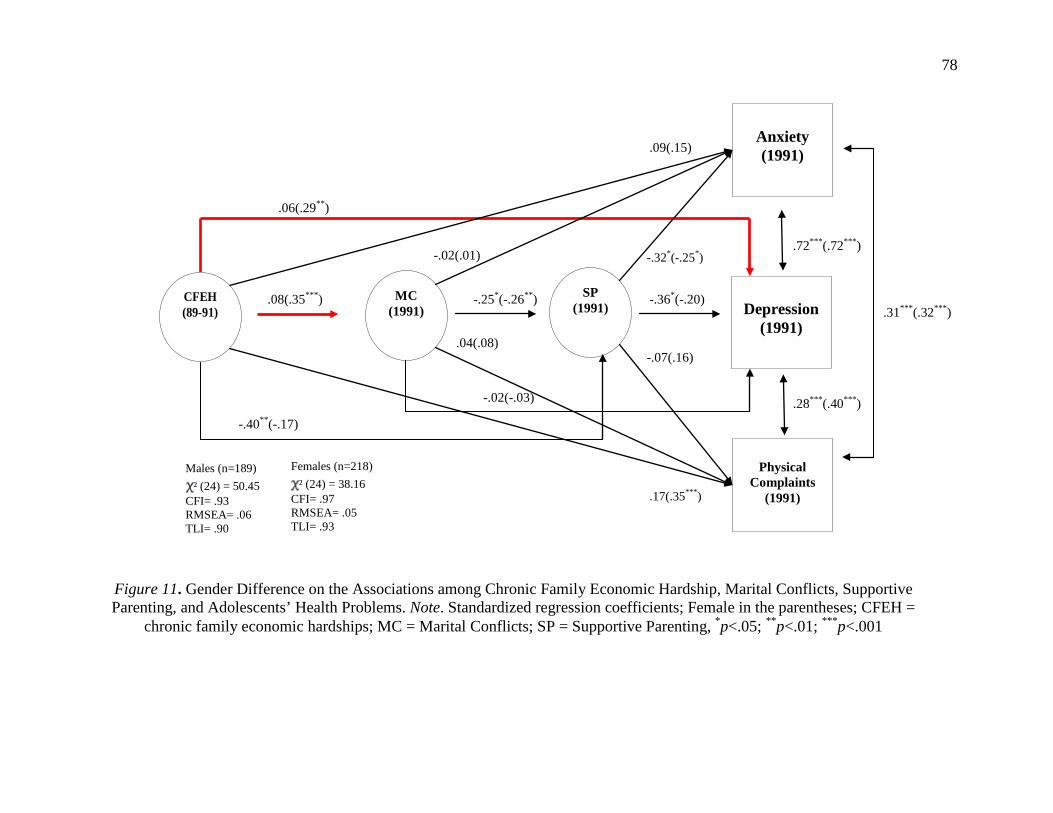
78
.06(.29**)
.09(.15)
.17(.35***)
-.02(.01)
.04(.08)
-.02(-.03)
-.36*(-.20)
-.32*(-.25*)
-.07(.16)
-.25*(-.26**) .08(.35***)
Figure 11. Gender Difference on the Associations among Chronic Family Economic Hardship, Marital Conflicts, Supportive Parenting, and Adolescents’ Health Problems. Note. Standardized regression coefficients; Female in the parentheses; CFEH =
chronic family economic hardships; MC = Marital Conflicts; SP = Supportive Parenting, *p<.05; **p<.01; ***p<.001
Anxiety (1991)
Depression
(1991)
Physical
Complaints (1991)
CFEH (89-91)
MC (1991)
Males (n=189) ² (24) = 50.45
CFI= .93 RMSEA= .06 TLI= .90
SP (1991)
Females (n=218) ² (24) = 38.16
CFI= .97 RMSEA= .05 TLI= .93
-.40**(-.17)
.31***(.32***)
.72***(.72***)
.28***(.40***)

79
Males .18
.37
Chronic family economic hardships
Depressive sym
ptoms 1.63
1.36
2.10 2.16
Females
Figure 12. Gender Difference of Chronic Family Economic Hardship on Depression Note. Unstandardized coefficient.

80
χ2(77)= 155.03 CFI= .97 RMSEA=.04 TLI =.94
-.17+
-.09
.54* .53***
-.21
-.05 .03
.77*** .66**
.53*** .53**
-.12
.38*** -.41***
-.22*
.01
.06
.13
.07
-.07
-.03
.17*
.24
.36***
.20
-.01
Initial Level 1991
Rate of change 1991-1994
Rate of change 1991-1994
Initial Level 1991
Initial Level 1991
Rate of change 1991-1994
Anxiety
Depression
Physical Complaints
Chronic Family
Economic Hardship
89-91
Marital Conflicts
1991
Parental supports
1991
Figure 13. Hypothesized Interlocking Model. Note. Standardized coefficients; +p<.10; *p<.05; **p<.01; ***p<.001
-.01
-.33*
-.24*
-.11
.31
.28
-.12
.24**
-.52+
.08
-.16

81
REFERENCES
Ajdacic-Gross , V., Horvath , S., Canjuga, M., Gamma, A., Angst, J., Rossler,, W., and Eich , D.
(2006). How ubiquitous are physical and psychological complaints in young and
middle adulthood? A longitudinal perspective. Social Psychiatry and Psychiatric
Epidemiology, 41, 881-888.
Amlund-Hagen, K., Myers, B. J., & Mackintosh, V. H. (2005). Hope, social support, and
behavioral problems in at-risk children. American Journal of Orthopsychiatry, 75 (2),
211-219.
Anderson, S. E., Cohen, P., Naumova, E. N., & Must, A. (2006). Association of depression and
anxiety disorders with weight change in a prospective community-based study of
children followed up into adulthood. Archives of Pediatrics and Adolescent Medicine,
160, 285–291.
Angold, A., Costello, E. J., Farmer, E. M. Z., Burns, B. J., & Erkanli, A. (1999). Child Behavior
Checklist-'selected items'. Journal of the American Academy of Child and Adolescent
Psychiatry, 38, 29-137.
Atkinson, T., Liem, R., & Liem, J. H. (1986). The social costs of unemployment: Implications
for social support. Journal of Health and Social Behavior, 27, 317-331.
Barnett, D., Manly, J., & Cicchetti, D. (1993). Defining child maltreatment: The interface
between policy and research. In D. Cicchetti & S. Toth (Eds.), Child abuse, child
development, and social policy (pp. 7-73). Norwood, NJ: Ablex.

82
Baron, R. M., and Kenny, D. A. (1986). The moderator mediator variable distinction in social
psychological research – Conceptual, strategic, and statistical considerations. Journal
of Personality and Social Psychology, 51, 1173-1182.
Barnow, S., Lucht, M., & Freyberger, H. J. (2005). Correlates of aggressive and delinquent
conduct problems in adolescence. Aggressive Behavior, 31, 24-39.
Baviskar S. (2010). Does child gender moderate the relationship between interparental conflict
and child outcomes? Findings from the Danish Longitudinal Study of Children. Norsk
Epidemiologi, 20(1), 63-75.
Beck, A. T., & Steer, R. A. (1987). Beck Depression Inventory manual. San Antonio, TX: The
Psychological Corporation.
Becker, S. (1993). The determinants of adolescent fertility with special reference to biological
variables Biomedical and demographic determinants of reproduction. Gray R, Lendon
H, Spira A (Eds). Oxford, England Clarendon Press.
Bentler, P. M., & Bonett, D. G. (1980). Significance tests and goodness of fit in the analysis of
covariance structures. Psychological Bulletin, 88, 588-606.
Bird, C. E., & Rieker, P. P. (2008). Gender and health: The effect of constrained choices and
social policies. New York: Cambridge University Press.
Boekaerts, M., & Roeder, I. (1999). Stress, coping, and adjustment in children with a chronic
disease: A review of the literature. Disability and Rehabilitation, 21, 311-337.
Boivin, M., Hymel, S., & Hodges, E. V. E. (2001). Toward a process view of peer rejection and
harassment. J. Juvonen & S. Graham, (Eds.), School-based peer harassment: The
plight of the vulnerable and victimized(pp. 265–289), Guilford Press, New York (2001).

83
Bolger, K. E., Patterson, C. J., & Kupersmidt, J. B. (1995). Psychological adjustment among
children experiencing persistent and intermittent family economic hardship. Child
Development, 66, 1107-1129.
Bradley, R. H., & Corwyn, R. F. (2002). Socioeconomic status and child development. Annual
Review of Psychology, 53, 371-399.
Bray, J. H., & Hetherington, E. M. (1993). Families in transition: Introduction and overview.
Journal of Family Psychology, 7, 3-8.
Brody, G. H., Stoneman, Z., Flor, D., McCrary, C., Hastings, L., & Conyers, O. (1994).
Financial resources, parent psychological functioning, parent co-caregiving, and early
adolescent competence in rural two-parent African-American families, Child
Development, 65, 590-605.
Browne, M.W., & Cudeck, R. (1993). Alternate ways of assessing model fit. In K. A. Bollen &
J.S. Long (Eds.), Testing structural equation models (pp. 136-162). Newbury Park.
CA: Sage.
Brookmeyer, K.A., Henrich, C.C., & Schwab-Stone, M. (2005). Adolescents who witness
community violence: Can parent support and prosocial cognitions protect them from
committing violence? Child Development, 76(4), 917-929.
Buehler, C., Krishnakumar, A., Stone, G., Anthony, C., Pemberton, S.,&Gerard, J., et al. (1998).
Interparental conflict styles and youth problem behaviors: A two sample replication
study. Journal of Marriage and the Family, 60, 119–132.
Buehler, C., & Gerard, J. M. (2002). Marital conflict, ineffective parenting, and children’s and
adolescent’s maladjustment. Journal of Marriage and Family, 64, 78-92.

84
Bugental, D. B. (2004), Thriving in the Face of Early Adversity. Journal of Social Issues, 60,
219–235.
Buri, J. R., Cooper, A. M., Ricktsmeier, L. M., & Komer, K. K. (1991, May). Toxic Familial
Effects of parental hostility. Paper session presented at the Annual Meeting of the
Midwestern Psychological Association, Chicago, IL.
Campbell, J., & Lewandowski, L. A. (1997). Mental and physical health effects of intimate
partner violence on women and children. Psychiatric Clinics of North America, 20,
353-374.
Carmines, E. G., & McIver, J. P. (1981). Analyzing models with unobserved variables: analysis
of covariance structures. In G.W. Bohmstedt & E.F. Borgatta (eds.), Social
measurement (pp. 65-115). Beverly Hills, CA: Sage Publications.
Cohen, S., & Herbert, T. B. (1996). Health Psychology: Psychological Factors and Physical
Disease from the Perspective of Human Psychoneuroimmunology. Annual Review of
Psychology, 47, 113-142.
Cole, D. A., & Carpentieri, S. (1993). Antisocial Behavior Instrument. Psychological Assessment,
5, 449-459.
Cole, D. A., & McPherson, A. E (1993). Relation of family subsystems to adolescent depression:
Implementing a new family assessment strategy. Journal of Family Psychology, 7,
119-133.
Conger, R. D. (1988). Developed for the Iowa Youth and Families Project.
Conger R.D., & Conger K.J. (2002). Resilience in Midwestern families: selected findings from
the first decade of a prospective, longitudinal study. Journal of Marriage and Family,
64, 361-373.

85
Conger, R. D., & Elder, G. H., Jr. (1994). Families in troubled times: The Iowa Youth &
Families Project. In R. D. Conger & G. H. Elder, Jr. (Eds.), Families in troubled times:
Adapting to change in rural America (pp. 3-20). Hillsdale, NJ: Aldine.
Conger, R. D., Lorenz, F. O., Elder, G. H., Jr., Melby, J. N., Simons, R. L., & Conger, K. J.
(1991). A process model of family economic pressure and early adolescent alcohol use.
Journal of Early Adolescence, 11, 430-449
Conger, R. D., Conger, K. J., Elder, G. H., Jr., Lorenz, F. O., Simons, R. L., & Whitbeck, L. B.
(1992). A family process model of economic hardship and adjustment of early
adolescent boys. Child Development, 63, 526-541.
Conger, R. D., Conger, K. J., Elder, G. H., Jr., Lorenz, F. O., Simons, R. L., & Whitbeck, L. B.
(1993). Family economic stress and adjustment of early adolescent girls.
Developmental Psychology, 29, 206-219.
Conger, R. D., Conger, K. J., & Elder, G. H., Jr. (1997). Family economic hardship and
adolescent adjustment: Mediating and moderating processes. In J. Brooks-Gunn & G.
Duncan (Eds.), Consequences of growing up poor (pp. 288-310). New York: Russell
Sage Foundation
Conger, R. D., & Donnellan, M. B. (2007). An interactionist perspective on the socioeconomic
context of human development. Annual Review of Psychology, 58, 175-199.
Conger, R. D. & Ge, X. (1999). Conflict and cohesion in parent–adolescent relations: Changes in
emotional expression from early to mid-adolescence. In M. Cox & J. Brooks- Gunn
(Eds.), Conflict and cohesion in families: Causes and consequences (pp. 185–206).
Mahwah, NJ: Erlbaum.

86
Conger, R. D., Ge, X., Elder, G. H., Jr., Lorenz, F. O., & Simons, R. L. (1994). Economic stress,
coercive family process and developmental problems of adolescents. Child
Development, 65, 541-561.
Conger, R. D., Elder, G. H., Jr., Lorenz, F. O., Conger, K. J., Simons, R. L., Whitbeck, L. B., et
al. (1990). Linking economic hardship to marital quality and instability. Journal of
Marriage and the Family, 52, 643-656
Conger, R. D., Rueter, M. A., & Elder, G. H., Jr (2002). Economic pressures in rural families:
Couple interactions that reduce risk for emotional distress and marital instability. In A.
Maney & J. Ramos (Eds.), Socioeconomic conditions, stress and mental disorders:
Toward a new synthesis of research and public policy. National Institute of Mental
Health.
Costello, E. J., Edelbrock, C. S., & Costello, A. J. (2005). National Institute of Mental Health
Diagnostic Interview for Children-Child Version. Journal of Consulting and Clinical
Psychology, 73, 389-399.
Costello, E. J., Mustillo, S., Erkanli, A., Keeler, G., & Angold, A. (2003). Prevalence and
development of psychiatric disorders in childhood and adolescence. Archives of
General Psychiatry, 60, 837–844.
Culpepper, L. (2009). Generalized anxiety disorder and medical illness. Journal of Clinical
Psychiatry, 70, 20-24.
Crockenberg, S., & Forgays, D.K. (1996). The role of emotion in children’s understanding and
emotional reactions to marital conflict. Merrill-Palmer Quarterly, 42, 22-48.
Crockenberg, S. & Langrock, A. (2001). Marital conflict and child adjustment: A test of the
specific emotions model. Journal of Family Psychology, 15,163-182.

87
Cummings, E. M., & Davies, P. T. (1994). Children and marital conflict: The impact of family
dispute and resolution. New York: Guilford Press.
Davies, P. T., & Cummings, E. M. (1994). Marital conflict and child adjustment: An emotional
security hypothesis. Psychological Bulletin, 116, 387-411.
Derogatis, L. R., & Melisaratos, N. (1983). The Brief Symptoms Inventory: An introductory
report. Psychological Medicine, 13, 596-605.
Donohue, B., Romero, V., & Hill, H. (2006). Treatment of co-occurring child maltreatment and
substance abuse. Aggression and Violent Behavior, 11, 626-640
Dowd, J. B , and Goldman N. (2006). Do Biomarkers of Stress Mediate the Relationship
Between Socioeconomic Status and Health? Journal of Epidemiology and Community
Health, 60, 633-639.
Egger, H. L., Costello, E. J., Erkanli, A., & Angold, A. (1999). Somatic complaints and
psychopathology in children and adolescents; stomach aches, musculoskeletal pains
and headaches. Journal of the American Academy of Child and Adolescent Psychiatry,
38, 852-860.
Eiser, C. (1990). Chronic childhood disease: An introduction to psychological theory and
Research. Cambridge, Cambridge University Press.
Eiser, C., & Havermans, T. (1992), Children's understanding of cancer. Psycho-Oncology, 1,
169–181.
Elder, G. H. & Caspi, A. (1988). Economic stress in lives: Developmental Perspectives. Journal
of Social Issues, 44, 25-45.

88
Elliott, T., & Mullins, L. L. (2004). Counseling families and children with disabilities. In D.
Atkinson & G. Hackett (Eds.), Counseling Diverse Populations, 3rd (pp. 151 – 170).
New York: McGraw-Hill.
El-Sheikh, M., Harger, J., & Whitson, S.M. (2001). Exposure to interparental conflict and
children’s adjustment and physical health: The moderating role of vagal tone. Child
Development, 72(6), 1617–1636.
Emery, R. E. (1982). Interparental conflict and the children of discord and divorce.
Psychological Bulletin, 92, 310 – 330.
Emery, R. E., & O'Leary, K. D. (1984). Marital discord and child behavior problems in a non-
clinic sample. Journal of Abnormal Child Psychology, 12, 411-420.
Fauber, R., Forehand, R., Thomas, A.M., & Wierson, M. (1990). A mediational model of the
impact of marital conflict on adolescents adjustment in intact and divorced families.
The role of disrupted parenting. Child Development, 61, 1112-1123.
Frosch, C. A.,&Mangelsdorf, S. C. (2001). Marital behavior, parenting behavior, and multiple
reports of preschoolers’ behavior problems: Mediation or moderation? Developmental
Psychology, 37(4), 502–519.
Furnham, A., & Kirtcaldy, B. D. (1997). Age and Sex differences in health beliefs and behavior.
Psychological Reports, 80, 63-66.
Gable, S., Belsky, J., & Crnic, K. (1992). Marriage, parenting, and child development: Progress
and prospects. Journal of Family Psychology, 5, 276-294.
Garber, J., Keiley M.K., & Martin, N.C. (2002) Developmental trajectories of adolescents’
depressive symptoms: Predictors of change. Journal of Consulting and Clinical
Psychology, 70, 79–95

89
Ge, X., Conger, R. D., & Elder, G. H., Jr. (2001). Pubertal transition, stressful life events, and the
emergence of gender differences in adolescent depressive symptoms. Developmental
Psychology, 37, 404-417
Ge, X., Conger, R. D., Lorenz, F. O., & Simons, R. L. (1994). Parents' stressful life events and
adolescent depressed mood. Journal of Health and Social Behavior, 35, 28-44.
Goodman, S. H., & Gotlib, I. H. (2002). Introduction. In S. H. Goodman & I. H. Gotlib (Eds.),
Children of depressed parents: Mechanisms of risk and implications for treatment (pp.
3 – 9).Washington, DC: American Psychological Association.
Goodwin, M. S., & Groden, J., Baron, G., Groden, G., Velicer, W. F., Lipsitt, L. P., Hofmann, S.,
& Hoppner, B. B. (2004, May). Cardiovascular responses to stress in individuals with
autism. Poster session presented at the annual meeting of the American Psychological
Society, Chicago, IL.
Gottman, J. M. (1990). How marriages change. In G. R. Patterson (Ed.), Depression and
aggression in family interactions (pp. 75-101). Hillsdale, NJ: Erlbaum.
Gottman, J. M., & Notarius, C. I. (2000). Decade review: Observing marital interaction. Journal
of Marriage and the Family, 62, 927–947.
Gordis, L, Berry, D.A,. Chu, S.Y., Fajardo, L.L., Hoel, D.G., and Laufman, L.R.(1997) National
Institutes of Health Consensus Development Conference Statement: breast cancer
screening for women ages 40–49. Journal of National Cancer Institute, 89, 1015–1026.
Gordis, E. B., Margolin, G., & John, R. S. (1997). Marital aggression, observed parental hostility,
and child behavior during triadic family interaction. Journal of Family Psychology, 11,
76-89.

90
Grych, J. H., & Fincham, F. D. (1990). Marital conflict and children’s adjustment: A cognitive-
contextual framework. Psychological Bulletin, 108, 267-290.
Gutman, L. M., & Sameroff, A.J. (2004). Continuities in depression from adolescence to young
adulthood: Contrasting ecological influences. Development and Psychopathology, 16,
967-984.
Halpern-Felsher, B. L., Connell, J. P., Spencer, M. B., Aber, J. L., Duncan, G. J., Clifford, E.,
Crichlow, W. E., Usinger, P. A., Cole, S. P., Allen, L., & Seidman, E. (1997).
Neighborhood and family factors predicting educational risk and attainment in African
American and White children and adolescents. In J. Brooks-Gunn, G. J. Duncan, & J.
L. Aber (Eds.), Neighborhood poverty: Context and consequences for children (Vol. 1,
pp. 146-173). New York: Russell Sage Foundation.
Hamlett, K. W., Pellegrini, D. S., & Katz, K. S. (1992). Childhood chronic illness as a family
stressor. Journal of Pediatric Psychology, 17, 33-47.
Hanson, T. L., McLanahan, S., & Thomson, E. (1997). Economic resources, parental practices,
and children’s wellbeing. In G.J. Duncan & J. Brooks-Gunn (Eds.), Consequences of
growing up poor (pp. 190-238). New York: Russell Sage Foundation.
Harold, G. T., & Conger, R. D. (1997). Marital conflict and adolescent distress: The role of
adolescent awareness. Child Development, 68, 333 – 350.
Herbert, T. B., & Cohen, S. (1993). Depression and immunity: A metaanalytic review.
Psychological Bulletin, 113, 472–486.
Hu, L., & Bentler, P.M. (1999). Cutoff criteria for fit indexes in covariance structural analysis:
Conventional criteria versus new alternatives. Structural Equation Modeling, 6, 1-15.

91
Hurlburt, M. S., Leslie, L. K., Landsverk, J., Barth, R. P., Burns, B. J., Gibbons, R. D., et al.
(2004). Contextual predictors of mental health service use among children open to
child welfare. Archives of General Psychiatry, 61(12), 1217-1224.
Jacques, H. A. K., & Mash, E. J (2004). A Test of the Tripartite Model of Anxiety and
Depression in Elementary and High School Boys and Girls. Journal of Abnormal Child
Psychology, 32, 13–25.
Jaser, S. S., Langrock, A. M., Keller, G., Merchant, M. J., Benson, M. A., Reeslund, K.,
Champion, J. E., & Compas, B. E. (2005). Coping with the stress of parental
depression II: Adolescent and parent reports of coping and adjustment. Journal of
Child and Adolescent Psychology, 34, 193 – 205.
Jenkins, J. M. (2000). Marital conflict and children’s emotions: The development of an anger
organization. Journal of Marriage and the Family, 62, 723–736.
Juvonen, K., Nishina, A., & Graham, S (2000). Peer harassment, psychosocial adjustment, and
school functioning in early adolescence. Journal of Educational Psychology 92, 349–
359.
Kaczynski, K. J., Lindahl, K. M., Malik, N. M., & Laurenceau, J-P. (2006). Marital conflict,
maternal and paternal parenting, and child adjustment: A test of mediation. Journal of
Family Psychology, 20, 199-208.
Kahn, J. R., & Fazio, E. M.(2005). Economic Status over the Life Course and Racial Disparities
in Health. Journal of Gerontology, Series B: Psychological Sciences & Social Sciences,
1, 76-84.

92
Karney, B. R., & Bradbury, T. N. (1995). Assessing longitudinal change in marriage: An
introduction to the analysis of growth curves. Journal of Marriage and Family 57(4),
1091-1108.
Katon, W., Elizabeth, H. B. Lin, M. D., & Kroenke, K. (2007). The association of depression and
anxiety with medical symptom burden in patients with chronic medical illness.
General Hospital Psychiatry, 29, 147– 155.
Katon, W., & Sullivan, M. D. (1990). Depression and chronic mental illness. Journal of Clinical
Psychiatry, 51, 3-14.
Katz, L.F., & Gottman, J.M. (1997). Buffering children from marital conflict and dissolution.
Journal of Clinical Child Psychology, 26, 157-171.
Kessler, R.C., Berglund, P., Demler, O., Jin, R., Merikangas, K.R. & Walters, E.E. (2005).
Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the
National Comorbidity Survey, Archives of General Psychiatry, 62, 593-602.
Kessler, R. C., & Walter, E. E. (1998). Epidemiology of DSM-III-R major depression and minor
depression among adolescents and young adults in the national comorbidity survey.
Depression and Anxiety, 7, 3-14.
Kitzmann, K.M. (2000). Effects of marital conflict on subsequent triadic family interactions and
parenting. Developmental Psychology, 36, 3-13.
Larson, J. F. (1984). The effect of husband’s unemployment on marital and family relations in
blue color families. Family relations, 33, 503-512.
Lavigne, J. V., & Faier-Routman, J. (1993). Correlates of psychological adjustment to pediatric
physical disorders: A meta-analytic review and comparison of existing models.
Journal of Developmental and Behavioral Pediatrics, 14, 117-123.

93
Leinonen, J.A., Solantaus, T.S., & Punamaki R. (2003). Parental mental health and children’s
adjustment: the quality of marital interaction and parenting as mediating factors.
Journal of Child Psychology and Psychiatry, 44(2), 227-241.
Lempers, J. D., Clark-Lempers, D., & Simons, R. L. (1989). Economic hardship, parenting, and
distress in adolescence. Child Development, 60, 25-39.
Lengua, L. J., Wolchick, S. A., & Braver, S. L. (1995). Understanding children’s divorce
adjustment from a ecological perspective. Journal of Divorce and Remarriage, 22, 25–
53.
Lewinsohn, P., Rohde, P., Seeley, J., & Fisher, S. (1993). Age-cohort changes in the lifetime
occurrence of depression and other mental disorders. Journal of Abnormal Psychology,
102, 110-120.
Lewinsohn, P. M., Klein, D. N., & Seeley, J. R. (1995). Bipolar disorder in a community sample
of older adolescents: prevalence, phenomenology, comorbidity, and course. Journal of
the American Academy of Child & Adolescent Psychiatry, 34, 454–463.
Liber, J.M., van Widenfelt, B.M, Goedhard, A.W., Utens, E.M.W.J, Adelinde, J.M., van der
Leeden, Markus, L.M.., & Treffers, P.D.A. (2008). Parenting and Parental Anxiety and
Depression as Predictors of Treatment outcome for childhood anxiety disorders: Has
the role of fathers been underestimated? Journal of Clinical Child & Adolescents
Psychology, 37(4), 747-758.
Lonigan, C. J., Phillips, B. M., & Hooe, E. S. (2003). Tripartite model of anxiety and depression
in children: evidence from a latent variable longitudinal study. Journal of Consulting
and Clinical Psychology, 71, 465–481.

94
Lorenz, F. O., Wickrama, K. A. S., & Conger, R. D. (2004). Modeling continuity and change in
family relations with panel data. In R. D. Conger, F. O. Lorenz & K. A. S. Wickrama
(Eds.), Continuity and change in family relations: Theory, methods, and empirical
findings (pp. 15-62). Mahwah, NJ: Erlbaum.
Luthar, S. S., Cicchetti, D., & Becker, B. (2000). The construct of resilience: A critical
evaluation and guidelines for future work. Child Development, 71, 543-562.
Lynch, J. W., G. A. Kaplan and S. J. Shema (1997). "Cumulative Impact of Sustained Economic
Hardship on Physical, Cognitive, Psychological and Social Functioning." The New
England Journal of Medicine, 337(26), 1889-1895.
MacKinnon, D. P., Warsi, G., & Dwyer, J. H. (1995). A simulation study of mediated effect
measures. Multivariate Behavioral Research, 30(1), 41-62.
Mauldon, J. (1990). The effect of marital disruption on children’s health. Demography, 27(3),
431–446.
Masten, A. S. (2001). Ordinary magic: Resilience processes in development. American
Psychologist, 56, 227-238.
McClelland, G.H., & Judd, C.M. (1993). Statistical difficulties of detecting interactions and
moderator effects. Psychological Bulletin, 114(2), 376-390
McDougall, J., King G., de Wit, D.J., Miller, L., Hong, S.J., Offord, D.R., Laporta, J., & Meyer,
K. (2004). Chronic physical health conditions and disability among Canadian school-
aged children: a national profile. Disability and Rehabilitation, 26(1), 35-45.
McLoyd, V.C. (1990). The Impact of Economic Hardship on Black Families and Children:
Psychological Distress, Parenting, and Socioemotional Development. Child
Development, 61, 311-346.

95
McLoyd, V. C. (1998). Socioeconomic disadvantage and child development. American
Psychologist, 53, 185 – 204.
Mechanic, D., & Hansell, S. (1987). Adolescent competence, psychological well-being, and self-
assessed physical health. Journal of Health and Social Behavior, 28, 364-374.
Melby, J. N., Conger, K. J., & Puspitawati, H. (1999). Insider, participant observer, and outsider
perspectives on adolescent sibling relationships. In F. M. Berardo & C. L. Shehan
(Eds.), Contemporary perspectives on family research: Through the eyes of the child:
Re-visioning children as active agents in family life (Vol. 1, pp. 329-351). Stamford,
Ct: JAI Press.
Melby, J. N., Conger, R. D., Conger, K. J., & Lorenz, F. O. (1993). Effects of parental behavior
on tobacco use by young male adolescents. Journal of Marriage and the Family, 55,
439-454
Melby, J. N., & Conger, R. D. (2001). The Iowa family interaction rating scales: Instrument
summary. In P. Kerig & K. Lindahl (Eds.), Family observational coding systems:
Resources for systematic research. Mahwah, NJ: Erlbaum.
Messer, S. C., Angold, A., Costello, E. J., & Burns, B. J. (2003). Child and Adolescent Burden
Assessment. Journal of the American Academy of Child and Adolescent Psychiatry, 42,
1370-1375.
Miech, R. A., Caspi, A., Moffit, T. E., Wright, B. R. E., & Silva, P. A. (1999). Low
socioeconomic status and mental disorders: A longitudinal study of selection and
causation during young adulthood. American Journal of Sociology, 104, 1096–1131.

96
Miller, G. E., Chen, E., & Zhou, E. S. (2007). If it goes up, must it come down? Chronic stress
and the hypothalamic-pituitary-adrenocortical axis in humans. Psychological Bulletin,
133, 25–45.
Moffitt, T. E. (1993). Adolescence-limited and life-course-persistent antisocial behavior: A
developmental taxonomy. Psychological Review, 100, 674-701.
Moffitt, T. E., Caspi, A., Harrington, H., Milne, B. J., Melchior, M., Goldberg, D., & Poulton, R.
(2007). Generalized anxiety disorder and depression: childhood risk factors in a birth
cohort followed to age 32. Psychological Medicine, 37, 441–452.
Mott, S. R., James, S. R., & Spherac, A. M. (1990). Chronic illness in children and families. In
Mott SR, James SR, Spherac AM (Eds). Nursing Care of Children and Families, 2nd
(pp 613–639). Lippincott Publishing, Inc, Philadelphia.
Mustillo, Sarah, Worthman, Carol, Erkanli, Alaattin, Keeler, Gordon, Angold, Adrian, &
Costello, E. Jane (2003). Obesity and Psychiatric Disorder. Developmental
Trajectories Pediatrics, 111, 851-859.
Muris, P., Schmidt, H., Lambrichs, R., & Meesters, C. (2001). Protective and vulnerability
factors of depression in normal adolescents. Behavior Research and Therapy, 39, 555-
565.
Newacheck, P. W., McManus,M., & Fox, H. (1991). Prevalance chronic illness: Prevalence,
severity, and impact. American Journal of Public Health, 82, 364-371.
Nicolotti, L., El-Sheikh, M., & Whitson, S. M. (2003). Children’s coping with marital conflict
and their adjustment and physical health: Vulnerability and protective functions.
Journal of Family Psychology, 17, 315–326.
97
O'Neil, K. A., Conner, B. T., & Kendall, P. C. (2011). Internalizing disorders and substance use
disorders in youth: Comorbidity, risk, temporal order, and implications for intervention.
Clinical Psychology Review, 31, 104–112.
O’Rand, A. M., & Hamil-Luker, J. (2005). Processes of cumulative adversity linking childhood
disadvantage to increased risk of heart attack. Journal of Gerontology-SS, 60B (Special
Issue II), 117–124.
Pappas, G., Queen, S., Hadden, W., & Fisher, G. (1993). The increasing Disparity in Mortality
Between Socioeconomic Groups in the United States. New England Journal of
Medicine, 329, 103-109.
Peterson, J.L., and Zill, N. (1986). Marital Disruption, Parent-Child Relationships, and Behavior
Problems in Children. Journal of Marriage and the Family 48(2), 295-307.
Patterson, G. R., DeBaryshe, B. D., & Ramsey, E. (1989). A developmental perspective on
antisocial behavior. American Psychologist, 44, 329–335.
Patterson, C. J., Vaden, N. A., Griesler, P. C., & Kupersmidt, J. B. (1991). Income level, gender,
ethnicity, and household composition as predictors of children's peer companionship
outside of school. Journal of Applied Developmental Psychology 12, 447-465.
Pearlin, L. I., Schieman, S., Fazio, E. M., & Meersman, S. C. (2005) Stress, health, and the life
course: Some conceptual perspectives. Journal of Health and Social Behavior, 46,
205–219.
Petersen, A.C., Sarigiani, P.A., & Kennedy, R.E. (1991). Adolescent Depression: Why More
Girls? Journal of Youth and Adolescence, 20, 247–271.
Phillips, K.A., & Diaz, S. F. (1997). Gender differences in body dysmorphic disorder. Journal of
Nervous and Mental Disease, 185, 570-577.

98
Piko, B. (2000). Perceived social support from parents and peers: which is the stronger predictor
of adolescent substance use? Substance Use and Misuse, 35(4), 617–630.
Piotrkowski, Chaya S., R. N. Rapoport, & R. Rapoport. (1987). Families and work. In Marvin B.
Sussman and S. K. Steinmets (Eds.), Handbook of Marriage and the Family (pp. 251-
284). New York: Plenum Press.
Pless, I. B., & Nolan. T. (1991). Revision, replication and neglect—research on maladjustment in
chronic illness Journal of Child Psychology and Psychiatry, 32, 347-365.
Radovanovic, D.M. (1993). Knowing systemic rules: From stages of disorder to second order
towards positive delinquency: A true story. Human Systems, 4, 235-258.
Rapee, R. M., & Heimberg, R. G. (1997). A cognitive-behavioral model of anxiety in social
phobia. Behavior Research and Therapy, 35, 741-756.
Reinherz, H. Z., Giaconia, R. M., Pakiz, B., Silverman, A. B., Frost, A. K., & Lef kowitz, E. S.
(1993). Psychosocial risks for major depression in late adolescence: A longitudinal
community study. Journal of the American Academy of Child and Adolescent
Psychiatry, 32, 1155-1163.
Reinherz, H. Z., Stewart-Berghauer, G., Moeykens, B. A., Pakiz, B., Frost, A. K., & Holmes, W.
M. (1989). The relationship of early risk and current mediators to depressive
symptomatology in adolescence. Journal of 'the American Academy of' Child and
Adolescent Psychiatry, 28, 942-947.
Repetti, R. L., Taylor, S. E., & Seeman, T. E. (2002). Risky families: Family social
environments and the mental and physical health of offspring. Psychological Bulletin,
128, 330-366.

99
Robila, M. & Krishnakumar, A. (2005). The impact of financial strain on marital conflict in
Romania. Journal of Family Psychology, 19(2), 242-251
Rogers, M., & Holmbeck, G.N. (1997). Effects of interparental aggression on children’s
adjustment: The moderating role of cognitive appraisal and coping. Journal of Family
Psychology, 11, 125-130.
Rogers, S. J., & White, L. K. (1998). Satisfaction with parenting: The role of marital happiness,
family structure, and parents’ gender. Journal of Marriage and the Family, 60, 293–
308.
Roy-Byrne, P. P., Davidson, K. W., Kessler, R. C., Asmundson, G. J. G., Goodwin, R. D., &
Kuzansky, L. (2008). Anxiety disorders and comorbid medical illness. General
Hospital Psychiatry, 30, 208-225.
Sanford, M., Szatmari, P., Spinner, M., Munroe-Blum, H., lamieson, E., Walsh, C., & Jones, D.
(1995). Predicting the one-year course of adolescent major depression. Journal of the
American Academy of Child and Adolescent Psychiatry, 34, 1618-1628.
Schwarts, C. E., Snidman, N., & Kagan, J. (1999). Adolescent Social Anxiety as an Outcome of
Inhibited Temperament in Childhood. Journal of the American Academy of Child &
Adolescent Psychiatry, 38, 1008-1015.
Silberg, J.L., Rutter, M., & Eaves, L. (2001). Genetic and environment influences on the
temporal Association between earlier anxiety and later depression in girls. Society for
Biological Psychiatry, 49, 1040-1049.
Simeonsson, R. J., McMillen, J. S., & Huntington, G. S. (2002). Secondary conditions in
children with disabilities: Spina bifida as a case example. Mental Retardation and
Developmental Disabilities Research Review, 8, 198–205.

100
Simon, N. M., & Fischmann, D. (2005). The implications of medical and psychiatric comorbidity
with panic disorder. Journal of Clinical Psychiatry, 66, 8-15.
Simons, R. L., Lorenz, F. O., Conger, R. D., & Wu, C. (1992). Support from spouse as mediator
and moderator of the disruptive influence of economic strain on parenting. Child
Development, 63, 1282-1301.
Simons, R. L., Whitbeck, L. B., Conger, R. D., & Melby, J. N. (1990). Husband and wife
differences in determinants of parenting: A social learning and exchange model of
parental behavior. Journal of Marriage and the Family, 52, 375-392.
Simons, R. L., Whitbeck, L. B., Melby, J. N., & Wu, C. (1994). Economic pressure and harsh
parenting. In R. D. Conger & G. H. Elder, Jr. (Eds.), Families in troubled times:
Adapting to change in rural America (pp. 223-234). Hillsdale, NJ: Aldine.
Silverstein, B., & Lynch A. (1998). Gender differences in depression: the role played by parental
attitudes of male superiority and maternal modeling of gender-related limitations. Sex
Roles, 38, 539-555.
Snyder, J., Bullard, L., Wagener, A., Leong, P.K., Snyder, J., Jenkins, M., & Brown, C. (2009).
Childhood anxiety and depressive symptoms: Trajectories, Relationship, and
association with subsequent depression. Journal of Clinical Child and Adolescent
Psychology, 38, 837-849.
Sobel, M. E. (1982). Asymptotic confidence intervals for indirect effects in structural models. In
S. Leinhardt (Ed.), Sociological methodology, (pp. 290-312). San Francisco: Jossey-
Bass.

101
Stoney, C. M., Niaura, R., Bausserman, L., & Matacin, M. (1999). Lipid reactivity to stress: I.
Comparison of chronic and acute stress responses in middle-aged airline pilots. Health
Psychology, 18, 241–250
Takkouche, B., Regueira, C., & Gestal-Otero, J. J. (2001). A cohort study of stress and the
common cold. Epidemiology, 12, 345-349.
Verbrugge, L. M. (1985). Gender and health: an update on hypotheses and evidence. Journal of
Health and Social Behavior, 26, 156-182.
Vilhialmsson, R. 1994 “Effects of social support on self-assessed health in adolescence.” Journal
of Youth and Adolescence, 23, 437-452.
Vilhjalmsson, R., & Thorlindsson, T. (1998). Factors related to physical activity: a study of
adolescents. Social Science Medicine. 47, 665–675
Wadsworth, M. (1997). Changing social factors and their long-term implications for health,
British Medical Bulletin, 53, 198–209.
Wadsworth, M.E., & Compas, B.E. (2002). Coping with family conflict and economic strain:
The adolescent perspective. Journal of Research on Adolescence, 12(2), 243-274.
Wallander, J. L., & Varni, J. W. (1998). Effects of pediatric chronic physical disorders on child
and family adjustment. Journal of Child Psychology and Psychiatry, 39(1), 29-46.
Wickrama, K.A.S., Beiser, M., & Kaspar, V. (2002). Assessing the longitudinal course of
depression and economic integration of South-East Asian refugees: An application of
latent growth curve analysis. International Journal of Methods in Psychiatric Research,
11, 154-168.

102
Wickrama, K. A. S., Conger, R. D., & Abraham, W. T. (2005). Early adversity and later health:
The intergenerational transmission of adversity through mental disorder and physical
illness. Journal of Gerontology, Series B 60B, Special Issue II, 125-129.
Wickrama, K. A. S., Conger, R. D., Lorenz, F. O., & Elder, G. H., Jr. (1998). Parental education
and adolescent self-reported physical health. Journal of Marriage and the Family, 60,
967-978.
Wickrama, K. A. S., Conger, R. D., Lorenz, F. O., & Jung, T. (2008, a). Family antecedents and
consequences of trajectories of depressive symptoms from adolescence to young
adulthood: A life course investigation. Journal of Health and Social Behavior, 49, 468-
483.
Wickrama, K. A. S., Surjadi, F. F., & Lorenz, F. O. (2008, b). The influence of work control
trajectories on men’s mental and physical health during the middle years: Mediational
role of personal control. Journal of Gerontology, Social Science, 63B, 135-145.
Wickrama, K. A. S., Conger, R. D., Wallace, L. E., & Elder, G. H., Jr. (1999). The
intergenerational transmission of health-risk behaviors: Adolescent lifestyles and
gender moderating effects. Journal of Health and Social Behavior, 40(3), 258-272.
Wickrama, K. A. S., Lorenz, F. O., & Conger, R. D. (1997). Parental support and adolescent
physical health status: A latent growth-curve analysis. Journal of Health and Social
Behavior, 38, 149-163.
Wickrama, K. A. S., Lorenz, F. O., Conger, R. D., & Matthew, L. (1995). Role identity, role
satisfaction, and perceived physical health. Social Psychology Quarterly, 58, 270-283.

103
Willet JB (1988) Questions and answers in the measurement of change. In EZ Rothkpf (ed.)
Review of Research in Education. Vol.15. Washington DC: American Educational
Research Association, pp. 345–422.
Willett, J.B., & Sayer, A.G. (1994). Using covariance structure to detect correlates and predictors
of individual change over time. Psychological Bulletin, 116(2), 363-381.
Wittchen, H. U., Kessler, R. C., Pfister, H., & Lieb, M. (2000). Why do people with anxiety
disorders become depressed? A prospective longitudinal community study. Acta
Psychiatrica Scandinavica, 102, 14-23.






![Council Policy - Financial Hardship Policy for Ratepayers · 2020-06-25 · 1 Council Policy Financial Hardship Policy for Ratepayers D20/27488[v2] 1. Title Financial Hardship Policy](https://img.pdfslide.us/doc/110x75/5f32eb42c78e59222a73ea4e/council-policy-financial-hardship-policy-for-ratepayers-2020-06-25-1-council.jpg)




















