Embed Size (px)
Citation preview

WEDNESDAY, OCTOBER 7, 2020
2:00 PM ET / 1:00 PM CT / NOON MT / 11:00 AM PT
CHRONIC DISEASE MANAGEMENT DURING COVID-19

Bipartisan membership organization
All 50 states and the territories
7,383 state legislators
All state legislative staff (30,000+)
Mission:
To improve the quality and effectiveness of state legislatures
To promote policy innovation and communication among state legislatures
To ensure states a strong, cohesive voice in the federal system
NATIONAL CONFERENCE OF STATE LEGISLATURES

CHRONIC DISEASE MANAGEMENT DURING COVID-19: AGENDA
COVID-19 Impact on Chronic Disease Susan Kansagra, MD, MBA, section chief, Chronic Disease and Injury, Division of Public Health, North
Carolina Department of Health and Human Services
Cardiovascular Disease Management Keith C. Ferdinand, MD, FACC, FAHA, FASPC, FNLA, professor of medicine, Tulane University School of
Medicine
State Legislative Actions and Policy Options Jack Pitsor, research analyst, NCSL
Discussion and Q&A

COVID-19 Impact on Chronic Disease
Susan Kansagra, MD, MBA
Section Chief, Chronic Disease and InjuryNC Division of Public HealthNC Dept of Health and Human Services
Board PresidentNational Association of Chronic Disease Directors

5► https://www.cdc.gov/chronicdisease/pdf/infographics/chronic-disease-H.pdf

6► https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-underlying-medical-conditions.html

7► https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-race-ethnicity.html

8
Prevalence of Chronic Disease Condition that Impact COVID Outcomes (NC)
51% 42%of adults in North Carolina are at higher risk for severe illness from COVID-19 based on being 65 or older, having at least one of the underlying health conditions, or both
of people in North Carolina have one of the health conditions that increases risk for a severe illness from COVID-19
https://files.nc.gov/covid/documents/dashboard/Risk-Factors-for-Severe-Illness-from-COVID-19.pdf

9
Impacts of COVID on Delayed Care for Chronic Diseases
Overall, 41% of US adults have avoided medical care during the pandemic because of concerns about COVID-19; 12% avoided urgent/emergency care and 31.5% avoided routine care.
• 55% of with 2 or more underlying conditions compared avoided care• 42% of people without insurance compared to 25% with insurance avoided care• 55% Hispanic; 48% Black, non-Hispanic; 36% White, non-Hispanic avoided care• 49% believed to be in a group at high risk for COVID-19 compared to 39% who were not• Impact of delays in care:
Heart Disease• Lasting damage to heart muscle from
delayed care for heart attack• Increased risk of heart failure and death
Cancer• Tumor progression• Delays early detection• Lowers rate of cancer survival
Diabetes• Poorer diabetes control• Increase complications like kidney
and eye disease
https://www.cdc.gov/mmwr/volumes/69/wr/mm6936a4.htm

10
Prevention on Chronic Diseases – NC Resources
https://www.diabetesfreenc.com/

11
NC Medicaid Telehealth Provisions Implemented for COVID-19
NC DHHS Medicaid implemented 125 telehealth flexibilities, which spanned 482 codes, during the public health emergency. Some of the provisions implemented were:
• 56 flexibilities for behavioral health, I/DD and TBI
• 15 flexibilities for CDSAs to bill for telehealth across multiple clinical services
• 6 flexibilities for pregnant and post partum services
• 6 flexibilities for DME prior authorizations
• 5 flexibilities for LEAs to bill across multiple therapies
• 4 flexibilities for teledentistry
• 4 flexibilities for outpatient specialized therapies (PT, OT, and Speech Audiology)
• 3 flexibilities for Well Child visits
• 3 flexibilities for optometry
• 2 flexibilities for respiratory therapy
• 2 flexibilities for physiological monitoring
• 2 flexibilities for dialysis services (ESRD and training)
• 2 flexibilities for consultants
There were 15 other general telehealth flexibilities implemented

12
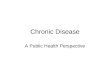
Deaths attributable to individual risk factors (in thousands), by disease
Danaei G, Ding EL, Mozaffarian D, Taylor B, Rehm J, et al. (2009) The Preventable Causes of Death in the United States: Comparative Risk Assessment of Dietary, Lifestyle, and Metabolic Risk Factors. PLOS Medicine 6(4): e1000058. https://journals.plos.org/plosmedicine/article?id=10.1371/journal.pmed.1000058c

13
A Healthier Population Increases Resiliency Against Health Threats
Creating a healthy, resilient population requires upstream policy, systems, and environmental changes
RIDOH Health Equity Framework adopted from Frieden T. A framework for public health action. AJPH. 2010.

14
Other Resources
https://chronicdisease.org/resource/resmgr/website-2020/covid/factsheet_covid19cd.pdf https://mcusercontent.com/f5eb710db3/files/5afc0b37-6559-43e1-8664-ec5ae0e13a6d/FS_CDpolicymakers2020FINALv3.pdf

POLL

Impact of COVID-19 on Cardiovascular Disease
ManagementKeith C. Ferdinand, MD, FACC, FAHA, FASPC, FNLAGerald S. Berenson Endowed Chair in Preventive Cardiology Professor of MedicineTulane University School of Medicine LA COVID-19 Health Equity Task Force Member

COVID-19: Cardiovascular Viewpoint
• Cardiovascular complications of COVID-19• Implications of delayed care on long term health and health care
systems• Disparities in cases and outcomes • Insights from the LA COVID-19 Health Equity Task Force

usaheartfacts.org

Coronavirus means Crown in Latin

Name of this Disease for Coronavirus :COVID-19
COVID-19:• 'CO' stands for 'corona,’• 'VI' for 'virus,’ • 'D' for disease• 2019

Visualizing What
COVID-19 Does to the
Body
https://www.neurodiem.com/

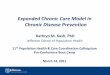
Mechanisms of New or Worsening Heart Failure With COVID-19
JACC HF online, 3 June 2020 https://doi.org/10.1016/j.jchf.2020.05.006

Numerous Variables Making African Americans More Vulnerable to COVID-19
…. “a mixture of the many difficulties faced by African Americans which may compound or even extend the burden for the coronavirus risk factors,” …Ferdinand, KC April 2020
https://www.nationalgeographic.com/history/2020/04/coronavirus-disproportionately-impacts-african-americans/

MMWR Early Release - Vol. 69, August 17, 2020


Numerous Variables Making African Americans More Vulnerable to COVID-19
• Working in service industries or “essential jobs” exposing themselves to infection;
• Using public transportation to get to work; • Lack of access to early testing; and • A historical distrust of the health-care system because of
previous bias.
https://www.nationalgeographic.com/history/2020/04/coronavirus-disproportionately-impacts-african-americans/

“…….sentinel event as an unexpected occurrence resulting in death or serious physical or psychological injury, or the risk thereof. Conventionally identified sentinel events, such as unintended retention of foreign objects and fall-related events, are used to evaluate quality in hospital care…”

Keith C. Ferdinand, Samar A. Nasser J Am Coll Cardiol. 2020 Jun, 75 (21) 2746-2748.

Remote Monitoring for Cardiovascular Risk Reduction: The Impact of COVID-19
https://www.keckmedicine.org/

Telehealth = Improved Healthcare?Flexibilities allow providers to:
• Conduct telehealth with patients in their homes and rural areas
• Deliver care to both established and (new?) patients • Bill for telehealth services (both video and audio-only) as if
provided in person• Educate patients in face-to-face visit• Loan (automated blood pressure cuff)




Thank You!

POLL

JACK PITSOR, RESEARCH ANALYST
TELEHEALTH STATE ACTIONS DURING COVID-19

All 50 states, D.C. and Puerto Rico modified their telehealth policies due to COVID-19.
35 states, D.C. and Puerto Rico enacted over 72 bills since March.
OVERVIEW OF STATE ACTIONS

Private Insurance Twenty states now maintain payment
parity requirements for private insurers (either permanently or temporarily).
Fifteen states and D.C. enacted other private insurance requirements during the pandemic.
ENHANCING PRIVATE INSURANCE AND MEDICAID COVERAGE
Medicaid Ten states enacted legislation extending
Medicaid coverage for telehealth. MD HB 1208—Chronic conditions case
management via telehealth

INCREASING PROVIDER AND PATIENT ACCESS TO TELEHEALTH
Out-of-State Providers & Provider-Patient Relationship
Originating Site Requirements
KY SB 150—Authorizes health practitioners licensed in another state or territory to deliver services via telehealth and waives in-person visit requirements
MN SF 4334—Expands the definition of originating site to include a patient’s home
Broadband Connectivity MS SB 3046—Establishes the COVID-19 Broadband
Provider Grant Program Fund

TEMPORARY VS. PERMANENT CHANGES
Extend beyond the declared emergency: CT HB 6001—Extends COVID-19
telehealth coverage requirements until March 2021
Enact permanent changes: NH HB 1623—Codifies the governor’s
telehealth emergency order into state law

ADDITIONAL RESOURCES—AND THANK YOU!
COVID-19 Resources
State Action on Coronavirus (COVID-19)
COVID-19: State Health Actions
Rural Health Care and COVID-19
The Health Workforce and COVID-19
Other Resources
Health Innovations State Law Database
Jack Pitsor, Research [email protected] | 303.856.1343

DISCUSSION AND Q&A
Please type your questions into the chat box in the lower left-hand corner of your
screen.