Embed Size (px)
Citation preview
4/9/2014 Choroidal Melanoma
http://emedicine.medscape.com/article/1190564-overview#showall 1/17
Choroidal Melanoma
Author: Enrique Garcia-Valenzuela, MD, PhD; Chief Editor: Hampton Roy Sr, MD more...
Updated: Mar 31, 2014
Practice Essentials
Choroidal melanoma is the most common primary malignant intraocular tumor and the second most common typeof primary malignant melanoma in the body. It most often affects whites of northern European descent.
Essential update: Early treatment may prevent metastatic death in patients with choroidal melanoma
In a prospective cohort study of 3072 patients with choroidal melanoma, researchers found that for some patients,
early treatment, rather than watchful waiting, might better prevent metastatic death.[1, 2]
For the study, researchers correlated age at death, cause of death, age at treatment, and survival predictors.Tumors ranged in size from 2.4 to 23.8 mm in basal diameter and from 0.6 to 18.3 mm in thickness, and thelargest basal diameter correlated with all survival predictors except chromosome 6p gain. Older age at treatmentwas correlated with largest basal tumor diameter, tumor thickness, TNM stage, ciliary body involvement,extraocular spread, chromosome 3 loss, and chromosome 8q gain. A total of 1005 patients died by the end of thestudy, and 561 of these patients died from metastatic disease from uveal melanoma. Median age at death waslower (68.6 years) for patients who died from metastatic melanoma than for patients who died from any cause(74.0 years). None of the survival predictors correlated with age at death among the patients who died of
metastasis except for mitotic count, which had a weak correlation.[1, 2]
Signs and symptoms
Choroidal melanomas remain asymptomatic for prolonged periods of time; they may be found incidentally duringophthalmoscopy. In general, the more anterior their origin, the longer the delay of any symptoms. Choroidalmelanoma may present with the following symptoms:
Blurred visual acuityParacentral scotomaPainless and progressive visual field lossFloatersSevere ocular painWeight loss, marked fatigue, cough, or change in bowel or bladder habits (suggests primary nonocularmalignancy with choroidal metastasis)
Ophthalmologic examination may reveal the following:
Small choroidal melanomas typically take the form of a nodular, dome-shaped, and well-circumscribedmass under the retinal pigment epitheliumAs choroidal melanomas grow, they may adopt more irregular configurations (eg, bilobular, multilobular, ormushroom shapes)Diffuse choroidal melanoma, characterized by lateral growth throughout the choroid with minimal elevation,
are more difficult to diagnose and often cause significant exudative retinal detachment[3]
Choroidal melanomas may have variable coloration, ranging from amelanotic to darkly pigmented; some arepartially pigmented
TodayNewsReferenceEducationLog InRegister
4/9/2014 Choroidal Melanoma
http://emedicine.medscape.com/article/1190564-overview#showall 2/17
If the tumor is light-colored, its abnormal vascularization usually can be seen ophthalmoscopicallyOverlying the choroidal melanoma, there are usually retinal pigment epithelial changes (eg, drusen),patches of atrophy, and orange discoloration; orange changes can occur in both malignant and benignlesionsChoroidal melanoma may remain undetected underneath a large exudative retinal detachment, a subretinalhemorrhage, or a vitreous hemorrhageInfrequent presentations of advanced choroidal melanoma are a painful blind eye with cataract and proptosisfrom tumor transscleral orbital extensionAnterior choroidal melanomas might show sentinel vessels (dilated episcleral blood vessels visible throughthe conjunctiva) that feed the metabolically active tumorTransscleral growth of an anterior choroidal melanoma (mainly through emissary channels) may appear onexamination as a small subconjunctival area of abnormal hyperpigmentation
Diagnosis
Liver enzyme levels are indicated in any patient with uveal melanoma, because the liver is the most common siteof choroidal melanoma metastasis. The most sensitive tests of hepatic function are serum levels of the following:
Alkaline phosphataseGlutamic-oxaloacetic transaminaseLactate dehydrogenaseGamma-glutamyl transpeptidase
Ultrasonography
A-scan ultrasonography of the eye is useful for tumors thicker than 2-3 mmChoroidal melanoma characteristically shows an initial prominent spike, followed by low-to-medium internalreflectivity with diminishing amplitude and a significant echoVascular pulsations can be seen as fine oscillations of the internal spiking pattern within the tumorPerforming sequential A-scans, with accurate dimension measurements, in cases of diagnostic uncertaintyis importantB-scan ultrasonography of the eye is a routine test used in the evaluation of any posterior segment mass; itis especially needed in patients with media opacityFor choroidal melanomas, B-scan ultrasonography is used to help establish the diagnosis, to evaluatepossible extraocular extension, to estimate tumor size for periodic observation, and to plan therapeuticintervention
Intraocular melanomas have several distinctive features, as follows:
Low-to-medium reflectivityExcavation of underlying uveal tissueShadowing of subjacent soft tissuesInternal vascularityAn acoustic quiet zone at the base of the tumor called acoustic hollowing
Ultrasound biomicroscopy (UBM) has the following advantages:
Provides excellent resolution for anterior ocular abnormalitiesCan differentiate very anterior choroidal melanomas from those of ciliary body originCan help define the tumor’s anterior borderIs also helpful in assessing angle-closure glaucoma
Angiography
Fluorescein angiography and indocyanine green angiography do not show pathognomonic signs of choroidalmelanoma but can help point to its diagnosisSmall choroidal melanomas may show fluorescein angiographic changes similar to some choroidal nevi,with such changes ranging from normal angiography to hypofluorescence secondary to blockage ofbackground fluorescenceLarger melanomas may show a patchy pattern of early hypofluorescence and hyperfluorescence followedby late intense stainingSimultaneous fluorescence of retinal and choroidal circulation within the tumor is fairly distinctive ofchoroidal melanomas
4/9/2014 Choroidal Melanoma
http://emedicine.medscape.com/article/1190564-overview#showall 3/17
Imaging studies
Obtain a chest x-ray to rule out possible lung metastasesCT scanning of the globe and orbit is useful for visualizing extraocular extension and may help differentiatebetween choroidal or retinal detachment and a solid tumorMRI of the globe and orbit can be used to determine extrascleral extension of the melanoma anddistinguish surrounding fluid from the tumor
Management
Several modes of treatment are available for choroidal melanomas, as follows:
Observation may be acceptable for posterior uveal tumors where diagnosis is not well established; inparticular, tumors of less than 2-2.5 mm in elevation and 10 mm in diameter can be observed until growth isdocumentedEnucleation is the classic approach to choroidal melanomas and has been the preferred treatment for large(basal diameter >15 mm and height >10 mm) and complicated tumors, which compromise visual functionand for which other therapies tend to failPlaque brachytherapy is a widely accepted alternative to enucleation for medium-sized posterior uvealmelanomas (< 10 mm in height and < 15 mm in diameter)External beam irradiation with protons or helium ions is a frequently used alternative for the treatment ofmedium-sized choroidal melanomas, although it has been used for larger tumorsPars plana vitrectomy endoresectionBlock excision (sclerouvectomy) is an alternative treatment method reserved for small tumors covering lessthan one third of the globe’s circumferenceLaser photocoagulation and transpupillary thermotherapy are used to treat selected small choroidalmelanomas that are located away from the fovea and are less than 3 mm in thicknessOrbital exenteration is a radical treatment reserved for cases with widespread orbital extension; it should beconsidered only in rare cases where marked discomfort is associated with massive orbital spread of themelanoma
Adjuvant systemic chemotherapy is not advocated
When distant metastases are found in the initial systemic workup, palliative systemic chemotherapy is theprimary treatment
Image library
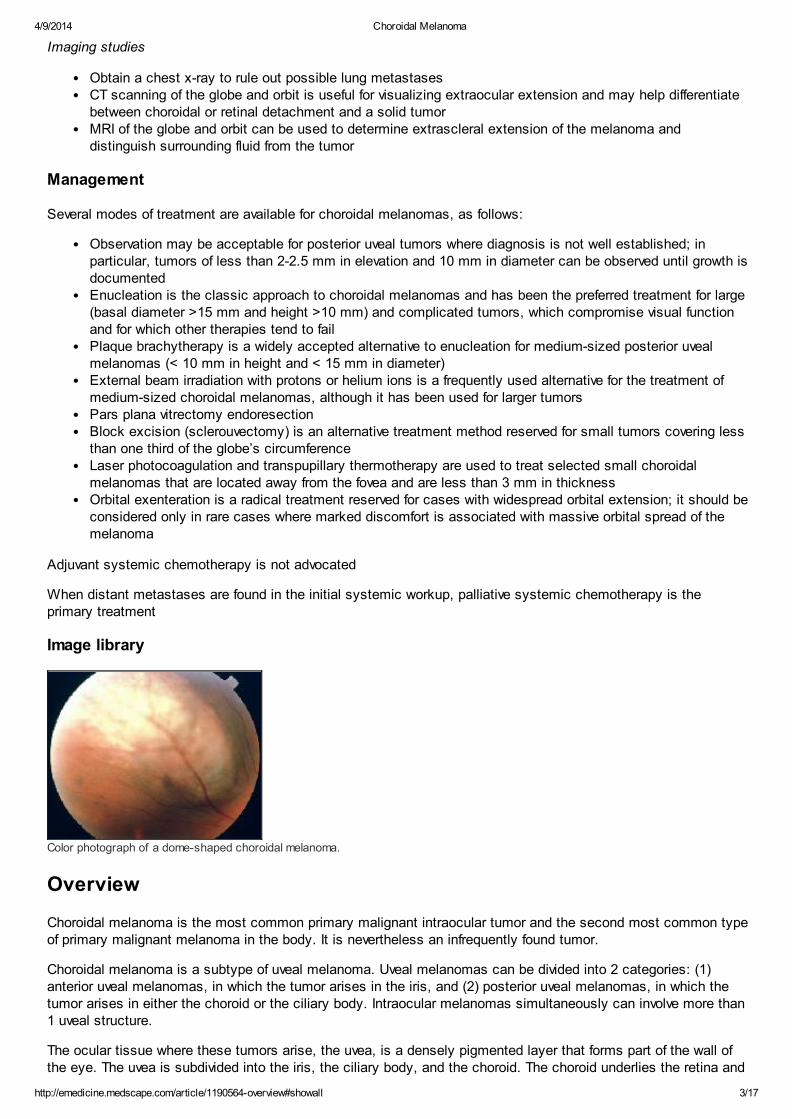
Color photograph of a dome-shaped choroidal melanoma.
Overview
Choroidal melanoma is the most common primary malignant intraocular tumor and the second most common typeof primary malignant melanoma in the body. It is nevertheless an infrequently found tumor.
Choroidal melanoma is a subtype of uveal melanoma. Uveal melanomas can be divided into 2 categories: (1)anterior uveal melanomas, in which the tumor arises in the iris, and (2) posterior uveal melanomas, in which thetumor arises in either the choroid or the ciliary body. Intraocular melanomas simultaneously can involve more than1 uveal structure.
The ocular tissue where these tumors arise, the uvea, is a densely pigmented layer that forms part of the wall ofthe eye. The uvea is subdivided into the iris, the ciliary body, and the choroid. The choroid underlies the retina and
4/9/2014 Choroidal Melanoma
http://emedicine.medscape.com/article/1190564-overview#showall 4/17
its pigment epithelium throughout the ocular fundus. The main function of the uvea is to provide oxygen and othernourishment to the highly metabolically demanding retinal photoreceptors. It is primarily a vascular tissue, withfenestrated capillaries and stroma containing melanocytes.
Go to Ciliary Body Melanoma, Conjunctival Melanoma, and Iris Melanoma for complete information on thesetopics.
Pathophysiology
Primary choroidal melanoma arises from melanocytes within the choroid. Most choroidal melanomas are believedto develop from preexisting melanocytic nevi, though de novo growth of choroidal melanomas also occurs. Threedistinct cell types are recognized in choroidal and other uveal melanomas: (1) spindle A, (2) spindle B, and (3)epithelioid. The last cell type usually has the most aggressive behavior and carries a poorer prognosis for thepatient’s long-term survival.
Choroidal melanomas may have variable coloration, ranging from darkly pigmented to purely amelanotic. Theytypically are dome-shaped. As they enlarge, if they break through the Bruch membrane, they can assume amushroom configuration. Other shapes found for these tumors are bilobular, multilobular, and diffuse. The last ofthese is characterized by lateral growth throughout the choroid with minimal elevation; it occurs in about 5% ofcases. Rarely, choroidal melanomas may arise in a multicentric distribution in 1 or both eyes.
Choroidal melanomas affect the retinal pigment epithelium as they push against it and deprive it of normalchoroidal circulation. Overlying retinal pigment epithelium usually develops areas of atrophy, drusen, and localizedpigment epithelial detachments.
Areas of phagocytic activity, where cellular debris from melanocytes is digested, give the pigment epitheliumpatches of coloration change. Macrophages within these typically orange areas contain melanin and lipofuscin.These changes can lead to choroidal neovascularization over the tumor, with consequent subretinal exudation,hemorrhage, and fibrous plaque formation.
Growth of choroidal melanomas can occur silently until it produces enough visual loss through various
mechanisms.[4] The tumor’s disruption of choroidal circulation and consequent ischemia typically causedegeneration of retinal photoreceptors and other retinal neurons. The retina overlying the tumor can separate intocystoid spaces and larger schisis cavities. There may be associated cystoid macular edema.
In general, the farther the tumor’s origin is from the optic nerve and fovea, the larger the tumor can become beforethe patient notices a visual field defect. Exudation of fluid into the subretinal space with consequent retinaldetachment may enlarge the field loss. This exudation can lead to total retinal detachment. Rarely, choroidalmelanomas can impinge into underlying posterior ciliary nerves, causing severe ocular pain.
Other signs and symptoms can result if the tumor grows anteriorly, pathologically involving the ciliary body,trabecular meshwork, and lens, with consequent ocular hypotension or hypertension and cataract. Large choroidalmelanomas can induce iris rubeosis. Erosion of the melanoma into blood vessels in adjacent tissues, or areas ofnecrosis within the tumor, can lead to vitreous hemorrhage or hyphema.
Choroidal melanoma ultimately causes death, practically always secondary to distant metastases rather thanlocal spread. Its metastatic potential depends on the histopathologic aggressiveness of the tumor cells.Unfortunately, it not infrequently metastasizes before diagnosis. If the melanoma does not show extraocularextension, it can only spread hematogenously, because there are no lymphatic vessels in the eye. It most oftenmetastasizes to the liver; other organs of dissemination include the lung, bone, skin, and central nervous system(CNS).
Less frequently, choroidal melanoma can grow transsclerally, through emissary channels, and metastasize locallyinto the orbit or rarely the conjunctiva. Choroidal melanoma almost never extends through the optic nerve; when itdoes, it is usually in juxtapapillary tumors or in diffuse choroidal melanomas.
Etiology
A particular predisposition exists for choroidal melanomas to occur in people with light-colored irides. Evidencepoints to sunlight exposure as a likely contributor to the development of choroidal melanoma.
Predisposing diseases for uveal melanomas include a family history of uveal melanoma, uveal nevus, congenital
4/9/2014 Choroidal Melanoma
http://emedicine.medscape.com/article/1190564-overview#showall 5/17
ocular melanocytosis, dysplastic nevus syndrome, and xeroderma pigmentosum.
Epidemiology
United States statistics
Incidence of primary choroidal melanoma is about 6 cases per 1 million population. Perhaps because of increasedsunlight exposure, there appears to be a higher incidence of uveal melanoma in the southern latitudes of theUnited States. Alternatively, this might be the effect of a tendency of older Americans to retire in the South.
International statistics
Incidence of choroidal melanoma is much higher in countries with large numbers of people of northern Europeandescent than elsewhere in the world. In Denmark and other Scandinavian countries, incidence is about 7.5 casesper million per year.
Age-related differences in incidence
Incidence of choroidal melanoma is highest around age 55 years. In Asians, although it is a very infrequent tumor,reports indicate a peak incidence at a somewhat younger age. Choroidal melanoma is exceptional in children.
Sex-related differences in incidence
Choroidal melanoma is found slightly more frequently in men for all age groups, except from 20-39 years, when asmall predilection exists for women.
Race-related differences in incidence
Choroidal melanoma and other uveal melanomas most often affect whites of northern European descent. Incidenceof choroidal melanoma among blacks is extremely rare. Hispanics and Asians are thought to have a small butintermediate risk compared to whites and blacks.
Clinical Presentation
Patient history
Choroidal melanomas remain asymptomatic for prolonged periods of time; they may be found incidentally duringophthalmoscopy. In general, the more anterior their origin, the longer the delay of any symptoms. Choroidalmelanoma may present with the following symptoms:
Blurred visual acuity consequent to various mechanisms, including growth of the melanoma into thesubfoveal retina, cystoid macular edema, retinal detachment, vitreous hemorrhage, cataract, and blockageof the visual axis directly by the tumorParacentral scotoma, occurring as the tumor affects the perifoveal retinaPainless and progressive visual field loss, occurring as peripheral melanoma grows or exudates subretinalfluidFloaters, developing when areas of necrosis within the tumor or adjacent structures produce vitreoushemorrhage or hyphemaSevere ocular pain, occasionally occurring secondary to impingement of choroidal melanomas on posteriorciliary nerves or to high intraocular pressure from acute angle-closure glaucomaHistory of weight loss, marked fatigue, cough, or change in bowel or bladder habits, which should promptconsideration of primary nonocular malignancy with choroidal metastasis
Physical examination
Patients with choroidal melanoma may present with painless visual loss or, occasionally, inflammation and painfrom a complicated tumor. However, many patients have no symptoms, and melanomas are discovered on routineophthalmologic examination.
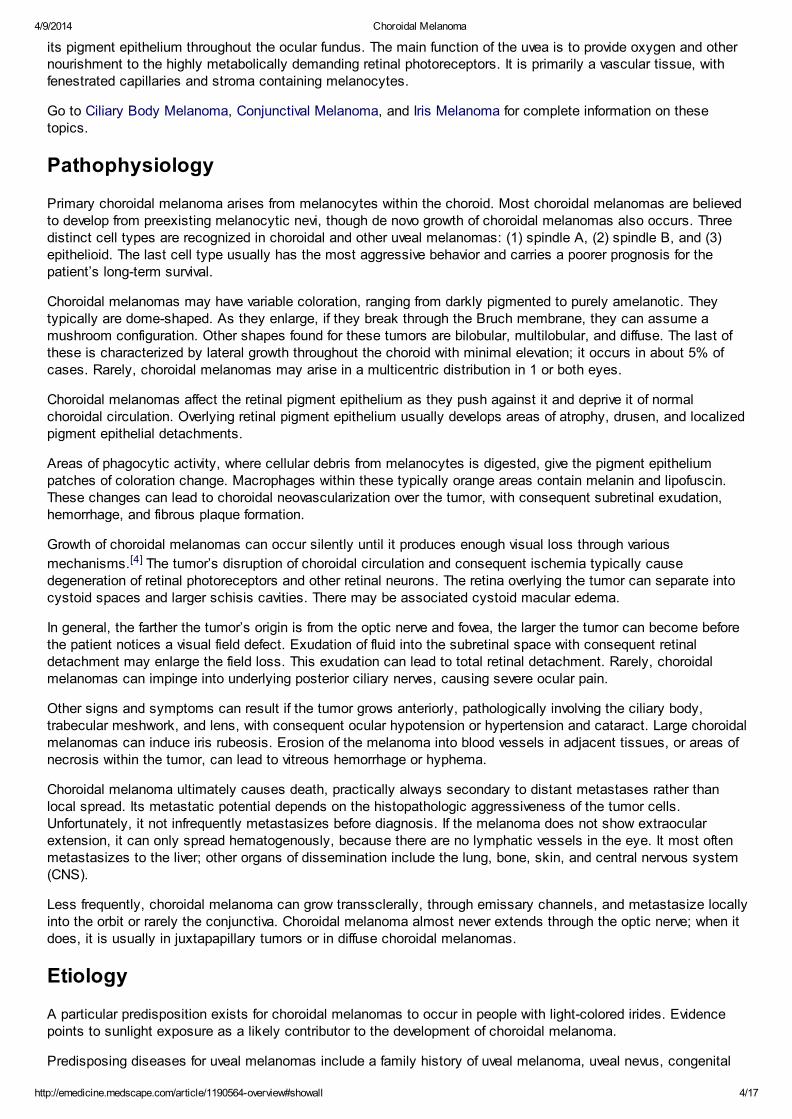
Small choroidal melanomas typically take the form of a nodular, dome-shaped, and well-circumscribed mass
4/9/2014 Choroidal Melanoma
http://emedicine.medscape.com/article/1190564-overview#showall 6/17
under the retinal pigment epithelium (see the image below). As they grow, they may adopt more irregularconfigurations (eg, bilobular, multilobular, or mushroom shapes).
Color photograph of a dome-shaped choroidal melanoma.
An unusual tumor type that may be found is diffuse choroidal melanoma, characterized by lateral growththroughout the choroid with minimal elevation. Diffuse melanomas are more difficult to diagnose and often cause
significant exudative retinal detachment.[3]
Choroidal melanomas may have variable coloration, ranging from amelanotic to darkly pigmented. Some tumorsare partially pigmented. If the tumor is light-colored, its abnormal vascularization usually can be seenophthalmoscopically. Overlying the choroidal melanoma there are usually retinal pigment epithelial changes (eg,drusen), patches of atrophy, and orange discoloration. Orange changes in the pigment epithelium have traditionallybeen regarded as strongly indicative of malignancy; however, it is now well known that they can be seen overbenign lesions as well.
Sometimes, a choroidal melanoma may remain undetected underneath a large exudative retinal detachment, asubretinal hemorrhage, or a vitreous hemorrhage. Infrequent presentations of advanced choroidal melanoma are apainful blind eye with cataract and proptosis from tumor transscleral orbital extension.
Anterior choroidal melanomas might show sentinel vessels (dilated episcleral blood vessels visible through theconjunctiva) that feed the metabolically active tumor. Transscleral growth of an anterior choroidal melanoma(mainly through emissary channels) may appear on examination as a small subconjunctival area of abnormalhyperpigmentation.
Transillumination can be used to find the borders of the tumor, especially if it is surrounded by exudative retinaldetachment. Its precision is dependent on even tumor pigmentation and if associated hemorrhage is present.
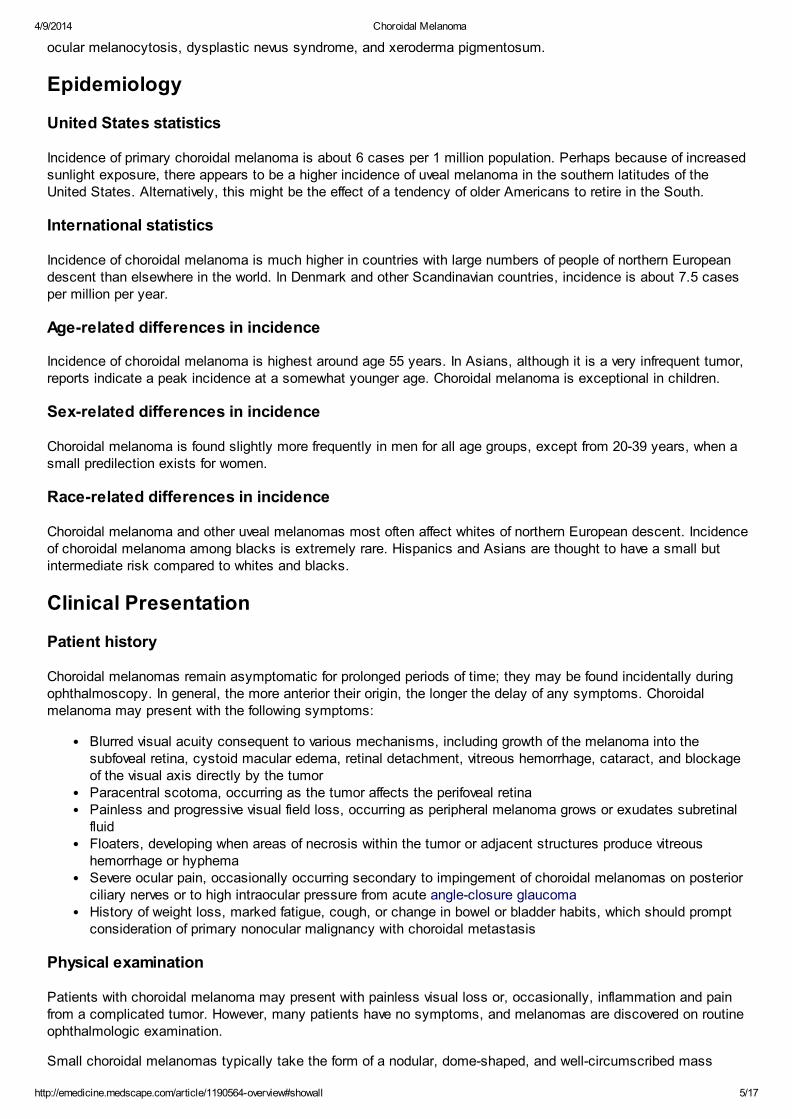
Overall accuracy of the clinical diagnosis of choroidal melanoma, using modern diagnostic tools, was shown to be
99.7% in a preliminary report from the Collaborative Ocular Melanoma Study.[5] Thorough evaluation of choroidalmelanoma should include a complete physical examination, with particular attention to the hepatic-abdominalregion and the skin and subcutaneous tissues (see the image below), which are frequent sites of metastaticspread.
Photograph show ing a skin metastasis of a posterior choroidal melanoma.
Differential Diagnosis
The differential diagnosis includes the following:
Choroidal Detachment
4/9/2014 Choroidal Melanoma
http://emedicine.medscape.com/article/1190564-overview#showall 7/17
Intraocular Foreign BodyChronic Angle Closure GlaucomaGlaucoma, HyphemaNeovascular GlaucomaCavernous HemangiomaVitreous HemorrhageHyphemaCiliary Body MelanomaConjunctival MelanomaIris Melanoma
Benign and malignant tumors, cysts, and other abnormal masses in the choroid, retina, and pigment epitheliummust be distinguished from choroidal melanomas.Other problems to be considered include the following:
Melanocytic nevusMelanocytomaMetastatic tumorsMedulloepithelioma (diktyoma)Choroidal osteomaAdenomaAdenocarcinomaCombined hamartoma of the retina and pigment epitheliumCongenital hypertrophy and reactive hyperplasia of the retinal pigment epitheliumRetinal cavernous hemangiomaPresumed acquired retinal hemangiomaLymphoid tumorHemangiopericytomaLeiomyomaNeurofibromaGlioneuromaAstrocytomaRhabdomyosarcomaPosterior uveitisSarcoid nodulesTubercular granuloma
Other choroidal masses can present with characteristics very similar to those of choroidal melanoma, making it achallenging diagnosis.
Laboratory Studies
The most common site of choroidal melanoma metastasis is the liver. Liver enzyme levels are indicated in anypatient with uveal melanoma. The most sensitive tests of hepatic function are serum levels of alkalinephosphatase, glutamic-oxaloacetic transaminase, lactate dehydrogenase, and gamma-glutamyl transpeptidase.
These test results are negative at the time of diagnosis in most patients with choroidal melanoma. If any of theselaboratory test results are abnormal, order ultrasonography and computed tomography (CT) of the liver.Unfortunately, both imaging modalities have low sensitivity for metastasis smaller than 10-20 mm in diameter.
Ultrasonography
A-scan ultrasonography of the eye is useful for tumors thicker than 2-3 mm. Choroidal melanoma characteristicallyshows an initial prominent spike, followed by low-to-medium internal reflectivity with diminishing amplitude and asignificant echo (see the image below). Vascular pulsations can be seen as fine oscillations of the internal spikingpattern within the tumor. Standardized ultrasonography has a diagnostic accuracy of more than 95%. Performingsequential A-scans, with accurate dimension measurements, in cases of diagnostic uncertainty is important.

4/9/2014 Choroidal Melanoma
http://emedicine.medscape.com/article/1190564-overview#showall 8/17
A-scan ultrasound of choroidal melanoma show ing low -to-medium internal reflectivity.
B-scan ultrasonography of the eye is a routine test used in the evaluation of any posterior segment mass. It isespecially needed in patients with media opacity. For choroidal melanomas, B-scan ultrasonography is used tohelp establish the diagnosis, to evaluate possible extraocular extension, to estimate tumor size for periodicobservation, and to plan therapeutic intervention.
B-scan ultrasound show ing acoustic hollow ing and uveal excavation in posterior choroidal melanoma.
B-scan ultrasound show ing acoustic hollow ing in intraorbital extension of a posterior choroidal melanoma.
Intraocular melanomas have several distinctive features, as follows:
Low-to-medium reflectivityExcavation of underlying uveal tissueShadowing of subjacent soft tissuesInternal vascularityAn acoustic quiet zone at the base of the tumor called acoustic hollowing
Ultrasound biomicroscopy (UBM) uses high-frequency waves, with excellent resolution for anterior ocularabnormalities. It can differentiate very anterior choroidal melanomas from those of ciliary body origin and can helpdefine the tumor’s anterior border. It is also helpful in assessing angle-closure glaucoma.
Angiography and Radiography
Fluorescein angiography and indocyanine green angiography do not show pathognomonic signs of choroidalmelanoma but can help point to its diagnosis.
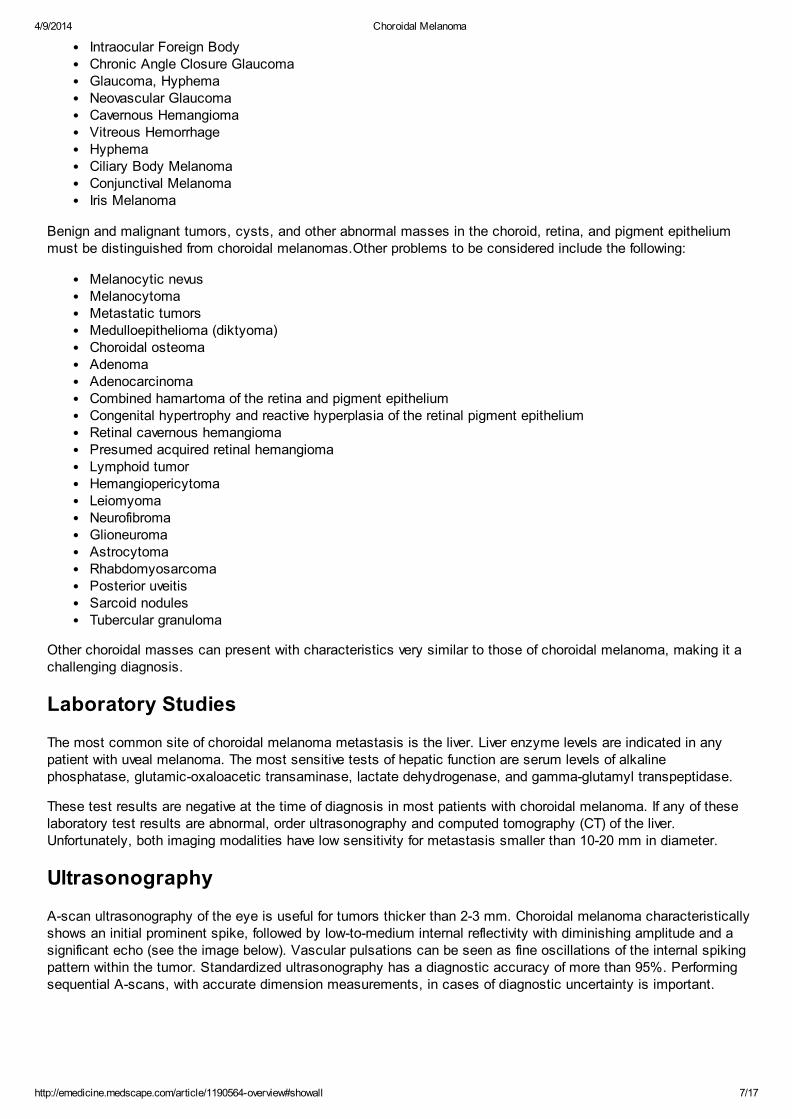
Small choroidal melanomas may show fluorescein angiographic changes similar to some choroidal nevi, with suchchanges ranging from normal angiography to hypofluorescence secondary to blockage of backgroundfluorescence. Larger melanomas may show a patchy pattern of early hypofluorescence and hyperfluorescencefollowed by late intense staining (see the image below).
4/9/2014 Choroidal Melanoma
http://emedicine.medscape.com/article/1190564-overview#showall 9/17
Late f luorescein angiogram of choroidal melanoma show ing early diffuse staining.
Some choroidal melanomas demonstrate intrinsic vascularization, visible throughout the angiogram (see the imagebelow). The angiographic sign, called the “double circulation pattern,” refers to simultaneous fluorescence of retinaland choroidal circulation within the tumor. When it occurs, it is fairly distinctive of choroidal melanomas.
Early f luorescein angiogram of choroidal melanoma show ing intrinsic vascularity.
Obtain a chest x-ray in patients with choroidal melanomas to rule out possible lung metastases.
Computed Tomography
Computed tomography (CT) scanning of the globe and orbit is more expensive than ultrasonography and is not assensitive. It is useful for visualizing extraocular extension and may help differentiate between choroidal or retinaldetachment and a solid tumor.
CT scan requires intravenous injection of contrast material. Choroidal melanoma shows enhancement withcontrast, whereas exudation does not. CT scan also is sensitive in detecting calcium, a feature of some tumorsthat are different than uveal melanomas (characteristically choroidal osteoma).
Magnetic Resonance Imaging
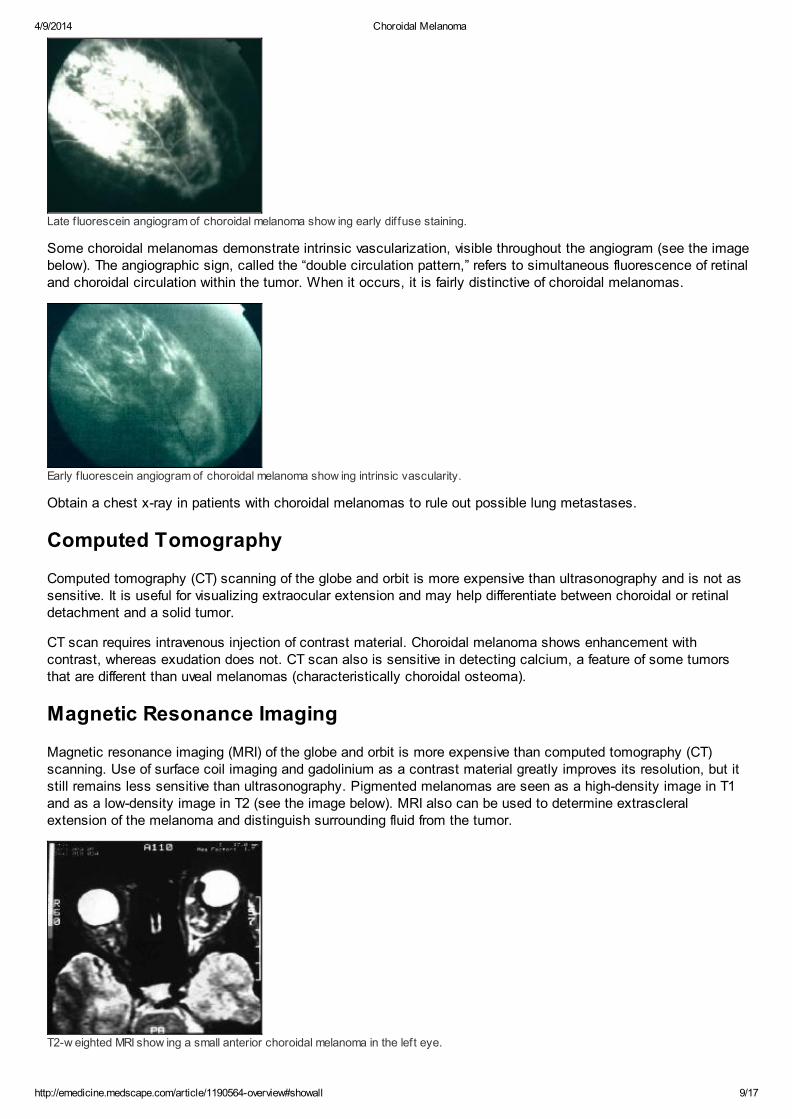
Magnetic resonance imaging (MRI) of the globe and orbit is more expensive than computed tomography (CT)scanning. Use of surface coil imaging and gadolinium as a contrast material greatly improves its resolution, but itstill remains less sensitive than ultrasonography. Pigmented melanomas are seen as a high-density image in T1and as a low-density image in T2 (see the image below). MRI also can be used to determine extrascleralextension of the melanoma and distinguish surrounding fluid from the tumor.
T2-w eighted MRI show ing a small anterior choroidal melanoma in the left eye.

4/9/2014 Choroidal Melanoma
http://emedicine.medscape.com/article/1190564-overview#showall 10/17
Biopsy
Fine-needle biopsy and incisional biopsy are not usually required but may be helpful in difficult diagnostic cases,particularly for distinguishing amelanotic melanomas from metastatic tumors, and in situations where the results ofother ancillary tests are equivocal. Fine-needle biopsy is increasingly being performed for prognostic purposes.
In experienced hands, both biopsy techniques have an accuracy of more than 95% in tumors larger than 3 mm.Incisional biopsy is more invasive and may have more associated complications, but it has less false-negative andfalse-positive results. The most common complication for tumor biopsy is intralesional or perilesional hemorrhage.
Risk of spread of cancerous cells in the case of fine-needle biopsy is small for choroidal melanoma (unlikeretinoblastoma). Follow biopsy with prompt treatment to prevent extrascleral extension.
Genetic analysis and karyotyping of biopsy specimens have gained increasing attention. Chromosome 3monosomy in the choroidal tumor has been shown to be associated with a significantly greater risk of developing
metastases.[6]
Specific genetic errors are becoming better understood, such as inactivation of BAP1 (BRCA-associated protein1), which is associated with metastatic spread, often through monosomy 3.
Analysis of tumoral expression of multiple genes has lead to the subdivision of uveal melanomas into 2 types.Around half of ocular melanomas are class 1, which carry a low risk of metastasis. The other half are class 2,which have a different gene expression pattern, frequently showing chromosome 3 monosomy, and carry a highrisk of metastasis. Gene expression profiling outperforms monosomy 3 at predicting metastatic spread.
However, because no effective treatment is available for metastatic disease, the clinical impact of performingroutine biopsies on choroidal melanoma is unclear at this point. Some experts have argued against this practice.
Histologic Findings
Histologic evaluation of the tumor after enucleation can confirm the diagnosis and determine the prognosis (see
the images below).[7]
Histologic section of an enucleated eye show ing a large dome-shaped choroidal melanoma.
Histologic section of an enucleated eye show ing a medium-sized mushroom-shaped choroidal melanoma w ith associated exudative
retinal detachment.
As noted (see Pathophysiology), 3 distinct cell types are recognized to occur in uveal melanomas: (1) spindle A,(2) spindle B, and (3) epithelioid. Spindle A cells have elongated nuclei and uncommonly have mitotic figures (seethe image below).
4/9/2014 Choroidal Melanoma
http://emedicine.medscape.com/article/1190564-overview#showall 11/17
Choroidal melanoma. Histologic section show ing spindle A cells in a uveal nevus.
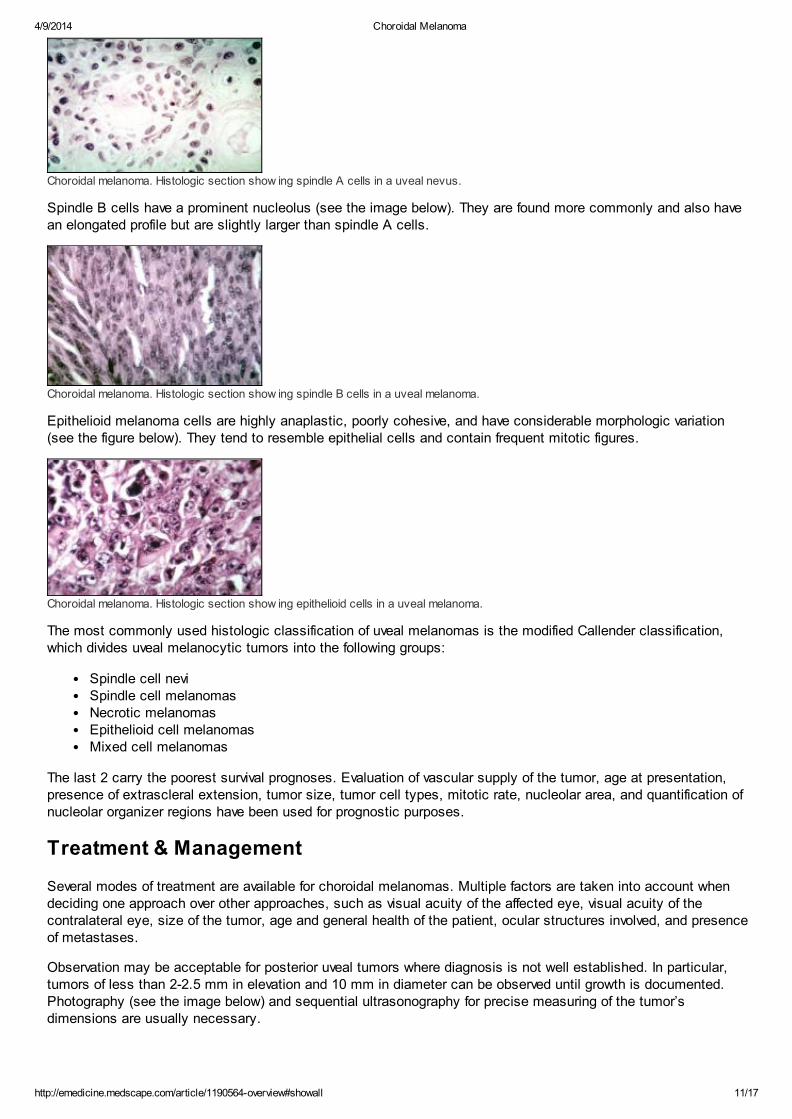
Spindle B cells have a prominent nucleolus (see the image below). They are found more commonly and also havean elongated profile but are slightly larger than spindle A cells.
Choroidal melanoma. Histologic section show ing spindle B cells in a uveal melanoma.
Epithelioid melanoma cells are highly anaplastic, poorly cohesive, and have considerable morphologic variation(see the figure below). They tend to resemble epithelial cells and contain frequent mitotic figures.
Choroidal melanoma. Histologic section show ing epithelioid cells in a uveal melanoma.
The most commonly used histologic classification of uveal melanomas is the modified Callender classification,which divides uveal melanocytic tumors into the following groups:
Spindle cell neviSpindle cell melanomasNecrotic melanomasEpithelioid cell melanomasMixed cell melanomas
The last 2 carry the poorest survival prognoses. Evaluation of vascular supply of the tumor, age at presentation,presence of extrascleral extension, tumor size, tumor cell types, mitotic rate, nucleolar area, and quantification ofnucleolar organizer regions have been used for prognostic purposes.
Treatment & Management
Several modes of treatment are available for choroidal melanomas. Multiple factors are taken into account whendeciding one approach over other approaches, such as visual acuity of the affected eye, visual acuity of thecontralateral eye, size of the tumor, age and general health of the patient, ocular structures involved, and presenceof metastases.
Observation may be acceptable for posterior uveal tumors where diagnosis is not well established. In particular,tumors of less than 2-2.5 mm in elevation and 10 mm in diameter can be observed until growth is documented.Photography (see the image below) and sequential ultrasonography for precise measuring of the tumor’sdimensions are usually necessary.

4/9/2014 Choroidal Melanoma
http://emedicine.medscape.com/article/1190564-overview#showall 12/17
Transpupillary photograph show ing a posterior choroidal melanoma.
Choice of treatment of choroidal melanoma remains controversial in many respects. Although enucleation hasbeen the treatment of choice in the past, it appears that vision-sparing approaches might offer similar degrees ofocular and metastatic tumor control—particularly because it is clear that in many patients at the time of diagnosis,posterior uveal melanomas already have spread through micrometastasis.
Systemic chemotherapy
Although undetected metastatic spread at the time of diagnosis and treatment of choroidal melanoma is a majorconcern in every patient, adjuvant systemic treatment is not advocated. This consensus comes from treatmenttrials with intraocular melanomas and extrapolation of the experience with cutaneous melanoma, where adjuvanttreatment has shown no benefit.
In cases where distant metastases are found during the initial systemic workup, treatment of the intraocularmelanomas becomes palliative. Systemic chemotherapy is the primary treatment.
Many modalities and combinations of chemotherapeutic and immunotherapeutic agents exist, but, for the mostpart, results continue to be disappointing. This is an area of intense medical research, with ever-increasingdegrees of biological sophistication being applied to new clinical trials.
Enucleation
Enucleation is the classic approach to choroidal melanomas and has been the preferred treatment for large (basaldiameter >15 mm and height >10 mm) and complicated tumors, which compromise visual function and for whichother therapies tend to fail.
Because of potential release of malignant cells into the bloodstream and orbital soft tissues during the surgicalprocedure, manipulation of the globe should be kept to a minimum. Particular care must be taken to avoidperforation of the globe during surgery. If transscleral extension is found (see the image below), the tumor shouldbe removed in 1 piece, followed by cryotherapy of the involved orbital soft tissues.
Photograph show ing an enucleated eye w ith advanced choroidal melanoma w ith transscleral extension.
The theoretical advantage of enucleation over globe-sparing treatments is a reduced risk of metastatic spread.However, the Collaborative Ocular Melanoma Study (COMS), in which medium-sized tumors were treated witheither iodine-125 brachytherapy (see below) or enucleation, found that the mortality rates after brachytherapy did
not differ from the mortality rates following enucleation for up to 12 years after treatment.[8, 9]
Some investigators have advocated pre-enucleation irradiation of the eye as a way to improve survival. However,the COMS demonstrated neither a positive nor a negative effect on the 10-year mortality rates among patientswhose eyes containing large choroidal melanomas were randomly assigned to treatment with enucleation alone or
to enucleation preceded by external radiation.[10]
Plaque brachytherapy
4/9/2014 Choroidal Melanoma
http://emedicine.medscape.com/article/1190564-overview#showall 13/17
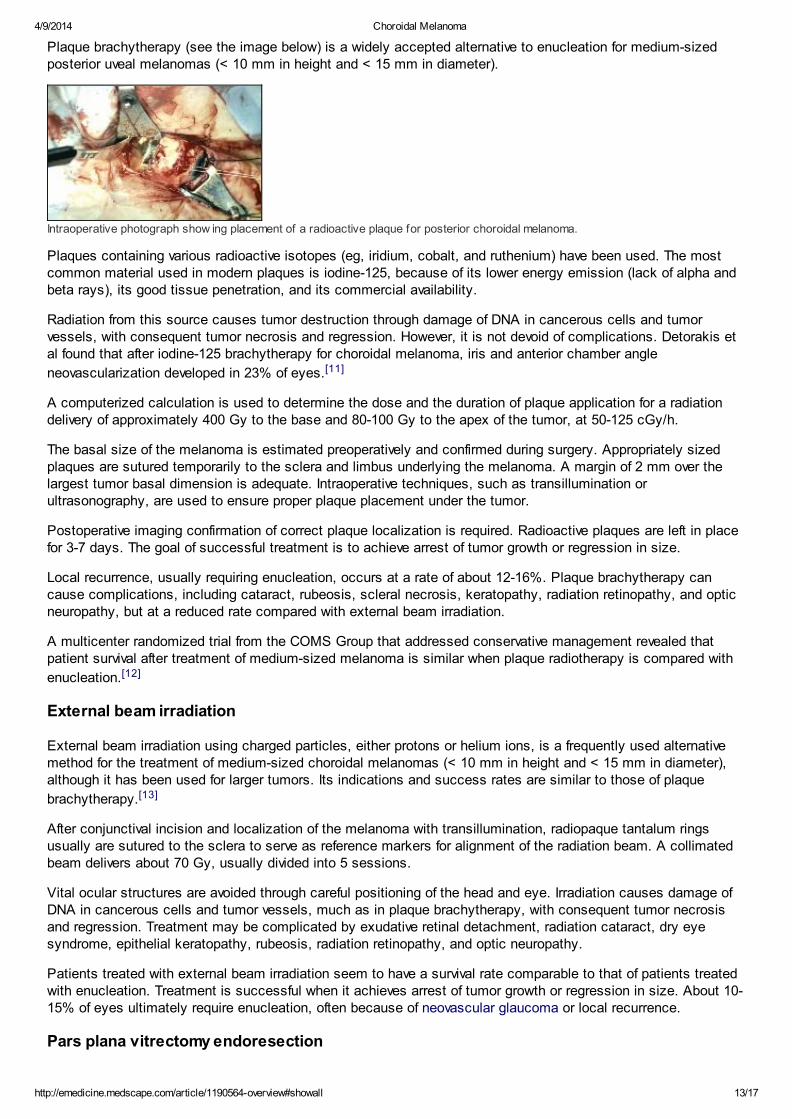
Plaque brachytherapy (see the image below) is a widely accepted alternative to enucleation for medium-sizedposterior uveal melanomas (< 10 mm in height and < 15 mm in diameter).
Intraoperative photograph show ing placement of a radioactive plaque for posterior choroidal melanoma.
Plaques containing various radioactive isotopes (eg, iridium, cobalt, and ruthenium) have been used. The mostcommon material used in modern plaques is iodine-125, because of its lower energy emission (lack of alpha andbeta rays), its good tissue penetration, and its commercial availability.
Radiation from this source causes tumor destruction through damage of DNA in cancerous cells and tumorvessels, with consequent tumor necrosis and regression. However, it is not devoid of complications. Detorakis etal found that after iodine-125 brachytherapy for choroidal melanoma, iris and anterior chamber angle
neovascularization developed in 23% of eyes.[11]
A computerized calculation is used to determine the dose and the duration of plaque application for a radiationdelivery of approximately 400 Gy to the base and 80-100 Gy to the apex of the tumor, at 50-125 cGy/h.
The basal size of the melanoma is estimated preoperatively and confirmed during surgery. Appropriately sizedplaques are sutured temporarily to the sclera and limbus underlying the melanoma. A margin of 2 mm over thelargest tumor basal dimension is adequate. Intraoperative techniques, such as transillumination orultrasonography, are used to ensure proper plaque placement under the tumor.
Postoperative imaging confirmation of correct plaque localization is required. Radioactive plaques are left in placefor 3-7 days. The goal of successful treatment is to achieve arrest of tumor growth or regression in size.
Local recurrence, usually requiring enucleation, occurs at a rate of about 12-16%. Plaque brachytherapy cancause complications, including cataract, rubeosis, scleral necrosis, keratopathy, radiation retinopathy, and opticneuropathy, but at a reduced rate compared with external beam irradiation.
A multicenter randomized trial from the COMS Group that addressed conservative management revealed thatpatient survival after treatment of medium-sized melanoma is similar when plaque radiotherapy is compared with
enucleation.[12]
External beam irradiation
External beam irradiation using charged particles, either protons or helium ions, is a frequently used alternativemethod for the treatment of medium-sized choroidal melanomas (< 10 mm in height and < 15 mm in diameter),although it has been used for larger tumors. Its indications and success rates are similar to those of plaque
brachytherapy.[13]
After conjunctival incision and localization of the melanoma with transillumination, radiopaque tantalum ringsusually are sutured to the sclera to serve as reference markers for alignment of the radiation beam. A collimatedbeam delivers about 70 Gy, usually divided into 5 sessions.
Vital ocular structures are avoided through careful positioning of the head and eye. Irradiation causes damage ofDNA in cancerous cells and tumor vessels, much as in plaque brachytherapy, with consequent tumor necrosisand regression. Treatment may be complicated by exudative retinal detachment, radiation cataract, dry eyesyndrome, epithelial keratopathy, rubeosis, radiation retinopathy, and optic neuropathy.
Patients treated with external beam irradiation seem to have a survival rate comparable to that of patients treatedwith enucleation. Treatment is successful when it achieves arrest of tumor growth or regression in size. About 10-15% of eyes ultimately require enucleation, often because of neovascular glaucoma or local recurrence.
Pars plana vitrectomy endoresection
4/9/2014 Choroidal Melanoma
http://emedicine.medscape.com/article/1190564-overview#showall 14/17
In a nested case-control study, endoresection for posterior choroidal melanomas provided outcomes similar to or
better than those obtained with iodine-125 plaque brachytherapy.[14] Metastatic spread was observed in 11(20.4%) of the 54 patients in the iodine-125 brachytherapy group, compared with only 1 (3.7%) of the 27 patientsin the endoresection group. No significant difference was found in overall or relapse-free survival between the 2groups.
Block excision
Block excision (sclerouvectomy), is an alternative treatment method for choroidal melanomas. It is reserved forsmall tumors covering less than one third of the globe’s circumference.
The goal of block excision is to salvage the eye, with most of these patients retaining some useful vision. Itconsists of full-thickness excision with in-block removal of tumor, choroid, retina, and sclera. A 3-mm margin ofhealthy tissue around the melanoma is included, followed by closure with a graft of banked sclera. Surroundtreatment with cryotherapy or laser usually is added.
The most common complications are vitreous hemorrhage, retinal detachment, residual tumor, and cataract. Risksare improved by a modified approach, lamellar sclerouvectomy, which uses a partial-thickness scleral flap andminimizes altering the retina and vitreous. In about 15-20% of cases, local reappearance of the melanomanecessitates subsequent treatment, usually enucleation.
Laser photocoagulation and transpupillary thermotherapy
Laser photocoagulation and transpupillary thermotherapy are used to treat selected small choroidal melanomas,when the lesions are located away from the fovea and are less than 3 mm in thickness.
Orbital exenteration
Orbital exenteration is a radical treatment reserved for cases with widespread orbital extension. Patients with suchadvanced melanomas are likely to have extensive distant metastases and poor prognoses, with or without orbitalexenteration surgery. The usefulness of such disfiguring surgery is not established; the procedure should beconsidered only in rare cases where marked discomfort is associated with massive orbital spread of themelanoma.
Consultations
It may be necessary to consult an oncologist and a radiation oncologist.
Further outpatient care
Irrespective of the treatment modality chosen, patients with choroidal melanomas need to be observed carefullyand for many years. This is particularly true for small tumors, when the diagnosis is not established clearly. Closeobservation and measurement of the dimensions of the tumors with any of the diagnostic tools mentioned earlier iscritical.
Repeat examinations usually are performed about every 3 months initially, and if no changes are seen, follow-upcare is performed every 6 months. If growth of the lesion is detected, consider further treatment. Choroidalmelanomas may show size regression starting several months after being treated with external beam irradiation orplaque brachytherapy. The goal of successful treatment is not necessarily reduction in size but long-term arrest ofthe tumor’s growth.
Repeat examinations and imaging tests are performed after all treatment modalities because of the possibility ofintraocular or extraocular tumor recurrence. Follow-up care in patients with treated choroidal melanomas shouldinclude thorough physical examinations, liver function tests, and imaging of lungs, repeated about every 6-12months. Early detection of distant metastases may affect management and survival.
Deterrence/prevention
Patients with choroidal nevi, a family history of uveal melanoma, congenital ocular melanocytosis, dysplasticnevus syndrome, and other predisposing conditions of uveal melanoma may benefit from annual carefulophthalmologic examinations.
4/9/2014 Choroidal Melanoma
http://emedicine.medscape.com/article/1190564-overview#showall 15/17
Limiting excessive ocular sunlight exposure through sunglasses or other means may have a theoretical preventiveeffect in patients with a predisposition to intraocular melanoma.
Prognosis
Visual prognosis is guarded for choroidal melanomas. Choroidal melanoma normally leads to partial or total visualloss in the affected eye. This is the result of either tumor destruction of ocular structures or consequence to thetreatment used. Patients with small- to medium-sized choroidal melanomas may be able to preserve very good
central vision, even after treatment.[4]
Choroidal melanoma is a disease with a high mortality rate, usually irrespective of the chosen treatment modality.About 30-50% of patients with choroidal melanoma will die within 10 years from diagnosis and treatment. Death isusually secondary to distant metastases, and the risk is greatest in larger tumors.
For large melanomas, the Collaborative Ocular Melanoma Study found that the 10-year rates of death secondaryto metastasis were 45% in the pre-enucleation radiation group and 40% in the enucleation alone group. Thereappears to be no survival benefit attributable to pre-enucleation radiation. The maximum diameter of the base of thetumor and older age were the primary predictors of time to death in patients with melanoma metastasis.
Previous publications have found several tumor features to correlate with increased mortality, including larger size,anterior location, transscleral extension, growth through the Bruch membrane, optic nerve extension, lack of
pigmentation, and histologic characteristics (eg, mitotic activity and cell type).[15] Although metastases from theprimary intraocular melanoma can first be detected years later, their highest incidence is in the first year afterdiagnosis. As yet, no effective treatment exists for metastatic uveal melanoma.
Contributor Information and DisclosuresAuthorEnrique Garcia-Valenzuela, MD, PhD Clinical Assistant Professor, Department of Ophthalmology,University of Illinois Eye and Ear Infirmary; Consulting Staff, Vitreo-Retinal Surgery, Midwest RetinaConsultants, SC, Parkside Center
Enrique Garcia-Valenzuela, MD, PhD is a member of the following medical societies: American Academy ofOphthalmology, American Society of Retina Specialists, Association for Research in Vision andOphthalmology, Retina Society, and Society for Neuroscience
Disclosure: Nothing to disclose.
Coauthor(s)Mauricio E Pons, MD Associate Physician, California Retina Associates
Mauricio E Pons, MD is a member of the following medical societies: American Academy of Ophthalmology,American Society of Retina Specialists, and Association for Research in Vision and Ophthalmology
Disclosure: Nothing to disclose.
James E Puklin, MD Professor, Department of Ophthalmology, Chair, Human Investigation Committee,Wayne State University School of Medicine
Disclosure: Nothing to disclose.
Cathleen A Davidson, MSc Clinical Staff, Department of Obstetrics and Gynecology, Laboratory of AssistedReproductive Technologies (ART), University of Michigan Medical School
Disclosure: Nothing to disclose.
Specialty Editor BoardRussell P Jayne, MD Consulting Vitreoretinal Surgeon, The Retina Center at Las Vegas
Russell P Jayne, MD is a member of the following medical societies: American Medical Association, AmericanSociety of Cataract and Refractive Surgery, and American Society of Retina Specialists
4/9/2014 Choroidal Melanoma
http://emedicine.medscape.com/article/1190564-overview#showall 16/17
Disclosure: Nothing to disclose.
Simon K Law, MD, PharmD Clinical Professor of Health Sciences, Department of Ophthalmology, JulesStein Eye Institute, University of California, Los Angeles, David Geffen School of Medicine
Simon K Law, MD, PharmD is a member of the following medical societies: American Academy ofOphthalmology, American Glaucoma Society, and Association for Research in Vision and Ophthalmology
Disclosure: Nothing to disclose.
Steve Charles, MD Director of Charles Retina Institute; Clinical Professor, Department of Ophthalmology,University of Tennessee College of Medicine; Adjunct Professor of Ophthalmology, Columbia College ofPhysicians and Surgeons; Clinical Professor Ophthalmology, Chinese University of Hong Kong
Steve Charles, MD is a member of the following medical societies: American Academy of Ophthalmology,American Society of Retina Specialists, Club Jules Gonin, Macula Society, and Retina Society
Disclosure: Alcon Laboratories Consulting fee Consulting
Lance L Brown, OD, MD Ophthalmologist, Affiliated With Freeman Hospital and St John's Hospital, RegionalEye Center, Joplin, Missouri
Disclosure: Nothing to disclose.
Chief EditorHampton Roy Sr, MD Associate Clinical Professor, Department of Ophthalmology, University of Arkansas forMedical Sciences
Hampton Roy Sr, MD is a member of the following medical societies: American Academy of Ophthalmology,American College of Surgeons, and Pan-American Association of Ophthalmology
Disclosure: Nothing to disclose.
References
1. Boggs W. Possible That Early Treatment of Choroidal Melanoma Might Prevent Metastatic Death.Medscape Medical News. Available at http://www.medscape.com/viewarticle/822126. Accessed March25, 2014.
2. Damato BE, Heimann H, Kalirai H, Coupland SE. Age, Survival Predictors, and Metastatic Death inPatients With Choroidal Melanoma: Tentative Evidence of a Therapeutic Effect on Survival. JAMAOphthalmol. Mar 13 2014;[Medline].
3. Shields CL, Kaliki S, Furuta M, Shields JA. DIFFUSE VERSUS NONDIFFUSE SMALL (=3 MMTHICKNESS) CHOROIDAL MELANOMA: Comparative Analysis in 1,751 Cases. The 2012 F. PhinizyCalhoun Lecture. Retina. Apr 11 2013;[Medline].
4. Factors predictive of growth and treatment of small choroidal melanoma: COMS Report No. 5. TheCollaborative Ocular Melanoma Study Group. Arch Ophthalmol. Dec 1997;115(12):1537-44. [Medline].
5. Accuracy of diagnosis of choroidal melanomas in the Collaborative Ocular Melanoma Study. COMS reportno. 1. Arch Ophthalmol. Sep 1990;108(9):1268-73. [Medline].
6. Prescher G, Bornfeld N, Hirche H, Horsthemke B, Jöckel KH, Becher R. Prognostic implications ofmonosomy 3 in uveal melanoma. Lancet. May 4 1996;347(9010):1222-5. [Medline].
7. Histopathologic characteristics of uveal melanomas in eyes enucleated from the Collaborative OcularMelanoma Study. COMS report no. 6. Am J Ophthalmol. Jun 1998;125(6):745-66. [Medline].
8. The Collaborative Ocular Melanoma Study (COMS) randomized trial of pre-enucleation radiation of largechoroidal melanoma III: local complications and observations following enucleation COMS report no. 11.Am J Ophthalmol. Sep 1998;126(3):362-72. [Medline].
4/9/2014 Choroidal Melanoma
http://emedicine.medscape.com/article/1190564-overview#showall 17/17
Medscape Reference © 2011 WebMD, LLC
9. The Collaborative Ocular Melanoma Study (COMS) randomized trial of pre-enucleation radiation of largechoroidal melanoma II: initial mortality findings. COMS report no. 10. Am J Ophthalmol. Jun1998;125(6):779-96. [Medline].
10. Ten-year follow-up of fellow eyes of patients enrolled in Collaborative Ocular Melanoma Study randomizedtrials: COMS report no. 22. Ophthalmology. May 2004;111(5):966-76. [Medline].
11. Detorakis ET, Engstrom RE Jr, Wallace R, Straatsma BR. Iris and anterior chamber angleneovascularization after iodine 125 brachytherapy for uveal melanoma. Ophthalmology. Mar2005;112(3):505-10. [Medline].
12. Chang MY, McCannel TA. Local treatment failure after globe-conserving therapy for choroidal melanoma.Br J Ophthalmol. May 3 2013;[Medline].
13. Phillips C, Pope K, Hornby C, Chesson B, Cramb J, Bressel M. Novel 3D conformal technique fortreatment of choroidal melanoma with external beam photon radiotherapy. J Med Imaging Radiat Oncol.Apr 2013;57(2):230-6. [Medline].
14. Caminal JM, Mejia K, Masuet-Aumadell C, Arias L, Piulats JM, Gutierrez C, et al. Endoresection VersusIodine-125 Plaque Brachytherapy for the Treatment of Choroidal Melanoma. Am J Ophthalmol. May 132013;[Medline].
15. Mortality in patients with small choroidal melanoma. COMS report no. 4. The Collaborative OcularMelanoma Study Group. Arch Ophthalmol. Jul 1997;115(7):886-93. [Medline].
16. Boggs W. Palladium-103 radiation effective for small choroidal melanoma. Medscape Medical News [serialonline]. June 25, 2013;Accessed July 1, 2013. Available at http://www.medscape.com/viewarticle/806892.
17. Semenova E, Finger PT. Palladium-103 Radiation Therapy for Small Choroidal Melanoma. Ophthalmology.Jun 14 2013;[Medline].





![Ophthalmology Update - Cleveland Clinicchoroidal nevi prevalence and choroidal melanoma incidence. The results, published in Ophthalmol-ogy [Singh AD, et al. Ophthalmology 2005;112:1784-89],](https://img.pdfslide.us/doc/110x75/5ed991a01b54311e7967ce4b/ophthalmology-update-cleveland-clinic-choroidal-nevi-prevalence-and-choroidal.jpg)
![OPEN ACCESS Case Report Congenital Choroidal Nevus in a ...choroidal nevus) [10]; likewise, the nevus is characterized by having a high internal reflectivity, unlike the melanoma that](https://img.pdfslide.us/doc/110x75/5ea21f6a6c088018070115eb/open-access-case-report-congenital-choroidal-nevus-in-a-choroidal-nevus-10.jpg)