Embed Size (px)
Citation preview
Francesco Menichetti (Pisa, Italy)
Choosing antibiotics in difficult to treat staphylococcal infections
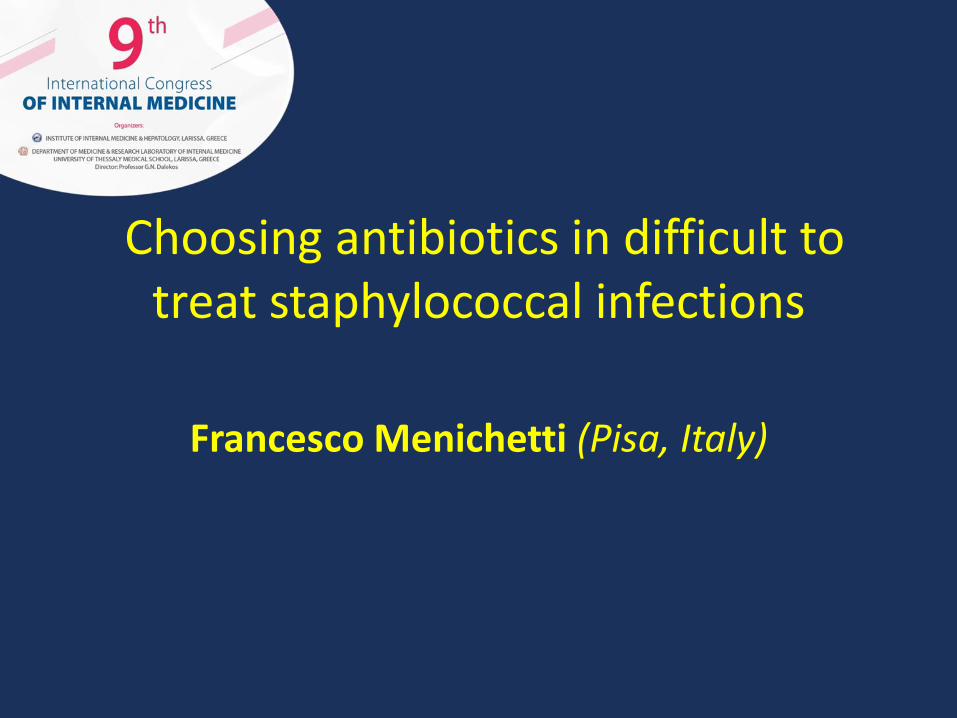
New anti gram-positives antibiotics
ABSSSI CAP HAP VAP note
CeftarolineZinforo
Astra Zeneca X X No VAP600 mg bid
CeftobiproleMabelio
Basilea X X No VAP500 mg bid
Telavancina *Vibativ
Astellas X X X Once-daily10 mg/KgNo IR
DalbavancinXydalba
Angelini X Once-weeklyIV 1500mg
OritavancinOrbactiv
The MedicinesCompany
X IV Single dose1200 mg
TedizolidSivextro
MSD X 200 mg IV/OSX 6 days
* When alternative treatment is not suitable
Review of new antibiotics
• Drug profile
• Personal experience
• Place in therapy today & tomorrow
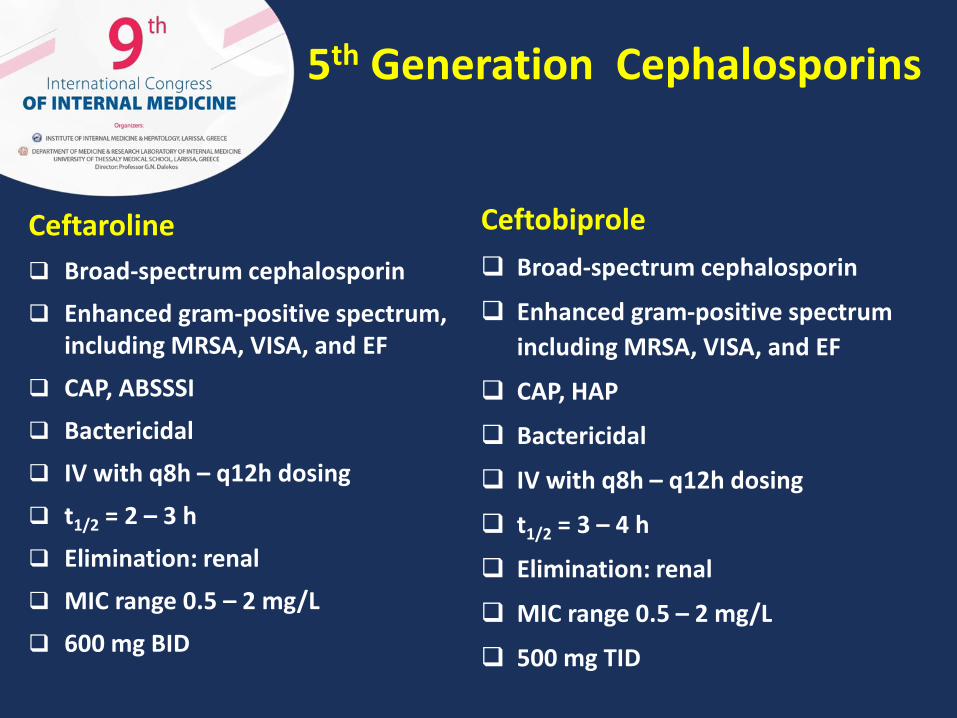
5th Generation Cephalosporins
Ceftobiprole
Broad-spectrum cephalosporin
Enhanced gram-positive spectrum
including MRSA, VISA, and EF
CAP, HAP
Bactericidal
IV with q8h – q12h dosing
t1/2 = 3 – 4 h
Elimination: renal
MIC range 0.5 – 2 mg/L
500 mg TID
Ceftaroline
Broad-spectrum cephalosporin
Enhanced gram-positive spectrum, including MRSA, VISA, and EF
CAP, ABSSSI
Bactericidal
IV with q8h – q12h dosing
t1/2 = 2 – 3 h
Elimination: renal
MIC range 0.5 – 2 mg/L
600 mg BID
Case 1: ceftaroline
• Male, 73 years-old
• HIV infection (2004), on Antiretroviral Therapy
• COPD (heavy smoker)
• Admitted for bilateral pneumonia
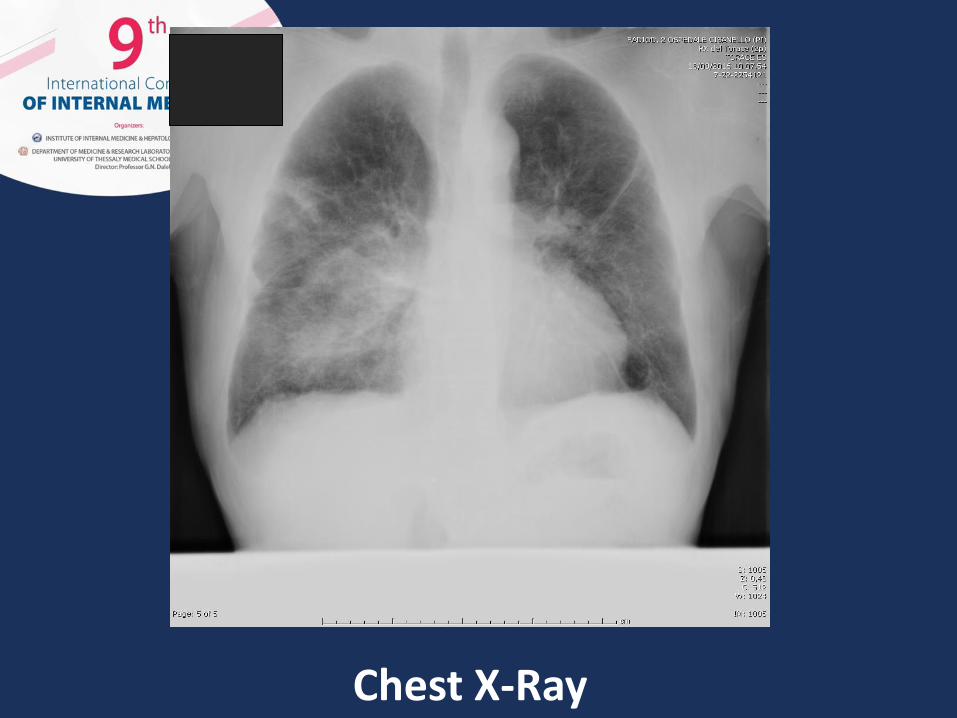
Chest X-Ray
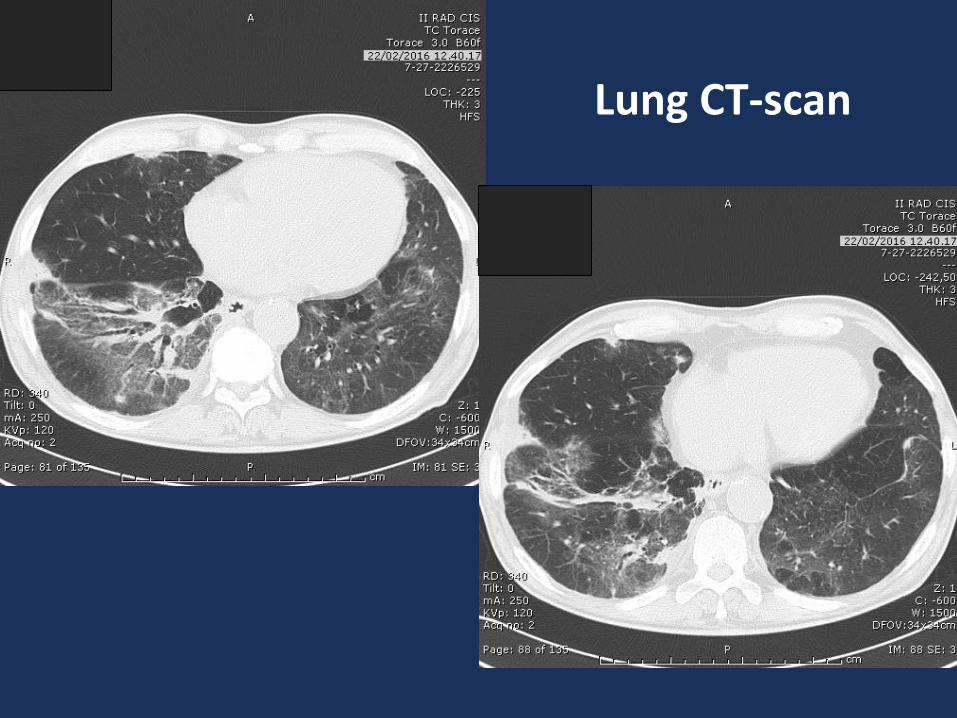
Lung CT-scan
MRSA bilateral pneumonia
• MRSA isolated from sputum & BAL
• MDR strain: Fluoroquinolone R, Gentamicin-R, Cotrimoxazole-R; susceptible to glycopeptideantibiotics, doxicicline, tygecicline, rifampin
• Ceftaroline MIC: 1 mg/ml (E-test)
MRSA bilateral pneumonia
• Ceftaroline 600 mg bid x 14 days,
• Favorable response
• C. difficile relapse: fidaxomicin
• Pathogen-directed therapy of CAP
Case 2: ceftobiprole
• Male, 93-years-old
• E. faecalis aortic valve endocarditis
• Spondylodiscitis L1/L2
• Treated with ampi/sulbactam plus daptomycin
• Bilateral nosocomial pneumonia
• No sputum, no BAL
• Urinary antigens (SP, LP): negatives
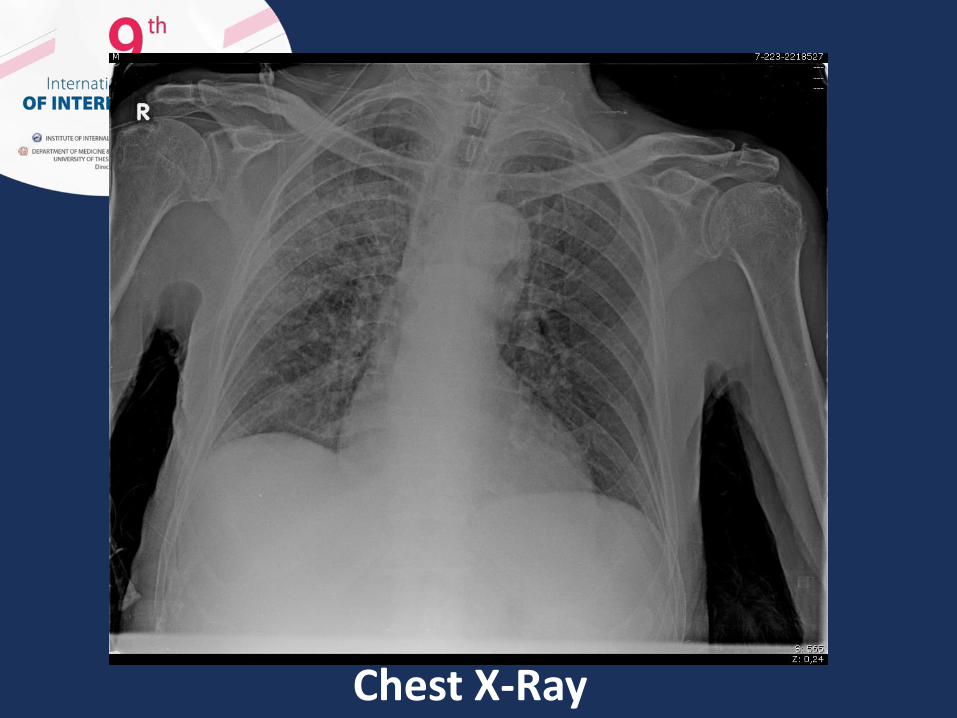
Chest X-Ray
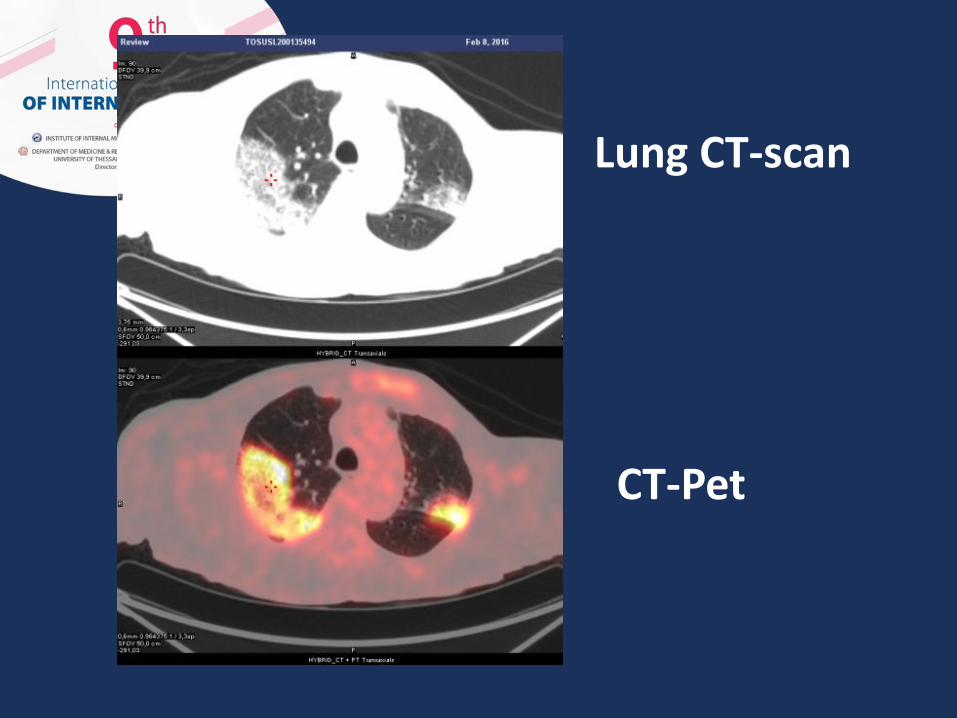
Lung CT-scan
CT-Pet
Case 2
• Ceftobiprole 500 mg tid x 21 days
• Patient improved, no toxicity
• Ceftobiprole combined with daptomycin wasthen continued for E. faecalis endocarditis
• Empiric therapy for nosocomial pneumonia
Case 3: ceftobiprole
• Male, 62 years-old
• Arterial hypertension, BPH
• Post surgical (removal of the nail) left foot ABSSSI
• Polimicrobial (MRSA+P.aeruginosa)
• MIC: MRSA 0.75 mg/l; P. aeruginosa: 2 mg/l

Case 3
• Previous antibiotic therapy
• Ceftobiprole 500 mg tid, 14 days
• No side effects
• Improved

Ceftobiprole monotherapy for nosocomial polimicrobial infection
(Off-label)
Ceftaroline/Ceftobiprole: overall personal impression
• Cephalosporins with anti-MRSA activity
• Ceftobiprole: activity against some gram-neg. rods(i.e.: P.aeruginosa)
• PK/PD, efficacy and safety of the class
• Good choice for CAP, HAP, ABSSSI with respect to combination antibiotic therapy
• Potentially useful, alone or in combo, for othersevere infections
Ceftaroline/Ceftobiprole: place in therapy today
Pneumonia
• CAP requiring hospitalization
• HAP (not VAP) ceftobiprole
ABSSSI
• ceftaroline
• Severe Infections (data required !!) due to MRSA, MSSA, (polimicrobial, ceftobiprole)
• Potentially useful for MRSA endocarditis, meningitis, bone infection, etc.
• Empiric monotherapy for pts with sepsis or febrileneutropenia (risk factors for MRSA)
• Not (alone) for ESBL-producers or carbapenemasegram-negative bugs
Ceftaroline/Ceftobiprole: place in therapy tomorrow
Why I consider/decide touse ceftaroline/ceftobiprole
• Monotherapy (in place of combo) for registeredindications (hospitalized CAP, HAP, ABSSI) especially(but not exclusively) for pts with MRSA risk factors
• Empiric, broad-spectrum, antibiotic therapy in ptswith sepsis syndrome (monotherapy or combo according to local epidemiology)
• Selected severe infections caused by susceptiblepathogens when a betalactam may be the preferredchoice
POTENTIAL COMPETITORS: LINEZOLID, DAPTOMYCIN,
TEICOPLANIN, VANCOMYCIN
Dalbavancin: a long-acting anti-gram-positive antibiotic for the treatment
of ABSSSI (and other severe infections)
Dalbavancin (Angelini)
• Activity vs most G+
• bactericidal
• Good PK profile (high concentrations, long half-life, low potential for interactions)
– 63% in bone similar to linezolid (60%)
• Good safety proflie
FDA approves Dalvance to treat skin infections QIDP; May 23, 2014
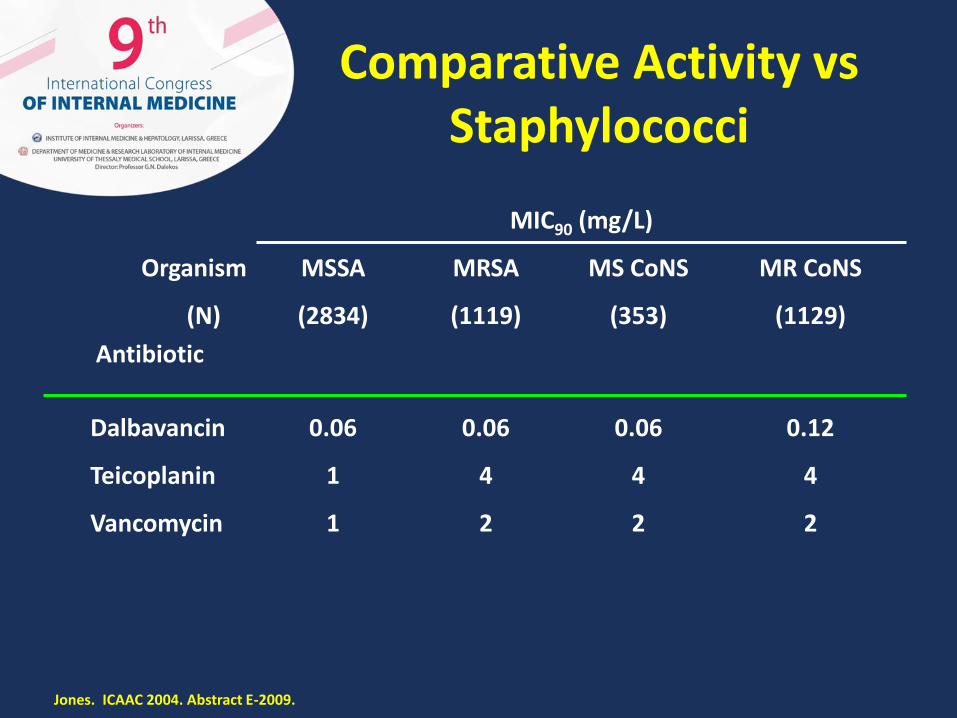
Comparative Activity vsStaphylococci
MIC90 (mg/L)
2221Vancomycin
4441Teicoplanin
0.120.060.060.06Dalbavancin
(1129)(353)(1119)(2834)(N)
Antibiotic
MR CoNSMS CoNSMRSAMSSAOrganism
Jones. ICAAC 2004. Abstract E-2009.
Personal experience
• Recurrent cellulitis (strepto, staphylo) in pts with post-surgical chronic arm lymphedema (i.e. mastectomy)
• Dalbavancin 1500 mg IV every 2/3 weeks for preventing recurrence
• A costly alternative to montly benzatin-penicillin
• Maximum-dose-limit ?
• Potential for decreasing the risk of recurrence i.e:. after 4-6 doses ??
• Prosthetic joint infections in place of chronicsuppressive oral/parenteral antibiotic therapy(linezolid, teicoplanin etc.)
• Need for defined etiology (MSSA/MRSA)
• Less pressure on gastrointestinal flora ?
• Less toxicity ?
• Chronic osteomyelitis: in place of daptomycin
Personal experience
De-escalation, step-down therapy
• Shifting from a glycopeptide/daptomycinantibiotic to complete/continue prolongedantibiotic course
• Selected case of MSSA/MRSA endocarditis, vascular prosthetic infection, vertebralosteomyelitis for an earlier discharge from hospital
Personal experience
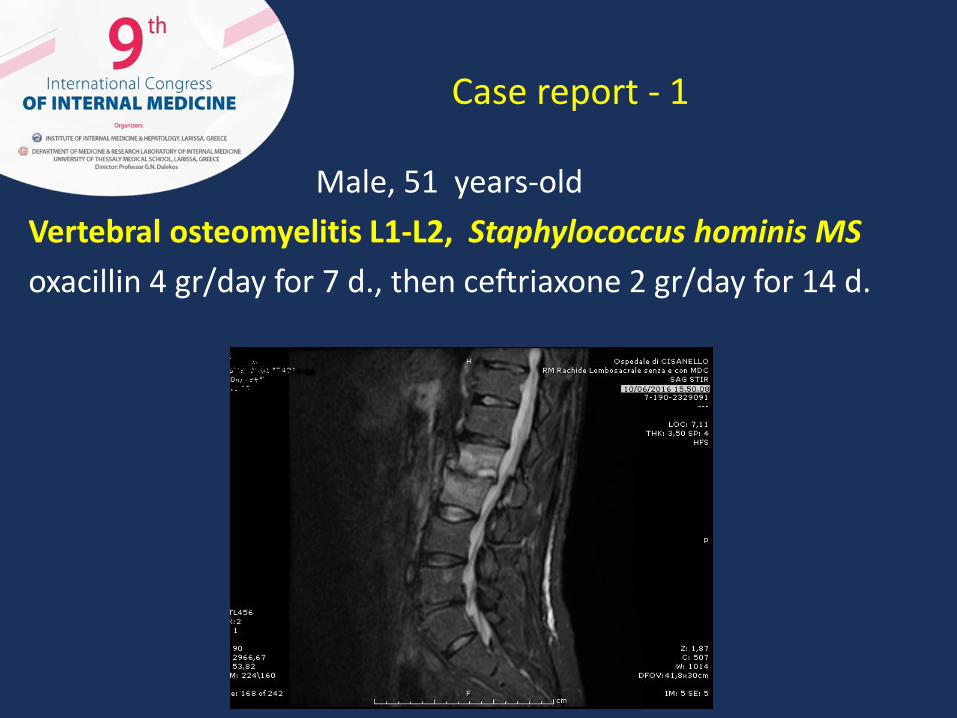
Case report - 1
Male, 51 years-old
Vertebral osteomyelitis L1-L2, Staphylococcus hominis MS
oxacillin 4 gr/day for 7 d., then ceftriaxone 2 gr/day for 14 d.
Case report - 1
• Need to discharge from hospital
• Need to complete 6 weeks of antibiotic therapy
• No vein acces (drug abuser)
• Dalbavancin 1500 mg every 15 d., three doses
• EOT: WBC 17300 6530/mmc; PCR 9,92 0,87 mg/dl
• No more pain, no more analgesic drugs
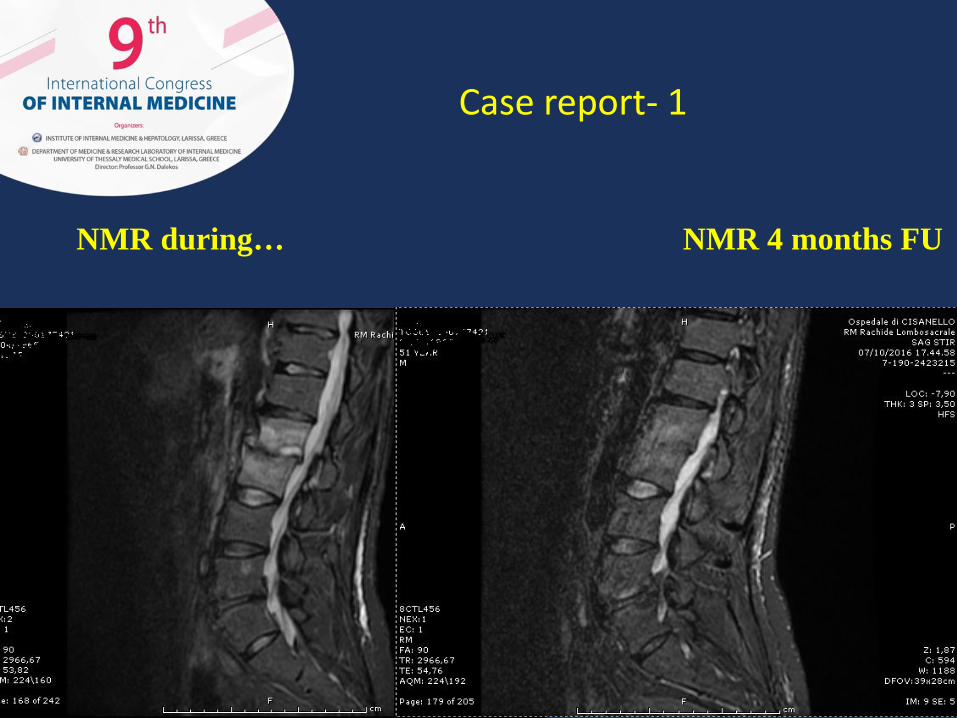
NMR during… NMR 4 months FU
Case report- 1
Male, 77 years-old
May 2016: low-grade fever, low-back pain
Aorto-bisiliac vascular prosthesis
Mild dementia, vascular enecephalophaty
September 2016 admitted to Vascular Surgery Unit
Mild increase of inflammation index
TTE: negative
Abdominal US: negative
Spine NMR …
Case report - 2

Spine NMR
Tonelli, GiuseppeTonelli, Giuseppe
E778F3DC-2B30-424B-9A95-AF0ADA399C7BE778F3DC-2B30-424B-9A95-AF0ADA399C7B
14/08/193914/08/1939
77 YEAR77 YEAR
MM
Page: 3 of 3Page: 3 of 3
Ospedale di Livorno Ospedale di Livorno
Scintigrafia globale corporea con cellule autologhe marcateScintigrafia globale corporea con cellule autologhe marcate
TC/SPET FUSIONTC/SPET FUSION
02/09/2016 15.00.0099FA247B-E58E-49E2-B650-D16D6843191399FA247B-E58E-49E2-B650-D16D68431913
------
------
------
IM: 0IM: 0
T: 256T: 256B: 0B: 0
Z: 0,62Z: 0,62
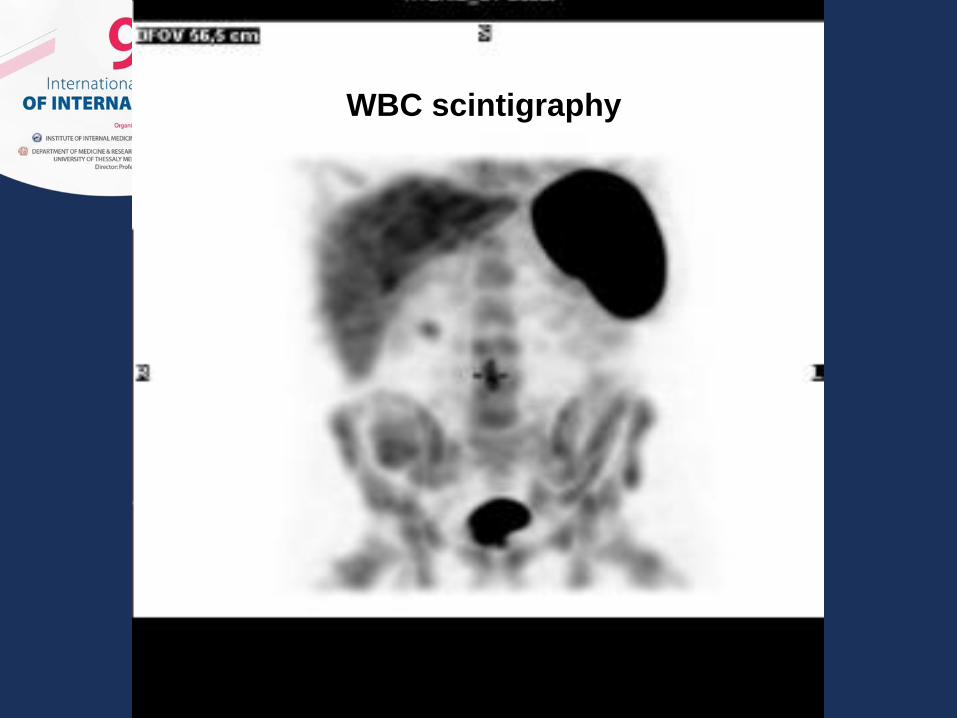
WBC scintigraphy
Case report 2
• Blood culture: MSSA
• Paravertebral needle aspirate: MSSA
• Vascular prosthesis MSSA infection with vertebral (L3-L4, L4-L5) and paravertebral tissue involvement
• High-risk for surgery: no prosthesis removal
• Long.term suppressive antibiotic therapy• Daptomycin + ceftaroline for 25 d.• Need to discharge, need to continue ATBT• Dalbavancin 1500 mg every 15 days for three doses…….
Dalbavancin: overall personal impression
• A lipo-glycopeptide with anti-MRSA activity
• PK/PD, efficacy and safety of the class
• Good choice for single shot therapy of ABSSSI with respect to prolonged treatment
• Advantage in terms of adherence, compliance, lenght of hospital stay
• Potentially useful, alone or in combo, for othersevere infections
Dalbavancin: overall personal impression
• A lipo-glycopeptide with anti-MRSA activity
• PK/PD, efficacy and safety of the class
• Good choice for single shot therapy of ABSSSI with respect to prolonged treatment
• Advantage in terms of adherence, compliance, long of hospital stay
• Potentially useful, alone or in combo, for othersevere infections

Dalbavancin: place in therapy today
ABSSSI
• Cellulitis
• Diabetic foot infection due to staphylococci
De-escalation, step-down therapy
• Shifting from a glycopeptide/daptomycin antibiotic to complete/continue prolonged antibiotic course
Situations warranting consideration for use of dalbavancin to treat ABSSSIs
• Pts necessitating IV therapy who are not candidates for indwelling intravenous catheters or with a history of intravenous catheter-related complications;
• Pts in whom deferment of hospital admission is planned;
• Pts requiring continuation of therapy at or after hospital discharge;
• Pts who are candidates for OPAT where home health or frequent infusion center visits are not feasible;
• Pts with a history or risk for non-compliance with oral therapy.

• Severe Infections (data required !!) due to MRSA, MSSA, other gram-positives
• Potentially useful for MRSA endocarditis, bacteremia, bone infection, etc.
• Empiric combo therapy for pts with sepsis or febrileneutropenia (risk factors for MRSA/streptococci)
Dalbavancin: place in therapy tomorrow
Type of infections
• ABSSSI: one-two shots!
– Erysipelas, cellulitis, abscess, skin ulces, nosocomial cellulitis
• CBSIs: empiric and targeted use
– One shot could be enough for CNS MR
• Bone and joint infections
• Endocarditis
Why I consider/decide to use Dalbavancin
• Monotherapy, for registered indications
• Empiric, broad-spectrum, antibiotic therapy in ptswith sepsis syndrome when an anti-gram-positive agent is required (combo according to localepidemiology)
• Selected severe infections caused by susceptiblepathogens when glycopeptide antibiotic or daptomycin may be the preferred choice
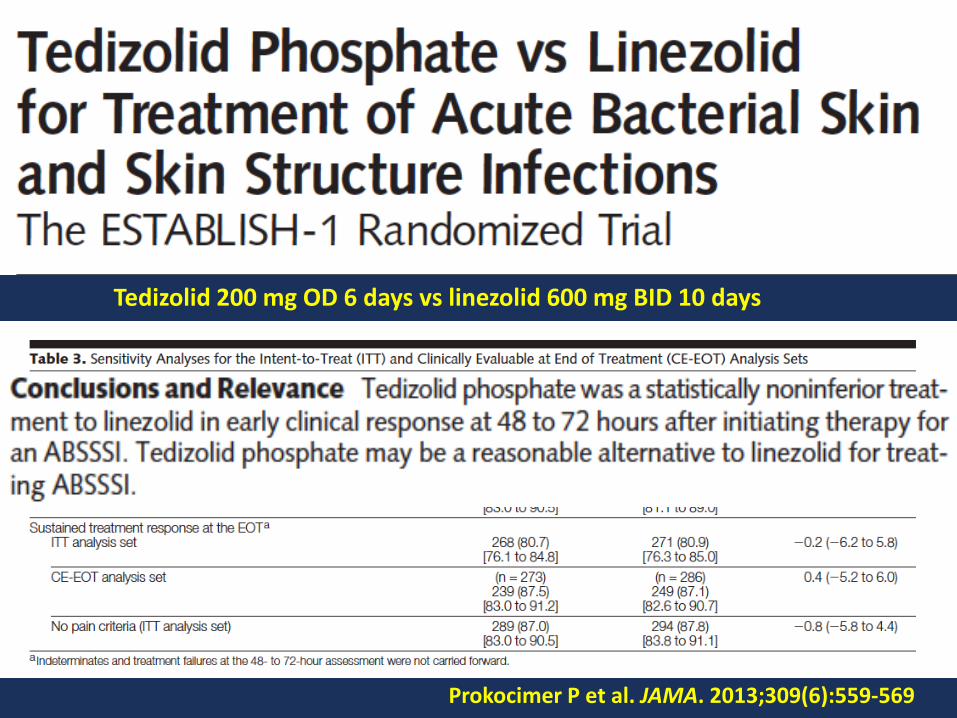
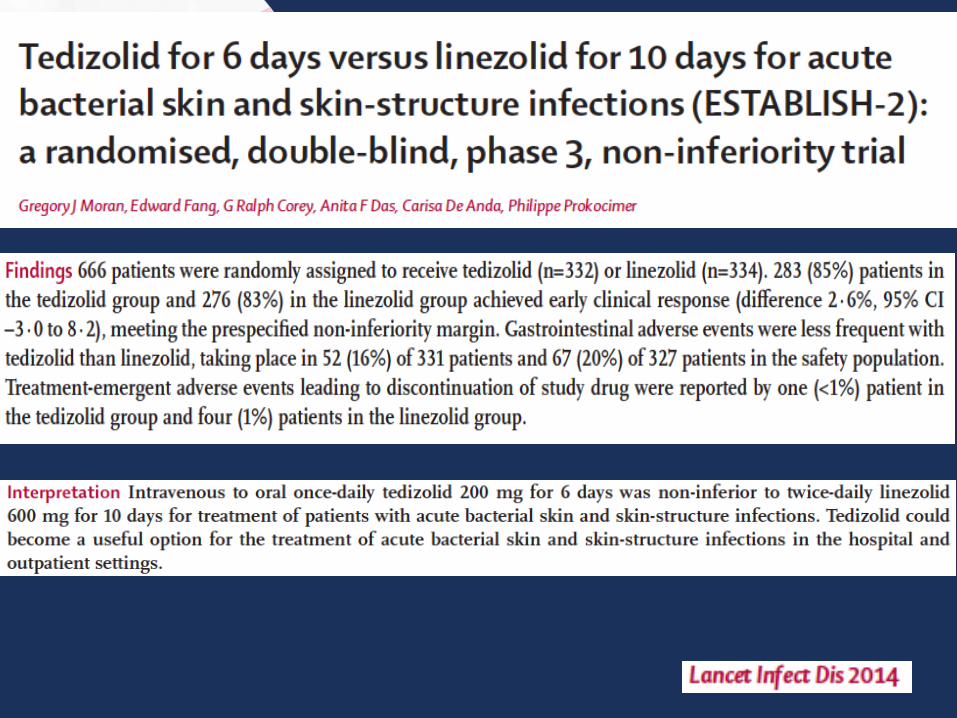
Tedizolid 200 mg OD 6 days vs linezolid 600 mg BID 10 days
Prokocimer P et al. JAMA. 2013;309(6):559-569
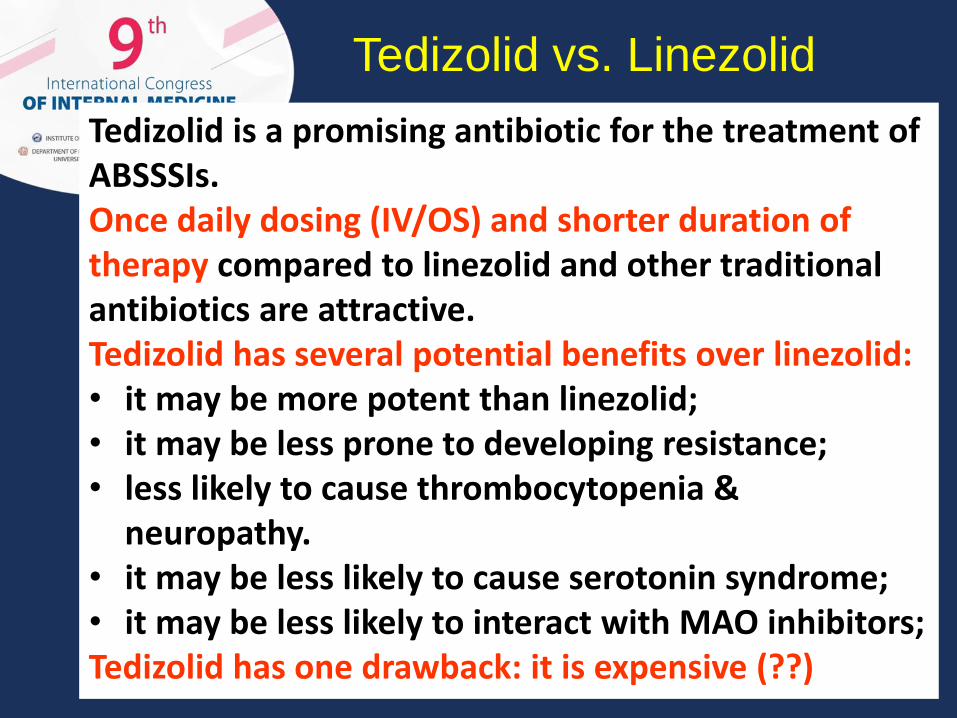
Tedizolid is a promising antibiotic for the treatment of ABSSSIs. Once daily dosing (IV/OS) and shorter duration of therapy compared to linezolid and other traditional antibiotics are attractive.Tedizolid has several potential benefits over linezolid:• it may be more potent than linezolid; • it may be less prone to developing resistance; • less likely to cause thrombocytopenia &
neuropathy.• it may be less likely to cause serotonin syndrome;• it may be less likely to interact with MAO inhibitors; Tedizolid has one drawback: it is expensive (??)
Tedizolid vs. Linezolid
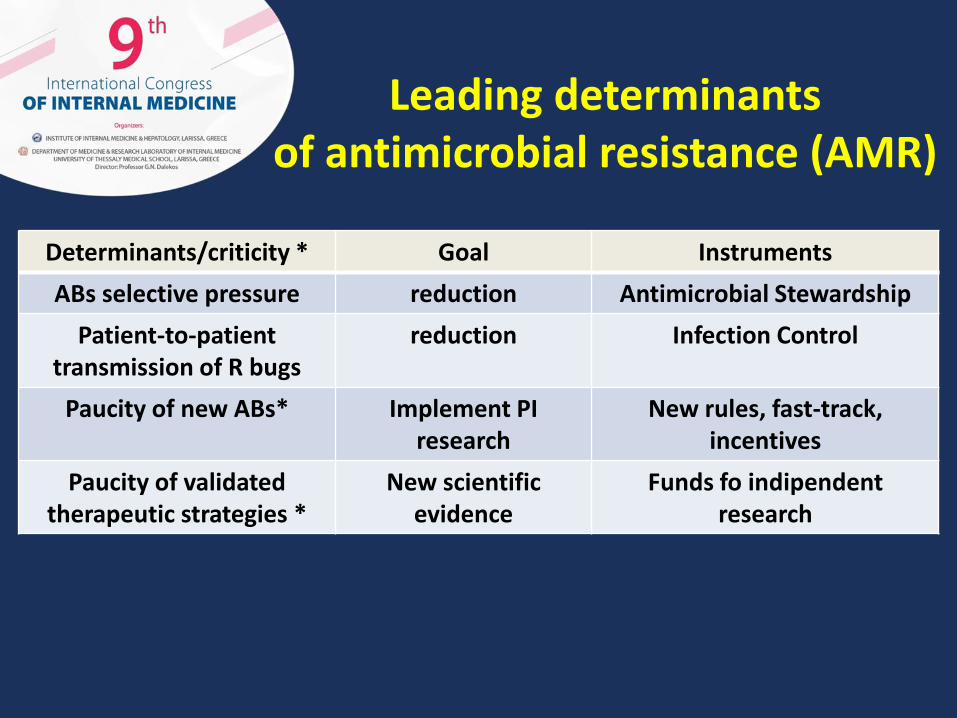
Leading determinantsof antimicrobial resistance (AMR)
Determinants/criticity * Goal Instruments
ABs selective pressure reduction Antimicrobial Stewardship
Patient-to-patienttransmission of R bugs
reduction Infection Control
Paucity of new ABs* Implement PI research
New rules, fast-track, incentives
Paucity of validatedtherapeutic strategies *
New scientificevidence
Funds fo indipendentresearch
The knowledge of new antibiotics:a clinician must !
• …..and a chance for the pts…….
• Curiosity, not indolent drug prescription !
• Evidence from registration RCT: insufficient
• Potential usefullness of personal experience
• Need to consider off-label use
• More independent clinical research