Embed Size (px)
Citation preview

www.elsevier.com/locate/jpedsurg
Journal of Pediatric Surgery (2007) 42, E19–E21
Choledocholithiasis in a 4-month-old infantMathew Thomas, Kavita Kadiwar, Bastian Domajnko, Mary Catherine Santos *
Division of Pediatric Surgery, University of Rochester Medical Center, Rochester, NY 14642, USA
⁎ Corresponding author. Tel.: +1 585 2E-mail address: [email protected]
0022-3468/$ – see front matter © 2007doi:10.1016/j.jpedsurg.2007.03.056
Abstract Cholelithiasis is increasingly being diagnosed in newborns and infants because of the morefrequent use of abdominal ultrasound. However, common bile duct stones causing obstruction orsymptoms in infancy are exceedingly rare and are not often reported in the literature. We report thesuccessful treatment of symptomatic choledocholithiasis in a 4-month-old patient with endoscopicretrograde cholangiopancreatography and endoscopic sphincterotomy.© 2007 Elsevier Inc. All rights reserved.
Index words:
Cholelithiasis;Choledocholithiasis;Endoscopicsphincterotomy
Choledocholithiasis in infants has rarely been reportedin the literature and its management is controversial. Theetiology of stones in the gallbladder or the bile ducts hasbeen attributed to prematurity, congenital heart disease,previous gastrointestinal surgery, and total parenteralnutrition. We describe the successful treatment of a4-month-old male infant with choledocholithiasis usingendoscopic retrograde cholangiopancreatography (ERCP)and endoscopic sphincterotomy (EST). The etiology in thiscase appeared to be resorption of a cephalohematomasustained at birth.
1. Case report
A 4-month-old male infant weighing 7.58 kg presentedwith a 2-week history of intermittent pale stools andjaundice. The infant was born at 40 weeks gestation byvacuum cesarean delivery that resulted in a cephalohema-toma. At birth, the patient was noted to have an indirecthyperbilirubinemia and received 4 days of phototherapy fortreatment of his jaundice. On admission, the patient was
73 1753.chester.edu (M.C. Santos).
Elsevier Inc. All rights reserved.
afebrile with age-appropriate vital signs. On physical exam-ination, the patient was active, appeared jaundiced, and had anontender, nondistended abdomen. The liver was palpableapproximately 2 cm below the costal margin. The remainderof the examination was unremarkable. Laboratory data showedthe following serum levels: total bilirubin, 8.1 mg/dL; directbilirubin, 6.0 mg/dL; aspartate aminotransferase (AST), 151 U/L; alanine aminotransferase (ALT), 165 U/L; alkalinephosphatase, 641 U/L; and gamma glutamyl transpeptidase(GGT), 1309 U/L; amylase, 38 U/L; and lipase, 17 U/L.
An ultrasound of the abdomen showed a distendedgallbladder with sludge and a calculus in the common bileduct (CBD) measuring approximately 9 mm in the long axis.The CBD was dilated at 4.7 mm. There was no intrahepaticor pancreatic ductal dilation but the distal duct was notvisualized. Magnetic resonance cholangiopancreatographyrevealed a round filling defect representing an obstructing4 mm stone just proximal to the ampulla of Vater.
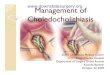
Endoscopic retrograde cholangiopancreatography wasperformed on the third day after admission (Fig. 1A, B);however, endoscopic extraction of the stone was unsuccess-ful because of the inability to maneuver the wire past theobstructing calculus (Fig. 2). A sphincterotomy wasperformed. Transient postprocedure elevation in amylaseand lipase were noted and the patient remained stablewithout clinical evidence of pancreatitis. The patient was

Fig. 1 (A, B) Serial magnetic resonance cholangiopancreato-graphy images showing abrupt cutoff of signal intensity along thedistal CBD (white arrows), consistent with an obstructing stone.
ig. 2 Endoscopic retrograde cholangiopancreatography imageshowing a filling defect suggestive of a CBD stone (arrow).
E20 M. Thomas et al.
observed for 3 more days to allow resolution of sphincteredema. Endoscopic retrograde cholangiopancreatographywas then repeated, this time with successful extraction of afriable, black-pigment stone from the CBD. Sludge was alsoremoved after dilation of the duct by using a balloonangiocatheter. Normalization of liver function tests wasnoted and the patient was discharged home 3 days after theprocedure with oral antibiotics. At 2-month follow-up, thechild was doing well. A repeat ultrasound showed normalresults: there were no gallstones, and the CBD was measuredat 1.5 mm.
2. Discussion
The incidence of cholelithiasis in infants has been on therise with the increased use of ultrasound for prenatal andpostnatal imaging. However, symptomatic choledocholithia-sis in infancy remains a rare entity. Overall, 0.15% to 0.22%of children develop gallstones, and 11% to 13% of childrenwith gallstone disease have CBD stones [1,2]. Freisen andRoberts [3] studied 693 children with symptomatic chole-lithiasis and found 41 children younger than 6 months tohave CBD stones.
Known risk factors for gallstone disease in childreninclude prematurity, total parenteral nutrition, use ofcertain medications (eg, furosemide, ceftriaxone), hemo-lytic disorders, and biliary tract disorders. Dehydrationand urinary tract infection have also been associated withgallstones in children [4]. In the study of Friesen andRoberts [3], the etiology of gallstones in infants between0 and 6 months included idiopathic causes (36.4%), totalparenteral nutrition (30%), abdominal surgery (30%),sepsis (15%), bronchopulmonary dysplasia (13%), hemo-lytic disease (5.5%), malabsorption (5.5%), necrotizingenterocolitis (5.5%), and hepatobiliary disease (3.6%).Gallstones in children are usually pigment stonesconsisting of calcium bilirubinate and are either blackor brown in color [3,5,6].
Because of the lack of systematic studies, the optimaltreatment of choledocholithasis in infants remains contro-versial. This may well be attributable to the exceedingly lownumber of reported cases in the literature. However,conservative management of asymptomatic neonatal andinfantile cholelithiasis has been shown to result in sponta-neous resolution with ranges from 20% to 80% of reportedcases [1,5-8]. Although 28% of cases of obstructive jaundice
F

E21Choledocholithiasis in a 4-month-old infant
attributable to CBD stones may resolve spontaneously,intervention is usually indicated in the symptomatic patient[9]. Treatment strategies for CBD stones in children includeopen cholecystectomy and CBD exploration, laparoscopiccholecystectomy combined with preoperative or postopera-tive ERCP and stone extraction, or laparoscopic cholecys-tectomy and laparoscopic CBD exploration [2,10,11].Almost all reported cases of symptomatic choledocholithia-sis in children required cholecystectomy.
Endoscopic sphincterotomy was first reported in 1974and since then has become popular in the management ofcholedocholithiasis in adults. Few case reports of theapplication of ERCP and EST in children are available.Most infants with complicated gallstone disease undergooperative management because of the feared complica-tions of ERCP and sphincterotomy, particularly in thisage group. Complication rates of ERCP in children andadults vary widely depending on the defining criteria forpancreatitis, especially the threshold of serum amylaselevels. In children, overall complications have beenreported from 8% to 11.6% in larger series studies, andinclude mostly pancreatitis (3%-8%), perforation (up to8%), and hemorrhage (up to 2.0%) [12-14]. In compar-ison, adult complication rates of 3% to 7% for all ERCPprocedures and up to 9.8% after therapeutic procedureshave been reported [15,16]. In expert hands, theprocedure may be safely performed in children. Theyoungest patient to undergo successful EST and extrac-tion of common duct stones reported in the literature is 8weeks old [17].
The case presented here represents 1 of the few reportsof successful EST and stone extraction in an infantyounger than 6 months of age. We pursued a nonoperativeapproach in this patient because the formation of gallstonesappeared to be caused by the resorption of a cephalohe-matoma sustained at birth. From our experience, wesuggest that the judicial use of ERCP and EST in experthands may be safely used for the management ofsymptomatic choledocholithasis in infants although longerfollow-up may be necessary.
References
[1] Vrochides DV, Sorrells DL, Kurkchubasche AG, et al. Is there a rolefor routine preoperative endoscopic retrograde cholangiopancreato-graphy for suspected choledocholithiasis in children? Arch Surg2005;140(4):359-61.
[2] Newman KD, Powell DM, Holcomb III GW. The management ofcholedocholithiasis in children in the era of laparoscopic cholecys-tectomy. J Pediatr Surg 1997;32:1116-9.
[3] Friesen CA, Roberts CC. Cholelithiasis: clinical characteristics inchildren. Case analysis and literature review. Clin Pediatr 1989;28:294-8.
[4] Klar A, Branski D, Akerman Y, et al. Sludge ball, pseudolithiasis,cholelithiasis and choledocholithiasis from intrauterine life to 2 years:a 13-year follow-up. J Pediatr Gastroenterol Nutr 2005;40:477-80.
[5] Allen B, Bernhoft R, Blanckaert N, et al. Sludge is calcium bilirubinateassociated with bile stasis. Am J Surg 1981;141:51-6.
[6] Stringer MD, Taylor DR, Soloway RD. Gallstone composition; arechildren different? J Pediatr 2003;142:435-40.
[7] Muller H, Greiner P, Brandis M. Gallstones in infancy. MonatsschrKinderheil 1994;142:603-8.
[8] Keller MS, Markle BM. Spontaneous resolution of cholelithiasis ininfants. Radiology 1985;157:345-8.
[9] Rowe MI, O'Neill JA, Grosfield JL, et al. Essentials of pediatricsurgery. St Louis, MO: Mosby Year-Book; 1995.
[10] Guelrud M, Mendoza S, Jaen D, et al. Endoscopic retrogradecholangiopancreatography and endoscopic sphincterotomy in infantsand children with jaundice due to common bile duct stones.Gastrointest Endosc 1992;38:450-3.
[11] Sanada Y, Yamaguchi M, Chiba M, et al. Endoscopic sphincterotomyand laparoscopic cholecystectomy in an infant with cholecysto-choledocholithiasis. J Pediatr Surg 1998;33(8):1312-4.
[12] Fox VL, Werlin SL, Heyman MB. Endoscopic retrograde cholangio-pancreatography in children. J Pediatr Gastroenterol Nutr 2000;30(3):335-42.
[13] Brown CW, Werlin SL, Geenen JE, et al. The diagnostic andtherapeutic role of endoscopic retrograde cholangiopancreatography inchildren. J Pediatr Gastroenterol Nutr 1993;17:19-23.
[14] Buckley A, Connon J. The role of ERCP in children and adolescents.Gastrointest Endosc 1990;36:369-72.
[15] Aliperti G. Complications related to diagnostic and therapeuticendoscopic retrograde cholangiopancreatography. Gastrointest EndoscClin N Am 1996;6:379-407.
[16] Freeman ML, Nelson DB, Sherman S, et al. Complications ofendoscopic biliary sphincterotomy. N Engl J Med 1996;335:909-18.
[17] Wilkinson ML, Clayton PT. Sphincterotomy for jaundice in a neonate.J Pediatr Gastroenterol Nutr 1996;23(4):507-9.