-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
1/57
I I N T R O D U C T I O N
Description of the Disease
The gallbladder is a small pear-shaped organ which aids in the
digestive
process. Its function is to store and concentrate bile - a
digestive liquid continually
secreted by the liver. The bile in turn emulsies fats and
neutralizes acids in partly
digested food. Despite its importance in the digestion of fat,
many people are
unaware of their gallbladder. ortunately enough, the gallbladder
is an organ that
people can live without. !erhaps, this fact contributes to the
la"ity of the ma#ority.
The gallbladder tends to be ta$en for granted % ignored of the
proper care and
conditioning. &ifestyle together with heredity, se", race
and age are #ust some
factors that leave a room for gallbladder complications to
occur.
's dened, cholecystitis is the in(ammation of the gall bladder.
It came from
the gree$ word )cholecyst* which means )gallbladder* and the
su+" )itis* which
means in(ammation. The in(ammation occurs mainly because of an
obstruction of
the cystic duct by a stone. loc$age of the cystic ductwith
gallstonescauses
accumulation of bile in the gallbladderand increased pressure
within the
gallbladder. oncentrated bile, pressure, and sometimes bacterial
infection irritate
and damage the gallbladder wall, causing in(ammation and
swelling of the
gallbladder. In(ammation and swelling of the gallbladder can
reduce normal blood
(ow to areas of the gallbladder, which can lead to cell death
due to insu+cient
o"ygen. ot everyone who has gallstones will go on to develop
cholecystitis. !eople
with history of gallstones are at high ris$ for having
cholecystitis, as well as those
who are obese and those with sedentary lifestyle. The most
common presenting
symptom of cholecystitis is upper abdominal pain. /owever, this
may appear
asymptomatic, initially. !hysical e"aminations may reveal fever,
tachycardia, and
tenderness in the 012 or epigastric region, often with guarding
behaviour.
Recent Trends, Innovations, and/ or Renements in Treatment
Robotic Scarless Gallbladder Sr!er" # ScienceDail" $Dec%
&&, '(&') *+
3assar 3oussef, 4.D., is the rst surgeon in altimore ity to
perform gallbladder
surgery using #ust one incision and the da 5inci 6urgical
6ystem. ecause the single
7 8 ! a g e
http://en.wikipedia.org/wiki/Cystic_ducthttp://en.wikipedia.org/wiki/Gallstoneshttp://en.wikipedia.org/wiki/Gallbladderhttp://en.wikipedia.org/wiki/Gallstoneshttp://en.wikipedia.org/wiki/Gallbladderhttp://en.wikipedia.org/wiki/Cystic_duct
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
2/57
incision of about an inch is made in the patient9s navel, he or
she is left without a
noticeable scar. 'dditional patient benets are less pain, less
blood loss and a faster
recovery compared even with minimally invasive gallbladder
removal that requires
multiple incisions. This is good news for the one million
'mericans who need theirgallbladders removed each year, most of
whom are candidates for this single-site,
robotic approach.
4ore than any other hospital in 4aryland, 6inai /ospital has
made technologic
investments in its da 5inci 6urgical 6ystem: in addition to
having da 5inci 6ingle-6ite
instruments that enable 3oussef to perform gallbladder removal,
the hospital has
two da 5inci units, an e"tra console allowing two surgeons to
operate in tandem on
a patient, and other advanced instruments. 6inai9s sister
hospital, orthwest, alsohas its own da 5inci 6urgical 6ystem.
3oussef has plans to train other surgeons on
the da 5inci, including those in 6inai9s surgical residency
program. 6inai /ospital is a
part of &iferidge /ealth, one of the largest, most
comprehensive providers of
health services in northwest altimore. &iferidge /ealth also
includes orthwest
/ospital, &evindale /ebrew ;eriatric enter and /ospital,
ourtland ;ardens
ursing < 0ehabilitation enter, and related subsidiaries and
a+liates.
Statistics $ocal - International)
'bout 7=->=? of 'mericans have gallstones, and as many as one
third of
these people develop cholecystitis. @n the other hand, Indian
and 6candinavian
people have the highest prevalence of cholecystitis, it aAected
>=.B million people
with a record of appro"imately C,=== deaths in >=7>.
/ospitalizations total up to
E,=== in the same year and over B==,=== have undergone
cholecystectomies.
In the !hilippines alone, B, =CE, =F= people are aAected by the
disease last >=77.
;enerally, the incidence of cholecystitis increases with age and
it is >-E times more
frequent in females than in males.
Ob.ectives of the Std"
% General Ob.ective
> 8 ! a g e
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
3/57
'fter the entire hospital rotation at 0afael &azatin
4emorial 4edical /ospital, the
student nurses will be able toG
Hnow and understand the disease process and concept of
holecystitis.
0% Specic Ob.ectives
'fter the entire hospital rotation at 0afael &azatin
4emorial 4edical /ospital, the
student nurses will be able toG
Co!nitive 0eview the !roper !hysical 'ssessment I!!'J and how to
do them e+ciently:
1nderstand the Disease !rocessG the causes, eAects,
management, treatment, and possible preventions:
Determine the !athophysiology of the condition with their
rationale for
occurrence of each manifestation:
Determine why certain management and medications are given and
provided
for the condition:
1nderstand how and why certain diagnostic tests are done for the
condition,
and
0eview the concepts about the 'natomy and !hysiology with
regards to thedisease condition.
1s"chomotor
!erform proper physical assessment I!!'J to the patient
e+ciently:
!erform thorough health history from patient and signicant
others:
!articipate in the course of care of patient:
!rovide health teachings to the patient about certain
interventions in the
maintenance of healthcare.
2ective
E 8 ! a g e
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
4/57
Kstablish rapport and therapeutic interaction with the patient
and signicant
others to obtain necessary information and positive compliance
to care being
provided:
!rovide care and health teachings necessary for the betterment
of the
condition of the patient.
6hare the learning acquired to co-student-nurses to increase
awareness and
help them if ever they will encounter patient with the same
condition.
I% N U R S I N G 3 I S T O R 4
0io!raphic Data
This is a case of a F years old ilipino named 4r. aguit who was
born on the
>Cth day of ebruary 7LC. /e is currently living at 'ngeles
ity. The client is
married and has si" children and one grandchild all of which
lives under the same
roof with him and his wife. The clientMs main language for
communication is
Hapampangan but he also $nows how to spea$ Tagalog and Knglish
as well.
's stated by the patient, he e"perienced dizziness and an
intolerable sharp
stabbing pain in his abdominal area on the day of his
hospitalization which made
him decide to go to the hospital. /e was brought by his wife and
was admitted at
@spital ing 'ngeles last ovember 7L,>=7E at CGFBpm with the
diagnosis of
)holecystitis: 'nemia to be considered* under the care of the
admitting physician
Dr. ala#adia.
1ast 5edical 3istor"
During the one on one interview of the student nurse with the
client, the
client stated that he has complete immunization as child and had
e"perienced only
F 8 ! a g e
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
5/57
a couple of minor illnesses for the past years such as cough,
common colds, and
fever.
The patient had no record of previous hospitalizations and that
this was his
rst time to be conned in a hospital. 'lthough on the year of
>==N, he had
e"perienced an accident wherein he fell down from the stairs in
the ;rotto in
amban, Tarlac which gave him a sprain in his left foot but the
client said that it was
not that serious and did not required hospitalization.
ifest"le
@ur client usually wa$es up at BG== in the morning so as to help
his wife
prepare his children to go to school, after which he gets ready
to go to wor$ as well.
/e wor$s N hours a day as a driver of dump truc$s under the
management of the
government. /e wal$s to and from his wor$ which basically
becomes his daily form
of e"ercise. The patient eats E times a day, brea$fast, lunch
and dinner respectively,
and he mentioned that he loves to eat food high in cholesterol
such as ried !or$,
and hicharon. /e said that he is not pic$y when it comes to food
but he en#oys
eating and get to eat a lot when heMs eating fatty foods because
it gives the food
more (avor and ma$es it savory.
/e has no vices, although he used to smo$e and drin$, according
to him he
decided to stop smo$ing ve months ago and was able to continue
that change until
now. 's for his alcohol consumption, the client said that he
only drin$s alcoholic
beverages during special occasions but in light to moderate
consumption only. @ne
of his ways to manage stress is to play with his grandchild,who
for the client, gives
#oy to the whole family and brighten up everyoneMs day in the
aguitMs residence.
1resent 3istor" of Illness
Chief Complaint6 Di77iness and bdominal 1ain on the RU8
' month prior to admission, 4r. aguit e"perienced right upper
quadrant pain
associated with a sense of bloatedness and dizziness. The pain
was tolerable so he
B 8 ! a g e
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
6/57
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
7/57
7&, at the level of B== cc, H5@, infusing well at his left
hand. !atient was on !@ and
complains of pain, with a pain scale of CQ7=. !atient was in
good grooming wearing
white shirt and maong pants.
5ital 6igns ta$en are as followsG
S=in6
6$in was warm to touch, sli!htl" dr", ro!h,and with good s$in
turgor.
either #aundice nor cyanosis observed. o bruises or
discolorations
observed. o edema noted.
3ead6
6$ull and face were symmetrical with an equal distribution of
hair. /air was
blac$ in color. There was no dandruA or infestation present. o
lesions,
lacerations, tenderness, masses and depressions noted.
:"es6
The client has straight normal eye condition: >ith sli!ht
icteric sclera.
!upil is brown in color and equal in size: reactive to light and
accomodation.
/ave thin eyebrows.
:ars6
6$in color is same as facial s$in, auricle aligned with outer
canthus of eye,
mobile, rm, and not tender: pinna recoils after it is folded:
presence of
cermen noted%
NoseG
C 8 ! a g e
9INDINGS I51R:SSION
0OOD 1R:SSUR: 7>=QN=
mm/g
ormal
1US: RT: CL bpm ormal
R:S1IRTOR4 RT: 7 cpm ormal
T:51:RTUR: EC.7 R
Qa"illa
ormal
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
8/57
ose is uniform in color and has sli!ht dischar!es: there are no
masses or
tenderness upon palpation.
5oth and Throat6
&ips are pale: tongue is at the center and has no discharge:
@ral cavity has
no sores and lesions.
Nec=
ec$ was symmetrical with no masses or swelling noted. o #ugular
vein
distention was noted. 0ange of motion was normal and moves
easily without
discomfort upon rotation, (e"ion, e"tension and
hypere"tension.
Thora? and n!s6
0espiratory rate was 7 cycles per minute with regular breathing
pattern.
6ymmetrical chest e"pansion was observed during respiration. o
use of
accessory muscles during breathing observed. hest wall was
intact: no
tenderness and masses noted. 1niform temperature also noted.
o
adventitious breath sounds heard upon auscultation. o cough
present. o
dyspnea, hemoptysis, hiccups noted.
bdomen6
bdomen >as sli!ht" enlar!ed and !loblarwhen patient was in
supine
position. Tenderness noted on the ri!ht pper @adrant >hen
palpated%
GenitoA Urinar"6
1nable to perform inspection in the genitourinary region.
/owever, patient
verbalized that he had not seen any discharges from her
genitalia nor
presence of papules or ulcerations. The patient voided with a
yellow colored
urine.
0ac= - :?tremities6
N 8 ! a g e
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
9/57
6ymmetrical shoulder movement observed during respiration. 6pine
was
located at the midline with no discrepancies noted. 6houlders,
arms, elbows
and forearms were free from nodules and deformities. 1pper
e"tremities were
not edematous. 0adial and brachial pulses were present. /ip
#oint and thighswere symmetrical with no deformities present. o
edema noted at both legs.
o in(ammation noted in the lower e"tremities
L 8 ! a g e
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
10/57
IB% D I G N O S T I C S N D 0 O R T O R 4 R : S U T S
Dia!nostic/aborator"procedres
Dateordered/
Datereslt$s)
in6
Indication$s)
or1rpose$s)
Reslt
Normalvale$nits
sed inthe
hospital)
nal"sisand
Interpretation of
Reslts
3emo!lobin
D@G 77-7C-7ED0G 77-7C-
7E
D@G 77->=-7ED0G 77->=-
7E
To measureprotein usedby red blood
cell todistributeo"ygen tothe othertissue andcell in thebody
NC
E
7F=-7N=gmQ&
There is lowhgb level.The patient is
possible tohave anemia.This indicatesthat thepatient haspoor
blood9sability tocarry o"ygenthroughouthis body.
3ematocrit D@G 77-7C-7ED0G 77-7C-7E
D@G 77->=-7ED0G 77->=-7E
To measurethe amountof blood thatis occupiedby the redblood
cell
=.>
=.7L
=.F=-=.BF&Q&
There is lowhct level.This meansthat there isinsu+cientblood
volumecomposed of0s, which
are theresponsiblefor carryingo"ygen in thebody.
7= 8 ! a g e
/K4'T@&@;3
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
11/57
R0C cont D@G 77-7C-7ED0G 77-7C-7E
D@G 77->=-7ED0G 77->=-7E
To measurethe numberof red bloodcells pervolume of
blood anddeterminefor presenceofpolycythemia,dehydration,and
anemia.
E.=E
>.>7
F.B-.E"7=7>Q&
Decreasedlevel of 0may indicatepresence ofanemia.
Decreasedlevel of 0may indicatepresence ofanemia.
0C ContD@G 77-7C-7ED0G 77-7C-7E
D@G 77->=-7ED0G 77->=-7E
To determineinfectionQin(ammation< also todetermineand
evaluatethe bodyMsphysiologiccapacity toresist
andovercomeinfection.
7B.=
7>.
B-7= "7=Q&
The elevatedvalue of theOs isindicative ofa
bacterialinfectionwhich maybe due to thein(amedgallbladder.
NetrophilsD@G 77-7C-7ED0G 77-7C-7E
To determinepossiblepresence ofinfectionsand tissuenecrosis
=.N7
=.C
.F=-CF? eutrophillevel is abovenormalrange. Itcouldsuggest
thatthere is apresence ofviralinfection,tissuenecrosis,
77 8 ! a g e
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
12/57
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
13/57
is in thenormal rangethis meansthat thereare lesschances of
developinghemorrhage.
0lood T"pe D@G 77->=-7ED0G 77->=-7E
' bloodtype is usedto classifybloodbasedon thepresence orabsence
ofinheritedantigenic6ubstanceson thesurfaceof red
bloodcells0sJ.
Type )'*0/ DJG!ositive
!atientMsblood type istype ', 0/positive.
Nrsin! Responsibilities
efore During 'fter
Chec= for the specic
test ordered b" thedoctor%:?plain the test and >h"is it
needed%
Knsure that the blood
sample is not ta$en from avein in the hand or armwith an
intravenous line./emodilution withintravenous or plasma willlower
the hematocrit valuefalsely.
Instruct the 6@ to apply
pressure to the puncturesite until bleeding stops.'ssess for
hematomaformation.Document the testperformed
:?plain to the patientthat it is normal for thepatient to feel
pain and
some discomforts >hileperformin! theprocedre%
:?plain to the client thatan amont of blood >illbe e?tracted
from thebrachial arm%
7E 8 ! a g e
http://en.wikipedia.org/wiki/Bloodhttp://en.wikipedia.org/wiki/Heredityhttp://en.wikipedia.org/wiki/Antigenhttp://en.wikipedia.org/wiki/Antigenhttp://en.wikipedia.org/wiki/Red_blood_cellhttp://en.wikipedia.org/wiki/Red_blood_cellhttp://en.wikipedia.org/wiki/Bloodhttp://en.wikipedia.org/wiki/Heredityhttp://en.wikipedia.org/wiki/Antigenhttp://en.wikipedia.org/wiki/Antigenhttp://en.wikipedia.org/wiki/Red_blood_cellhttp://en.wikipedia.org/wiki/Red_blood_cell
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
14/57
Dia!nostic/aborator"
procedres
Date
ordered/Date
reslt$s)
in6
Indication$s
)
or
1rpose$s)
Reslt
Normal
vale
$nits
sed in
the
hospital)
nal"sis andInterpretatio
n of Reslts
0lood Urea
Nitro!en
$0UN)
D@G 77->=-
7E
D0G 77->=-
7E
To assess
renal
functions
and the
ability of
$idneys toe"crete urea
and protein.
TraditionalG
E=.=
6.IG
7=.C7
TraditionalG
L- >=mgQdl
6.IG
E.>-
C.7mmolQ&
'n increase in
the level of
1 indicates
an impaired
$idney
function.
SG1T
$Serm
Gltamic
1"rvicATransaminas
e)
D@G 77->=-
7E
D0G 77->=-
7E
6;!T is a
specic
indicator of
liverdysfunction.
6.IG
EC.=
6.IG
>7-C> ulQl
The result is
within normal
range.
0U D@G 77->=-
7E
D0G 77->=-
7E
Determines
how much
uric acid is
present in
your blood.The test can
help
determine
how well
your body
produces
TraditionalG
7B.F
6.IG
L7.E
TraditionalG
E.B-
N.BmgQdl
6.IG
>=N-B=umolQ&
'n increase in
the level of
1 indicates
a impaired
$idneyfunction.
7F 8 ! a g e
&@@D /K4I6T03
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
15/57
and removes
uric acid.
30s!
$3epatitis 0
srfaceanti!en
screenin!)
D@G 77->=-
7E
D0G 77->=-7E
Diagnosis of
acute,recent, or
chronic
hepatitis
infection
Determinatio
n of chronic
hepatitis
infection
status
on
0eactive
on
0eactive
NTIA 3CB
Screenin!
D@G 77->=-
7E
D0G 77->=-
7E
Diganosis of
/epatitis
5irus.
on
0eactive
on
0eactive
Nrsin! Responsibilities
efore During 'fter
Chec= for the specictest ordered b" thedoctor%
Oipe with cotton balls andalcohol the site whereinsertion is
done
Tell the 6@ when the needlewill be inserted for them toget
prepared
Instruct the 6@ to applypressure to the puncturesite until
bleeding stops.
:?plain the test and >h"is it needed%
'ssess the site forhematoma formation.
7B 8 ! a g e
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
16/57
Inform that there are nofood or id restrictions
Inform that the testre@ires blood sample,
tell >ho >ill do the testand >hen
Tell that there >ill bediscomfort from theneedle that >ill
beinserted and pressrefrom the torni@et%
If the patient is bein!treated for infection,advise that the
test >illbe repeated severaltimes to maintain thepro!ress%
Document the testperformed.
:?plain to the client thatan amont of blood >illbe e?tracted
from thebrachial arm%
!urpose 0esult Interpretation
7 8 ! a g e
1&T0'6@1D 0K!@0T
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
17/57
3O:
0DO5INUTRSOUND
4edical test that uses high-
frequency sound waves to
capture live images from
the inside of your body,
which help the military
detect planes and ships
also allows doctor to see
problems with organs,
vessels, and tissues without
needing to ma$e an
incision.
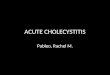
Ri!ht iver obeG 7F.= " 77.N " 7=.B cmeft iver obe G E.LN " F.LB
" E.C7 cmGallbladder G N.7= " >.B cmSpleen G 77.> " E.N
cm1ancreas G =.LB " 7.7> " =.Lcm / "
" TJRi!ht Eidne" G L.FC " F.FF cmCortical Thic=ness67.L cmeft
Eidne" G L.> " B.>7 cmCortical Thic=nessG 7.LL cm1rostate G
>.N7 " >.N " >.CLcm 77.CgramsJ
The liver and spleenare slightly enlarged.It has smooth contour
and homogenousparenchymal echo pattern.
The !allbladderis slightly dilated. The wallsare thic$ened o.BN
cmJ There are severalhigh lever echoes noted within, measuringan
average of =.FLcm. The c"stic dct is7=mm with an 77mm
shadowingcalcication at the pro"imal segment.
1ancreas is normal in size. !arenchymalechopattern is uniform.
1ancreatic dctsare not dilated.
Urinar" bladder is adequately distended.o intravesical echoes
seen. The prostate!land is not enlarged. !arenchymalechopattern is
homogenous.
@bstructed biliarydisease with the
presence of stonesin the cystic duct.Intrahepatic ductsare
dilated and gallbladder isdistended. onsiderhocystitis.
Nrsin! Responsibilities $hole abdominal Ultrasond)6
1reprocedral Care6
7. hec$ for the specic test ordered by the doctor.>. hec$ for
materials needed.E. 6ecure a laboratory request.
F. K"plain the procedure to the 6@.
B. Inform that there the patient is not allowed to eat and can
only drin$
with small amount of water in ta$ing medicines.
. Inform the patient about the procedure. Tell himQher that
there will be
no discomfort while doing the procedure.
7C 8 ! a g e
http://www.healthline.com/human-body-maps/chest-blood-vesselshttp://www.healthline.com/human-body-maps/chest-blood-vessels
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
18/57
Drin! the test patient care.
7. 'ssisting to adhere to standard precautions.
>. !rovide emotional support.
E. 'ssist the patient and the physician during the procedure
1ostprocedral Care6
7. @btain results and secure it to the patientMs chart.
>. 0efer the results to the physician.
E. Document the test performed.
Dia!nostic/aborator"procedres
Dateordered/
Datereslt$s)
in6
Indication$s)or
1rpose$s)
Reslt
Normalvale$nits
sed inthe
hospital)
nal"sis andInterpretation
of Reslts
URIN4SIS D@G 77-7C-
7ED0G 77-7C-
7E
The
diagnostictest is
performed
for the
general
evaluation
of the
patientMs
health. It
helps in
identifyingmetabolic
and
systemic
diseases or
olorG 3ellow 6traw to
dar$yellow
0esult indicates
normal nding.
Transparency
6lightly
turbid
lear
0esult may
indicate the
presence of
particulate
matters such as
bile, bacteria, pus
and hemolysis.
p/G .B
'cidicJ
p/ .B %
N.=
0esult indicates
normal nding.
reshly voided
urine is normally
somewhat acidic
7N 8 ! a g e
10I'&36I6
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
19/57
disorders
that aAect
the $idney
and
urinary
tract.
1rinalysis
is ordered
to identify
any
deviation
that may
indicate
the
diagnosisof the
patient.
6p. ;r.G 7.=>= 7.==B %
7.=EB
0esult is within
normal range.
'lbuminG SE
Trace
egative
%J
unctionalalbuminuria maybe present duringacute illness butis
#ust temporary.This may alsoindicate 0enaldisease
6ugarGegative %J
egative%J
0esult indicatesnormal nding.
5ICROSCO1IC 9INDINGS
!us cellsG
=.>Qhpf
Kpithelial
ellsGew
one 0esult may
indicate urinary
tract infection
alterations in$idney function.
7L 8 ! a g e
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
20/57
NURSING R:S1ONSI0IITI:S6
1re procedral care6
7. hec$ the doctorMs order.
>. K"plain to the patient and 6@ the procedure and purpose
of
urinalysis.
E. !rovide clean specimen cup.
F. K"plain to the patient to obtain midstream urine.
B. 'dvise the patient to wash urinary meatus prior to collecting
the
specimen to avoid contamination.
. Inform the patient that there is no (uid and food
restriction
needed.
>= 8 ! a g e
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
21/57
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
22/57
The biliary system consists of the organs and ducts bile ducts,
gallbladder,
and associated structuresJ that are involved in the production
and transportation of
bile. The transportation of bile follows this sequenceG
Ohen the liver cells secrete bile, it is collected by a system
of ducts
that (ow from the liver through the right and left hepatic
ducts.
These ducts ultimately drain into the common hepatic duct.
The common hepatic duct then #oins with the cystic duct from
the
gallbladder to form the common bile duct, which runs from the
liver to
the duodenum the rst section of the small intestineJ.
/owever, not all bile runs directly into the duodenum. 'bout
B=
percent of the bile produced by the liver is rst stored in
the
gallbladder, a pear-shaped organ located directly below the
liver.
Then, when food is eaten, the gallbladder contracts and
releases
stored bile into the duodenum to help brea$ down the fats.
9nctions of the 0iliar" S"stem
The biliary system9s main function includes the followingG
>> 8 ! a g e
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
23/57
a. to drain waste products from the liver into the duodenum
b. to help in digestion with the controlled release of bile
0ile is the greenish-yellow (uid consisting of waste products,
cholesterol, and bile
saltsJ, required for the digestion of food. It is secreted by
the liver cells to perform
two primary functions, including the followingG
a. to carry away waste products, and
b. to brea$ down fats during digestion
ile salt is the actual component which helps brea$ down and
absorb fats. Oithout
adequate bile, our body cannot metabolize fats which can result
in a deciency ofthe fat-soluble vitamins ', D, K and HJ. Oe may
also have problems digesting the
essential fatty acids. 'mongst other symptoms we could have
trouble utilizing
calcium, have dry s$in, peeling on the soles of your feet, etc.
@ne way we can tell
we have trouble digesting fats is if we have e"cessive burping
that starts shortly
after eating a meal that has fat in it. Oe might feel nauseous
or e"perience gas and
bloating. ile, which is e"creted from the body in the form of
feces, is what gives
feces its dar$ brown color.
G0DD:R
The gallbladder is a small pouch that sits #ust under the liver.
The gallbladder or
cholecyst or gall bladderJ is a small non-vital organ that aids
in the digestive
process and stores bile produced in the liver. It stores bile
produced by the liver.
'fter meals, the gallbladder is empty and (at, li$e a de(ated
balloon. efore a meal,
the gallbladder may be full of bile and about the size of a
small pear.
>E 8 ! a g e
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
24/57
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
25/57
C4STIC DUCT
The cystic duct is the short duct that #oins the
gall bladder to the common bile duct. It usually
lies ne"t to the cystic artery. It is of variable
length. It contains a 9spiral valve9, which does
not provide much resistance to the (ow of bile.
ile can (ow in both directions between the
gallbladder and the common hepatic duct andthe commonJ bile
duct. In this way, bile is
stored in the gallbladder in between meal times
and released after a fatty meal.
CO55ON 3:1TIC DUCT
The common hepatic duct is the duct formed by the convergence of
the righthepatic duct which drains bile from the right functional
lobe of the liverJ and the
left hepatic duct which drains bile from the left functional
lobe of the liverJ. The
common hepatic duct then #oins the cystic duct coming from the
gallbladder to form
the common bile duct.
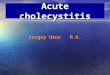
PATHOPHYSIOLOGY
(Book Based)
>B 8 ! a g e
Precipitating Factors:
Diet
Medications and Oral Contraceptives
Obesity
Rapid Weight Loss
Spinal Cord Injury
Primary iliary Cirrhosis
Diabetes Mellitus
!emolytic Syndromes
Ileal Disease" Resection and ypass
iliary In#ection
Predisposing Factors:
$ender
%ge
Race
!eredity
Pregnancy
acterial
hydrolysis
of lecithin
1ncon#ug
ilirubin t
to form
insolubprecipita
ormatio
alciuilirubin
&iver e"
som
uncon#u
bilirubinbile
alcium e
bile pass
along w
otheelectroly
Increase in
uncon#ugate
d bilirubin 0elease offatty acids
The bacteria
hydrolyze
con#ugated
bilirubin
Invasion
ofbacteria
&iver
e"crete
con#ugated
bilirubin intobile
&iver e"crete
relatively high
proportion of
cholesterol inthe bile
&iver cells
also
secrete
bile salts0esidual ormation ofmi"ed micelles
6ome of the
unilamellarvesicles
&iver cells secrete
cholesterol into bile
along with
phospholipid in the
form of unilamellarvesicles
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
26/57
> 8 ! a g e
ucleation of
cholesterol
cr stals
ormation of
rystals
ile is
supersaturated
with cholesterol
The cholesterol
carrying capacity
of the micelles
and residual
vesicles is
Cholesterol
Gallstones
5i?ed
Stones
leu$ocyte
s
hydrolyze
bilirubin
con#ugate
s and
'ttractionof
&eu$ocyte
acteriarelease
lytic
enzyme
0ro>n
1i!ment
Gallstones
ormation of
alcium
ilirubinate
A fatty acids fo
comple" wi
0lac
1i!me
Gallsto
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
27/57
>C 8 ! a g e
6Q6
Indigestion,
5it 'DKH
deciency,ibrosis
&iver irrhosis
Irritation of th
gallbladder w
/ydrolization of lecithin
intolysolecithinDamages muco
cells due to dete
action of bile sa
0elease of
phospholipase from the
epithelium of the
Disruption of mu
coat of the gallbla
epithelium
/epatomegaly
6Q6 #aundice,
ecteric sclera,
pruritus, dar$
urine
U levels of
bilirubinQbile
pigments in the
circulation
'bsence of ile
in the duodenum
!rolong
holestasis
holestasis
@bstruction of the
common bile duct by
gallstones
holedocholelithiasi
s
@bstruction o
cystic duct
gallstone
;allstone tries to
go out of the
C3O:IT3ISIS
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
28/57
>N 8 ! a g e
6Q6 iliary olic,
Tenderness,
4urphyMs sign,
nausea and
vomiting, fever,
elevated wbc
K0esistance to
portal blood (ow
ibrous nodules distorts
the architecture of the
CUT:
C3O:C4ST
0elease of prostagla
within the gallblad
F
!ortal /ypertension
Increase
pressure in
Kdema, hemorrhag
suppuration of t
gallbladder wa
acteria invade
in#ured gallblad
through the blo
lymphatic or b
ducts form ad#a
organs
Kmpyema of
gallbladder
K"tern
surface o
gallbladd
scarred
layered
brino
e"udates
distend
I @T T0K'T
;@@D !0@;@6I6
I T0K'TKDG
@pen holecystectomy
&aparoscopic
holecystectomy
&itotripsy
1rsodeo"ycholicacid
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
29/57
>L 8 ! a g e
Gangrenos
!"o#ec$stitis
ecrosis
1lcerations of the
mucosa
Ischemia
ompromised blood
(ow to the mucosa
and lymphatic stasis
IncreasedIntraluminal pressure
ompression of
blood vessels
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
30/57
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
31/57
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
32/57
E> 8 ! a g e
F
loc$age or increase
pressure in the portal veincauses blood to bac$(ow to
the diAerent vessels located
near the esophagus and ;ITluid shifting fro
the portal vein t
peritoneal cavit
Increase pressur
peritoneal capill
6pleen enlarges to
compensate
decreased liver
6hunting of blood
into the splenic vein
&iver is unable to
convert the
protein byproduct
ammonia into
&iver failure
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
33/57
EE 8 ! a g e
/ypovolemi
/ypovolemic
Death
6
D
6eptic
6Q6
Thrombocyto
penia,
anemia,
leu$openia
Death
Increases in blood
waste product since
spleen is not able
to properly destroy
0Ms
Increase in sizedecreases the
spleenMs ability to
function properly or
loss of function
6Q6
'steri"i
6Q6 eve
diarrhea
abdomin
6pontaneo
acterial !erit
Invasion ofbacteria fro
the blood, o
lymph or
through the
's
0upture
;astroesophageal
5arices
6plenomegal
6Q6 'nore"ia, ausea,&iver tenderness,aundice
/K!'TI
Development of a
large pale nucleus,
a prominent
nucleolus, and
margination of
'strocytes become
swollen
'strocytes may
undergo 'lzheimer
type II astrocytosis
4orphologic
changes in
'mmonia enters
general circulation
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
34/57
S"nthesis of the Disease6holecystitis is dened as in(ammation of
the gallbladder that occurs most
commonly because of an obstruction of the cystic duct from
cholelithiasis. It is
caused by an obstruction of the cystic duct, leading to
distention of the gallbladder.
's the gallbladder becomes distended, blood (ow and lymphatic
drainage are
compromised, leading to mucosal ischemia and necrosis.
1redisposin! 9actors6
Gender6 Oomen have twice the ris$ as men of developing
cholesterol gallstones
because estrogen increases biliary cholesterol secretion. efore
puberty this ris$ is
negligible, and beyond menopause the increased ris$
disappears.
EF 8 ! a g e
erebral edema
Increased
intracranial
rain /ernation
/epatic oma
D:T3
http://emedicine.medscape.com/article/171886-overviewhttp://emedicine.medscape.com/article/171886-overview
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
35/57
!e6The incidence increases with age. &ess than B-? of the
population under age
F= have stones, in contrast to >B-E=? of those over N=.
Race6 !revalence highest in orth 'merican Indians, hilean
Indians, and hilean
/ispanics, greater in orthern Kurope and orth 'merica than in
'sia, lowest in
Vapan: familial disposition: hereditary aspects
3eredit"6 amily history alone imparts increased ris$, as do a
variety of inborn
errors of metabolism that lead to impaired bile salt synthesis
and secretion or
generate increased serum and biliary levels of cholesterol, such
as defects in
lipoprotein receptors hyperlipidemia syndromesJ, which engender
mar$ed
increases in cholesterol biosynthesis.
1re!nanc"6 !regnancy is an independent ris$ factor for
cholesterol gallstones. Theris$ increases with increasing parity,
especially with more than two children. During
pregnancy, elevated estrogen and progesterone levels increase
biliary cholesterol
secretion. Klevated progesterone also inhibits gallbladder
contractility. F=? of
women develop biliary sludge in their gallbladder and 7>? of
women form their rst
stones during pregnancy. The incidence of gallstones is higher
in women with
multiple pregnancies.
1recipitatin! 9actors6
Diet $3i!h 9at, 3i!h Sodim)6Increased inta$e of calories, rened
carbohydrate,
cholesterol, and saturated fats has all been postulated to cause
cholesterol
gallstones. !atients with cholesterol gallstones secrete a
greater fraction of dietary
cholesterol into bile than do normal sub#ects.
5edications and Oral ContraceptivesG /ypolipidemic agents
clobrate,
gembrozilJ that lower serum cholesterol by increasing biliary
cholesterol secretion
increase the ris$ of cholesterol gallstones by twofold to
threefold. ompetitive
inhibitors of E-hydro"y-E-methylglutaryl coenzyme ' /4;o'J
reductase
lovastatin, simvastatin, pravastatinJ decrease biliary
cholesterol saturation.
Kstrogen therapy is associated with an increased ris$ of
developing cholesterol
EB 8 ! a g e
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
36/57
gallstones. @ral contraceptive steroids increase biliary
cholesterol secretion and
saturation but do not aAect gallbladder motility.
Obesit"G @besity is strongly associated with increased gallstone
prevalence. The
ris$ is proportional to the increase in total body fat. @bese
people synthesize more
cholesterol in both hepatic and nonhepatic tissues, transport it
to the liver, and
secrete more of it into the bile, leading to bile that is often
greatly supersaturated
with cholesterol.
Rapid ei!ht oss6@bese patients undergoing rapid weight loss
7->? of body
weight or appro"imately 7-> $gQwee$J, either by very low
caloric dieting or gastric
stapling, have a >B-F=? chance of developing gallstones
within F months. During
rapid weight loss, biliary cholesterol saturation increases
acutely as cholesterol is
mobilized from adipose tissue and s$in and secreted into
bile.
Spinal Cord In.r"6!atients with spinal cord in#ury have 7=?
incidence of forming
gallstones within the rst year after in#ury. This high ris$,
which is >= times normal,
is believed to be secondary to abnormal gallbladder motility and
probably biliary
hypersecretion of cholesterol from the progressive reduction in
body mass.
1rimar" 0iliar" Cirrhosis6!atients with primary biliary
cirrhosis have an increased
prevalence of gallstones. 6tone analysis has not been performed,
but the elevated
cholesterol saturation of bile in these patients suggest that
they form cholesterol
stones.
Diabetes 5ellits6Despite obesity and increased total body
cholesterol synthesis
and decreased gallbladder motility seen in patients with
diabetes, diabetes mellitus
itself does not appear to be an independent ris$ factor for
cholesterol gallstone
disease.
3emol"tic S"ndromes6 Inherited hemolytic anemia, sic$le cell
disease,
sphericytosis, thalassemia, chronic hemolysis associated with
articial heart vavles,
and malaria dramatically increase the ris$ of pigment stone
formation because of
increased biliary secretion of total bilirubin con#ugates,
especially bilirubin
monoglucoronide, at the e"pense of the bilirubin diglucuronide,
the predominant
con#ugate in healthy individuals.
E 8 ! a g e
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
37/57
Ileal Disease, Resection and 0"pass6 !atients with ileal
dysfunction have a
stri$ingly increased ris$ for developing gallstones. ;allstones
develop in E=-B=? of
patients with ileal hronMs disease: the ris$ correlates
positively with the e"tent and
duration of ileal dysfunction, 'lthough ilieal disease or
resection leads to cholesterol
supersaturation and cholesterol stone formation in some patients
, careful studies
now show that most patients with ilieal dysfuncyion form blac$
pigment, not
cholesterol stones.
0iliar" Infection6 rown pigment stones are frequently found in
the intrahepatic
bile ducts and are always associated with infection by colonic
organisms usually
K.coli, or parasitic infestation 'scaris lumbricoides, or other
helminthesJ.
Intraductal stones developing after cholecystectomy are
invariable associated with
bile stasis, biliary tree infection, andQor retained suture
material.
Si!ns and S"mptoms6
0iliar" Colic/ 5oderate to Severe 1ain6The most common symptom
is in pain
the right upper part of the abdomen or epigastrium. This can
cause an attac$ of
abdominal pain, called biliary colic, whichG develops quic$ly,
is severe, lasts about
one to three hours before fading gradually, isn9t helped by
over-the-counter and
isn9t helped by passing wind. The pain may radiate to the bac$,
right scapula or
shoulder. The pain often begins suddenly following a meal. The
pain of biliary colic is
caused by the functional spasm of the cystic duct when
obstructed by stones,
whereas pain in acute cholecystitis is caused by in(ammation of
the gallbladder
wall.
Tenderness6 !alpation of the abdomen frequently elicits
localized tenderness in the
right upper quadrant which is associated with guarding and
rebound tenderness.
5rph"s Si!n6The patient with acute in(ammation of the
gallbladder might have
a positive 4urphyMs sign, which is inspiratory arrest during
deep palpation in the
right upper quadrant.
EC 8 ! a g e
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
38/57
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
39/57
EL 8 ! a g e
Irritation of the Spersaton of 0i
Srface chan!es9ormation
small
Increased mcos
Cr"stal
enlar!es
Increased
mcos
Obstrction of
2ectation and Obstrction
of the
Common 0ile Dct
0acterial
invasion
iver
Impairme
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
40/57
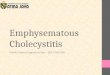
S"nthesis of the Disease6;allstones can form anywhere in the
biliary tree, however the point of origin is
within the gallbladder. ;allstones develop when an individual
eats too much fatty
and salty foods that causes an increase in bile cholesterol,
therefore, causing an
irritation of the gall bladder. The surface changes within the
gallbladder and mucous
secretion increases as a form of a compensatory mechanism. The
bile, however,
becomes more viscous ma$ing hard for the gallbladder to contract
and secrete bile.
6mall crystals form and enlarges into visible stones. These
stones or what we
commonly call )gallstones* tries to get out of the gallbladder.
The stone then passes
on the cystic and common bile ducts which later on causes an
obstruction. 6ince
there is an obstruction, the gallbladder can no longer secrete
bile causing
indigestion, vitamin ',D,K and H deciency and gray stool. There
will also be an
increase in the levels of bilirubinQbile pigments in the
circulation, thus, ma$ing the
F= 8 ! a g e
Inammation
HUNDIC: N:5RU8 pain
$) 5rph"s
Increase
d 0C
C3O:C4STITIS
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
41/57
sclera and the s$in yellowish in color. 'lso, this obstruction
causes an irritation in
the gallbladder wall, and an in(ammatory response happens
through the release of
prostaglandins. Ohen prostaglandins are released, symptoms such
as tenderness,
012 pain, murphyMs sign, nausea, vomiting, anore"ia and an
elevated wbc
happensQmanifests. Thus, cholecystitis happens.
1redisposin! 9actors6
!e6The incidence increases with age. &ess than B-? of the
population under age
F= have stones, in contrast to >B-E=? of those over N=.
1recipitatin! 9actors6
Diet $3i!h 9at, 3i!h Sodim)6Increased inta$e of calories, rened
carbohydrate,
cholesterol, and saturated fats has all been postulated to cause
cholesterol
gallstones. !atients with cholesterol gallstones secrete a
greater fraction of dietary
cholesterol into bile than do normal sub#ects.
Si!ns and S"mptoms6
Tenderness6 !alpation of the abdomen frequently elicits
localized tenderness in the
right upper quadrant which is associated with guarding and
rebound tenderness.
5rph"s Si!n6The patient with acute in(ammation of the
gallbladder might have
a positive 4urphyMs sign, which is inspiratory arrest during
deep palpation in the
right upper quadrant.
Nasea and Bomitin!6These signs and symptoms may accompany a
gallbladder
attac$. !ain is usually accompanied by nausea and vomiting.
oss of appetite and nore?ia6The pain often begins suddenly
following a large
or rich meal. !eople tend not to eat, especially fatty or oily
foods, in order not to
e"perience that pain. at absorption is also impaired for the
lac$ of bile salts, 's a
result, rapid loss of weight and anore"ia can occur.
F7 8 ! a g e
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
42/57
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
43/57
RR0(? cpm
Problem : Activit! Intolerance
Cues Nursing Diagnosis Scientific Explanation Planning
Intervention
Subjective Cues:
%"Maniat mi$ala
ku hospital
mangalamut naku!"
,s verali#e$ y the
patient!
Objective Cues:
%Difficulty in
changing e$
position
%@enerali#e$+eakness
%Aimite$ range of
motion
%Nee$s assistance
+hen $oing ,DA
:e!g! going to toilet8
changing clothes!;
%.ital Signs
/P0 (1)'2)mm3g
4emp0 5&!(C
PR0 &6 pm
RR0(? cpm
%,ctivity Intolerance
relate$ to general
+eakness!
%,ctivity intolerance is
affecte$ y any $isor$er
that impairs the aility
of the nervous system8
musculoskeletal
system8 car$iovascular
system8 respiratory
system an$ vestiular
apparatus!
,fter < hours of
nursing
interventions the
client +ill e ale
to0
%I$entify
alternative +ays
to maintain
$esire$ activity
level!
%,sk the client aout the
usual level of energy!
%I$entify factors8 such as
age an$ painful
con$itions!
%Instruct the client in
unfamiliar activities an$
in alternate +ays of
$oing familiar activities!
%Discuss +ith client'S9
the relationship of illness
' $eilitating con$ition to
inaility to perform
$esire$ activities!
%I$entify an$ $iscuss
symptoms for +hich
client nee$ to see
me$ical assistance or
evaluation!
FE 8 ! a g e
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
44/57
Problem ": Ris# $or %e$icient &lui% 'olume
Cues Nursing Diagnosis Scientific Explanation Planning
Intervention
Subjective Cues:
%"Mana+a ku pong
$anum" ,s
verali#e$ y the
patient!
Objective Cues:
%Dry skin
%@eneral +eakness
%Dry lips
%.ital Signs
/P0 (1)'2)mm3g
4emp0 5&!(C
PR0 &6 pm
RR0(? cpm
Risk for $eficient
flui$ volume relate$
to ina$e>uate flui$
intake
Deficient *lui$ .olume
is $ecrease$
intravascular8
interstitial8 an$'or
intracellular flui$! 4his
refers to $ehy$ration8
+ater loss alone
+ithout change in
so$ium!
,fter < hours of
nursing
intervention the
client +ill e ale
to0
%Demonstrate
ehaviors or
lifestyle changes
to prevent
$evelopment of
flui$ volume
$eficit!
%Evaluate nutritional
status8 noting current
intake8 type of $iet!
%Monitor I'9 alance8
eing a+are of altere$
intake or output!
%Estalish in$ivi$ual
flui$ nee$s ' replacement
sche$ule!
%Provi$e supplemental
flui$s8 as in$icate$!
Problem (: )no*le%+e ,e$icit
Cues Nursing Diagnosis Scientific Explanation Planning
Intervention
Subjective Cues:
%"Nanu +ari
talagang kun$isyun
ku " ,s verali#e$
y the patient!
Objective Cues:
Deficient kno+le$ge
relate$ to con$ition8
prognosis8 treatment8
self-care an$
$ischarge nee$s!
4here is this presence
of kno+le$ge $eficit
$ue to some unfamiliar
information that causes
some confusion to the
client that nee$s to e
$iscusse$!
,fter < hours of
nursing
intervention the
client +ill e ale
to0
%.erali#e
%Provi$e explanations
of'reasons for test
proce$ures an$
preparation nee$e$!
%Revie+ $isease
process'prognosis!
FF 8 ! a g e
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
45/57
%*re>uently asking
>uestion aout his
con$ition8 treatment
an$ $iet!
%orrie$ ga#e
un$erstan$ing of
$isease process8
prognosis an$
potential
complications!
Discuss hospitali#ation
an$ prospective
treatment as in$icate$!
Encourage >uestions8
expression of concern!
%Revie+ $rug regimen8
possile si$e effects!
%Instruct patient to avoi$
foo$'flui$s high in fats
or gastric irritants!
%Suggest patient to limit
gum che+ing8 sucking
on stra+' har$ can$y orsmoking!
T"pe of IB9 General Description Indication/
1rposes
Date
Ordered/D
ate
Started/Da
te
Chan!ed
Clients
Response to
Treatment
FB 8 ! a g e
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
46/57
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
47/57
Nursing Prolems0
(! ,cute pain
1! ,ctivity
intolerance
5! Imalance nutrition0
Aess than o$yre>uirements
.ital Signs
4EMP!
PR :pm;
RR:pm;
/P:mm3g;
5?!& C22
1)
())'?)
5?!6 C2=
(2
(()'&)
5&!( C&6
(?
(1)'2)
Diagnostic an$ Aaoratory
Proce$ure
3ematology
/loo$ chemistry
Me$ical Management0(!I.*
1! Drugs
9mepra#ole
Meperi$ine
3y$rochlori$e
Metocloprami$e Ceftriaxone So$ium
Brso$iol
Aactulose
5! Diet
D=ARs (A
NP9 except me$ication
C/R +' /RP
D=ARs (A
PNSS (A
PNSS (A
NP9
C/R +' /RP
PNSS (A
Soft Diet
May sit up on e$
1TI:NT ND 3IS CR:6 DI:T
FC 8 ! a g e
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
48/57
T"pe of:?ercise
GeneralDescription
Indication /1rposes
Clients Response and/orReaction to the Diet
Complete0ed Rest >ith0athroom1rivile!es
5a" sit p on
bed
!atient should beon bed most of thetime to decreaseo"ygen
demandand to lessen thefeeling of pain buthe can go to thebathroom
whenneeded.
' type of e"ercisewherein the patientis being0epositioned
every7-> hours.
This was orderedto conserveenergy, promoterecovery andprovide
rest toprevent fatigueand feeling ofpain. It is alsoordered
todecrease o"ygendemand.
To improvecirculation, toprevent
venousstasis,thrombophlebitis,respiratorycomplications ands$in
brea$down.
The patient was $ept in bed mostof the time and was able
toconserve energy through bedrest as evidenced by
patientMsverbalization of decreasedfatigue and wea$ness.
!atient did not manifest pain in
the calf upon dorsi(e"ion on thefoot and maintained
s$inintegrity.
1TI:NT ND 3IS CR:6 CTIBIT4
T"pe of Diet GeneralDescription
Indication /1rposes
DateOrdered
Clients
Responseand/or
Reaction tothe Diet
FN 8 ! a g e
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
49/57
N1O $Nothin!1er Orem)
Soft Diet
!@ orders are nothingper orem diets whichmeans that the
patientis not allowed any typeof food or drin$.
This is to introduce adiet that is easy todigest and allow the
;Itract to be ad#ustedwith limitation of foodsrich in fats.
To assess theclientMs labresultswithout anyvariance of
aAected food.
6oft diet wasordered toallow the ;Itract toreceive foodsthat are
easyto digest soas to preventgastricirritation andto
promoteeasierdigestion
ovember7L, >=7E
ovember>7, >=7E
'dministration ofI5 preventedthe patient fromdehydration.
Thepatient
cooperated wellwith theprescribed diet.
;I discomfortli$e abdominalpain waslessenedbecause of
thedecreasedcontraction ofthe gallbladder
CI:NTS DRUG T3:R134
Name
Dosa!e,
Rote
and
9re@enc
"
General ctionIndication /
1rpose
Date ordered,
Date
performed,
chan!ed or
D/C
C
Res
me
>it
side
0rand Name6!rilosec,
0apine",
Wegerid, &osec.
Generic
Name6
@meprazole.
Dosa!eMF=mg
Rote
M
Intravenou
s
MThought to be agastric pump
inhibitor in that it
bloc$s the nal
step of acid
production by
inhibiting the
/SQHS 'T!ase
M6hort % termtreatment of active
duodenal ulcer.
Xwith clarithomycin
to treat duodenal
ulcer associated
with H.pylori.
Date Ordered6ovember 7L,
>=7E
Date
1erformed6
ovember 7L,
>=7E
CNS/ead
Dizzi
GI6 '
!ain,
3em
FL 8 ! a g e
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
50/57
Classication6
!roton !ump
Inhibitor
9re@enc
"
M@nce a
day
system at the
secretory surface
of the gastric
parietal cell. oth
basal and
stimulated acid
secretions are
inhibited.
X6hort-term
treatment of active
benign gastric
ulcer.
X&ong-term
treatment of
hypersecretory
conditions.
X0educe ris$ of
upper ;I leeding
in critically ill
clients.
Date Chan!ed6
Q'
Discontine6
Q'
6
/em
'nem
5isc
!ain,
mala
Name
Dosa!e,
Rote
and
9re@enc
"
General ctionIndication /
1rpose
Date ordered,
Date
performed,
chan!ed or
D/C
C
Res
me
>it
side0rand Name6
Demerol
Dosa!e
M>Bmg
X@ne-tenth as
potent an
analgesic as
X'nalgesic for
moderate to severe
pain.
Date Ordered6
ovember 7L,
>=7E
N
e2e
B= 8 ! a g e
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
51/57
Generic
Name6
4eperidine
/ydrochloride
Classication6
arcotic
'nalgesic
Rote
M
Intravenou
s
9re@enc
"
M's
needed
morphine. Its
analgesic eAect is
only one-half when
given !@ rather
than parenterally.
/as no antitussive
eAects and does
not produce
miosis. &ess
smooth muscle
spasm,
constipation, and
antitussive eAect
than than
equianalagesic
doses of morphine.
Date
1erformed6
ovember 7L,
>=7E
Date Chan!ed6
Q'
Discontine6
Q'
ma
b" t
Name
Dosa!e,
Rote
and
9re@enc
"
General ctionIndication /
1rpose
Date ordered,
Date
performed,
chan!ed or
D/C
C
Res
me
>it
sid
B7 8 ! a g e
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
52/57
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
53/57
" D/C>it
sid0rand Name6
0ocephin
Generic
Name6
eftria"one
6odium
Classication6
ephalosporin
Dosa!e
M7g
Rote
MIntraven
ous
9re@enc
"
MqN
X Oor$s by
inhibiting the
mucopeptide
synthesis in the
bacterial cell wall.
The beta-lactam
moiety of eftri"one
binds to
cabo"ypeptidases,
endopeptidases, and
transpeptidases in
the bacterial
cytoplasmic
membrane. These
enzymes are
involved in cell-wallsynthesis and cell
division. y binding
to these enzymes,
eftria"one results
in the formation of
defective cell walls
and cell death.
XIntra-abdominal
infections due to
K.coli, H.
penumoniae, .
fragilis, lostridium
species most
strain of . di+cle
are resistantJ and
!eptostreptococcus
species.
Date Ordered6
ovember 7L,
>=7E
Date
1erformed6
ovember 7L,
>=7E
Date
Chan!ed6
Q'
Discontine6
Q'
No
e2e
man
b" t
BE 8 ! a g e
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
54/57
Name
Dosa!e,
Rote
and
9re@en
c"
General ctionIndication /
1rpose
Date ordered,
Date
performed,
chan!ed or
D/C
Cl
Resp
med
>ith
side0rand Name6
1sosan
Generic
Name6
1rsodiol
Classication6
;allstone
solubilizing
drug
Dosa!e
M>==mg
7
capsuleJ
Rote
M@ral
9re@en
c"
Mid
Xaturally occurring
bile acid that inhibits
the hepatic
synthesis and
secretion of
cholesterol: it also
inhibits intestinal
absorption of
cholesterol. 'cts to
solubilize cholesterol
in micelles and to
cause dispersion ofcholesterol as liquid
crystals in aqueous
media. 'bout L=? is
absorbed in the
small intestine after
!@ administration.
1ndergoes a
signicant rst-pass
eAect where it is
con#ugated with
either glycine or
taurine and then
secreted into hepatic
bile ducts.
XDissolution of
gallstones in clients
with radiolucent,
non-calcied
gallstones in whom
elective surgery
would be ris$y or in
those who refuse
surgery.
Date Ordered6
ovember 7L,
>=7E
Date
1erformed6
ovember 7L,
>=7E
Date Chan!ed6
Q'
Discontine6
Q'
GI6
aus
vom
abdo
pain
chole
CNS
/ead
fatig
BF 8 ! a g e
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
55/57
Name
Dosa!e,
Rote
and
9re@en
c"
General ctionIndication /
1rpose
Date ordered,
Date
performed,
chan!ed or
D/C
C
Res
me
>it
side0rand Name6
ephulac,
hronulac,
onstilac,
onstulose
Generic
Name6
&actulose
Classication6
ephalosporin
Dosa!e
ME= cc
Rote
M@ral
9re@en
c"
Monce a
day at
bed
time.
XIn the colon,
&actulose is bro$en
down primarily to
lactic acid.
4etabolized in the
colon by bacteria.
XTreatment of
constipation:
prevention and
treatment of portal-
systemic
encephalopathy,
including stages of
hepatic precoma
and coma.
Date Ordered6
ovember 7L,
>=7E
Date
1erformed6
ovember 7L,
>=7E
Date Chan!ed6
Q'
Discontine6
Q'
GI6 '
disco
and
aus
5om
BB 8 ! a g e
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
56/57
BII% CONCUSION
@ur gallbladder is one of the important organs in our body.
/owever, ma#ority of
us tend to forget its function and importance. holecystitis or
the in(ammation of
the gallbladder because of an obstruction is a disease that
requires a medical
attention. It adds on the morbidity and mortality rate of gall
stone diseases. Thus, it
is one of the common diseases in our country since one
contrubuting factor is the
food that we eat. This obstruction needs immediate attention
because it may cause
many complications. The harm that gallstones could give is that
they may leave the
gallbladder and enter the small intestine which causes the
patient to e"perience
abdominal pain.
Through this study, everyone will become aware of hisQher health
and daily
lifestyles. Therefore, we conclude that in order to lower the
ris$ of having this $indof condition, each and every one of us must
be conscious on our diet especially
when it comes to our food preferences. Though there is a saying
that, )4as
masarap pag bawal*, we should still be cautious of the foods
served in our dining
table % especially if itMs high in sodium and fat. 's Dr. /arry
Vohnson stated that the
secret to good health lies in every decision that human beings
ma$e.
B 8 ! a g e
-
8/9/2019 CHOLECYSTITIS CASE STUDY Version 2.0.docx
57/57
BIII% R:CO55:NDTIONS
To the !hilippine ;overnment, they may be aware of increasing
incident of thedisease condition in our country and that they may
help those who are less
fortunate by ma$ing the health care services more aAordable and
acceptable:
or the students who will study holecystitis as their case, that
they may $now
the diAerent causes of the said condition and understand the
pathology of the
disease and how the signs and symptoms manifest. That they may
also $eep in
mind the importance of the patientMs information which could be
obtained on the
chart.
or student nurses who will be handling patients with this
condition, health
education must always be done during nurse-patient interaction.
Teaching patients
proper ways in maintaining healthy lifestyle and importance of
proper nutrition.
or patients with ris$ factors in developing any of the
conditions that lead to
biliary obstruction, awareness of the signs and symptoms can
improve chances for
early diagnosis and improved outcome.