Embed Size (px)
Citation preview

CHKD RESIDENCY HANDBOOK: THE KD WAY
Edition 1
Malvika Kapoor, MD
Rachel Mayer, MD
Alicia Cousins, MD
Forward by C.W. Gowen Jr.

2
FORWARD
I was quite honored to be asked to write the forward for this booklet. Malvika,
Rachel, and Alicia have pulled together many resources, graphs, and tables
which are important to the way we deliver healthcare at CHKD.
In years past, we had laminated, colored cards held together by a metal ring
which included everything we could think of to help with patient care. Soon,
there were so many cards that it was impossible to carry and to find
information. There were a series of three (3) books entitled “The Whole
Pediatrician’s Catalog” written by Frank Oski, MD. Dr. Oski was a brilliant
pediatrician and he, too, saw the value of having information readily available
in one book (make that 3 books)!
This booklet is an excellent way to combine pertinent information into one
place. Use it well and always remember to let us know when you find a data
table or the latest in management and care. We can include that information in
the next edition.
Thanks once more to Malvika, Rachel, and Alicia for having the determination to
pull together pertinent information into a booklet that we could easily refer to
as “The KD Way.” Please give us your feedback.
C.W. Gowen, Jr., MD
Chair of Pediatrics

3
TABLE OF CONTENTS
Table of Contents
CHKD Information: ..................................................................................... 4
Nursery/NICU ............................................................................................ 8
Emergency Department: ............................................................................ 18
General Pediatrics: .................................................................................. 22
WARDS/CARDIOLOGY ................................................................................... 42
PICU: .................................................................................................... 48

4
CHKD INFORMATION: IMPORTANT NUMBERS: Michelle: 9763 Tricia: 7272 Pravash: 9994 Fax: 9766 Admit Pagers: C: 5371 H: 5998 K: 6001 D: 6002 CHKD Phone #: C: 5371 H: 5457/5371 K:5479 D:5370 Resident Lounge: 7072, 7340, 7305, 9079 CHKD Pharmacy: 7163, 9863 ED Pharm: 5456 On Call: 456-6180 Team C (Jessica): 8058 Team K: 5492 Team H Rx: 5651, 5250 Radiology: 9290 Reading room: 9389 Halifax: 893-1400
PICU main: 7315 PICU Attending: 8030 PICU Resident: 5302/7330 Mike Chicella: 8034 Surgery Simon: 1125 Tammy Simon: 6076 Nurse Supervisor: 8040 Medical Records: 7221 NICU Main: 7448 A (60-68): 8450 B (1-8): 8451 C (9-12): 7440 D (13-19): 8454 E (20-26): 8455 F (27-33): 8456 G (34-40): 8457 H (41-48): 8458 I (49-56): 8459 7D Step-down: 8168 Blue Team:9073 Red Team: 7452 VAT: 8836 Genetics: 9723
SNGH: 388-xxxx Level 1: 9656 Level 2: 5812 Senior: 0819 Level 2 Charge RN: 8131 OB Resident Room: 5813 Sentara Lab: 3448 Yolanda (Discharge): 0403 SW (Kelli): 0422 RT: 0450/0451 Pharmacy: 0692 GAP: 87400 (A side 42048, B side 42047) Doc: 8939 ED: 9247 3C: 8155 TCU: 8123 7C W (1-6) : 8776, 8764 7B (7-14): 8745 7C (15-37): 7442 8B (1-15): 7773 8C (16-30): 7510
How to Roll your pager: Dial 11, *Simon#, #, 1,1, Covering ID, # How to Unroll your pager: Dial 11,*Simon#, #, 1, 2

5
DEPARTMENT OF PEDIATRICS FACULTY LIST 2019-2020

6
DEPARTMENT OF PEDIATRICS FACULTY LIST 2019-2020

7
HOW TO DO AN EFFECTIVE TIME OUT:You must verbalize all of the following components:
● Correct patient (checking arm-bands for name & MRN) ● Correct procedure ● Accurate procedure consent (procedures involving Moderate Sedation require a
separate MS ● consent) ● Correct side and site are marked and visible ● Correct patient position (must state the position of the patient and that it is correct for
the procedure) ● Relevant images and results are appropriately displayed and labeled (if applicable) ● Safety precautions based on patient’s history & medications (if applicable) ● Need for administration of antibiotics or fluids for irrigation purposes (if applicable)
ELECTIVESAllergy/Immunology
Anesthesia
Cardiology
Child Abuse
Community Pediatrics
Dermatology
Emergency Medicine
Endocrinology
ENT
Gastroenterology
Genetics
Global Health
Hematology/Oncology
Infectious Diseases
Nephrology
Neurology
Orthopedic Surgery
Pediatric Surgery
Physical Medicine and
Rehab
Psychiatry
Pulmonology
Radiology
Research
Rheumatology
Rural Medicine
Sleep Medicine
Sports Medicine
Vascular Access Team
Core Electives: Team C Senior, Allergy/Immunology, Cardiology, Child Abuse Pediatrics, Dermatology, Endocrinology, Gastroenterology, Genetics, Hematology/Oncology, Infectious Diseases, Nephrology, Neurology/EEG, Psychiatry, Pulmonology, Rheumatology * Remember, 4 core electives are required for graduation All goals and objectives for each rotation can be found at chkdresed.org

8
NURSERY/NICU: APGAR SCORING:
Indicator 0 Points 1 Point 2 Points
A Appearance
(color)
Blue/pale
throughout
Pink body, blue
extremities
Pink throughout
P Pulse Absent Below 100 Above 100
G Grimace (reflex
irritability)
Floppy Minimal response to
stimulation
Prompt response to
stimulation
A Activity (muscle
tone)
Flaccid/limp Flexed arms and
legs
Vigorous activity
R Respiration Absent Weak/irregular cry Vigorous cry
Report total out of 10
Term Classifications:
Premature: < 34 weeks gestation
Late pre-term: 34 0/7 weeks through 36 6/7 weeks
Early term: 37 0/7 weeks through 38 6/7 weeks
Full term: 39 0/7 weeks through 40 6/7 weeks
Late term: 41 0/7 weeks through 41 6/7 weeks
Postterm: 42 0/7 weeks and beyond

9
Phototherapy Tools: Prior to 48 hours of life, and < 35 weeks gestation, use table:
Once 48 hours old, and <35 weeks gestation utilize Premie Bili Recs at pbr.stanfordchildrens.org
o Need infants post-menstrual age and total serum bilirubin o Categories are:
Prematurity alone Prematurity with additional neurotoxicity risk factors
Neurotoxicity Risk Factors:
Serum albumin levels < 2.5 g/dL
Rapidly rising TSB levels suggesting hemolytic disease
Those who are clinically unstable:
Blood pH < 7.15
Blood culture positive sepsis in the prior 24 hours
Apnea and bradycardia requiring cardio-respiratory resuscitation (bagging and or intubation) during the previous 24 hours
Hypotension requiring pressor treatment during the previous 24 hours
Mechanical ventilation at the time of blood sampling
If > 35 weeks gestation, use the nomogram, or Bilitool at BiliTool.org o Need infants date and time of birth, and date and time of blood sampling OR infants age in
hours at time of blood sampling, and total serum bilirubin o Categories are:
Lower Risk: >= 38 weeks and well Medium Risk: >= 38 weeks and neurotoxicity risk factors or 35-37 6/7 weeks and well High Risk: 35 to 37 6/7 weeks and neurotoxicity risk factors Neurotoxicity Risk Factors:
Isoimmune hemolytic disease
G6PD deficiency
Asphyxia
Significant lethargy
Temperature Instability
Sepsis
Acidosis
Albumin < 0.3 g/dL
Birth Weight Light level Exchange
Transfusion
500-1000 g 5 13
751-1000g 5 15
1001-1500 g 6-8 13-15
1501-2000 g 8-9 15-18

10
BILIRUBIN NOMOGRAM:
EXCHANGE TRANSFUSION:

11
Newborn Nursery Bilirubin Guidelines: Obtain Transcutaneous Bilirubin at:
o 12 hours for DAT + o 24 hours for LPT or SGA o 36 hours for AGA or LGA
Repeat check as T/D Bilirubin if: o Within 2 points of light level o Greater than 10 o Concerned for rate of rise or any other reason
Newborn Nursery Blood Sugar Guidelines Obtain Qac blood sugars for:
o LGA or IDM infants for 12 hours o SGA or LPT infants for 24 hours
Follow flow sheet posted in Nursery
Criteria for Neonatal Follow-up Clinic 1. All infants less than or equal to1250 grams 2. Meningitis 3. Seizures 4. HIE, symptomatic birth asphyxia 5. Severe IUGR <10% 6. Severe hypoglycemia resistant to therapy 7. Hyperbilirubinemia or polycythemia requiring an exchange transfusion 8. Recurrent apnea, discharged on apnea monitor (Must be former NICU patient) 9. PPHN, severe MAS, Nitric Oxide therapy, ECMO, hypothermia therapy 10. Chronic lung disease—home on oxygen monitor 11. Grade 3 IVH, Grade 4 IVH, PVL, Hydrocephalus, VP shunt 12. Toxic exposure in utero to alcohol, drugs (NICU patients only) 13. Teenage mother 16 and under (NICU patients only) 14. Congenital infections 15. Severe chronic illness 16. Microcephaly/Macrocephaly 17. Concerns for developmental delay of a NICU infant under the age of two years 18. Failed hearing screen
Donor Human Milk: Infants ≤1500 grams or ≤ 32 weeks at Sentara Norfolk General, and all babies that medically require it in CHKD NICU. Obtaining PICC consents: Consent must authorize insertion by “Dr. Green/PICC Team” and read “Peripherally Inserted Central Catheter with multiple attempts” for the description of procedure.

12
Women’s Health Social Work Referrals PLEASE indicate the reason for referral when entering a consult
1. Adolescent patients, 17 and younger 2. Patients CURRENTLY involved in a domestic violence relationship 3. Current pregnancy is a result of sexual assault 4. HIV positive patients diagnosed during CURRENT pregnancy 5. Patients with mental health issues and NOT on medication or being treated by a physician 6. History of postpartum depression 7. Patients with significant cognitive difficulties 8. Documented history of substance abuse DURING PREGNANCY ONLY 9. Positive urine drug screen on delivery for patient and/or infant 10. Previous CPS involvement (documented or suspected) 11. Patients who plan to place infant for adoption 12. If a parent has not visited or called regarding their infant in SCN only after the bedside nurse has
documented failed attempts to reach the parent 13. History of fetal demise ONLY when the parent is demonstrating poor bonding with infant and
increased anxiety, with CURRENT pregnancy and the mother’s behavior has been DOCUMENTED 14. Homelessness:
1. Triage and Preterm Labor -Staff can provide list of homeless resources or refer to a case manager.
2. Postpartum -SW needs to be notified to help ensure safety of infant at time of discharge.
CCHD Screen: Failure-Repeat screening in 1 hour (up to 2 times):
● <90% in right hand or foot – ALWAYS a positive screen ● 90-95% in right hand and foot ● >3% difference noted between right hand and foot
*If remains under 95% or >3% difference at 3rd
screen – positive screen
Eye Exam: ● < 26 wks = 6 wks ● 26 – 30 wks = 4 wks ● > 30 wks AND ≤ 1500 g = 4 wks ● < 33 wks AND Mech.Vent. or CPAP = 4 wks
CSS :< 32 wks or < 1500 g = 1 wk. f/u 1 mo, at Term AGA, 3-6 mo and PRN. Consider in children with
genetic syndromes.
Hearing Screen: ● ≥ 34 wks or once in open crib. ● Hospitalized > 5 days, repeat in 6 months. ● Referred = repeat 1 month, and obtain Urine CMV ● + Risk Factor = repeat within 3 months

13
Infection: ● Neonatal Sepsis Risks: Preterm, GBS+, prolonged ROM > 18 hrs, maternal signs/symptoms of
intra-amniotic infection. Remember to use the EOS calculator from Kaiser Permanente to stratify the risk of neonatal infection in infants >/= 35 weeks gestational age
○ Can be found online, or free app ("EOS Calculator") ○ https://neonatalsepsiscalculator.kaiserpermanente.org/ ○ Use incidence of 0.6/1000 live births ○ Use highest maternal temperature ○ Use Classification criteria to determine course of action
Classification for EOS Calculator
Well Appearing No persistent physiologic abnormalities
Equivocal One persistent physiologic abnormality > 4 hrs, or two or more physiologic abnormalities lasting for > 2 hrs
o Tachycardia (HR > 160) o Tachypnea (RR > 60) o Temperature instability (> 100.4˚F or < 97.5˚F) o Respiratory distress (grunting, flaring, or retracting) not
requiring supplemental O2
Note: abnormality can be intermittent
Clinical Illness Persistent need for NCPAP / HFNC / mechanical ventilation (outside of the delivery room)
Hemodynamic instability requiring vasoactive drugs
Neonatal encephalopathy /Perinatal depression o Seizure o Apgar Score @ 5 minutes < 5
Need for supplemental O2 > 2 hours to maintain oxygen saturations > 90% (outside of the delivery room)
● Chorioamnionitis: Maternal T > 38°C + ≥ 2 of: ↑WBC, Tachycardia, Fetal Tachycardia, Uterine
Tenderness, and/or foul odor of amniotic fluid. ● ANY concern for sepsis = Ampicillin/Gentamicin, Blood Culture, CBC w/Diff, consider LP and
Urine Culture. CRP more helpful after first few days. Use Ampicillin/Amikacin at CHKD NICU due to gentamicin resistance rates.
● I:T ratio = (immature WBCs)/(immature + segs). If > 0.2 = concerning. (immature = bands, myelocytes, promyelocytes, metamyelocytes, etc)
● HSV concern: HSV ½ PCR swabs from eyes, nares, mouth, anus-send to CHKD, serum HSV PCR and ASTR, +/- LP with HSV PCR and/or MEP PCR, +/- IV Acyclovir. Follow red book algorithm
● Necrotizing Enterocolitis: Treat with Amp/Gent/Ox. If doing a rule out, will continue treatment for 48 hours following KUB, clinical picture and lab work and reassessing at that point. If treating, course is typically 10 days.
Hepatitis B: Maternal HBsAg Negative
o Birth weight >= 2000 g -> give hepatitis B vaccine within 24 hours of birth o Birth weight < 2000 g -> give hepatitis B vaccine at 1 month of age/at hospital discharge
(whichever is first)
Maternal HBsAg Positive o All newborns at all birth weights -> give hepatitis vaccine and HBIG within 12 hours of birth
Maternal HBsAg Unknown

14
o All newborns at all birth weights -> give hepatitis vaccine within 12 hours of birth o Birth weight >= 2000 g -> give HBIG within 7 days of birth if maternal status is confirmed
positive OR by 7 days of life/at hospital discharge (whichever is first) if maternal status remains unknown
o Birth weight < 2000 g -> give HBIG within 12 hours of birth unless maternal status is confirmed negative by that time
Incubator:
● Can trial open crib when infant is 1800 gm & incubator setting is 28 degrees ● ISC mode regulates the temp based on what the baby’s temperature is reading ● NTE mode- incubator is set at one temperature based on baby’s age and size to give the minimum
energy expenditure. ● Humidity at SNGH:
○ Less than 750g, days 1-7 at 80%, days 8-14 at 60% ○ 751g-1200g, days 1-7 at 70%, days 8-14 at 50%
Heparinized lines:
● UVL/UAL: 0.5 U of heparin per 1ml of fluid ● PICC: 1U heparin per 1ml of fluid
Nursery Numbers: What to calculate: How to calculate:
Total Fluids (TF) (ml/kg/day) Total ml for day/weight
Feeds (kcal/kg/day) (ml/kg/day) x kcal/oz / 30ml/oz
IVF/TPN (kcal/kg/day) (ml/kg/day) X % dextrose X 0.034
Lipids Lipids in ml/kg/day X 2
Amino Acids Amino Acids in g/kg/day X 4
UOP (ml/kg/hr) ml for day/weight/24 hours
Ostomy/Sump/drain (ml/kg/day) ml for day/weight
Calculating GIR Rate X %dextrose / (weight x 6)
IVF/TPN: Start with D10 Water at 80ml/kg/day (remember, do not give neonates sodium on DOL 1+)
Can start infant on D10PNC if <1500g (remember, it arrives cold)
Order a TPN panel if suspecting will need TPN, or at least a BMP, Mag, Phos, and Trig level for DOL 2, and daily for 3 days -> In NICU, order MPT to obtain BMP, Mag, Phos, Trig labs
If not planning for TPN, order BMP daily while on fluids (can be spaced once stable)
After obtaining 24 hour BMP, can transition to D10L (D10 with electrolytes-10mEq KCl+15 mEq NaCl)
The traditional TPN panel can be a Monday only lab
As able to advance feeds (typically based on clinical status and serum sodium) can decrease IVF to keep total fluids at:
o DOL 1: ~80 mL/kg/day

15
o DOL 2: ~100 mL/kg/day o DOL 3: ~120 mL/kg/day o Goal: ~160 mL/kg/day if not requiring respiratory support, otherwise 130-140 mL/kg/day
When weaning by GIR, decrease by GIR of 1 mg/kg/min for every 2 glucoses >60
Ventilation:
Volume Guarantee: How to start:
Weight VT (ml/kg) I-Time PEEP <1.0 kg 4.5-6 0.25-0.35 5-6
1.0-1.5kg 4.5-6 0.3-0.4 5-6
>1.5kg 5-6 0.3-0.4 5-6
BPD - old 7-10 0.5-0.6 6-10
Weaning: o Wean rate, monitor PIP o If O2<30%, PIP <18, and PEEP <6, consider extubation
Low PIP : in patients with PIP <10 cmH20 o Look for increased WOB, increased O2 requirement, and increased RR and PaO2 o Increase Vt 0.5-1 ml/kg for weight <1.0 kg o Increase Vt 1-2 ml/kg for weight >1.0kg
High PIP : Underinflation or Opacification o Increase Ti and/or increase PEEP
o Can also be due to large air leak
NIPPV: How to start:
o Rate: <1000g - 40, >1000g - 30 (rate should support 50% of the total RR) o PIP: 18 or 2 above previous intubated setting
Max 26 cmH20 o PEEP: 5-6 (Max 7 cmH20)
Weaning: o PIP is first - by 2 until reaching 14 or 16 cmH20 o Rate (once PIP is 14-16 cmH20)
<1000 g - 40 to 30 (by 10) >1000 g - 30 is the minimum
o Wean PIP more, to 14 if not already there o Wean PEEP by 1 to 5 or 6 o Once stable on Rate 30, PIP 14, PEEP 5 for 4 hours then can consider transition to HFNC o Transition to HFNC via Vapotherm at 4-6 L/min

16
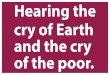
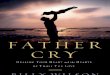
Fetal Circulation (with approximate oxygen saturations):
Umbilical Line Depth:
UVC (cm) UAC (cm) 3 ∗ 𝐵𝑊 𝑔 + 9
2+ 1
4 ∗ 𝐵𝑊 𝑘𝑔 + 7
Umbilical Line Depth:
Weight (g) UVC (cm) UAC (cm)
1000 7 8
1500 8 9
2000 9 9
3000 10 10
4000 12 12
5000 13 12 *adapted from the Umbilical Line Training Handbook
Goal Radiographic Depth:
UVC UAC
T8-T10 L3-L5 (low lying)
T6-T10 (high-lying)

17

18
EMERGENCY DEPARTMENT: Available Powerplans in ED: ED Trauma 1 ED Daibetic Ketoacidosis ED Sepsis/SIRS
ED Trauma 2 ED Fever and Neutropenia ED Sickle Cell with Fever (with or without pain)
ED Adult Chest Pain ED Fever in Young Infants ED Sickle Cell with pain (no fever)
ED Abdominal Pain ED Fractures ED Syncope
ED Altered Mental Status/Ingestion
ED Gyn ED VP Shunt
ED Anaphylaxis ED HSV Neonate Intranasal Medications
ED Asthma (<20kg, >20kg) ED Hydration Procedural Sedation Orders
ED Croup ED Migraine Relabel for Home Use
ED CSF ED SCAN Transfusion Request
ED Diabetes - New Onset ED Seizure

19
ED Trauma Performance Checklist Entering the Trauma Bay
1. Introduces self to the team and identifies their role ―I am Dr. George, PEDS resident. I will be MD 1 (or MD 2).‖
Yes No
2. Positions self at the head of the bed (or to patients right side if MD 2). Yes No
Primary Survey
3. Airway Assessment (MD 1)
a. Asks patients name Yes No
b. Physically inspects the mouth Yes No
c. States ―Airway patent‖ Yes No
d. Physically inspects the neck Yes No
e. States ―Trachea midline‖ Yes No
f. States ―C-spine is immobilized properly‖ Yes No
4. Breathing Assessment (MD 2)
a. Physically inspects the chest Yes No
b. States ―Chest rise is symmetric‖ Yes No
c. Listens for breath sounds bilaterally Yes No
d. States ―Breath sounds are equal bilaterally‖ Yes No
5. Circulation Assessment (MD 2)
a. Feels for distal pulses Yes No
b. Feels for central pulses if distal pulses absent Yes No
c. States ―2+ central and distal pulses‖ Yes No
d. Confirms IV/IO access Yes No
6. Disability Assessment (MD 2)
a. Assesses eye GCS Yes No
b. Assesses verbal GCS Yes No
c. Assesses motor GCS Yes No
d. States appropriate GCS Score (15) Yes No
e. Assesses pupils Yes No
f. States ―pupils equal, reactive (larger #-->smaller #) bilaterally‖ Yes No

20
g. States ―moving hands and feet bilaterally‖ Yes No
7. Environment and Exposure (MD 2)
a. Requests that all clothing be removed by the team Yes No
b. Visual inspects the body Yes No
c. States ―no gross deformities or bleeding‖ Yes No
d. Asks for team members for rolling (1 for c-spine, 2 for rolling) Yes No
e. Asks for patient roll on c-spine team member’s count Yes No
f. Visually/palpation inspects the back asking for pt feedback Yes No
g. States ―No CTLS tenderness, no bruising/abrasions to the back‖ Yes No
h. Removes backboard from patient Yes No
i. If moving lower extremities, does not check rectal tone and states ―No gross blood or bruising at perineum‖
Yes No
j. Covers patient back up again Yes No
Next Steps (MD 2)
8. Assures that heart rate, BP, pulse oximetry and temperature have been collected Yes No
9. States ―primary survey is within normal limits. Is everyone comfortable moving on to the secondary survey?‖
Yes No
10. Notes patient warmth and modesty maintained Yes No
11. Checks with documenting nurse, if any missing exam needed Yes No
12. Checks with nurses/attending to see if computer orders needed Yes No

21
Symptoms of Toxicities-

22
GENERAL PEDIATRICS:
Pediatric Blood Pressures
Normal Blood Pressures in Children
Age Systolic (mmHg) Diastolic (mmHg)
Neonate (1 day) 60-76 30-45
Neonate (4 day) 67-84 35-53
Infant (1 month) 73-94 36-56
Infant (3 month) 78-103 44-65
Infant (6 month) 82-105 46-68
Infant (1 year) 67-104 37-58
Child (2 years) 70-106 42-63
Child (7 years) 79-115 57-76
Adolescent (15 years) 93-131 64-83
Hypotension by Age
Age Hypotension Systolic BP (mmHg)
Term neonates (0-28) <60
Infants (1-12 months) <70
Children 1-10 years <70 + (age in years x2)
Children > 10 years <90 For accurate blood pressures, see Peds BP app (iPhone) or the following link:
https://www.mdcalc.com/aap-pediatric-hypertension-guidelines for calculations accounting for age, gender and height.
Based on 2017 AAP Clinical Practice Guideline for Screening and Management of High Blood Pressure in Children and Adolescents- see document for more detail about management.
If the initial BP is elevated (≥90th percentile), providers should perform 2 additional oscillometric or auscultatory BP measurements at the same visit and average them.
Classification of Blood Pressure
Stage Children and Adolescents 1–<13 y of Age Adolescents ≥13 y of Age
Normal BP <90th percentile
<120/<80 mm Hg
Elevated BP ≥90th percentile to <95th percentile or 120/80 mm Hg to <95th percentile (whichever is lower)
120/<80–129/<80 mm Hg
Stage 1 hypertension ≥95th percentile to <95th percentile + 12 mmHg, or 130/80 to 139/89 mm Hg (whichever is lower)
130/80–139/89 mm Hg
Stage 2 hypertension ≥95th percentile + 12 mm Hg, or ≥140/90 mm Hg (whichever is lower)
≥140/90 mm Hg

23
How to Fortify Breast Milk: - Add ½ teaspoon Neosure/Enfacare to 45 mL of breastmilk to get 24 kcal/oz - Add 1 teaspoon Neosure/Enfacare to 45 mL of breastmilk to get 27 kcal/oz - Add 1 ½ teaspoon Neosure/Enfacare to 45 mL of breastmilk to get 30 kcal/oz
How to fortify Formula: - 1 scoop of powder for 2 oz of water for 20 kcal/oz - 3 scoops of powder for 5 ½ oz of water for 24 kcal/oz - 3 scoops of powder for 5 oz of water for 27 kcal/oz
Expected oral intake for newborn: -feed on demand, no schedule -should be feeding at least Q2-Q3 hours, with waking to feed
Breast pumps can often be covered by insurance. Family needs to bring insurance card to visit to be provided with a pump.

24
Newborn Exam
Expected weight gain for term newborn: 20g-30g per day
General/Measurements:
Weight and Length
Frontal Occipital Circumference (FOC)
—be sure to check these measurements ON the growth chart (and remeasure if needed)
Adjust for gestational age (Fenton Growth Curve) or Genetic syndromes (Trisomy 21)
Infant activity, skin color, breathing, vitale (HR/RR), etc. Overall gestalt.
Head:
Any dysmorphic features Fontanelles and sutures Eyes: pupil reaction, red reflex, conjunctival injection/discharge/hemorrhage Ears: low set, angled, normal position, shape Nose: patent, symmetric Mouth: mandible size, cleft palate/lip, frenulum, uvula Neck: torticollis, clavicles, webbing/clefts/masses
Chest : Heart, lungs, work of breathing, chest shape, etc.
Skin : Jaundice (check skin, eyes/sclera, frenulum)
Nevus Simplex: salmon patch, often on forehead, upper eyelid, nape of neck; fade over time
Nevus flammeus: port-wine stain; dark purple/red; assoc Sturge-Weber & Klippel-Trenaunay-Weber
Hemangioma: benign vascular tumor; often self involutes; large lesions may require treatment
Erythema toxicum: diffuse papules with erythematous base; can come & go; resolves within 14 days
Pustular melanosis: pustules without erythema that leave hyperpigmented macules that fade
Milia: white papules on nose
Dermal melanosis: blue-gray macules common over sacrum
Cafe au lait spots: light-brown macule; benign or assoc McCune-Albright or neurofibromatosis
-Document number and size in chart
Cutis marmorata: reticular mottling of skin; often response to cold resolving with warmth

25
Abdomen:
General: scaphoid, distended, discolored
Umbilical cord: erythema, hernia, drainage
Genitourinary
Female, Male, Ambiguous genitalia
Testes: descended bilaterally (must palpate both)
Scrotum: hydroceole or hernia present?
Penis: circumcised versus uncircumcised, position of meatus, chordee, buried penis
Anus/Rectum: patency, anal wink, sacral dimple/tuft
Extremities
Hands/Feet: polydactyly/syndactyly, supernumerary digits, single palmar crease
Arms: Erb or Klumpke palsy
Legs/Hips: Clubfoot, developmental dysplasia of the hip (Ortolani and Barlow maneuvers)
Neurologic
Reflexes: Babinski, suck, grasp, root, symmetric moro, etc.
Tone, cry
Voluntary motor activity
Source: A Comprehensive Newborn Examination: Part I and II. MARY L. LEWIS, MD, Dwight D. Eisenhower Army Medical Center, Fort Gordon, Georgia

26
Pediatric Vaccine Schedule
Visit Immunizations Task List** Screening Labs
2 weeks Edinburgh Postnatal Depression Score (EPDS)
1 month Edinburgh Postnatal Depression Score (EPDS)
Look at newborn screen. Repeat hearing screen?
2 months Pentacel (Dtap/HiB/IPV), HepB, Rotavirus, PCV-13
Edinburgh Postnatal Depression Score (EPDS)
4 months Pentacel (Dtap/HiB/IPV), Rotavirus, PCV-13 (No HepB unless infant did not receive at birth)
Edinburgh Postnatal Depression Score (EPDS)
6 months Pentacel (Dtap/HiB/IPV), HepB, Rotavirus, PCV-13
Edinburgh Postnatal Depression Score (EPDS)
Repeat hearing screen?
9 months ASQ
1 year MMR, Varicella, Hep A (no combo vaccines)
CBCA, Venous Lead
15 months Dtap, PCV-13, and HIB OR Pentacel plus PCV-13
18 months Hep A MCHAT, ASQ
24 months MCHAT, ASQ CBCA, Venous Lead
30 months ASQ, +/- MCHAT
4 years Kinrix (Dtap, IPV) and ProQuad (MMR, Varicella)
+/- Lipid Profile (between 3-5 years if there is FH or Risk Factors
9-12 years (adolescent)
Tdap, Menactra, HPV PHQ-9 -Lipid profile (between 9-11 AND 17-21) -Consider STI Screening (RPR, Gc/CL, etc) -CBCA for menstruating females
16-18 years (adolescent)
Menactra (5 years after 1st dose), Bexero (16 years) -2nd dose after 1 month
PHQ-9
*If no Pentacel – Pediarix (Dtap/ HepB/IPV) plus HiB , Rotateq, and PCV-13 *Need Hep B if they don’t get it at birth

27
Asthma

29

30
Dermatology Basic Terminology
Configuration: linear, grouped, target (concentric rings), annular (grouped circle), nummular (round/coin shaped/discoid), geographic, gyrate (whirling circle), Distribution:
1) Acral: relating to distal extremities 2) Blaschko lines: relating to the developmental lines of Blaschko 3) Dermatomal: lesion confined to segment of skin with single spinal nerve innervation 4) Extensor/Flexural: involving extensor/flexural surfaces of limbs 5) Follicular: lesions in or around hair follicles 6) Generalized: lesions distributed randomly over most of the body 7) Herpetiform: solid papules within a cluster 8) Photosensitive: increase in reactivity due to sunlight
Morphology:
color (red, pink, violaceous, brown, black, blue, orange, yellow)
consistency (soft, firm, hard, fluctuant, sclerosed)
temperature (warmer or cooler than surrounding tissue)
shapes (macule, papule, bulla, etc.) 1) Macule: patch of skin that is altered in color but not elevated 2) Patch: a large area of color change with smooth surface 3) Papule: elevated, solid, palpable lesion ≤ 1 cm in diameter 4) Nodule: elevated, solid, palpable lesion >1cm 5) Cyst: papule or nodule with fluctuance (containing fluid or semifluid material) 6) Plaque: circumscribed, palpable lesion >1cm in diameter, usually elevated 7) Vesicle: small blister ≤ 1 cm in diameter that contains liquid 8) Pustule: similar to vesicle but containing pus 9) Bulla: large blister >1 cm in diameter containing liquid 10) Abscess: localized collection of pus 11) Wheal: transient elevation of skin due to dermal edema
Skin Surface -Scaling or hyperkeratosis – an increase in the dead cells on the surface of the skin (stratum corneum). Descriptive terms: Desquamation (skin coming off in scales), Lichenoid (apparent scale is tightly adherent to skin surface), Keratotic (horny scale), Exfoliation (peeling skin), Maceration (moist peeling skin), Verrucous (warty)
Secondary changes
1) Lichenification: caused by chronic rubbing, which results in palpably thickened skin with increased skin markings and lichenoid scale. It occurs in chronic atopic eczema and lichen simplex.
2) Crusting: the result of plasma exuding through an eroded epidermis. It is rough on the surface and is yellow or brown in colour. Bloody crust appears red, purple or black.
3) Dystrophy: degeneration or abnormal formation of the skin. It is often used to refer to nail diseases. 4) Excoriation: a loss of the epidermis and a portion of the dermis due to scratching or an exogenous
injury. It may be linear or punctate. 5) Erosion: a sore due to superficial or partial destruction of surface tissue such as the skin. 6) Fissure: a split, crack, erosion or narrow ulceration of the skin. 7) Fungating: refers to a large malignant tumour that is erupting like a mushroom or fungus. 8) Granulation tissue: made of a mass of new capillaries and fibrous tissue in a healing wound. 9) Ulcer: full-thickness loss of the epidermis plus at least a portion of the dermis; it may extend into the
subcutaneous tissue. An ulcer heals with a scar. 10) Granuloma: a type of inflammation characterised by histiocytes. 11) Hypertrophy: explains that some component of the skin such as a scar is enlarged or has grown
excessively.

31

32
Developmental Milestones
Milestone Red Flags
Developmental Milestones Rebecca J. Scharf, MD, MPH,* Graham J. Scharf, MA,† Annemarie Stroustrup, MD, MPH
Speaking/Hearing 2 or more languages in the household is NOT a reason for speech delay.

33
Adolescent Encounter
How to do it:
When interviewing an adolescent, request that parents/siblings leave the room when asking sensitive questions. Emphasize that private interviewing is routine and helps develop independence in medical care.
HEADSSS Assessment
Home Including who, where, recent moves, relationships, violence
Education Employment
where, year, academic performance, bullying, disciplinary actions, future plans, jobs
Eating weight, dieting, exercise, menstruation
Activities sports, organized groups, clubs, parties, TV/computer use
Drugs and EtOH cigarettes, alcohol, illicit drugs; use by patient, friends or family
Sex relationships, activity, # partners, gender of partners, abuse, pregnancy risk, contraception, STI
SI, depression, Self-harm
feelings of sadness, thought of self-harm or suicidal ideation PHQ-9 questionnaire
Safety use of safety gear (helmets, seatbelts); exposure to violence at home/school, firearms at home
For details, see: http://www.bcchildrens.ca/youth-health-clinic-site/documents/headss20assessment20guide1.pdf
Depression PHQ-9: see form in clinic

34
Tanner Staging Adrenarche (Male and Female)
I II III IV V
No hair Downy hair Scant terminal hair Terminal hair that fills the entire triangle over the pubic region
Terminal hair that extends onto the thighs
Thelarche (Female)
I No palpable glandular tissue
II Breast bud palpable under areola
III Breast tissue palpable outside areola
IV Areola elevated above contour of breast
V Areolar mound recedes back to single breast contour with areolar hyperpigmentation and
papillae
Male Genital Development
I Testicular volume <4mL
II TV: 4-8mL (1st pubertial sign in male);
penis begins to grow
III TV: 9-12mL; increase in length and width of penis
IV TV: 15-20mL; continued penis growth
V TV: >20mL; mature penis size

35
Precocious Puberty Precocious puberty signs and symptoms include the following before age 8 in girls and before age 9 in boys.
Breast growth and first period in girls
Enlarged testicles and penis, facial hair and deepening voice in boys
Pubic or underarm hair
Rapid growth
Acne
Adult body odor HPG Review: Hypothalamus (GnRH)--> Pituitary (LH, FSH) --> ovaries (estrogen) and testes (testosterone) Benign Variants
Repeated evaluation warranted. -Premature Adrenarche: isolated pubic and/or axillary hair, acne, and apocrine odor (angrogen-mediated) -Premature Telarche: isolated breast development in girls
Central Precocious Puberty (CPP) -Idiopathic (80-90% of girls, 25-60% of boys) -CNS lesion (obtain MRI of brain with contrast) -CNS irradiation (often causing growth hormone (GH) deficiency) -Other CNS lesion (hydrocephalus, cyst, trauma, midline defect, inflammatory disease) -Genetics
Peripheral Precocious Puberty (PPP) -Ovarian cysts (most common cause of PPP in females) -Ovarian tumors (granulosa cell tumors, sertoli/leydig cell tumors, pure leydig cell tumor, gonadoblastoma) -Leydig cell tumors (consider in any male with assymetric testicular enlargement) -hCG-secreting germ cell tumor -Familial male-limited precocious puberty (aka testotoxicosis) -Primary hyopthyroidism -Exogenous sex steroids (estrogen creams/ointments/sprays, estrogen in soy, some herbal remedies) -Adrenal pathology (androgen producing tumor, congenital adrenal hypoplasia, etc) -McCune-Albright (irregular cafe-au-lait spots, PPP, fibrous dysplasia)
Workup
-thorough history and physical exam -bone age -LH, FSH (Morning draw) -estrogen, testosterone, DHEAS -Brain MRI with contrast (all boys with CPP and girls 6yo and under with CPP) -consider pelvic/testicular ultrasound
Nonprogressive precocious puberty
Central precocious puberty (CPP)
Peripheral precocity
Tanner stage
No progression in Tanner staging during 3 to 6 months of observation
Progression to next pubertal stage in 3 to 6 months
Progression
Growth velocity
Normal for bone age Accelerated (>6 cm per year) Accelerated
Bone age Normal to mildly advanced Advanced for height age Advanced for height age Serum estradiol
Prepubertal Prepubertal to pubertal Increased in ovarian causes of peripheral precocity, or with exogenous estrogen exposure
Serum testosterone
Prepubertal Prepubertal to pubertal Pubertal and increasing
Basal serum LH
Prepubertal Pubertal◊ Suppressed or prepubertal
GnRH stimulation test
LH peak in the prepubertal range Lower stimulated LH to FSH ratio
LH peak elevated (in the pubertal range) Higher stimulated LH to FSH ratio
No change from baseline, or LH peak in the prepubertal range
© 2019 UpToDate, Inc. and/or its affiliates. All Rights Reserved.

36
ADHD/Vanderbilt Scoring/Diagnosis
--Scoring is also detailed in the Vanderbilt Task List in Powerchart--
Parent Assessment Follow-up ■ Calculate Total Symptom Score for questions 1–18.
■ Calculate Average Performance Score for questions 19–26.
Teacher Assessment Follow-up ■ Calculate Total Symptom Score for questions 1–18.
■ Calculate Average Performance Score for questions 19–26.

37

38
Contraception
Mostly managed by Adolescent Gynecology Specialist. https://www.contemporarypediatrics.com/contemporary-pediatrics/news/contraception-guidelines-adolescents?page=full

39
Ointment and Cream Medication Size References
1 oz (28g) 15 grams
80 grams 60 grams
396 grams 454 grams

40

41

42
WARDS: HOSPITALIST MUST CALL: For patient safety, please call hospitalist on call so that they can be aware when the following patient diagnosis/situations arise on either new or established patients:
● Admission diagnosis/conditions: o Sepsis o Bacterial meningitis o Septic arthritis o Aggression o Patients with single ventricle physiology ** o Patient with Pulmonary hypertension** o Patients over 21 years old -> effort should be made to transfer to adult hospital o Patients who have a durable DNR
● Situations to call for on admission or while inpatient o Care Team o CAHR Tool firing while in 1C status o Transfer to PICU or concern for ICU level care o Patients requiring surgery consult o Positive blood culture o Requiring 2 or more racemic epinephrine (after treatment with steroids) o Requiring Q1 albuterol treatments o Hypernatremia with Na >160 o Non-ingestion related altered mental status o Oxygen requirement of > 6L (face mask) o Pregnancy o Bronchiolitic being placed on HFNC
**These patients should not be admitted to hospitalist at all. Please call the hospitalist to have a discussion with the ED attending.
CARDIOLOGY MUST CALL: This list is not an all-inclusive list. If you have any concerns please call the Cardiologist.
1. Deviation from plan of the day
2. Increasing respiratory support
3. Hemodynamic instability
4. Any other concerns
Cardiology Post-Catheterization Discharge List:
Make sure all patients have a discharge echocardiogram, EKG, and CXR
Make sure patient has been afebrile for 24 hours
Needs to be on all po meds
No Antiarrhythmic issues
RA for > 12 hours
Eating, drinking, urinating, and stooling appropriately
No other social/home care issues

43
Enoxaparin (Lovenox) Dose adjustment: Anti-Xa factor Level Hold next dose? Dose change: Repeat Anti-Xa:
<0.35 No Increase by 25% 4h after next morning dose
0.35-0.49 No Increase by 10% 4h after next morning dose
0.5-1.0 No No next day, then once a week 4 hours after morning dose
1.01-1.5 No Decrease by 20% Deforenext morning dose ; administer decreased dose if level <0.5 units/ml and recheck 4 hours post administration
1.51-2.0 3h Decrease by 30% Before next morning dose and recheck 4 hours post administration
>2.0 Until anti-Xa factor <0.5 units/mL
Decrease by 40% Q12h until <0.5 units/ml. Then administer decreased dose and recheck 4 hours after administration.
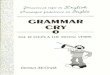
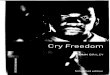
INTERPRETING EKG:
Determining QRS Axis on EKG
1. Look at the most equivocal lead - your axis is
perpendicular to this lead vector
2. Look at leads I - if positive, the vector is towards this
lead and if negative, the vector is away from this lead.
3. Look at lead aVF - if positive, the vector is towards
this lead and if negative, the vector is away from this lead.
Note: Sinus nodal rhythm is when P wave is positive in leads I and aVF.

44
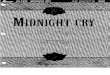
EKG leads and Anatomical Positions:
Grading Heart Murmurs:
Grade 1 – barely audible with stethoscope on chest
Grade 2 – faint but easily audible with stethoscope on chest
Grade 3 – loud, easily heard with stethoscope on chest
Grade 4 – loud, easily heard with stethoscope on chest, palpable thrill
Grade 5 – heard with the stethoscope slightly off chest, palpable thrill
Grade 6 – no stethoscope needed to hear murmur, palpable thrill
Heart Sounds and Their Location in the Cardiac Cycle:

45
Locations of Loudest Intensity for Common Heart Murmurs:

46
Pediatric EKG Pearls:
● Right Ventricular Enlargement (not hypertrophy) ○ r-S-R’ (in V1)
● Rate ● Rhythm: P waves must be up in leads I and AVF to be ―sinus‖ rhythm ● Axis: P, QRS, and T
○ P and T waves should both be up in Leads I, AVL, AVF, and down in AVR ○ Between 3 days old and adolescence, the T wave should be inverted in V1 ○ If the P is inverted in Lead I, the Dx is inverted leads, dextrocardia, or left atrial rhythm. ○ AV canal gives a pink baby with a superior vector in QRS ○ Noonan syndrome has a superior vector 50% of the time ○ LBBB can give a superior vector ○ An inverted T in Lead III is consistent with MVP
● Interval : PR should be less than approximately 0.15 seconds ○ QRS should be less than 0.10 seconds ○ QTC = QT/square root of the preceding RR interval and should be < 0.45
Note: All patients on IMCU are on telemetry, and all children with significant cardiac concerns should be on telemetry. This should be checked every morning prior to rounds, and at least once at night for overnight residents responsible for these patient. To check telemetry:
1. Go to patient’s window on one of the telemetry stations in PICU/IMCU 2. Go to Alarm Review 3. Scroll through the alarms: remember the telemetry may pick up outside noise or not correctly
categorize a type of arrhythmia. When looking through these ensure that there is an appropriate pleth and see if patient’s tracings actually match the recorded arrhythmia (ie is the PVC actually without a p-wave or is it a conducted PAC).

47
COMMON FIRST LINE AGENTS FOR DISEASES: Disease: First line agent:
Cellulitis Clindamycin
Acute Otitis Media Amoxicillin
Pneumonia Amoxicillin/ Ampicillin
UTI 1st or 2
nd generation cephalosporin, alternatively:
TMP/SMX
Gonorrhea IM ceftriaxone
Chlamydia Po Azithromycin
Fever + Neutropenia Cefepime (meropenem if AML)
Fever in Onc patient w/o Neutropenia Ceftriaxone
Neonatal Sepsis: Ampicillin, Amikacin/Gentamicin, +/- Oxicillin
Fever + Sickle Cell Disease Ceftriaxone (also can add Vanc if concerned for meningitis or azithromycin if concerned about acute chest)
*information adapted from pediatric red book. Reminders: - Should use ceftriaxone in neonates with caution due to displacement of bilirubin from serum albumin and a possible risk of bilirubin encephalopathy. -IV erythromycin and azithromycin associated with infantile hypertrophic pyloric stenosis, and these infants would be followed for signs and symptoms of pyloric stenosis. - Treat gonorrhea with ceftriaxone and azithromycin for possible chlamydial co-infection as well as trends towards gonorrhea resistance to ceftriaxone monotherapy.
LABS INCLUDED IN PANELS:

48
PICU: IMPORTANT EQUATIONS: Minute Ventilation:
𝑀𝑖𝑛𝑢𝑡𝑒 𝑣𝑒𝑛𝑡𝑖𝑙𝑎𝑡𝑖𝑜𝑛 (𝑀𝑉) = 𝑅𝑒𝑠𝑝𝑖𝑟𝑎𝑡𝑜𝑟𝑦 𝑟𝑎𝑡𝑒 𝑅𝑅 𝑥 𝑇𝑖𝑑𝑎𝑙 𝑉𝑜𝑙𝑢𝑚𝑒 (𝑇𝑉)
Cardiac Output:
𝐶𝑎𝑟𝑑𝑖𝑎𝑐 𝑂𝑢𝑡𝑝𝑢𝑡 𝐶𝑂 = 𝐻𝑒𝑎𝑟𝑡 𝑅𝑎𝑡𝑒 𝐻𝑅 𝑥 𝑆𝑡𝑟𝑜𝑘𝑒 𝑉𝑜𝑙𝑢𝑚𝑒 (𝑆𝑉)
Compliance:
𝐶𝑜𝑚𝑝𝑙𝑖𝑎𝑛𝑐𝑒 =𝐶𝑎𝑛𝑔𝑒 𝑖𝑛 𝑣𝑜𝑙𝑢𝑚𝑒
𝐶𝑎𝑛𝑔𝑒 𝑖𝑛 𝑝𝑟𝑒𝑠𝑠𝑢𝑟𝑒
Ohm's Law:
𝐹𝑙𝑜𝑤 =𝑐𝑎𝑛𝑔𝑒 𝑖𝑛 𝑝𝑟𝑒𝑠𝑠𝑢𝑟𝑒
𝑟𝑒𝑠𝑖𝑠𝑡𝑎𝑛𝑐𝑒
Poiseuille's Law:
𝑅𝑒𝑠𝑖𝑠𝑡𝑎𝑛𝑐𝑒 𝑅 =8𝜇𝐿
𝜋𝑟4
Mean Airway Pressure:
𝑀𝑒𝑎𝑛 𝐴𝑖𝑟𝑤𝑎𝑦 𝑃𝑟𝑒𝑠𝑠𝑢𝑟𝑒 𝑀𝐴𝑃 = 𝑃𝐼𝑃 − 𝑃𝐸𝐸𝑃 𝑥 𝑇𝑖
𝑇𝑡𝑜𝑡 + 𝑃𝐸𝐸𝑃
A good way to estimate this is 1/3 PIP + 2/3 PEEP
Oxygenation Index:
𝑂𝐼 = 𝐹𝑖𝑂2 𝑀𝐴𝑃
𝑃𝑎𝑂2
Mild ARDS: 4-8
Moderate ARDS 8-15
Severe ARDS >16
Consider HFOV for OI of 20-25
Consider ECMO for 30-40 A-a Gradient:
𝐴 − 𝑎 𝐺𝑟𝑎𝑑𝑖𝑒𝑛𝑡 = [ 𝐹𝑖𝑂2 𝑃𝑎𝑡𝑚 − 𝑃 20 − 𝑃𝑎𝐶𝑂2
0.8 − 𝑃𝑎𝑂2
approximate PaO2 = 7(FiO2 - PaCO2)
Normal A-a < 15 Parkland Formula (for 2
nd and 3
rd degree burns):
𝑉𝑜𝑙𝑢𝑚𝑒 = 4 ∗ 𝑚𝑎𝑠𝑠 𝑘𝑔 ∗ 𝑏𝑜𝑑𝑦 𝑝𝑒𝑟𝑐𝑒𝑛𝑡 𝑜𝑓 𝑏𝑢𝑟𝑛 (%)
1/2 of this volume should be replaced within the first 8 hours and the next ½ should be replaced over the next 16 hours
Fluid of choice: LR Caution: Correcting serum sodium too quickly can lead to cerebral or pulmonary edema.

49
UNDERSTANDING VENTILATION:
Abbreviation Term Definition
PIP Peak Inspiratory Pressure Maximal Airway Pressure. Total pressure delivered (used to overcome both respiratory system compliance as well as airway resistance). Sum
of PEEP and IP (in a pressure control mode)
PEEP Positive End Expiratory Pressure
Pressure maintained at the airways at the end of expiration. The pressure applied to the lungs never drops below this value.
IP or ΔP Inspiratory Pressure or Delta Pressure
Difference between PIP- PEEP
Vt Tidal Volume Volume of gas entering the patient's lung during inspiration
It Inspiratory Time Time spent in inspiration (can be set, i.e. during control breath, or determined by the patient, i.e. during a spontaneous pressure support
breath)
Et Expiratory time Time spent in expiration. Generally not directly set but determined by the set rate and inspiratory time. For example, a respiratory rate of 20 breaths/min means each breath is 3 seconds. If Itime is set at 1 second,
then Etime is necessarily 2 seconds
I:E Inspiratory:Expiratory time ratio
Generally, expiration takes longer than inspiration. A typical ratio is 1:2 (may need to be much greater, i.e. 1:4, with obstructive lung disease or
high airway resistance)
RR Respiratory Rate Respiratory rate as set on the ventilator (patient will receive at least these many breaths/min but can spontaneously breathe above this set
rate)
FIO2 Fraction of Inhaled Oxygen Varies from 21% (room air) to 100% with >50-60% considered toxic (reactive oxygen species, free radical formation etc). Historically,
subambient (ie <21% O2 was sometimes utilized in the cardiac unit to help "balance" circulation (reduce Qp in favor of Qs).
PS Pressure Support Extra pressure given to support the patient's spontaneous breaths above the set rate (ie instead of the IP or set volume, they receive the
set pressure support when they take their spontaneous breath)
There are 2 common modes of ventilation:
1. SIMV: (Synchronized Intermittent Mechanical Ventilation) – Recognizes patient’s breathing cycle and will fit ventilator breaths in the beginning of inspiration. Patient can still take spontaneous breaths that are unassisted in-between ventilated breaths. Less likely to stack breaths
2. SIMV PC (Synchronized Intermittent Mechanical Ventilation - Pressure control)

50
a. Fixed pressure that is given to patient. Observe delivered Tidal Volumes to assess compliance.
3. SIMV- PRVC (Synchronize d Intermittent Mechanical Ventilation) a. Delivers a pre-set volume at the lowest required peak pressure and adjusts with each breath
to meet the preset tidal volume. Assess the delivered PIP that is administered to assess the compliance of the lungs.
SHOCK ASSESSMENT:
Appearence (Pallor, distressed)
Mental status (appropriate vs. altered)
Vital signs (Specifically tachycardia, hypotension, tachypnea)
Perfusion/ peripheral pulses
UOP (remember, generally a good rule to remember is at least 1cc/kg/hour except in older adolescents where normal urination is 0.5cc/kg/hr)
Labs: (obtain if concerned, and look at if assessing for shock) o BUN/CR o Blood cultures (central vs. perpheral) /Tracheostomy cultures/ Urine cultures o Lactic Acid o Bicarbonate o Anion gap

51
BRAIN DEATH:

52
USING PRESSORS:
RASS SCORING:

53
Acknowledgements:
Dear Residents,
Welcome to CHKD! This family has a personal investment into making you the
best physician you can be. Although you are never alone, we wanted to give
you the tools to practice with confidence and give you some guidance whether
it be on the wards or outpatient. This is our first iteration of the CHKD
Handbook, and although it does not encompass everything, it is a start. We
understand that medicine is fast paced and ever-changing, and therefore even
information that was correct a year ago may be outdated now. Please reach out
to us if you find things that may be helpful or need to be changed for further
editions via emails. Our heartfelt thank you to Dr. Gowen for his enthusiasm
and support. Thank you to the following people for making this handbook
possible:
Dr. Sanaz Devlin Dr. Brett Siegfried
Dr. Natasha Sriraman
Dr. Thomas Cholis Dr. Alexander Ellis
Dr. Thomas W. Hubbard
Malvika Kapoor, MD
Rachel Mayer, MD Alicia Cousins, MD