Embed Size (px)
DESCRIPTION
CT colorectal
Citation preview
Chimioterapia in cancerul colorectal
Dr Cainap Calin
Martie 2015
Chimioterapia - indicatii? • ADJUVANT
• NEOADJUVANT
• METASTATIC
CHIMIOTERAPIA ADJUVANTA
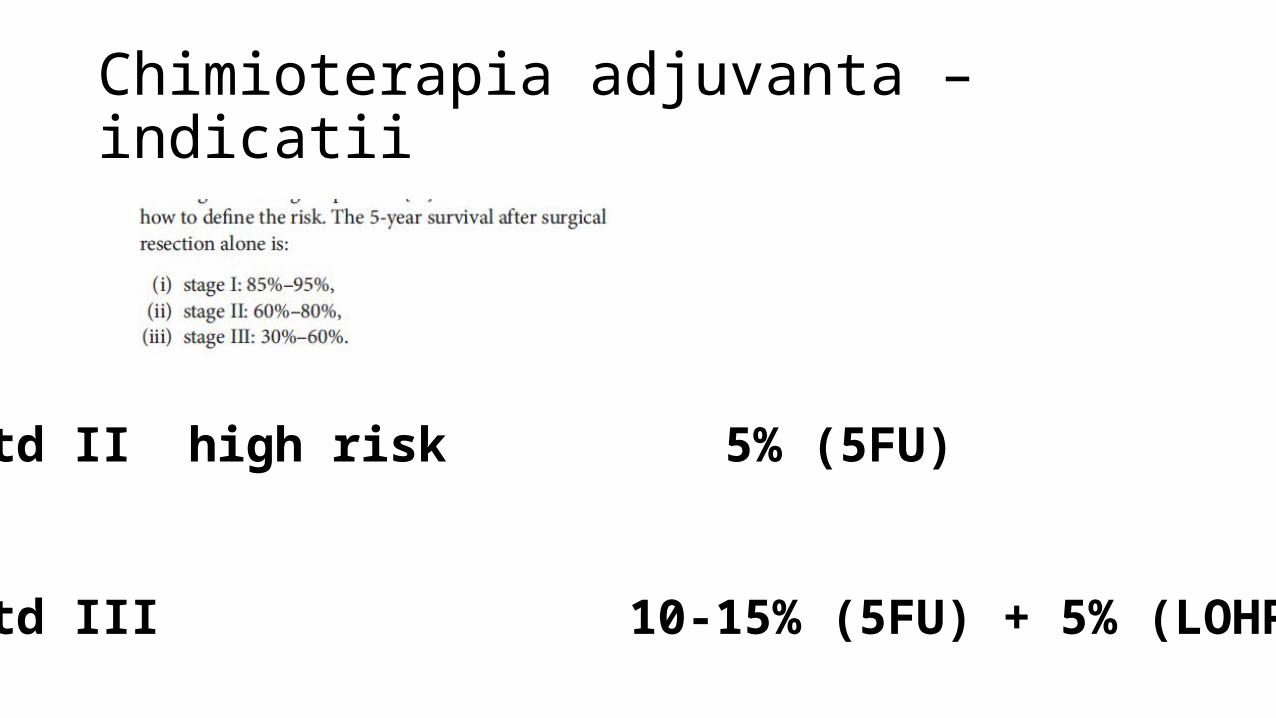
Chimioterapia adjuvanta – indicatii
Chimioterapia adjuvanta – indicatii
Std II high risk 5% (5FU)
Std III 10-15% (5FU) + 5% (LOHP)
Std II high risk• Excizie sub 12 ggl (std II – N=14 ggl)
• G3
• Ocluzie / perforatie
• Invazie L,V, perineurala
• ACE crescut persistent postoperator (ACE si CA 19-9 crescuti preoperator – pronostic negativ)
Std II high risk• Status MMR (mismatch repairs) la pacientii sub 70 de ani
• MMR H / MSI– 10-15% din std II nu beneficiaza de aportul chimioterapiei adjuvante • (STATUSUL NU INTERESEAZA LA PACIENTII CU STD III)
JCO 2010;28;3219-3226
• Pacientii peste 70 de ani beneficiaza = < 70 de ani• Toxicitatea 5FU = la < sau > 70 de ani• Aditia LOHP la pac peste 70 de ani creste toxicitatea fara avantaj de
OS
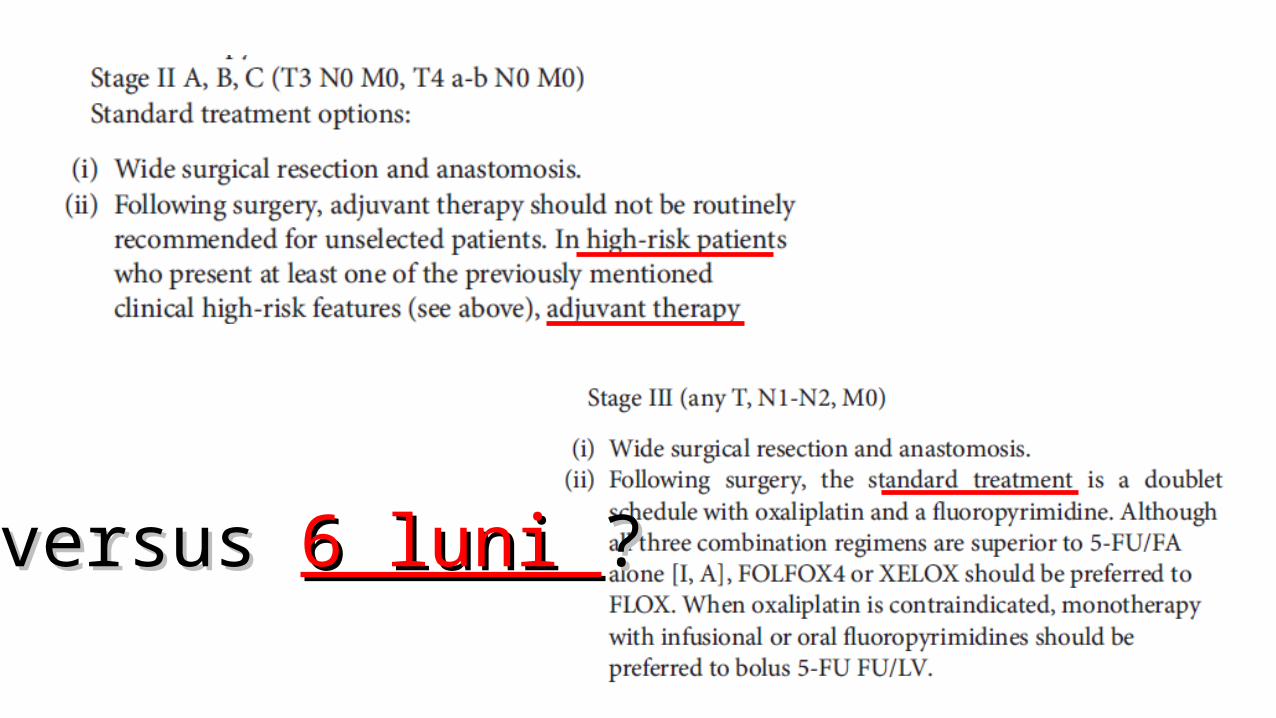
3 versus 3 versus 6 luni 6 luni ??
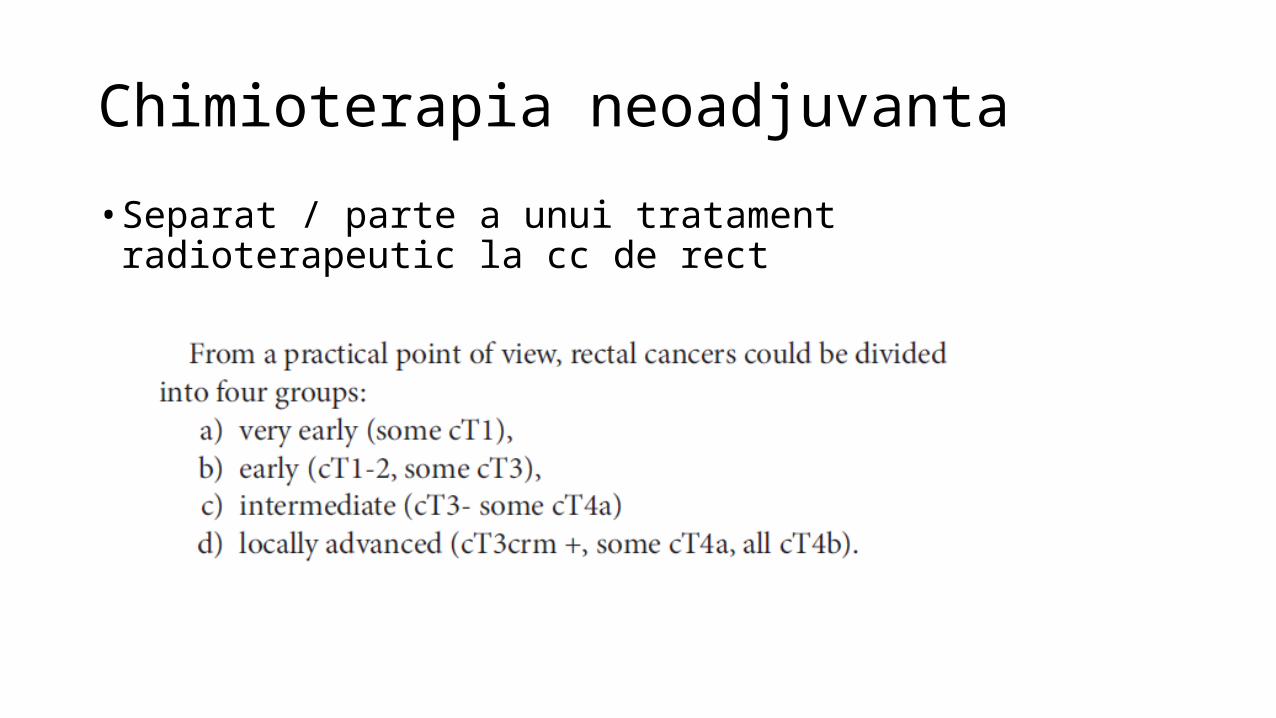
Chimioterapia neoadjuvanta• Separat / parte a unui tratament radioterapeutic la cc de rect

Chimioterapia neoadjuvanta• Separat / parte a unui tratament radioterapeutic la cc de rect
• T3 mai ales cu invazia tesutului perirectal, T4, N+, T2 situat jos / perete anterior
7 zile7 zile
6-8 sapt6-8 sapt
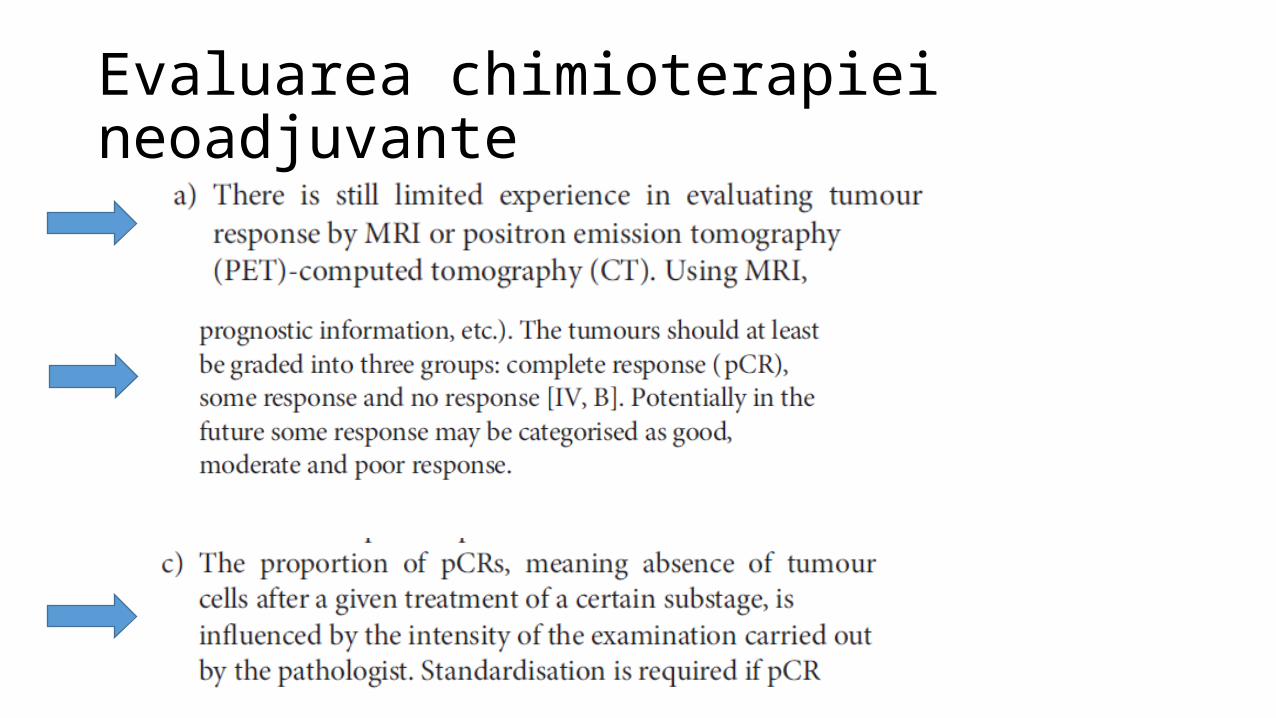
Evaluarea chimioterapiei neoadjuvante
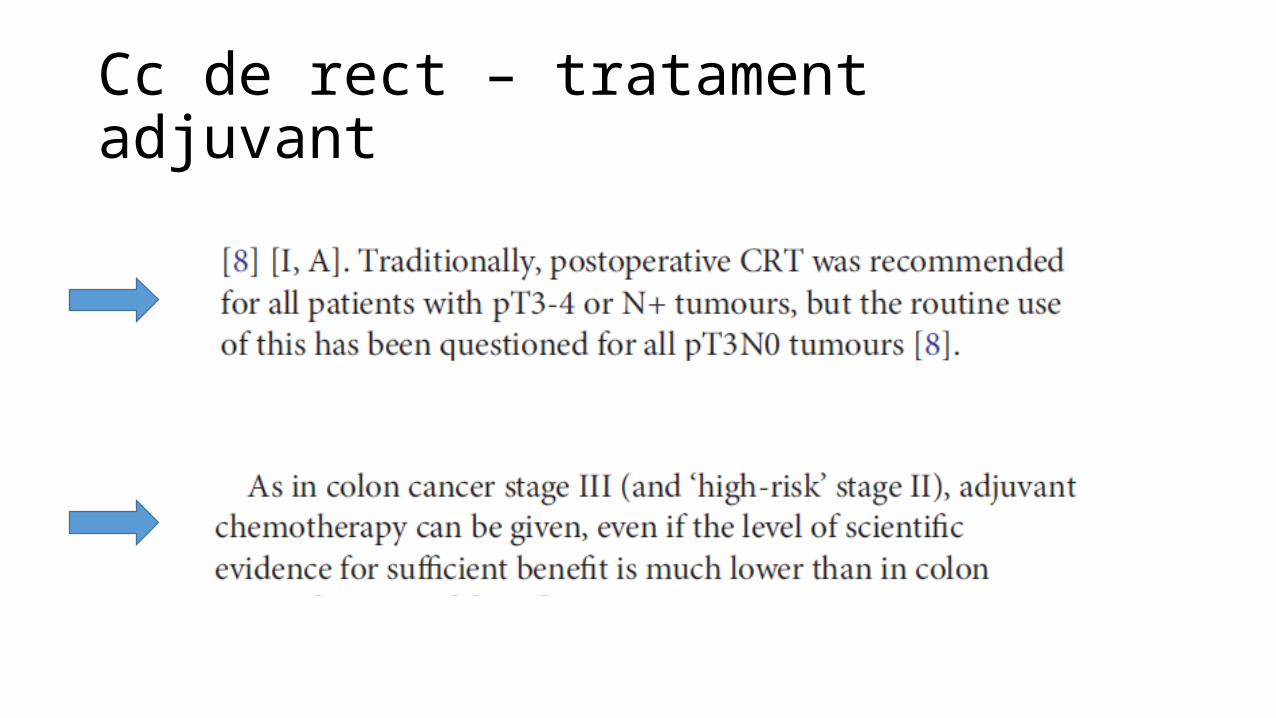
Cc de rect – tratament adjuvant
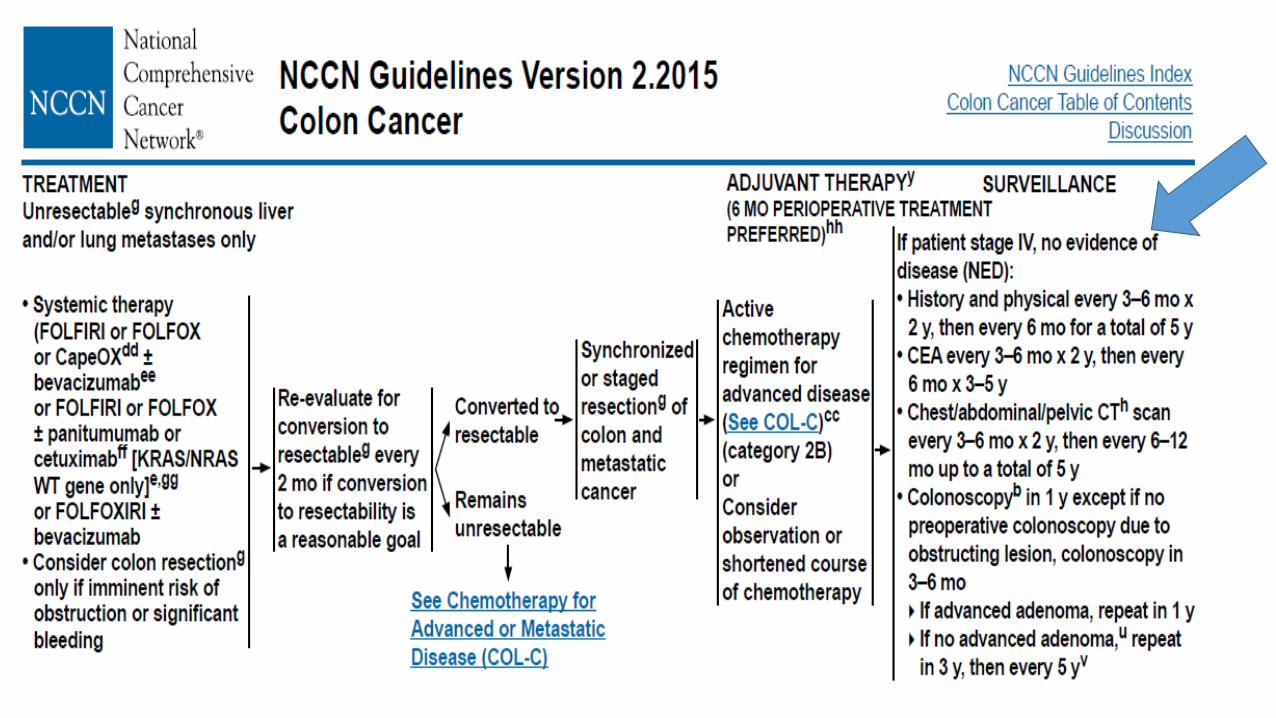
Cc de colon / rect metastatic
1.Ocluzie/ perforatie1.Ocluzie/ perforatie
2.Rezectie metastaze2.Rezectie metastaze
3.Rezectie tu primara3.Rezectie tu primara
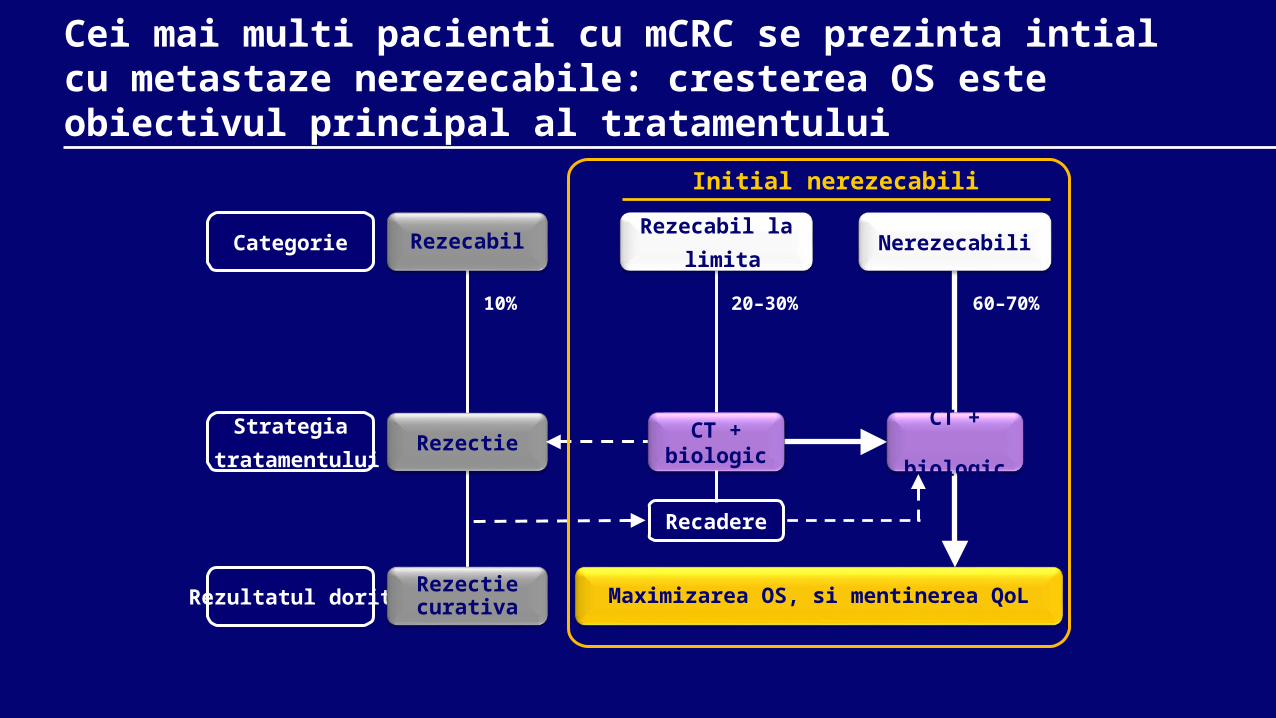
Rezectie
Maximizarea OS, si mentinerea QoL
Strategia tratamentului
Rezultatul dorit Rezectie curativa
10%
Categorie Rezecabil
Cei mai multi pacienti cu mCRC se prezinta intial cu metastaze nerezecabile: cresterea OS este obiectivul principal al tratamentului
20–30% 60–70%
Rezecabil la limita
Nerezecabili
CT +biologic
CT + biologic
Recadere
Initial nerezecabili
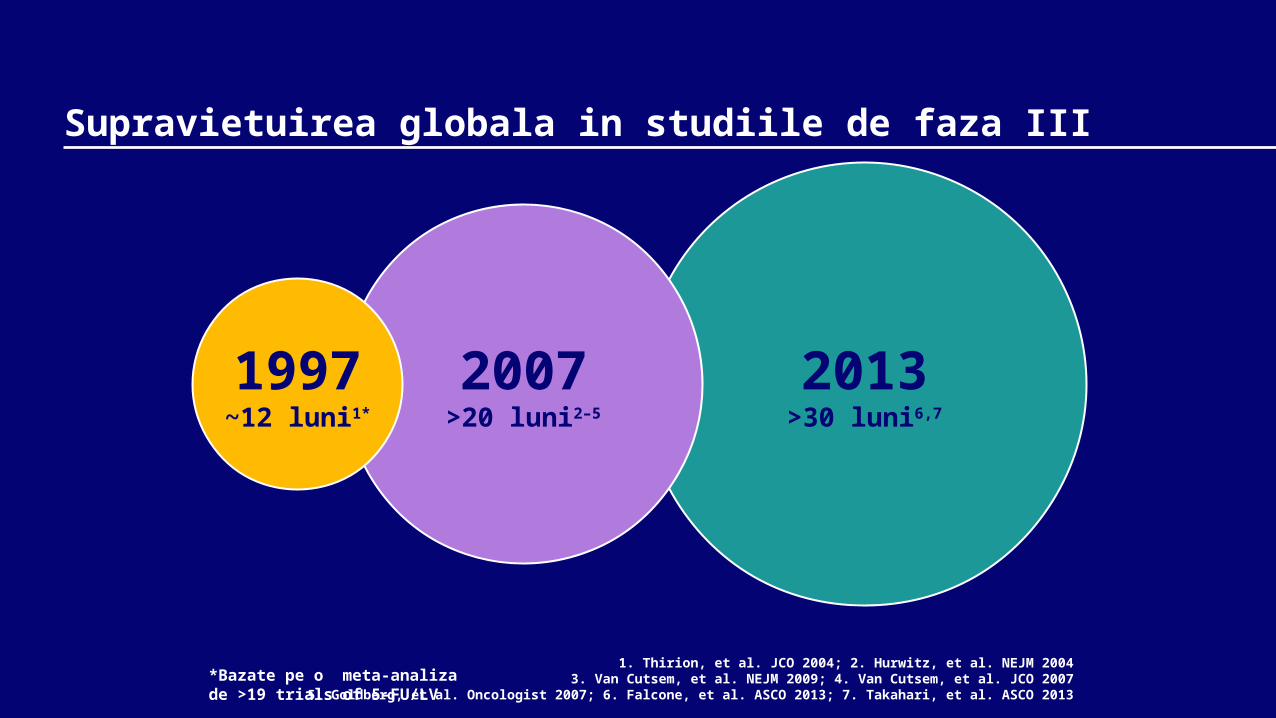
2013>30 luni6,7
Supravietuirea globala in studiile de faza III
2007>20 luni2–5
1997~12 luni1*
1. Thirion, et al. JCO 2004; 2. Hurwitz, et al. NEJM 20043. Van Cutsem, et al. NEJM 2009; 4. Van Cutsem, et al. JCO 2007
5. Goldberg, et al. Oncologist 2007; 6. Falcone, et al. ASCO 2013; 7. Takahari, et al. ASCO 2013*Bazate pe o meta-analizade >19 trials of 5-FU/LV
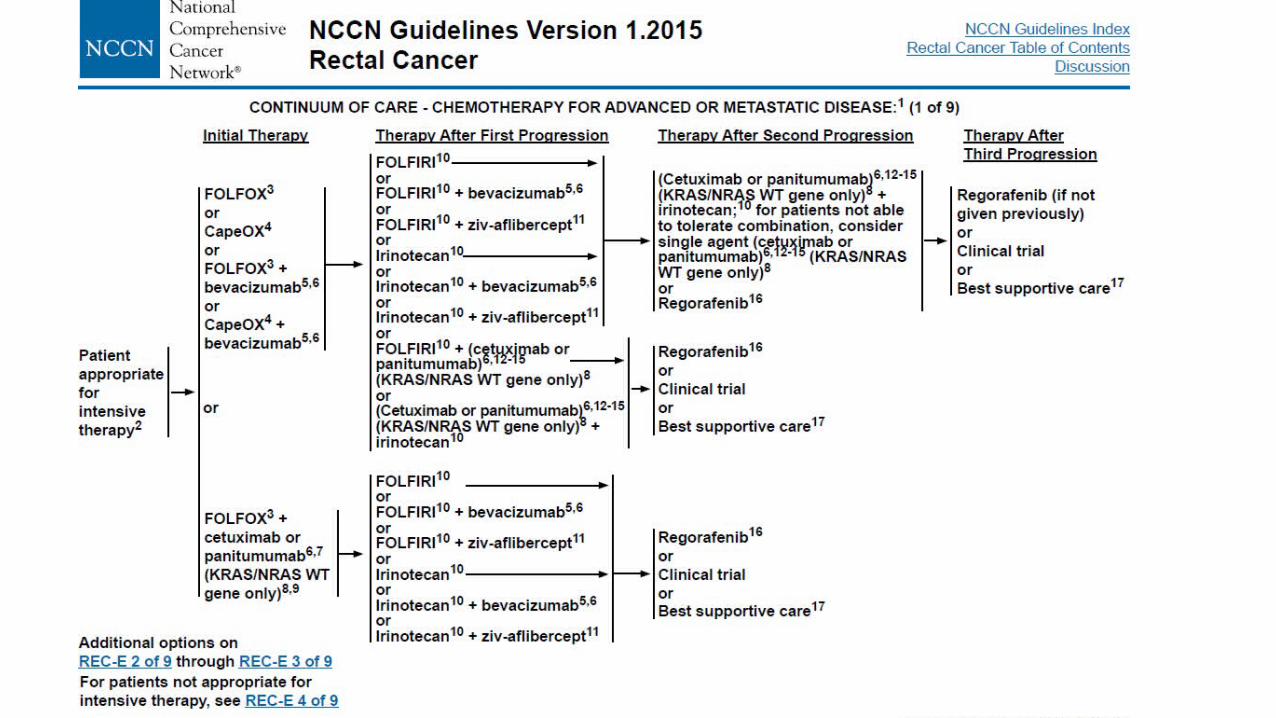
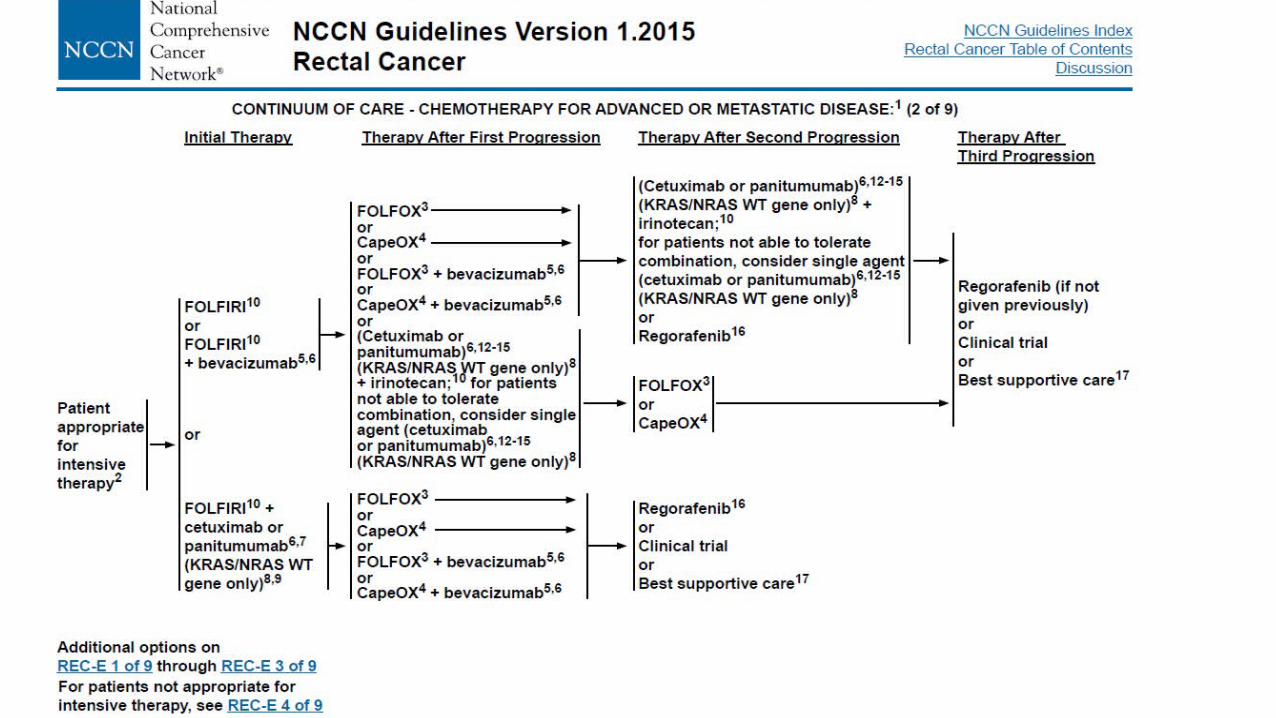
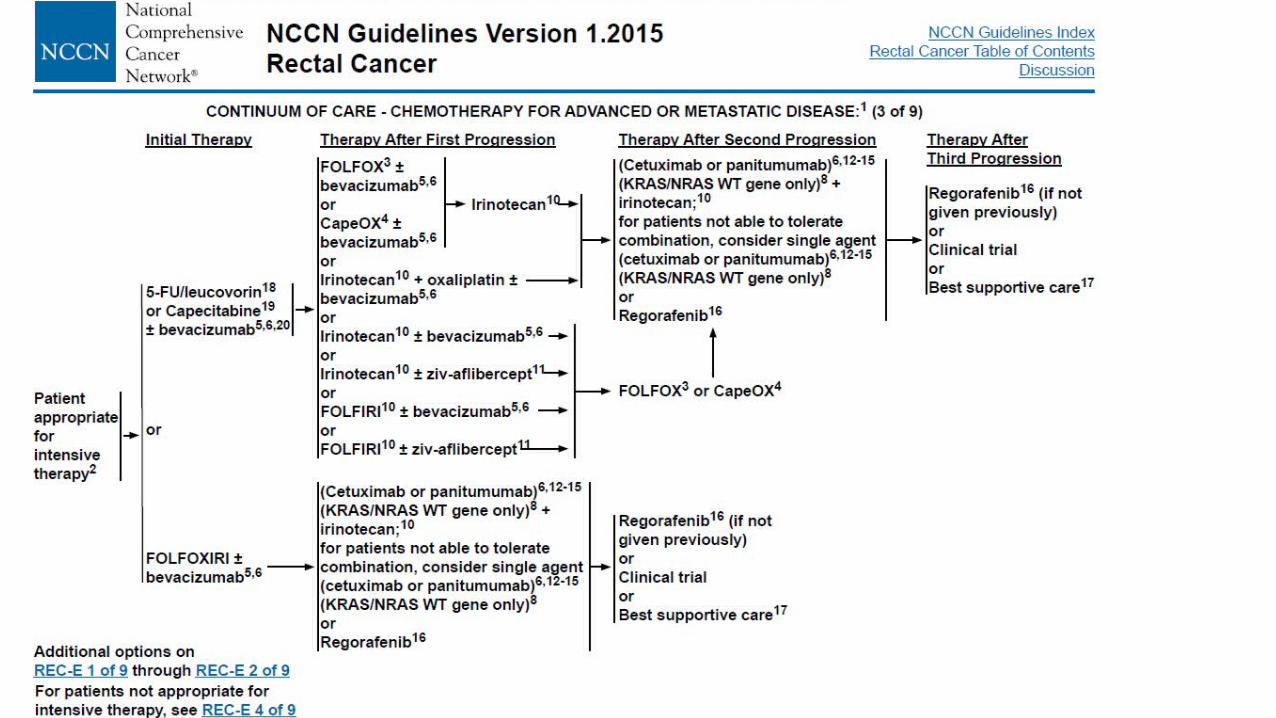
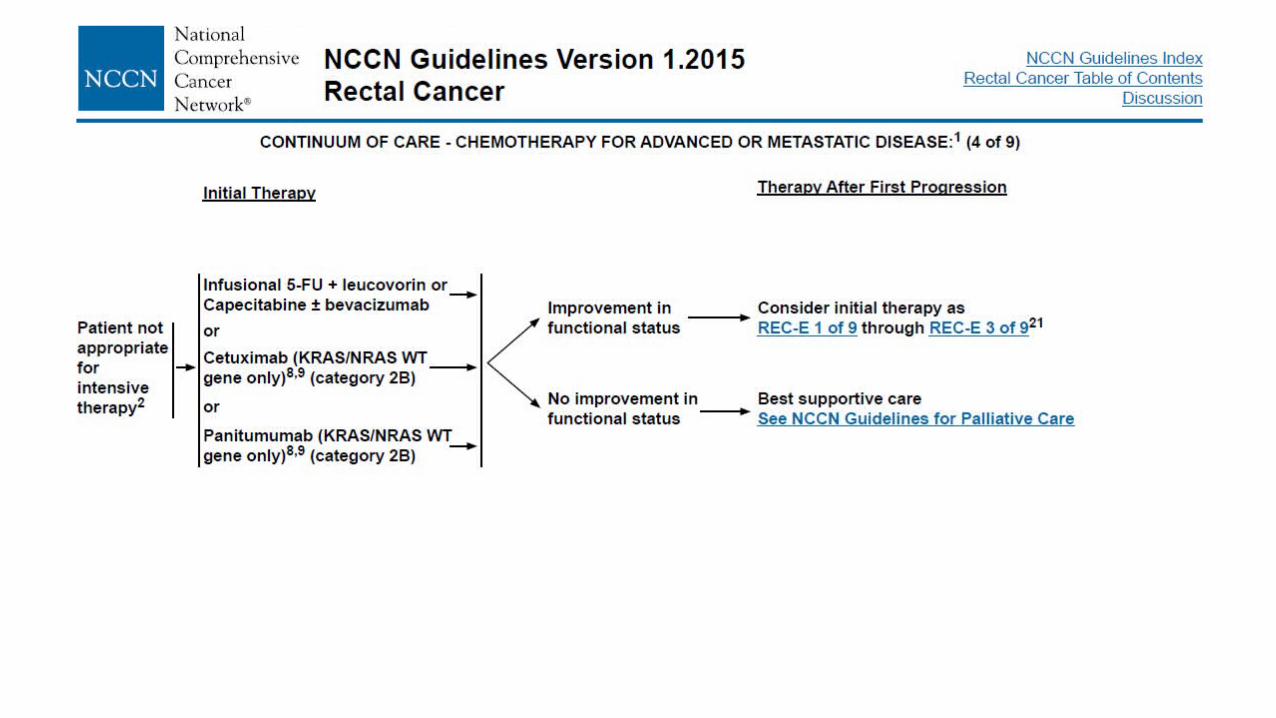
Cc de rect metastatic
Cc de colon / rect metastatic
Cc de colon / rect metastatic
Cc de colon / rect metastatic
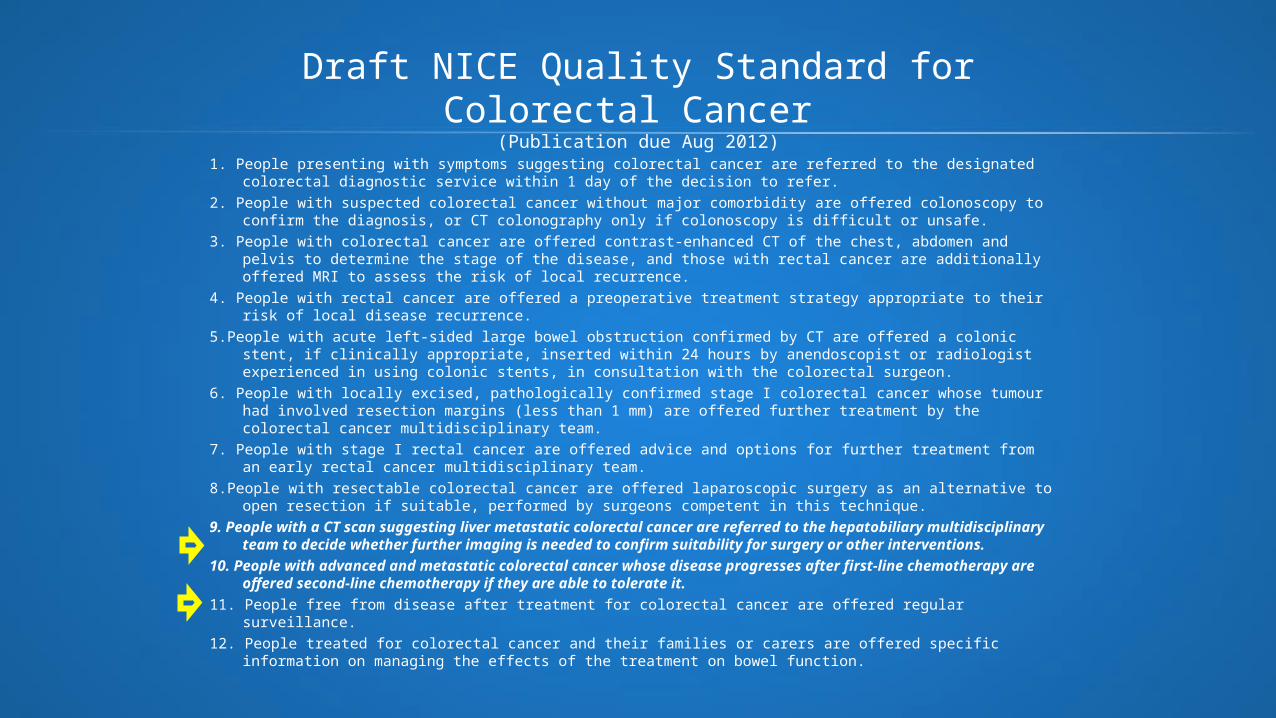
Draft NICE Quality Standard for Colorectal Cancer (Publication due Aug 2012)
1. People presenting with symptoms suggesting colorectal cancer are referred to the designated colorectal diagnostic service within 1 day of the decision to refer.
2. People with suspected colorectal cancer without major comorbidity are offered colonoscopy to confirm the diagnosis, or CT colonography only if colonoscopy is difficult or unsafe.
3. People with colorectal cancer are offered contrast-enhanced CT of the chest, abdomen and pelvis to determine the stage of the disease, and those with rectal cancer are additionally offered MRI to assess the risk of local recurrence.
4. People with rectal cancer are offered a preoperative treatment strategy appropriate to their risk of local disease recurrence.
5.People with acute left-sided large bowel obstruction confirmed by CT are offered a colonic stent, if clinically appropriate, inserted within 24 hours by anendoscopist or radiologist experienced in using colonic stents, in consultation with the colorectal surgeon.
6. People with locally excised, pathologically confirmed stage I colorectal cancer whose tumour had involved resection margins (less than 1 mm) are offered further treatment by the colorectal cancer multidisciplinary team.
7. People with stage I rectal cancer are offered advice and options for further treatment from an early rectal cancer multidisciplinary team.
8.People with resectable colorectal cancer are offered laparoscopic surgery as an alternative to open resection if suitable, performed by surgeons competent in this technique.
9. People with a CT scan suggesting liver metastatic colorectal cancer are referred to the hepatobiliary multidisciplinary team to decide whether further imaging is needed to confirm suitability for surgery or other interventions.
10. People with advanced and metastatic colorectal cancer whose disease progresses after first-line chemotherapy are offered second-line chemotherapy if they are able to tolerate it.
11. People free from disease after treatment for colorectal cancer are offered regular surveillance.12. People treated for colorectal cancer and their families or carers are offered specific information on managing the
effects of the treatment on bowel function.
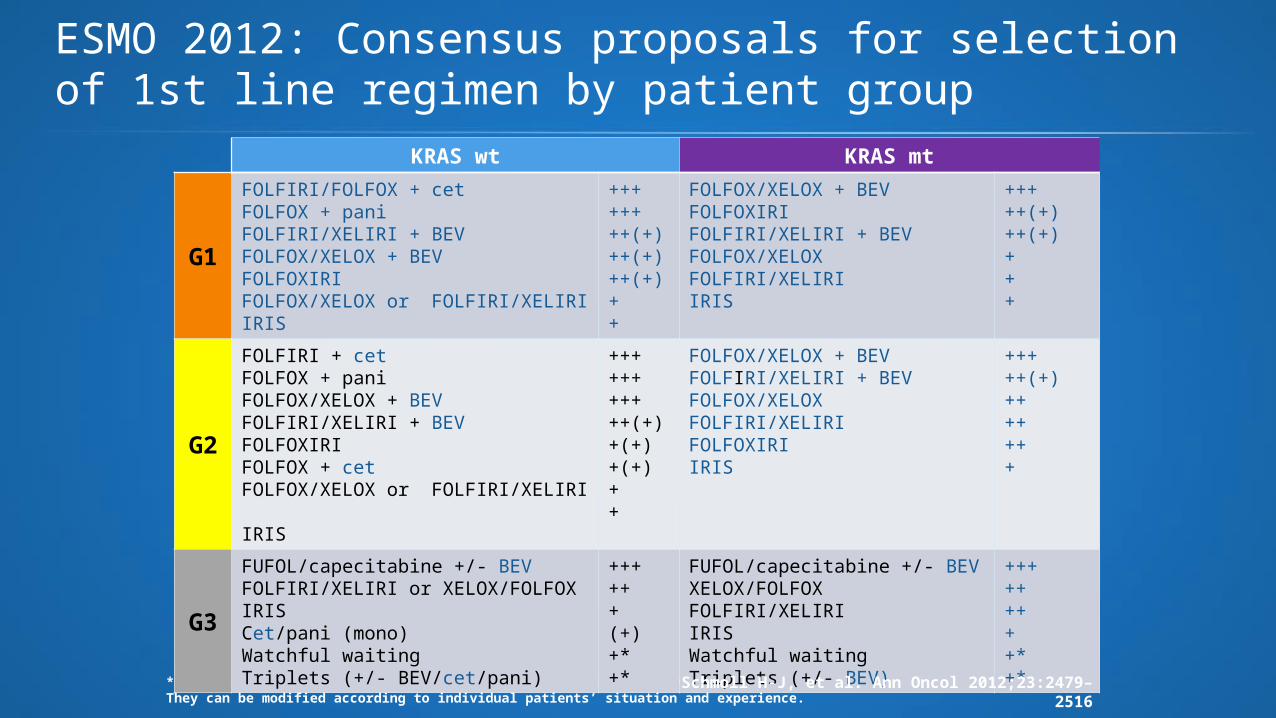
ESMO 2012: Consensus proposals for selection of 1st line regimen by patient group
*Selected patients; +/++/+++/(+) Consensus recommendation reflecting likelihood/uncertainty of efficacy. They can be modified according to individual patients’ situation and experience.
KRAS wt KRAS mt
G1
FOLFIRI/FOLFOX + cetFOLFOX + pani FOLFIRI/XELIRI + BEVFOLFOX/XELOX + BEVFOLFOXIRI FOLFOX/XELOX or FOLFIRI/XELIRIIRIS
++++++++(+)++(+)++(+)++
FOLFOX/XELOX + BEVFOLFOXIRI FOLFIRI/XELIRI + BEVFOLFOX/XELOX FOLFIRI/XELIRI IRIS
+++++(+)++(+)+++
G2
FOLFIRI + cetFOLFOX + pani FOLFOX/XELOX + BEVFOLFIRI/XELIRI + BEVFOLFOXIRI FOLFOX + cetFOLFOX/XELOX or FOLFIRI/XELIRI IRIS
+++++++++++(+)+(+)+(+)++
FOLFOX/XELOX + BEVFOLFIRI/XELIRI + BEVFOLFOX/XELOXFOLFIRI/XELIRI FOLFOXIRIIRIS
+++++(+)+++++++
G3
FUFOL/capecitabine +/- BEVFOLFIRI/XELIRI or XELOX/FOLFOXIRISCet/pani (mono) Watchful waitingTriplets (+/- BEV/cet/pani)
++++++(+)+*+*
FUFOL/capecitabine +/- BEVXELOX/FOLFOX FOLFIRI/XELIRIIRISWatchful waitingTriplets (+/- BEV)
+++++++++*+*
Schmoll H-J, et al. Ann Oncol 2012;23:2479–2516
Secvența corectă de tratament?• Rolul intervenției chirurgicale la cazuri la care nu
avem tulburări de tranzit sau sângerare?Cochrane Database Syst Rev. 2012 Aug 15;8Non-resection versus resection for an asymptomatic primary tumour in patients with unresectable stage IV colorectal cancer.Cirocchi R, Trastulli S, Abraha I, Vettoretto N, Boselli C, et all.
•Randomised controlled trials and non-randomised controlled studies
A total of 798 studies
1.086 patients (722 patients treated with primary tumour resection, and 364 patients managed first with chemotherapy and/or radiotherapy).
Resection of the primary tumour in asymptomatic patients .... is not associated with a consistent improvement in overall survival..... does not significantly reduce the risk of complications from the primary tumour (i.e. obstruction, perforation or bleeding).
Ann Surg Oncol. 2008 Dec;15(12):3440-6. Chemotherapy has also an effect on primary tumor in colon carcinoma.
Karoui M, et all.
CT induces major histological response in 70% of colon cancers.
Response to CT in the primary and the corresponding liver metastases are correlated.
These results support a policy of initial CT management for stage IV colon cancer and may warrant future studies of neoadjuvant CT in locally advanced colon carcinomas.
Mutation and Copy Number Discordance in Primary vs. Metastatic Colorectal Cancer (mCRC)<br />
Presented By Scott Kopetz at 2014 ASCO Annual Meeting
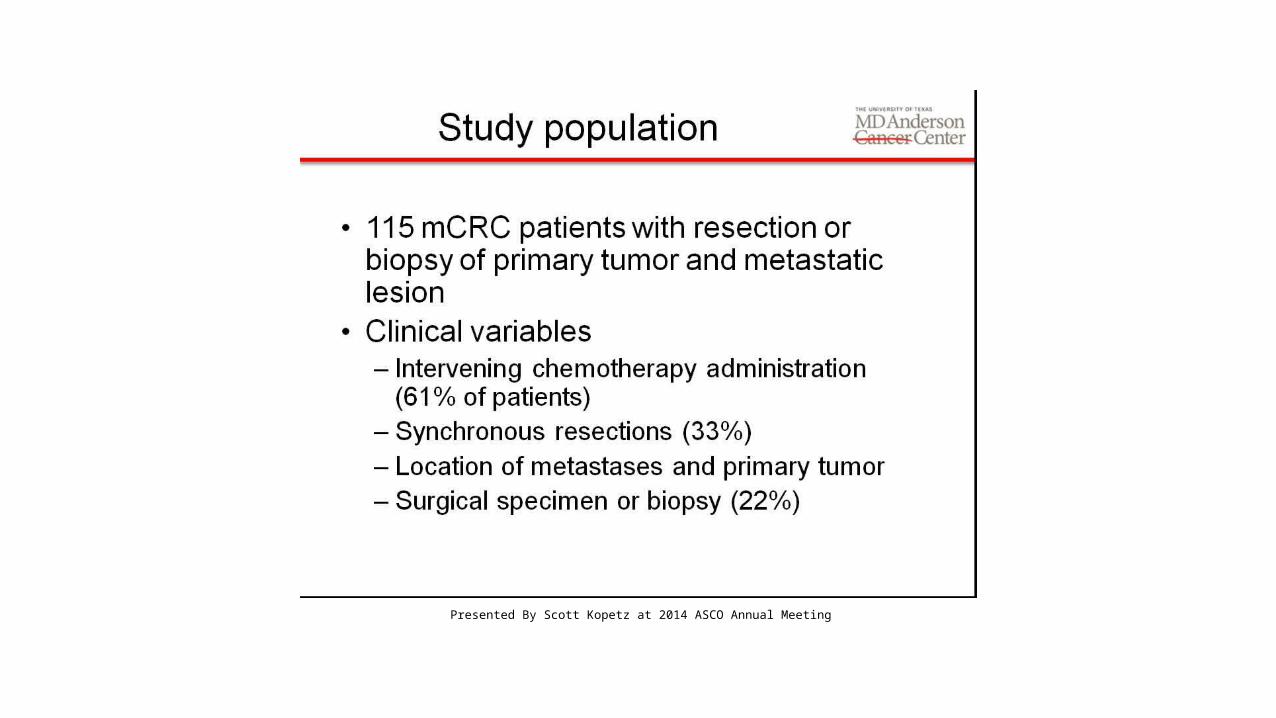
Study population
Presented By Scott Kopetz at 2014 ASCO Annual Meeting
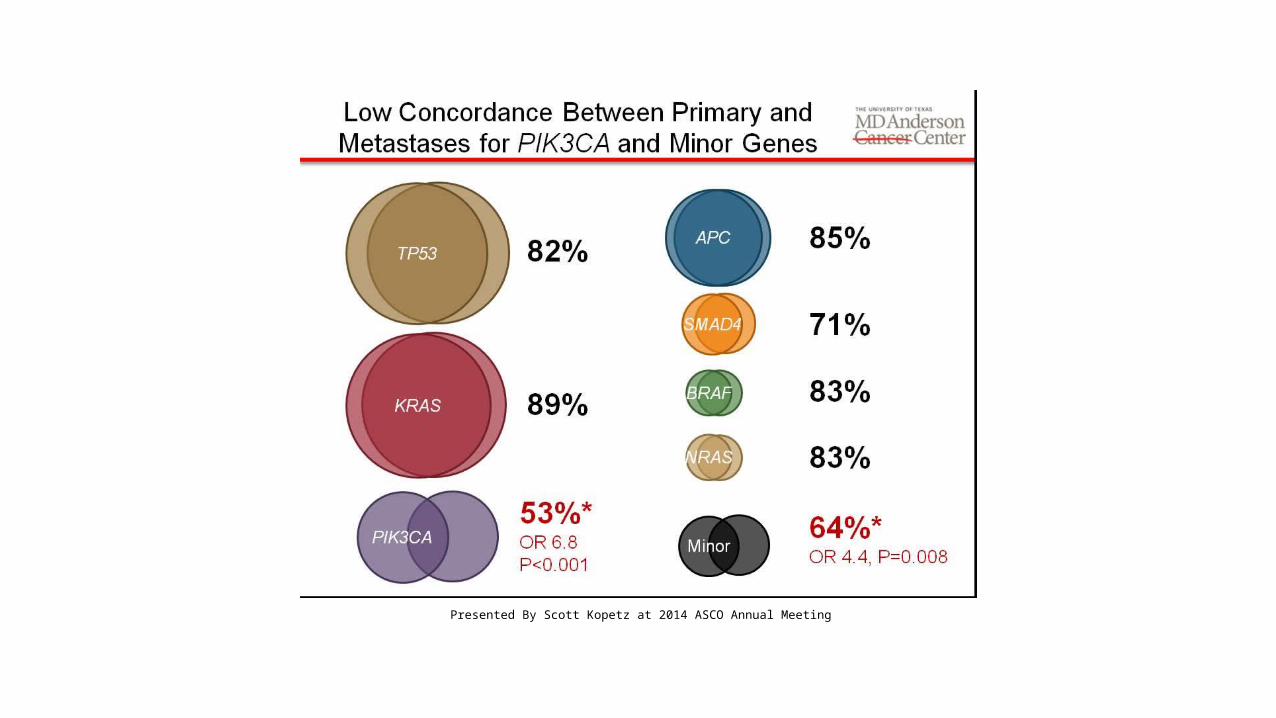
Low Concordance Between Primary and Metastases for PIK3CA and Minor Genes
Presented By Scott Kopetz at 2014 ASCO Annual Meeting
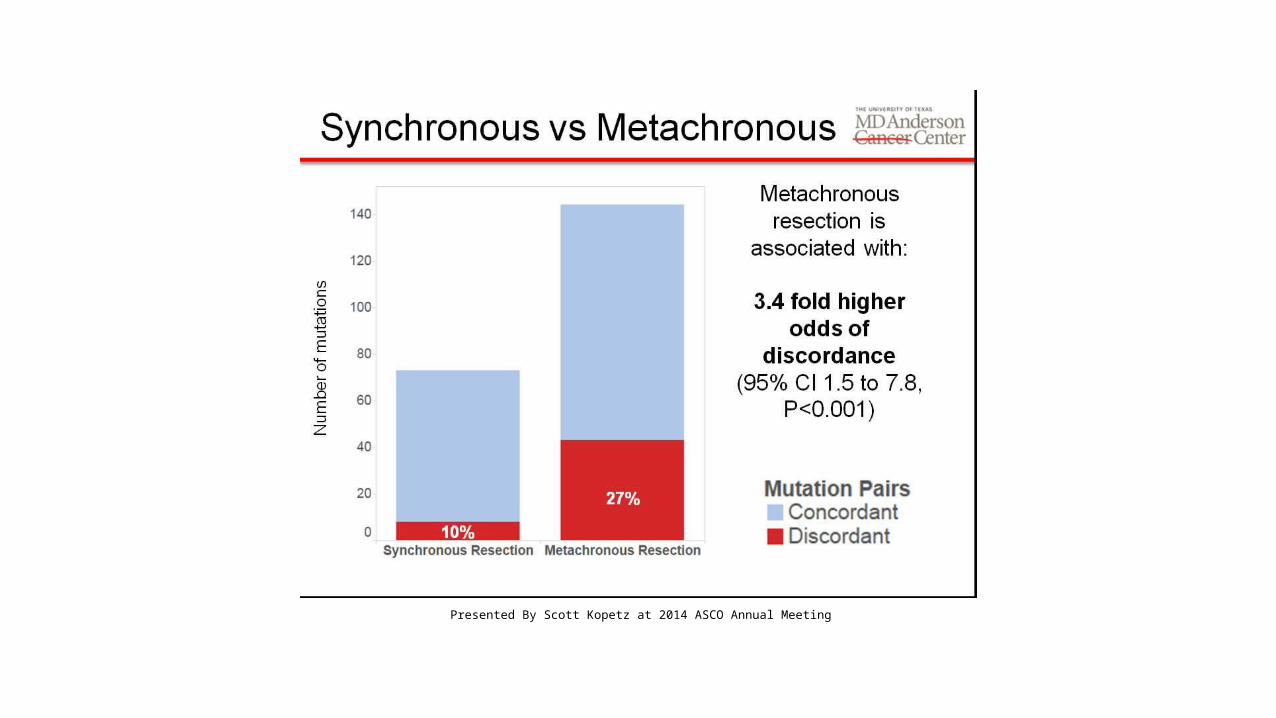
Synchronous vs Metachronous
Presented By Scott Kopetz at 2014 ASCO Annual Meeting
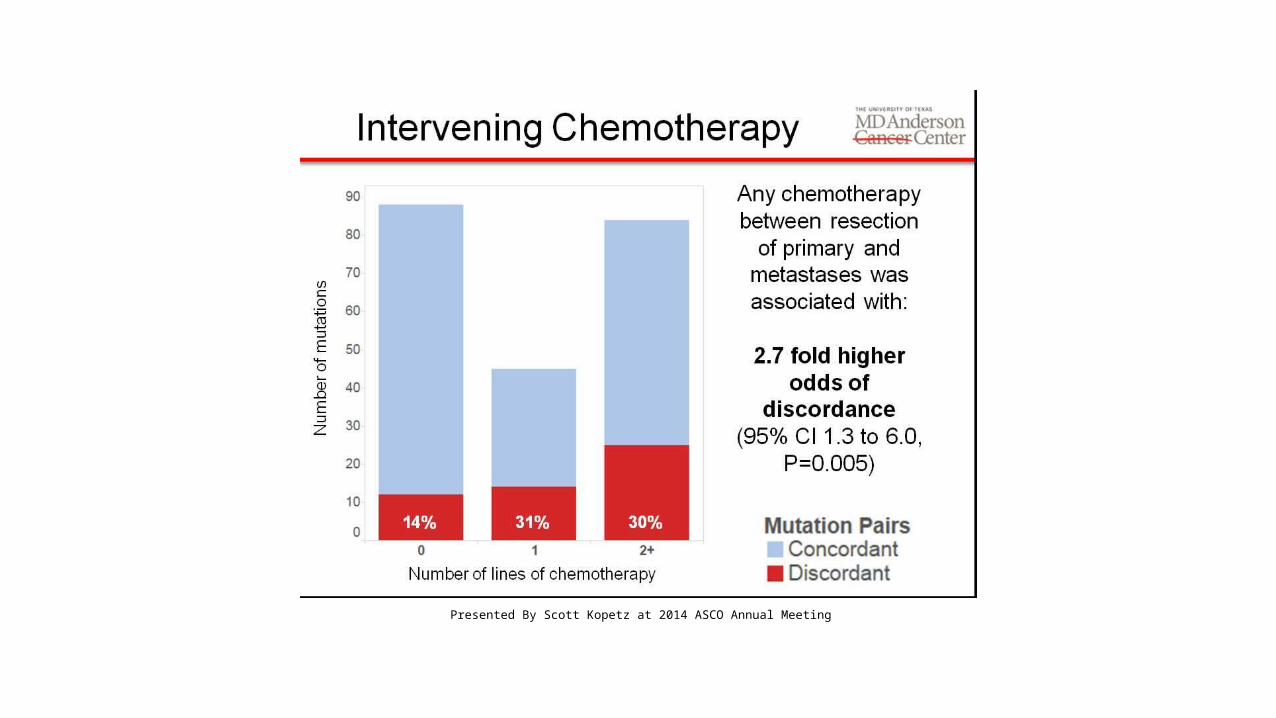
Intervening Chemotherapy
Presented By Scott Kopetz at 2014 ASCO Annual Meeting
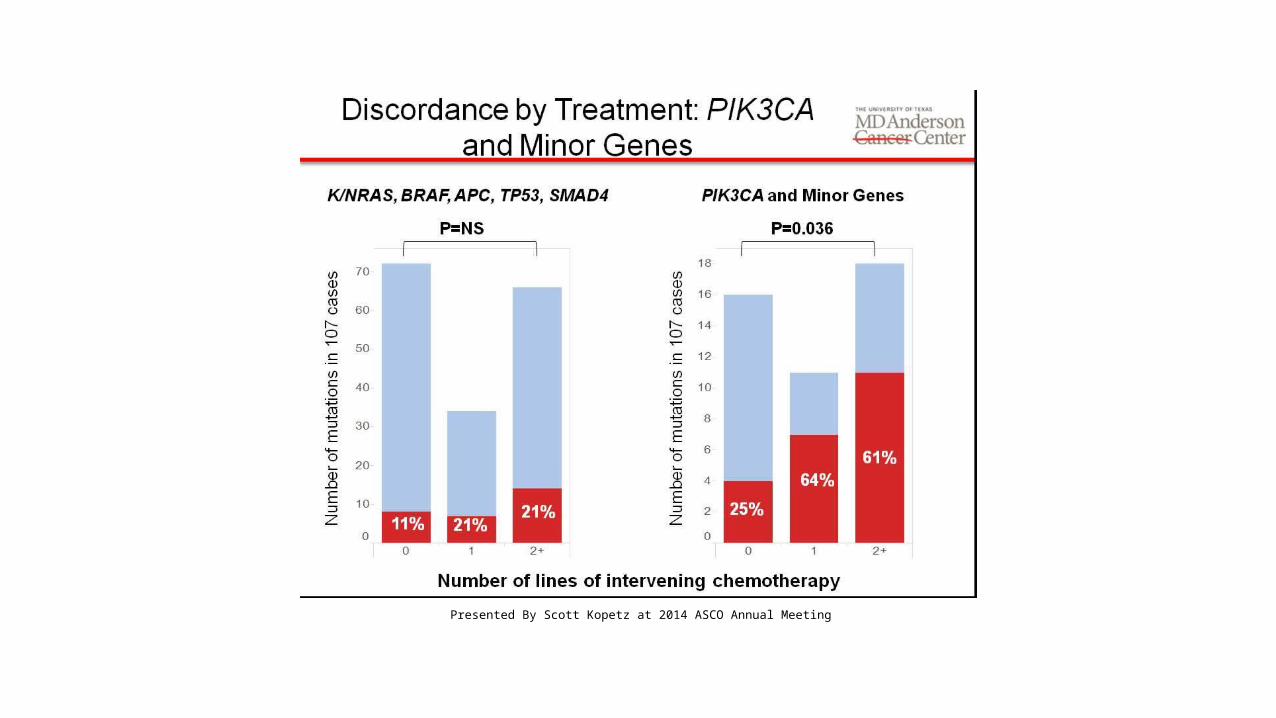
Discordance by Treatment: PIK3CA and Minor Genes
Presented By Scott Kopetz at 2014 ASCO Annual Meeting
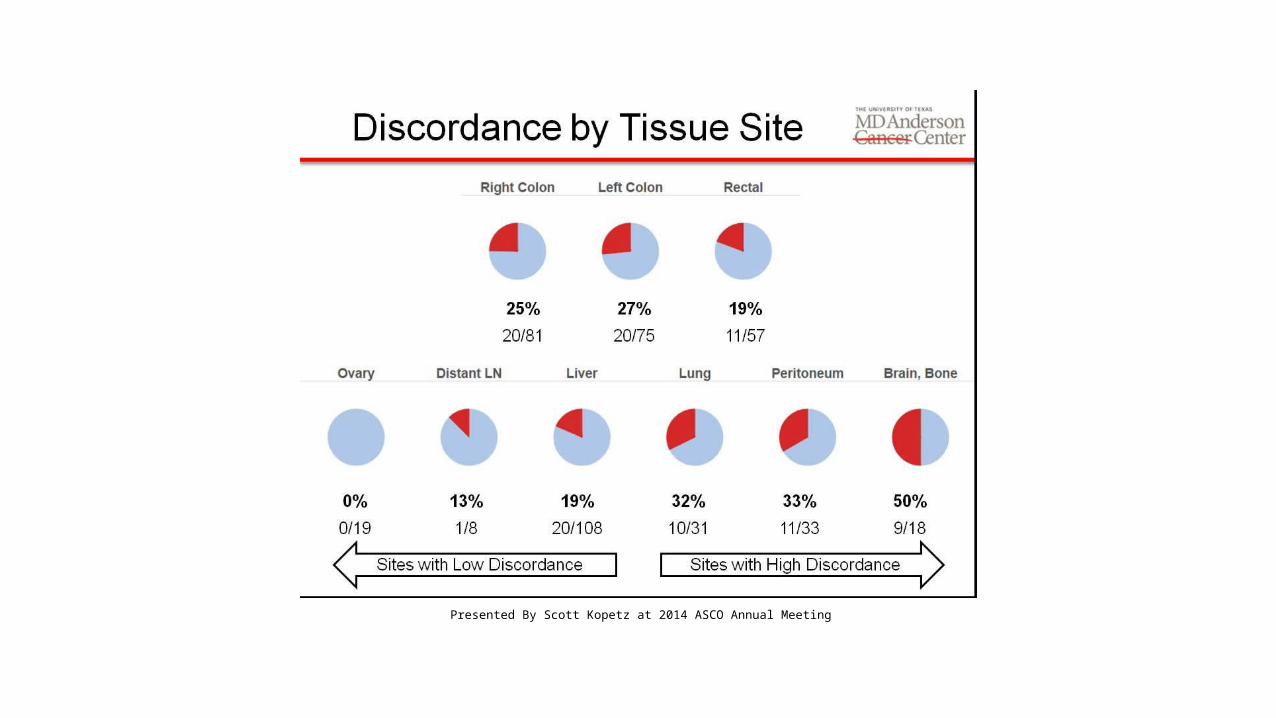
Discordance by Tissue Site
Presented By Scott Kopetz at 2014 ASCO Annual Meeting
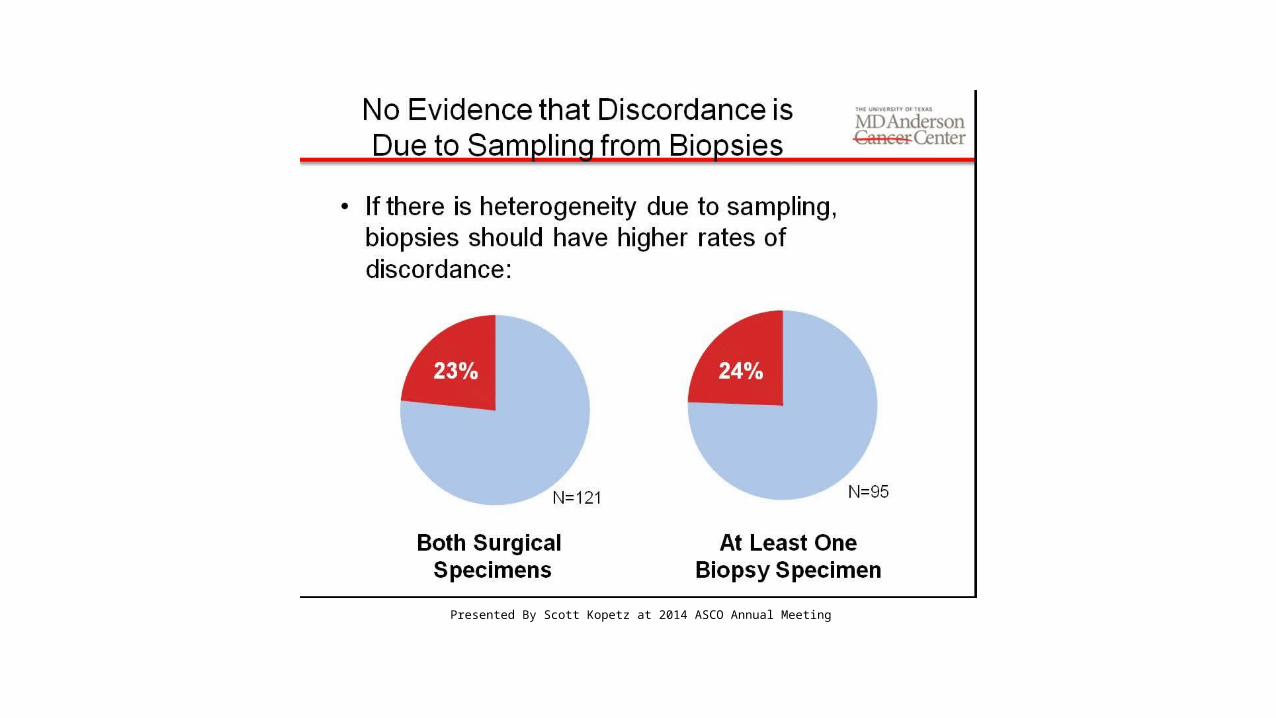
No Evidence that Discordance is <br />Due to Sampling from Biopsies
Presented By Scott Kopetz at 2014 ASCO Annual Meeting