Embed Size (px)
DESCRIPTION
A Journal for Physicians
Citation preview
ElEctronic MEdical rEcords
p. 4
cath lab sEts standard
p. 8
PulMonology drug rEsEarch
p. 10
raPid assEssMEnt tEaM
p. 12
diagnosing joint Pain
p. 15
transPort adds sErVicE
p. 18
a journal for PhysiciansissuE 2, 2009
Proudly serving children since 1948, children’s hospital & Medical center is the only full-service, pediatric health care center in nebraska. located in omaha, it provides expertise in more than 30 pediatric specialty services to children and families across a five-state region and beyond. the 145-bed, nonprofit hospital houses the only dedicated pediatric emergency department in the region and offers 24-hour, in-house services by pediatric critical care specialists. children’s hospital & Medical center has achieved the Magnet designation for nursing excellence and is an infoWorld 100 award winner for innovation in information technology. a pediatric affiliation established between children’s hospital & Medical center and the university of nebraska Medical center college of Medicine supports enhancements in pediatric education, research and clinical care. children’s is also the primary teaching site for the family practice and joint pediatric residency programs at creighton university and unMc. for more information on children’s hospital & Medical center go to childrensomaha.org.

PulMonology drug rEsEarch shoWs ProMisE
p. 10 children’s is playing a significant role in research studies involving several new pulmonary-related drugs. six promising cystic fibrosis drug studies are currently underway.
raPid assEssMEnt tEaM has iMPact
p. 12 formal assessment team can be activated to bring a “second set of eyes” to the bedside to serve as an early warning system.
diagnosing joint Pain
p. 15 Myriad causes of pediatric joint pain call for accurate diagnosis by a physician or subspecialist who can make a determination based on physical examination.
cath lab sEts standard
p. 8 Visitors from around the country come to children’s, designated as a toshiba show site, to see the cath lab and talk with the medical professionals who use it.
ElEctronic rEcords rEducE Errors
p. 4 children’s award-winning computerized medical records and order entry systems reduce prescription and transcription errors.
contEnts
tracking h1n1
p. 7
nEW Physicians
p. 17
outrEach clinic schEdulE
p. 19
also:
childrEn’s connEction adVisory council
shahab f. abdEssalaM, M.d.daVid M. christEnsEn, M.d.brady a. kErr, M.d.john d. kuglEr, M.d.josEPh t. (jay) snoW, M.d.jayEsh c. thakkEr, M.d.don W. coultEr, M.d.PEggy hogan, r.n., Physician liaison
transPort adds sErVicE
p. 18 With a new, colorful ambulance and enhanced pediatric and newborn service, children’s expert transport team bridges the gap between children’s hospital & Medical center and other medical facilities.
ElEctronic MEdical rEcords iMProVE PatiEnt outcoMEs
ElEctronic MEdical rEcords
p. 4

There could be millions of reasons why Children’s Hospital & Medical Center is determined to implement electronic medical records (EMR), computerized physician order entry (CPOE) and other information technology advancements throughout the hospital and Children’s Physicians pediatric offices. After all, the federal government is offering $48.8 billion in American Recovery and Reinvestment Act funds to medical facilities and hospitals that implement and demonstrate “meaningful use” of an EMR system. There’s even the reported cost savings technology may provide.
At Children’s, however, there is only one primary reason to adopt the latest in information technology systems, says Chief Medical Informatics Officer George Reynolds, M.D., MMM, associate professor of Pediatrics, UNMC College of Medicine.
The patient.
“Children’s has been traveling down that path toward fully electronic records and voluntary CPOE for several years, long before the Recovery Act program was announced,” Dr. Reynolds says. “And we’ve continued doing it, not because of the potential government payments, but because it’s right for the patient.
“The promise of significant government money is nice, but improving outcomes and reducing medical errors is priceless.”
Children’s went live with CPOE in its Pediatric Intensive Care Unit (PICU) in June 2007. “We started with the PICU because we felt the people there would be highly motivated to tackle the new technology,” Dr. Reynolds says.
The hospital has since gone live with CPOE in its Newborn Intensive Care Unit, the medical-surgical areas, the emergency department and the operating room areas.
“We’ve reached 87 percent adoption of CPOE,” Dr. Reynolds says, “and that percentage continues to go up.”
The hospital utilizes the Eclipsys system for its inpatient areas, and the Epic system for the ambulatory side, where Children’s Physicians network of area offices has been fully electronic for nearly two years. Specialty physicians have been converting to electronic records since the summer of 2008 and were expected to be completely switched by the end of 2009.
From comprehensive management of medical information and its secure exchange, to the improvement of patient care through reduced errors, health information technology (IT) is a valuable tool, Dr. Reynolds says.
“IT makes patient data universally available,” he says. “Whether a physician is at the patient’s bedside, or in his medical office, or on vacation, he or she can still communicate with
and see the patient’s medical records.”
Health IT has the potential to improve health care quality, increase the efficiency of care provision, reduce unnecessary health care costs, increase administrative efficiencies, decrease paperwork and expand access to affordable care. “That’s tremendously powerful,” Dr. Reynolds says.
CPOE, combined with clinical decision support (CDS), is making a positive impact at Children’s by reducing the number of prescribing and transcription errors by 60 percent.
“The physician can prescribe a medication and the computer will be able to analyze the patient data and advise on dose, range, allergies and other factors,” Dr. Reynolds says. “As patients and the management of their data get more complex, it can be virtually impossible to stay on top of it all. With CDS, the computer does that for you by acting as a guide.”
CDS signals an on-screen alert when the order is in question for that particular patient. These alerts fire regardless of whether the order is being entered directly by the physician (CPOE) or is being transcribed by a nurse or pharmacist.
“We’ve seen 40 percent fewer CDS alerts when using CPOE, compared to non-CPOE orders,” Dr. Reynolds says. “They are exactly the same alerts for the same reasons, yet CPOE has
“WHETHER A PHySICIAN IS AT THE PATIENT’S bEDSIDE, IN HIS OFFICE, OR ON vACATION, HE OR SHE CAN STIll COMMUNICATE WITH AND SEE THE PATIENT’S MEDICAl RECORDS.”
gEorgE rEynolds, M.d., MMMchiEf MEdical inforMatics officErassociatE ProfEssor of PEdiatrics, unMc collEgE of MEdicinE
p. 5
Physicians’ Priority linE 1.888.592.7955

Children’s is playing a vital role in the fight against H1N1 swine flu by helping the state of Nebraska actively track H1N1 in young people.
Children’s provides daily reports to the Nebraska Department of Health and Human Services based on the number of children seeking care for influenza-like symptoms in the hospital’s Emergency Department.
“As our numbers increased, we identified the need to provide flu-specific tracking,” said Megan Connelly, Emergency Department (ED) manager. “The ED staff worked closely with IT to develop an electronic report that could help us easily determine how many probable flu cases we were seeing each day.”
The tracking began Sept. 2, 2009 and shows a dramatic increase in children seeking care for symptoms associated with H1N1. Specific categories include cough, fever, sore throat, and general “flu-like” symptoms.
“We can immediately see the trend, and even drill down to the hours of the day when we’re seeing the most children in the Emergency Department. Over the long term, we would hope our tracking can help the state determine when and if H1N1 activity has reached its peak in the pediatric population.”
The surveillance may also be of interest to the national Centers for Disease Control and Prevention as health experts work to learn more about H1N1 and its particular impact on children.
EMErgEncy dEPartMEnt suPPorts nEbraska’s PEdiatric h1n1 tracking Efforts
tracking h1n1
p. 7
cath lab continuEs to sEt standard for diagnostic iMaging
cath lab sEts standard
p. 8

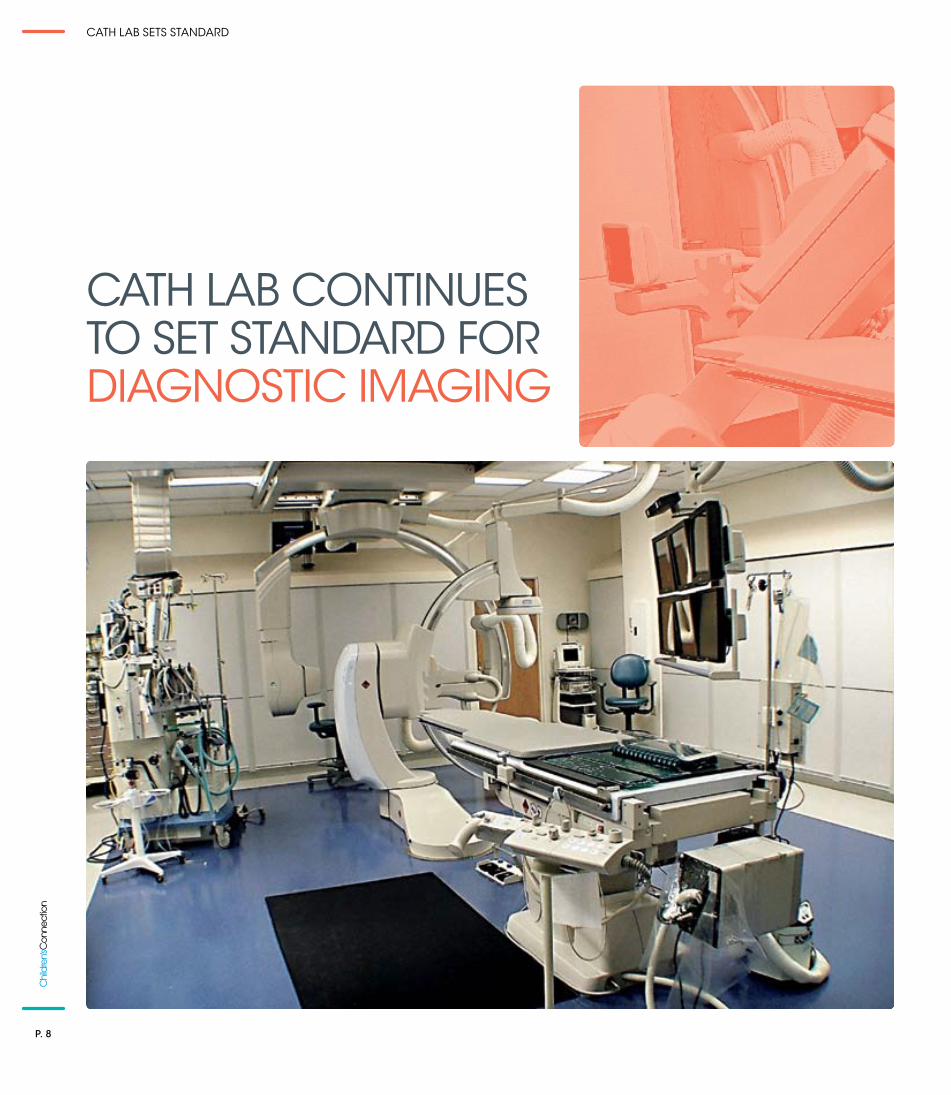
The 4-month-old baby was brought to Children’s Hospital & Medical Center by helicopter with a racing heart that could not be slowed by medicine.
Rushed to the state-of-the-art Hybrid Catheterization & Electrophysiology laboratory at Children’s, a catheter was inserted to produce a 3D image of the baby’s heart electrically and pinpoint the source of the arrhythmia.
“Once we found the cells that were the focus of the rapid heartbeat, we treated the heart with ablation, sending radio-frequency energy to the tip of the catheter to kill those cells,” says laboratory Manager Stacey Froemming, RCPT. “We created a scar on the muscle of that part of the heart to block those signals. It worked remarkably well.”
An amazing procedure on a heart no bigger than a golf ball, made possible in large part by the catheterization lab, one of the largest and most advanced in the nation.
The 1,000-square-foot facility features a Toshiba flat panel diagnostic imaging X-ray system, capable of rotating 180-degrees in multiple planes around the patient while still capturing high-resolution images and affording patient access to several medical specialists at the same time.
In April, Children’s and Toshiba American Medical Systems entered into a formal
agreement recognizing the lab as an official “Toshiba Show Site.” visitors from around the country come to Children’s to see the lab and speak with the medical professionals who use it.
The agreement with Toshiba gives Children’s “the vehicle and the mechanism to have continuing access to the best equipment available,” says Children’s Interventional Cardiologist Jeffrey Delaney, M.D., assistant professor of Pediatrics, UNMC College of Medicine. “Toshiba has done this for us so we can offer our patients a lab that really has no peer in the United States.”
As part of the agreement, the flat panel detectors and X-ray tubes were recently replaced with Toshiba’s newest high-resolution detector and high heat x-ray tube. Children’s was the first lab in the country to be retrofitted with these newest products and software.
“The flat panel detectors increased the resolution and are much more efficient in creating the digital image,” Froemming says. “X-ray tube power is rated according to heat capacity. The upgrade increased our heat capacity from 1.5 million units to 5 million. That’s astounding.”
In September 2008, invasive electrophysiology including catheter ablation procedures were moved to Children’s. This allows patients to undergo multiple diagnostic procedures without transferring between two facilities.
Patient volume for the lab at Children’s is expected to be up from about 350 in 2008 to between 350 and 400 in 2009, Froemming says.
“We are able to accommodate the volume thanks to having the most advanced equipment available and a medical team with the training and experience to utilize it to its fullest extent,” he says. “Our reputation and prominence among pediatric hybrid cath labs in the U.S. is pretty much unequalled.”
“WE can offEr our PatiEnts a lab that rEally has no PEEr in thE unitEd statEs.”jEffrEy dElanEy, M.d.intErVEntional cardiologistchildrEn’s hosPital & MEdical cEntErassistant ProfEssor of PEdiatrics, unMc collEgE of MEdicinE
Physicians’ Priority linE 1.888.592.7955
p. 9
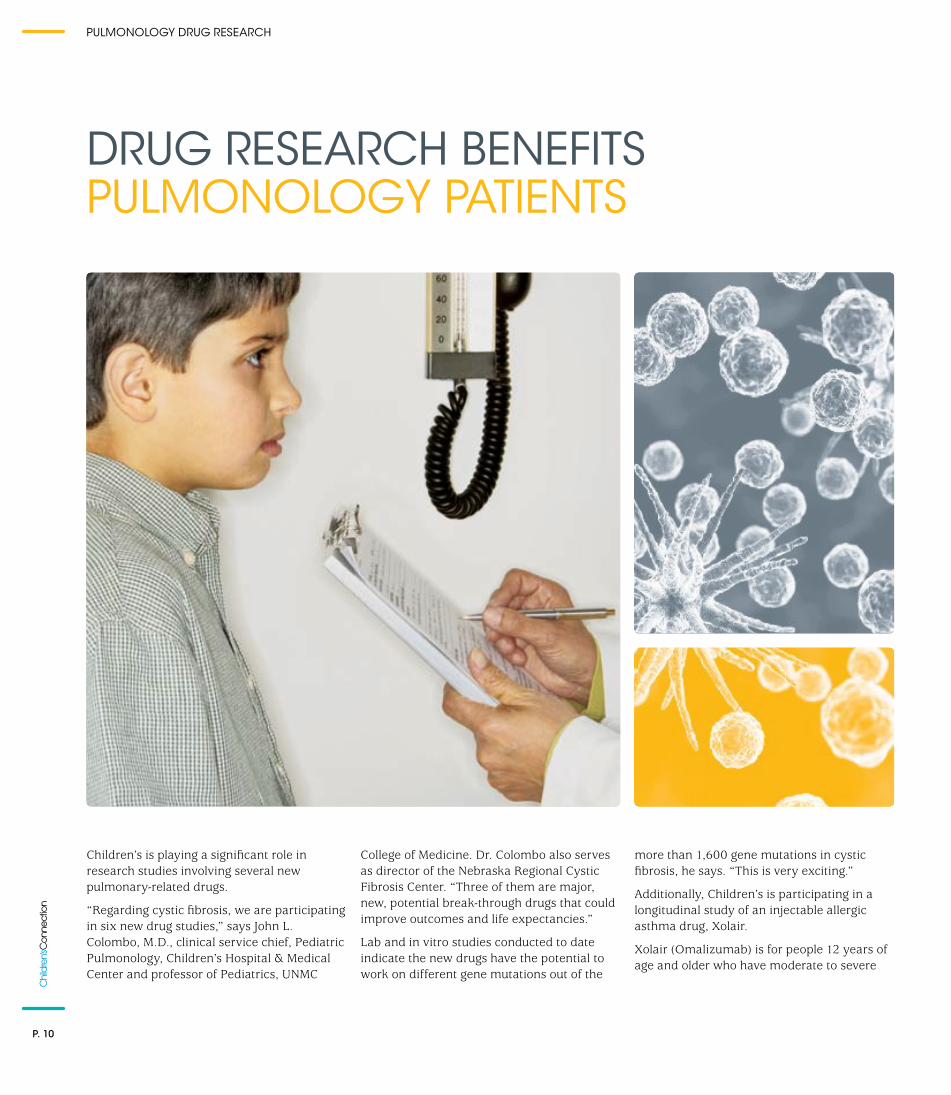
Children’s is playing a significant role in research studies involving several new pulmonary-related drugs.
“Regarding cystic fibrosis, we are participating in six new drug studies,” says John l. Colombo, M.D., clinical service chief, Pediatric Pulmonology, Children’s Hospital & Medical Center and professor of Pediatrics, UNMC
College of Medicine. Dr. Colombo also serves as director of the Nebraska Regional Cystic Fibrosis Center. “Three of them are major, new, potential break-through drugs that could improve outcomes and life expectancies.”
lab and in vitro studies conducted to date indicate the new drugs have the potential to work on different gene mutations out of the
more than 1,600 gene mutations in cystic fibrosis, he says. “This is very exciting.”
Additionally, Children’s is participating in a longitudinal study of an injectable allergic asthma drug, Xolair.
Xolair (Omalizumab) is for people 12 years of age and older who have moderate to severe
drug rEsEarch bEnEfits PulMonology PatiEnts
PulMonology drug rEsEarch
p. 10

persistent asthma that is triggered by year-round allergens in the air. Xolair helps reduce the number of attacks in people with allergic asthma who still have asthma symptoms even though they are taking inhaled steroids.
“It’s an extremely effective drug,” Dr. Colombo says, “but it’s only for difficult, poorly controlled asthma cases.”
The body produces the antibody Immunoglobulin E (IgE) in response to certain allergens. For many people with asthma, IgE triggers the release of chemicals which may lead to an allergic asthma attack.
Xolair is the only anti-IgE therapy available. It works by binding to the antibody and preventing it from being active. The drug lasts from two to four weeks, depending on the dosage, Dr. Colombo says.
The FDA-mandated, Phase Iv study is currently in its fourth year of five. Children’s and UNMC are two of 400 sites nationwide participating in the study, he says, “and we have the second highest average patient year data being collected.”
Researchers are seeing indications that Xolair might also be effective on allergies besides asthma, he says, such as eczema and allergic rhinitis. “It has tremendous potential and I believe it will prove to be a very valuable treatment.”
Dr. Colombo received his medical degree from UNMC in 1975. He completed his pediatric residency at UNMC in 1978 and his pediatric pulmonary fellowship at Tulane University School of Medicine in New Orleans in 1981. In addition to his duties at Children’s, he is professor of Pediatrics and a graduate faculty member at UNMC.
Swallowing is so natural that unless we have a sore throat, most of us never think about it. yet there are children with maladies of the trachea or esophagus, or head and neck problems for whom swallowing is next to impossible.
And that makes vital actions like eating – and in many cases, sleeping – equally difficult.
“Some pediatric patients have a complete aversion to having anything in their mouths, including food,” says John l. Colombo, M.D., director of the combined Children’s and University of Nebraska Medical Center (UNMC) Pediatric Pulmonology Division. “Others eat but aspirate food into their lungs. A lot of them have sleep problems as well.”
The pediatric specialists at Children’s help meet the needs of these patients through the Aerodigestive Clinic and the Sleep Disorders Clinic, the only programs of their kind in the region.
The Aerodigestive Clinic treats children with pulmonary, gastrointestinal and ear, nose or throat problems by bringing together pulmonologists, gastroenterologists, ear nose and throat physicians, speech therapists,
dietitians and nurses who are specially trained to treat these disorders.
Some patients are on ventilators or have tracheostomy tubes. “The most common time they need these is when they sleep, yet the very thing they need to breathe during sleep may interfere with it,” Dr. Colombo says. “because of their technology dependency, some of these kids have extreme difficulty getting the sleep their bodies require.”
He says Children’s is in the process of expanding the Sleep Centers lab from three beds to four. Patients come in and spend the entire night while being monitored for sleep difficulties. Parents are allowed to stay the night.
“There are many adult sleep programs, but we are one of very few pediatric programs, and the only one in Nebraska and the region that serves all-age children,” says Dr. Colombo.
The sleep clinic includes a psychologist and a pediatric pulmonologist who are board certified in sleep medicine. “That, too, is a rarity,” Dr. Colombo says.
“REGARDING CySTIC FIbROSIS, WE ARE PARTICIPATING IN SIX NEW DRUG STUDIES. THREE OF THEM ARE MAJOR, NEW, POTENTIAl bREAk-THROUGH DRUGS THAT COUlD IMPROvE OUTCOMES AND lIFE EXPECTANCIES.”
john l. coloMbo, M.d.clinical sErVicE chiEf, PEdiatric PulMonologychildrEn’s hosPital & MEdical cEntErProfEssor of PEdiatrics, unMc collEgE of MEdicinE
clinics sErVE uniquE nEEds of PatiEnts With sWalloWing disordErs
p. 11
Physicians’ Priority linE 1.888.592.7955
When it comes to Code 4 events occurring outside the Intensive Care Unit, fewer is definitely better.
In 2007, there were 12 such events at Children’s Hospital & Medical Center. In 2009 through October, there were none.
What changed?
In May of 2008, Children’s implemented a Rapid Assessment Team (RAT) program. The team is comprised of clinical staff who “bring a second set of eyes to the patient bedside,” says Donnetta Perkins, R.N., PMP, manager of programs and systems development at Children’s.
Initially established to respond to requests for assessment from hospital medical staff, the program has since been expanded to include “Condition Help,” which allows a patient’s family member to ask for an activation of the team.
The goal is to improve patient care by identifying those who are clinically deteriorating and are at increased risk for cardiac or respiratory arrest. “by identifying these at-risk patients early, we can monitor them more closely, and move them to ICU if necessary prior to a critical event,” Perkins says.
The RAT is similar to initiatives in place at other U.S. children’s hospitals. Many were prompted by the nationally publicized case of Josie king, an 18-month-old girl who died in 2001 at the Johns Hopkins Children’s Center in baltimore after a series of miscommunications and medical errors.
Josie’s mother, Sorrel king, has since crusaded to encourage family involvement in the care of pediatric patients, and to emphasize the need for open, respectful and informative communication between patient families and medical caregivers. The Josie king Foundation
raPid assEssMEnt tEaM targEts non-icu codE 4 EVEnts
raPid assEssMEnt tEaM
p. 12

promotes a number of safety initiatives, including Condition Help, which seeks to empower patient families to activate an early response team.
The implementation of a formal assessment team at Children’s replaces informal procedures that had existed for many years, Perkins says. “Prior to having the RAT, if there were questions concerning a patient’s condition, a call would be placed to the attending physician, or the staff would call our PICU and the charge nurse or intensivist would come and examine the child.”
In devising the team at Children’s, a committee examined several initiatives aimed at improving patient safety and mortality, including those promoted by the Institute for Healthcare Improvement (IHI).
Concerns were addressed regarding decisions being made without informing the attending physicians, and the number of times a critical care intensivist might be called upon as part of the team. Instead, a hospitalist was incorporated as the team’s lead physician, Perkins says, and every possible attempt is made to contact the attending physician prior to activating the assessment team.
In its first year, there were 12 activations of the RAT at Children’s by hospital medical personnel. Through September 2009, there were 10.
Meanwhile, the number of Code 4 events occurring outside the ICU dropped from 12 in 2007 to three in 2008 – and to zero through September 2009.
“The Rapid Assessment Team appears to be having a dramatic impact on the number of Code 4 events taking place outside the ICU setting,” Perkins says.
There have been no patient family activations of the RAT since the Condition Help aspect of the program was initiated in May. Its availability is made known to families through signs in patient rooms and brochures explaining the program and listing how, why and when parents can call to request a RAT activation.
David Christensen, M.D., senior vice president of Medical Affairs and chief medical officer at Children’s, says the RAT program exists to augment, not supersede, the care provided by the patient’s attending physician.
“It’s one more added resource that our pediatric patients and their families, as well as their attending physicians, receive here at
“THIS PROGRAM IS TRUly FOCUSED ON THE WEll-bEING OF THE PATIENT.”
daVid christEnsEn, M.d.sEnior VicE PrEsidEnt of MEdical affairs and chiEf MEdical officErchildrEn’s hosPital & MEdical cEntEr
nuMbEr of codE 4 EVEnts occurring outsidE of icu
2007 2008 2009
(through Sept.)
12
30
p. 13
Physicians’ Priority linE 1.888.592.7955

Children’s,” Dr. Christensen says. “We have an extraordinarily thorough system in place for patient care. With the Rapid Assessment Team, we have a phenomenal backup system, as well.”
Perkins says an interdisciplinary committee at Children’s titled “Watchful Eye” meets quarterly and examines data and evaluations from all RAT activations. “We look at everything, from Code 4 data to unplanned transfers and other information.”
Children’s also has conducted a trial of the Pediatric Early Warning Scores (PEWS) program, where assessments of patients are suggested by an ongoing evaluation of three criteria: behavior, cardiovascular and respiratory.
In PEWS, patients are assigned a “score” from zero to 3 for each condition. For example, a
child whose respiratory condition is within normal parameters with no retractions would have a score of zero, while a child who is 5 below baseline parameters with retractions or grunting, or is receiving 50 percent FiO2 or 8-plus liters per minute, would be scored a 3.
The scores for each criterion are added together, and the patient is assigned a color code from green to red, and a corresponding schedule for reassessment. A score of zero to 2 (green) would require a reassessment every four hours, while a score of 5 or greater (red) would require a reassessment every 30 minutes.
“by assigning them a score that reflects their risk for the likelihood of being transferred to ICU, it helps identify priorities for the physicians and the charge nurse,” Perkins says. “When a change in shift occurs, if incoming staff see they have one child red
and two in orange, they know right away who needs to be checked more often.”
She said the initial trial of the PEWS program was well received. It is expected to be incorporated on all medical/surgical floors at some time in 2010.
“It’s a good, standardized system enabling people to talk the same language and know when a patient is getting into trouble,” Perkins says.
Dr. Christensen says the RAT and PEWS programs are rooted in Children’s mission, “so that all children may have a better chance to live.”
“These programs are truly focused on the well-being of the patient,” he says. “Their care is the number one priority of all we do here.”
“it’s a good, standardizEd systEM
Enabling PEoPlE to talk thE saME
languagE and knoW WhEn a
PatiEnt is gEtting into troublE.”
donnEtta PErkins, r.n., PMP, ManagEr of PrograMs and systEMs dEVEloPMEntchildrEn’s hosPital & MEdical cEntEr
raPid assEssMEnt tEaM
p. 14

When diagnosing the type and cause of joint pain in some of his patients, Children’s Pediatric Rheumatologist Adam Reinhardt, M.D., assistant professor of Pediatrics at UMNC College of Medicine, sometimes asks an unusual question: Do you know any party tricks, the kind you can do with your fingers or arms?
“Children often don’t understand what you mean by being loose-jointed or double-jointed,” Dr. Reinhardt explains. “but when I ask if they ever do any tricks for their friends like at parties or on the playground, quite often you can see the recognition light up across their faces. Then they show me.”
Joint pain can be experienced by up to 30 percent of all children and adolescents, Dr. Reinhardt says. Some of it is mild while other forms can be excruciating.
Causes for pediatric joint pain range from hypermobility, or joint looseness, to more serious disorders, even leukemia. That is why joint pain should be diagnosed by a subspecialist who can recognize and accurately determine which of the multitude of causes is responsible, Dr. Reinhardt says.
“Inflammatory joint pain and mechanical joint pain have different sources and require different treatments,” he says. “It’s important to examine the patient for structural abnormalities as well as malignancies, or signs of inflammatory arthropathy such as juvenile idiopathic (rheumatoid) arthritis.”
Joints are held in place by a number of tendons, muscles, ligaments and the joint capsule. When these are loose, joints can display more motion than normal. Activities that put stress on these loose joints can irritate them and cause pain.
benign hypermobility joint syndrome (bHJS) is a laxity of joints that can be a source of joint or muscle pain typically noted after exercise and activity during the day, or while resting at night.
“Hypermobility is a common reason for mild joint pain,” Dr. Reinhardt says. “Over a period of time, the extra mobility around the joint can cause discomfort.”
Some children simply have joints that are looser than those in other children. Some children with hypermobile joints complain of pain, while others with equally loose joints have no pain.
Hypermobility can be treated by strengthening the muscles around the joint to compensate for the extra flexibility. Such strengthening needs to come from a guided daily physical therapy program. “you have to avoid inactivity, but also avoid impact-type activities in order to prevent dislocation and further injury,” he says.
because the issue behind hypermobility is the looseness of the joint rather than inflammation, the effect of medication may be limited.
ProPEr diagnosis crucial in trEating PEdiatric joint Pain
PEdiatric joint Pain
p. 15

Another common cause of joint pain in childhood results from benign nocturnal pains which are often referred to as “growing pains.” The pain is not, however, caused by rapid growth.
“Typically, children will have no daytime symptoms and yet will wake up at night with pain that will often bring tears to their eyes,” Dr. Reinhardt says.
Treatment can include reassurance from the child’s parents and perhaps some light massage or stretching activities until the child can return to sleep, he says. “Ultimately, all children will outgrow the condition.”
It is critical that an accurate diagnosis of bHJS or benign nocturnal pains of childhood is made in order to rule out more serious causes of joint pain.
“The possibility of leukemia needs to be eliminated in all children with joint pain, especially if it occurs at night,” he says. “We can do this through the use of screening labs such as a CbC (complete blood count), ESR (sedimentation rate) and by examining the markers of cell turnover. Those will always be normal in a child with benign hypermobility and ‘growing pains.’”
Joint pain caused by malignancies can be differentiated from benign nocturnal pains because it continues throughout the day, not just at night, he says.
Pain or stiffness in the morning can also be a symptom of an inflammatory arthropathy such as juvenile idiopathic arthritis (JIA).
“Any type of arthritis generally improves some with activity,” Dr. Reinhardt says. “Stiffness, however, is a good sign of inflammation, as is joint swelling. lack of movement overnight can prompt morning pain, as can the phenomenon of ‘jelling,’ when a child sits inactive for an extended period of time, at school or while riding in a car.”
JIA is the most frequent rheumatic disease in children and one of the most common chronic pediatric illnesses. It has several subtypes. Two of the most common are oligoarticular arthritis, which affects four joints or less, and polyarticular arthritis, which involves five or more joints.
JIA can not only lead to functional disability of the involved joints but also cause eye inflammation, which can result in blindness if undetected.
Treatment often depends upon the subtype. Physical therapy may restore lost joint motion, increase flexibility and strengthen muscles. Medications may be employed to reduce inflammation and relieve swelling and pain. The choices include non-steroidal anti-inflammatory drugs (NSAIDs) such as naproxen or ibuprofen, COX II inhibitors such as Celebrex, corticosteroid injections,
and disease modifying anti-rheumatic drugs (DMARDs) such as methotrexate.
The diagnosis of JIA begins with a detailed physical examination and a complete clinical history, Dr. Reinhardt says.
“There is no lab test that will tell you the answers you need,” he says. “The child should be seen by someone who is comfortable examining joints, because joint pain, ANA (antinuclear antibodies) or rheumatoid factor tests are not good diagnostic screening markers for JIA. They alone are typically not useful in differentiating a normal child from a child with JIA.”
Dr. Reinhardt invites physicians with questions about pediatric joint pain to call the Physicians’ Priority line at 1-888-592-7955. “We can discuss symptoms, possible therapies and the need for a referral.”
Good candidates for referral are those experiencing a history of pain with a history of morning stiffness, limitation or swelling.
“The key in treating juvenile arthritis,” Dr. Reinhardt says, “is the earlier, more aggressive the treatment, the better the outcome.”
“IT’S IMPORTANT TO EXAMINE THE PATIENT FOR STRUCTURAl AbNORMAlITIES AS WEll AS MAlIGNANCIES, OR SIGNS OF INFlAMMATORy ARTHROPATHy SUCH AS JUvENIlE IDIOPATHIC (RHEUMATOID) ARTHRITIS.”
adaM rEinhardt, M.d.PEdiatric rhEuMatologistchildrEn’s hosPital & MEdical cEntErassistant ProfEssor of PEdiatrics, unMc collEgE of MEdicinE
PEdiatric joint Pain
p. 16
nEW
Ph
ysic
ian
sEMErgEncy dEPartMEntpatRiCK DoHeRtY, M.D. dr. doherty received his medical degree from creighton university school of Medicine. he completed his pediatric residency at the creighton-nebraska universities health foundation. he works in children’s hospital & Medical center’s Emergency department.
gi/hEPatologyRYan FiSCHeR, M.D.dr. fischer received his medical degree from the university of nebraska Medical center college of Medicine. he completed his pediatric residency at nationwide children’s hospital in columbus, ohio and fellowships in pediatric gastroenterology and pediatric transplant hepatology at children’s hospital of Pittsburgh. he is a pediatric gastroenterologist/hepatologist at university of nebraska Medical center.
urgEnt carECaRRie HoaRtY, M.D.dr. hoarty received her medical degree from the university of nebraska Medical center college of Medicine. she completed her residency in internal medicine/pediatrics with the creighton-nebraska universities health foundation. she is a pediatrician in children’s urgent care.
infEctious disEasEJeSSiCa niCHolS, M.D.dr. nichols received her medical degree from texas a&M university college of Medicine in college station, texas. she completed her pediatric residency at East carolina university school of Medicine in greenville, nc. she is a pediatric infectious disease specialist.
nEurologyiVan paVKoViC, M.D. dr. Pavkovic received his medical degree from rush university in chicago. he completed his residency in internal medicine/pediatrics and his fellowship in pediatric neurology at the university of Michigan hospital in ann arbor. he is a child neurologist at children’s hospital & Medical center.
gastroEntErologyRUben QUiRoS, M.D.dr. quiros received his medical degree from universidad nacional de Panama school of Medicine in Panama city, Panama. he completed pediatric residencies at hospital del nino de Panama and duPont institute/nemours foundation in Wilmington, del. he is a pediatric gastroenterologist and clinical service chief at children’s hospital & Medical center.
urgEnt carECHaRleS RUSH, M.D.dr. rush received his medical degree from creighton university school of Medicine. he completed his pediatric residency at cardinal glennon children’s hospital in st. louis. he is a pediatrician at children’s hospital & Medical center’s urgent care at West Village Pointe.
anEsthEsiaRaCHel SpitZnaGel, M.D. dr. spitznagel received her medical degree from the university of nebraska Medical center college of Medicine. she completed her residency in anesthesiology at the feinberg school of Medicine, northwestern university in chicago, and her fellowship in pediatric anesthesiology at children’s Memorial hospital in chicago. she is a pediatric anesthesiologist at children’s hospital & Medical center.
radiologyJoHn WenDel, M.D. dr. Wendel received his medical degree from the Mayo Medical school. he completed his residencies in diagnostic radiology and pediatric radiology at the university of texas Medical branch hospital in galveston. he is a pediatric radiologist at children’s hospital & Medical center.
radiologyliSa WHeeloCK, M.D. dr. Wheelock received her medical degree from creighton university school of Medicine. she completed her internal medicine residency at creighton university Medical center and her radiology residency at the university of nebraska Medical center. she completed her pediatric radiology fellowship in 2009 and is now a pediatric radiologist at children’s hospital & Medical center.
p. 17
nEW Physicians
Children’s has added a pediatric component to its existing ground transport service for newborns and infants. Critical care nurse practitioners and specially trained transport nurses provide the most advanced, cutting- edge care for both newborn and pediatric patients and then continue that specialized care during transport to Children’s Hospital & Medical Center. The team bridges the gap between Children’s and other medical facilities.
If a child is younger than 2 months old, the Newborn Critical Care Transport Team will respond. Any child over the age of 2 months will receive care from Children’s specialized Pediatric Critical Care Transport Team, the only such team in the state of Nebraska. both teams serve Nebraska, western Iowa, northern Missouri, northern kansas, eastern Colorado and South Dakota – anywhere in the region where there’s a child in need.
The team has years of experience in pediatric and newborn critical care and has received extensive training and certification in order to perform the necessary skills associated with transport including intubation, intraosseous access and needle thoracentesis.
The medical control team of physicians includes a neonatologist or pediatric intensivist who communicates with the team upon their arrival and makes an assessment to develop a plan of care for each patient. They are always available to board the transport vehicle as needed.
Children’s is the only hospital in the region offering both neonatal and pediatric ECMO. Upon arrival at the hospital, patients can be treated by specialists in NICU or PICU, supported by cardiology and cardiac surgery and subspecialists in nearly all pediatric medical disciplines.
One call to the Physicians’ Priority line at 1-888-592-7955 activates the team, which consults with the referring physician to arrange for the most appropriate form of transport. based on the patient’s needs, Children’s can arrange for transport via helicopter, fixed wing or ground service.
transPort adds sErVicE
PEdiatric rEsourcE dirEctory
Children’s Hospital & Medical Center has a pediatric resource directory available in printed form and downloadable at www.ChildrensOmaha.org/PediatricResourceDirectory.
If you would like a printed copy, please call 402.955.6957.
The directory highlights various specialty services available to health care providers across the region. It is a quick reference tool, but is not intended to serve as a complete medical staff directory. A more comprehensive listing is available online 24/7 at www.ChildrensOmaha.org.
1.888.592.7955Physicians’ Priority linE
your 24-hour link to pediatric specialists for physician-to-physician consults, referrals, admissions and newborn transport service.
transPort adds PEdiatric sErVicE
The colorful new ambulance you may see on the road is the area’s first ambulance dedicated to the transportation of young patients. Children’s Hospital & Medical Center’s child-friendly ambulance transports newborn and pediatric patients who are critically ill or have suffered a serious injury.
The ambulance features pediatric-specific medications, medical devices and equipment, maximizing safety and
effectiveness. A child-friendly atmosphere is created inside the ambulance with pictures, coloring books and a DvD player to distract children and help ease fears and anxiety.
American Medical Response (AMR) is partnering with Children’s to provide ambulance service. A back-up ambulance is available if the main vehicle is responding to a transport call.
nEW aMbulancE EnhancEs rEgional PrEsEncE
p. 18
Physicians’ Priority Line (physician-to-physician consult and referral line)1.888.592.7955
Transport (Physicians’ Priority Line) 1.888.592.7955
Hospitalist Service 402.955.5400 or 1.888.592.7955
PICU 402.955.4200
NICU 402.955.6230
childrEn’s hosPital & MEdical cEntEr outrEach clinics
outrEach clinic schEdulE
Clinic Location Rotation Frequency Phone
CaRdIoLogy
Carl Gumbiner, M.D. Norfolk, Neb Monthly 402.955.4350
North Platte, Neb Quarterly 402.955.4350
Kearney, Neb Quarterly 402.955.4350
Lincoln, Neb Semi-Monthly 402.486.1500
David Danford, M.D. Hastings, Neb Monthly 402.955.4350
Grand Island, Neb Quarterly 402.955.4350
Lincoln, Neb Semi-Monthly 402.486.1500
Scott Fletcher, M.D. Columbus, Neb Quarterly 402.955.4350
Sioux City, Iowa Semi-Annually 402.955.4350
Holdrege, Neb Semi-Annually 402.955.4350
Lincoln, Neb Semi-Monthly 402.486.1500
Christopher Erickson, M.D. Lincoln, Neb Semi-Monthly 402.486.1500
Shelby Kutty, M.D. Lincoln, Neb Semi-Monthly 402.486.1500
Jeffrey Delaney, M.D. Lincoln, Neb Semi-Monthly 402.486.1500
John Kugler, M.D. Lincoln, Neb Semi-Monthly 402.486.0500
ENdoCRINoLogy
Monina Cabrera Sioux City, Iowa Semi-Monthly 402.955.3871
Kevin Corley, M.D. Lincoln, Neb Weekly 402.486.1500
Jean-Claude Des Mangles, M.D. Lincoln, Neb Monthly 402.486.1500
gaSTRoENTERoLogy
Fernando Zapata, M.D. Sioux City, Iowa Monthly 402.955.5700
HEmaToLogy/oNCoLogy
David Gnarra, M.D. Lincoln, Neb Weekly 402.486.1500
Clinic Location Rotation Frequency Phone
NEURoLogy
Young Oliver, M.D. Sioux City, Iowa Monthly 402.955.5372
Ivan Pavkovic, M.D. Lincoln, Neb Semi-Monthly 402.486.1500
NEURoSURgERy
Mark Puccioni, M.D. Lincoln, Neb Monthly 402.486.1500
oRTHoPaEdICS
Paul Esposito, M.D. Lincoln, Neb Weekly 402.486.1500
Brian P. Hasley, M.D. Lincoln, Neb Weekly 402.486.1500
PULmoNoLogy
Mark Wilson, M.D. Sioux City, Iowa Monthly 402.955.5570
Lincoln, Neb Weekly 402.486.1500
John Colombo, M.D. Lincoln, Neb Weekly 402.486.1500
Paul Sammut, M.D. Lincoln, Neb Weekly 402.486.1500
RHEUmaToLogy
Adam Reinhardt, M.D. Lincoln, Neb Monthly 402.486.1500
SURgERy
Shahab Abdessalam, M.D. Lincoln, Neb Monthly 402.486.1500
Kenneth Azarow, M.D. Lincoln, Neb Monthly 402.486.1500
Robert Cusick, M.D. Lincoln, Neb Monthly 402.486.1500
Stephen Raynor, M.D. Lincoln, Neb Monthly 402.486.1500
p. 19
Childrensomaha.org
1.888.592.7955Physicians’ Priority linE
your 24-hour link to pediatric specialists for physician-to-physician consults, referrals, admissions and neonatal transport service.
The Physicians’ Priority line usage has increased by 20 percent during the past 12 months. In a recent survey of referring physicians, the majority of physicians rated their experience with the service as excellent.





























