Embed Size (px)
Citation preview

Journal of Pediatric Urology (2013) 9, 731e737
REVIEW ARTICLE
Childhood vesicoureteral reflux studies:Registries and repositories sources andnosology*
Russell W. Chesney*, Andrea B. Patters
Department of Pediatrics, Le Bonheur Children’s Hospital, University of TennesseeHealth Science Center, 50 N. Dunlap, Memphis, TN 38103, USA
Received 7 February 2012; accepted 11 September 2012Available online 5 October 2012
KEYWORDSUrinary tractinfection;Vesicoureteral reflux;Registry;Repository;Reflux nephropathy
* For the RIVUR Trial investigators:Marva Moxey-Mims.* Corresponding author. Tel.: þ1 901E-mail address: [email protected]
1477-5131/$36 ª 2012 Journal of Pedhttp://dx.doi.org/10.1016/j.jpurol.20
Abstract Despite several recent studies, the advisability of antimicrobial prophylaxis andcertain imaging studies for urinary tract infections (UTIs) remains controversial. The role of ve-sicoureteral reflux (VUR) on the severity and re-infection rates for UTIs is also difficult toassess. Registries and repositories of data and biomaterials from clinical studies in childrenwith VUR are valuable. Disease registries are collections of secondary data related to patientswith a specific diagnosis, condition or procedure. Registries differ from indices in that theycontain more extensive data. A research repository is an entity that receives, stores, processesand/or disseminates specimens (or other materials) as needed. It encompasses the physicallocation as well as the full range of activities associated with its operation. It may also bereferred to as a biorepository. This report provides information about some current registriesand repositories that include data and samples from children with VUR. It also describes theheterogeneous nature of the subjects, as some registries and repositories include only dataor samples from patients with primary reflux while others also include those from patients withsyndromic or secondary reflux.ª 2012 Journal of Pediatric Urology Company. Published by Elsevier Ltd. All rights reserved.
Ranjiv Mathews, Saul Greenfield, Tej Mattoo, Alejandro Hoberman, Ron Keren, Myra Carpenter and
287 6106; fax: þ1 901 287 4478.du (R.W. Chesney).
iatric Urology Company. Published by Elsevier Ltd. All rights reserved.12.09.003

732 R.W. Chesney, A.B. Patters
Introduction
Appropriate methods for the evaluation and treatment ofchildren with vesicoureteral reflux (VUR) remain a knottyproblem [1]. Doubts have been raised about the role oflong-term antibiotic prophylaxis in preventing urinarytract infection (UTI) and renal scarring in children withVUR [2]. Surgical intervention trials using re-implantationor endoscopic injection of biologically inert materialshave been associated with high success for the resolutionof reflux, but do not always translate to reduction in thefrequency of urinary tract infections or scarring [3]. Anumber of prospective, interventional clinical trials thataim to examine the role of VUR as a risk factor for UTI andrenal scarring have either recently been completed or areongoing. Some are randomized and controlled [1,4,5],and all potentially contain a sufficient number of subjectsto allow for complex analysis. Several of these studiesform the basis of national or international registriesand/or repositories that potentially allow for furtherand ongoing analysis of well characterized patientpopulations. In this review of registries and repositorieswe endeavor to clarify these, to compare prospectiveregistries and to explain the nature of the patientsherein.
Patient or disease registries are defined as collections ofsecondary data related to patients with a specific diagnosis,condition or procedure, and they contain a substantialamount of patient information [6]. Registries differ fromindices in that they contain more extensive data: an indexis generally a list of cases that contains minimal informa-tion. A repository is an entity that receives, stores,processes and/or disseminates specimens and other items,such as images, as needed. It encompasses the physicallocation as well as the full range of activities associatedwith its operations. It may also be referred to as a bio-repository [6]. In general, a repository has a “repositoryallocation committee” (RAC), which is responsible forascertaining if requests for datasets and biospecimens meetthe criteria for valid research studies. The RAC is alsoresponsible for assuring that critical last remaining speci-mens are not removed without valid scientific justification.Repositories, therefore, contain biological material frompatients often described in registries. This paper will definethe locations and describe the fundamental nature of thepatient populations of a number of substantial registriesand repositories.
Methods
All of the studies evaluated relate to VUR in children ofspecified age ranges: no adults were included. The inclu-sion and exclusion criteria were those of the underlyingstudies and can vary from study to study. Most of theregistries and repositories examined were recentlyconvened and have readily available and fairly extensivedata, either published or web-based, concerning patientdemographics, primary and secondary outcomes, length offollow-up, and whether or not the trial was interventional.Several of these trials have been closed, but others areongoing [4,7e12].
Because the purpose of this report is to catalog some ofthe registries and repositories available, and to discusstheir heterogeneous nature, no information regarding theprimary or secondary outcomes of the patient groups wasevaluated or analyzed. In general, we sought registries andrepositories from national or international multi-centerstudies.
Results
Registries: location and features
Some of the extant national patient registries for childrenwho have established VUR at the time of study entry areshown in Table 1 and arise from several countries, includingAustralia (ANZDATA), Italy (ItalKid), Greece (Patras),Sweden (the Swedish Reflux Trial in Children), and otherEuropean nations, as well as the United States and SouthAmerica. One large, all-encompassing registry is the UnitedStates Renal Data System (USRDS), a large data set that has“de-identified” information on subjects of all ages who arereceiving renal replacement therapy or have undergonea renal transplant. In this system, pediatric data aredivided into several age categories: 0e4 yrs, 5e10 yrs,11e15 yrs, and 16e20 yrs. This data set includes childrenwith VUR and end stage renal disease. Each year a newgroup of patients enters the data set and a group ofpatients leaves due to death or entering adulthood (>20years of age).
One distinction of VUR registries is that several, such asANZDATA, USRDS, Patras and RIVUR continue to collect dataprospectively, whereas the International Reflux Study, theSwedish Reflux Trial in Children, and the studies of Roussey-Kesler, Pennisi, Montini and Garin are closed [4,9e13]. Allpotentially offer data sources for analysis. Moreover, someof these large national registries contain data from subjectswith renal disorders other than VUR, but do include chil-dren with reflux nephropathy. Hence, certain registriescontain data from subjects where only primary VUR isconsidered (e.g., RIVUR and ItalKid), while others catego-rize patients with either primary or syndromic reflux and/orno reflux (USRDS, ANZDATA, the Swedish Reflux Trial, theRoussey-Kesler study and the Garin study). This createsa problem in nosology, or the classification of disease, ofwhich potential investigators should be cognizant. Tables 1and 2 list several national registries and their studycharacteristics.
The International Reflux Study in Children comparedthe long-term outcome of medical versus surgical treat-ment of children with severe VUR in 438 patients initiallyfollowed over five years. Some of the children in theEuropean limb of the study (306) were followed fora longer period of time, and 252 were included in the final10-year report [13]. The ANZDATA registry contains datafrom all children under the age of 18 who have receivedrenal replacement therapy (RRT) since the inception ofRRT in Australia and New Zealand. Of those 1485 children,35.8% were diagnosed with structural anomalies includinghypoplasia/dysplasia, posterior urethral valves, or refluxnephropathy [14]. This registry did not include childrenwith primary reflux. The prospective and population-

Table 1 Details of some registries that are no longer enrolling participants and are considered closed.
Study Site Format No. enrolled %female Urolog imaging Reference
International Reflux Study inChildren (IRSC)
United States,Canada, Europe
Long-term outcome of medicalor surgical treatment ofchildren < 11 y with gradeIII/IV VUR
438 (252 followedfor 10 y)
76.1 Urogra hy, VCUG, DMSAscan f r selected ptsin 5e1 yrs of follow-up
Pediatr Nephrol (2006)21:785 [email protected]
The Swedish Reflux Trialin Children
Sweden Prospective, randomized,controlled trial of gradeIII/IV reflux followed for 2 y
203, non-syndromicreflux
63.1 VCUG DMSA scanwith f llow-up
J Urol (2010) 184: 274-304(several articles) [email protected]
Chronic Kidney Disease inChildren (CKiD)
USA Prospective observationalcohort with mild to moderatelyimpaired renal function
586 enrolled; 87 withreflux nephropathy(mainly 2�), CAKUT
33 VCUG Clinicaltrials.gov;NCT00327860
The ESCAPE Trial Europe Prospective, randomized,controlled study of intensevs standard blood pressurecontrol in children with CKD
385 (264 with hypo/dysplasia)
41 New Engl J Med (2009) 361:1639 [email protected]
Ab prophylaxis, UTIand VUR study
France Prospective, randomized;antibiotic prophylaxis for lowgrade VUR in children 1 moto 3 y
225 69 Ultras nd, VCUG J Urol (2008) 79:[email protected]
VUR, Ab prophylaxisand UTI afterpyelonephritis study
USA, Chile,Spain
Prospective, randomized,controlled, 3e18 y old withprimary VUR
236 (113 with VUR) 75 Ultras nd, VCUG,DMSA an
Pediatr (2006) 117:[email protected]
Antibiotic prophylaxisand recurrentUTI in children
AustraliaNew Zealand
Prospective, low-dosecontrolled continuous SX/TMPvs placebo to prevent reinfection;42% of pts with reflux; ages 1 moto 10 y
576 64% Not re uired; most hadultras nd, VCUG andDMSA an
NEJM (2009) 361:[email protected]
Italian Renal InfectionStudy Group
(IRIS) (Montini study)
Northeast Italy Multicenter randomized,controlled, open labelprophylaxis after first UTI;co-trimazole or co-amoxiclavor no therapy, ages 2 mo to < 7 y
338 69% Ultras nd, VCUG, DMSA Pediatr (2008) 122:[email protected]
Effect of prophylaxisin childrenwith reflux onpreventing pyelonephritisand renal scarring(Pennesi study)
Northern Italy Prospective SX/TMP vs no antibiotic;grades IIeIV reflux; ages 1e30 mo
100 50% Repea d VCUGand D SA scan
Pediatr (2008) 121:[email protected]
Ab, antibiotic; CAKUT, congenital anomalies of the kidney and urinary tract; DMSA, dimercaptosuccinic acid; ESRD, end stage renal isease; GFR, glomerular filtration rate; mo, months;pts, patients; TMP/SX, trimethoprim/sulfamethoxazole; VCUG, voiding cystourethrography; VUR, vesicoureteral reflux; y, years.
Child
hoodve
sicoureteralrefluxstu
dies
733
ic
po0
,o
ou
ousc
qousc
ou
teM
d
Table
2Detailsofsomeregistriesthatare
currentlyenrollingparticipants
andare
consideredopen.
Registry
Site
Form
at
No.enrolled
Gender
Urologicim
aging
Reference
AustraliaNew
Zealand
DialysisandTransplant
Registry
(ANZDATA)
Australia,
New
Zealand
ESR
Din
childrensince
1963
.Originallyretrospective,
now
real-timeeve
nt-based
reporting/
annualsurvey
1485
(280
withreflux
nephropathy,
butnumber
declinedwithreco
gnition
ofCAKUT)
45.4%female
Urography,
VCUG
Pediatr
Nephrol(200
9)24
:171
9ANZDATA.org
ItalianPediatric
Registry
ofChronic
RenalFailure
inChildren(ItalKid)
Italy
Chronic
renalfailure
inch
ildrenwithGFR<
75ml/min/1
.73m
2;
1�&
2�reflux,
allgrades
1197
(hyp
oplasia
withreflux
in30
9)
33%female,but
includesposterior
urethralva
lvesand
CAKUT
VCUG
RandomizedIntervention
forChildrenwith
Vesico
ureteralReflux
(RIVUR)
USA
ProspectiveUTIwith
1�VUR,interventional
2months<
6ye
ars
GradesIe
IVVUR
607
92%female
Ultrasound,VCUG,
DMSA
scanwith
follow-up
Clinicaltrials.gov;
NCT00
4057
04
Patras
Greece
ProspectiveUTI,
GradesIe
VVUR
296(refluxin
62)
46.8%female
Ultrasound,VCUG,
DMSA
scan
Pediatrics(201
0)12
6:e51
3sfouza
s@gm
ail.com
UnitedStatesRenalData
System
(USR
DS)
USA
Inform
ationanddata
from
childrenwithESR
Dsince
1988
;allpts
on
dialysise
allreflux
425withreflux
nephropathy
in20
00e20
09
60%female
Notalw
ays
specified
USR
DS@
usrds.org
734 R.W. Chesney, A.B. Patters
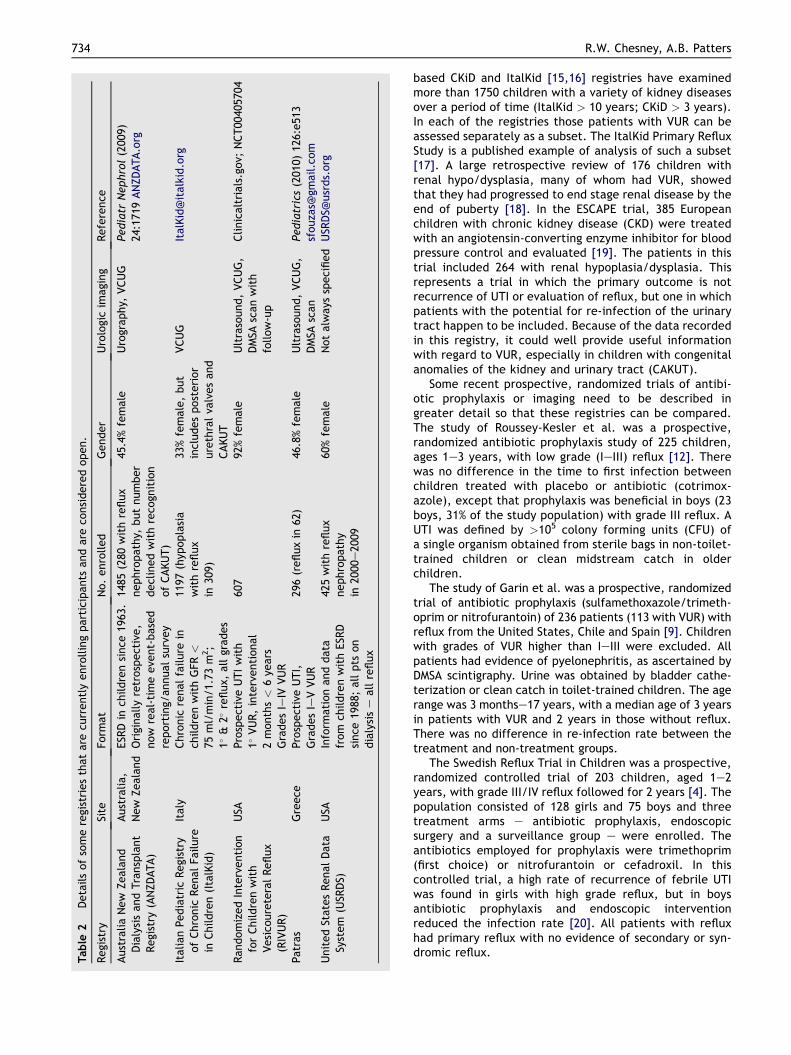
based CKiD and ItalKid [15,16] registries have examinedmore than 1750 children with a variety of kidney diseasesover a period of time (ItalKid > 10 years; CKiD > 3 years).In each of the registries those patients with VUR can beassessed separately as a subset. The ItalKid Primary RefluxStudy is a published example of analysis of such a subset[17]. A large retrospective review of 176 children withrenal hypo/dysplasia, many of whom had VUR, showedthat they had progressed to end stage renal disease by theend of puberty [18]. In the ESCAPE trial, 385 Europeanchildren with chronic kidney disease (CKD) were treatedwith an angiotensin-converting enzyme inhibitor for bloodpressure control and evaluated [19]. The patients in thistrial included 264 with renal hypoplasia/dysplasia. Thisrepresents a trial in which the primary outcome is notrecurrence of UTI or evaluation of reflux, but one in whichpatients with the potential for re-infection of the urinarytract happen to be included. Because of the data recordedin this registry, it could well provide useful informationwith regard to VUR, especially in children with congenitalanomalies of the kidney and urinary tract (CAKUT).
Some recent prospective, randomized trials of antibi-otic prophylaxis or imaging need to be described ingreater detail so that these registries can be compared.The study of Roussey-Kesler et al. was a prospective,randomized antibiotic prophylaxis study of 225 children,ages 1e3 years, with low grade (IeIII) reflux [12]. Therewas no difference in the time to first infection betweenchildren treated with placebo or antibiotic (cotrimox-azole), except that prophylaxis was beneficial in boys (23boys, 31% of the study population) with grade III reflux. AUTI was defined by >105 colony forming units (CFU) ofa single organism obtained from sterile bags in non-toilet-trained children or clean midstream catch in olderchildren.
The study of Garin et al. was a prospective, randomizedtrial of antibiotic prophylaxis (sulfamethoxazole/trimeth-oprim or nitrofurantoin) of 236 patients (113 with VUR) withreflux from the United States, Chile and Spain [9]. Childrenwith grades of VUR higher than IeIII were excluded. Allpatients had evidence of pyelonephritis, as ascertained byDMSA scintigraphy. Urine was obtained by bladder cathe-terization or clean catch in toilet-trained children. The agerange was 3 monthse17 years, with a median age of 3 yearsin patients with VUR and 2 years in those without reflux.There was no difference in re-infection rate between thetreatment and non-treatment groups.
The Swedish Reflux Trial in Children was a prospective,randomized controlled trial of 203 children, aged 1e2years, with grade III/IV reflux followed for 2 years [4]. Thepopulation consisted of 128 girls and 75 boys and threetreatment arms e antibiotic prophylaxis, endoscopicsurgery and a surveillance group e were enrolled. Theantibiotics employed for prophylaxis were trimethoprim(first choice) or nitrofurantoin or cefadroxil. In thiscontrolled trial, a high rate of recurrence of febrile UTIwas found in girls with high grade reflux, but in boysantibiotic prophylaxis and endoscopic interventionreduced the infection rate [20]. All patients with refluxhad primary reflux with no evidence of secondary or syn-dromic reflux.

Childhood vesicoureteral reflux studies 735
In a randomized trial in Italy 100 patients with grades II,III, IV reflux were assigned to receive sulfamethoxazole/trimethoprim or to serve as controls [11]. Patients wereaged 1e30 months and urine was obtained by sterile bagtechnique. The males (50%) were not circumcised. Therewas no evidence of benefit from antibiotic prophylaxis, butcontrol patients were not given a placebo.
In a multicenter, randomized, controlled, noninferioritytrial from Italy that enrolled 338 children with primaryreflux, aged 2 months to <7 years and 69% female, partic-ipants received either co-trimoxazole or co-amoxiclav or noprophylaxis for 12 months [10]. The grades of reflux werenone to IeIII. There was no difference in the primaryoutcome of reduction of recurrence of febrile UTI betweengroups. Urine was collected by sterile urinary bag and twoconsecutive and concordant urinalyses were necessary torule out false-positive tests.
A large (576 children) placebo-controlled trialregarding the efficacy of antibiotics was performed inAustralia in children under 18 years [5]. The median age atentry was 14 months; 64% of patients were female and 42%had known VUR while in the study. A UTI developed in 55of 288 patients on placebo and 36 of 288 receivingtrimethoprim/sulfamethoxazole (p < 0.02), demon-strating the value of continuous antibiotic prophylaxis.Urine was collected by suprapubic aspiration, urinarycatheter or midstream clean catch in children who weretoilet-trained.
The RIVUR study has enrolled a baseline population of607 patients with grades IeIV VUR in a randomized,placebo-controlled trial designed to measure recurrence ofUTI (primary outcome). Participants were aged 2 months to6 years, predominantly female (92%) and Caucasian (81%),and most commonly had grades II/III reflux (80%). Outcomeof patients randomized to placebo or trimethoprim/sulfa-methoxazole will be analyzed after 24 months with initial,12 month and 24 month DMSA scan to determine rate ofscarring. Quality of life and dysfunctional voiding scoreswere measured in all patients. Urine was obtained bybladder catheterization or midstream collection in toilet-
Table 3 Biomedical repositories.
Repository Number of samples
Urologic Diseases Database and Repositoryfor Biosamples and Data
Many studies,thousandsof samples
CKiD e 2008 586RIVUR e 2010 600 anticipatedIrish Primary VUR Repository e 2007 609UK/Slovenia Repository e 2001e2010 661Dutch - Italian Repository e 2008 95
New York City e Columbia UniversityRepository e 2010
3144
Iowa-Ohio State e PittsburghRepository e 2010
380 (100 with reflu
Montreal Children’s Hospital eMcGill University e 2010
142
trained children. The outcome results await the conclusionof the study in 2013.
Several large national registries are available, includingANZDATA, ItalKid, USRDS, CKiD and the ESCAPE trial (Tables1 and 2). These registries contain patients with heteroge-neous renal disorders, including glomerulonephritis, renaldysplasia/hypoplasia, and reflux nephropathy. In contrastto the previously mentioned trials, these registries do notfocus on UTIs or VUR, but do contain many patients withthese disorders, especially syndromic VUR.
A non-interventional study of reflux (Patras, Greece)assessed 296 children by use of DMSA scan to determinethe value of scan following a febrile UTI to identify dilatingVUR [8]. Patients were <24 months of age (47% female)and urine was collected by suprapubic aspiration orbladder catheterization. The data from this study sug-gested that acute DMSA scan has limited overall ability toidentify VUR.
Biomaterial repositories
There exist several biomaterial repositories that are listedin Table 3. The biorepositories of the Irish Primary VURrepository, the UK/Slovenia Repository, the Dutch ItalianRepository, the New York City e Columbia UniversityRepository, the Iowa e Ohio State e Pittsburgh Repositoryand the Montreal Children’s Hospital Repository all containbiologic materials obtained from children with VUR. Theserepositories are often, but not always, separate from thelarge registries. The Urologic Diseases Database andRepository for Biosamples is sponsored by the NationalInstitute of Diabetes and Digestive and Kidney Diseases(NIDDK) of the National Institutes of Health (NIH). Both theCKid and the RIVUR repositories are part of this system.Among the features of the listed repositories are thefollowing: they include samples from subjects with primaryVUR and without obstruction, or subjects with CAKUT. Allsubjects have a positive VCUG as an entry criterion andthey may include familial VUR or index cases only. Subjectsare North American, European or Chilean. No ethnic groups
Reference
http://www.niddkrepository.org
Clinicaltrials.gov; NCT00327860Clinicaltrials.gov; NCT00405704J Med Genet (2007) 44:710 [email protected] Am Soc Nephrol (2010) 21:113 [email protected] Am Soc Nephrol (2008) 19:825 [email protected] Genet (2011) 43:321 Ali Gharavi(ag2239@columbia edu), Richard Lifton([email protected]

736 R.W. Chesney, A.B. Patters
are excluded. The biomaterials stored include blood, urine,immortalized cells, hair, and fingernail clippings. Hair andnails are not always kept, but can be used to assess envi-ronmental toxins.
Discussion
The purpose of this report is to clarify the nature of extantregistries and repositories, and to briefly summarize themakeup of the populations studied. The aim is to makestudents of reflux aware of the heterogeneous nature of thepatients studied, as well as the rich sample size.
One of the dilemmas in understanding the association ofVUR, renal scarring, and the natural course of CKDprogression in reflux nephropathy is the paucity of studiesof the natural history of syndromic and non-syndromic VUR[7,21,22]. Many studies have examined children witha variety of kidney diseases. In these registries thosepatients with VUR can often be assessed separately asa subset. This overall picture of CAKUT and renal hypo-dysplasia progressing to ESRD versus the apparently morebenign course of children with primary VUR defines thenosologic problem in considering VUR. With increasingevidence that VUR is not a prerequisite for the develop-ment of pyelonephritis, reflux nephropathy may representmainly an embryologically derived renal parenchymalabnormality [7]. Simply put, not all VUR has the same bio-logic profile.
The aim of creating registries with data from childrenwith VUR is not only to understand the short-termoutcomes, but also to potentially evaluate long-termoutcomes if cohort studies are undertaken. Similarly, theaim of creating repositories with stored genetic material isto understand genotype/phenotype correlations and thegenetic bases of long-term outcomes.
An examination of these registries shows heterogeneitywithin these patients on whom extensive data are kept,with some patients not having VUR (Tables 1 and 2). Again,this heterogeneity leads to nosologic issues. Older registriesof VUR subjects tended to include children with CAKUT andreflux nephropathy. Newer registries are more likely toevaluate primary, non-syndromic VUR. In addition, theextensive changes in urinary tract imaging mean that thedata from techniques such as DMSA, radionuclide imagingand radionuclide voiding studies are not always found inolder registries, but are likely found in newer ones. Forexample, only in the final (10-year) follow-up of theInternational Reflux Study were DMSA scans performed toidentify new scars. Finally, another heterogeneous featureis that the period of follow-up of patients in these registriescan vary from one year to more than 10 years.
There is considerable value in several recent studies (lis-ted in Tables 1 and 2) because they have prospectivelyrecruitedandwell definedpatients, and theage, gender, VURgrade and outcomes are well described [4,5,8e12]. All thesesubjects were followed for a definite predetermined timeperiod. Studies emanating from Europe and Australia havemore males than American trials do, which has been attrib-uted to the lower rates of circumcision in these populations[1]. An ideal study should obtain urine by bladder catheteri-zation or suprapubic aspiration in non-toilet-trained children
[5,8,9] rather than sterile-bag urine collection [4,10e12], anopinion also expressed by Hoberman and Keren [1]. Anotherissue can be insufficient statistical power to detect clinicallyimportant differences: in order to detect a reduction in theabsolute risk of recurrent UTI of 10%, a study would need toenroll roughly 600 children [1,23]. Several of these registrieshave fewer than 300 patients enrolled (Tables 1 and 2).
Biorepositories also contain materials from patients withCAKUT and reflux nephropathy or primary non-syndromicVUR [24]. Several repositories include material fromaffected and non-affected relatives of patients withfamilial VUR, while others only include samples from theindex case. Material from a repository may not be madeavailable until a study has finished enrolling subjects orwhen the study is closed (when baseline and primaryoutcome results are published). Also, access to a goldstandard biorepository with electronic data management isnot always possible. Frequently, a grant from the NIH orother agency and/or an agreement to collaborate with theinvestigative team is required.
The greater the diversity and amount of materialsavailable for genetic or other studies, the more the resultsof studies that utilize the materials can be generalized. Asa goal for future large cohort studies of VUR, an attemptshould be made to create both a registry and a repositorywhere relevant data and material from subjects and familymembers can be stored. These materials will have to be“de-identified” to meet privacy guidelines. In the future,more complex genetic analyses will be performed as tech-niques for genome-wide searches become more rapid andless expensive. Two additional themes of study should be anexamination of genes of interest in the entire urinary tractand correlation of genetic/genomic information withimaging results. Because of the manner in which renaldevelopment occurs, genes of interest should alwaysinclude those evident in the urethra, bladder and ureters aswell as the kidney. Mutations or polymorphisms in devel-opmental genes should be examined as well as those rele-vant to the mature kidney. When properly stored urine isavailable, urine proteomics can be correlated with bothgenetic/genomic information and the results of imagingstudies.
One of the many issues with the use of registries is atwhat point in time the material and data are made avail-able to the scientific community. Data and materials remainthe property of the primary investigators until the study isdeemed closed. This is typically considered to haveoccurred once the baseline and main outcomes publicationsare accepted and published. At this time, data collectedunder the aegis of national funding agencies is madeavailable to other investigators. A mechanism for investi-gators to access registry data or repository biomaterials isto submit a grant application to the funding agency for anancillary study. These ancillary studies generally ask ques-tions that are not the primary or secondary outcomes of theparent study.
For individuals wishing to access data for analyses, thequestion as to who “owns” the data is also pertinent. Whilea study is still active the data are under the guardianship ofthe data-coordinating center. Once the primary outcomestudies are performed and published the data becomepublic or available through limited access. The studies that
Childhood vesicoureteral reflux studies 737
underlie these registries are funded by national researchagencies rather than pharmaceutical or device companies.
The request for material should be in the form of anancillary study for up to two years after the study outcome ispublished. Following that time period, applications to obtainrepository samples should be reviewed by the repositoryallocation committee and the institutional review board.
With improvement in data collection, imaging tech-niques, and the evaluation of genetic and proteomicbiomaterials, the information from patients enrolled in VURstudies can be analyzed in many ways and new questionscan be asked. To accomplish these goals, a standardizationof the operation of registries and repositories would beoptimal, including a web-based portal of access.
Acknowledgments
The authors thank the RIVUR participants, their families andthe participating physicians, investigators and staffs formaking this research possible. The authors have no financialor personal conflicts of interest to disclose. Ethical approvalwas not required for this review. The Randomized Inter-vention for Children with Vesicoureteral Reflux trial wassupported by cooperative agreements U01 DK074059(Carpenter), U01 DK074053 (Hoberman), U01 DK074082(Mathews), U01 DK074064 (Keren), U01 DK074062 (Mattoo),U01 DK074063 (Greenfield) from the National Institute ofDiabetes and Digestive and Kidney Diseases, National Insti-tutes of Health, Department of Health and Human Services.The trial was also supported by the Children’s Hospital ofPhiladelphia Clinical and Translational Science Award(UL1TR000003) from the National Center for ResearchResources, now at the National Center for AdvancingTranslational Sciences, National Institutes of Health. Thecontent is solely the responsibility of the authors and doesnot necessarily represent the official views of the NationalInstitute of Diabetes and Digestive and Kidney Diseases orthe National Institutes of Health. The RIVUR website islocated at http://www.cscc.unc.edu/rivur/.
References
[1] Hoberman A, Keren R. Antimicrobial prophylaxis for urinarytract infection in children. N Engl J Med 2009;361:1804e6.
[2] Keren R, Carpenter MA, Hoberman A, Shaikh N, Matoo TK,Chesney RW, et al. Rationale and design issues of therandomized intervention for children with vesicoureteralreflux (RIVUR) study. Pediatrics 2008;122(Suppl. 5):S240e50.
[3] American Urological Association. Policies, guidelines &quality, http://wwwauanetorg/content/guidelines-and-quality-care/guidelines-and-quality-carecfm; 2010.
[4] Brandstrom P, Esbjorner E, Herthelius M, Holmdahl G,Lackgren G, Neveus T, et al. The Swedish reflux trial in chil-dren: I. Study design and study population characteristics. JUrol 2010;184:274e9.
[5] Craig JC, Simpson JM, Williams GJ, Lowe A, Reynolds GJ,McTaggart SJ, et al. Antibiotic prophylaxis and recurrent urinarytract infection in children. N Engl J Med 2009;361:1748e59.
[6] National Heart Lung and Blood Institute. Biologic specimenand data repository information coordinating center, https://biolinccnhlbinihgov/glossary/; 2010.
[7] Craig JC, Williams GJ. Denominators do matter: it’s a myth-eurinary tract infection does not cause chronic kidneydisease. Pediatrics 2011;128:984e5.
[8] Fouzas S, Krikelli E, Vassilakos P, Gkentzi D, Papanastasiou DA,Salakos C. DMSA scan for revealing vesicoureteral reflux inyoung children with urinary tract infection. Pediatrics 2010;126:e513e9.
[9] Garin EH, Olavarria F, Garcia Nieto V, Valenciano B, Campos A,Young L. Clinical significance of primary vesicoureteral refluxand urinary antibiotic prophylaxis after acute pyelonephritis:a multicenter, randomized, controlled study. Pediatrics 2006;117:626e32.
[10] Montini G, Rigon L, Zucchetta P, Fregonese F, Toffolo A,Gobber D, et al. Prophylaxis after first febrile urinary tractinfection in children? A multicenter, randomized, controlled,noninferiority trial. Pediatrics 2008;122:1064e71.
[11] Pennesi M, Travan L, Peratoner L, Bordugo A, Cattaneo A,Ronfani L, et al. Is antibiotic prophylaxis in children withvesicoureteral reflux effective in preventing pyelonephritisand renal scars? A randomized, controlled trial. Pediatrics2008;121:e1489e94.
[12] Roussey-Kesler G, Gadjos V, Idres N, Horen B, Ichay L,Leclair MD, et al. Antibiotic prophylaxis for the prevention ofrecurrent urinary tract infection in children with low gradevesicoureteral reflux: results from a prospective randomizedstudy. J Urol 2008;179:674e9 [discussion 9].
[13] Jodal U, Smellie JM, Lax H, Hoyer PF. Ten-year results ofrandomized treatment of children with severe vesicoureteralreflux. Final report of the international reflux study in chil-dren. Pediatr Nephrol 2006;21:785e92.
[14] Orr NI, McDonald SP, McTaggart S, Henning P, Craig JC.Frequency, etiology and treatment of childhood end-stagekidney disease in Australia and New Zealand. Pediatr Neph-rol 2009;24:1719e26.
[15] CKiD. A prospective cohort study of kidney disease in children,http://wwwstatepijhsphedu/ckid/; 2010.
[16] Ardissino G, Dacco V, Testa S, Bonaudo R, Claris-Appiani A,Taioli E, et al. Epidemiology of chronic renal failure in children:data from the ItalKid project. Pediatrics 2003;111:e382e7.
[17] Marra G, Oppezzo C, Ardissino G, Dacco V, Testa S, Avolio L,et al. Severe vesicoureteral reflux and chronic renal failure:a condition peculiar to male gender? Data from the ItalKidProject. J Pediatr 2004;144:677e81.
[18] Gonzalez Celedon C, Bitsori M, Tullus K. Progression of chronicrenal failure in children with dysplastic kidneys. PediatrNephrol 2007;22:1014e20.
[19] Wuhl E, Trivelli A, Picca S, Litwin M, Peco-Antic A, Zurowska A,et al. Strict blood-pressure control and progression of renalfailure in children. N Engl J Med 2009;361:1639e50.
[20] Brandstrom P, Esbjorner E, Herthelius M, Swerkersson S,Jodal U, Hansson S. The Swedish reflux trial in children: III.Urinary tract infection pattern. J Urol 2010;184:286e91.
[21] Montini G, Tullus K, Hewitt I. Febrile urinary tract infections inchildren. N Engl J Med 2011;365:239e50.
[22] Shaikh N, Ewing AL, Bhatnagar S, Hoberman A. Risk of renalscarring in children with a first urinary tract infection:a systematic review. Pediatrics 2010;126:1084e91.
[23] Mathews R, Carpenter M, Chesney R, Hoberman A, Keren R,Mattoo T, et al. Controversies in the management of ves-icoureteral reflux: the rationale for the RIVUR study. J PediatrUrol 2009;5:336e41.
[24] Lambert HJ, Stewart A, Gullett AM, Cordell HJ, Malcolm S,Feather SA, et al. Primary, nonsyndromic vesicoureteric refluxand nephropathy in sibling pairs: a United Kingdom cohort fora DNA bank. Clin J Am Soc Nephrol 2011;6:760e6.