Embed Size (px)
Citation preview

1282
withdrawal of cimetidine, concentrations of N-nitroso compoundsremained increased is supported by a recent American study. 14The pH does not have to be raised throughout the 24 h period for
significant bacterial growth to occur as long as a pH of 4 or more isreached for part of the time. Muscroft et al. 15 have shown that 45%of aspirates from forty-four fasting patients taking cimetidine 1 gdaily contained >106 bacteria/ml 2-4 h after the last dose, comparedwith 4% of fifteen comparable patients not taking the drug and 94%of the organisms isolated were from the aspirates with a pH>4.Debate on N-nitroso compounds and human gastric cancer
continues but some involvement seems likely.16 Brimblecombeshould provide details of"the extensive studies of which he is aware,both completed and in progress, which have not demonstrated anyaetiological link between cimetidine treatment and the developmentof gastric cancer" in man.We agree with a Lancet editorial of Oct. 24 (p. 906) that we need to
know more about what H2 blockers do to the gastric flora. IfN-nitrosamine concentrations are raised in certain conditions withan increased risk of gastric cancer then this is a hint which must notbe ignored.Gastrointestinal Unit,Wexham Park Hospital,Slough, Berkshire
Leatherhead Food Research Association,Leatherhead, Surrey
Department of Pharmacology,Guy’s Hospital Medical School,London SE1
P. I. REEDK. HAINES
C. L. WALTERSS. L. R. SMITH
F. R. HOUSE
SUPPORTIVE CARE FOR LEUKAEMIA PATIENTS INBONE MARROW APLASIA
SIR,-The report by Dr Watson and his colleagues (Oct. 31,p. 957) is a rather whimsical review of the relative demands on sup-portive care of patients receiving remission-induced therapy (RI)and bone marrow transplantation (BMT) for acute myeloid leuk-aemia (AML).
It is hardly surprising that BMT patients need less support thanRI patients for the very good reason that the clinical and haema-tological status of the patients in the two groups is generally verydifferent and the conundrum was artificial from the start. It would,perhaps, have been more valuable to have compared the amount ofsupportive care given during the consolidation and maintenancephases of chemotherapy with that given to post-transplantationpatients. The support needed by the former group certainlydeserves more attention since it is easy to overtreat patients in thisphase, and deaths in remission are occasionally the result.
’
Among the first 75 adult patients with AML treated in Cambridgewith the DAT regimen were 65 who achieved complete remission.The average age of the remitters was 49 -1 years (range 14-84). Theaverage number of days in hospital after complete remission was 15(range 0-35) and the number of units of packed red cells andplatelets tranfused per patient was 5 - 5 (range 0-22) and 0 - 3 (range0-24) respectively. Apart from consolidation and maintenancechemotherapy 25% of the patients received six intrathecal
injections as CNS prophylaxis and routinely remained in hospitalovernight for these to be given; a few patients were admitted for thepatient’s convenience because the centre serves some remote areasof East Anglia. The supportive care given after relapse is notincluded in this analysis.
- Watson and colleagues’ cautionary note to prospectiveparticipants in marrow transplantation is welcome, for, although asuperficial reading of their paper might lead one to conclude that thecase for BMT is almost complete, the reference to previouslypublished work does not underline the fact that, for patients
14 Stockbrügger RW, Eugenides N, Bartholomew B, Walters CL, Thompson REM, HillMJ, Cotton PB. Cimetidine-treatment, intragastric bacterial overgrowth and itsconsequences. Gastroenterology 1981; 80: 1295 (abstr).
15. Muscroft TJ, Youngs D, Burdon DW, Keighley MRB. Cimetidine and the potentialrisk of postoperative sepsis. Br J Surg 1981; 68: 557-59.
16. Schmähl D. Carcinogenic substances and carcinogenesis and their clinical significance.In: Herfarth Ch, Schlag P, eds. Gastric cancer. Berlin: Springer-Verlag, 1979:15-19.
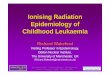
DAT therapy for AML.Actuarial curve of survival after remission (all ages).
receiving bone marrow transplants, "disease free" has little
meaning if leukaemia is replaced by uncontrollable graft-versus-host disease or pneumonitis. Nor are the results of BMT always asgood as those for standard chemotherapy.In the current (8th) M.R.C. Acute Myeloid Leukaemia Trial, 12
patients, all under the age of 40, have received a bone marrow graftin first remission from HLA identical siblings. 8 patients have diedand the median duration of survival after transplantation is 16months. Even allowing for an average interval of 3 months betweenremission and transplantation the prognosis for these patients wasworse than for the 65 patients of all ages who were treated withchemotherapy; the median duration of survival following remissionfor this group is 21 months and the Kaplan-Meier curve of survivalis shown in the figure.BMT may indeed be a valuable option to be considered in the
small number of patients with AML who are below the age of 40 andhave suitable donors. It is quite possible that, when compared withgroups receiving present forms of chemotherapy, there will be ahigher proportion of long-term survivors but the follow-up periodsfor the transplanted patients so far have, with few exceptions, beenrather short.
Department of Haematological Medicine,University Clinical School,Cambridge CB2 2QL
J. K. H. REESF. G. J. HAYHOE
CHILDHOOD LEUKAEMIA AND SOCIAL STATUS
SiR,—Dr McWhirter and colleagues (Nov. 7, p. 1051) reportedthe results of a population-based study of social class as a prognosticfactor in childhood acute lymphoblastic leukaemia (ALL). Theyhave shown worse survival in children of fathers from lower social
class, by comparing percentage survival and median survival in twoaggregated groups. We have applied the more sensitive logrank testfor trend to disaggregated groups from a larger population-basedstudy over a similar period and have not been able to confirm thesefindings.The Royal Manchester Children’s Hospital paediatric oncology
unit serves an area of North-West England which has a totalpopulation of over four million. The Manchester children’s tumourregistry records all cases of malignancy in the region, I and 96% ofchildren with ALL were treated with full conventional
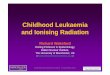
chemotherapy, including CNS prophylaxis, and followed up duringthe period 1971-78. The father’s occupation could be recorded in201 of the 209 children, and this was then classified, according to theOffice of Population Censuses and Surveys system, to groups I-V.Life table curves for length of first remission were compared bylogrank test for trend (see figure).2 The percentages of children ineach social class still in first remission five years after treatmentstarted are shown in the table.
1. Draper G, Birch J, Bithell J, et al Childhood cancer m Britain 1953-75 London: HMStationery Office (in press).
2. Peto R, Pike MC, Armitage P, et al. Design and analysis of randomised clinical trialsrequiring prolonged observation of each patient. Br J Cancer 1977; 35: 1-39.

1283
TIA1E IN MONTHS
Social class and length of f"11’St remission.
Although there is a trend for longer remission times with lower social classthis fails to reach statistical significance (p = 0 . 11).*= Number corresponding to social class.
SOCIAL CLASS AND LENGTH OF FIRST REMISSION
The results suggest a trend for better prognosis with lower socialclass but this is not significant. We have not therefore been able tofind support for the hypothesis that worse prognosis is associatedwith lower social class.
Departments of Paediatric Oncologyand Haematology,
Royal Manchester Children’s Hospital;and Department of Medical Statistics,
Christie Hospital, Manchester
I. M. HANN*M. K. PALMERP. H. MORRIS-JONESD. I. K. EVANS
*Present address: Department of Haematology, Royal Free Hospital, London NW3 2QG.
CAMPYLOBACTER SEROTYPES AND EPIDEMIOLOGY
SiR,—Two letters from Canada in The Lancet of Nov. 14 indicatethe possible value of serotyping in the epidemiology ofCampylobacter infection. Dr Lior and colleagues (p. 1103) havestudied 21 heat-labile antigens by the simple technique of bacterialagglutination while Dr Karmali’s team (p. 1104) has used passivehaemagglutination for a study of heat-stable antigens.Karmali et al. recognised that a patient may be infected with two
or more serotypes simultaneously; and, with one of their fourisolates, they showed that eleven colonies from the primary culturewere all of the same serotype. Another of their isolates, however,was designated as type 13,16: does this imply a mixed culture or dideach colony react with both antisera?
.
With Bordetella pertussis, it is not uncommon for the serotype tochange during a patient’s infection, so that two or more serotypesmay be found amongst the colonies of a primary culture. I
Serotyping is, therefore, of no value in tracing the source of infec-tion with B. pertussis; and it is not surprising for two siblings to be
1. Stanbridge TN, Preston NW. Variation of serotype in strains of Bordetella pertussis. JHyg (Camb) 1974; 73: 305-10.
infected with different serotypes (say, type 1,2 and type 1,3), eventhough the’ dates of onset of their illness suggest that one wasinfected from the other. A similar change of serotype in a singlepatient has been reported with Vibrio cholerae.Until we know more about the antigenic stability of strains of
Campylobacter, therefore, it may be unwise to rely on serologicalfindings as an epidemiological tool. But this does not preclude apossibly important role for the serotype antigens in immunity, as isundoubtedly the case with pertussis infection.Pertussis Reference Laboratory,University Medical School,Manchester M13 9PT N. W. PRESTON
GAS-LIQUID CHROMATOGRAPHY ANDCLOSTRIDIUM DIFFICILE
StR,—I read with interest the letter by Dr Potvliege and colleagues(Nov. 14, p. 1105). Although I do not understand the thinkingbehind the belief that the volatile fatty acid profile generated bypure strains of Clostridium difficile from glucose in vitro should bethe same as that produced in mixed culture in a complex mileu invivo, they did produce some interesting data. I find it difficult,however, to accept their interpretation. They state that gas-liquidchromatography (GLC) "seems a good screening method forexcluding C. difficile infection". However, GLC would have given anegative result for 11 of the 28 stool samples that were culture/toxinpositive. If they had used their GLC method to exclude C. difficileinfection they would have missed 39% of their positive samples.Although most people would readily accept a small number of falsepositive results in a screening procedure, a figure of 39% falsenegatives is unacceptable.In our experience C. bifermentans and C. sporogenes can be isolated
as a component of the normal gastrointestinal flora. More
importantly, in most cases Potvliege et al. will be dealing with anabnormal faecal flora due to the administration of antibiotics and ithas been shown that species of clostridia not normally. classed ascomponents of the normal faecal flora (e.g., C. oroticum) can beisolated in increased numbers from the faeces of healthy volunteersreceiving antibiotics. 1
Clinical Research Centre,Harrow, Middlesex HA 1 3UJ S. P. BORRIELLO
NEUROLOGICAL MANIFESTATION OF ACUTEHAEMORRHAGIC CONJUNCTIVITIS DUE TO
ENTEROVIRUS 70
SIR,-Wadia et al.2 have reported the reappearance of a
neurological illness following acute haemorrhagic conjunctivitis(AHC) in India in May, 1981. This association was first observed in1971.3 Epidemic and sporadic AHC has persisted in India since1971, but without the neurological sequelae.Two widespread epidemics of AHC in India in 1975 and in 1979
were due to Coxsackievirus A24.4,s In the first quarter of 1981Coxsackievirus conjunctivitis also prevailed, but since May therehas been an epidemic of AHC due to enterovirus 70 (EV70). Wehave found the isolation of Coxsackievirus easy but that of EV70difficult. Recently in several patients with AHC we have foundseroconversion or 4-fold or greater antibody rises against EV70 andno evidence of Coxsackievirus infection. Thus we believe that this isthe first AHC epidemic due to EV70 in India after the 1971epidemic.
1. Sutter VL, Fmegold SM. The effect of antimicrobial agents on human faecal flora:studies with cephalexin, cyclacillin and clindamycin. In: Skinner FA, Caer JG, eds.The normal microbial flora of man. London: Academic Press. 1974: 229-40
2. Wadia NH, Wadia, PN, Katrak SM, Misra VP. Neurological manifestations of acutehaemorrhagic conjunctivitis. Lancet 1981; ii: 528
3. Wadia NH, Irani PF, Katrak SM. Neurological complications of a new conjunctivitis.Lancet 1972; ii, 970.
4. Christopher S, John TJ, Charles V, Ray S. Coxsackievirus A24 variant EH24/70 andenterovirus type 70 in an epidemic of acute haemorrhagic conjunctivitis: a
preliminary report. Indian J Med Res 1977; 65: 593-95.5. Indian Council of Medical Research. Annual report of the ICMR Centre of Advanced
Research in Virology. 1980: 9.