Embed Size (px)
DESCRIPTION
Iron deficiency anemia , presentation , diagnosis ,management
Citation preview

1st May 2010 Khorfakkan Scientific Anemia Day 1
Khorfakkan Scientific
anemia Day 1st May 2010

1st May 2010 Khorfakkan Scientific Anemia Day 2
Typical Scenario
*18 month old child brought in by mom for check up•Healthy, URTI a few weeks ago (in daycare)•Picky eater, but drinks lots of milk* Growing well, pudgy•Grand-mother thought he was a bit pale

1st May 2010 Khorfakkan Scientific Anemia Day 3
Physical exam
*Pale, chubby, wt at 95%, ht at 60%*HR 140, RR 20, BP 90/50, SPO2 97%*Conjunctiva and mucous membranes slightly pale*Chest clear*No organomegaly, no adenopathy

1st May 2010 Khorfakkan Scientific Anemia Day 4
Lab values
*CBC Hgb 5.4, Plt 735, WBC 8.5 with normal diff*MCV, MCHC decreased*Retic count low*Smear Microcytic, hypochromic cells*Ferritin

1st May 2010 Khorfakkan Scientific Anemia Day 5
Microcytic, hypochromic
cells

1st May 2010 Khorfakkan Scientific Anemia Day 6
Why is it important to know how
to diagnose and treat IDA?

1st May 2010 Khorfakkan Scientific Anemia Day 7
30% of the world’s population has anemia,
1 billion have IDA Global prevalence
is 53.6% in preschool children
ANEMIA – A PUBLIC HEALTH PROBLEM
McLean E, Egli I, Cogswell M, de Benoist B,Wojdyla D. Worldwide prevalence of anemia in preschool aged children, pregnant women and non-pregnant women of reproductive age.Ch1:1-12.In: Kraemer K, ed. Nutritional Anemia. Sight and Life press. Basel, Switzerland. 2007.

1st May 2010 Khorfakkan Scientific Anemia Day 8
Anemia is a severe public health problem in Africa, Asia, Latin America
and the Caribbean
ANEMIA – A PUBLIC HEALTH PROBLEM
World Health Organization (WHO). Nutrition. Geneva: WHO, www. who.int/nutrition/en: WHO 2007

1st May 2010 Khorfakkan Scientific Anemia Day 9
Iron deficiency identified as one of ten most serious risk in countries
with high infant and adult mortalities
ANEMIA – A PUBLIC HEALTH PROBLEM
World Health Organization. The world health report 2002: reducing risks, promoting healthy life. Geneva, Switzerland: World Health Organization, 2002.

1st May 2010 Khorfakkan Scientific Anemia Day 10
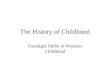
Anemia as a
public health
problem by country;
preschool children

1st May 2010 Khorfakkan Scientific Anemia Day 11
Anemia prevalence and number of Individuals affected in preschool-age children in each WHO region

1st May 2010 Khorfakkan Scientific Anemia Day 12
• ~ 2 billion anemic
• Severe anemia →high mortality
• Mild to moderate anemia– Impairs child development– Decreases work capacity
Iron Deficiency/Anemia: A Major Global Problem

1st May 2010 Khorfakkan Scientific Anemia Day 13
Conceptual diagram of
the relationshipbetween iron
deficiency and anemia
in a hypothetical population
Yip R. Iron nutritional status defined. In: Filer IJ, ed. Dietary Iron: birth to two years. New York, Raven Press, 1989:19-36.

1st May 2010 Khorfakkan Scientific Anemia Day 14
ANEMIA
Definition Anemia is defined as:A decrease in the concentration of circulating red blood cells or in the hemoglobin concentration and a concomitant impaired capacity to transport oxygen.
McLean E, Cogswell M, Egli I, Wojdyla D, de Benoist B.Worldwide prevalence of anaemia, WHO Vitamin and Mineral Nutrition Information System, 1993-2005.Public Health Nutr. 2009 Apr; 12(4):444-54. Epub 2008 May 23.

1st May 2010 Khorfakkan Scientific Anemia Day 15
ANEMIAWHO Diagnosis Hemoglobin below 11gm/dl in pre school
children.
UNICEF/UNU/WHO. Iron deficiency anemia: assessment, prevention and control. A guide for programme managers.WHO/NHD,2001 [report no.01.3]

1st May 2010 Khorfakkan Scientific Anemia Day 16
IRON DEFICIENCY ANEMIA
One of the 15 leading causes of global disease burden
Boccio JR, Iyengar V. Iron deficiency: causes, consequences, and strategies to overcome this nutritional problem. Biol Trace Elem Res. 2003 Jul; 94(1):1-32. Review
Global picture
•25 Million DALYs lost due to IDA
Stoltzfus R., Stiefel H., Iron deficiency and the global burden on disease. Symposium: Integrating programs to move iron deficiency and anemia control forward. Marrakesch, Morocco, 6 February 2003

1st May 2010 Khorfakkan Scientific Anemia Day 17
Iron deficiency
Is an abnormal value for at least two of three laboratory indicators of iron status:
1. Serum ferritin 2. Transferrin
saturation 3. Free erythrocyte protoporphyrin
As defined by the National Health and Nutrition Examination Survey (NHANES)

1st May 2010 Khorfakkan Scientific Anemia Day 18
IRON DEFICENCY
STAGES
Prelatent reduction in iron stores without reduced serum iron levelsLatentiron stores are exhausted, but the blood hemoglobin level remains normalIron deficiency anemiablood hemoglobin concentration falls below the lower limit of normal

1st May 2010 Khorfakkan Scientific Anemia Day 19
Functions of
Iron
Formulation of hemoglobin Binding O2 to RBC and transport Formulation of cytochrome myoglobin Regulation of Body temperature

1st May 2010 Khorfakkan Scientific Anemia Day 20
Functions of
Iron
Muscle activity Catecholamine metabolism Immune system Brain Development & functionThyroid function
Cont.

1st May 2010 Khorfakkan Scientific Anemia Day 21
Iron Concentration
In Brain
25%25%
50%50%
75%75%
100%100%
BirthBirth 22 YearsYears
10 10 YearsYears
Adult Adult HumanHuman
MaximumMaximum
MyelinationMyelination

1st May 2010 Khorfakkan Scientific Anemia Day 22
ANEMIAIron deficiency anemia occurs when iron deficiency is severe enough to reduce hemoglobin levels below normal.
NHANES 1999-2000

1st May 2010 Khorfakkan Scientific Anemia Day 23
Normal values
Harriet Lane Handbook, The John Hopkins
Hospital,15th edition
AGE HgbMean/ (-
2SD)
HCT%Mean/ (-
2SD)
MCVMean/ (-2SD)
Newborn 16.5 (13.5) 51 (42) 108 (96)
1 Month 13.9 (10.7) 44 (33) 101 (91)
2 Months 11.2 (9.4) 35 (28) 95 (84)
6 Months 12.6 (11.0) 36 (31) 76 (68)
> 6 Months 12.5 (11.0) 36 (33) 81 (70+ age per yr)

1st May 2010 Khorfakkan Scientific Anemia Day 24
http://www.cdc.gov/hemochromatosis/training/pathophysiology/iron_cycle_popup.htm
Iron cycle

1st May 2010 Khorfakkan Scientific Anemia Day 25
Mechanism
of developmen
t of
Anemia Normal Iron deficiency anemia

1st May 2010 Khorfakkan Scientific Anemia Day 26
Factors
Contribute
To the
Development
Of
Anemia
http://www.caribou.bc.ca/schs/medtech/rice/IronDeficiency.html

1st May 2010 Khorfakkan Scientific Anemia Day 27
Iron deficiency
Anemia
http://www.caribou.bc.ca/schs/medtech/rice/IronDeficiency.html
•Dietary iron deficiency is the usual cause• Iron def. is common in children 9mo-3yr•Infants less than 6 months generally do not develop iron def. •Iron def. anemia in a child over 3yr should prompt consideration of occult blood loss

1st May 2010 Khorfakkan Scientific Anemia Day 28
Iron deficiency
Anemia
(cont.)
•Dietary deficiency
•Increased demand (growth)
•Impaired absorption
•Blood loss (e.g.) - gut problems - lung - nose - kidney - menstrual problems - trauma
Causes

1st May 2010 Khorfakkan Scientific Anemia Day 29
Iron deficiency Anemia
(cont.)
•Pallor is the most important sign •Mild to Moderate iron deficiency ( hemoglobin levels of 6 -10 g/dL) few symptoms of anemia; irritable, Pagophagia•Severe iron deficiency ( hemoglobin levels of 6 -10 g/dL) Irritability , Anorexia, Tachycardia, Cardiac dilation, Systolic murmurs
Clinical Manifestation

1st May 2010 Khorfakkan Scientific Anemia Day 30
Iron deficiency Anemia
(cont.)
Clinical Manifestation (Cont.)
Iron deficiency may have effects on neurologic and intellectual functionsIron – deficiency anemia and even iron deficiency with out anemia affect : *Attention span *Alertness *Learning

1st May 2010 Khorfakkan Scientific Anemia Day 31
Iron deficiency Anemia
(cont.)
Clinical Manifestation (Cont.)
Decreased cognitive performance often accompanies iron deficiency and iron deficiency anemia
Murray-Kolb LE, Beard JL. Iron treatment normalizes cognitive functioning in young women. Am J Clin Nutr. 2007; 85:778-787.

1st May 2010 Khorfakkan Scientific Anemia Day 32
Iron deficiency Anemia
(cont.)
Clinical Manifestation (Cont.)
Koilonychia: "spoon nails” Iron deficiency anemia

1st May 2010 Khorfakkan Scientific Anemia Day 33
Iron deficiency Anemia
(cont.)
Clinical Manifestation (Cont.)
Smooth, bald, burning tongue; Iron deficiency anemia

1st May 2010 Khorfakkan Scientific Anemia Day 34
Iron deficiency Anemia
(cont.)
Clinical Manifestation (Cont.)
Angular Cheilosis or Stomatitis

1st May 2010 Khorfakkan Scientific Anemia Day 35
Iron deficiency Anemia
(cont.)
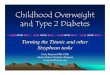
Bone marrow
ABSENT IRON STORES IN BONE MARROW IN IRON DEFICIENCYABSENT IRON STORES IN BONE MARROW IN IRON DEFICIENCY
Normal control Iron deficiency

1st May 2010 Khorfakkan Scientific Anemia Day 36
Laboratory Findings
Prelatent Hgb (N), MCV (N), iron absorption (), transferrin saturation (N), serum ferritin (), marrow iron ()
LatentHgb (N), MCV (N), TIBC (), serum ferritin (), transferrin saturation (), marrow iron (absent)
Iron deficiency anemia Hgb (), MCV (), TIBC (), serum ferritin (), transferrin saturation (), marrow iron (absent)

1st May 2010 Khorfakkan Scientific Anemia Day 37
Laboratory Findings (Cont.)
•With increasing deficiency ,RBCs become deformed and misshapen and present characteristic : - Microcytosis
- Hypochromia
- Poikilocytosis - Increased RBC distribution width (RDW)• Reticulocyte percentage may be normal or moderately elevated • Nucleated RBCs occasionally seen• Thrombocytosis (some time) • Normal white blood cells

1st May 2010 Khorfakkan Scientific Anemia Day 38
Laboratory Findings (Cont.)
•Additional diagnostic tests - Free erythrocyte protoporphyrin (elevated) - Serum ferritin (decreased) - Serum iron (decreased) - Iron binding capacity (increased) - Iron saturation (decreased)

1st May 2010 Khorfakkan Scientific Anemia Day 39
Differential Diagnosis
Other hypochromic microcytic anemias
•1.ß-Thalassemia trait * mild microcytic anemia * elevated levels of hemoglobin A2 and/or fetal hemoglobin concentration * Serum iron, total iron-binding capacity (transferrin) and ferritin are normal

1st May 2010 Khorfakkan Scientific Anemia Day 40
Differential Diagnosis
Other hypochromic microcytic anemias
2. a-Thalassemia trait * presence of familial hypochromic microcytic anemia * normal results of iron studies * normal levels of Hgb A2 and Hgb F *In new born ,3 -10% hemoglobin Barts (gamma 4)
(Cont.)

1st May 2010 Khorfakkan Scientific Anemia Day 41
Differential Diagnosis
Other hypochromic microcytic anemias
3. Hgb H disease * a form of a-Thalassemia results from deletion of three of the four a-globin genes * hypochromia and microcytosis * a mild hemolytic component from instability of the ß-chian tetramers (Hgb H)
(Cont.)

1st May 2010 Khorfakkan Scientific Anemia Day 42
Differential Diagnosis
Other hypochromic microcytic anemias
4. The anemia of chronic disease (ACD) * Elevated FPR * Coarse basophilic stippling of the RBC is frequently prominent * Elevations of blood lead. FEP, and urinary coproporphyrin levels Serum transferrin receptor (TIR) level is useful in distinction between iron- deficiency anemia and anemia of chronic disease
(Cont.)

1st May 2010 Khorfakkan Scientific Anemia Day 43
IRON DEFICIENCY versus ACD
Other hypochromic microcytic anemias
Serum Iron Transferrin Ferritin
Iron Deficiency
ACD

1st May 2010 Khorfakkan Scientific Anemia Day 44
PRINCIPLESPRINCIPLES OFOF
TREATMENTTREATMENT
1.Use oral iron
2.Replace iron deficit in total
3.Establish
and treat
the cause

1st May 2010 Khorfakkan Scientific Anemia Day 45
PRINCIPLESPRINCIPLES OFOF
TREATMENTTREATMENT
4.The therapeutic dose should be
calculated interms of
elemental iron
5. A daily total of 4 -6 mg/kg of elemental iron in
three divided doses provides
an optimal amount of iron
6.A parenteral iron
preparation (iron dextran) is an effective form of iron
(Cont.)

1st May 2010 Khorfakkan Scientific Anemia Day 46
PRINCIPLESPRINCIPLES OFOF
TREATMENTTREATMENT
(Cont.)
The regular
response of iron-deficiency anemia
to adequate amounts of iron is
an important diagnostic and
therapeutic features.

1st May 2010 Khorfakkan Scientific Anemia Day 47
PRINCIPLESPRINCIPLES OFOF
TREATMENTTREATMENT
(Cont.)
Oral administration of simple ferrous
salts ( sulfate, gluconate, fumartate) provides inexpensive
and satisfactory therapy

1st May 2010 Khorfakkan Scientific Anemia Day 48
Elemental iron (EI) in various forms of iron
tablets
1.Ferrous sulfate (20%EI) (300 mg tablets) 60 mg
2.Ferrous gluconate (12 %EI) (300 mg tablets) 34 mg
3.Ferrous fumarate (33 %EI)(200 mg tablets)66 mg

1st May 2010 Khorfakkan Scientific Anemia Day 49
Parenteral therapy
indications•poor compliance•severe bowel disease•intolerance of oral iron•chronic hemorrhage•acute diarrhea disorder

1st May 2010 Khorfakkan Scientific Anemia Day 50
Parenteral therapy
Iron dextran: (IM-IV) 50 mg
iron/mL Low and high
molecular weight
Ferric gluconate complex (IV) less incidence of allergic reactions
Iron sucrose: (IV) safe even with sensitivity to iron dextran

1st May 2010 Khorfakkan Scientific Anemia Day 51
Parenteral therapy
Ferumoxytol: safe and effective
as a rapid intravenous infusion up to 510 mg
in patients with chronic kidney disease and on
dialysis.
Ferric carboxymaltose: (IV) given at single doses of up to 1000 mg iron per week over of 15
minutes
(Cont.)

1st May 2010 Khorfakkan Scientific Anemia Day 52
Blood transfusion
•Is indicated only when •1.Anemia is very severe 2.Superimposed infection may interfere with the response
Packed or sedimented
RBCs should be
administered slowly
In severely anemic children with
hemoglobin values less than 4 g/dL
should be given only2 -3 mL/kg of packed cells at any one time

1st May 2010 Khorfakkan Scientific Anemia Day 53
Responses to iron therapy in iron- deficiency anemia
Time after Iron Administration
Response
12 -24 hr Subjective improvement; decreased irritability,
increased appetite
36 -48 hr Initial bone marrow response
48 -72 hr Reticulocytosis, peak at 5 -7 days
4 -30 days
Increase in hemoglobin level
1 -3 mo Repletion of stores

1st May 2010 Khorfakkan Scientific Anemia Day 54
Failure of iron therapy
occur when:
1. A child does not receive the prescribed medication2. Iron is given in a form that is poorly absorbed 3. There is continuing unrecognized
blood loss such as : * intestinal or pulmonary loss * loss with menstrual periods 4. An incorrect original diagnosis

1st May 2010 Khorfakkan Scientific Anemia Day 55
Short term Prevention of IDA In infancy
•Avoid gestational ID • Try to prevent premature delivery and low birth weight• Increase birth spacing• Delay pregnancy beyond teens• Delay ligation of umbilical cord (by 30-60 seconds)

1st May 2010 Khorfakkan Scientific Anemia Day 56
Short term prevention of IDA In children and adolescents
•Avoid gestational ID • Try to prevent premature delivery and low birth weight• Increase birth spacing• Delay pregnancy beyond teens• Delay ligation of umbilical cord (by 30-60 seconds)

1st May 2010 Khorfakkan Scientific Anemia Day 57
Sustainable approaches to elimination of micronutrient deficiency e.g. iron
Iron fortification of foods, foods in the target group:• Foods consumed regularly• Consumed in sufficient quantities• Consumed in stable amounts• Centrally processed foods• Foods that are easy to fortify

1st May 2010 Khorfakkan Scientific Anemia Day 58
Iron obtained from animal products is much more easily absorbed by the body than iron from plant sources,

1st May 2010 Khorfakkan Scientific Anemia Day 59
Home Message
•Anemia is a sign, not a disease. •Anemias are a dynamic process. •Its never normal to be anemic.•The diagnosis of iron deficiency anemia mandates further work-up

1st May 2010 Khorfakkan Scientific Anemia Day 60Good to have you with us, Farquhar. We could do with some fresh blood in this place.'

1st May 2010 Khorfakkan Scientific Anemia Day 61