Embed Size (px)
Citation preview
CHILDHOOD AND ADOLESCENT DIABETES
Dr Machira E
DEFINITION OF DIABETES
A metabolic syndrome characterized by hyperglycaemia as key biochemical abnormality.
• Defects in insulin production
• Autoimmune or other destruction of beta cells
• Insulin insensitivity
• Impaired action of insulin on target tissues
DIABETES EPIDEMIC
• 230 million affected in 2006
• 350 million within 20 years
• Most rapid in Indian and Asian subcontinents
• 350 fold variation in incidence worldwide.
• Highest known in Finland and lowest in china
Epidem cont
Annual incidence varies worldwide;0.1 China, Venezuela38.0 Finland
Most European countries 20/100,000 50% of cases occur during purberty
Principal Aims of treatment
• achieve good metabolic control• attain normal growth and development• avoid serious hypoglycemia• prevent long term complications of diabetes
TYPES OF DIABETES Type 1 DM Type 2 DM MODY Atypical DM Neonatal DM Diabetes Secondary to;
• Cystic fibrosis• Steroid treatment• Pancreatectomy for persist hyperinsulinaemic
hypoglycaemia of infancy
NEONATAL DM
incidence 1:400,000 births transient, thought due to delay in the maturation
of the ß-cells → hypoinsulinaemia small gestational age present in the first few days or weeks with
polydipsia, polyuria, marked weight loss, severe dehydration, vomiting
have hyperglycaemia, glycosuria but no ketonuria
NEONATAL DM cont…
Treatment of Neonatal DM; rehydrate give continuous infusion of insulin once stable give once daily long acting s.c
insulin treatment needed for a few days to 18
months (median 3 months) some may develop permanent DM, others
develop T2DM later in life
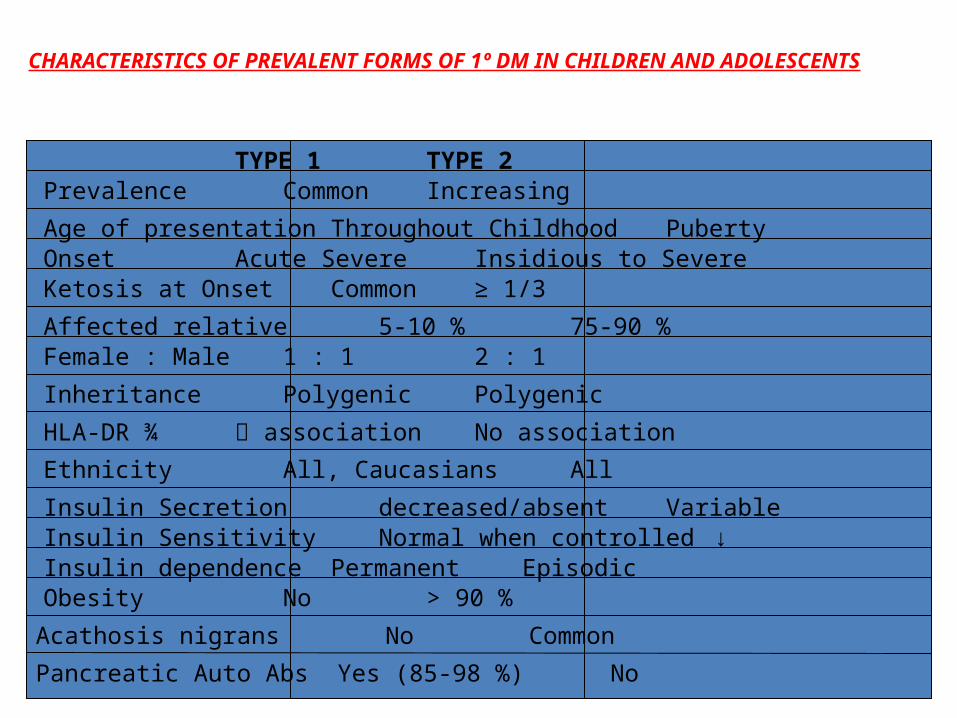
CHARACTERISTICS OF PREVALENT FORMS OF 1º DM IN CHILDREN AND ADOLESCENTS
TYPE 1 TYPE 2Prevalence Common Increasing
Age of presentationThroughout Childhood PubertyOnset Acute Severe Insidious to SevereKetosis at Onset Common ≥ 1/3
Affected relative 5-10 % 75-90 %Female : Male 1 : 1 2 : 1
Inheritance Polygenic Polygenic
HLA-DR ¾ association No association
Ethnicity All, Caucasians All
Insulin Secretion decreased/absent VariableInsulin Sensitivity Normal when controlled ↓Insulin dependencePermanent EpisodicObesity No > 90 %
Pancreatic Auto Abs Yes (85-98 %) No
Acathosis nigrans No Common
EPIDEMIOLOGY OF TYPE 1• Increasing in recent years
• Geographic variation: incidence increasing in specific areas with trend toward earlier age of presentation.
• Relative affluence• Lack of treatment• Age of onset peaks
Preschool: 5-7 years Puberty
• Autumn/winter peaks
Aetiology of type1 DM
1. AUTOIMMUNE2. NON AUTOIMMUNE( IDIOPATHIC)
PATHOGENESIS(AUTOIMMUNE)
• Immunological activation
• Progressive beta-cell destruction
• Insufficient beta-cell function
• Dependent on exogenous insulin
• Risk of ketoacidosis
IDIOPATHIC TYPE
Non-autoimmune type 1 diabetes
• No autoimmune markers
• Permanent insulinopenia
• Ketoacidosis
• People of African and Asian origin
DIAGNOSISTYPE 1 DMSymptoms may be present from 1 week to 6 months Polyuria (nocturnal enuresis), polydipsia, weight loss, anorexia or hyperphagia, lethargy,
constipation, blurred vision, infection (esp. perineal candiadiasis in girls, infants and toddlers of both gender)
T1DM classic symptoms ± DKA T2DM - symptoms + ketonuria in 1/3 of adolescents
- symptoms + DKA in 25 % of adolescentsLAB TESTS
RBS > 11.1 mmol/l (IGT RBS= 7.8-11.1)FBS > 7.0 mmol/l (IFG FBS=6.1-6.9)2 hr pp > 11.1 mmol/l
OGTT - 75g in water in children > 43 kg - 1.75 g/kg in water in children < 43kg
Serum C-peptide Serum insulin levels Islet cell antibodies
Uncertain diagnosis:Oral glucose tolerance test
• 75 g glucose load after 8 hours fasting
• Readings taken in fasting state and at 1 and 2 hours
• Possible problems
Impaired glucose toleranceImpaired fasting glucose
• Intermediate states• Increased risk of developing diabetes • Prevention strategies to prevent or
delay progression• Increased risk of cardiovascular
disease
DIAGNOSIS cont …
TYPE 2 DM
prevalence is parallel to childhood obesity in the UK present in 2 % of children < 16 yrs of age in the USA present in 35 % of newly diagnosed
patients 10-19 yrs puberty plays a key role due to the insulin
resistance 75 % have acanthosis nigrans at presentation absence of obesity doesn’t R/O T2DM
DIAGNOSIS cont …
patient may be symptomless screen patients who are obese with F h/o DM blood glucose serum c-peptide and insulin levels ancanthosis nigrans hypertension polycystic ovary syndrome – 30 % IGT, 4 % T2DM dyslipidaemia
Risk factors for T2DM
insulin resistance – usually associated with obesity
F h/o DM in 1st or 2nd degree relative ethnicity; African-American, Hispanic,
Caribbean, Asian-American small for gestational age (IUGR) maternal gestational diabetes insulin resistance of puberty lack of physical activity high calorie diet
TREATMENT
1. PHARMACOLOGIC• INSULIN.2. NONPHARMACOLOGIC• DIET• EXERCISE• BEHAVIOUR CHANGE3. SELF MANAGEMENT
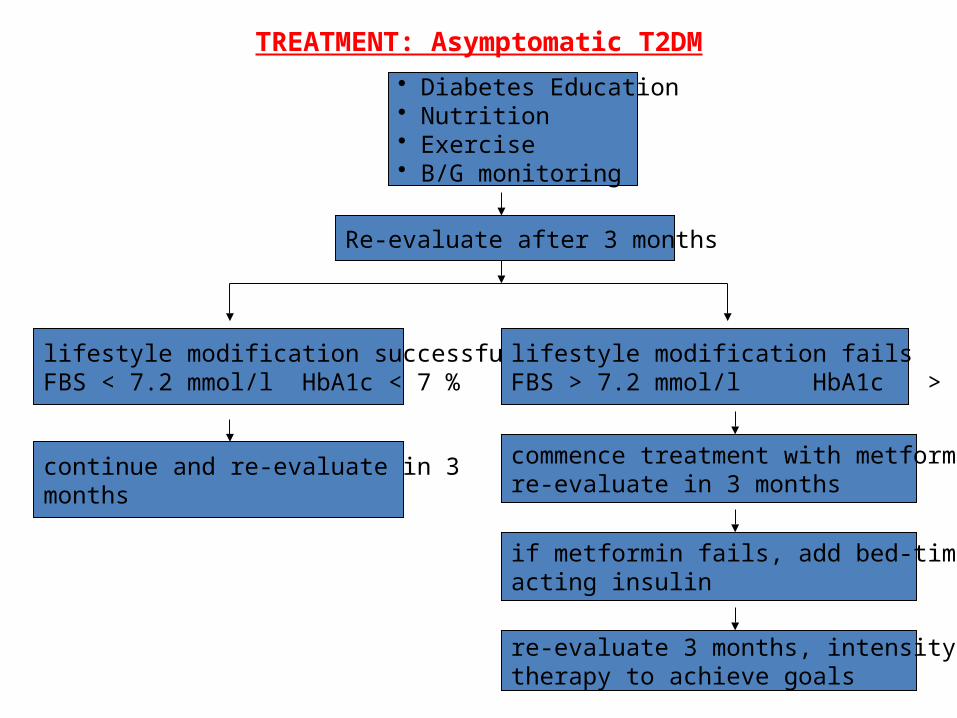
TREATMENT: Asymptomatic T2DM• Diabetes Education• Nutrition• Exercise• B/G monitoring
Re-evaluate after 3 months
lifestyle modification successfulFBS < 7.2 mmol/l HbA1c < 7 %
lifestyle modification failsFBS > 7.2 mmol/l HbA1c > 7 %
continue and re-evaluate in 3 months
commence treatment with metformin,re-evaluate in 3 months
if metformin fails, add bed-time long acting insulin
re-evaluate 3 months, intensity insulintherapy to achieve goals
PHARMACOLOGIC THERAPYInsulin + metformin only medications approved by FDA in
children with T2DM Patient with - severe hyperglycaemia
- weight loss- ketosis or ketoacidosis …require
treatment as in T1DM until B/G levels are normal Since patients are insulin resistant they require ~ 2
iu/kg/day initially, which is ↓ gradually as patient is put on metformin and may be weaned off insulin
give metformin as 500mg o.d, 500mg b.d, max 2g daily long acting insulins i.e insulatard,glargine are effective
basal insulins given together with metformin
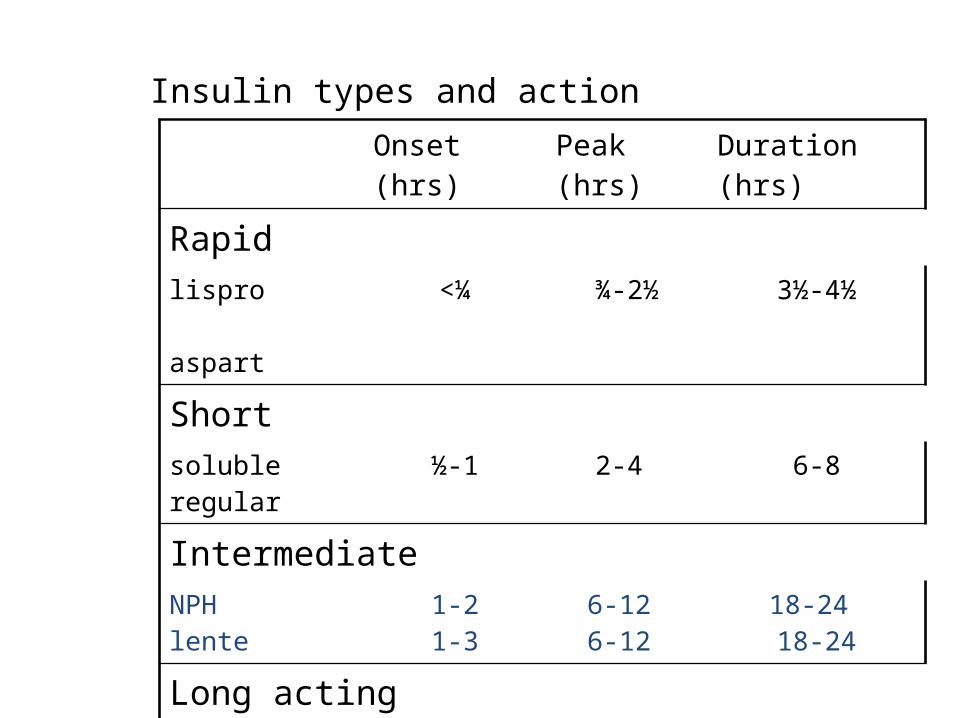
Insulin types and actionOnset (hrs) Peak (hrs) Duration (hrs)
Rapidlispro aspart
<¼ ¾-2½ 3½-4½
Shortsolubleregular
½-1 2-4 6-8
IntermediateNPHlente
1-21-3
6-12 6-12
18-24 18-24
Long actingultralente glarginedetemir
4-63-41-2
8-20 3-243-8
24 or more≥24 or more 12-24 (dose-dependent)
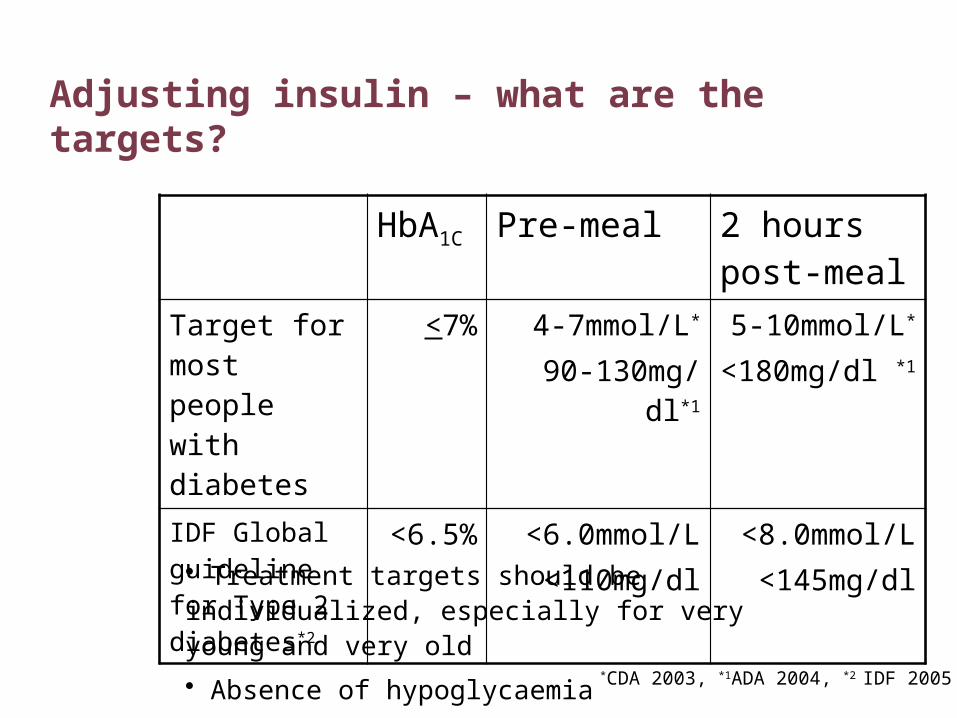
HbA1C Pre-meal 2 hours post-meal
Target for most people with diabetes
<7% 4-7mmol/L*
90-130mg/dl*15-10mmol/L*
<180mg/dl *1
IDF Global guideline for Type 2 diabetes*2
<6.5% <6.0mmol/L<110mg/dl
<8.0mmol/L<145mg/dl
Adjusting insulin – what are the targets?
*CDA 2003, *1ADA 2004, *2 IDF 2005
• Treatment targets should be individualized, especially for very young and very old
• Absence of hypoglycaemia
Adjusting insulin
Pattern management• Watch levels for 2-3 days
• Address hypoglycaemia first
• Aim for target fasting levels next
• Adjust by 2-4 units or 10%
• Wait 2-3 days
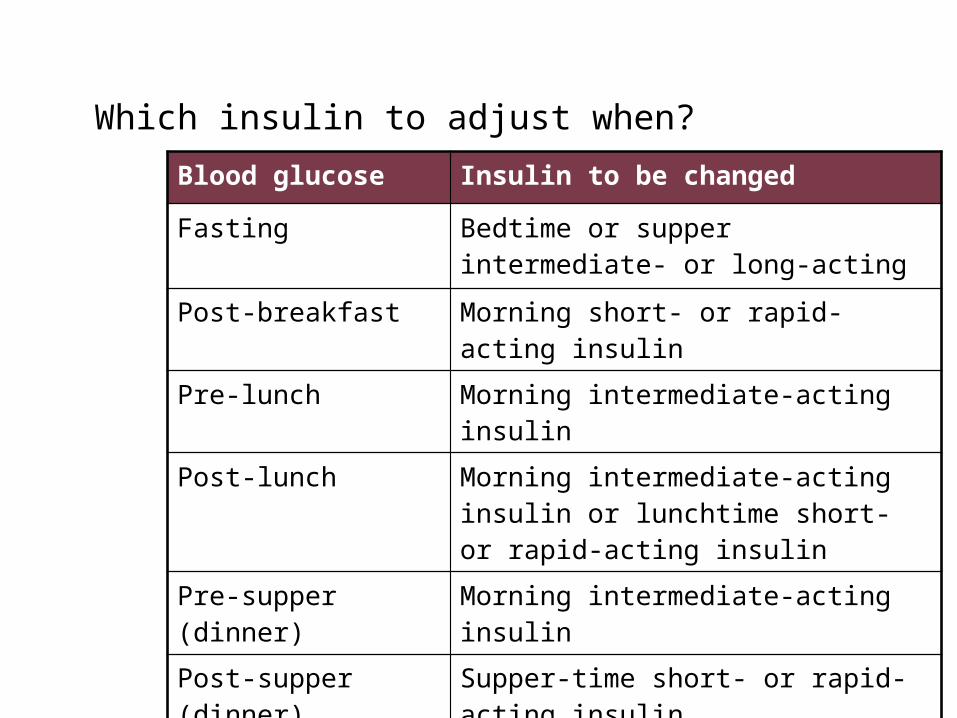
Which insulin to adjust when?Blood glucose Insulin to be changed
Fasting Bedtime or supper intermediate- or long-acting
Post-breakfast Morning short- or rapid-acting insulin
Pre-lunch Morning intermediate-acting insulin
Post-lunch Morning intermediate-acting insulin or lunchtime short- or rapid-acting insulin
Pre-supper (dinner) Morning intermediate-acting insulin
Post-supper (dinner) Supper-time short- or rapid-acting insulin
During the night Supper-time or bedtime intermediate-acting
Insulin practicalities
Timing• Soluble insulin: 30-45 minutes pre-meal• Short-acting insulin analogues: no more than 15 minutes
pre-meal and can be given post-meal• Intermediate- or long-acting insulins do not have to be
given in relation to a meal
Side effects
• Hypoglycaemia
• Weight gain
• Lipohypertrophy
• Lipoatrophy
• Insulin oedema
• Allergic reaction
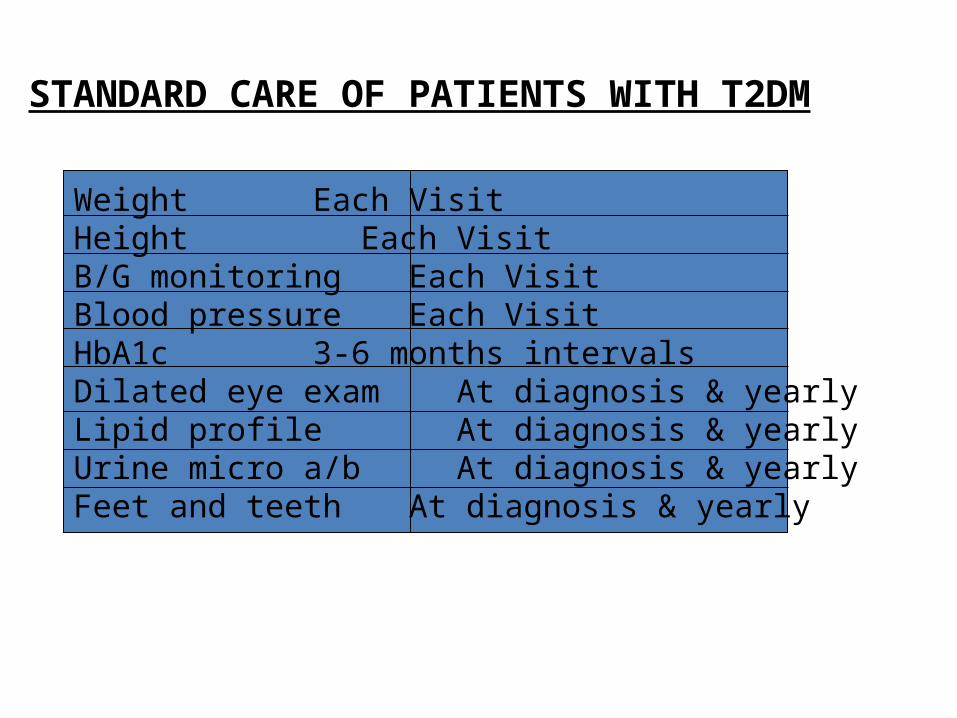
STANDARD CARE OF PATIENTS WITH T2DM
Weight Each VisitHeight Each VisitB/G monitoring Each VisitBlood pressure Each VisitHbA1c 3-6 months intervalsDilated eye exam At diagnosis & yearlyLipid profile At diagnosis & yearlyUrine micro a/b At diagnosis & yearlyFeet and teeth At diagnosis & yearly
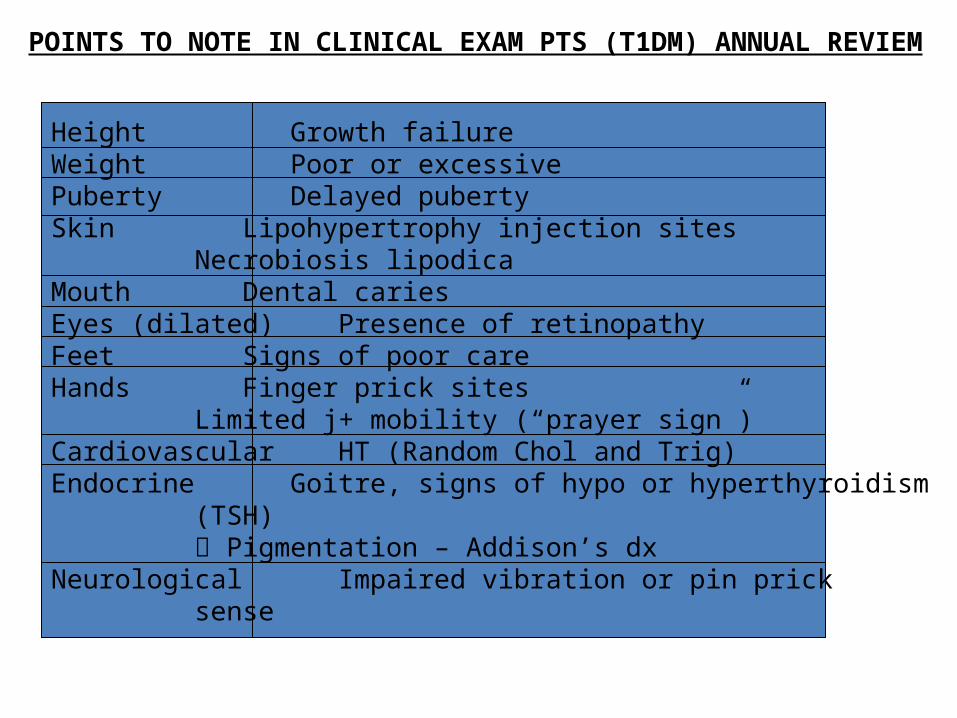
POINTS TO NOTE IN CLINICAL EXAM PTS (T1DM) ANNUAL REVIEM
Height Growth failureWeight Poor or excessivePuberty Delayed pubertySkin Lipohypertrophy injection sites
Necrobiosis lipodicaMouth Dental cariesEyes (dilated) Presence of retinopathyFeet Signs of poor careHands Finger prick sites
Limited j+ mobility (“prayer sign”)Cardiovascular HT (Random Chol and Trig)Endocrine Goitre, signs of hypo or hyperthyroidism
(TSH) Pigmentation – Addison’s dx
Neurological Impaired vibration or pin pricksense
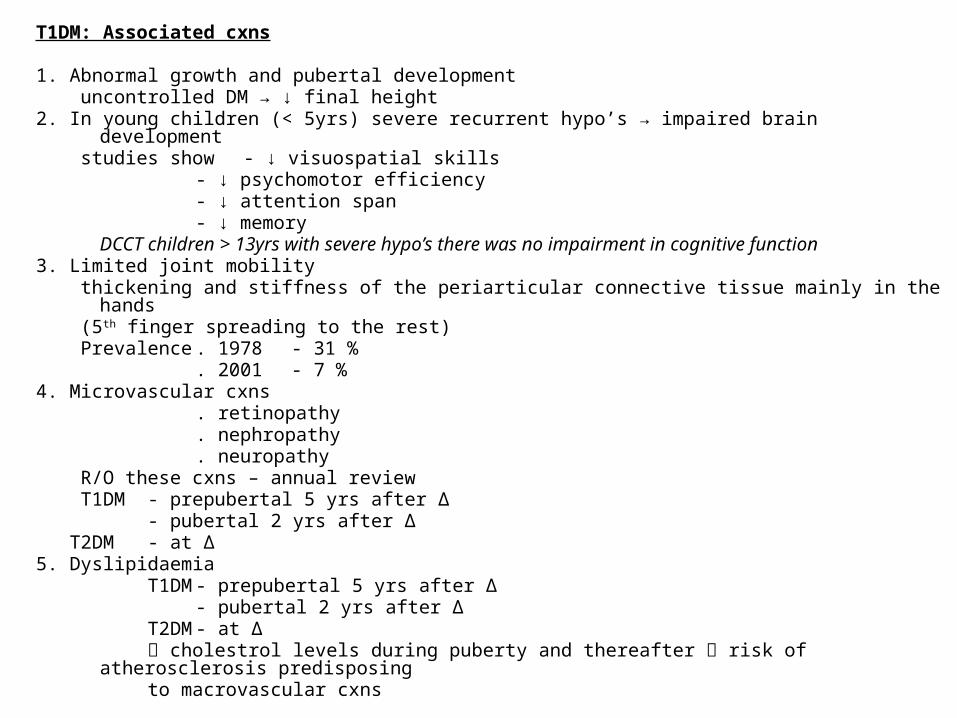
T1DM: Associated cxns
1. Abnormal growth and pubertal development uncontrolled DM → ↓ final height2. In young children (< 5yrs) severe recurrent hypo’s → impaired brain development studies show - ↓ visuospatial skills
- ↓ psychomotor efficiency- ↓ attention span- ↓ memory
DCCT children > 13yrs with severe hypo’s there was no impairment in cognitive function3. Limited joint mobility thickening and stiffness of the periarticular connective tissue mainly in the hands (5th finger spreading to the rest) Prevalence . 1978 - 31 %
. 2001 - 7 %4. Microvascular cxns
. retinopathy
. nephropathy
. neuropathy R/O these cxns – annual review T1DM- prepubertal 5 yrs after ∆
- pubertal 2 yrs after ∆ T2DM - at ∆5. Dyslipidaemia
T1DM - prepubertal 5 yrs after ∆- pubertal 2 yrs after ∆
T2DM - at ∆ cholestrol levels during puberty and thereafter risk of atherosclerosis
predisposing to macrovascular cxns
Education to parents and children
Knowledge of DM• pre-existing• current - what is DM, causes, consequence, life long cxns
Concept of “diabetes team” Insulin;
• role• types (short, long acting)• injection techniques• storage
B/G monitoring• when and how• interpretation of B/G levels
and adjustment of insulin doses Diet Exercise
• effect of exercise on CHO and insulin requirements
Education to parents and children cont …
Hypoglycaemia• causes• consequences - neurological impairement < 5 yrs
- hypo unwareness• treatment - sweets, sweet drink, sandwich
- glucose powder- glucagon I.M inject < 5 yrs 0.5mg
> 5 yrs 1.0mg- 10 % dextrose I.V 5ml/kg
• prevention - B/G < 4mmol/l during day- B/Bed : younger child (8 p.m) … B/G > 9mmol/l : older child (10 p.m) … B/G > 7mmol/l if less give additional night snack
Measurement of urinary ketones- when and how
Foot care
Education to parents and children cont …
Dental care “Honeymoon period”
- what is it- adjustment of insulin doses
Management of DM during intercurrent illnesses- continue insulin- monitor B/G regularly- test for urinary ketones regularly- eat CHO reg.- adjust dose of insulin to treat hyperglycaemia- hypoglycaemia … correct it
• ↓ insulin dose• encourage patient to eat small meals frequently
- treat underlying illness long term microvascular cxns importance of carrying patient identification
- medical card- bracelet
Education to parents and children
importance of follow-up by team- Paediatrician/Endocrinologist, Diabetic
Educators,Nutritionist, Podiatrist, Dentist, Opthalmologist
Diabetes youth campsAdolescents – smoking, Alcohol