Embed Size (px)
DESCRIPTION
Learning Disorders: Treatments and prevention Early identification and treatment, e.g., reading recovery, parental reading; Later, special placements Children are usually in regular classrooms with extra assistance either in or outside of classroom Direct instruction is necessary, e.g., sound-letter correspondence, steps in math problems, monitoring spelling and grammar Whole language vs. Code-empasis model of reading instruction. The former is good to create initial interest, but skills must be taught Metacognitive training: What are you doing? How long has it taken? Am you “on task”? External cues
Citation preview

Child Psychopathology
Learning Disability InterventionsVideotape
Attention DeficitsChapter 5

LD: Cycle of failure and motivation
• There is a cycle of failure, internal attributions of failure (“I am stupid”), external blame (“School is dumb”), loss of motivation to try, (“What is the point”), leading to further failure, which becomes self-fulfilling.
• Comorbid depression, anxiety, and self-esteem problems• Conflict with parents• Conflict with teachers• Peer problems can arise• Cycle must be stopped• Build on successes

Learning Disorders: Treatments and prevention
• Early identification and treatment, e.g., reading recovery, parental reading; Later, special placements
• Children are usually in regular classrooms with extra assistance either in or outside of classroom
• Direct instruction is necessary, e.g., sound-letter correspondence, steps in math problems, monitoring spelling and grammar
• Whole language vs. Code-empasis model of reading instruction. The former is good to create initial interest, but skills must be taught
• Metacognitive training: What are you doing? How long has it taken? Am you “on task”? External cues

Attention Deficits

C ore S ym p tom s o f a tten tion a l p rob lem s
A g e A p p rop ria teIn a tten tion
H yp erac tivity Im p u ls ivity
S ym p tom sA tten tion d e fic its

Additional criteria for ADHD
• Excessive, longterm, pervasive behaviors• Significant problems in multiple settings• Rule out other accounts of behavior• Onset before age 7 and go on for 6 months• Age inappropriate and persistant• DSM-IV describes predominantly inattentive
(ADHD-PI), hyperactive/ impulsive (ADHD-HI), and combined types

Associated Characteristics
• Deficits in metacognition and executive function• Difficulty applying intelligence and social skills to
everyday situations• Comorbid (~50%) learning disabilities• Health problems (allergies, ears, sleep)• Accident prone, clumsy, risky behaviors• Interpersonal problems with family, teachers. peers• Can lead to ODD, CD, anxiety, depression, Tourettes

Assessment of attentional problems
• Behavioral ratings– Multiple reporters and contexts (e.g., parents, teachers)– Hyperactivity, inattention, impulsivity
• Behavioral observations– In vivo (home, school) and in offic; What is “off task”; How do we
compare to others?– Recording devices (e.g., “wiggleometer”)
• Specific tasks– Matching familiar figures– Continuous Performance Task (CPT)
• Medical, family, school histories

The CPT: Measures of sustained attention and vigilence
AACZAAAZAAAABZAAAZABZAAAZ
O O O
C C C
A sequence of letters flash on a computer screen. Press the key when a “Z” follows an A, and at no other time. Scores: Omissions (O), Commissions (C)
Correct response: X X X

Prevalence
• 3-5% of school children• more common in boys than girls• more common in low SES groups• found in all cultures• 25 to 50% “grow out” of the problems or learn
to cope with the symptoms• school environment crucial: what are the
attentional demands? How much structure?

What does not cause ADHD
Old misconceptions about the causes of ADHD include - artificial flavoring and food additives- sugar and caffeine- “bad parenting”- food allergies- fluorescent lighting- misalignment of the spine
These theories were easily accepted by society,although there was little scientific evidence to back them up.

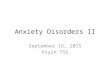
ADHD may be related to underarousal
The brain with ADHD has much less activity (red/orange/white) than the brain without ADHD. It shows that people with ADHD do not have enough activity in their brain to focus on what they are doing or control their thoughts

Theories of ADHD
• Deficits in arousal; underarousal, therefore hyperactivity for self stimulation
• Motivation deficits; low sensitivity to rewards and punishments
• Deficits in self regulation, metacognition; thus poor maintenance of effort
• Deficits in behavioral inhibition• Deficits in temporal processing and awareness; “do
this for 10 minutes”

Etiology
• Strong genetic component– 50% of behavior ratings accounted for by genetics– one or both parents often was “very active”– Treatments involve raising brain activity– Reticular activating system may cause underselectivity
• Neurobiological evidence related to dompaminergic, norepinephrine, serotonin
• Pre- and perinatal factors (prenatal alcohol, anoxia)• Family problems may be consequent to difficulties
– it is hard to parent a child with ADHD
• Toxins, allergies, diet have not received scientific support