Embed Size (px)
Citation preview

www.chcmj.ac.in
MEDICAL JOURNAL
In this issue
Polycystic Ovary Syndrome is an Epiphenomenon - An Opinion
Original Articles
Think Thyroid - Think Life: Pregnancy with Thyroid Disorders
Mitral Stenosis and Pregnancy - Perioperative Considerations
Case Reports
Newer Options in Management of Fibroid Uterus
Recurrent Pregnancy Loss - Obstetric Anti - Phospholipid Syndrome
From the Pages of History
Interview with – Prof. Sir Sabaratnam Arulkumaran
Volume - 5, Number - 3
July - Sep 2016
pISSN NO. 2277 - 8845 l eISSN NO. 2278 - 2044
International Peer Reviewed Journal
Chettinad Health City
Indexed in
INDEX COPERNICUS l GENAMICS JOURNAL SEEK l GOOGLE SCHOLAR
RESEARCH BIBLE l DIRECTORY OF SCIENCE l JOURNAL INDEX.NET
CITEFACTOR.ORG l DIRECTORY OF RESEARCH JOURNAL INDEXING l


Design & IT Support
Mr. S. T. Manigandan
Mr. SpK. ChidambaramRegistrar - CARE
Chief Editor
Dr. N. Pandiyan
Deputy Chief Editors
Dr. V. G. Ramesh
Dr. Pradeep G. Nayar
Editors
Dr. D. C. Mathangi
Dr. Sanjay Theodore
Dr. V. Anitha
National Editors
Dr. Dalim Kumar BaidyaAIIMS, New Delhi.
Dr. Suresh NairSri Chitra Institute of Medical Sciences & Technology, Thiruvananthapuram.
Dr. Vedantam RajshekharCMC,Vellore.
Dr. K.A.AbrahamApollo Hospitals, Chennai.
Dr. P.B.SeshagiriIISc, Bangalore.
Dr. Satish Kumar AdigaManipal University, Manipal.
Dr. M. BalasubramanyamMadras Diabetes Research Foundation
Dr. A.G.Narayana SwamySaveetha Medical College, Chennai.
Dr. K.JaishankarMadras Medical Mission, Chennai.
Dr.Thilaka MuthiahAIIMS, New Delhi.
Ms.T.PrathimaKMC, Manipal.
Dr. M. Narayana Reddy
Dr. D. Rajasekaran
Dr. A. Ruckmani
Dr. Sanjay Andrew Rajaratnam
Dr. B. Srinivasan
Dr. M. S. Srinivasan
Dr. Stephen Sudhakar
Dr. L. Uma Devi
Dr. Vasantha N Subbiah
Dr. R. Vijayashree
Mrs. Veena M Joseph
All rights are reserved
Chettinad Health City Medical Journal is published by the Chettinad Academy of Research & Education.
Apart from the fair dealing for the purposes of research or private study, or criticism or review, no part of the publication can be reproduced, stored, or transmitted in any form or by any means without prior permission.
Chettinad Health City Medical Journal and /or its publisher cannot be held responsible for errors or for any conse-quences arising from the use of the information contained in this journal. The appearance of advertising or product information in the various sections of the journal does not consti-tute an endorsement or approval by the journal and / or its publisher of the quality or the value of the said product or of claims made for it by its manufac-turer.
EDITORIAL OFFICE
Dr. N. Pandiyan
Chief Consultant,
Department of Reproductive Medicine,
Chettinad Health City,
Rajiv Gandhi Salai, (OMR, Chennai),
Kelambakkam, Kanchipuram Dist.,
Tamil Nadu - 603 103 India
T. +91 (0)44 4742 8300
F. +91 (0)44 4741 3343
Email:[email protected]
PUBLISHED BY
Chettinad Academy of Research & Education
WEBSITEwww.chcmj.ac.in
All disputes within the jurisdiction of the Madras High Court only
Legal Support
Mr. Balaji
Chettinad Academy of Research & Education (CARE)
Dr. K. RavindranVice Chancellor - CARE
Editorial Advisors
Dr. K. Ramesh Rao
Dr. R. Murugesan
Dr. P. Rajesh
Mrs. L. Lakshmi
Associate Editors
Dr. K. Senthil Kumar
Dr. P. Thirunavukarasu
Dr. D. Ramesh Raja
Dr. Shah Dupesh Khan
Assistant Editors
Dr. Sarah Subhashini P
Dr. Puvithra T
Statistical Advisor
Dr. S. Govindaraju
International Editors
Dr. Jayant G Mehta,BHR University Hospitals
NHS Trust, UK
Dr. Sudha Sundar,University of Birmingham, UK
Dr. Ram Dhillon,Middlesex University, UK
Dr. Malini Moni,Johns Hopkins University, USA
Dr. Sandro EstevesAndrology & Human Reproduction
Clinic, Brazil
Dr. Shankar GopinathBaylor College of Medicine, USA.
Dr. Arun ChandranUniversity of Florida, USA.
Dr. R. Arun Kumar
Dr. R. Ganesan
Dr. Indhumathi
Dr. S. B. Jothi Ramalingam
Dr.A. Krishnamoorthy
Dr. Lailu Mathews
Dr. E. Malligai
Dr. C. Manohar
Dr. N. Meenakshi
Dr. R. Murali
Dr. Nagajothi
Section Editors

Chettinad Health CityMEDICAL JOURNAL
pISSN NO. 2277 - 8845
eISSN NO. 2278 - 2044
Contents
EditorialVasantha N Subbiah
Perspective Article
Polycystic Ovary Syndrome is an Epiphenomenon - An OpinionPuvithra T, Pandiyan N
Original Article
Association Between Body Mass Index & Asthma Control Among Adult Asthmatics Population in South India: Cross Sectional Observational StudySuresh S, Aruna Shanmuganathan, Meenakshi N, Subramanian S, Nisha Ganga, Senthilvel Vasudevan
Study 0f Seroprevalence 0f Hepatitis B Virus In Routine Medico Legal Autopsies Ramalingam S, Narendar R
Perception Regarding Oral Health & Disease Among Medical Practitioners of Durg, Chhattisgarh – A Cross Sectional StudyAbhinav Parakh, Ashok Kumar Mohapatra, Yunus GY, Rohit Agrawal, Ram Tiwari, Anubhuti Jain
Review Article
Think Thyroid - Think Life: Pregnancy with Thyroid DisordersMuthukumaran Jayapaul
Mitral Stenosis and Pregnancy - Perioperative ConsiderationsLailu Mathews
Case Report
“The Balloon of Hope” - Successful Management of Tight Mitral Stenosis with Balloon Mitral Valvuloplasty In An Antenatal WomanSindhura M, Famida A M, Vijayalakshmi K, Pradeep Nayar
Uterine Papillary Serous Carcinoma Sathiya S, Famida A M, Vijayalakshmi K, Sailatha R, Renuka S
Malignant Mixed Mullerian Tumor of the UterusRijaphin R, Kavitha D, Anoop Sreevalsan, Vasantha N Subbiah
An Ovarian Juvenile Granulosa Cell Tumor in Adult Renuka S, Famida A M, Vijayalakshmi K, Sailatha R, Sathiya S
Asymptomatic Large Placental Chorioangioma In A PrimigravidaBinu Pattayail, Swarnapriya K, Vasantha N Subbiah
Class Room
Newer Options in Management of Fibroid UterusNalini A P, Kavitha Karthikeyan
Recurrent Pregnancy Loss - Obstetric Anti - Phospholipid SyndromeRajeswari S, Vignesh M
From the Pages of History
Heritage Museum at IOG (Gifford Museum)Famida AM
Interview with the Stalwart
Interview with – Prof. Sir Sabaratnam ArulkumaranVasantha N Subbiah, Vijayalakshmi K
105
106
108
112
120
127
132
137
140
144
147
150
153
157
164
165

Editorial
105
Warm greetings from the editorial team. The journal has evolved and grown over the last five years and is one of the widely accessed Indian journal. This issue has contributions from researchers and clinicians of various disciplines in medicine and Dentistry.
The perspective article on Polycystic Ovarian Syndrome (PCOS ) being an epiphenomenon puts forth an interesting opinion that excessive weight gain is the harbinger of PCOS and all other long term adverse health issues.
The original article discusses the association between body mass index and poor asthma control in adults suffering from this condition. It highlights one more complication that obese individuals suffer from, in addition the multitude of health problems that beset them. On a lighter note, “The dead do tell tales”, our second original article is a study on sero-prevalence of Hepatitis-B in medico-legal autopsies at a tertiary care Hospital, and it stresses the need for practicing univer-sal precautions even while working in the mortuary.
Modern day medical practitioners need to have a thorough working knowledge about oral health diseases. Poor oral health has a significant association with systemic illnesses and hence timely referral of patients with dental problems to dentists can prevent complications.
The review article on pregnancy with thyroid disorders is a comprehensive, lucid presentation of the thyroid physiology and various disorders affecting the gland in the pregnant woman, and its effect on the fetus /neonate. The review article on the peri -operative considerations in Mitral stenosis complicating pregnancy highlights the need for a multidisciplinary
Prof. Dr. Vasantha N. Subbiah
Prof. Dr. Vijayalakshmi. K
Email: [email protected]
approach in the care of such women, during pregnancy and childbirth and the specific anesthetic modifications needed during operative delivery.
Interesting case reports from the speciality of Obstet-rics and Gynecology, presented here reveal the wide variety of experiences that a practitioner of this discipline is exposed to.
Our classroom section has two articles, one on the newer modalities in the management of fibroid uterus and another on Obstetric Antiphospolipid Antibody syndrome. Both of them will enlighten the readers by their clear and extensive coverage of the topics.
The art of aiding childbirth with instruments has under-gone several innovations over centuries culminating in the current day use of forceps and ventouse. The pages from history take us through a guided tour of the heritage museum at the Institute of Obstetrics and Gynaecology, Madras Medical College, Chennai, India which houses some of the rarest collection of obstetric instruments and specimens.
The concluding article of this issue, is the interview with a stalwart. We have had the honour of interview-ing the legendary Prof. Sir, Sabaratnam Arulkumaran, a world renowned Obstetrician and Gynecologist who has served as president of FIGO(International Federa-tion of Obstetrics and Gynecology), the highest admin-istrative body for Obstetricians & Gynecologists world over. He has shared his thoughts and advice for the younger generations of Obstetricians. It has been an intellectually stimulating exercise for us to have brought out this issue of the journal. We hope you thoroughly enjoy reading it.

Chettinad Health City Medical Journal
Polycystic Ovary Syndrome is an Epiphenomenon - An Opinion
Perspective Article
Puvithra.T*, N.Pandiyan**
*Assistant Professor, **Prof & HOD, Department of Andrology & Reproductive Medicine, Chettinad Super Speciality Hospital,Chennai, India
Corresponding author - Dr.Puvithra ([email protected])
Chettinad Health City Medical Journal 2017; 5(3): 106 - 107
106
'Look deep into Nature, and you will understand everything better' - said Albert Einstein. Nature acclimatizes itself to the various influences, both external and from within. Yet, nature has a check on these changes, to prevent the undesirable consequences that can occur. The same statement holds good for the hypothalamo-pituitary gonadal axis, which is the primary regulator of the human reproductive function. The dormant hypothalamo-pituitary ovarian (HPO) axis in a child is awakened by complex neuro-endocrine mechanisms to signal the onset of puberty. Though the exact stimulus is yet to be identified, the onset of puberty in an individual predominantly depends on his/her body weight, being earlier in obese girls, and delayed in obese boys.1 This explains the requirement of optimum weight for normal functioning of the reproductive axis, and its extreme sensitivity to significant variation in the body weight. We have mentioned ‘significant’ and not exact values because, the weight change which leads to disturbances in the HPO axis can vary in each individual.
Studies are being published since the mid - 20th century, reaffirming that significant weight loss leads to amenorrhea.2 The association between body fat and reproduction is perchance an evolutionary phenomenon, programmed to prevent pregnancy until adequate fat stores are available for the mother and the growing fetus.
In a similar manner, weight gain also causes disarray in the normal functioning of the HPO axis. Though there are a large number of studies associating obesity with Polycystic ovary syndrome (PCOS), there has not been much explanation for PCOS in women with normal or low body mass index (BMI). There are quite a few studies which have proposed that weight gain could be the major cause for anovulation and polycystic ovary syndrome (PCOS) even in non-obese women.3 Inappropriate dietary habits and inadequate exercise lead to hyperglycemia and hyperinsulinemia. The increased circulating insulin decreases the levels of Sex-hormone binding globulin and thereby results in an increase in the free circulating testosterone, which gets converted to estrogen. The free testosterone prevents atresia of recruited cohort of immature
the increased circulating estrogen disturbs the function of the hypothalamo-pituitary ovarian axis, altering the secretion of gonadotropins, causing anovulation, which is the commonest cause of infertility. It is therefore evident that these series of events can occur even with a small, but significant gain in weight in a woman with genetic predisposition to PCOS.
The aforementioned hyper-hormonal state has been implicated in various pregnancy and fetal complications of PCOS. Studies report an increased incidence of gestational diabetes, preeclampsia and neonatal complications.4 Current emphasis is on epigenetics and the oocyte of the female child in-utero being exposed to this adverse hormonal milieu. Therefore, anovula-tion in PCOS women, can also be considered as a sign of nature trying to protect the mother and the fetus, from being exposed to the adverse hormonal milieu of hyperinsulinemia and hyperandrogenemia. It is a known fact that weight reduction causes spontaneous ovulation. But, rather than focusing on the primary cause, which is excess weight, we have been using alternative, easier strategies like ovulation induction. Spontaneous ovulation and pregnancy also avoids risks of multiple pregnancy and ovarian hyperstimulation syndrome (OHSS).
Ovulation induction with selective estrogen receptor modulators or gonadotropins can lead to follicle growth and ovulation. But the PCOS induced hormonal changes remain. Therefore, the aim should be to prevent weight gain by health education at high school level or insist on losing the weight gained after adolescence, which is going to be a much difficult task, yet worth attempting. It is important to treat the cause, rather than override or supersede the condition by ovulation induction strategies.
Furthermore, the hyper-hormonal status has been incriminated in a myriad of chronic health issues like Diabetes mellitus, Hypertension, Cardiovascular and Cerebro-vascular diseases. Unopposed estrogen action on the endometrium in anovulatory women also predisposes to endometrial malignancy.5
All these undesirable conditions right from infertility to malignancy, initially start with simple weight gain.
Dr.Puvithra completed her graduation from Annamalai University with internship at CMC Vellore in the year 2007. She has done her DNB in Obstetrics and Gynaecology. She completed her Fellowship in Clinical Andrology and Reproductive Medicine at Chettinad Hospital and Research Institute and is currently working as Assistant Professor in the department. Her area of interest is Polycystic Ovary Syndrome.
Volume 5, Number 3

Perspective Article Polycystic Ovary Syndrome is an Epiphenomenon - An Opinion
References
PCOS is enroute from weight gain to all long term health issues, and not the cause (Fig.1)
Volume 5, Number 3
Fig. 1 : Diagrammatic representation of consequences
of Weight gain in women
GDM – Gestational Diabetes mellitus; Type 2 DM – Type 2 Diabetes mellitus; CAD – Coronary Artery Disease; CVD – Cerebrovascular disease
The hypothalamo-pituitary ovarian axis, can be there-fore considered as the first checkpoint for weight alterations, sending warning signals in the form of oligomenorrhea or amenorrhea. If intervened at this point, by measures aimed at optimizing the body weight, further progression of the problem and the long-term health sequelae can be prevented.
Wang Y. Is obesity associated with early sexual maturation? A comparison of the association in American boys versus girls. Pediatrics. 2002;110(5):903-10.
Frisch RE, McArthur JW. Menstrual cycles (fatness as a determinant of minimum weight for height necessary for their maintenance or onset). Science. 1974; 185: 949 – 51
Puvithra T, Pandiyan N. Is Weight Gain the Precipitating Factor for Polycystic Ovarian Syndrome? A Hypothesis Based on a Retrospec-tive Study. Chettinad Health City Medical Journal. 2015; 4(3): 120 – 4
Boomsma CM, Eijkemans MJC, Hughes EG, Visser GHA, Fauser BCJM, Macklon NS. A meta-analysis of pregnancy outcomes in women with polycystic ovary syndrome. Human Reproduction Update. 2006; 12(6): 673 – 83.
Adam Balen. Polycystic ovary syndrome and cancer. Human Reproduction Update. 2001;7(6):522-5.
1)
2)
3)
4)
5)
Acknowledgement : We thank Dr.Radha Pandiyan for her support and valuable comments on this topic.
The authors declare no conflicts of interest.
107

Chettinad Health City Medical Journal
Association Between Body Mass Index & Asthma Control Among AdultAsthmatics Population in South India: Cross Sectional Observational Study
Original Article
Suresh.S*, Aruna Shanmuganathan**, N. Meenakshi***, Subramanian.S****, Nisha Ganga*****, Senthilvel Vasudevan******
Post Graduate*, Professor**, Prof & HOD***, Professor****, Senior Resident*****, Department of Respiratory Medicine,
Chettinad Hospital & Research Institute, Chennai, India.
***** Lecturer in Biostatistics and Epidemiology, King Saud Bin Abdulaziz University for Health Sciences, Riyadh, Kingdom of Saudi Arabia.
Corresponding author - Suresh S ([email protected])
Chettinad Health City Medical Journal 2017; 5(3): 108 - 111
Introduction Asthma affects 334 million people worldwide1 with Indian Prevalence of 2-3.5% in adults2. Uncontrolled asthma is a socioeconomic burden with significant impact on morbidity and mortality having global preva-lence of 30-50%3. The risk factors for uncontrolled asthma are multifactorial and vary in different geographic region and races. Demography, BMI, Pollu-tion, patient compliance to treatment, GERD and other comorbidities has been identified with poor asthma control. Obesity has been shown to be not only a risk factor for developing asthma but also associated with inadequate asthma control and poor quality of life. The association of obesity with asthma varies across differ-ent age groups, genders and races.The mechanism by which obesity predisposes to asthma and poor control are probably multifactorial ranging from mechanical alteration to systemic and airway inflammation and metabolic dysregulation that influences lung function and response to therapy4. Since studies on obesity and
asthma are limited in the Indian population the present study was undertaken to correlate asthma control with BMI.
Materials and methodsThe study was conducted at Department of Respiratory Medicine, Chettinad Hospital and Research Institute, Kancheepuram district, South India. This is a cross sectional observational study from May 2016 – October 2016. Study was conducted after obtaining informed consent and approval from the institutional ethics committee. Data was entered and analyzed with SPSS 17. Categorical variables were analysed with Pearson’s chi square test. P - value of <0.05 was taken as statistically significant.
Inclusion criteria • Age > 18 years
• Diagnosed with asthma for > 1 year
Dr. Suresh. S did his MBBS in Pondicherry Institute of Medical Science, Puducherry. Currently he is pursuing his final year post graduation in M.D Respiratory Medicine. He has presented scientific papers and poster in various National Pulmonology conferences.
Abstract
Background: Optimal asthma control is essential to prevent morbidity and mortality. Several factors including demographical, psychosocial and environmental have been associated with poor control. Obesity, apart from being a risk factor for asthma has also shown to be associated with poor asthma control. Hence the present study was undertaken to correlate Body Mass Index (BMI) with control of Asthma.
Aim of the study: To assess the association of BMI with Asthma control.
Materials and methods: The study was conducted at Department of Respiratory Medicine, Chettinad Hospital and Research Institute, Chennai, South India. This was a cross sectional observational study from May 2016- October 2016. Total of 49 asthma patients were included and grouped into level of control as per GINA guidelines. Demographic data including BMI were noted. Data analysis was done using appropriate statistical analysis.
Results: Mean age was 33.2 ± 12.9 years with slight female preponderance (F: M, 1.1:1). Mean BMI was 26.4 ± 4.0 and majority (42.8%) belonged to overweight group followed by 22.4 % were in the obese group. The percent-age of partly controlled and uncontrolled asthma was 44.8% and 55.2% respectively. BMI showed a signifi-cant correlation with both partly controlled and uncontrolled asthma (p-value <0.05). However, BMI did not show any significant association with gender.
Conclusion: Partly controlled and uncontrolled asthma patients were mostly associated with overweight and obese phenotypes. Hence, achievement of ideal BMI is necessary to achieve optimal asthma control and prevent exacerbation and complication.
Key Words: Asthma, Body Mass Index, Partly Controlled, Uncontrolled, Association
Volume 5, Number 3
108

Original Article Association Between Body Mass Index & Asthma Control Among Adult Asthmatics Population in South India: Cross Sectional Observational Study
109
• Physician-diagnosed asthma: shortness of breath, wheeze, cough, chest tightness, rhonchi on auscultation
And/Or
• Spirometry diagnosed asthma FEV1/FVC ratio less than 0.75-0.8 in adults (GINA -Global Initiative of Asthma guidelines)
• Good bronchodilator reversibility (FEV1 increases by more than 12% and 200 ml post bronchodilator or after 4 weeks of anti-inflammatory treatment)- GINA guidelines-2015.
• Control of asthma was assessed as per GINA guidelines
Exclusion criteriaOther Causes of Obstructive Airway Disease (OAD)
like Post TB sequelae, COPD and Bronchiectasis
ResultsAge and gender distribution: Out of 49 Asthma patients mean age was 33.2 ± 12.9 years with slight female preponderance F: M ratio was 1.1:1. (Fig 1 & 2)
Association of Asthma control with BMIThe percentages of partly controlled and uncontrolled asthma were 44.8% and 55.2%respectively.BMI showed a significant association with both partly controlled and uncontrolled asthma with p – value <0.05 as shown in (Table 2 & Fig 4)
Volume 5, Number 3
Fig 1: shows distribution of Age
Fig 2: shows gender distribution
BMIMean BMI was 26.38 and majority were in overweight group (42.8%) followed by 22.4 % were in the obese group. (Table 1 & Fig. 3)
Body Mass Index(Kg/m2)
Normal (18.5-24.9)
Over weight (25-29.9)
Obese (>30)
No. ofPatients
17
21
11
Percentage
32.6%
42.8%
22.4%
Table 1: Distribution of Body Mass Index amongAsthma patients
Fig 3: Shows distribution of BMI among Asthmapatients
Variables
PartlyControlled
Un controlled
Normaln (%)17 (32.6)
11(50.0)
6(22.2)
OverWeightn (%)21 (42.8)
11(50.0)
10(37.0)
Obesen (%)11 (22.4)
10(0)
11(40.7)
p - Value
0.002*
0.003*
Yates’ Chi - Square p - value < 0.01 StatisticallyHighly Significant
Table: 2 Association of Asthma Control with BMI
Fig 4: Correlation of Asthma Control with BMI

Volume 5, Number 3
DiscussionAccording to GINA guidelines optimal control of asthma is essential to prevent morbidity and mortality of the disease. Several asthma phenotypes based on risk factors have been identified including allergy, occupation, exercise induced, nocturnal (GERD) and the obesity asthma phenotype5. Several studies have shown that asthma and obesity are associated with severity of disease, poor control and inadequate response 6-8. Research is ongoing regarding mechanisms involved in asthma obesity phenotype.
Our study identified increasing BMI to be associated with both partly controlled and uncontrolled asthma. Overweight and obese subjects were significantly associated with poor asthma control. Similar observation by Barros9 et al in Brazil showed obese asthmatics to have worse asthma control. Several American studies by Peters10 et al, Stansford7 et al and Akerman11et al also showed same conclusion. However, studies on the obese asthma phenotype are limited in Indian population. A few contradictory studies by Sclerisme-Beaty12 et al, Sastre6 et al have shown no association of BMI with asthma control. The association between BMI and Gender was not statistically significant in our study. Few studies have showed a positive association with BMI and asthma control in women suggesting gender difference in obese individual14. Several mechanisms to explain the association of obesity with more severe disease and poor control have been elucidated including mechanical airway changes, leptin adiponectin pathway in systemic inflammation, oxidative stress and steroid resistance.
Fig 6: Mechanisms of Obese Asthma4.
A variety of mechanisms have been proposed as drivers of the physiologic and clinical observations in obese asthmatics, including changes in adipokines; T-helper type 1 (Th-1) skewed airway inflammation; lower asymmetric dimethylarginine (ADMA) to L-arginine ratio resulting in increased oxidative stress and decreased physiologic nitric oxide (NO), a mediator in smooth muscle dilatation; reduced functional residual capacity and expiratory reserved volume due to excess abdominal adiposity; interleukin-17 (IL-17) associated airway inflam-mation; steroid resistance and dampened response to mitogen-activated protein (MAP) kinase phosphatase-1 (MKP-1).
Interventional studies evaluating weight loss by surgical and nonsurgical means and on asthma control have shown significant improvement in airway hyper responsiveness and control13.But other studies do not demonstrate similar results14-15
ConclusionObesity and being overweight are risk factors for partly controlled and uncontrolled asthma. Hence large scale follow up studies to determine the effect of interventions to achieve optimum BMI with control of Asthma are needed.
The author declares no conflict of interest.
AcknowledgementsI would like to thank all the patients who have participated in our study.
The Global Asthma Report. http://www.globalasthmareport.org;2014 Agarwal R, Denning DW, Chakrabarti A. Estima-tion of the burden of chronic and allergic pulmo-nary aspergillosis in India. PLos ONE 2014 Dec;10.1371:e114745
Chung KF, Wenzel SE, Brozek JL, Bush A, Mario Castro, Peter Sterk J et al. International ERS/ATS Guidelines on Definition, Evaluation, and Treat-ment of Severe Asthma. European Respiratory Journal, 2013; 48(5):1261-1533.
Baffi CW, Winnica DE, Holguin F. Asthma and obesity: mechanisms and clinical implications. Asthma Research and Practice. 2015; 1(1): 1-7.
Shannon Novosad, Supriya Khan, Bruce Wolfe, Akram Khan. Role of Obesity in Asthma Control, the Obesity-Asthma Phenotype. Journal of Allergy. 2013.2013:538642
Sastre J, Olaguibe JM, Vina AL, Vega JM, Del Pozo V, Picado C .Increased body mass index does not lead to a worsening of asthma control in a large adult asthmatic population in spain. Journal of Investigational Allergology and Clinical Immunology.2010; 20(7):551–5.
Stanford RH, Gilsenan AW, Ziemiecki R, Zhou X, Lincourt WR, Ortega.H .Predictors of uncontrolled asthma in adult and pediatric patients: analysis of the asthma control characteristics and prevalence survey studies .Journal of Asthma. 2010;47(3):257 - 62.
Taylor B, Mannino D, Brown C, Crocker D, Twum-Baah, Holguin F. Body mass index and asthma severity in the National Asthma Survey. Thorax. 2008; 63(1):14-20.
Barros LL, Souza-Machado A, Corrêa LB, Santos JS, Cruz C, Leite M, et al .Obesity and poor asthma control in patients with severe asthma. Journal of Asthma.2011; 48(2):171-6.
References
1)
2)
3)
4)
5)
6)
7)
8)
9)
Original Article Association Between Body Mass Index & Asthma Control Among Adult Asthmatics Population in South India: Cross Sectional Observational Study
110

Volume 5, Number 3
Peters J.I, McKinney J.M, Smith.B, Wood.P, Forkner.E, Galbreath A.D. Impact of obesity in asthma: evidence from a large prospective disease management study. Annals of Allergy, Asthma and Immunology.2011;106(1):30-5
Akerman.M.J, Calacanis.C.M, Madsen.M.K. Relationship between asthma severity and obesity .Journal of Asthma.2004; 41(5):521-6.
Clerisme-Beaty EM, Karam S, Rand C, Patino CM, Bilderback A, Riekert KA, et al. Does higher body mass index contribute to worse asthma control in an urban population?. Journal of Allergy and Clinical Immunology.2009; 124(2):207–12.
10)
11)
12)
Stenius-Aarniala B, Poussa T, Kvarnstrom J, Gronlund E-L, Ylikahri M, Mustajoki P. Immediate and long term effects of weight reduction in obese people with asthma: randomized controlled study. British Medical Journal. 2000; 320(7238):827-32. Aaron SD, Fergusson D, Dent R, Chen R, Vandemheen KL, Dales RE. Effect of weight reduction on respiratory function and airway reactivity in obese women. Chest.2004; 125(6):2046–52.
Adeniyi FB, Young T. Weight loss interventions for chronic asthma. Cochrane Database of Systematic Reviews. 2012 Jul; 11(7):CD009339.
13)
14)
15)
111
Original Article Association Between Body Mass Index & Asthma Control Among Adult Asthmatics Population in South India: Cross Sectional Observational Study

Chettinad Health City Medical Journal
Study 0f Seroprevalence 0f Hepatitis B Virus In Routine Medico LegalAutopsies
Original Article
Ramalingam S*, Narendar R*
*Assistant Professor, Institute of Forensic Medicine, Madras Medical College, Chennai, India.
Corresponding author - Dr.S.Ramalingam ([email protected])
Chettinad Health City Medical Journal 2017; 5(3): 112 - 119
Introduction Autopsy examination is not only used for medico legal purpose but also in doing medical research and education by identifying new diseases or new manifestations of already existing diseases. It was mentioned in various studies by various authors that apart from establishing the cause of death it also helps in improving the quality in clinical service by evaluating the therapeutic effectiveness of various strategies1-3. The infectivity status of the deceased person was not known in majority of the cases subjected for autopsy, as said before. An autopsy may expose the prosecutors and other personnel to wide varieties of blood borne
and aerosolized infectious agents such as retro virus, hepatitis B and C viruses, and Mycobacterium tuberculosis4. Several studies revealed the increased prevalence of hepatitis B, C, D, G, tuberculosis, HIV, prion diseases, hantavirus, measles, HTLV-1 or bacte-rial infections in mortuary workers5.Despite the precautions taken to control the infection and availabil-ity of various vaccines, the health care professionals who had engaged themselves in the medical and medico legal practice face the risk of access to blood-borne viral infections by exposing them to body tissues or body fluids which are often loaded with infectious pathogens, irrespective of the stage of human remains. Safety becomes an issue, both in
Dr.S.Ramalingam, did his graduation from Chengalpattu Medical College and underwent DNB training in Department of General Surgery, Stanley Medical College, India. Later he did his post graduation in Forensic Medicine in the Institute of Forensic Medicine, Madras Medical College, Chennai, India. His academic interest is to create Medico - legal awareness among the medical fraternity and make them realise and understand the importance of Forensic Medicine. Dr.S.Ramalingam, currently is working as Assistant Professor, in the Institute of Forensic Medicine, Madras Medical College, Chennai, India. He
holds the post of Member representative in various associations - South India Medico-legal Association (SIMLA), Indian Academy of Forensic Medicine (IAFM), Tamilnadu Medico Legal Society (TNMLS) and Indian Academy of Medico Legal Experts (IAMLE).
Abstract
Background: An autopsy may subject the prosecutors and others to a wide variety of infectious agents, including blood borne and aerosolized pathogens such as human immunodeficiency virus, hepatitis B and C viruses, and My cobacterium tuberculosis. Several studies revealed the increased prevalence of hepatitis B, C, D, G, tuberculosis, HIV, prion diseases, hanta virus, measles, HTLV-1 or bacterial infections in mortuary workers. Safety becomes an issue, both in medical and ecological aspects regarding the protection of environment with the high seroprevalence of HIV and hepatitis viruses. The Study has been carried out to find the seroprevalence of Hepatitis B virus in 515 medico legal autopsies at our centre between April 2014 and September 2014.
Materials & Methods: The samples were tested blindly that the identity of the individual was unknown. The samples were collected via cardiac chamber at the time of autopsy. The samples were tested using HbsAg ELISA kit. The results were recorded in proforma and analyzed.
Results: Out of the 515 samples tested, Males occupy predominant number of cases, accounts for about 86.6% of study samples, whereas female constitute only 13.2% of the study sample. Of the 515 samples tested, HbsAg were detected in 18 samples (3.5%) using ELISA kit. All the positive cases were not previously known to have HBV-infection. Data such as demographics, cause of death, brought dead or treated, post mortem interval and positivity for HbsAg are recorded. In this study the prevalence of HBV is 100 % in Transgender as only one case was tested and it came as positive which is followed by male population.
Conclusion: The present study concludes that testing of HBV in medico legal autopsies is a convenient and effective method in monitoring the surveillance of HBV-infection in the general population and it can be used for epidemiological studies. . In screening postmortem blood for HbSAg, the present study represents that HbSAg ELISA kit is simple, rapid, no special equipment are required, even whole blood can be used and has very high sensitivity of 99.58% and specificity of 100%.
Key Words: Autopsy; Hepatitis B; Infection; High risk Autopsy; Universal Precaution
Volume 5, Number 3
112

Original Article Study of Seroprevalence of Hepatitis B Virus In Routine Medico Legal Autopsies
medical and ecological aspects regarding the protection of environment with the high seroprevalence of HIV and hepatitis viruses6. The highest rate of laboratory- acquired air borne and blood borne infections from the dead bodies was seen in autopsy workers, which was also established by the studies conducted between 1970 and 1989 in British clinical laboratories6,7. However, in many forensic situations the statistical risk of hepatitis and HIV infection are markedly greater in autopsies on bodies of homosexuals and drug abusers than in the general autopsy population8.
Aims and Objectives1)To study the seroprevalence of Hepatitis B virus among the routine cases brought for Medico Legal Autopsies. 2) To analyze the risk ratio and create awareness among the heath care personnel who handles dead bodies. 3) To diagnose the clinically unde-tected HBV cases. 4) To determine whether postmor-tem of dead bodies which are thought to be at low risk groups, are safe or not.
Methodology (Materials & Methods)The identity of the individual is not revealed at any part of the study. The samples were collected via cardiac chamber at the time of autopsy.
Subject Selection: Study was conducted on those cases, coming for Medico Legal autopsy to the Institute of Forensic Medicine, Madras Medical College, Chennai - 600003. The identity of the individual should not be disclosed in any part of the study.
Inclusion Criteria: All dead bodies subjected for autopsy
Exclusion Criteria: All decomposed dead bodies subjected for autopsy
Principle of the Test: Human HBsAg ELISA Kit which contains polystyrene micro well strips that are pre-coated with monoclonal antibodies specific to HBsAg is used to detect the presence of HBsAg in the given sample by using antibody "sandwich" ELISA method
Volume 5, Number 3
The amount of color intensity can be measured by deter mining absorbance using 450nm as reading wavelength with 620-690 nm reference wavelength which is proportional to the amount of antigen captured in the wells, and to its amount in the sample respectively. Wells remain colorless if it contains samples negative for HBsAg. (Fig 1)
Add serum or plasma sample of the deceased to the Polystyrene microwells whose strips are pre-coated with monoclonal antibodies specific to HBsAg
During incubation, if HBsAg is present in the sample, the specific Ag Ab complex formed is captured on the solid phase.
Then add the second antibody conjugated the enzyme horseradish peroxidase (the HRP-Conjugate) directed against a different epitope of HBsAg into the wells.
During the process of second incubation step, these HRP-conjugated antibodies and the anti-HBs-HBsAg complexes which are previ-ously formed during the first incubation bound to each other. After that, washing the wells removes the unbound HRP-conjugate.
Chromogen solutions A and B are added into the wells.
The colorless chromogens which are added are hydrolyzed by the bound HRP-conjugate in presence of the antibody-antigen-antibody (HRP) "sandwich" immune complex to a blue-colored product.
Once the reaction with sulfuric acid stops, the blue color turns yellow.
a)
b)
c)
d)
e)
f)
g)
Fig 1: Diagram of Generic 'Antigen Sandwich'Elisa for Completed Generic Elisa Assay
A – Blank G - Sample 1 Positive
B C D - Negative controls H - Sample 2 Negative
E F - Positive controls
Limitations of the test 1. Only un-pooled human serum or plasma can be used
2. HBV infection cannot be excluded without considering the other evidences for the same by taking only the negative HBsAg obtained
Performance Characteristics (i) Diagnostic specificity: 99.58%
(ii) Diagnostic sensitivity: 100%
Analysis and ResultsOut of the 515 samples tested, Males occupy the predominant number of cases, which accounts for about 86.6% of study samples, whereas female constitutes only 13.2% of the study sample. Of the 515 samples tested, HbsAg were detected in 18 samples (3.5%) using ELISA kit. All the positive cases were not previously known to have HBV-infection. Data such as demographics, cause of death, brought dead or treated, post mortem interval and positivity for HBsAg are recorded. Out of the 18 positive samples, 13 were male and 4 were female and 1 transgender. (Fig 2)
113

Volume 5, Number 3
Fig 2: Sex distributions among the study sample
Among 515 cases analyzed, predominant numbers of cases are male patients (86.6%). Out of the 18 positive cases, thirteen cases were positive among the males (72.2%) with 2.9 % of overall positive cases and four cases were positive among the females (22.22 %) with 5.9 % of overall positive cases, one case was found in transgender (5.5 %) with 0.2 % of overall positive cases. In this study the prevalence of HBV is 100 % in Transgender as only one case was tested and it came as positive which is followed by male population. (Fig 3)
Among 515 cases analyzed, predominant number of cases falls under age group between 21 to 30 and 41 to 50, followed by age group between 31to 40 and 51 to 60. Out of the 18 cases, six cases were positive in the age group 21-30, five cases were positive in the age group 41-50, four cases were positive in the age group 31-40 and three cases were positive in the age group 51-30 indicating that highest Seroprevalence was in the age group 21-30. (Fig 4) & (Fig 5)
Fig 3: Positivity among both the sexes
Fig 4: Age distribution among the study sample
Fig 5: Positivity percentage among the agedistribution in study sample
Among 515 cases analyzed, predominant number of cases falls under the category of Road Traffic Accidents (51.46%), followed by Fall from height (11.46%), Natural cause (10.3%), Poisoning (7057%) and others. Out of the 18 positive cases, four cases were positive in Natural cause, Three cases were positive in the RTA, Hanging and Murder cases, two cases were positive in TTA and Poisoning and one case was positive in the Fall from height. Even though Road traffic accidents constitute the majority of samples collected (51.46%) and Natural cause (with 7.56 % of Seroprevalence) constitutes 22.23 % of overall positive samples, highest Seroprevalence was noted in case of Hanging with 15.79% (Three cases were positive out of nineteen cases) with 16.67% of overall positive samples (Three out of eighteen cases). (Fig 6)
Original Article Study of Seroprevalence of Hepatitis B Virus In Routine Medico Legal Autopsies
Fig 6: Distribution of manner of death among thestudy sample
This shows that HBV screening is of great importance among the cases we receive for autopsy irrespective of manner of death. Hanging and natural cause in our study showed a relatively higher prevalence of HBV infections compared with other manners of deaths. (Fig 7)
114

This shows that HBV screening is of great importance among the cases we receive for autopsy as their HBV status was not known (66.67% were brought dead with no details regarding history of exposure or blood transfusion or HBV/HIV status)
Among 515 samples analyzed, predominant number of samples was collected between 12 to 24 hours (51.1%), followed 6 to 12 hours (19.6%) and 24 to 36 hours (19.6%). Out of the 18 positive cases, thirteen cases were positive among the samples which were collected 12 to 24 hours after death (positive percentage of 4.94%) with 72.22 % of overall positive cases. (Fig 10) & (Fig 11)
Among 515 cases analyzed, predominant number of cases falls under the category of Hospital treated patients (82.33%). In this study, Out of the 18 positive cases, twelve cases were positive among the brought dead category (13.2%) with 66.67 % of overall positive cases and six cases were positive among the hospital treated category with 33.33% of overall positive cases. (Fig 8) & (Fig 9)
Fig 7: Distribution of percentage of positive casesof the study sample among the manner of death
Fig 8: Distribution of brought dead and treatedcase among study sample
Fig 9: Distribution of Positive case among thebrought dead and treated case in the study sample
Fig 10: Distribution of Post mortem interval amongthe study sample
Fig 11: Distribution of Positive percentage amongPost mortem interval in the study sample
Volume 5, Number 3Original Article Study of Seroprevalence of Hepatitis B Virus In Routine Medico Legal Autopsies
The samples collected up to 36 hrs after death showed positive results for HBsAg. This shows that HBV screening is of great importance among the cases we receive for autopsy as HBsAg was detected even in the post mortem blood samples and hence consider all cadaver as a potential source of infection to health care workers (Fig 12)
Fig 12: Distribution of Occupation amongthe study sample
115

Volume 5, Number 3
This shows that HBV screening is of great importance among the Coolie and commercial sex workers which showed a relatively higher prevalence of HBV infections compared with other occupations (Fig 13)
This shows that HBV screening is of great importance in the Spouse and children when the deceased was found to be positive in autopsy samples. Dead bodies brought as unknown without no relatives showed a relatively higher prevalence of HBV infections compared with other category. Hence unless clearly indicated, unknown bodies should not be subjected for autopsy as a routine procedure.
DiscussionThe high frequency of the Hepatitis B virus infection among the deceased and longevity of the virus in their body tissues and fluids leads to an increased morbidity and mortality among the mortuary workers9. Amongst all the parenteral viruses, Hepatitis B virus has the highest transmissibility rate with a rate of about 100 times greater than HIV5,6,10. Carolin et al11 suggested that post-mortem blood samples should be collected within 24 hours. Challine et al recommended 12 h maximum time for drawing post-mortem blood samples.11 In my study HBsAg was detected in the post mortem blood samples up to 36 hours. In the year 2012 about 119,000 cases of viral hepatitis due to varied etiologies were reported in India12. In South-East Asia, the burden of chronic HBV infection was estimated as 100 million12. After HEV, HBV is the second most common cause of acute viral hepatitis in India with over 40 million HBV carriers12. In India, every year one million populations are at risk and about 100,000 die from HBV infection12. Though uncommon in India, HDV infection is observed in 10% to 20% of HBV positive patients12. In India, the epidemics due to the unsafe practice of sharing injection among IV drug users and healthcare personnels caring the infected people 46% of hepatitis B carriage and 38% of HCV infection were documented12. In India, perinatal transmission rate of HBV infection increases to 90% if the mother is positive for both HBsAg and hepatitis B e-antigen (HBeAg) rather than only HBsAg positive in which case it is only 10%12. Universal immunization against hepatitis B was introduced in India in 10 states in the year 2002 and in 2011 countrywide. A pentavalent vaccine which was introduced recently in some states gives protection against HBV also12.
Before commencing the postmortem, due to various reasons including social and cultural restrictions it will not be practically possible to collect detailed and reliable information about the risk factors which will help in assessing the HBV status of the deceased. Even if the history obtained from the relatives lacks the existence of risk factor it doesn’t means its non existence. Hence, a reliable bed side test which can be performed easily and rapidly to detect HBV infection in the mortuary will be very useful. Hence routine testing in all medico-legal autopsies irrespective of their previous HBV status will help in identifying the carriers. Li et al reported 23% prevalence of hepatitis B in forensic autopsy performers13. Plessis et al reported 8% prevalence of hepatitis B in forensic autopsy performers14.
In this study, the eighteen positive cases out of 515 cases were not known to have HBV which means they are clinically undetected for HBsAg. This indicates the presence of high risk people in the routine
Fig 13: Distribution of Positive percentage amongthe various occupational groups in the study sample
Among 515 cases analyzed, predominant number of cases falls under the Married category (78.1%) followed Single (21%). Out of the 18 positive cases, thirteen cases were positive in married population and four cases were positive in Singles. Even though Married population constitute the majority of samples collected (78.1%) with 72.33 % of overall positive samples, Both Married and Single constitutes Seroprevalence of about 3% positive percentage with unknown category having highest Seroprevalence of 20% (One in five cases positive) with 5.56% of overall positive samples (One out of eighteen cases). (Fig 14) & (Fig 15)
Fig 14: Distribution of Marital status amongthe study sample
Fig 15: Distribution of positive percentage amongthe marital status in the study sample
Original Article Study of Seroprevalence of Hepatitis B Virus In Routine Medico Legal Autopsies
116

medico-legal autopsies. The post mortem survival of the HBV was estimated in many studies. HBV survive outside the human body for up to 7 – 10 days and can withstand drying for at least a week5. When stored at 30-32 degree Celsius, HBV retains its infectivity for at least 6 months and when frozen at -15 degree Celsius, its infectivity will be retained for up to 15 years. The presence of very high viral load in blood and other body fluids during the early phase of infection suggests the need for practicing universal precaution which ensures efficient protection of autopsy personnel during routine medico legal autopsies.
The presence of HBsAg and anti - HBsAg in the postmortem serum which is stored for relatively long periods of time makes its detection a most reliable measure of antemortem HBV infection. Furthermore, it has been demonstrated that by assessing the post mortem changes in the serological parameters Kitchen and Newham established the post mortem stability of serological markers up to 24 hours after death 1 1, 15. Schuller demonstrated that the post mortem stability of the stability of the antibodies was similar when compared to the ante mortem screening done in live donors16.
The post mortem hemolysis, decomposition and bacterial contamination in dead bodies may not affect proteins such as the globulins that comprise antibodies 8, 13. In this study, it was estimated that the postmortem interval was ranging from 6 hours to 36 hours for detection of HBsAg. The viral load of the cadaver, viral strain, anti viral therapy taken when deceased is alive and the temperature of the cold storage in which the body is stored will influence the postmortem viral level. HBV is transmitted from person to person when they come in contact with body fluids such as blood, Cerebro spinal fluid, vaginal secretions, seminal discharges, breast milk, amniotic f luid, pericardial fluid and synovial fluids. Others body fluids like saliva, lachrymal secretions and urine unless they found to be contaminated with blood in adequate volume are not implicated in the transmission of HBV.
Weston and Lober in his study have recognized that nearly one third of the surgical glove puncture which occur with incidence of 8% during post-mortem remains undetected by the forensic pathologist who is performing the autopsy for a longer duration which cause preexisting injuries in his hand to be bathed with the infectious blood for a prolonged period of time17.
In my present study, the samples were tested blindly by not disclosing the identity of the individual in each and every stage. This study includes all types of cases from the general population which are brought for medico legal autopsy. Blood samples from heart were collected from 515 cases which are brought to Madras Medical College and Rajiv Gandhi Government General Hospital for medico legal autopsy. All the blood samples which were collected were tested for HBsAg using standard Human HBsAg ELISA kits which has a sensitivity and specificity of 99.58% and 100% respectively.
Out of 515 cases which were tested for HBsAg, eighteen cases were positive and among which thirteen
Volume 5, Number 3
were male, four were female and one was transgender. The positivity of 18 cases among 515, though look statistically insignificant, is higher than voluntary screening programs conducted by many organisations. Dr. Nirali shah et al in his study on the samples of voluntary blood donors demonstrated the Seroprevalence of HIV, HBV, HCV and syphilis which was found to be 0.154%, 0.887%, 0.101%and 0.22% respectively18. There are people who abstain from doing this screening blood test in many voluntary screening programs, which does not affect in this study. Thus, epidemiologically, routine screening for the presence of HBV in all dead bodies brought for medico legal autopsies is a sensitive indicator.
There are two varied opinions regarding the handling of the dead bodies harboring HBV in routine medico legal autopsies. One school of thought says that the universal precaution should be followed in all cases which are brought for autopsies which is practically difficult to follow in the developing country like India as it is not cost effective. The second thought says that universal precautions should be followed if the test done before doing autopsy in mortuary is positive which will reduce cost of burden to the management by reducing the need for the supply and use of personnel equipment kit for the autopsy personnel.
Limitation of The StudyIf the post mortem time interval is prolonged, the various factors such as lysis of RBC’s, autolysis, contamination by bacteria and loss due to decomposi-tion which will affect the postmortem testing of blood and body fluids are enhanced, but immunoglobulins, are considered as less likely to be affected by such factors mentioned before. This screening test for the HBsAg may not be sensitive if the person was in the window period.
ConclusionThe health care professionals who are involved in the postmortem work are exposed to a greater risk of occupational health hazard due to higher prevalence of various infectious diseases among the general population6. It is wise to practice the Universal Precautions in almost all dead bodies considering it as infectious as it becomes practically impossible to know the medical status of each and every body subjected for autopsy. The autopsy based occupational health hazards can be reduced by focusing on improvement in assessment, training, education, personal protection, autopsy techniques and autopsy room. Health care professionals involved in postmortem practice should be aware of the biohazards and radiation risks associated with the cadaver, instruments they handle and the atmosphere in which they work and take necessary steps to minimize the risks. Careful practice avoids many accidents in mortuary. The present study concludes that routine testing of HBV in all cases which are brought for medico legal autopsies is not only a convenient and effective method which is used to monitor the prevalence of HBV-infection among the general population, but also as a safety measure for utopsy personnel and as a study tool in epidemiological studies too19. There is no need for a
Original Article Study of Seroprevalence of Hepatitis B Virus In Routine Medico Legal Autopsies
117

Volume 5, Number 3
aspecial equipment to do this screening in postmortem blood samples for detection of HBsAg. The HBsAg ELISA kit which was used in this study has not only 99.58% sensitivity and 100% specificity but also simple to use and rapid in getting the result, can be used for doing the routine screening test in medico legal autopsies. Even whole blood can be used in this kit.
HBV positivity rate in my study population is 3.49%. The HBV status of all the eighteen seropositive post mortem blood samples was not known prior to autopsy testing. Even with a needle stick injury during autopsy, rate of infection appears to be less than 1%. Taking universal precautions with every autopsy is not practi-cal and economical in developing countries like India. Therefore, screening of postmortem samples and knowing the deceased HBV serological status prior to autopsy may be worthwhile in cases at high risk of HBV infection, preferably when the HBV status of the deceased is not known at the time of doing postmortem.
To conclude with universal precautions should be followed during routine autopsy procedures. Only experts and health care professionals those who are skilled in handling the infected materials are allowed to enter in to the postmortem examination room. Only those experienced professionals should conduct the autopsy examination as it is proved through many studies that the risk of accidental infection was more common, when the post mortem procedure was done by an inexperienced person5. Studies reported that the occurrence of lacerated wound in the body of the performer in 1 in every 11 autopsies conducted by inexperienced persons 6,20. Postmortem examination should not involve those persons with breach in the skin or mucosa or body immunity. The internal atmosphere of the postmortem examination room should be in such a way with sufficient space to avoid overcrowding and provide proper ventilation. Protective measures such as wearing gloves, headwear, masks, eyewear, shoes and full-covered gown should be given to and used by the mortuary staff while they are doing the postmortem work. Wearing double gloves during the autopsy or any surgical procedure will help us to minimize the risk of exposing themselves to the infected blood.
As all know that prevention is always better than cure, the preventive measures such as screening and immunization of the high risk group persons should be adopted. The group is considered as high risk or not based on the various factors such as history of exposure to infected samples and infected personnel, risk involved in their routine day to day practices and risk involved in the occupation in which they are engaged. Recommended safety measures should be followed in all areas wherever we comes in contact with blood and body fluids such as Delivery, Surgeries, Blood Transfusion, Intramuscular or intravenous injections, unprotected Sex and in autopsies.
Landefeld CS, Chren MM, Myers A, Geller R, Robbins S, Goldman L. Diagnostic yield of the Autopsy in a University Hospital and a Community Hospital. N Engl J Med. 1988;318(19):1249-54.
Harris MD, Blundell JW: Audit of Necropsies in a British District General Hospital. J Clin Pathol. 1991;44(10):862-5.
Gut AL, Ferreira AL, Montenegro MR. Autopsy: Quality Assurance in the ICU. Intensive Care Med. 1999;25(4)SSS:360-3
Nolte, Kurt B, Taylor, David G, Richmond, Jonathan. Biosafety considerations for autopsy American Journal of Forensic Medicine & Pathol-ogy. 2002;23(2):107-22
Sorin H, George CC, Mihai C, Mugurel CR, Elena N, Dan D. Infectious Risks In Autopsy Practice. Rom J Leg Med. 2011;19(3):183-8
Sharma BR, Reader MD. Autopsy Room : A Potential Source of Infection at Work Place in Developing Countries. Am J Infectious Diseases. 2005;1(1):25-33
Grist NR, Emslie JA. Association of Clinical Pathologist’s Surveys of Infection in British Clinical Laboratories. J Clin Pathology. 1994;47(5):391-4
Klatt EC, Noguchi TT. The Medical Examiner and Aids. Am J Forensic Med Pathol.1988;9(2):141-8
Galloway A, Snodgrass JJ. Biological and Chemical Hazards of Forensic Skeletal Analysis. J Forensic Sci.1998;43(5): 940–8.
Glick M, Muzuyka BC, Garfunkel AA. Viability, Transmissibility and Risk Assessment of HIV. Comp Contin Educ Dentist.1992;13(5): 374–80.
Carolin E, Birgit W, Ann-Sophie S, Ina W, Susanne P, Thomas M, et al. A Prospective Time-Course Study on Serological Testing for Human Immunodeficiency Virus, Hepatitis B Virus and Hepatitis C Virus with blood samples taken up to 48 H after death. J Med Microbiology.2011;60(Pt 7): 920–6
Quarterly Newsletter From The National Centre For Disease Control (NCDC) January-March 2014; 3(1):1–3
CDC. Biosafety in Microbiological and Biomedical Laboratories 5th Edition: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Institutes of Health, HHS Publication No. (CDC) 21-1112, Revised December 2009.
du Plessis, R, Webber, Saayman G. Bloodborne Viruses in Forensic Medicine Practice in South Africa. Am J Forensic Med Pathol. 1999;20(4): 364-8
References
1)
2)
3)
4)
5)
6)
7)
8)
9)
10)
11)
12)
13)
14)
Original Article Study of Seroprevalence of Hepatitis B Virus In Routine Medico Legal Autopsies
118

Volume 5, Number 3
Kitchen AD, Newham JA. Qualification of Serological Infectious Disease Assays for the Screening of tissue samples from deceased donors. Cell Tissue Bank.2011;12(2)117–24.
Baleriola C, Johal H, Robertson P, Jacka B, Whybin R, Taylor P, et al. Infectious Disease Screening of Blood Specimens collected Post-Mortem Provides comparable results to Pre-Mortem Specimens. Cell Tissue Bank. 2012;13(2):251-8
Weston J, Locker G. Frequency of glove puncture in the Post Mortem room. J Clin Pathol. 1992;45(2):177–8.
15)
16)
17)
Shah N, Shah JM, Jhaveri P, Patel K, Shah CK, Shah NR. Seroprevalence of HBV, HCV, HIV and Syphilis among Blood Donors at a Tertiary Care Teaching Hospital in Western India.Gujarat Medical Journal. 2013; 68(2):35-9.
Al-Wali A. Biological safety. In: Burton JL, Rutty GN, eds. The hospital autopsy. London: Arnold, 2001:25–36.
Butts JD. Forensic Pathology Automatically Exposure Prone. N C Med J. 1995;55(6): 210.
18)
19)
20)
Original Article Study of Seroprevalence of Hepatitis B Virus In Routine Medico Legal Autopsies
119

Chettinad Health City Medical Journal
Perception Regarding Oral Health & Disease Among Medical Practitioners of Durg, Chhattisgarh – A Cross Sectional Study
Original Article
Abhinav Parakh*, Ashok Kumar Mohapatra**, Yunus GY***, Rohit Agrawal****, Ram Tiwari*****, Anubhuti Jain******
*Senior Resident, Department of Public Health Dentistry, Govt Dental College & Hospital, Raipur, Chhattisgarh,
**Professor & H.O.D, Department of Public Health Dentistry, Rungta College of Dental Sciences & Research, Kohka – Kurud
Road, Bhilai, Chhattisgarh, ***Reader, Department of Public Health Dentistry, Rungta College of Dental Sciences & Research,
Kohka – Kurud Road, Bhilai, Chhattisgarh, ****Reader, Department of Public Health Dentistry, Maîtri College of Dentistry &
Research Centre, Durg, Chhattisgarh, *****Senior Lecturer, Department of Public Health Dentistry, Rungta College of Dental
Sciences & Research, Kohka – Kurud Road, Bhilai, Chhattisgarh, ******Post Graduate student, Department of Public Health
Dentistry, Rungta College of Dental Sciences & Research, Kohka – Kurud Road, Bhilai, Chhattisgarh
Corresponding author - Abhinav Parakh - ([email protected])
Chettinad Health City Medical Journal 2017; 5(3): 120 - 126
Introduction Oral health is an essential component of health throughout life. Oral health contributes to morbidity and mortality throughout one’s lifespan1. Poor oral health and untreated dental diseases have a long lasting impact on individual’s quality of life affecting basic human needs such as ability to eat and drink, swallow, maintain proper nutrition, smile and communicate1.
Oral diseases have important side effects on overall health, while systemic conditions may also influence oral health1. Therefore, oral health needs to be addressed by a multi-professional approach and at the same time be integrated into health promoting strategies and practices2. In addition, the common risk factor approach for chronic diseases calls for multi – professional collaboration3,4. Thus oral health promotion is needed within health care practices of physicians.
Oral diseases are usually overshadowed by other health needs, which are perceived to be more obvious and urgent by the attending physician, the individual patient themselves and their relatives5. But recently the dynamic interaction between oral diseases and systemic diseases has become a thought provoking and a research leading hypothesis. Researchers have studied in detail the potential mechanisms by which oral bacteria may contribute to systemic inflammation6. A large number of clinical studies have investigated the association between oral diseases and myriad systemic conditions, including cardiovascular diseases7, diabetes8, pneumonia9, rheumatoid arthritis10, and pregnancy outcomes11,12. This makes routine oral examination an extremely important and a viable area for the early diagnosis and prompt treatment of oral and non oral diseases13,14.
Dr. Abhinav Parakh received his Master’s degree in Public health Dentistry from Ayush & Health Sciences University, India and is currently associated with Government Dental College & Hospital, Raipur, India as a Faculty in Department of Public Health Dentistry with the role of educating and training Under Graduate students. He has a keen interest in research work related to Oral health care delivery systems primarily, though he also has been associated with many research works related to Tobacco & Oral health and Tobacco Cessation Programs. Several of his research works have been published in International and National Peer reviewed Journals.
Abstract
Objectives: The study was undertaken to address this crucial issue, in an attempt to assess the perception regarding the common oral and dental problems among the general medical practitioners in Durg district of Chhattisgarh state.
Methodology: A descriptive cross sectional questionnaire survey was conducted among registered medical practitioners in Durg district of Chhattisgarh state. A pre tested questionnaire was used for the survey. The study was carried out over a period of 2 weeks in the month of January 2015. The questionnaire was personally administered by the investigator.
Results: The response rate was 85%. 50% of the study subjects reported that patients with oral problems report to their clinic frequently. Around 34% of the study subjects only examined and prescribed medications whereas 66% of the study subjects examined the patients and perform adequate referral to dentists. The knowledge of the medical practitioners was inadequate.
Conclusion: Screening and referral by medical practitioners would surely benefit their patients by improving access to dental care.
Key Words: Oral health, perception, tooth diseases, physicians, referral
Volume 5, Number 3
120

Original Article Perception Regarding Oral Health & Disease Among Medical Practitioners
of Durg, Chhattisgarh – A Cross Sectional Study
121
India is a country with varied ethnic groups, geographic characters, culture, and religion with population of 1.22 billion15. Among them, 68.84% of the population is residing in rural areas where only 10% of manpower resources are available and vice versa in urban areas. The dentist population ratio is 1:10,000 in urban areas and 1:250,000 in rural areas16. For the population residing in rural areas, oral health care is provided by the general medical practitioners. Hence medical practitioners need to actively participate and play a pivotal role in oral health promotion. The need of the hour is for medical practitioners to have adequate knowledge about oral health as they are the one to whom majority of the population approach.
Health professionals have the potential to promote and improve oral health of the masses by delivering oral health messages, advocating regular dental visits and also conducting activities within their scope of duties. Dental knowledge of qualified medical practitioners is different when compared to the general public and also to that of dental practitioners. Even though they are qualified in the medical faculty their knowledge about dental diseases, relationship of oral health with systemic diseases and life threatening dental diseases are scarce17. Not much research on general physicians’ awareness of oral health in the central region of India is available on search of literature. Hence, this study was undertaken to address this crucial issue, in an attempt to assess the perception regarding the common oral and dental problems among the general medical practitioners in Durg district of Chhattisgarh state.
Methodology
1. Study designA descriptive cross sectional questionnaire survey was conducted among registered medical practitioners in Durg district of Chhattisgarh state. A pre tested questionnaire was used for the survey. All questions used in the questionnaire were close ended.
2. Sample size and sampling methodSampling frame comprised of all the medical practitioners registered with Indian Medical Association (IMA) of Durg district. A list of all the registered medical practitioners in Durg was obtained from the local branch of IMA. All the medical practitioners were personally contacted and those who provided consent and returned the completed questionnaire were included in the study.
Inclusion criteria:
• Medical practitioners registered with the Indian Medical Association of Durg branch
• Practicing in private clinics in Durg
• Providing consent to be included in the study and returning a completely filled questionnaire
Volume 5, Number 3
3. Ethical Clearance & Informed consentThe study protocol was approved by the Institutional Review Board of Rungta College of Dental Sciences & Research, Bhilai. Individual written informed consent was obtained from each of the study participants after explaining the objectives of the study.
4. QuestionnaireThe questionnaire of the study was developed from previously validated survey18 with certain required modifications. First, the questionnaire was assessed for face and content validity by experts in dental public health for relevancy and clearness. Then, a pilot survey was conducted among medical practitioners (n=10) and based on the study subjects opinion regarding the clarity of questions, the questionnaire did not required any revision. The internal consistency of the questionnaire was checked by subjecting the data to Cronbach's alpha test. The Cronbach's alpha was found to be 0.93 (93%) reflecting a high degree of reliability.
The questionnaire included the demographic details and the information related to importance of oral health, oral health maintenance, relationship of oral diseases with systemic diseases and oral diseases and their management.
5. Collection of dataThe study was carried out over a period of 2 weeks in the month of January 2015. The questionnaire was personally administered by the investigator. The medi-cal practitioners were approached personally and the purpose of the study was explained. It was also mentioned that responses would remain confidential. It took around 10 minutes to complete the questionnaire. The filled questionnaire was collected after being answered by the participants and subjected to statistical analysis.
6. Statistical analysisData obtained from this questionnaire was analysed using the SPSS statistical package (version 18; Chicago, IL, USA). The data was subjected to descriptive analysis (frequency distributions).
ResultsOut of 102 study subjects, 63 (61.8%) were males and 39 (39.2%) were females (Table 1). The mean age of the study subjects was 35.35 ± 9.07 with a range of 25 – 60. The experience of the practitioners varied from 1 -34 years with a mean of 8.06 ± 8.55 years. One hundred and two completely filled questionnaires out of the one hundred twenty distributed, giving a response rate of 85%. 50% of the study subjects reported that patients with oral problems report to their clinic frequently. Around 34% of the study subjects only examined and prescribed medications whereas 66% of the study subjects examined the patients and perform adequate referral to dentists. The results of the study are shown in the following table (Table 1).

Volume 5, Number 3
A.
Perception of study subjects regarding relation of oral health with general health
Question Agree Disagree Neither agree nor disagree
Oral health is an integral part of general health
102 (100%) 00 00
Oral health has an influence on the overall quality of life.
99 (97.1%) 00 03 (2.9%)
Certain systemic diseases can manifest in the oral cavity
99 (97.1%) 03 (2.9%) 00
Oral diseases have an implication on certain systemic diseases/conditions like cardiovascular diseases, Pregnancy, low birth weight babies, preterm baby etc.
93 (91.2%) 03 (2.9%) 06 (5.9%)
Dental care is important for pregnant women
99 (97.1%) 03 (2.9%) 00
B. Perception of study subjects regarding aetiology and prevention of dental caries
Dental caries (tooth decay) and gum diseases are plaque mediated diseases
93 (91.2%) 00 09 (8.8%)
Dental caries is a complex disease but can be prevented by adopting healthy oral health behaviours
90 (88.2%) 00 12 (11.8%)
Micro‑organisms that cause dental caries are transmitted mainly from the mother to the child
18 (17.6%) 60 (58.9%) 24 (23.5%)
Frequent consumption of sugar containing food is more detrimental than the quantity of the sugar consumed
63 (61.8%) 33 (32.3%) 06 (5.9%)
Proper brushing of teeth and flossing will enable to prevent both dental caries and gum diseases
75 (73.5%) 24 (23.6%) 03 (2.9%)
Fluorides have a protective role against dental caries
102 (100%) 00 00
C. Perception of study subjects regarding maintenance of dentition
Proper maintenance of deciduous dentition is not important because they are going to be replaced by permanent dentition.
27 (26.5%) 69 (67.6%) 06 (5.9%)
Artificial teeth can perfectly replace the function of natural teeth. Hence, too much care for natural teeth is unwarranted.
33 (32.4%) 63 (61.7%) 06 (5.9%)
D. Perception of study subjects regarding oral cancer aetiology
Question Agree Disagree Neither agree nor disagree Tobacco is the only risk factor for oral cancer
42 (41.2%) 54 (52.9%) 06 (5.9%)
All precancerous lesions of the oral cavity invariably lead to oral cancer
Table 1 : Results
if the predisposing factors are removed
30 (29.4%) 60 (58.8%) 12 (11.8%)
Original Article Perception Regarding Oral Health & Disease Among Medical Practitioners
of Durg, Chhattisgarh – A Cross Sectional Study
122

123
Volume 5, Number 3
E. Perception of study subjects regarding alignment of teeth and para-functional habits
Question Agree Disagree Neither agree nor disagree Alignment of teeth is done for aesthetic purpose only
69 (67.6%) 27 (26.5%) 06 (5.9%)
Para‑functional habits like thumb sucking, lip biting, lip sucking and nail biting are very common among children. Do these habits need to be curbed?
102 (100%) 00 00
F. Perception of study subjects regarding oral diseases
Question Agree Disagree Neither agree nor disagree Soft drinks can cause loss of dental enamel which is the hardest tissue in the human body
99 (97.1%) 03 (2.9%) 00
Saliva can be used in the diagnosis of oral as well as certain systemic diseases
81 (79.4%) 18 (17.7%) 03 (2.9%)
G. Perception of study subjects regarding periodontal diseases
Question Options Response
In oral cavity, periodontal diseases affects:
a. Enamel & Dentin b. Mucosa of lip, cheek,
hard and soft palate c. Gums and tooth socket d. All of the above
3 (2.9%) 3 (2.9%) 60 (58.8%) 36 (35.4%)
H. Perception of study subjects regarding traumatic dental injuries
Question Options Response
A tooth fallen out of socket due to trauma can be re‑implanted into the tooth socket
a. Possible, can be done b. Should not be done c. Don’t know
60 (58.8%) 21 (20.6%) 21 (21.6%)
Mouthguards are useful in preventing sport related injuries/trauma
a. Agree
b. Disagree
c. Neither agree nor disagree
96 (94.2%) 03 (2.9%) 03 (2.9%)
DiscussionOral diseases are of public health interest and are preventable. Early detection of oral diseases facilitates prompt treatment and restoration to normal health and function. Delay in referral has a devastating effect on the associated morbidity and mortality. The role played by medical practitioner to improve the oral health of the population depends on his knowledge about oral disease and its impact on general health.19-22
Interdisciplinary approach has become the patient management strategy in recent decades. This approach requires close cooperation between doctors and dentists. A team of well informed medical practitioners and dentists can benefit the society. Medical practition-ers can act as good source of knowledge providers to the general public.23-26
Rapid growth in information technology has placed a significant burden on the public to acquire relevant information. Poor literacy skills can affect public’s ability to seek further health information and make informed healthcare decisions. Medical practitioners form an important link in the dissemination of relevant knowledge to the general public.23-29
This cross sectional study was undertaken to assess the perception of general medical practitioners regarding oral diseases. In the present study there was a unanimous agreement among the medical practitioners that oral health is a part of general health. Most of the medical practitioners were of the view that certain systemic diseases can manifest in oral cavity and oral diseases have an implication on certain systemic diseases such as diabetes mellitus and cardiovascular disorders.
Original Article Perception Regarding Oral Health & Disease Among Medical Practitioners
of Durg, Chhattisgarh – A Cross Sectional Study

Volume 5, Number 3
The results are in concordance with studies by Patil A et al., Srinidhi S et al19 and Umesh et al26. This finding suggests that the respondents were conversant with the vast body of evidence linking oral and systemic health.30-33
This could be because the MBBS curriculum in India includes a dental posting in which they have an expo-sure to dental health aspects which improves their awareness, knowledge and attitude towards dentistry. The implications of the knowledge include the dilemma of patients being managed by these respondents that may need a dental referral, but are denied due to the ignorance of physician.
It was also observed that most of the medical practitioners in our study felt confident with the oral examination. Most of them asserted that they did examine the oral cavity of their patients routinely, though this response could also have been made due to an interviewer bias. The results of this study agreed with those of the study of Morgan et al.34
Results of the study showed that medical practitioners were aware regarding the causes of dental diseases. Around 92% of the respondents answered that dental caries and periodontal diseases are plaque mediated. This is comparatively more than a study reported by Srinidhi S et al19. But, only 17.6% of the medical practitioners were aware of the fact that dental caries causing bacteria can be transmitted from the mother to the child. Child-rearing habits which facilitate saliva transfer from adults to the child, such as sharing of food and utensils and habits which involve close contact, such as breast feeding and sleeping beside the mother, were also significantly associated with colonization of S. Mutans. 35,36
Regarding maintenance of dentition, many of the medi-cal practitioners did not give importance to mainte-nance of deciduous dentition as they were of the view that it is eventually going to be replaced. Surprisingly, around one third of the respondents replied that too much care for natural teeth is unwarranted as artificial teeth can perfectly replace the function of missing teeth. This highlights that more comprehensive knowledge need to be provided to the medical practitioners.
However, knowledge regarding oral cancer was not up to mark. Around 40% of the medical practitioners believed that tobacco is the sole risk factor for oral cancer and around 30% were of the opinion that all pre cancerous lesion of oral cavity invariably lead to oral cancer even if the pre disposing factors are removed.
It is however, unrealistic to expect all the medical practitioners to be conversant with all the nuances of the oral health and diagnosis. The identification of specific areas that have important health implications for the patient, and at the same time, the conditions to which the doctors can be easily sensitized to, is there-fore a priority.
Limitations of the study are that the number of items in our instrument (questionnaire) had to be limited,
because of the nature of the sample. We did not expect the busy medical practitioners to devote more than 15 minutes of their time in answering our questions. Hence, though the questions covered a gamut of important areas, no in-depth probing could be carried out. Hence a focus group interview would probably be a better way for gathering more information in the specific area.
Recommendations• To conduct seminars for newly graduated medical practitioners to update their dental knowledge especially on common misconceptions.
• To encourage newly graduated medical practitioners to examine the oral cavity (including teeth and gums) during their general examination for patients.
• To encourage the setting up of multi speciality clinics including medical practitioners and dental practitioners for the benefit of providing services under one roof.
• To conduct continuing education programmes to improve their knowledge, attitude and awareness about various dental diseases.
ConclusionTo conclude, the knowledge regarding oral health and disease among medical practitioners was inadequate. Therefore, it is imperative to educate and empower medical practitioners about oral health to change the perception of dentists as the only ones responsible for maintaining good oral health in the population.
Inglehart MR, Filstrup SL, Wandera A:Oral health and quality of life in children. In Oral health- related quality of life. Edited by Inglehart MR,Bagramian RA. Chicago: Quintessence Publishing Co; 2002:79–88
Petersen PE:Global policy improvement of oral health in the 21st century–implications to oral health research of World Health Assembly 2007, World Health Organization. Community Dent Oral Epidemiol 2009, 37:1–8
World Health Organization (WHO): Global strategy for the prevention and control of non communicable diseases. Geneva: WHO; 2000.
Sheiham A, Watt RG: The common risk factor approach: a rational basis for promoting oral health. Community Dent Oral Epidemiol 2000,28(6):399–406.
Opeodu OI, Ogunrinde TJ, Fasunla AJ. An assessment of medical doctors' perception of possible interrelationship between oral and general health. Eur J Gen Dent. 2014;3(2):120-4
Teles R, Wang CY:Mechanisms involved in the association between periodontal diseases and cardiovascular disease. Oral Dis.2011,17(5):450-461
References
1)
2)
3)
4)
5)
6)
Original Article Perception Regarding Oral Health & Disease Among Medical Practitioners
of Durg, Chhattisgarh – A Cross Sectional Study
124

125
Volume 5, Number 3
Hung HC, Joshipura KJ, Colditz G, Manson JE, Rimm EB, Speizer FE, et al. The association between tooth loss and coronary heart disease in men and women. J Public Health Dent.2004;64(4):209–215
Lalla E, Papapanou PN. Diabetes mellitus and periodontitis: a tale of two common interrelated diseases. Nat Rev Endocrinol. 2011;7(12):738–748
Scannapieco FA, Bush RB, Paju S. Associations between periodontal disease and risk for nosocomial bacterial pneumonia and chronic obstructive pulmonary disease, a systematic review. Ann Periodontol. 2003;8(1):54–69
Dissick A, Redman RS, Jones M, Rangan BV, Reimold A, Griffiths GR, et al. Association of periodontitis with rheumatoid arthritis: a pilot study. J Periodontol. 2010;81(2):223–230
Canakci V, Canakci CF, Canakci H, Canakci E, Cicek Y, Ingec M, et al. Periodontal disease as a risk factor for preeclampsia: a case control study. Aust NZ J Obstet Gynaecol. 2004;44(6):568–573
Meurman JH, Furuholm J, Kaaja R, Rintamaki H, Tikkanen U. Oral health in women with pregnancy and delivery complications. Clin Oral Investig. 2006;10(2):96–101.
Chen ZY, Chiang CH, Huang CC, Chung CM, Chan WL, Huang PH, et al. The association of tooth scaling and decreased cardiovascular disease: a nationwide population-based study. Am J Med 2012;125(6):568–575
Stewart JE, Wager KA, Friedlander AH, Zadeh HH. The effect of periodontal treatment on glycemic control in patients with type 2 diabetes mellitus. J Clin Periodontol 2001;28(4):306–310 http://www.indiaonlinepages.com/population/india-current-population.html.
Kishor KM. Public health implications of oral health–inequity in India. J Adv Dent Res 2010;1:1-10.
Jagadish Chandra, Chandu GN, Prashant GM. Dental awareness and attitudes of medical practitioners of Davangere city. Journal of Indian Association of Public Health Dentistry 2006;8:38-43.
Sujatha BK, Yavagal PC, Gomez MS. Assessment of oral health awareness among undergraduate Medical Students in Davangere city: A cross-sectional survey. J Indian Assoc Public Health Dent 2014;12:43-46
Srinidhi S, Ingle NA, Chaly PE, Reddy C. Dental Awareness and Attitudes among Medical Practi-tioners in Chennai. J Oral Health Comm Dent 2011; 5(2): 73-78
7)
8)
9)
10)
11)
12)
13)
14)
15)
16)
17)
18)
19)
Rabiei. Physicians’ knowledge of and adherence to improving oral health. BMC Public Health 2012;12:855.
Rajmohan M, Madankumar PD, Shivakumar M, Uma KS. Awareness on oral health among Ayurvedha and Siddha practitioners in Chennai, Tamil Nadu – a questionairre study. Medical Journal of Islamic World Academy of Sciences. 2012; 20(2):43-48
Shah HG, Ajithkrishnan CG, Sodani V, Chaudhary NJ. Knowledge, attitude and practices among Gynecologists regarding Oral Health of expectant mothers of Vadodara City, Gujarat. International Journal of Health Sciences 2013; 7(2):136-140.
Rajesh H, Boloor V, Rao A, Prathap S. Knowledge of periodontal disease among group of health care professionals in Yenepoya University, Mangalore. J Educ Ethics Dent. 2013;3:60-5.
arumathi T, Saravanakumar B, Datta M, Nagar-athnam T. Awareness and Knowledge of Common Oral Diseases Among Primary Care Physicians. Journal of Clinical and Diagnostic Research. 2013;7(4): 768-771
Sharath KS, Prabhu M, Thomas B, Shetty S. Cross sectional study of attitude, practice and Knowl-edge of oral hygiene practices and dental Treat-ment in health care professionals in south Canara district. NUHS 2014;4(4): 28-32
Umesh, Nagesh L, Chavan S. Assessment of knowledge, attitude and practices of medical practitioners towards dental care in rural areas of davangere taluk. International Journal of Current Research. 2014; 6(10):9275-9278.
Opeodu OI, Ogunrinde TJ, Fasunla AJ. An assessment of medical doctors' perception of possible interrelationship between oral and general health. Eur J Gen Dent. 2014;3(2):120-124
Caukeri K, Karbhari N. Dental Screening And Referral Services By Medical Officers In PHC’s Of Solapur District, Maharashtra. International Journal of Development Research 2014; 4(5):969-973.
Nagarakanti S, Epari V, Athuluru D. Knowledge, attitude, and practice of medical doctors towards periodontal disease. J Indian Soc Periodontol. 2013;17(1):137-139.
Jeffcoat MK, Geurs NC, Reddy MS, Goldenberg RL, Hauth JC. Current evidence regarding periodontal disease as a risk factor in preterm birth. Ann Periodontol. 2001;6(1):183-188.
Saini R, Saini S, Sugandha R. Periodontal disease: The sixth complication of diabetes. Journal of Family and Community Medicine. 2011;18(1):31.
20)
21)
22)
23)
24)
25)
26
27)
28)
29)
30)
31)
Original Article Perception Regarding Oral Health & Disease Among Medical Practitioners
of Durg, Chhattisgarh – A Cross Sectional Study

Volume 5, Number 3
Garcia RI, Nunn ME, Vokonas PS. Epidemiologic associations between periodontal disease and chronic obstructive pulmonary disease. Ann Periodontol 2001;6(1):71-77
Beck JD, Offenbacher S. The association between periodontal diseases and cardiovascular diseases: A state-of-the-science review. Ann Periodontol. 2001;6(1):9-15
R Morgan, J Tsang, N Harrington, L Fook. Survey of hospital doctors’ attitudes and knowledge of oral conditions in older patients. Postgrad Med J. 2001;77(908):392-394.
32)
33)
34)
Caufield PW, Cutter GR, Dasanayake AP. Initial acquisition of mutans streptococci by infants: Evidence for a discrete window of infectivity. J Dent Res. 1993;72(1):37-45
Wan AK, Seow WK, Purdie DM, Bird PS, Walsh LJ, Tudehope DI. A longitudinal study of Streptococcus mutans colonization in infants after tooth eruption. J Dent Res 2003;82(7):504-508.
35)
36)
Original Article Perception Regarding Oral Health & Disease Among Medical Practitioners
of Durg, Chhattisgarh – A Cross Sectional Study
126

Chettinad Health City Medical Journal
Think Thyroid - Think Life: Pregnancy with Thyroid DisordersReview Article
Muthukumaran Jayapaul*
Consultant Endocrinologist, Arka Center for Hormonal Health, Chennai, India
Corresponding author - Muthu Kumaran Jayapaul - ([email protected])
Chettinad Health City Medical Journal 2017; 5(3): 127 - 131
Introduction Thyroid dysfunction is one of the most common endocrine disorders encountered during pregnancy1. Overt thyroid dysfunction is prevalent in up to one percent of all pregnancies. Untreated or sub - optimal management of thyroid dysfunction can cause serious consequences both for the mother and the fetus. There is good clinical evidence, which demonstrates that treatment of overt thyroid disease negates most adverse outcomes. Subclinical thyroid dysfunction is more widely prevalent and the prevalence varies in different populations. Treatment for sub-clinical disease in pregnancy is evolving and remains a hot topic of discussion. Universal screening for thyroid dysfunction in pregnancy remains controversial. Various professional societies have reviewed the available clinical evidence and published guidelines on the management of thyroid disease in pregnancy2-4. In this clinical review we review the current evidence for screening and management of both overt and subclinical thyroid disease in pregnancy.
Physiological changes associated with pregnancyA normal pregnancy results in a number of physiological changes, to meet for the increased metabolic changes during pregnancy. The two major changes in thyroid function are the increasing thyroid binding globulin (TBG) concentrations and stimulation of the Thyroid stimulating hormone (TSH) receptor by human chorionic gonadotrophin (hCG) during the first trimester. During pregnancy, serum TBG concentra-tion increases up to twice the normal level due to increase in estrogen and decreased clearance of TBG due to sialylation5. The thyroid gland in turn has to produce more Thyroxine (T4) and Triiodothyronine (T3) to maintain satisfactory free hormone levels for both the mother and the fetus. The total T4 and T3 hormone concentrations rise during the first trimester of pregnancy and reaching steady state levels around 20 weeks. The second major change to thyroid function occurs during the first trimester of pregnancy due to the stimulatory effects of hCG on the TSH receptor.
Dr. Muthu Kumaran Jayapaul is a Consultant Endocrinologist and also the Managing Director of Arka Center for Hormonal Health Pvt Ltd, Adyar, Chennai. He has completed specialist training in the UK in Endocrinology, Diabetes and Internal medicine. His other credentials include an internationally accredited research degree MD (UK) (University of Newcastle - upon - Tyne, UK) in Diabetes and Genetics which is held only by a few endocrinologists in India. He has worked as a full-time research fellow in diabetes and genetics in the prestigious Endocrine unit based in Royal Victoria Infirmary, Newcastle-upon-Tyne. He has published papers in international and national journals. His special interests include prevention of type 2 diabetes, genetic endocrine disorders and thyroid cancer.
Abstract
Thyroid dysfunction is a common problem encountered during pregnancy in clinical practice. There is good evidence that treatment of overt thyroid dysfunction negates risk imparted to both the mother and fetus. Clinical data on the treatment of subclinical disease is evolving and remains a topic of discussion. Various societies have published guidelines on the management of thyroid disease during pregnancy. Thyroid Stimulating Hormone (TSH) remains the most reliable test during pregnancy. Interpretation of thyroid function in pregnancy depends on the accurate knowledge of the stage of pregnancy and if available trimester specific reference ranges in that particular population. The most common cause of hypothyroidism during pregnancy is chronic autoimmune thyroiditis. Overt Hypothyroidism is associated with increased risk of several complica-tions including preeclampsia, pre-term delivery, low birth weight, increased risk of caesarean section, peri-natal morbidity and mortality, postpartum hemorrhage and possible neuropsychological and cognitive impair-ment. In patients with pre - existing hypothyroidism, an increased requirement of thyroxine around 25-50 % may be needed during the first and second trimester of pregnancy. Untreated or sub - optimally managed maternal hyperthyroidism has been associated with preterm delivery, recurrent fetal loss, and low birth weight, pre-eclampsia and high risk of heart failure. Anti-thyroid medications Propylthiouraacil and Carbimazole remain the main mode of treatment. The most important factor in the management of thyroid disease in pregnancy is to consider normal physiology in pregnancy before considering treatment.
Key Words: Thyroid, Pregnancy, Hypothyroidism, Hyperthyroidism, Grave’s disease, Sub - clinical hypothyroidism, Hyperemesis gravidarum
Volume 5, Number 3
127

Review Article Think Thyroid - Think Life: Pregnancy with Thyroid Disorders
Serum HCG concentrations starts to increase soon after fertilization and peaks around 12 weeks of pregnancy. HCG belongs to a family of glycoprotein hormones and is made of 2 sub-units. It shares a common alpha sub-unit with TSH and has a unique beta-subunit. Due to this close homology with TSH, HCG exhibits a stimulatory activity over the TSH receptor causing mild hyperthyroidism between 10-12 weeks when HCG activity is at its peak. During this period, Serum total T4 and T3 concentrations increase with minor increase in free thyroid hormone levels. This is mirrored by appropriate reduction in TSH. In a small proportion of women the TSH may be low or even become undetectable. This suppression is always proportional to the HCG peak between 10 – 12 weeks gestation and is transient and physiological. The HCG starts declining at the end of first trimester, free hormones start to normalize and TSH rises back to normal by 16-20 weeks of gestation6.
Volume 5, Number 3
Fig 1 : Thyroid hormonal changes in Pregnancy Adapted from Glinoer et al. 1997 Ref:1
Physiologic Change
Serum thyroxine-binding globulin
Plasma volume
D3 expression in placenta and (?) uterus
First trimester in hCG
Renal I- clearance
T4 production; fetal T4 synthesis during second and third trimesters
Oxygen consumption by feto-placental unit, gravid uterus, and mother
Thyroid-Related Consequences
Total T4 and T3; T4 production
T4 and T3 pool size; T4 production;cardiac output
T4 production
Free T4; basal thyrotropin; T4 production
Iodine requirements
Basal metabolic rate; cardiac output
Table 1: Normal thyroid physiology and pregnancyGlinoer D, De NP, Bourdoux P et al. Regulation of maternal thyroid during pregnancy. J. Clin. Endocrinol.
Metab. 71(2), 276–287 (1990).
Normal range of TSH in PregnancyThyroid dysfunction has to be diagnosed in pregnancy by a thyroid function test due to indistinguishable symptoms of pregnancy as well as the asymptomatic nature of sub-clinical thyroid disease. The serum TSH concentration is the most reliable test during pregnancy. The American thyroid association has recommended using trimester specific reference ranges for TSH during pregnancy. If these ranges are not provided by the laboratory, the following reference ranges can be used: first trimester, 0.1 – 2.5 mIU/L; second trimester, 0.2 – 3.0 mIU/L and third trimester, 0.3 – 3.0 mIU/L2,7,8. The correct interpretation of thyroid function in pregnancy requires the accurate knowledge of the woman’s gestational age and if available the appropriate population–based reference interval.
Hypothyroidism complicating PregnancyThe most common cause of hypothyroidism during pregnancy is chronic autoimmune thyroiditis, provided iodine insufficiency is not prevalent in the population. In iodine insufficient areas, iodine deficiency can be a cause for goiter and hypothyroidism. Other rare causes are drugs including anti-thyroid medications, pituitary disorders, prior radioiodine treatment and previous thyroid surgery. Untreated or sub-optimal treatment of hypothyroidism can cause adverse effects both to the mother and fetus. Overt Hypothyroidism is associated with increased risk of several complications including preeclampsia, pre-term delivery, low birth weight, increased risk of cesarean section, peri-natal morbidity and mortality, postpartum hemorrhage and possible neuropsychological and cognitive impairment9. The prevalence of overt hypothyroidism has been estimated to 0.3 – 0.5 %10.
128

Volume 5, Number 3
Subclinical hypothyroidism is more common than overt hypothyroidism and the risk of complications are proportional to the severity of hypothyroidism. Early studies have estimated the prevalence of subclinical disease around 2.5 %, however recent estimates using the new criteria have reported prevalence as high as 27 %. Ablavich et al showed about 60% risk of fetal loss with untreated or less than optimally treated hypothyroidism11,12. Leung et al found a 22% increased risk of gestational hypertension when compared to controls 13. Overt maternal hypothyroidism is associated with neonatal neurologic developmental delay because of inadequate transfer of thyroid hormones to the fetus. The fetus is totally dependent on maternal thyroxine levels because the fetal thyroid starts to function only around 12 - 14 weeks of gestation. Untreated hypothyroidism is also associated with increased risk of fetal death. A large randomized trial over 4500 women in the first trimester of pregnancy were assigned to universal screening or case finding groups14. All patients in the universal screening group and high-risk patients in the case finding group were tested for thyroid function and ATPO antibodies in the first trimester. Patients were treated if they had positive ATPO antibodies and an increased TSH of > 2.5 mIU/l. The low-risk women in the universal screening group found to have sub-clinical hypothyroidism, TSH >2.5 and positive antibody titres, who underwent treatment had a lower risk of miscarriage, pre-eclampsia, gestational diabetes and pre-term labor. But this study failed to show any advantage of the universal screening strategy when compared to a case finding strategy 14.
Universal screening for asymptomatic pregnant women for hypothyroidism during the first trimester remains controversial. Because of insufficient evidence for universal TSH screening, most professional societies including the American Thyroid Association (ATA), The Endocrine society and the American College of Obstetricians and Gynecologists (ACOG) recommend targeted case finding than universal screening. The ATA recommends testing only if an individual has a positive family history of thyroid disease, TPO antibodies, type 1 diabetes, history of preterm delivery or miscarriage, head and neck radiation, infertility, morbid obesity, from an area of iodine insufficiency or age > 30 years. In women who fulfill the screening criteria, TSH can be measured in the first trimester and if it is greater than 2.5 mIU/L, free T4 estimation can be done to estimate the degree of hypothyroidism. In these women the risk could be further assessed by checking for anti - thyroid peroxidase (ATPO) antibodies 15,16.
Grave’s disease. Gestational thyrotoxicosis is also a frequent occurrence in the first trimester and may be present in up to 3% of all pregnancies. This is a transient phenomenon and it is important to differentiate the same from Grave’s hyperthyroidism hence unwarranted treatment may be prevented as levels spontaneously return to normal around 14 – 18 weeks gestation18,19.
Hyperthyroidism complicating PregnancyOvert Hyperthyroidism can adversely affect the mother and the fetus, depending on the severity of the disease. Untreated or sub - optimally managed maternal hyperthyroidism has been associated with preterm delivery, recurrent fetal loss, and low birth weight, pre-eclampsia and high risk of heart failure. Overt thyrotoxicosis occurs in 0.2 – 0.4 % of all pregnancies and the diagnosis is based on suppressed TSH with elevated free T4 and free T3 levels 2,3,17. The most common cause of hyperthyroidism in pregnancy is
Grave’s disease in pregnancyGrave’s disease is diagnosed when there is a history of pre-existing thyroid disease, presence of goiter, thyroid-related ophthalmopathy or the presence of TSH receptor antibody (TRAb). The goal of hyperthyroidism treatment is to maintain serum free T4 concentration in the upper normal range. The dose of anti-thyroid medications should be titrated depending on serum free T4 and TSH measurements undertaken every 4 weeks with regular clinical assessment. Once euthyroid status is achieved, the anti-thyroid drugs (ATD) dose should be titrated down actively and maintained at the lowest dose required to maintain euthyroidism. When thyroid function becomes stable less frequent monitoring, every 6 to 8 weeks is sufficient.
The most common ATDs used in pregnancy are Propylthiouracil (PTU) and Carbimazole (CBZ) to minimize adverse outcomes. However, the use of these drugs are associated with birth defects like aplasia cutis, choanal atresia or esophageal atresia in a small but significant proportion of exposed children20,21. Propylthiouracil is the preferred ATD of choice in the first trimester since placental transfer of PTU is significantly less compared to Carbimazole. However, since the concern of hepatotoxity with PTU, most professional societies have advised usage of Carbimazole in the second and third trimester of pregnancy22. The natural course of Grave’s hyperthyroidism gradually improves in late stages of pregnancy and some women will need reduction of medications in the second and third trimester. Beta-blockers may be used in patients who are troubled by severe hyper metabolic symptoms due to hyperthyroidism. It is better to stop beta-blockers after a few weeks since long-term use of Beta-blockers is associated with intrauterine growth retardation, fetal bradycardia and neonatal hypoglycemia23. Radioctive iodine therapy and functional nuclear imaging are contraindicated in pregnancy. Surgery can be rarely performed in the second trimester if euthyroid status is not possible using current medical strategies.
Neonatal ThyrotoxicosisOne percent of newborns born to women with Grave’s disease have hyperthyroidism due to trans-placental transfer of TSH receptor stimulating antibodies. High levels of maternal TRAb had been associated with fetal hyperthyroidism. A maternal TRAb test performed between 24-28 weeks of gestation is a good predictor of impending thyrotoxicosis in the neonatal period24,25. Fetal tachycardia, growth restriction, accelerated bone maturation; heart failure or hydrops are suspicious findings suggestive of fetal hyperthyroidism 26.When present at birth, most of neonatal hyperthyroidism is self - limiting. If treatment becomes necessary PTU,
Review Article Think Thyroid - Think Life: Pregnancy with Thyroid Disorders
129

Volume 5, Number 3
propranolol and prednisolone could be used. If TRAB levels are very high in the 3rd trimester, treatment of the mother with PTU enables the drug to cross through the placenta to protect fetus. Rarely the child develops his or her own TSH receptor antibody and present with hyperthyroidism around 3-6 months. Most of these infants invariably have a very strong family history of Grave’s disease and carry a risk of 20% mortality and persistent brain dysfunction.
Hyperemesis gravidarumIt is a syndrome of severe nausea and vomiting leading to at least 5% loss of body weight, dehydration, and ketosis. It occurs in around 0.1 - 0.2 percent of pregnancies. And these women have higher serum HCG and estradiol concentrations than normal pregnant women. The absence of goiter, ophthalmopathy, absence of the common symptoms and signs of hyperthyroidism and the presence of vomiting can differentiate it from Grave’s disease 27. 60% of these women have a subnormal serum TSH level (< 0.4 mU/L) and another 50% have an elevated serum free T4 concentration. Severity of the vomiting is positively correlated with maternal free T4 levels but not to thyroid function. This is most likely to be due to HCG stimulation of the thyroid gland. This does not require any active treatment but for supportive care until normalization of free T4 levels, which happens by mid-gestation19,27.
Postpartum thyroiditisPostpartum thyroiditis is a destructive thyroiditis due to autoimmune mechanism within one year of delivery. It can present as transient hyperthyroidism, transient hypothyroidism or hyperthyroidism followed by hypothyroidism18. The reported prevalence varies from 1-17 % globally but the mean prevalence rates are approximately around 7 - 8 percent. Very high prevalence is noted in patients with Type 1 Diabetes, previous post-partum thyroiditis and positive anti-thyroid peroxidase antibodies. In one particular study when patients were followed up for a period of around 8 years, one third developed permanent hypothyroidism28,29. The biochemical and clinical features are very similar to patients suffering from painless autoimmune thyroiditis. Radioiodine uptake scan may show a poor or very low uptake during the hyperthyroid phase. Nuclear imaging is a relative contraindication for breastfeeding and feeding the baby should be avoided for at least 1 week.
ConclusionKnowledge regarding maternal thyroid disease during pregnancy has increased tremendously over the last decade. Overt maternal thyroid dysfunction is associ-ated with increased risk of adverse outcomes during pregnancy and appropriate treatment abates risk. The debate continues with regards to, if treatment of sub-clinical thyroid dysfunction improves outcomes in the mother and the newborn. The current data available are mostly from observational studies with cross-sectional thyroid function testing with indecisive results. Data from prospective longitudinal randomized controlled trails are the need of the hour in the management of sub-clinical thyroid disease in pregnancy. With the current evidence available, one has to consider normal physiology and its variations during pregnancy before considering treatment.
Glinoer D. The regulation of thyroid function in pregnancy: pathways of endocrine adaptation from physiology to pathology. Endocrine reviews. 1997 Jun;18(3):404-33.
Stagnaro-Green A, Abalovich M, Alexander E, Azizi F, Mestman J, Negro R, et al. Guidelines of the American Thyroid Association for the diagnosis and management of thyroid disease during pregnancy and postpartum. Thyroid. Oct;21(10):1081-125.
Bahn RS, Burch HB, Cooper DS, Garber JR, Greenlee MC, Klein I, et al. Hyperthyroidism and other causes of thyrotoxicosis: management guidelines of the American Thyroid Association and American Association of Clinical Endocrinolo-gists. Endocr Pract. May-Jun;17(3):456-520.
Garber JR, Cobin RH, Gharib H, Hennessey JV, Klein I, Mechanick JI, et al. Clinical practice guidelines for hypothyroidism in adults: cospon-sored by the American Association of Clinical Endocrinologists and the American Thyroid Association. Thyroid. Dec;22(12):1200-35.
Ain KB, Mori Y, Refetoff S. Reduced clearance rate of thyroxine-binding globulin (TBG) with increased sialylation: a mechanism for estrogen-induced elevation of serum TBG concentration. The Journal of clinical endocrinology and metab-olism. 1987 Oct;65(4):689-96
Ballabio M, Poshychinda M, Ekins RP. Pregnancy-induced changes in thyroid function: role of human chorionic gonadotropin as putative regulator of maternal thyroid. The Journal of clinical endocr-inology and metabolism. 1991 Oct;73(4):824-31
Dashe JS, Casey BM, Wells CE, McIntire DD, Byrd EW, Leveno KJ, et al. Thyroid-stimulating hormone in singleton and twin pregnancy: importance of gestational age-specific reference ranges. Obstetrics and gynecology. 2005 Oct;106(4):753-7.
Soldin OP, Tractenberg RE, Hollowell JG, Jonklaas J, Janicic N, Soldin SJ. Trimester-specific changes in maternal thyroid hormone, thyrotropin, and thyroglobulin concentrations during gestation: trends and associations across trimesters in iodine sufficiency. Thyroid. 2004 Dec;14(12):1084-90.
Krassas GE, Poppe K, Glinoer D. Thyroid function and human reproductive health. Endocrine reviews. Oct;31(5):702-55.
Lazarus J, Brown RS, Daumerie C, Hubalewska-Dydejczyk A, Negro R, Vaidya B. 2014 European thyroid association guidelines for the management of subclinical hypothyroidism in pregnancy and inchildren. European thyroid journal. Jun;3(2):76-94.
References
1)
2)
3)
4)
5)
6)
7)
8)
9)
10)
Review Article Think Thyroid - Think Life: Pregnancy with Thyroid Disorders
130

Volume 5, Number 3
Abalovich M, Gutierrez S, Alcaraz G, Maccallini G, Garcia A, Levalle O. Overt and subclinical hypothyroidism complicating pregnancy. Thyroid. 2002 Jan;12(1):63-8.
Krassas GE, Pontikides N, Kaltsas T, Papadopoulou P, Paunkovic J, Paunkovic N, et al. Disturbances of menstruation in hypothyroidism. Clinical endocri-nology. 1999 May;50(5):655-9.
Leung AS, Millar LK, Koonings PP, Montoro M, Mestman JH. Perinatal outcome in hypothyroid pregnancies. Obstetrics and gynecology. 1993 Mar;81(3):349-53.
Negro R, Schwartz A, Gismondi R, Tinelli A, Mangieri T, Stagnaro-Green A. Universal screen-ing versus case finding for detection and treatment of thyroid hormonal dysfunction during pregnancy. The Journal of clinical endocrinology and metabolism. Apr;95(4):1699-707.
Liu H, Shan Z, Li C, Mao J, Xie X, Wang W, et al. Maternal subclinical hypothyroidism, thyroid autoimmunity, and the risk of miscarriage: a prospective cohort study. Thyroid. Nov;24(11):1642-9.
Negro R, Schwartz A, Gismondi R, Tinelli A, Mangieri T, Stagnaro-Green A. Thyroid antibody positivity in the first trimester of pregnancy is associated with negative pregnancy outcomes. The Journal of clinical endocrinology and metabolism. Jun;96(6):E920-4.
Glinoer D. Thyroid hyperfunction during pregnancy. Thyroid. 1998 Sep;8(9):859-64.
De Groot L, Abalovich M, Alexander EK, Amino N, Barbour L, Cobin RH, et al. Management of thyroid dysfunction during pregnancy and postpartum: an Endocrine Society clinical practice guideline. The Journal of clinical endocrinology and metabolism. Aug;97(8):2543-65.
Goodwin TM, Montoro M, Mestman JH. Transient hyperthyroidism and hyperemesis gravidarum: clinical aspects. American journal of obstetrics and gynecology. 1992 Sep;167(3):648-52.
Andersen SL, Olsen J, Laurberg P. Antithyroid Drug Side Effects in the Population and in Pregnancy. The Journal of clinical endocrinology and metabolism. Apr;101(4):1606-14.
11)
12)
13)
14)
15)
16)
17)
18)
19)
20)
Andersen SL, Olsen J, Wu CS, Laurberg P. Birth defects after early pregnancy use of antithyroid drugs: a Danish nationwide study. The Journal of clinical endocrinology and metabolism. Nov;98(11):4373-81.
Bahn RS, Burch HS, Cooper DS, Garber JR, Greenlee CM, Klein IL, et al. The Role of Propylthiouracil in the Management of Graves' Disease in Adults: report of a meeting jointly sponsored by the American Thyroid Association and the Food and Drug Administration. Thyroid. 2009 Jul;19(7):673-4.
Lydakis C, Lip GY, Beevers M, Beevers DG. Atenolol and fetal growth in pregnancies compli-cated by hypertension. American journal of hypertension. 1999 Jun;12(6):541-7.
Zimmerman D. Fetal and neonatal hyperthyroid-ism. Thyroid. 1999 Jul;9(7):727-33.
Peleg D, Cada S, Peleg A, Ben-Ami M. The relationship between maternal serum thyroid-stimulating immunoglobulin and fetal and neonatal thyrotoxicosis. Obstetrics and gynecology. 2002 Jun;99(6):1040-3
Luton D, Le Gac I, Vuillard E, Castanet M, Guibourdenche J, Noel M, et al. Management of Graves' disease during pregnancy: the key role of fetal thyroid gland monitoring. The Journal of clinical endocrinology and metabolism. 2005 Nov;90(11):6093-8.
Tan JY, Loh KC, Yeo GS, Chee YC. Transient hyperthyroidism of hyperemesis gravidarum. Bjog. 2002 Jun;109(6):683-8.
Nicholson WK, Robinson KA, Smallridge RC, Ladenson PW, Powe NR. Prevalence of postpar-tum thyroid dysfunction: a quantitative review. Thyroid. 2006 Jun;16(6):573-82.
Stagnaro-Green A, Schwartz A, Gismondi R, Tinelli A, Mangieri T, Negro R. High rate of persistent hypothyroidism in a large-scale prospec-tive study of postpartum thyroiditis in southern Italy. The Journal of clinical endocrinology and metabolism. Mar;96(3):652-7.
21)
22)
23)
24)
25)
26)
27)
28)
29)
Review Article Think Thyroid - Think Life: Pregnancy with Thyroid Disorders
131

Chettinad Health City Medical Journal
Mitral Stenosis and Pregnancy - Perioperative ConsiderationsReview Article
Lailu Mathews*
*Professor and Head, Department of Anesthesiology, Chettinad Hospital & Research Institute, Chennai, India.
Corresponding author - Lailu Mathews - ([email protected])
Chettinad Health City Medical Journal 2017; 5(3): 132 - 136
Introduction Cardiovascular disease in pregnancy has been estimated to be 0.1-4.1%1. The common cardiac diseases during pregnancy ranges from congenital and acquired cardiac defects to peripartum cardiomyopathy. Valvular heart disease is the commonest cardiac condition in young women planning pregnancy. Cardiac disease is an important non obstetric cause of maternal mortality2. Although most women are aware of their diagnosis prior to pregnancy, symptoms manifest for the first time during pregnancy. Though pregnancy is tolerated well in patients with mild valvular disease, pregnancy is not advisable in those with severe mitral stenosis (MS), severe symptomatic aortic stenosis(AS) and valve lesions associated with severe left ventricular (LV) dysfunction or significant pulmonary hypertension3. Pre conception counseling and if indicated, valve intervention should be recommended when planning for pregnancy3,4. Cardiac disease associated with pregnancy represents a unique challenge to the anesthesiologist. All patients with significant cardiac disease have to be jointly managed by the cardiologist, obstetrician and anesthesiologist.
Rheumatic heart disease is still the most common cardiac illness, especially in a developing country like India where it constitutes 80% of the cardiac diseases during pregnancy5. In the developed nations, rheumatic heart disease is less common and complex congenital heart diseases have increased recently. This review article focuses on the peri operative considerations in pregnant patients with mitral stenosis.
Pregnancy risk assessmentRisk assessment of pregnancy is very important in a pregnant woman with heart disease6. Pre conception counseling previewing the risk of pregnancy for both mother and fetus, long term outcome of pregnancy on the heart, maternal life expectancy, genetic consultation, contraception safety and efficacy, modification of cardiac medications and optimization of cardiac status should be clearly explained. The risk assessment indices that are widely in practice are CARPREG ( Cardiac disease in Pregnancy), BACH (Boston Adult Congenital Heart), ZAHARA ( Zwangerschap bij vrouven met een Aangeboren HARtAfwijking- II (interpreted as “Pregnancy in women with CHD II risk index”), modified World Health Organization (WHO) classification7. The modified WHO risk classification is a reliable system for risk prediction according to many studies8. The modified WHO classification divides cardiac lesions as low risk (WHO I), medium risk (WHO II), high risk (WHO III) and lesions in which pregnancy is contraindicated (WHO IV) 9.
General considerations in pregnant patients with cardiac diseasePregnancy is accompanied by physiological variations in the cardiovascular system. Four principal cardiovascular variations normally occurring during pregnancy that can have significant anesthetic implications10 :
Prof. Lailu Mathews completed her graduation and post graduation from Christian Medical College, Ludhiana in the year 1994.She has worked in prestigious institutions like Institute of Cardiovascular Diseases- Madras Medical Mission, College of Oncological Sciences, Chennai and Pondichery Institute of Medical Sciences. She has many publications to her credit. She is a peer reviewer for the esteemed journal Annals of Cardiac Anaesthesia. Her areas of interest are paediatric anaesthesia and thoracic anaesthesia. At present she is the Professor and Head of the Department of Anaesthesiology & Critical Care at Chettinad Hospital & Research Institute.
Abstract
Cardiovascular disease in pregnancy has been estimated to be 0.1-4.1%. The incidence of pregnancies in women with cardiac disease is on the rise due to an increase in the number of women with heart disease reaching childbearing age as a result of the developments in the management of cardiovascular diseases and advances in reproductive medicine, advancing maternal age with associated diabetes mellitus, hypertension, pre eclampsia and multiple fetal pregnancies. Cardiac disease has thus evolved as an important cause of non obstetric maternal mortality. Rheumatic mitral stenosis is one of the most common cardiac illnesses complicating pregnancy. Patients with severe mitral stenosis usually do not withstand the cardiovascular demands of pregnancy. Therefore, a multidisciplinary approach is required to reduce the morbidity and mortality during the antenatal and postnatal period. The role of anesthesiologist and perioperative considerations in such patients leading to prevention of complications with successful outcome of the mother and fetus are discussed.
Key Words: Mitral stenosis, pregnancy, caesarean section
Volume 5, Number 3
132

Review Article Mitral Stenosis and Pregnancy - Perioperative Considerations Volume 5, Number 3
progression of stenosis, left atrium dilates and left atrial pressure increases leading to a pressure gradient between the left atrium and left ventricle during diastole. The back pressure on the pulmonary vessels leads to pulmonary congestion with symptoms like dyspnea and hemoptysis, and in severe cases pulmonary edema. The symptoms may present for the first time during pregnancy due to hemodynamic changes accompanying pregnancy. Reduction in functional capacity, arrhythmias like atrial fibrillation and pulmonary edema are the most common cardiac complications13-15. Complications are related to the severity of MS and baseline New York Heart Association (NYHA) functional class 13,14.
The cardiovascular changes are ordinarily well tolerated in a healthy young parturient but in patients with cardiac disease these variations place the myocardium under stress. In general, regurgitant lesions are well tolerated in pregnancy because the increased plasma volume and low systemic vascular resistance results in elevated cardiac output whereas stenotic lesions are poorly tolerated with advancing pregnancy due to the incomplete left ventricular filling and consequent inability to increase the cardiac output.
Risk factors for perinatal complications are poor maternal functional class, left heart obstruction, maternal age <20 or >35 years, multiple gestation, smoking during pregnancy and anticoagulant therapy, which are further escalated in women with concomitant obstetric risk factors11.
Mitral StenosisMitral stenosis(MS) is the most common valve lesion in women of childbearing age. Rheumatic MS forms 88% of the heart diseases complicating pregnancy in the tertiary referral centers in India 5. It accounts for nearly 90% of rheumatic heart disease in pregnancy, with 25% of patients first experiencing symptoms only during pregnancy12. An anatomically moderate lesion may become functionally severe with the distinct increase in cardiac output that is associated with pregnancy, labor and delivery. Other valve lesions like mitral regurgitation(MR), aortic stenosis (AS) and aortic regurgitation(AR)are also associated with rheumatic fever but less frequently.
Mitral stenosis may present as an isolated lesion or along with right sided or aortic valve disease. Women with mitral stenosis often do not tolerate the cardiovascular demands of pregnancy. Heart rate, cardiac output, red cell mass and plasma volume which are normally increased during pregnancy are not tolerated by patients with MS, according to the severity of the stenosis, leading to increased left atrial pressure and cardiac decompensation.
PathophysiologyNormal mitral valve orifice has a surface area of 4 to 6 cm2. Patients become symptomatic when the area is 2 cm2 or less. MS prevents emptying of left atrium (LA)
There is a 50% rise in intravascular volume that peaks by third trimester. This relative volume overload is not tolerated in patients with low cardiac output due to any cause.
Systemic vascular resistance decreases progressively during pregnancy, so that normal mean arterial pressure is maintained despite 30 to 40% rise in cardiac output.
Significant changes in cardiac output happens during labor and immediately following delivery.
Hypercoagulability associated with pregnancy and the indication for anticoagulant therapy in patients prone to arterial thrombosis and embolization (chronic atrial fibrillation and prosthetic heart valves).
1)
2)
3)
4)
Atrial arrhythmias and heart failure often occur in the third trimester when the hemodynamic changes of pregnancy are at its peak. Complications can also occur at the time of labor and delivery or within the first week post partum13. Patients with atrial fibrillation(AF) are at risk for cerebrovascular accident and transient ischemic events. The sudden increase in preload immediately after delivery due to auto transfusion from the uterus may flood the central circulation resulting in severe pulmonary edema. Auto transfusion continues for 24 to 72 hours after delivery. Thus the risk of pulmonary edema is extended into the postpartum period16.
Maternal outcome correlates well with NYHA functional classification and severity of the stenosis - severe (67%), moderate (38%), mild (26%) 17,18. Mortality rates for NYHA Class I and II were < 1% whereas for NYHA Class III and IV the mortality rates were 5 to 15%. A system for foreseeing complications during pregnancy was developed by Siu et al based on NYHA classification as follows19:
ManagementManagement of the parturient with mitral stenosis requires multidisciplinary approach by the obstetrician, cardiologist, anesthesiologist and neonatologist for optimal maternal and fetal outcome. Cardiac decompensation should be Management of the parturient with mitral stenosis requires multidisciplinary approach by the obstetrician, cardiologist, anesthesiologist and neonatologist for optimal maternal and fetal outcome. Cardiac decompensation should be avoided during the antenatal period with regular check-up for volume overload and pulmonary edema. In symptomatic patients, medical management includes bed rest, oxygen therapy, diuretics and beta blockers20. Beta blockers prolong the diastolic filling time and reduce left atrial pressure21. Recent trials infer that Digoxin has no role in the treatment of cardiac failure22.
History of heart failure, arrhythmia, transient ischemic attack or stroke
Baseline NHYA class III or more or cyanosis
Systemic ventricular dysfunction (Ejection fraction <40%)
Pulmonary hypertension
Left heart obstruction – severe aortic stenosis or symptomatic /severe mitral stenosis
Severe aortic or mitral regurgitation with NYHA Class II or IV symptoms.
1)
2)
3)
4)
5)
6)
133

134
Volume 5, Number 3
AF demands aggressive treatment with Digoxin and beta blockers to revert it to sinus rhythm and anticoagulants to prevent systemic embolization. Cardioversion is indicated if pharmacologic therapy fails to control the ventricular response. Anticoagulants even in the absence of AF is useful 23,24. Women who are refractory to medical therapy, mitral balloon valvuloplasty may be considered. Mitral valve surgery should be considered in patients who are not candidates for balloon valvuloplasty. Major concern regarding cardiopulmonary bypass during pregnancy is fetal mortality; therefore valve surgery is considered only if other therapies have failed because it carries a significantly high fetal mortality risk of 20 to 30%13,25,26. For women who remain stable throughout pregnancy, vaginal delivery with adequate pain relief is the preferable mode of delivery3. Analgesia during the first stage of labor is focused on reducing the pain related increase in catecholamine levels and preventing aortocaval compression. Analgesia for labor and vaginal delivery is best accomplished with lumbar segmental epidural analgesia to prevent fluctuations in hemodynamic parameters. Segmental epidural analgesia allows for careful titration of drug to the desired level of analgesia while minimizing undesirable hemodynamic changes. An opioid like fentanyl added to the dilute local anesthetic mixture enhances the quality of analgesia without causing sympathetic blockade. During second stage of labor, only the uterine contraction force is permissible rather than the maternal expulsive effort that is associated with Valsalva maneuver. Hence the second stage of labor should be shortened by instrumentation22. Epidural analgesia with low concentration of Bupivacaine and Fentanyl reduces systemic vascular resistance and preload27. Caesarean section is indicated for obstetric reasons only.
Anesthetic considerations in operative deliveryAnesthetic options for caesarean delivery must take account of the additional potential hazards of marked fluid shifts secondary to anesthesia technique, operative blood loss and mobilization of blood in the post partum period. In a study by Goldszmidt and others, only 29-31% of the 522 women with heart disease required caesarean section and nearly 70% of them underwent vaginal delivery under epiduralanalgesia28. A safe anesthetic technique is graded epidural anesthesia whereby the anesthesiologist can titrate the dose of local anesthetic and prevent the occurrence of hemodynamic instability and its consequences. Epidural anesthesia is preferred over spinal anesthesia because of the slower onset of blockade and better controllable hemodynamics29. Prophylactic ephedrine administration as a prophylactic measure for hypotension must be avoided 30. If a vasopressor is indicated, the drug of choice is low dose phenylephrine.
The most basic principles of obstetric anesthetic management are 31
Hence the goals of anesthetic management in patients with MS are 22
Standard of care monitoring of parturient and fetus Provision of aspiration prophylaxis.
3)
4)
Maintenance of acceptable low heart rate as the time required for left ventricular filling is prolonged in MS.
Immediate treatment of AF and reversion to sinus rhythm
Avoidance of aortocaval compression
Maintenance of adequate venous return and systemic vascular resistance
Prevention of pain, hypoxemia, hypercarbia and acidosis which increases pulmonary vascular resistance.
1)
2)
3)
4)
5)
Patients who are asymptomatic at term generally require increased vigilance but do not require invasive hemodynamic monitoring. Symptomatic patients are at risk in the peripartum period and invasive hemodynamic monitoring is indicated 32.
General anesthesia (GA) provides stable hemodynamics if cardiovascular effects that accompany laryngoscopy and intubation as well as with suction and extubation are curtailed. Anesthetic induction agent should not produce wide fluctuations in hemodynamics. Etomidate is an ideal choice. A beta blocker like Esmolol and an opioid like Fentanyl should be administered before or during induction of GA. Methyl ergometrine should be avoided as it may produce hypertension, tachycardia and increased pulmonary vascular resistance33. Oxytocin should be used cautiously as it can lower the SVR and elevate PVR resulting in a drop in cardiac output32.
Modified rapid sequence induction (RSI) using etomidate, remifentanil and succinyl choline is an ideal choice in patients with severe MS with pulmonary hypertension. Maintenance of anesthesia may be with oxygen, air, isoflurane, opioids and vecuronium22.Emergence must be carefully controlled to ensure return of protective reflexes and avoidance of tachycardia29. An increase in central circulatory blood volume may occur suddenly in the immediate post partum period and this intravascular load is poorly tolerated in patients with fixed cardiac output 34.
Tailoring the anesthetic management according to the patient’s cardiovascular status and practitioner’s knowledge and experience of the existing treatment options leads to a successful outcome in these patients27. Post operatively, the patient should be managed in a High dependent unit (HDU) or Intensive care unit (ICU) for monitoring of fluid therapy, oxygen saturation and hemodynamics. During the first 24 to 72 hours significant fluid shift occurs, which may lead to congestive cardiac failure (CCF). Effective post operative analgesia may be provided by continuous epidural analgesia or patient controlled analgesia (PCA). Early ambulation to minimize the risk of deep vein thrombosis and paradoxical embolism should be weighed against the risk of cardiovascular stress.
Provision for maintenance of uteroplacental circulation by avoidance of aortocaval compression Sympathetic blockade should be minimized and intra operative volume to be maintained.
1)
2)
Review Article Mitral Stenosis and Pregnancy - Perioperative Considerations

135
Volume 5, Number 3
Shaikh SI, Lakshmi RR, Hegade G. Perioperative anesthetic management for cesarean section in patients with cardiac disease. Anaesth Pain & Inten-sive Care. 2014;18(4):377-85.
Elakayam U, Goland S, Pieper PG, Silverside CK. High risk cardiac disease in pregnancy: Part 1. J Am Coll Cardiol. 2016; 68(4); 396-410.
Regitz-Zagrosek V, Blomstrom Lundqvist C, Borghi C, Cifkova R, Ferreira R, Foidart JM, et al. ESC guidelines on the management of cardiovascular diseases during pregnancy. Eur Heart J 2011;32(24):3147–97.
Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP 3rd, Guyton RA, et al. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63(22): 2438-88.
Bhatla N, Lal S, Behera G, Kriplani A, Mittal S, Agarwal N, et al. Cardiac disease in pregnancy. Int J Gynaecol Obstet. 2003; 82(2): 153-9
Kovacs AH, Harrison JL, Colman JM, Sermer M, Siu SC, Silversides CK. Pregnancy and contraception in congenital heart disease: What women are not told. J Am Coll Cardiol. 2008; 52(7): 577-8.
Drenthen W, Boersma E, Balci A, Moons P, Roos-Hesselink JW, Mulder BJ et al. Predictors of pregnancy complications in women with congenital heart disease. Eur Heart J. 2010;31 (17):2124–32
Balci A, Sollie-Szarynska KM, van der Bijl AG, Ruys TP, Mulder BJ, Roos-Hesselink JW, et al. Prospec-tive validation and assessment of cardiovascular and offspring risk models for pregnant women with congenital heart disease. Heart. 2014;100(17):1373–81.
Thorne S, Nelson-Piercy C, MacGregor A, Gibbs S, Crowhurst J, Panay N, et al. Pregnancy and contra-ception in heart disease and pulmonary arterial hypertension. J Fam Plann Reprod Health Care .2006;32(2):75–81.
References
1)
2)
3)
4)
5)
6)
7)
8)
9)
ConclusionRheumatic mitral stenosis continues to be the most common cardiac disease complicating pregnancy. A thorough understanding of the physiological changes in pregnancy and the pathological impact of mitral stenosis on pregnancy is mandatory. A multidisciplinary approach and anesthetic planning in order to optimize cardiac function during the peripartum period considerably reduces the mortality and morbidity. The mode of delivery and anesthetic technique could be tailored as per the patient’s cardiac condition resulting in successful outcome of the mother and fetus.
Clark SL. Cardiac disease in pregnancy. Obstet Gynecol Clin North Am. 1991;18(2): 237-56.
Siu SC, Colman JM, Sorensen S, Smallhorn JF, Farine D, Amankwah KS, et al. Adverse neonatal and cardiac outcomes are more common in pregnant women with cardiac disease. Circulation 2002;105(18):2179–84.
Sugrue D, Blake S, MacDonald D. Pregnancy complicated by maternal heart disease at the National Maternity Hospital, Dublin, Ireland: 1969 to 1978. Am J Obstet Gynecol .1981; 139(1): 1-6.
Silversides CK, Colman JM, Sermer M, Siu SC. Cardiac risk in pregnant women with rheumatic mitral stenosis. Am J Cardiol .2003;91(11):1382–5.
Hameed A, Karaalp IS, Tummala PP, Wani OR, Canetti M, Akhter MW, et al. The effect of valvular heart disease on maternal and fetal outcome of pregnancy. J Am Coll Cardiol. 2001;37(3):893–9.
Le_sniak-Sobelga A, Tracz W, KostKiewicz M, Podolec P, Pasowicz M. Clinical and echocardio-graphic assessment of pregnant women with valvu-lar heart diseases— maternal and fetal outcome. Int J Cardiol. 2004; 94(1):15–23.
Warnes CA. Pregnancy and heart disease. In: Libby P, Bonow RO, Mann DL, Zipes DP, editors. Braunwald’s Heart Disease: A Text book of Cardio-vascular Medicine. 8th ed. Philadelphia PA: WB Saunders; 2007.pp. 1967-82.
Sawhney H, Aggarwal N, Suri V, vasishta K, Sharma Y, Grover A. Pregnancy outcomes in women with heart disease. Int J Gynaecol Obstet. 2003; 80(1):9-14.
Silversides CK, Colman JM, Sermer M, Siu SC. Cardiac risk in pregnant women with rheumatic mitral stenosis. Am J Cardiol. 2003;91(11):1382-5.
Siu SC, Sermer M, Harrison DA, Grigoriodis E, Liu G, Sorensen S, et al. Risk and predictors for pregnancy-related complications in women with heart disease. Circulation. 1997;96(9):2789-94.
Al Kasab SM, Sabag T, al Zaibag M, Awaad M, al Bitar I, Halim MA, et al. Beta- adrenergic blockade in the management of pregnant women with mitral stenosis. Am J Obstet gynecol. 1990;165(1):37-40.
Chohan U, Afshan G, Monem A. Anesthesia for caesarean section in patients with cardiac disease. J Pak Med Assoc. 2006;56(1):32-38.
Kannan M, Vijayanand G. Mitral stenosis and pregnancy: Current concepts in anaesthetic practice. Indian J Anaesth. 2010;54(5):439-44.
Reimold SC, Rutherford JD. Valvular heart disease in pregnancy. N Engl J Med. 2003; 349(1):52-9.
Hameed A, Akhter MW, Bitar F, Khan SA, Sarma R, Goodwin TM, et al. Left atrial thrombosis in pregnant women ith mitral stenosis and sinus rhythm. Am J Obstet gynecol.2005;193(2):501-4.
10)
11)
12)
13)
14)
15)
16)
17)
18)
19)
20)
21)
22)
23)
24)
Review Article Mitral Stenosis and Pregnancy - Perioperative Considerations

136
Volume 5, Number 3
Weiss BM, von Segesser LK, Alon E, Seifert B, Turina MI. Outcome of cardiovascular surgery and pregnancy: a systematic review of the period 1984–1996. Am J Obstet Gynecol. 1998;179(6 Pt 1):1643–53.
Parry AJ, Westaby S. Cardiopulmonary bypass during pregnancy. Ann Thorac Surg 1996;61(6): 1865–9.
Ngan Kee WD, Shen J, chiu AT, Lok I, Khaw KS. Combined spinal-epidural analgesia in the management of laboring parturients with mitral stenosis. Anesth Intensive Care. 1999;27(5):523-6.
E. Goldszmidt a, A. Macarthur a, C. Silversides b, J. Colman b, M. Sermer c, S. Siu d. Anesthetic management of a consecutive cohort of women with heart disease for labor and delivery. Interna-tional Journal of Obstetric Anesthesia. 2010; 19(3): 266-72
Kuczkowski KM. Anesthesia for the parturient with cardiovascular disease. South Afr J Anaesth Analg.2003 9(2), 18-25.
25)
26)
27)
28)
29)
Ziskind S, Etchin A, Frenkel Y, Mashiach S, Lusky A, Goor DA, et al. Epidural anesthesia with the trendelenberg position for cesarean section with or without a cardiac surgical procedure in patients with severe mitral stenosis: A hemodynamic study. J Cardiothorac anesth 1990; 4(3): 354-9.
Malinow AM, Ostheimer GW. Anesthesia for the high-risk parturient. Obstet gynecol 1987; 69(6):951-64.
Clark SL, Phelan JP, Greenspoon J, Aldahl D, Horenstein J. Labor and delivery in the presence of mitral stenosis: central hemodynamic observa-tions. Am J Obstet Gynecol 1985; 152(8): 984-8.
Secher NJ, Arnsbo P, Wallin L. Hemodynamic effects of oxytocin(syntocinon) and methyl ergometrine(methergin) on the systemic and pulmonary circulations of pregnant anaesthetized women. Acta Obstet Gynecol Scand. 1978; 57(2):97-103.
Ducey JP, Ellsworth SM. The hemodynamic effects of severe mitral stenosis and pulmonary hyperten-sion during labor and delivery. Intensive Care Med. 1989; 15(3): 192-5.
30)
31)
32)
33)
34)
Review Article Mitral Stenosis and Pregnancy - Perioperative Considerations
Diagnose the condition
A 66 year old gentleman with vague chest discomfort and occasional palpitation. His ECG is shown below
Dr. M.Chokkalingam, Consultant Cardiologist, CSSH. Answer in page : 163

Chettinad Health City Medical Journal
“ The Balloon of Hope” - Successful Management of Tight MitralStenosis with Balloon Mitral Valvuloplasty In An Antenatal Woman
Case Report
Sindhura M*, Famida A M**, Vijayalakshmi K**, Pradeep Nayar***
Postgraduate 1st yr*, Professor**, Department of Obstetrics and Gynecology, Professor & HOD***, Department of Cardiology,
Chettinad Hospital & Research Institute, Chennai , India.
Corresponding author - M. Sindhura - ([email protected])
Chettinad Health City Medical Journal 2017; 5(3): 137 - 139
Introduction Rheumatic valvular disease is one of the major cardiac problems complicating pregnancy in India. In a survey conducted in 1995 the incidence of rheumatic mitral stenosis was 5.4 per 1,000 school children.1This problem has been reduced to 0.5–0.64 per 1,000 in another survey conducted in 2002.2 As per a study done at a tertiary centre, rheumatic mitral stenosis accounts for 88% of the heart diseases complicating pregnancy.3
Cardiovascular disease complicating pregnancy has an overall incidence of 1-3%.It causes 10-15% of maternal mortality. Mitral stenosis is the most common valvular lesion in women of reproductive age group. As per Indian statistics from studies conducted in 2005, in rural areas, rheumatic heart disease had a prevalence rate of was 4.8/1000. In urban areas it was found to be much less and the rate was 1.98/1000. 4
Mitral stenosis is often associated with mitral regurgitation, but maternal morbidity is mostly seen with mitral stenosis. There is a significant reduction in mortality and morbidity by application of cardiac interventional procedures, multidisciplinary approach and better perinatal care. 5
Case ReportMrs. A, 26 years old G2A1 with mitral stenosis who had undergone Open mitral valvotomy at 14 years of age in 2004. Her Menstrual history reveals regular cycles 3/30 days. Her Last Menstrual Period was on 17/5/15 and her Expected date of delivery was on 24/2/16. She was admitted at 15 weeks gestation for evaluation. 2D-Echo evaluation after admission showed Mitral valve orifice of 0.9 cm2 (severe mitral stenosis) and an Ejection Fraction of 62%. As she was in her early second trimester she was counseled and planned for
Percutaneous balloon mitral valvuloplasty at 20 weeks of gestation and discharged. She was readmitted at 19 weeks with complaints of class III Dyspnoea.
On ExaminationShe was moderately built and nourished. Height - 150 cms. Weight - 62 kgs. No pallor, no icterus, no cyanosis, no clubbing, no pedal edema. Heart rate: 88bpm. Pulse - Regular, Normal in volume and character. Blood Pressure was 90/60mmHg. Cardiovascular system examination showed normal S1,S2 and a Grade 3/5 mid-diastolic murmur heard in the mitral area. Respiratory system examination was normal. P/A: uterus was 20 weeks size and Fetal heart rate was good.
Investigations: All lab parameters were within
normal limits.
2D ECHO: Rheumatic heart disease - Severe residual mitral stenosis, Mitral Valve Orifice Area - 0.9cm2, mild mitral regurgitation, Grade 3 t ricuspid regurgitation with mild pulmonary artery hypertension, left atrium dilated, left ventricular systolic function - normal and Ejection Fraction was 62%.
TreatmentShe was stabilized with beta blockers (T.Metoprolol - 12.5 mg BID). An anomaly scan was done and showed no anomalies. She was taken up for elective Balloon Mitral Valvuloplasty(Figure 1).The procedure was done at 20 weeks gestational age on 30/9/15. The procedure was uneventful and the patient was shifted to cardiac Intensive Care Unit in a hemodynamically
Dr. M.Sindhura is an undergraduate from Dr.Pinnamaneni Institute of Medical Sciences and Research Foundation, Chinoutpally, Andhra Pradesh. She is presently doing her Postgraduation in the Department of Obstetrics and Gynecology in Chettinad Hospital & Research Institute,Chennai.
Abstract
Mitral Stenosis is one of the most common manifestation of rheumatic heart disease. In pregnant women it is the most commonly seen acquired valvular lesion. It is also one of the common causes of maternal death from cardiac diseases world over. Mortality remains low in women from developed countries but there is a rise in rate of fetal morbidity as the severity of mitral stenosis worsens. Presenting a case of pregnant woman with severe mitral stenosis, successfully managed with balloon mitral valvuloplasty at mid trimester of pregnancy.
Key Words: Mitral stenosis, Balloon, Mitral valvuloplasty.
Volume 5, Number 3
137

Case Report “ The Balloon of Hope” - Successful Management of Tight Mitral Stenosis with Balloon Mitral Valvuloplasty In An Antenatal Woman
stable condition. She recovered well and was discharged with T. Propranolol 10mg BID. and T.Furosemide 20mg OD after a week stay.
Her Post procedure echo showed mild residual mitral stenosis and mitral orifice area was 1.7cm2, with mild mitral regurgitation.
Volume 5, Number 3
Fig 1 : BMV fluroscopic image of trans mitralplacement of catheter
FollowupPatient was on regular antenatal care. At every visit she was reviewed by both obstetrician and cardiologist.At 37 weeks she was admitted and antepartum fetal surveillance done. At 38 weeks she was taken up for Elective LSCS in view of Cephalopelvic disproportion, under Infective Endocarditis cover. She delivered a live boy baby of weight 3.380kgs, with APGAR 8/10, 9/10. Post operative period was uneventful. Suture removal was done on post operative day 10 and patient discharged.
DiscussionMitral stenosis (Fig 2) is a condition in which there is a fixed cardiac output caused by left atrial outflow obstruction leading to increase in the pressure of left atrium and pulmonary vasculature.6 The severity is graded as shown in Table 1.
Fig 2 : Schematic diagram showing Mitral stenosis
Measurement
MVArea(cm2)
MPG(mmHg)
PA Pr (mm Hg)
Normal
4.0 -6.0
<2
10 -20
Mild
1.5 -2.5
2 - 6
<30
Moderate
1.0 -1.5
6 -12
30 - 50
Severe
<1.0
>12
>50
Table 1 : Grading of Mitral Stenosis 7
Hemodynamic Parameter
Blood Volume
Cardiac output
Stroke volume
Heart rate Intravascular volume
Systemic vascular resistance
Blood Pressure
Oxygen consumption
Change during normal pregnancy
Increases by 40 - 50%
Increases by 30 - 50% above the baseline
Increases by 30%
Increases by 10 - 15 beats per minute Increases by 45%
Decreases by 20%
Decreases by 10mm Hg
Increases by 30 - 40%
Table 2: Cardiovascular Changes In Pregnancy 8
138

Volume 5, Number 3Case Report “ The Balloon of Hope” - Successful Management of Tight Mitral Stenosis with Balloon Mitral Valvuloplasty In An Antenatal Woman
Effect of Mitral Stenosis on PregnancyMother can have Pulmonary oedema or atrial fibrillation while fetus shows Intrauterine fetal growth restriction and Preterm birth.9
Effect of Pregnancy on Mitral StenosisPregnancy brings about the various hemodynamic changes (Table 2), so that asymptomatic patients may develop symptoms or complications.10 In Pregnant women with mitral stenosis there is an increase in maternal morbidity and adverse fetal outcome if they are not tackled.
Prepregnancy CounsellingPre pregnancy counseling should be started from adolescence.It should provide the information about all the risks of pregnancy which affect their health and of their fetus.It gives an opportunity for the assessment of the woman’s cardiac condition and review of current medications.Contraceptive advice should be given regarding the risks of thrombosis or infection associated with various contraceptive methods.11 Barrier methods are safe in all cardiac patients and have added the benefit of protection against the sexuall transmitted infections.
Criteria for Percutaneous Mitral ValvuloplastyPatient should have moderate to severe Mitral stenosis with no calcified leaflets of the valves and no significant regurgitation or arrthymias.12 Advantages of BMV include percutaneous approach under local anaesthesia with good hemodynamic results in selected patients.
Disadvantages: Preterm uterine contractions (increased risk for abortion), Maternal arrhythmias leading to fetal distress, Ionizing radiation exposure to the fetus, Cardiac tamponade requiring surgical intervention.
Newer Advances in BmvTransthoracic esophageal echo [TTE] is used with fluroscopy to guide BMV. It is an useful adjunct to fluroscopy in trans - septal puncture. It helps in visualization of valve anatomy, determination of transvalvular gradients and MVA , detection of MR and allows early detection of c omplications. Transesophageal echo [TEE] is superior to TTE in excluding left atrial thrombi and in monitoring wire and balloon positioning.
ConclusionBalloon mitral valvuloplasty in mid trimester of pregnancy is a relatively safe and effective interventional cardiac procedure which gives optimum results.13 It helps the patients with moderate to severe mitral stenosis and overcomes the risks associated with the diseased valve.14 Improvements in the procedure by the use of TEE has reduced the radiation exposure for the fetus.
Padmavati S. Present status of rheumatic fever and rheumatic heart disease in India. Indian Heart J.1995;47(4):395-8.
References
1)
Misra M, Mittal M, Singh R, Verma A, Rai R, Chandra G, et al. Prevalence of rheumatic heart disease in school-going children of Eastern Uttar Pradesh. Indian Heart J 2007;59:42-3.
Bhatla N, Lal S, Behera G, Kriplani A, Mittal S, Agarwal N, et al. Cardiac disease in pregnancy. Int J Gynaecol Obstet 2003;82(2):153-9.
Malhotra M, Sharma JB, Tripathii R, Arora P, Arora R. Maternal and fetal outcome in valvular heart disease. Int J Gynaecol Obstet 2004 Jan;84(1):11-6.
Elkayam U, Bitar F. Valvular heart disease and pregnancy. J Am Coll Cardiol. 2005;46(2):223-30.
Fligner CL, Reichenbach DD. Pathology and etiology of heart disease. In:Otto CM,ed. Valvular Heart Disease. Philadelphia, PA: WB Saunders; 1999: 13 - 42.
American College of Cardiology/American Heart Association Task Force on Practice Guidelines; Society of Cardiovascular Anesthesiologists; Society for Cardiovascular Angiography and Interventions. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines(writing Committee to Revise the 1998 Guidelines for the Management of patients with Valvular Heart Disease): developed in collaboration with the society of Cardiovascular Anesthesiologists:endorsed by the Society for Cardiovascular Angiography and Interventions and the Society of Thoracic Surgeons. Circulation.2006;114(5):e84-e231.
Karamermer Y, Roos Hesselink JW. Pregnancy and adult congenital heart disease. Expert Rev Cardiovasc Ther.2007;5(5):859-69.
Siu SC, Sermer M, Harrison DA, Grigoriadis E, Liu G, Sorensen S, et al. Risk and predictors for pregnancy-related complications in women with heart disease. Circulation 1997;96(9):2789-94.
Silversides CK, Colman JM, Sermer M, Siu SC. Cardiac risk in pregnant women with rheumatic mitral stenosis. Am J Cardiol 2003;91(11):1382-5.
Thorne S, Mac Gregor A, Nelson-piercy C. Risks of contraception and pregnancy in heart disease. Heart.2006;92(10):1520-25.
Nobuyoshi M, Arita T, Shirai S. Percutaneous balloon mitral valvuloplasy: a review. Circulation.1998;97(3):e211-e219.
Fawzy ME, Kinsara AJ, Stefadouros M, Hegazy H, Kattan H, Chaudhary A, et al. Long-term outcome of mitral balloon valvotomy in pregnant women. J Heart Valve Dis. 2001;10(2):153-7.
De Souza JA, Martinez EE Jr, Ambrose JA, Alves CM, Born D, Buffolo E, et al. Percutaneous balloon mitral valvuloplasty in comparison with open mitral valve commissurotomy for mitral stenosis during pregnancy. J Am Coll Cardiol. 2001;37(3):900-3.
2)
3)
4)
5)
6)
7)
8)
9)
10)
11)
12)
13)
14)
139

Chettinad Health City Medical Journal
Uterine Papillary Serous Carcinoma Case Report
Sathiya S*, Famida A M**, Vijayalakshmi K**, Sailatha R*, Renuka S***
*Associate Professor, **Professor, ***Assistant Professor, Department of Obstetrics and Gynaecology, Chettinad Hospital & Research Institute, Chennai, India.
Corresponding author - Sathiya S - ([email protected])
Chettinad Health City Medical Journal 2017; 5(3): 140 - 143
140
Introduction Uterine serous carcinoma(USC), also known as uterine papillary serous carcinoma (UPSC) and uterine serous adenocarcinoma, is an uncommon form of endometrial cancer which is usually seen in postmenopausal women.1 Uterine papillary serous carcinoma(UPSC) comprises lesser than 10% of all endometrial cancers, it is the most intrusive subtype of endometrial carcinoma.2 It is diagnosed on endometrial biopsy, performed in women with post-menopausal bleeding. Endometrial hyperplasia or hormonal therapy is not an origin for UPSC. It usually occurs in patients with endometrial atrophy and is classified as type II endometrial cancer.1
Uterine papillary serous carcinoma (UPSC) shares typical pathological features, genetic features and clinical features with Mullerian origin of other serous cancers. Papillary serous is the most frequent histological type of ovarian tumor associated with mutations in BRCA gene3. Because of its similarities histologically, UPSC may be a manifestation of a field error in carriers of BRCA1, which also comprises ovarian malignancy, fallopian tube malignancy, and primary peritoneal malignancies.
Case PresentationMrs. N, 70yrs old nulligravida, post menopausal 20 years back, came with the chief complaints of vague lower abdominal pain and discomfort since 1 month and post menopausal bleeding since 6 days. She has history of Diabetes Mellitus, Hypertension, Hypothyroid and Medical renal disease Grade I.
Her general and systemic examination were normal.
Per abdomen examination - Soft, Mild Suprapubic tenderness +, No guarding/ rigidity, No palpable mass, No organomegaly.
Per speculum – Minimal bleeding present
Per vaginal examination – Cervix - high up, pointing upwards, Uterus-bulky, 8-10 wks size, Fornices free.
Transvaginal scan - Uterus - 8.8x3.4 cms, Bulky, Endometrial thickness-32mm. Diffuse areas of echogenicity with two small anechoic areas (0.2x0.1cms) seen within the endometrial cavity.
Differential Diagnosis considered were, Endometrial Carcinoma, and Submucosal fibroid.
All preoperative Investigations were done and were normal.
Tumor markers were elevated (Ca 125- 53units/ml, LDH- 236unit/l)
Patient was taken up for examination under anesthesia and Endometrial biopsy taken
HPE Report - Suggestive of uterine papillary serouscarcinoma.
MRI done - Suggestive of Endometrial mass probably Endometrial Carcinoma with pelvic lymph node involvement. (Fig 1)
Dr.Sathiya.S is an undergraduate from Mahatma Gandhi Medical College and Research Institute, Puduchery. She completed her post graduation (MD) in Obstetrics and Gynaecology from Raja Muthiah Medical College and Research Institute, Annamalai University. She is presently working as an Associate Professor in Obstetrics and Gynecology department, Chettinad Hospital & Research Institute, Chennai, India.
Abstract
Uterine papillary serous carcinoma is a distinct subtype of endometrial carcinoma by its histological features exhibiting papillary architecture, poor differentiation and advanced stage when the patient presents initially. Uterine papillary serous carcinoma(UPSC) comprises lesser than 10% of all endometrial cancers, it is the most intrusive subtype of endometrial carcinoma. This is a case report of a 70 year old symptomatic nulliparous woman, in whom endometrial biopsy revealed uterine papillary serous carcinoma.
Key Words: Postmenopausal, Endometrial Carcinoma, Papillary Serous.
Volume 5, Number 3
Fig 1 : MRI showing Uterine Papillary SerousCarcinoma Patient was taken up for StagingLaparotomy

Case Report Uterine Papillary Serous Carcinoma Volume 5, Number 3
Under General anaesthesia, Vertical paramedian incision made. Peritoneal washings obtained. Intra-operative findings-Uterus-10wks size, Bilateral ovaries atrophic, Pelvic and para-aortic lymph nodes enlarged, Sigmoid mesentery infiltration present. Proceeded with Total abdominal hysterectomy with bilateral salpingo - oophorectomy with pelvic and para-aortic lymph node dissection and resection of sigmoid mesentery with omental sampling was done and specimen sent for HPE. Intraperitoneal drain was placed.
2 units of Packed Red Blood Cell transfusion done intraoperatively. Postoperatively treated with antibiotics and analgesics. Post-op period was uneventful.
HPE Report - Papillary serous carcinoma o f endometrium. Tumor involves >1/2 of myometrium. Cervical stroma not involved by tumor. Right pelvic, left pelvic, paraaortic lymph nodes and sigmoid colon are involved by tumor. Right ovary and left fallopian tube are involved by tumor.
Diagnosis - Uterine Papillary Serous Carcinoma - Stage III C2.
Patient advised for post operative chemotherapy and pelvic radiation.
Discussion
History2
In 1981 - Lauchlan & Hendrikson – First identified the condition
In 1983 - Bokhman – 1st proposed hypothesis of 2 distinctly different forms of endometrial carcinoma
Types 4,5
Type - I - Estrogen dependent (90%)(adenocarcinoma–adenoacanthoma, adenosquamous, secretory, ciliated & villoglandular variants)
Type - II - Nonestrogen dependent (10%)(Uterine papillary serous carcinoma & clear cell carcinoma)
Feature
Estrogen stimulation
Growth
Precursor lesion
Age (initial diagnosis)
Built
Histology
Histology Grade
Depth of invasion
Molecular Changes
Type - I
Present
Slow
Atypical hyperplasia
Pre / Perimenopausal
Obese
Endometroid
High, Intermediate or low
Usually superficial
Defects inDNA mismatch repair PTEN inactivation
Type - II (UPSC)
Absent
Rapid
Endometrial glandular dysplasia
Postmenopausal
Thin
Serous,clear cell
High
Often deep
P53 mutation HER-2/neugene amplification
Table 1 : Features of Type I and Type II Endometrial Carcinoma4
UPSC - Its Significance l Distinct subtype of Endometrial carcinoma both clinically and pathologically l Typically arises in postmenopausal women l Endometrial hyperplasia is not a source of UPSC l Not hormone dependent and very aggressive l Seen in patients with endometrial atrophy l Outcome is identical to that of high grade ovarian carcinoma in serous type
Incidence Of Endometrial Carcinoma6
4th most common cancer following Carcinoma Breast, Colorectal Carcinoma & Carcinoma Lung
Developed countries – 22/100,000 (41,000 new cases-USA)
Urban India – 5.8 / 100,000
Rural India – 0.8 / 100,000
Although UPSC is not so common than its endometroid cancer analogue, it explains for a disproportionately high cancer related deaths due to endometrial malignancy.
UPSC – 5-8% of endometrial cancer.
UPSC - 40% endometrial cancer related deaths.
DiagnosisUsually present with postmenopausal bleeding, occasionally abdominal mass
Tissue diagnosis – Endometrial biopsy / Dilatation and Curettage.
141

Volume 5, Number 3
Tumor marker - Ca-125
Ultrasound, Computed Tomography & Magnetic resonance Imaging - for diagnosis & to look for metastasis
HistologyMarked nuclear atypia (enlarged size with irregular nuclear membrane) is seen. There are nipple shaped structures (papillae) with fibrovascular cores, Psammoma bodies and Cilia.
Stage III B : Vaginal or parametrial metastasisStage III C 1 : Metatstasis to pelvic lymph nodesStage III C 2 : Metatstasis to para aortic lymph nodesStage IV A : Invasion of the bowel or bladderStage IV B : Distant metastasis
Survival Rate7
Earlier Stage I & II : 35 - 50%
Stage III & IV : 0 - 15%
Recent Gynaecology Oncology Group (GOG) – 5 year survival rate
Stage I : 50 – 75%
Stage II : 50%
Stage III : 20%
Stage IV : 10%
Treatment6,7
Surgical – Total abdominal hysterectomy with bilateral salpingo-oophorectomy with pelvic and para-aortic lymphadenectomy and omental sampling.
The tumor spreads quickly into myometrium and lymphatic system
If tumor spreads – cytoreduction followed by radiation therapy and/ or chemotherapy
Radiation – Shows no increase in survival rate
Chemotherapy – Beneficial- yet more data needed
Women with advanced stage UPSC are best treated with optimal cytoreduction of metastatic disease followed by adjuvant platinum based chemotherapy (carboplatin and paclitaxel or cisplatin and adriamycin).Careful long term surveillance following surgery is indicated due to its high recurrence rate. 3
Fig 2 : Histology of Uterine papillary serouscarcinoma
Staging Of UPSC : FIGO 7
Stage I A - Tumor is limited to less than half the myometrium
Stage I B - Tumor is limited to more than half the myometrium
Stage II - Cervical stromal invasionStage III A : Tumor invades serosa or adnexa
142
Stage
Stage IA, gradeI-II
Stage IA - grade III, Stage IB,
Stage II
Stage III A, grade I-II
Stage IIIa, high grade,
III B, C
Stage IV
Recommendation
Total abdominal hysterectomy with bilateral salpingo-oophorectomy, withlymph node sampling
Total abdominal hysterectomy with bilateral salpingo-oophorectomyfollowing which pelvic irradiation is given
Total abdominal hysterectomy with bilateral salpingo-oophorectomyfollowing which pelvic irradiation is given
Total abdominal hysterectomy with bilateral salpingo-oophorectomyfollowing which chemotherapy and pelvic irradiation are given
Systemic treatment; chemotherapy and/or progestins are given
Recent AdvancesAbout 60% of UPSC’s was found to have an overexpression of HER2/neu protein, as in breast cancer. Monoclonal antibody - Trastuzumab (Herceptin), has been tested with little success, in phase –II trial. 9
ConclusionUPSC reveals atypical findings on MR imaging: low intensity on T2WI and rapid strong enhancement on dynamic MRI. If UPSC is preoperatively diagnosed in cytological examination, we should be careful in staging because this tumor shows atypical findings on MR imaging and often has dissemination and distant metastases.10
Table 2: Treatment Guidelines of Endometrial Malignancy8
Case Report Uterine Papillary Serous Carcinoma

Volume 5, Number 3
87% of cases report Type I endometrial cancer (endometrioid subtype). 13 - 15% of cases reports Type II papillary serous type and clear cell type. Endometrioid subtype is hormone dependent, while a major molecular aberration p53 mutation is seen in type II cancers with serous type. Outcome and biology is identical to that of high grade ovarian malignancy in serous type. For solitary or isolated recurrences, surgery is a preferable option. Chemotherapy profits for patients with disseminated or metastatic disease. Hormonal therapy with medroxyprogesterone is a justifiable option for patients with type I endometrial malignancy with spread of the disease. Paclitaxel, Carboplatin, and adriamycin are the most effective drugs used in chemotherapy.
Hendrickson M, Ross J, Eifel P, Martinez A, Kempson R. Uterine papillary serous carcinoma: a highly malignant form of endometrial adenocarci-noma. Am J Surg Pathol. 1982 Mar;6(2):93-108.
Jemal A, Siegel R, Xu J, Ward E. Cancer Statistics,2010. CA Cancer J Clin.2010; 60 (5): 277 - 300.
Kelly MG, O’malley DM, Hui P, McAlpine J, Yu H, Rutherford TJ et al. Improved survival in surgical stage I patients with uterine papillary serous carcinoma (UPSC) treated with adjuvant platinum based chemotherapy. Gynecol Oncol 98(3): 353-9.
Grundker C, Gunthert AR, Emons G. Hormonal heterogeneity of endometrial cancer. Adv Exp Med Biol.2008:630:166-88.
References
1)
2)
3)
4)
Bokhman JV. Two pathogenetic types of endometrial carcinoma. Gynecol Oncol.1983;15(1):10-7.
Fader AN, Boruta D, Olawaiye AB, Gehrig PA. Uterine papillary serous carcinoma:epidemiology, pathogenesis and management. Curr Opin Obstet Gynecol.2010;22(1):21-2.
Chan JK, Loizzi V, Youssef M, Osann K, Rutgers J, Vasilev SA et al. Significance of comprehensive surgical staging in noninvasive papillary serous carcinoma of the endometrium. Gynecol Oncol.2003; 90(1):181-5.
Colombo N, Preti E, Landoni F, Carinelli S, Colombo A, Marini C et al. Endometrial Cancer: ESMO Clinical Practice Guidelines. Ann Oncol 2013; 24 (Suppl 6): vi33-vi38.
Santhin AD, Bellone S, Roman JJ, McKenney JK, Pecorelli S. Trastuzumab treatment in patients with advanced or recurrent endometrial carcinoma overexpressing HER2/neu. Int J Gynaecol Obstet. 2008; 102(2): 128-31.
Park BK, Kim B, Park JM, Ryu JA, Kim MS, Bae DS et al. Differentiation of the various lesions causing an abnormality of the endometrial cavity using MR
5)
6)
7)
8)
9)
10)
Case Report Uterine Papillary Serous Carcinoma
143

Chettinad Health City Medical Journal
Malignant Mixed Mullerian Tumor of the Uterus
Case Report
Rijaphin R*, Kavitha D**, Anoop Sreevalsan***, Vasantha N Subbiah****
*Assistant Professor, **Senior Resident, ***Professor, ****Professor & HOD, Department of Obstetrics and Gynaecology,
Chettinad Hospital & Research Institute.
Corresponding author - Rijaphin.R ([email protected])
Chettinad Health City Medical Journal 2017; 5(3): 144 - 146
144
Introduction Carcinosarcomas of the uterus are mixed tumors which has both epithelial and mesenchymal components1. They contribute to 1/3rd of uterine sarcomas. The most common site of these tumors being endometrium but it can also involve any part of the female genital tract such as ovary, vagina, cervix, vulva, fallopian tube. These malignancies commonly involve the post-menopausal age group although few cases have been reported in younger age group. The clinical features include vaginal bleeding which is abnormal, pain abdomen or pelvic pain and mass on clinical examination. They have a poor prognosis. Some of the poor prognostic factors are advanced stage of the disease, invasion of the myometrium. The stromal / mesenchymal/ sarcomatous counter part may be either homologous or heterologous. The heterogenous components can either be a chondrosarcoma or rhabdomyosarcoma or osteosarcoma. Malignant Mixed Mullerian Tumor of the Uterus share the same staging as carcinomas of uterus. This case report is a patient with carcinosarcoma with heterogenous components.
Case ReportA 62 Year old, multiparous ,obese, non hypertensive, non diabetic woman presented with post-menopausal per vaginal bleeding since 5 months, intermittent abdominal pain for 2 months . P/S – cervix healthy, P/V Examination- bulky uterus, mobile, fornices free. Chest X-ray – NAD, USG: - Revealed an ill - defined heterogeneous mass of about 6×4.3 cm in the uterine body,suggesting a possibility of neoplastic pathology.
MRI was done - No involvement of myometrium, no nodes, no liver involvement.Diagnostic curettage was done & sample was sent to Department of Pathology for a histopathological examination, which showed a Malignant Mixed Mullerian Tumor with Heterologous Elements. Pre-operative evaluation was done.This was followed by surgery after getting informed consent. Staging laparotomy proceeded to Total Abdominal Hysterectomy with Bilateral Salpingo- Oophorectomy with Bilateral Pelvic lymphadenectomy, infracolic omentectomy, peritoneal biopsies from paracolic areas taken. Intra op findings- No ascites, 50ml peritoneal washings obtained after saline wash, uterus bulky, subserous pedunculated fibroid present, B/L tubes and ovaries normal, omentum appears normal, pelvic lymph nodes normal, paraaortic lymphnodes normal,inferior surface of diaphragm, liver normal. In pathologic evaluation, grossly, the tumor was polypoid, friable with areas of haemorrhages and necrosis measuring 7×5×3.5cm and filling the uterine cavity. Light microscopy of the mass revealed a heterologous malignancy of biphasic type. The epithelial parts of the tumor had glandular component with papillary pattern at places and focal squamous differentiation. Histopathological examination - Malignant mixed mullerian tumor heterogenous type extending to lower uterine segment. Myometrium not involved. 16 Lymph nodes identified - no tumor deposits. Leiomyoma present. parametrium,omentum, peritoneum not involved. Stage of the tumor was 1. As this was an aggressive tumor the patient was referred to Rajiv Gandhi Government hospital for the adjuvant therapy and follow-up.
Dr. Rijaphin is an undergraduate from Sri Ramachandra Medical College and Research Institute, Chennai. She completed her post graduation (MD) in Obstetrics and Gynaecology from Stanley Medical College and Research Institute, MGR University. She has worked in Government Kasturibha Gandhi Hospital. She is currently working as Assistant Professor in the Department of Obstetrics and Gynaecology, Chettinad Hospital & Research Institute, Chennai, India.
Abstract
Malignant mixed mullerian tumor of the uterus also called carcinosarcoma is a high grade sarcoma of uterus similar to leiomyosarcoma and undifferentiated uterine sarcoma.Although it is a rare tumor which constitutes about 3-4% of uterine malignancy, it is highly aggressive and contributes to a significant percentage of mortality among uterine malignancy. This malignancy is biphasic, it has two-components both epithelial and stromal (mesenchymal differentiation).The present case is of a 62 year old post-menopausal female who had per vaginal bleeding since 5 months. Ultrasonography revealed thickened endometrium and an ill-defined heterogenous soft tissue mass.Diagnostic curettage was done, which on histopathological examination showed Malignant Mixed Mullerian Tumor with heterologous elements. Panhysterectomy was done, and the diagnosis of Malignant Mixed Mullerian Tumor of the uterus was confirmed.
Key Words: Malignant Mixed Mullerian Tumor, Uterus, Postmenopausal.
Volume 5, Number 3

Case Report Malignant Mixed Mullerian Tumor of the Uterus Volume 5, Number 3
type 1, is typically associated with hyperestrogenism, obesity (due to aromatization of androgens into estrogen),and hyperlipidemia, have well or moderately differentiated, typically endometrioid histology, and have a good prognosis (approximately 85%-90% 5-year survival rate). They are frequently associated with PTEN mutations. Type 2 endometrial carcinomas, which represent 10% to 15% of endometrial carcinomas, are typically seen in women without these clinical features. They typically have poorly differentiated endometrioid or serous histology and a worse prognosis (55%-60% 5-year survival rate) and are more often associated with p53 mutations.
Risk factors for carcinosarcoma include obesity, exogenous estrogen use,and nulliparity3, similar to that of endometrial carcinoma. Oral contraceptives and smoking are thought to be protective.4 Some cases may result from prior pelvic radiation.5,6 There is also an association between long-term tamoxifen treatment and malignant mixed mullerian tumor.Prognosis depends on the tumor stage , depth of myometrial invasion .Inner third of myometrium is involved in 80% of cases and 40% have deep invasion of myometrium. Lymphovascular space invasion is detected in many cases, with extrauterine spread and metastases at the time of presentation. In general, most metastatic deposits and foci of lymphatic and vascular space invasion are composed of the carcinomatous element, with sarcomatous metastases being rare.7,8 .
Treatment includes panhysterectomy with or without pelvic lymphadenectomy.Depending on the surgical staging ,grade,histological type ,presence of metastasis,lymphovascular space invasion adjuvant radiotherapy and or chemotherapy is planned. Adjuvant radiotherapy including both external beam radiotherapy and intravaginal brachytherapy can be given to postoperative patients in early stage.
DiscussionMalignant mixed Mullerian tumor of the uterus also called Carcinosarcoma which is the preferred term according to the World Health Organization (WHO) is a biphasic tumor which has both epithelial and malignant mesenchymal counterparts.2 These malignancies are monoclonal with probably sarcomatous differentiation.They are rare tumors comprising 5% or less of uterine malignancies. Their 5-year survival rate is anywhere between of 5% to 40%.It is commonly seen in postmenopausal age group, but can also rarely occur in younger population, the most prevalent age being 65 years. Although relatively rare, carcinosarcomas of the uterus, and of the gynecologic and urinary tracts in general, are more common than in other sites, such as lung, possibly because the epithelial stem cells are mesodermal in origin. The symptom triad of MMMTare abdominal pain, profuse bleeding per vaginum and expulsion of necrotic tissue 3. Clinicopathologic data support separation of carcinomas arising in the endometrium into 2 types. The more common type of neoplasm,
Fig 1: specimen of total abdominal hysterectomyshowing polypoidal tumor mass in uterine cavitywith haemorrhagic and necrotic areas.
Fig 2: Specimen showing uterus with cervix B/Ltubes and ovaries and infracolic omentectomy
Fig 3: HPE showing both carcinomatous (epithelial) and sarcomatous ( mesenchymal /stromal)elements of MMMT with numerous mitotic figures. McCluggage WG. Uterine carcinosarcomas
(malignant mixed Mullerian tumors) are metaplastic carcinomas. Int J Gynecol Cancer. 2002;12(6):687-90.
Silverberg SG, Major FJ, Blessing JA, Fetter B, Askin FB, Liao SY. Carcinosarcoma (malignant mixed mesodermal tumor) of the uterus. A Gynecologic Oncology Group pathologic study of 203 cases. Int J Gynecol Pathol.1990; 9(1):1-19.
Rani K, Jenna – Lynn S. Uterine Carcinosarcomas (Malignant Mixed MullerianTumors): A review with special emphasis on the controversies in Management. Hindawi Publishing Corporation, Obstetrics & Gynaecology International. 2011;Volume 2011. 13 pages.
Zelmanowicz A, Hildesheim A,Sherman ME, Sturgeon SR, Kurman RJ, Barrett RJ. Evidence for a common etiology for endometrial carcinomas and malignant mixed mullerian tumors. Gynecol Oncol. 1998; 69(3):253-7.
References
1)
2)
3)
4)
145

Volume 5, Number 3
Bitterman P, Chun B, Kurman RJ. The significance of epithelial differentiation in mixed mesodermal tumors of the uterus. A clinicopathologic and immunohistochemical study. Am J Surg Pathol. 1990;14(4):317-28.
Sreenan JJ, Hart WR. Carcinosarcomas of the female genital tract. A pathologic study of 29 metastatic tumors: further evidence for the dominant role of the epithelial component and the conversion theory of histogenesis. Am J Surg Pathol.1995;19(6):666-74.
7)
8)
Ali S, Wells M. Mixed Mullerian tumors of the uterine corpus: a review.Int J Gynecol Cancer. 1993;3(1):1-11.
Pothuri B, Ramondetta L, Martino M, Alektiar K, Eifel PJ, Deavers MT.Development of endometrial cancer after radiation treatment for cervicacarci-noma. Obstet Gynecol. 2003;101(5):941-5.
5)
6)
Case Report Malignant Mixed Mullerian Tumor of the Uterus
146

Chettinad Health City Medical Journal
An Ovarian Juvenile Granulosa Cell Tumor in Adult Case Report
Renuka S*, Famida A.M**, Vijayalakshmi K**, Sailatha R***, Sathiya S***
*Assistant Professor, **Professor, ***Associate Professor. Department of Obstetrics and Gynaecology, Chettinad Hospital &
Research Institute, Chennai, India.
Corresponding author - Renuka S - ([email protected])
Chettinad Health City Medical Journal 2017; 5(3): 147 - 149
Introduction Granulosa cells are somatic cells of the sex cord of the ovary which are closely associated with the developing oocyte .Functions of Granulosa cell is production of sex steroids and varying peptides required for folliculogenesis and ovulation. Granulosa cell tumors (GCT) are derived from granulosa cells. It has an incidence of < 5% of ovarian tumors and > 70% of sex chord stromal tumors 1.
Histological types are Adult Granulosa cell tumors, seen in Perimenopausal and postmenopausal women (50 -55 years) and Juvenille Granulosa cell tumors seen in Premenarchal and young girls (5% of all Granulosa cell tumors)1.
Case ReportMrs Y,43 Years old Nulligravida was admitted with complaints of spotting per vaginum for 2 months and lower abdominal pain on and off .Patient also gave history of irregular menstrual cycles, which last for 5 days every 40 to 60 days. Her last menstrual periods was 2 months back. On examination, patient’s vitals were stable, Per Abdomen-Mass of 32 weeks size, irregular, firm in consistency, associated with tenderness on deep palpation. The lower border could not be made out. Per speculum examination showed healthy cervix and vagina, pin hole os, and bleeding through os. Per vaginal examination revealed a bulky uterus, with fullness of anterior and posterior fornices.
Laboratory Finding: Hb - 11.6g /dl, Serum urea-6mg / dl, Serum creatinine - 0.6mg/dl, USG - Right ovary multiloculated cyst present. Endometrial Thickness-12mm, Fractional curettage - No evidence of hyperplasia/malignancy.
Treatment Given: Laparotomy was done and proceeded with Total Abdominal Hysterectomy, Right Ovariotomy and Left salpingo-oophorectomy and infracolic omentectomy. Intra operative findings – Right ovarian tumor 20x20cm size, weighing 3 kg , irregular margins with smooth wall and cystic in consistency , capsule intact. (Fig 1). Uterus and cervix normal , No omental deposits or visceral deposits. Nodes not palpable
Dr. Renuka S is an undergraduate from Sri Ramachandra Medical College and Research Institute, Chennai. She completed her post graduation (MD) in Obstetrics and Gynaecology from Raja Muthiah Medical College and Research Institute, Annamalai University. She is currently working as Assistant Professor in the Department of Obstetrics and Gynaecology, Chettinad Hospital & Research Institute, Chennai, India.
Abstract
Granulosa cell tumors(GCT) derive from cells of the sex cord, and produce hormones. In most of the cases they manifest through the symptoms of compressive growth. This case report discusses about a perimenopausal patient ,who was hospitalised with lower abdominal pain, without any pressure symptoms and diagnosed to have a large tumor in the abdomen. The tumor was completely removed through staging laparotomy and sent for frozen section ,followed by hysterectomy with bilateral salpingectomy and left oophorectomy.
Key Words: Granulosa cell tumor, Juvenile, Sex cord tumor
Volume 5, Number 3
Fig 1 : Specimen of Ovarian Cyst
Histopathology Report showed Multiloculated mitoti-cally active granulosa cell tumor-right ovary. Nuclear grooving, inconspicuous nucleoli, moderate cytoplasm and extensive luteinisation present. (Fig 2, 3)
147

Case Report An Ovarian Juvenile Granulosa Cell Tumor in Adult Volume 5, Number 3
Molecular GeneticsHigh frequency of mutation suggests pathognomonic for Adult GCT and non appearance of this mutation in Juvenile GCT suggests that these are two different tumors. Granulosa cell proliferation is based on different signal pathways and alteration of these pathways lead to uncontrolled proliferation of these cells resulting in GCT. Pathways involved are Adenyl cyclase / cAMP / Protein Kinase A - activated by FSH on FSH receptor. MAPK and Phosphatidyl inositol 3 kinase pathway - triggered by epidermal growth factor.VEGF and its receptors are involved in angiogenesis.7
Tumor Markers17B Estradiol, Inhibin, Mullerian inhibiting substance, Follicular Regulating protein.8
Prognostic FactorsDepends on Age, Tumor Size, Rupture of the Tumor, Mitotic Activity, Nuclear Atypia, Aneuploidy, P53 over expression and Stage of the disease9
Kottarathil VD, Antony MA, Nair IR, Pavithran K. Recent Advances in Granulosa Cell Tumor Ovary: A Review. Indian J Surg Oncol . 2013; 4 (1): 37 - 7.
References
1)
Fig 2 : Microscopic Appearance of JuvenileGranulosa cell tumor
Fig 3 : Mitotic Figure
Immunohistochemistry was positive for immunohisto-chemical stain for inhibin. This is a marker for differen-tiating sex cord stromal tumors from non sex cord stromal tumors.2
Final Diagnosis of Malignant juvenile granulosa cell tumor of ovary (FIGO STAGE 1A) was made.
Discussion
Juvenile Granulosa Cell TumorUsually Granulosa cell tumors (GCT) are unilateral Mass – Tan yellow color due to steroid production. Contains solid and cystic areas. Size of the tumor is > 10 cm in around 73.5% of the cases.3 Juvenile GCT average around 12.4 cm (5 to 26 cm). Granulosa cells have characteristic coffee bean nuclei. Well differentiated GCT have a microfollicular, macrofollicular trabecular and holotubular pattern. Microfollicular is the most common type and have the characteristic Call – Exner body. 4
Microscopic AppearanceTwo characteristic distinguishing features of Juvenile from Adult type are5
Nuclei of Juvenile GCT are rounded , hyperchromatic and grooved with moderate to abundant eosinophilic or vaculated cytoplasm Theca cell component is luteinized Cuboidal cells with occasional nuclear grooves
FOXL2 gene encodes the transcription factor for the normal development for the granulosa cell and mutation of it is encountered in GCT. The mutation is seen in 97% of Adult GCT and 10% of Juvenile GCT.6
Stage
Early stage (1&2)
Late stage (3&4)
5 years
89%
72%
10 years
89%
57%
TreatmentGCT are usually diagnosed by histopathological findings.4 Clinical Suspicion is based on existence of adnexal mass with features of hyperestrogenism, thickened endometrium and increased serum inhibin. Surgical staging remains to be the initial management of a suspected case of GCT. Postoperatively, treatment with platinum based chemotherapy may be the treatment of choice. This is due to the ease of its administration, wide accessibility and better tolerance.10 Stage 1 & 2 disease have very good prognosis1. Stage 1C disease correlated with poor prognostic factors like large tumor size or high mitotic index have a higher chance of relapse and may benefit with post operative treatment .The efficacy of radiation in GCT is not well defined. Recently, drugs like Tyrosin Kinase inhibitors, Bortezomib, Bevacizumab, may play a greater role in the treatment of GCT.11
ConclusionLifelong follow – up of patients diagnosed with GCT is necessary. Follow-up includes clinical examination and tumor markers like inhibin B. This is primarily due to an increased risk of recurrence years after apparent clinical cure of the primary tumor.
Survival by Stage – Park et al (1)
148

Zhao C, Vinh TN, McManus K, Dabbs D, Barner R, Vang R. Identification of the most sensitive and robust immunohistochemical markers in different categories of ovarian sex cord-stromal tumors. Am J Surg Pathol. 2009;33(3):354–66.
Ranganath R, Sridevi V, Shirley SS, Shantha V. Clinical and pathologic prognostic factors in adult granulosa cell tumors of the ovary. Int J Gynecol Cancer. 2008;18(5):929-33
Lee IH, Choi CH, Hong DG, Song JY, Kim YJ, Kim KT. Clinicopathologic characteristics of granulosa cell tumors of the ovary: a multicenter retrospec-tive study. J Gynecol Oncol. 2011;22(3):188 - 95.
Schumer ST, Cannistra SA . Granulosa cell tumor of the ovary. J Clin Oncol.2003;21(6)P:1180 - 9.
Shah SP, Köbel M, Senz J, Morin RD, Clarke BA, Wiegand KC et al. Mutation of FOXL2 in granulosa-cell tumors of the ovary. N Engl J Med. 2009;360:2719–29
2)
3)
4)
5)
6)
Volume 5, Number 3
BJamieson S, Fuller PJ. Molecular pathogenesis of granulosa cell tumors of the ovary. Endocr Rev. 2012;33(1):109-44.
Long WQ, Ranchin V, Pautier P, Belville C, Denizot P, Cailla H, et al. Detection of minimal levels of serum anti-Mullerian hormone during follow-up of patients with ovarian granulose cell tumor by means of a highly sensitive enzyme-linked immunosorbent assay. J Clin Endocrinol Metab. 2000;85(2):540–4
Ayhan A, Salman MC, Velipasaoglu M, Sakinci M, Yuce K. Prognostic factors in adult granulosa cell tumors of the ovary: a retrospective analysis of 80 cases. J Gynecol Oncol. 2009;20(3):158–63
Uygun K, Aydiner A, Saip P, Kocak Z, Basaran M, Dincer M, et al. Clinical parameters and treatment results in recurrent granulosa cell tumor of the ovary. Gynecol Oncol. 2003; 88(3):400-3
Gershenson DM, Copeland LJ, Kavanagh JJ, Stringer CA, Saul PB, Wharton JT. Treatment of metastatic stromal tumors of the ovary with cisplatin, doxorubicin, and cyclophosphamide. Obstet Gynecol. 1987;70(5):765–9.
7)
8)
9)
10)
11)
Case Report An Ovarian Juvenile Granulosa Cell Tumor in Adult
149

Chettinad Health City Medical Journal
Asymptomatic Large Placental Chorioangioma In A Primigravida
Case Report
Binu Pattayail *, Swarnapriya K**, Vasantha N Subbiah***
*Assistant Professor, ** Associate Professor, ***Professor & HOD, Department of Obstetrics and Gynaecology,
Chettinad Hospital & Research Institute.
Corresponding author - Binu P - ([email protected])
Chettinad Health City Medical Journal 2017; 5(3): 150 - 152
150
Introduction Most common placental tumors are benign in nature and chorioangioma of placenta are the most common among them. They constitute 1% of all pregnancies1. Most commonly they present as single tumor but they can also be multiple. Chorioangioma literally means abnormal proliferation of new blood vessels from the chorionic tissue 1-3.
Placental chorioangioma which are smaller than 5 cm are considered small and generally don’t cause any complications. Large tumors cause complications by acting as arteriovenous shunts4. The gold standard diagnostic tool in diagnosing placental chorioangioma is Doppler ultrasound1. Whenever placental chorioangiomas are asymptomatic their management is conservative. Inspite of that, aggressive monitoring of pregnancy and fetal condition is suggested to pick up any early maternal and fetal complications.
Case Presentation26 years old primigravida booked in CHRI a known case of hypothyroidism on treatment, with impaired glucose tolerance on diet control was diagnosed to have a large chorioangioma in growth scan at 32 weeks of size 6x6cm. Patient was followed up with serial growth scan and Doppler twice weekly, and modified biophysical profile twice weekly. No maternal and fetal complications developed throughout pregnancy. Pregnancy was terminated at 38 weeks by elective LSCS in view of large chorioangioma . Alive girl baby of 3.1kg with Apgar 8/10, 9/10 delivered. Placental vascular tumor of 6x7cm attached to the site of cord insertion removed in toto (Fig 1). Prophylactic oxytocics given in view of increased chances of postpartum hemorrhage. Intraoperative and postoperative period uneventful, mother and baby
discharged on post - op 4 day. Histopathological examination revealed chorioangioma with 4 vessels in umbilical cord.
Dr. Binu finished her MBBS and MS OG from Bangalore Medical College and Ramaiah Medical College respectively. She also finished her DNB OG . She has keen interest in laparoscopy, so she went on to do a year fellowship in endogynaecology, recognised by MGR University. At present she is an Assistant Professor in Chettinad Hospital and Research Institute.
Abstract
Chorioangioma of placenta is a benign angioma of placenta . It usually does not cause any symptoms but sometimes may be associated with adverse maternal and fetal complication especially when it reaches large size. We present a case of large chorioangioma in which there were no maternal or fetal complications. The placental tumor size remained the same throughout pregnancy and an uncomplicated term delivery occurred. Placental chorioangioma got confirmed by macroscopic and histopathological examination.
Key Words: Chorioangioma, Placenta, Large
Volume 5, Number 3
Fig 1 : Gross Appearance Of Chorioangioma
DiscussionChorioangioma of placenta is benign angioma of chori-onic tissue1. The neoplastic diseases of placenta are divided into - trophoblastic and nontrophoblastic. Nontrophoblastic diseases are almost always benign. Teratoma and chorioangioma fall into the category of nontrophoblastic diseases1-3 . The most common histological type being chorioangioma1. 1% of histopathological examination of placenta shows chorioangioma (Fig 2). Till date the largest retrospective

Case Report Asymptomatic Large Placental Chorioangioma In A Primigravida Volume 5, Number 3
Ultrasound Diagnosis The first case of chorioangioma was reported by Clarke in 197811. Antenatal ultrasound helps in diagnosis and follow up of fetus, hence timely delivery can be done8. Gray-scale findings are well-defined echogenic mass which is complex . The mass is different from the rest of placenta, and it protrudes into amniotic cavity near the cord insertion8.
The gold standard of diagnosing chorioangioma is Doppler Ultrasound examination. Doppler ultrasound can differentiate chorioangioma from placental teratoma, leiomyoma and blood clot12. On Doppler, feeding vessel has similar pulsatile flow as of umbilical artery but the flow has low resistance due to arteriovenous shunt13(Fig 3). Doppler ultrasound along with fetal echocardiography can diagnose fetuses with cardiac failure. Fetal cordocentesis can be done to diagnose fetal anemia, at the same setting, blood transfusion to fetus can be done14. Amniotic fluid and serum level of alpha-fetoprotein (AFP) is increased in placental chorioangioma, although it is not specific for placental chorioangioma. AFP can also be increased in various other maternal and fetal conditions15.
study conducted had an evidence of 138 chorioangioma in 22000 placentas examined, which makes the incidence of 0.6%5 .
Increased incidence of placental chorioangioma is associated with maternal age, diabetes, hypertension, female sex of the baby, first delivery , multiple pregnancies6,7 .Chorioangioma starts as early as 16th day of fertilization, although it has not being documented in first trimester8. There are three histological patterns of placental chorioangiomas :angiomatous, cellular, degenerated9 . The angioma-tous is commonest histological subtype comprising of numerous capillaries and blood vessels which is surrounded by placental stroma. There is no malignant potential5 .
Fig 2: Microscopic examination of chorioangioma
Fig 3: Doppler imaging of chorioangioma
Clinical Features and Complications Small tumors which are < 5cm are usually asymptomatic and do not cause maternal and fetal complications. Large tumors > 5cm probably cause complications by acting as large arteriovenous shunts. Maternal complications are -preeclampsia, placental abruption, polyhydramnios, preterm labour. Out of these, polyhydramnios and preterm delivery are most common complications , latter caused due to polyhydramnios. Fetal congestive cardiac failure is caused because of increased blood flow through the vascular channels with low resistance acting as an arteriovenous shunt. Other fetal complications are - fetal thrombocytopenia, hemolytic anemia, cardiomegaly, non immunologic fetal hydrops, umbilical vein thrombosis, intrauterine growth restriction, brain infarction, fetal cerebral embolism, and intrauterine and neonatal death10.
The mechanism of polyhydramnios are - ( 1 ) Increased intravascular pressure caused by blood flow obstruction in the tumor near umbilical cord insertion leads to increased transudation into amniotic cavity. ( 2 )Large surface area of enlarged vessels of the tumor also causes increased transudation.(3) Partial placental insufficiency due to shunting of the fetal blood into vessels of placental chorioangioma11.
InterventionsAsymptomatic chorioangioma do not require any intervention, follow up with scan and Doppler is adequate. Chorioangioma with complications before the period of viability requires interventions. Various techniques include - fetal transfusions16, fetoscopic laser coagulation of vessels supplying chorioangioma17, chemosclerosis with absolute alcohol18 and endoscopic surgical devascularization. In presence of polyhydramnios therapeutic amniocentesis and maternal indomethacin therapy is recommended. Steroid administration before 34 weeks is given for fetal lung maturity. Management of chorioangioma is usually conservative. Fetoscopic laser ablation of feeding vessel is considered successful even in large chorioangiomas18.
Image source : Pranay R Shah; Chorioangioma from poly to oligohydramnios - case report from JSAFOG. International scientific journals from Jaypee.
151

152
Volume 5, Number 3Case Report Asymptomatic Large Placental Chorioangioma In A Primigravida
Differential Diagnosis Degenerated myomas, placental teratoma, and blood clot are the differential diagnosis of chorioangioma. Doppler demonstrates presence of vascular channels in chorioangioma whereas in others it’s absent. Echo pattern of chorioangioma remains same, while of blood clot differs. Myoma is seen on maternal surface, partial mole has diffuse pattern8.
ConclusionChorioangioma warrants institutional and timely delivery due to high incidence of fetal death. Antenatal ultrasound is used for diagnosis. Doppler is the gold standard to diagnose chorioangioma. Regular follow-up and timely intervention is the key. Our case was monitored with regular ultrasound and Doppler examinations. The size of the chorioangioma remained same. There were no maternal and fetal complications. Histopathological examination confirmed benign nature and no further follow-up was needed.
Very few rare cases ofchorangiocarcinoma have been reported and are characterized by atypical trophoblasts with high mitotic index. These cases require follow-up of the mother and infant to exclude malignancy13.
Elsayes KM, Trout AT, Friedkin AM, Liu PS, Bude RO, Platt JF, et al. Imaging of the placenta: a multimodality pictorial review.Radiographics. 2009;29(5):1371–1391
Prashanth A, Lavanya R, Girisha KM, Mundkur A. Placental Teratoma Presenting as a Lobulated Mass behind the Neck of Fetus: A Case Report. Case Rep Obstet Gynecol. 2012;2012:857230. Miliaras D, Anagnostou E, Papoulidis I, Miliara X. Non-trophoblastic tumor of the placenta with combined histologic features of chorangioma and leiomyoma. Placenta. 2011;32(1):102–104.
Bashiri A, Furman B, Erez O, Wiznitzer A, Holcberg G, Mazor M. Twelve cases of placental chorioangioma - Pregnancy outcome and clinical significance. Arch Gynecol Obstet. 2002;266(1):53–55.
Kuhnel P. Placental chorioangioma. Acta Obstetri-cia et Gynecologica Scandinavica. 1933;13:143–145.
Hirata GI, Masaki DI, O’Toole M, Medearis AL, Platt LD. Color flow mapping and Doppler velocimetry in the diagnosis and management of a placental chorioangioma associated with nonim-mune fetal hydrops. Obstet Gynecol. 1993;81(5(Pt 2)):850–852.
References
1)
2)
3)
4)
5)
6)
Guschmann M, Henrich W, Entezami M, Duden-hausen JW. Chorioangioma – new insights into a well-known problem. Results of a clinical and morphological study of 136 cases. J Perinat Med. 2003;31(2):163–169.
Bracero LA, Davidian M, Cassidy S. Chorioan-gioma: diffuse angiomatous form. www.thefetus.net. 1993
Marchetti AA. A consideration of certain types of benign tumors of the placenta. AJOG. 1939;38(6):1090.
Duro EA, Moussou I. Placental chorioangioma as the cause of non-immunologic hydrops fetalis; a case report. Iran J Pediatr. 2011;21(1):113–115.
Asokan S, Chad AK, Gard R. Prenatal diagnosis of placental tumor by ultrasound. J Clin Ultrasound. 1978; 6(3):180–181.
Bromley B, Benacerraf BR. Solid masses on the fetal surface of the placenta: differential diagnosis and clinical outcome. J Ultrasound Med. 1994;13(11):883–886.
Sepulveda W, Aviles G, Carstens E, Corral E, Perez N. Prenatal diagnosis of solid placental masses: the value of color flow imaging. Ultrasound Obstet Gynecol. 2000;16(6)554–558.
Gruca-Stryjak K, Ropacka-Lesiak M, Breborowicz G. Intrauterine blood transfusion in case of placental chorangioma. Ginekol Pol. 2011;82(4):304–308.
Androutsopoulos G, Gkogkos P, Decavalas G. Mid-trimester maternal serum hCG and alpha fetal protein levels: clinical significance and prediction of adverse pregnancy outcome. Int J Endocrinol Metab.2013;11(2):102–106.
Zalel Y, Weisz B, Gamzu R, Schiff E, Shalmon B, Achiron R. Chorioangiomas of the placenta: sonographic and doppler flow characteristics. J Ultrasound Med. 2002;21(8):909–913.
Quintero RA, Reich H, Romero R, Johnson MP, Gonçalves L, Evans MI. In utero endoscopic devascularization of a large chorioangioma. Ultrasound Obstet Gynecol. 1996;8(1)48–52.
Wanapirak C, Tongsong T, Sirichotiyakul S, Chanprapaph P. Alcoholization: the choice of intrauterine treatment for chorioangioma. J Obstet Gynaecol Res. 2002;28(2)71–75.
7)
8)
9)
10)
11)
12)
13)
14)
15)
16)
17)
18)

Chettinad Health City Medical Journal
Newer Options in Management of Fibroid Uterus
Class Room
Nalini A P*, Kavitha Karthikeyan**
*Professor, **Assistant Professor, Chettinad Hospital & Research Institute, Chennai, India
Corresponding author - A.P.Nalini ([email protected])
Chettinad Health City Medical Journal 2017; 5(3): 153 - 156
Introduction Leiomyoma, commonly referred to as fibroid is a benign monoclonal tumor arising from uterine myometrial cells. The true prevalence cannot be estimated as there are a lot of asymptomatic patients in whom fibroids may be an incidental sonographic finding. Lifetime risk of a female >45 years acquiring fibroid uterus is 60% with an average of 40 to 80% incidence at 50years.1 Fibroids can be intramural, submucous or subserous depending on the location within the uterus. Rarely, we also encounter cervical, broad ligament and parasitic fibroids. There is a definite genetic predisposition for the origin of fibroids with further growth stimulated by estrogen, progesterone and growth factors like IGF 1 and IGF 2. Common symptoms include heavy menstrual bleeding, dysmenorrhea, pelvic pain, urinary disturbances and pressure symptoms. They can also be associated with reproductive problems like subfertility and miscarriage.2 Fibroids can undergo degeneration,torsion,hemorrhage, infection and very rarely malignant transformation.
The most frequently used investigation for diagnosis is transabdominal and transvaginal ultrasound.3 It can be supplemented by saline infusion for precise diagnosis of sub mucous fibroids. MRI is the most accurate modality for evaluating uterine myomas with sensitivity of 88% - 93% and specificity of 66% - 91%.4 Symptomatic fibroids and asymptomatic ones that enlarge the uterus to >14 weeks size require treatment. Previously, the standard treatment for fibroids has always been surgical, like myomectomy or hysterectomy. Fibroids are still the most common indication for hysterectomy. 5,6 Hysterectomy is associated with perioperative and postoperative morbidity and mortality.6 Hysterectomy can be done by abdominal,vaginal and laparoscopic approaches. Myomectomy is the conservative surgical procedure done with the aim of preserving the uterus. It can be done by hysteroscopic, vaginal, abdominal and laparoscopic routes. Surgical treatment is a major public health cost.7 Symptomatic patients with small fibroids can be expectantly managed with analgesics and antifibrinolytics8. There are a wide range of options between expectant management and surgery. The gynecologist has a significant role in proper counselling and aiding the patient for choosing the appropriate management.
Medical Management Drugs for managing fibroids can be used safely only for short term with temporary benefits in certain situations like medically unfit perimenopausal patients, preoperatively to reduce the size of fibroids and as a part of research. Antifibrinolytics like tranexamic acid , combined oral contraceptives (COC) and progesterones have been used to reduce blood loss associated with uterine fibroids. The effect of COCs and progesterone in reducing the size of fibroids is not documented.9
Mirena Intrauterine system (IUS)
The levonorgesterol containing IUS has shown to reduce menstrual blood loss by 74% over 3months without systemic side effects of progesterones10. Insertion of the device may require anesthesia at times, which is overcome by recently available equivalents like Emily. There is difficulty expected during insertion especially in l arge myomas distorting the cavity. Expulsion of the device is also noted in these patients. No significant reduction in myoma or uterine volume was observed in these patients even after 1 year of use. 11
GnRH analogues
GnRH analogues like leuprolide acetate cause inhibition of pituitary gonadal axis and reduce the size of fibroids temporarily12, and can be used preoperatively. Hysterectomy becomes easier with reduced blood loss, but in those planned for myomectomy cleavage plane is lost and dissection becomes difficult. Smaller myomas temporarily get unnoticed but recur later. Taking into consideration the cost, side effects like menopausal symptoms and bone demineralization with long term use, they should be used in carefully chosen patients.
Selective estrogen receptor modulators (SERM)
SERMs such as raloxifene and ormeloxifene have been tried with the hypothesis that they modulate estrogen receptors in fibroids, causing shrinkage. Raloxifene has been shown to reduce fibroid size in postmenopausal and not pre menopausal women.13 Ormeloxifene in standard therapeutic dosage of 60 mg for a period of 6 months is effective in preventing
Dr.A.P.Nalini is Professor of Obstetrics and Gynaecology at Chettinad Hospital and Research Institute. She retired as a professor from Stanley Medical College. She has been an undergraduate and postgraduate teacher for three decades.
Volume 5, Number 3
153

Class Room Newer Options In Management of Fibroid Uterus
further growth of fibroids and reduces menstrual blood loss . It can be used as an interim treatment to delay surgery.14
Selective progesterone receptormodulators (SPRM)
There is recent biochemical evidence that progesterone stimulates fibroid growth. SPRMs of recent research in treatment of fibroids include mifepristone, asoprisnil, telapristone and ulipristal acetate.15 These drugs are associated with reduction in pain, bleeding and size of fibroids without side effects of estrogen deficiency as noted with GnRH analogues.
Mifepristone
This is an antiprogesterone used in doses of 5-50mg /day. A dose of 25 mg/day for 3 months effectively controls bleeding, reduces uterine and myoma volume, avoids blood transfusion and hysterectomy in many symptomatic patients.16 Patient compliance is good because of the low cost and low incidence of side effects. Endometrial hyperplasia is an adverse effect with long term use.
Ulipristal acetate
This SPRM has been approved for short term therapy of symptomatic fibroids.17 Daily dosage of 5-10 mg for three months showed effective control of bleeding and reduction in size of fibroids. Long term use causes cystic glandular dilatation of endometrium classified by pathologists as PAEC (PRM induced endometrial changes). These changes should not be considered as hyperplasia. More studies are needed to evaluate the effects on endometrium.
Aromatase inhibitors
It has been proven that fibroids have increased expression of aromatase enzyme. Drugs like letrozole and anastrozole block conversion of androgens to estrogens and cause shrinkage of fibroids.18 They are as effective as GnRH analogues but with less side effects. There is insufficient evidence about subsequent reproductive outcome.
Somatostatin analogues
There is a proven role for IGF1 and IGF 2 in the initiation and growth of fibroids. Lanreotide, a long acting somatostatin analogue which reduces growth hormone secretion is shown to reduce myoma size.19 Not many side effects have been reported except gall stone formation. These group of drugs have a potential for novel therapy, for fibroid uterus.
Others
Use of Cabergoline ,a dopamine agonist reduced fibroid size by about 50% within 6 weeks20. Gestrinone with antiestrogen and antiprogesterone properties has been reported to reduce myoma size by 60%21. This drug has androgenic side effects which will restrict its usage. Vitamin D and green tea extracts are observed to have potential role in treatment of fibroids. More clinical trials are required before we initiate their routine use in clinical practice22.
Volume 5, Number 3
Minimally Invasive ProceduresUterine artery embolization, Magnetic Resonance guided focused ultrasound therapy (MRgFUS) and myolysis are minimally invasive alternative procedures to surgery in the treatment of fibroids.
Uterine Artery Embolization
Fig 1 : Uterine artery embolization techniqueSource of image : British Fibroid Trust.org.uk
Uterine artery embolization (UAE) for fibroids also known as uterine fibroid embolization is an image guided minimally invasive procedure to treat symptomatic fibroids. Under fluoroscopy guidance embolic agents are injected into arteries that supply fibroids which cause them to shrink (Fig 1). The size has been reported to reduce by around 50%.23 The procedure requires availability of a specially trained interventional radiologist. The ideal candidates are premenopausal women with symptomatic fibroids <24 weeks size, without coexistent endometriosis or adenomyosis. It is not indicated in postmenopausal women, pregnancy, infertility, renal diseases and those with allergy to the contrast. The advantages are it is a minimally invasive safe procedure with rapid recovery and permanent shrinkage of fibroids.
The procedure is done under local anesthesia supplemented with sedation. A catheter is introduced through femoral artery to reach the uterine artery and specifically to branches that supply the fibroid under fluoroscopy guidance. Polyvinyl alcohol particles or Trisacryl gelatin microspheres are injected into the catheter until they block blood flow to the fibroid. The duration of the procedure is around 1 hour and patients need to rest for 6 hours. Post procedure pelvic pain and fever require analgesic use for 2 weeks. Some patients have vaginal discharge and bleeding.24 Immediate complications include hematoma formation, thrombosis, pseudoaneurysm, infection, post embolization syndrome - a flu like illness. Late complications include amenorrhea, premature menopause and adhesion formation . Fibroid expulsion occurs in 10% patients especially with submucous fibroids.
Magnetic resonance guided focused ultrasound procedure (MRgFUS)
Fig 2 : MRI image of MRgFUS therapySource of image : UCSF Radiology – University of California,
154
Volume 5, Number 3
MRgFUS or High frequency focused ultrasound(HIFU) is a non invasive treatment option for fibroids. This uses high intensity focused ultrasound to destroy the fibroids under real time monitoring (Fig 2). Symptomatic fibroids preferably 1- 4 in number which are enhancing in MRI show good results25. The procedure is contraindicated in patients with adhesions due to previous surgeries, pedunculated fibroids, co-existent adenomyosis and those in whom MRI is contraindicated. Effects on fertility is still unknown. The procedure is done under mild sedation . After proper positioning in MRI chamber ,the frequency and acoustic power are modified to produce appropriate therapeutic temperature of 70 to 80°C which will induce tissue necrosis26. Post procedure complications include skin burns, thermal bowel injury, Deep Vein Thrombosis and sciatic nerve damage. Shrinkage of fibroid may occur in over 3-4 months while pelvic pain, pressure symptoms and abdominal pain tend to resolve earlier.
Myolysis
Various forms of myolysis using cryotherapy, bipolar, radiofrequency, laparoscopy, MRI guided laser have been done with variable results.27
VizAblate is a new transcervical device that combines real time intrauterine sonography with radiofrequency ablation for treatment of fibroids. This device avoids thermal injury to bowel and bladder. This can be considered for future use.28
Laparoscopic USG guided radiofrequency volumetric thermal ablation of uterine myoma is done using a device Accessa29. Further research is required to enable its wider usage.
Carbon dioxide and Nd: YAG laser are used for devascularizing myomas especially submucous types30.
Uterine Artery LigationIt is similar in principle and results to UAE but easier to perform. Simultaneous occlusion of uterine ovarian anastomosis achieved better resolution of symptoms with less effect on future fertility31.
Soliman AM, Yang H, Du EX, Kelkar SS, Winkel C. The direct and indirect costs of uterine fibroid tumors: A systematic review of the literature between 2000 and 2013. Am J Obstet Gynecol 2015;213(2):141–60.
Visvanathan D, Bown S, Cutner A. Review of the conservative surgical treatment of uterine fibroids. Rev Gynaecol Pract 2004;4(1):20–6
Versey MP, Villard-Mackintosh L, McPherson K, Coulton A, Yeates D. The epidemiology of hysterectomy; findings in a large cohort study.Br J Obstet gynecol. 1992;99:402-40
Swimms-Stewart D, Fletcher H. Counselling patients with uterine fibroids: a review of management and complications. Obstet Gynecol 2012;1-6
Friedman AJ, Daly M, Jineau–Norcross M, Gleuson R, Reun MS, Celoff M. Long term medical therapy in leiomyoma uterus: a prospec-tive randomized study of leuprolide acetate depot plus either estrogen-progesterone or progester-one add back for 2 years. Hum Reprod. 1994;9(9):1618-25
Irwine GA, Campbell brown MB, Lumsden MA, Heikkilä A, Walker JJ, Cameron IT. Randomized comparative trial of the levonorgestrel intra uterine system and norethisterone for treatment of idiopathic menorrhagia. Br J Obstet Gynecol. 1998;105(6):592-8
Marico T, Ohara N, Matsico H, Zu Q, Chen W, Sitruk-Ware R. Effects of levonorgestrol releas-ing system and progesterone receptor modulator on uterine leiomyomas. Contraception. 2007;75(6):s99-103
Rutldge SL, Spongy CY, Snow R. Leupride acetate treatment and myoma arterial size. Obstet Gynecol:1997;176:1026-29
Palomba S ,Sammartino A,Dicarlo C,Affinito P, Zullo F, Nappi C. Effects of raloxifene treatment in uterine leiomyomas in postmenopausal women. Fertil Steril. 2001;76(1);38-43
Dasgupta M, Karvo B, Biswas R, Bag T, Dutta S. Evaluation of the SERM ormeloxifene in the treatment of uterine fibroids in the reproductive age group. J Syndromes. 2016;3(2):5
Talaulikar VS, Manyonda I. Progesterone and progesterone receptor modulators in the management of symptomatic uterine fibroids. Eur J Obstet Gynecol Reprod Biol. 2012;165:135–140
Shika S,Neeru G, Ekta S, Mathur AS, Garima G. Effect of mifepristone in treatment of uterine myoma in perimenopausal women. J Midlife health 2013;4(1);22-6
5)
6)
7)
8)
9)
10)
11)
12)
13)
14)
15)
16)
Parker WH. Etiology, symptomatology, and diagnosis of uterine myomas. FertilSteril. 2007;87(4):725-36
National institute of health and clinical excel-lence. Uterine artery embolization for fibroids. London: NICE;2010.
Levens ED, Wesley, Premkumar A, Blocker W, Neiman CK. Magnetic resonance imaging and transvaginal ultrasound for determining fibroid burden: implication for research and clinical care: Am J Obstet Gynecol. 2009;200(5):53
Byun JY,Kim SE, Choi BG, Ko GY, Jung SE, Choi KH. Diffuse and focal adenomyosis:MR imaging findings. Radiographics.1999;19(Suppl 1):s161-70
References
1)
2)
3)
4)
Class Room Newer Options In Management of Fibroid Uterus
155

Volume 5, Number 3
Kalampolas T,Kamath M,Boutas L. Ulipristal acetate for uterine fibroids. A systematic review and meta analysis. Gynecol Endocrinol. 2016;3(2):91-6
Varelas FK, Papanicolaou AN, Vavatsi-Christaki N, Makedos GA, Vlassis GD. The effect of anastrazole on symptomatic uterine leiomyomata. Obstet Gynecol. 2007;110(3):643–9.
practice committee of the American Society for Reproductive Medicine and Society of Reproductive surgeons. Myomas and reproductive function. Fertil Steril. 2008;90(3):S125-30
Melli MS, Farzadi L, Madarek EO. Comparison of the effect of gonadotropin-releasing hormone analog (Diphereline) and Cabergoline (Dostinex) treatment on uterine myoma regression. Saudi Med J. 2007; 28(3):445-50.
La Marca A, Giulini S, Vito G, Orvieto R, Volpe A, Jasonni VM. Gestrinone in the treatment of uterine leiomyomata: effects on uterine blood supply. Fertil Steril. 2004; 82(6):1694-6
Sharan C, Halder SK, Thota C, Jaleel T, Nair S, Al-Hendy A. Vitamin D inhibits proliferation of human uterine leiomyoma cells via catechol-O-methyltransferase. Fertil Steril. 2011 Jan; 95(1):247-53
Goodwin SC, Spies JB, Worthington-Kirsch R, Peterson E, Pron G, Li S, et al. Uterine artery embolization for treatment of leiomyomata: long-term outcomes from the fibroid registry. Obstet Gynecol. 2008; 111(1):22-33.
Ravina JH, Herbreteau D, Ciraru-Vigneron N, Bouret JM, Houdart E, Aymard A, et al. Arterial embolisation to treat uterine myomata. Lancet. 1995; 346(8976):671-2.
17)
18)
19)
20)
21)
22)
23)
24)
Stewart EA, Gedroyc WM, Tempany CM, Quade BJ, Inbar Y, Ehrenstein T, et al. Focused ultrasound treatment of uterine fibroid tumors: safety and feasibility of a noninvasive thermoablative technique. Am J Obstet Gynecol. 2003; 189(1):48-54.
Tempany CM, Stewart EA, McDannold N, Quade BJ, Jolesz FA, Hynynen K. MR imaging-guided focused ultrasound surgery of uterine leiomyomas: a feasibility study. Radiology. 2003;226:897–905.
Goldfarb H. Myolysis Revisited. JSLS. 2008; 12(4): 426–30.
Garza-Leal JG, Toub D, Hernández L. Transcervical, intrauterine ultrasound-guided radiofrequency ablation of uterine fibroids with the VizAblate System: safety, tolerability, and ablation results in a closed abdomen setting. Gynecol Surg. 2011;8(3):327–34.
Chudnoff SG, Berman JM, Levine DJ, Harris M, Guido RS, Banks E. Outpatient procedure for the treatment and relief of symptomatic uterine myomas. Obstet Gynecol. 2013;121(5):1075–82
Donnez J, Squifflet J, Polet R, Nisolle M. Laparoscopic myolysis. Hum Reprod Update. 2000;6(6):609-13.
Akinola OI, Fabamwo AO, Akinola RA, Ottun TA, Akinniyi A, Akpan AE. Uterine artery ligation for the treatment of fibroids. Acta Obstet Gynecol Scand. 2009;88(1):59-62.
25)
26)
27)
28)
29)
30)
31)
Class Room Newer Options In Management of Fibroid Uterus
156
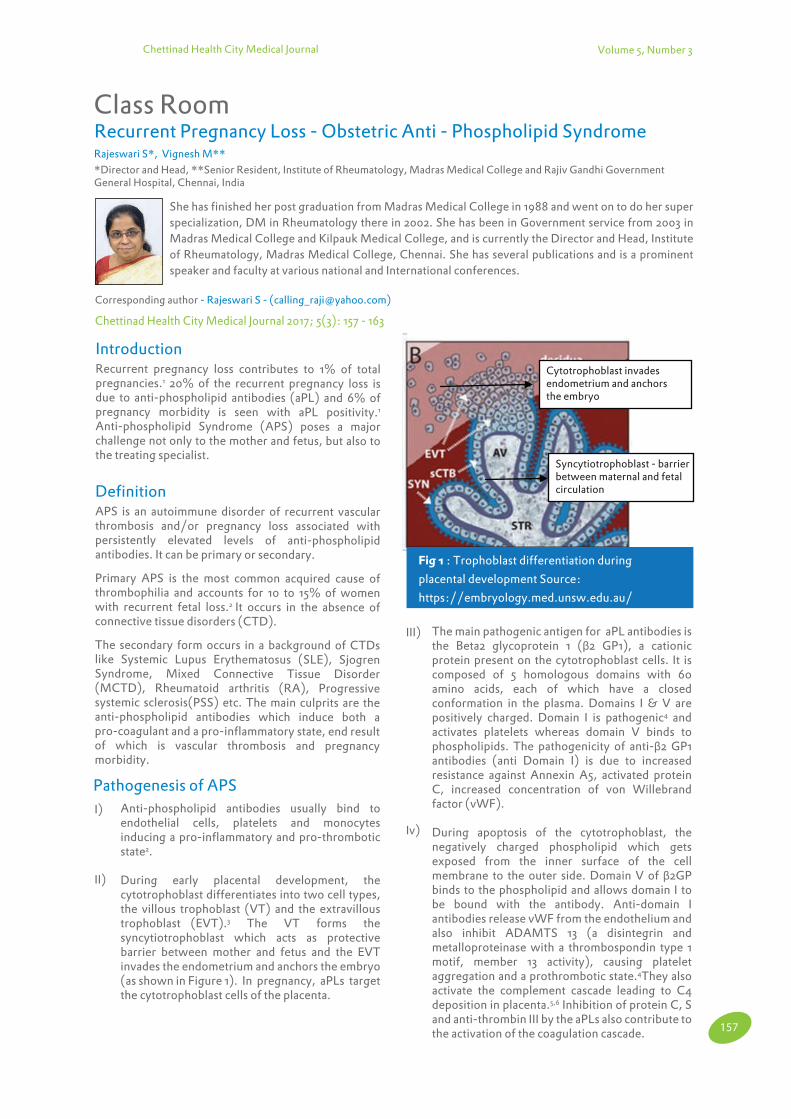
Chettinad Health City Medical Journal
Recurrent Pregnancy Loss - Obstetric Anti - Phospholipid SyndromeClass Room
Rajeswari S*, Vignesh M**
*Director and Head, **Senior Resident, Institute of Rheumatology, Madras Medical College and Rajiv Gandhi Government General Hospital, Chennai, India
Corresponding author - Rajeswari S - ([email protected])
Chettinad Health City Medical Journal 2017; 5(3): 157 - 163
Introduction Recurrent pregnancy loss contributes to 1% of total pregnancies.1 20% of the recurrent pregnancy loss is due to anti-phospholipid antibodies (aPL) and 6% of pregnancy morbidity is seen with aPL positivity.1 Anti-phospholipid Syndrome (APS) poses a major challenge not only to the mother and fetus, but also to the treating specialist.
DefinitionAPS is an autoimmune disorder of recurrent vascular thrombosis and/or pregnancy loss associated with persistently elevated levels of anti-phospholipid antibodies. It can be primary or secondary.
Primary APS is the most common acquired cause of thrombophilia and accounts for 10 to 15% of women with recurrent fetal loss.2 It occurs in the absence of connective tissue disorders (CTD).
The secondary form occurs in a background of CTDs like Systemic Lupus Erythematosus (SLE), Sjogren Syndrome, Mixed Connective Tissue Disorder (MCTD), Rheumatoid arthritis (RA), Progressive systemic sclerosis(PSS) etc. The main culprits are the anti-phospholipid antibodies which induce both a pro-coagulant and a pro-inflammatory state, end result of which is vascular thrombosis and pregnancy morbidity.
She has finished her post graduation from Madras Medical College in 1988 and went on to do her super specialization, DM in Rheumatology there in 2002. She has been in Government service from 2003 in Madras Medical College and Kilpauk Medical College, and is currently the Director and Head, Institute of Rheumatology, Madras Medical College, Chennai. She has several publications and is a prominent speaker and faculty at various national and International conferences.
Volume 5, Number 3
Anti-phospholipid antibodies usually bind to endothelial cells, platelets and monocytes inducing a pro-inflammatory and pro-thrombotic state2.
During early placental development, the cytotrophoblast differentiates into two cell types, the villous trophoblast (VT) and the extravillous trophoblast (EVT).3 The VT forms the syncytiotrophoblast which acts as protective barrier between mother and fetus and the EVT invades the endometrium and anchors the embryo (as shown in Figure 1). In pregnancy, aPLs target the cytotrophoblast cells of the placenta.
Pathogenesis of APS
I)
II)
Cytotrophoblast invadesendometrium and anchorsthe embryo
Syncytiotrophoblast - barrierbetween maternal and fetalcirculation
Fig 1 : Trophoblast differentiation during
placental development Source:
https://embryology.med.unsw.edu.au/
The main pathogenic antigen for aPL antibodies is the Beta2 glycoprotein 1 (β2 GP1), a cationic protein present on the cytotrophoblast cells. It is composed of 5 homologous domains with 60 amino acids, each of which have a closed conformation in the plasma. Domains I & V are positively charged. Domain I is pathogenic4 and activates platelets whereas domain V binds to phospholipids. The pathogenicity of anti-β2 GP1 antibodies (anti Domain I) is due to increased resistance against Annexin A5, activated protein C, increased concentration of von Willebrand factor (vWF).
During apoptosis of the cytotrophoblast, the negatively charged phospholipid which gets exposed from the inner surface of the cell membrane to the outer side. Domain V of β2GP binds to the phospholipid and allows domain I to be bound with the antibody. Anti-domain I antibodies release vWF from the endothelium and also inhibit ADAMTS 13 (a disintegrin and metalloproteinase with a thrombospondin type 1 motif, member 13 activity), causing platelet aggregation and a prothrombotic state.4They also activate the complement cascade leading to C4 deposition in placenta.5,6 Inhibition of protein C, S and anti-thrombin III by the aPLs also contribute to the activation of the coagulation cascade.
III)
Iv)
157

Class Room Recurrent pregnancy loss - Obstetric Anti - Phospholipid Syndrome Volume 5, Number 3
Hence obstetric APS is not a single disease entity. Multiple factors play a role on the placental as well as the endometrial cells as follows
a. Mechanisms on placental cell5
The role of annexin V is to prevent exposure of phospholipids to the outer surface of the trophoblast layer and anti-annexin V antibodies expose the phospholipids activating coagulation cascade.
Antiphospholipid antibodies impair invasion and proliferation of trophoblastic cells. Antiphosphatidyl serine antibodies are responsible for syncytiotrophoblast fusion impairments.7 Serum beta human Chorionic Gonadotropin levels have been found to be decreased in patients with APS.
Anti - phospholipids also interfere with endometrial differentiation and angiogenesis. Anti β2 GP1 antibodies inhibit angiogenesis, vascular endothelial growth factor (VEGF) secretion and NFkB (Nuclear Factor Kappa B) activation.8 The placenta is made dysfunctional by thrombosis and fibrin deposits. It appears shrunken, hemorrhagic and edematous.
Innate immunity also plays a major role. Toll - like receptor 2 (TLR2) and TLR 4 pathologically activate endothelial cells, monocytes and platelets.8-13 Translocations of TLR 7 and TLR 8 have been noted in endosomes of human monocytes.14
HLA associations include HLA DR7, HLA DR4 and HLA DR3. Epitope mimicry is also thought to play a role in producing the autoimmune status.15
Exposure of tissue factor, increased plasminogen activator inhibitor I and induction of apoptosis of cytotrophoblasts predisposes to APS.
v)
vi)
vii)
viii)
ix)
x)
Thrombosis by aspecific mechanism
Inflammation and complement activation
TLR 4 (Toll Like Receptor 4) activation by a PL8 - 13
Defective placentation
i)
ii)
iii)
iv)
Migration: decrease in IL-6 and STAT3 expression16
Invasion: decrease in integrin expression
Differentiation: decrease in β-hCG secretion and decrease in fusion
b. Mechanisms on endometrial cells 5
i) Angiogenesis inhibition by decrease in VEGF (Vascular Endothelial Growth Factor) secretion
ii) Inhibition of NFκB (Nuclear Factor Kappa B) activation8.
(a)
(b)
(c)
Clinical ManifestationsMajority of the patients present with recurrent fetal loss beyond 20 weeks and may exceed 90% in untreated patients.17 Aspirin and heparin can reduce the fetal loss by 25%.7 Other manifestations include severe pre-eclampsia and preterm birth, before 34th week of gestation. Severe preeclampsia manifests as central nervous system symptoms like headache, visual distur-bance, liver dysfunction, blood pressure greater than 160/110 mmHg, thrombocytopenia with platelets less than 1 lakh/mm3, renal dysfunction and pulmonary edema.
These patients are at high risk of placental insufficiency leading to Intra uterine growth restriction(IUGR) and oligohydramnios. Placental insufficiency is assessed by an abnormal or non-reassuring Non stress test (NST). An abnormal Doppler wave study indicates an increased resistance to blood flow which reflects as fetal hypoxia. Amniotic fluid index (AFI) less than 5 indicates oligohydramnios and post natal birth weight might be less than the 10th percentile for the gestational age.
Previous fetal loss is a compounding risk factor for further fetal loss, preeclampsia, premature birth and placenta mediated complications in patients with obstetric anti phospholipid syndrome. Multiorgan failure during pregnancy has been described by Asherson18 and by Kochenour19 in the post-partum period.
Obstetric APS is more than a single disease entity affecting both mother and the child as depicted in Figure 2. Other features include thrombosis, both venous and arterial. It can occur in Inferior vena cava (IVC), pulmonary veins, hepatic, renal veins, leg veins, cerebral arteries, coronaries, brachial, mesenteric & extremity arteries. Catastrophic events like strokes, pulmonary hypertension, pulmonary infarct, ARDS & diffuse alveolar hemorrhage can occur.
Gangrene, livedo reticularis, cutaneous ulcers are the skin manifestations. Eye involvement in the form of Central retinal artery or venous occlusions can occur. Avascular necrosis of bones and renal involvement are other manifestations. Chorea gravidarum, autoimmune hemolytic anemia and thrombocytopenia, positive direct Coomb’s test can occur along with prolonged activated partial thromboplastin time (aPTT) or prothrombin time (PT).
Fig 2: Obstetric APS more than a single diseaseentity5
Preconception?
l Infertility?[23]
l Increased risk of DVT and PE due to hormonal Stimulation [59]
l Implantation failure? [24,25]
Mother during pregnancy:
l Increased risk of DVT and PE
l Increased risk of thrombocytopenia
l Preeclampsia and eclampsia
l Abruptio placentae
Foetus:
l Early miscarriage
l Stillbirth
l Prematurity, IUGR
Infants?
l Increased risk of
neuro psychological
disorders? [26]
Dvt: deep venous thrombosis; PE: pulmonary embolism; IUGR: Intrauterine growth restriction
158

Volume 5, Number 3
Diagnosis of APSThe Sapporo criteria for classification of anti-phospholipid syndrome was amended in May 2012 and presented in Sydney, The Sydney Classification criteria20. This includes both clinical and laboratory criteria for classifying APS as follows:
Clinical Criteria
1.Vascular thrombosis One or more clinical episodes of arterial, venous, or small vessel thrombosis in any tissue or organ confirmed by Imaging, Doppler, or histopathological examination (without significant vessel wall inflammation)
2. Pregnancy morbidity (normal morphology on ultrasonography or direct examination findings) with either of the following
l One or more unexplained fetal deaths at > 10 weeks gestation
l One or more premature births at <34 weeks gestation due to severe preeclampsia, eclampsia, or placental insufficiency.
l Three or more unexplained consecutive spontaneous abortions at <10 weeks gestation, excluding maternal anatomic or hormonal abnormalities and paternal and maternal chromosomal causes
Laboratory Criteria
l Anticardiolipin (aCL) antibody
l IgG / IgM isotype in medium/high titer [>40 IgG phospholipid units (GPL), >40 IgM phospholipid units (MPL)] on 2 or more occasions 12 weeks apart
l Anti - β2-GP1
l IgG or IgM isotype in serum or plasma (in titers> 99thpercentile) measured by ELISA on 2 or more occasins 12 weeks apart.
l Lupus anticoagulant on 2 or more occasions at least 12 weeks apart.
DiagnosisOne clinical criteria and one laboratory criteria should be satisfied on 2 occasions more than 12 weeks apart and < 5years before the clinical episode classifies the patient to have APS. Lupus anticoagulant (LA) carries the highest risk of arterial and venous thrombosis. Those with “Triple positive” antibodies i.e aCL, LA and Anti β2GP1 are at highest risk for thrombosis.21
The differential diagnosis for catastrophic anti-phospholipid syndrome include thrombotic thrombocytopenic purpura(TTP), Hemolytic anemia with elevated Liver enzymes and low platelets (HELLP syndrome) and Acute Fatty Liver of Pregnancy(AFLP).22 (as shown in Table 1)
Features
Fever
Microangiopathic hemolytic anemia (MAHA)
Thrombocytopenia
Renal
Hypertension
Hepatic
Hypoglycemia
Hepatic infarcts
Pulmonary
Disseminated intravascular Coagulation
ADAMTS13 <5%
TTP
+++
+++++
+
++
+++
+
-
-
-
-
+++++
CAPS
+
+
+++
++++
+
+
-
+
+++++
+
-
HELLP
-
+++++
+++
+++
++++
+
-
+
-
+++
-
AFLP
++
+
-
+++++
++
+++++
+++
-
-
++++
-
Table 1: Differential diagnosis of Catastrophic APS23
TreatmentTreatment of obstetric APS requires, preventing thrombus development, giving safe drugs before and during pregnancy and in the postpartum period to prevent complications. The proposed management for APS is described. (Flow chart 1 and Tables 2, 3 and 4)
Class Room Recurrent pregnancy loss - Obstetric Anti - Phospholipid Syndrome
159

Volume 5, Number 3
Flowchart 1: Proposed line of management of APS:5
APS with prior fetal death or recurrent pregnancy loss
Heparin in prophylactic doses (15,000-20,000 U of unfractionated heparin or equivalent per day) administered subcutaneously in divided doses with low-dose aspirin daily
Calcium and vitamin D supplementation
Optimal management uncertain; options include no treatment or daily treatment with low-dose aspirin
FeaturePregnant
Management
Non pregnant
APS with prior thrombosis or stroke
Heparin to achieve full anticoagulation (does not cross the placenta)
Warfarin administered daily in doses to maintain international normalized ratio of 2.5 and in recurrent thrombosis INR is maintained between 3-4 with the addition of low dose aspirin
APS without prior pregnancy loss or thrombosis
No treatment or daily treatment with low-dose aspirin or daily treatment with prophylactic doses of heparin plus low-dose aspirin; optimal management uncertain
No treatment or daily treatment with low - dose aspirin; optimal manage-ment uncertain
aPL Antibodies Without APS
LAC or medium to high level of aCL IgG
No treatment No treatment
Low levels of aCL IgG, only aCL IgM, or only aCL IgA without LA, aPL, or aCL
No treatment No treatment
Table 2 : Proposed Management For Women With Apl Antibodies5,30
Class Room Recurrent pregnancy loss - Obstetric Anti - Phospholipid Syndrome
160

Volume 5, Number 3
Scenarios Management
APS with thrombosis on warfarin
Continue warfarin. Stop warfarin within 14 days of missing period and check pregnancy and start heparin at therapeutic doses once pregnancy is confirmed
APS with thrombosis and pregnancy morbidity As above + start low dose aspirin
APS with pregnancy morbidity aloneStart low dose aspirin preconceptionally start heparin at prophylactic doses once pregnancy is confirmed
aPL antibodies+ No treatment
Table 3 : Pre-conceptional management of APS5,30
Scenarios Management
APS with thrombosis UFH/LMHW therapeutic doses
APS with thrombosis and pregnancy morbidity UFH/LMWH therapeutic doses + low dose aspirin
Table 4 : Ante partum management of APS 5,30
APS with pregnancy morbidity alone UFH/LMHW prophylactic doses + low dose aspirin
APS antibodies+Pregnancy Low dose aspirin
DrugsDrugs approved during pregnancy include low dose aspirin, unfractionated heparin, low molecular weight heparin (LMWH) and newer anticoagulants Danaparoid (Heparinoid) and Fondaparinaux (anti Xa). Warfarin is indicated only in the second trimester and postpartum period.
Anticoagulation during pregnancy needs to be taken care specially, taking into consideration the maternal peripartum state, fetal safety etc. Heparins are commonly used as they do not cross the placenta. Among these, the choice would be Low molecular weight heparin(LMWH) except during the final weeks of pregnancy, as they are easily adminis-tered, do not require monitoring and have a more predictable response than unfractionated heparin(UFH).23
Unfractionated heparin is cost effective and is the drug of choice during labour, perioperative period and when creatinine clearance is < 30ml/min.23
Danaparoid is a heparinoid but considered as a LMWH by some. It acts by inhibiting activated factor X (Xa). It does not cross the placenta and is reserved for patients with heparin induced thrombocytopenia.23
Warfarin is better avoided in pregnancy, as it is teratogenic; with the highest risk between 6 and 12 weeks of gestation. It can cause embryopathy, fetal bleeding and miscarriage. When there is no other choice, it may be relatively safe during the second trimester only 24 - 27 and in the post - partum period.
Warfarin should be titrated to an INR (International Normalized Ratio) of 2.0-3.0.28 To counteract bleeding, vitamin K and fresh frozen plasma can be given.
How and when to start heparin? A baseline platelet count and serum creatinine are mandatory. Platelet counts are assessed on day 3, weekly during first two weeks and monthly thereafter, when on heparin. LMWH are preferred as they do not cross the placenta and are safe for the fetus.29 For those requiring antico-agulation during pregnancy, LMWH is the preferred drug. It is started after confirmation of pregnancy. Both LMWH and prophylactic unfractionated heparin are given subcutaneously although the latter can be given intravenously when constant levels need to be maintained and when rapid discontinuation is necessary (eg. delivery, surgery). Prefilled preserva-tive free syringes are better since preservative contain-ing heparins are contra indicated in pregnancy.
For LMWH, therapeutic dosage is based on body weight and anti-factor Xa levels. It is administered subcutaneously 12th hourly (eg.Enoxaparin 1mg/kg or dalteparin 100 units/kg). If necessary, peak anti-factor X a activity levels are tested 4-6 hours after the last dose (recommended levels are 0.6 to 1.0 units/ml). For unfractionated heparin therapeutic dosage is administered intravenously and is adjusted to maintain an activated partial thrompoplastin time 1.5 to 2.5 times baseline.29
Prophylactic LMWH is administered as a single subcutaneous dose of 40 mg every day. Prophylactic
Class Room Recurrent pregnancy loss - Obstetric Anti - Phospholipid Syndrome
161

Volume 5, Number 3
subcutaneous injection starting from 5000 units in the first trimester and increasing by 2500 units every trimester.
Switching from subcutaneous to intravenous heparin should be done prior to labor in patients requiring continuous anticoagulation. At the onset of labor heparin is discontinued and resumed 4 to 6 hours after normal delivery and 6 to 12 hours after caesarean in prophylactic dose.
In the event of bleeding with heparin, protamine sulphate may have to be given intravenous at a dose of 1-1.5mg IV for every 100 units of heparin and aPTT is monitored 15min after protamine and again after 6-8 hours.23,28
IVIG (Intravenous Immunoglobulin) is another drug which can modulate aCL levels in refractory APS and so is plasma exchange. For patients with SLE, immunosuppression is required, the safest drugs are hydroxychloroquine and azathioprine. Plasma exchange is in the investigational phase.
PrecautionsObstetric patients who were recently treated with steroids should take steroid supplementation during labor. Pregnancy by itself does not harm the mother or fetus.30
In the event of a low platelet count, epidural anesthesia should not be given and use of forceps or vacuum extractor should be done with discretion.30
Counseling and patient education are very important. USG is done every 3-4 weeks starting from 20 weeks. Viability of pregnancy can be assessed by USG. Screening should be done to rule out thrombosis, thromboembolism, decreased fetal movement or severe preeclampsia. In patients with refractory thrombocytopenia either during early second trimester or during Caesarean section, splenectomy may be considered.30
ConclusionObstetric anti-phospholipid syndrome is a great challenge to the mother and fetus. A better understanding of the pathological mechanisms is needed for therapeutic interventions. Screening for anti-phospholipid syndrome improves pregnancy outcomes. SLE with APS requires both thromboprophylaxis and immunosuppression. Multidisciplinary management with a strict follow up is needed.
Di Prima FA, Valenti O, Hyseni E, Giorgio E, Faraci M, Renda E, et al. Antiphospholipid Syndrome during pregnancy: the state of the art. J Prenat Med. 2011; 5(2): 41–53.
Giannakopoulos B, Krilis SA. The pathogenesis of the antiphospholipid syndrome. N Engl J Med. 2013;368(11):1033–44.
References
1)
2)
Evain-Brion D, Guibourdenche J, Tsatsaris V, Fournier T. Human trophoblast differentiation. Bull Acad Natl Med. 2009;193(5):1017-25
Mahler M, Norman GL, Meroni PL, Khamashta M. Autoantibodies to domain 1 of beta 2 glycoprotein 1: a promising candidate biomarker for risk management in antiphospholipid syndrome. Autoimmun Rev. 2012;12(2):313–7.
Marchetti T, Cohen M, de Moerloose P. Obstetri-cal Antiphospholipid Syndrome: From the Pathogenesis to the Clinical and Therapeutic Implications. Clin Dev Immunol. 2013;2013:159124.
Cavazzana I, Manuela N, Irene C, Barbara A, Sara S, Orietta BM et al., Complement activation in anti-phospholipid syndrome: a clue for an inflammatory process? J Autoimmun. 2007;28(2-3)160-4.
Adler RR, Ng AK, Rote NS. Monoclonal antiphos-phatidyl serine antibody inhibits intercellular fusion of the choriocarcinoma line, JAR. Biol Reprod. 1995 Oct;53(4):905–10.
Dunoyer-Geindre S, de Moerloose P, Galve-de Rochemonteix B, Reber G, Kruithof EKO. NFkap-paB is an essential intermediate in the activation of endothelial cells by anti-beta(2)-glycoprotein 1 antibodies. Thromb Haemost. 2002;88(5):851–7.
Satta N, Kruithof EKO, Reber G, de Moerloose P. Induction of TLR2 expression by inflammatory stimuli is required for endothelial cell responses to lipopeptides. Mol Immunol. 2008;46(1):145–57.
Raschi E, Testoni C, Bosisio D, Borghi MO, Koike T, Mantovani A, et al. Role of the MyD88 transduction signaling pathway in endothelial activation by antiphospholipid antibodies. Blood. 2003;101(9):3495–500.
Vega-Ostertag M, Casper K, Swerlick R, Ferrara D, Harris EN, Pierangeli SS. Involvement of p38 MAPK in the up-regulation of tissue factor on endothelial cells by antiphospholipid antibodies. Arthritis Rheum. 2005;52(5):1545–54.
Satta N, Dunoyer-Geindre S, Reber G, Fish RJ, Boehlen F, Kruithof EKO, et al. The role of TLR2 in the inflammatory activation of mouse fibroblasts by human antiphospholipid antibodies. Blood. 2007;109(4):1507–14.
Satta N, Kruithof EKO, Fickentscher C, Dunoyer-Geindre S, Boehlen F, Reber G, et al. Toll-like receptor 2 mediates the activation of human monocytes and endothelial cells by antiphosph-olipid antibodies. Blood. 2011;117(20):5523–31.
Prinz N, Clemens N, Strand D, Pütz I, Lorenz M, Daiber A, et al. Antiphospholipid antibodies induce translocation of TLR7 and TLR8 to the endosome in human monocytes and plasmacytoid dendritic cells. Blood. 2011 Aug 25;118(8):2322–32.
3)
4)
5)
6)
7)
8)
9)
10)
11)
12)
13)
14)
Class Room Recurrent pregnancy loss - Obstetric Anti - Phospholipid Syndrome
162

Volume 5, Number 3
Christiansen OB, Ulcova-Gallova Z, Mohapeloa H, Krauz V. Studies on associations between human leukocyte antigen (HLA) class II alleles and antiphospholipid antibodies in Danish and Czech women with recurrent miscarriages. Hum Reprod. 1998;13(12):3326–31.
Mulla MJ, Myrtolli K, Brosens JJ, Chamley LW, Kwak-Kim JY, Paidas MJ, et al. Antiphospholipid antibodies limit trophoblast migration by reducing IL-6 production and STAT3 activity. Am J Reprod Immunol. 2010;63(5):339–48.
Cowchock FS, Reece EA, Balaban D, Branch DW, Plouffe L. Repeated fetal losses associated with antiphospholipid antibodies: a collaborative randomized trial comparing prednisone with low-dose heparin treatment. Am J Obstet Gynecol. 1992;166(5):1318–23.
Asherson RA, Khamashta MA, Ordi-Ros J, Derksen RH, Machin SJ, Barquinero J, et al. The “primary” antiphospholipid syndrome: major clinical and serological features. Medicine (Baltimore). 1989;68(6):366–74.
Kochenour NK, Branch DW, Rote NS, Scott JR. A new postpartum syndrome associated with antiphospholipid antibodies. Obstet Gynecol. 1987;69(3 Pt 2):460–8.
Miyakis S, Lockshin MD, Atsumi T, Branch DW, Brey RL, Cervera R, et al. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS). J Thromb Haemost. 2006;4(2):295–306.
Tripodi A. Laboratory testing for lupus anticoagu-lants: a review of issues affecting results. Clin Chem. 2007;53(9):1629–35.
15)
16)
17)
18)
19)
20)
21)
Kazzaz NM, McCune WJ, Knight JS. Treatment of catastrophic antiphospholipid syndrome. Curr Opin Rheumatol. 2016;28(3):218-27.
Hughes S, Szeki I, Nash MJ, Thachil J. Anticoagula-tion in chronic kidney disease patients—the practical aspects. Clin Kidney J. 2014;7(5):442–9. Howie PW. Anticoagulants in pregnancy. Clin Obstet Gynaecol. 1986 Jun;13(2):349–63.
Rutherford SE, Phelan JP. Thromboembolic disease in pregnancy. Clin Perinatol. 1986;13(4):719–39.
Iturbe-Alessio I, Fonseca MC, Mutchinik O, Santos MA, Zajarías A, Salazar E. Risks of anticoagulant therapy in pregnant women with artificial heart valves. N Engl J Med. 1986;315(22):1390–3. Pauli RM, Lian JB, Mosher DF, Suttie JW. Associa-tion of congenital deficiency of multiple vitamin K-dependent coagulation factors and the pheno-type of the warfarin embryopathy: clues to the mechanism of teratogenicity of coumarin deriva-tives. Am J Hum Genet. 1987;41(4):566–83. Holbrook A, Schulman S, Witt DM, Vandvik PO, Fish J, Kovacs MJ, et al. Evidence-Based Manage-ment of Anticoagulant Therapy. Chest. 2012;141(2 Suppl):e152S–e184S
Forestier F, Daffos F, Capella-Pavlovsky M. Low molecular weight heparin (PK 10169) does not cross the placenta during the second trimester of pregnancy study by direct fetal blood sampling under ultrasound. Thromb Res. 1984;34(6):557-60.
Teresa G Berg. Antiphospholipid Syndrome and Pregnancy Treatment & Management: Approach Considerations, Obstetric Care, Nonobstetric Care. 2017; Available from: http://emedicine.medscape.com/article/261691-treatment
22)
23)
24)
25)
26)
27)
28)
29)
30)
Class Room Recurrent pregnancy loss - Obstetric Anti - Phospholipid Syndrome
ECG discussion
The ECG shows a intermittent CHB with ventricular paced rhythm - Bipolar VVI pacemaker. Ventricular rate 90/mt. Sinus capture beats(4th, 6th and 8th QRS complexes) seen. The P wave preceding the capture beat is fused with the preceding T wave. The pause following the capture beat is long signifying ventricular sensing and appropriate inhibition by the pacemaker, thus ruling out pacemaker dysfunction. The pacemaker was checked and found that the rate was set at 90/mt. It was readjusted to 70/mt, following which patient symptoms improved.
- Dr.M.Chokkalingam, Consultant Cardiologist, CSSH
Answer to : Diagnose the Condition
163

Chettinad Health City Medical Journal
Heritage Museum At IOG (Gifford Museum)From The Pages of History
Famida AM*
*Professor, Department of Obstetrics and Gynecology, Chettinad Hospital & Research Institute, Chennai, India
Corresponding author - Famida AM - ( [email protected])
Chettinad Health City Medical Journal 2017; 5(3): 164
164
Many museums have artistic paintings, jewels and old weapons. Here is the museum which has ancient specimens and surgical instruments and such a museum is at the Institute of Obstetrics and Gynecology (Gifford School Museum).
The Gifford school museum is situated at Institute of Obstetrics and Gynecology at E gmore. This Government maternity hospital was started near Egmore railway station in 1844 and it was later shifted to this location. The new hospital started in 1881 and the architecture was so interesting as it was shaped like a female pelvis. All the work was done under the guidance of GG Gifford and the museum is in a block named after him.1 Few years later major expansion took place and all old buildings were converted into various blocks, however this old block was left untouched-Gifford school was established in 1911 and here is one of the oldest museums in India, which actually became custodian to the heritage building itself. It is considered as a special and sacred space - where specimens were kept over a century and half intact for generations to see and learn from (Fig 1). Gifford school has three main portions. The front portion is the lobby which leads to the museum, the rear portion houses an auditorium with a gallery type class room(Fig 2), where we take tutorial classes for undergraduate students even today and is also used for conducting examinations.
In 2010, when Dr. Radhabai Prabhu took over as Director, when she was remounting the specimens, she stumbled across large boxes kept in a small room under gallery class. Surprisingly, the boxes revealed weird looking instruments (Fig 3) in large numbers. It was very difficult to identify the instruments. She made extensive internet search and she was able to identify some of the instruments and still most of the instruments could not be labelled.2,3 Today,
Volume 5, Number 3
Fig 2 : Classroom(gallery type)
Fig 3 : Instruments at Gifford school
Fig 4 : Display at the museum
www.sid_thewanderer.com/2016/07/museum-of-chennai-gifford-school-iog.html.
www.mmc.tn.gov.in/Department/IOG/ins_IOG.html.
https://sriramv.wordpress.com/government_hospital-for-women-and-children-egmore.
References
1)
2)
3)
the museum possesses around 200 ancient Obstetrics & Gynecology instruments from 16th century and around 200 rare specimens (Fig 4). This Gifford school is a ‘Heritage Site’, as declared by the heritage conserva-tion committee. I had a great opportunity to visit the museum when Dr. Radhabai Prabhu invited us. I wish all medical students and medical fraternity could visit this place.
Fig 1 : Rare Pathology specimens

Chettinad Health City Medical Journal
Interview with – Prof. Sir Sabaratnam ArulkumaranInterview with Stalwart
*Vasantha N Subbiah, ** Vijayalakshmi K
*Professor and HOD, **Professor, Department of Obstetrics and Gynaecology, Chettinad Hospital And Research Institute.
Chettinad Health City Medical Journal 2017; 5(3): 165 - 166
Sir, how did you feel, when you had to leave Srilanka , where you grew up and your father was in a prominent position as Director of Jaffna Cooperative Society, to go to Singapore ?
It was a difficult decision to leave. I had a desire to do academic obstetrics and gynecology. I could not get an academic position in Sri Lanka as there were only three medical schools in the country at that time. Singapore offered that possibility and hence I left.
Sir, who has been the best influence in your life?
My parents – my father supported my enthusiasm to do my best and my mother moulded my character. After marriage – my wife Gayathri gave me the freedom to pursue my academic pursuits and looked after our family well.
Sir, what inspired you to do your Masters in Obs and Gyn even after you had completed your Diploma in Child Health from the University of Ceylon?
I liked Pediatrics and Obstetrics and Gynecology. The children suffering from illness created emotional stress to me and the possibility of doing surgery enticed me to do Obs & Gyn.
Sir, during your tenure as President of FIGO what were the challenges you faced with regard to Women”s health issues in the third world countries?
There were many but the most urgent need was to prevent innocent mothers dying for want of resources and skilled care that does not cost much. My three areas of focus were contraception, provision of safe abortion and emergency obstetric care especially management of PPH.
Sir, what do you perceive as your greatest achievement till date in your Professional life?
Being academic clinician alone does not change policies. Policies and their implementation is best
Professor Sir Sabaratnam Arulkumaran is a world renowned Obstetrician and Gynaecologist of Srilan-kan Tamil descent who has served as President of the world’s highest organization for Obstetrics and Gynaecology speciality , the International Federation of Gynaecology and Obstetrics (FIGO ) from 2002 to 2006. Sir S Arulkumaran graduated with an honours MBBS degree from the University of Ceylon in 1968. He went on to obtain his MD and Phd degrees from the National University of Singapore. After a stint of 15 years in Singapore he moved to the United Kingdom in 1997. He
was professor and head of the OBGYN department at St. George’s University of London from 2001 -2013. He held various positions at the FIGO , like treasurer, Secretary – General before going on become its President. He has held several prestigious positions such as President of the Royal College of Obstetricians and Gynaecologists (2007-2010) and president of the British Medical Association (2013-2014). He is an honorary fellow of various colleges of Obstetricians and Gynaecologists like ACOG, RANZCOG, FOGSI, SASOG, SLCOG, SOGOC to name a few. He has a keen interest in Research and academics. Sir Arulkumaran has been editor in chief of ”Best Practices and Research in Clinical Obstetrics and Gynaecology“ since 1998.
Volume 5, Number 3
1)
2)
3)
done through Professional organizations. Hence my greatest achievement was to become President of the Royal College of O&G, British Medical Association and FIGO that enabled me to work with like-minded colleagues to improve delivery of health care.
Sir, the FIGO and various national federations of Obs&Gynae, are we on the right track in tackling maternal mortality?
Yes - we are in the right track – In 2015 we recognized that Globally we did not reach 75% reduction but we achieved about 50% reduction. If we pursue our effort we can achieve considerable reduction.
Sir, please describe your feelings when you were conferred Knighthood by Her Majesty the Queen!
It was a magnificent feeling – being recognized for my services to medicine and health care.
Sir, you have written and published many books and papers. Which aspect of Obstetrics is closest to your heart?
My main interest is high risk obstetrics and intrapartum care – I worked and researched mainly in intrapartum care as this area of work if well done would reduce the number of maternal and neonatal morbidity and mortality.
Sir, what are the key areas of research that we as Obstetricians and Gynecologists must focus upon?
All areas of obstetrics and gynecology are important. The key areas of research should be on those that affects more women and the areas that may have an impact on future health. In Obstetrics pre-eclampsia, preterm labor and intrauterinegrowth restriction and in Gynecology reproductive tract malignancies especially cervical cancer, subfertility and care of the aging population.
5)
6)
7)
8)
4)
9)
165

Interview Interview with Stalwart – Professor Sir Sabaratnam Arulkumaran Volume 5, Number 3
Sir, on a personal note, have you been able to spend quality time with your family?
My frank answer is not enough time – there are so many hours in a day and the more you do in one area you sacrifice other pleasures. What-ever time we spent together was pleasant and I am grateful to God for giving me an understanding family.
10) Sir, what advice would you like to give post graduates and young consultants throughout the world who are following your footsteps and your writings (books).
Be committed, compassionate, communicate well, have confidence by having the knowledge and skills needed, be a leader and team player and have patient’s need as first and self needs as secondary.
11)
166

-----------------------------------------------
-----------------------------------------------
-----------------------------------------------
Organized by Department of Andrology & Reproductive Medicine
Chettinad International Fertility Colloquium, 2016on
Male and Female Reproduction - 25.09.2016
Organized by Department of Psychiatry
CHETPSYCON - 2016 “Essentials in General Hospital Psychiatry” - 28.09.2016
Organized by Anaesthesiology & Critical Care
CHETANCON 2016 Commemorating "World Anaesthesia Day" - 15.10.2016

Chettinad Academy of Research & EducationCourses Offered 2017 - 18
I. Under Graduate CoursesM.B.B.S. (4 ½ years + 1 year internship)
B.Sc. (Allied Health Sciences) (3 years +1 year internship)
B.Sc. (Medical Bionanotechnology) (3 Years)
B.Sc. (Medical Biotechnology) (3 Years)
B.Sc. (Medical Genetics) (3 Years)
II. Post Graduate CoursesMedical Post Graduate Courses - M.D. Pre and Para Clinical (3 years)
M.D. (Anatomy)
M.D. (Physiology)
M.D. (Biochemistry)
M.D. (Pathology)
M.D. (Microbiology)
M.D. (Pharmacology)
M.D. (Community Medicine)
Medical Post Graduate Courses - M.D./M.S. Clinical Courses (3 years)
M.D. (General Medicine)
M.D. (Anesthesiology)
M.D. (Dermatology, Venerology and Leprosy)
M.D. (Respiratory Medicine)
M.S. (Orthopedics)
M.S. (Ophthalmology)
M.D. (Paediatrics)
M.D. (Psychiatry)
M.D. (Radio-diagnosis)
M.S. (Otorhinolaryngology)
M.S. (General Surgery)
M.S. (Obstetrics and Gynecology)
Post Graduate Courses (2 years)
M.Sc. (Tissue Engineering & Regenerative Medicine)
M.Sc. (Medical Genetics & Molecular Diagnostics)
M.Sc. (Medical Bionanotechnology)
M.Sc. (Medical Biotechnology)
M.Sc. (Clinical Research & Experimental Medicine)
M.Sc. (Marine Pharmacology)
M.Sc. (Human Nutrition)
M.Sc. (Occupational Health & Industrial Safety)
M.Sc. (Health & Yoga)
M.Sc. (Computational Biology)
M.Sc. (Bioinformatics)
M.Sc. (Counseling Psychology)
M.Sc. (Pharamaceutical Chemistry)
Post Graduate - Super Speciality Courses D.M. / M.Ch Courses (3 years)
D.M. (Cardiology)
D.M. (Neurology)
D.M. (Neonatology)
D.M. (Gastroenterology)
M.Ch. (Cardio Vascular & Thoracic Surgery)
M.Ch. (Neuro Surgery)
M.Ch. (Urology)
M.Sc. - (Allied Health Sciences) (2 years)
1. (Echocardiography & Cardiovascular Imaging Technology)
2. (Radiology and Imaging Science Technology)
Post Graduate Courses in Nursing (2 years)
M.Sc. Medical Surgical Nursing - (Cardio Vascular and
Thoracic Nursing)
III. POSTGRADUATE DIPLOMA COURSESPostgraduate Diploma in Clinical Embryology (1 year)
IV. NURSING COURSESB.Sc. (Nursing) (4 years)
Post Basic B.Sc Nursing (2 years)
V. Ph.D Program(1) Ph.D CARE Fellowship (JRF) Full time &
Part time Ph.D. Under the Faculty of Medicine,
Nursing & Allied Health Sciences.
(2) Post Doctoral Fellowship

![ROLL NO APP NAME DOB TICK NO SUBC DTOFDME … · 8202500639 MANIGANDAN G S 04051989 8000388 8201001 16.07.2012 7.00 A.M. Group Centre CRPFAvadiChennai-600065[Board-1] 8202500642 VINOTH](https://img.pdfslide.us/doc/110x75/5f7299b3a9e9e64c001b739b/roll-no-app-name-dob-tick-no-subc-dtofdme-8202500639-manigandan-g-s-04051989-8000388.jpg)



























