Embed Size (px)
Citation preview
1150
Chemotherapy-Induced Neutropenia and Fever inPatients with Metastatic Breast Carcinoma ReceivingSalvage Chemotherapy
BACKGROUND. Chemotherapy-induced neutropenia and associated fever and in-Zia Rahman, M.D.
fection are the most common complications of systemic chemotherapy. In thisLaura Esparza-Guerra, R.N.retrospective analysis, the authors evaluated the incidence of neutropenic fever,Hwee-Yong Yap, M.D.infection, and mortality in relation to the level of neutropenia, performance status,Giuseppe Fraschini, M.D.course number of chemotherapy, bone marrow metastasis, and age among patientsGerald Bodey, M.D.with metastatic breast carcinoma receiving salvage chemotherapy.Gabriel Hortobagyi, M.D.METHODS. A total of 174 patients with previously treated metastatic breast carci-
noma enrolled on 4 consecutive Phase II protocols were evaluated.Department of Breast Medical Oncology, Divi-
RESULTS. Twenty-three percent of the patients had an episode of neutropenicsion of Medicine, The University of Texas M. D.fever (41 episodes among 40 patients). The incidence of neutropenic fever did notAnderson Cancer Center, Houston, Texas.increase until the absolute neutrophil count (ANC) had decreased to less than 500/
mL, and then fever incidence had a linear relationship with decreasing ANC (linear
trend, P õ 0.01). A source of infection was documented in 59% of the neutropenic
fever episodes. The incidence of infection did not increase significantly until the
ANC had decreased to less than 250/mL (P õ 0.01). The risk of neutropenic fever
and infection was also significantly higher when patients had poor performance
status or were undergoing the initial courses of chemotherapy. Patients with bone
marrow metastases also had a higher frequency of fever, infection, and death, but
these differences were not statistically significant.
CONCLUSIONS. For patients with metastatic breast carcinoma receiving salvage
chemotherapy, the risk of fever increases with decreasing ANC, but the risk of
infection does not increase significantly until ANC decreases to less than 250/
mL. Poor performance status, initial courses of chemotherapy, and bone marrow
metastases further increase the risk of fever, infection, and death. Cancer
1997;79:1150–7. q 1997 American Cancer Society.
KEYWORDS: neutropenic fever, breast carcinoma, drug therapy, complications.
In North America, breast carcinoma is the most common malignancyamong women, accounting for 32% of their cancers.1 In 1995, there
were estimated to be approximately 183,400 new cases and 46,240deaths from breast carcinoma in the United States.1 Almost all deathsPresented in part at the 1983 Annual Meetingare from metastatic or recurrent disease, and the current standardof the American Society of Clinical Oncology,
San Diego, California. treatment for hormone receptor-negative and hormone-resistantmetastatic breast carcinoma consists of systemic cytotoxic chemo-
Address for reprints: Zia Rahman, M.D., The therapy.University of Texas M. D. Anderson Cancer Cen- Myelosuppression, especially neutropenia, is one of the most fre-ter, 1515 Holcombe Blvd., Box 56, Houston, TX
quently encountered complications of chemotherapy. The relation-77030.ship between infections and neutropenia was first described about30 years ago in patients with acute leukemia receiving chemotherapy.2
Received July 29, 1996; revision received No-vember 20, 1996; accepted November 20, 1996. Since then, considerable progress has been made in the management
q 1997 American Cancer Society
/ 7b50$$0950 02-24-97 16:16:12 cana W: Cancer

Neutropenic Fever in Breast Carcinoma Patients/Rahman et al. 1151
of fever and infection in neutropenic patients.3 Em- trials conducted by the Department of Breast MedicalOncology of The University of Texas M. D. Andersonpiric broad-spectrum antibiotic therapy has been the
cornerstone of the management of fever in patients Cancer Center were reviewed. These trials utilized sin-gle-agent etoposide, teniposide, mitoxantrone, or bi-with chemotherapy-induced neutropenia.3–8
It is widely appreciated that patients with solid santrene. All patients had measurable or evaluablemetastatic breast carcinoma; and for all of them, priortumors are not as severely immunocompromised as
are patients with hematologic malignancies. Unfortu- front-line therapies, including at least one doxorubi-cin-containing regimen, were ineffective.nately, there have been very few studies evaluating the
significance of chemotherapy-induced neutropenia Patients had complete blood cell counts (CBCs),including differential counts, performed at leastand the associated risk of fever and infection for pa-
tients with solid tumors.9,10 Almost all reported studies weekly. For the purposes of this study, neutropeniawas defined as an ANCõ1000/mL. The ANC was calcu-of chemotherapy-induced neutropenia with fever have
been in patients with hematologic malignancies and lated by multiplying the white blood cell count by thepercentage of neutrophils and bands. The ANCs wererecipients of bone marrow transplants.4,11–14 The prin-
ciples developed for managing disease in these pa- grouped in the following ranges of cells/mL: fewer than100, 100–249, 250–499, 500–999, 1000–1999, andtients have been applied to the management of che-
motherapy-induced neutropenia and fever in patients 2000. Fever was defined as oral temperature greaterthan 38.57 C.with solid tumors.
Most metastatic solid tumors are not curable with All patients had a physical examination, CBC, se-rum electrolyte measurements, hepatic and renalchemotherapy. The main objectives of chemotherapy
in this setting are to palliate symptoms and prolong function tests, chest roentgenogram, and other appro-priate radiologic tests to evaluate measurable diseasesurvival. In this setting, physicians try to avoid exces-
sive risk of complications in their patients. One of the prior to the start of therapy. Patients who had anypersistent abnormality of the hematologic parametersmost common side effects of chemotherapy is myelo-
suppression, and increased risk of fever and infections also had bone marrow aspiration and biopsy to evalu-ate involvement with the metastatic breast carcinoma.associated with it. It has become the general practice
to reduce doses of myelosuppressive drugs for the next Other patients were not required to have bone marrowevaluation. The performance status was recorded ac-cycle for patients who develop chemotherapy-induced
neutropenia. Growth factors are increasingly being cording to Zubrod’s scale.18 All CBCs and differentialcounts were obtained from the patients’ medical re-used to prevent neutropenia and associated infectious
complications.15–17 Both of these measures are taken cords. Patients who presented with fever underwent acomplete physical examination and laboratory tests,in the absence of accurate information about the risk
of complications associated with chemotherapy-in- including CBC with differential count, serum electro-lyte measurements, hepatic and renal function tests,duced neutropenia for patients with solid tumors re-
ceiving palliative chemotherapy. and chest roentgenogram. At least two sets of bloodcultures (one from the vascular access device and theWhat predicts poor outcome and increased mor-
bidity of chemotherapy-induced neutropenia? This is other from a peripheral vein) and a urine culture wereobtained. If there was another evident source of infec-an important consideration in the palliative setting,
where quality of life is of paramount importance. This tion, then additional appropriate cultures were ob-tained. Patients were admitted to the hospital andquestion becomes even more critical for patients re-
ceiving second-line chemotherapy because of the cu- treated with broad-spectrum intravenous antibiotics.If all cultures were reported negative, patients contin-mulative toxicity of prior chemotherapy. In this study,
we retrospectively analyzed the relationship between ued intravenous antibiotics for a minimum of 1 weekor for 4 days after defervescence, whichever periodthe degree of neutropenia and fever with and without
infection in patients with metastatic breast carcinoma was shorter. Patients were considered to have a sourceof infection if in an appropriate clinical setting theyreceiving standard dose salvage chemotherapy. We
also evaluated the association of these complications had positive cultures, a new infiltrate on chest radio-graphs, or evidence of skin or oropharyngeal infection.with absolute neutrophil count (ANC), bone marrow
involvement with metastatic disease, course number Patients with documented infections were continuedon an appropriate course of antibiotics.of chemotherapy, performance status, and age.
The statistical analysis for correlation of ANC, fe-ver, and infectious complications with prognostic pa-MATERIALS AND METHODS
The medical records of all patients with metastatic rameters, i.e., age, performance status, the presence ofbone marrow involvement, and chemotherapy coursebreast carcinoma enrolled in four consecutive Phase II
/ 7b50$$0950 02-24-97 16:16:12 cana W: Cancer
1152 CANCER March 15, 1997 / Volume 79 / Number 6
TABLE 1Patient Characteristics
No. of patients 174Total no. of courses 610Total evaluable courses 455Median age, yrs (range) 54 (29–74)Median performance status on Zubrod’s scale (range) 1 (0–3)Median no. of mos of prior chemotherapy 27
number, was performed with Sigmastat statistical soft-ware (Jandel Corporation, San Rafael, CA) using thechi-square test and the z-test.
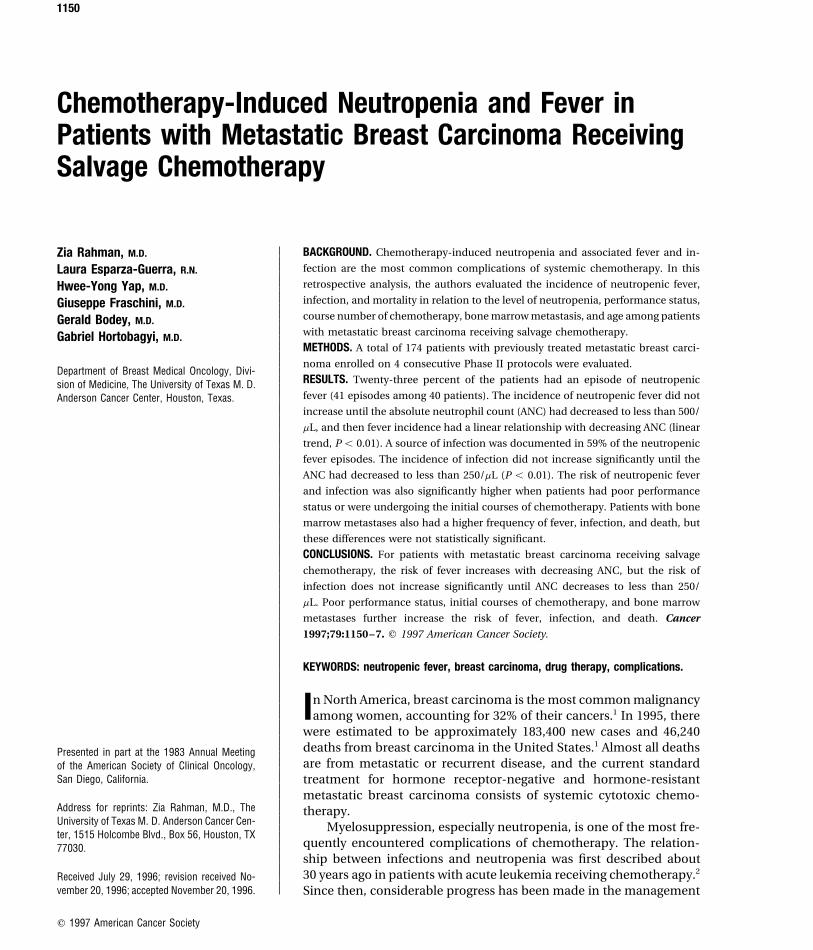
RESULTSA total of 174 patients with metastatic breast carci-noma received a total of 610 courses of chemotherapyin these 4 consecutive Phase II trials (Table 1). Themedian number of courses was 3 (range, 1–17), andthe median age was 54 years (range, 29–74 years). For455 courses of chemotherapy, CBCs with differentialcounts, obtained at least weekly, were available. Only
FIGURE 1. The relationship between absolute neutrophil count (ANC)these 455 courses were evaluated for the relationship
and neutropenic fever after salvage chemotherapy is shown for patientsbetween ANC, fever with or without documented in-
with metastatic breast carcinoma. When the ANC decreases to a levelfection, course number of chemotherapy, bone mar-
below the threshold of 500/mL, the incidence of neutropenic fever increasesrow involvement by the tumor, performance status,
in a linear trend (P õ 0.01). *:Number of courses with fever/number ofand age.
courses with nadir ANC in the same range.
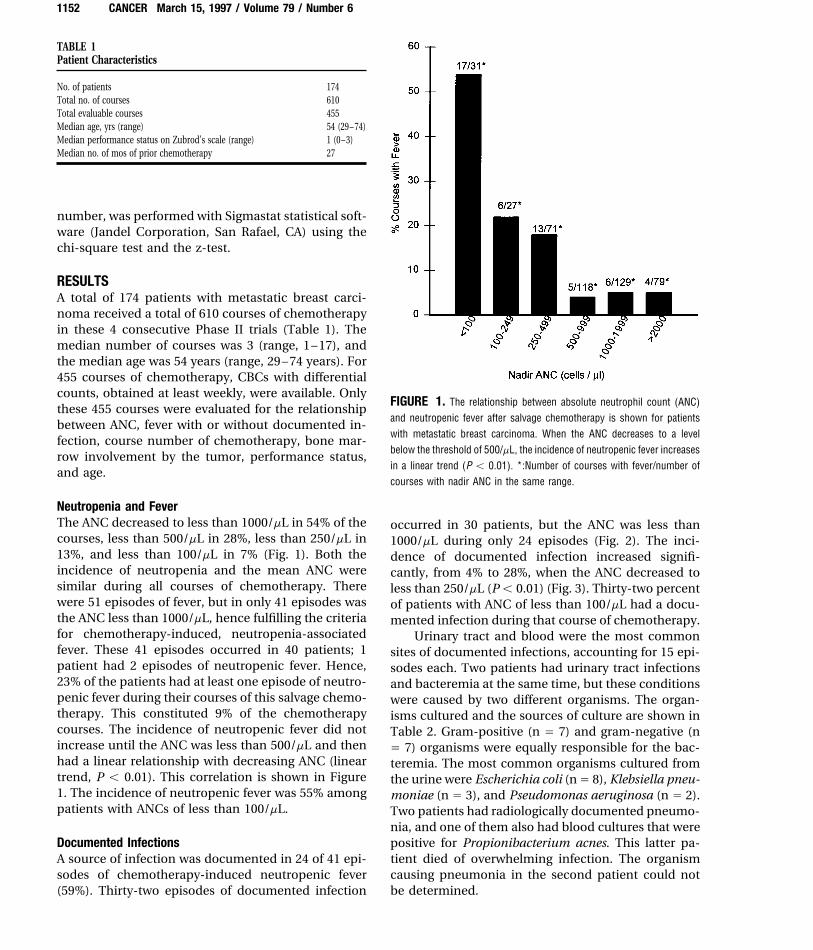
Neutropenia and FeverThe ANC decreased to less than 1000/mL in 54% of the occurred in 30 patients, but the ANC was less thancourses, less than 500/mL in 28%, less than 250/mL in 1000/mL during only 24 episodes (Fig. 2). The inci-13%, and less than 100/mL in 7% (Fig. 1). Both the dence of documented infection increased signifi-incidence of neutropenia and the mean ANC were cantly, from 4% to 28%, when the ANC decreased tosimilar during all courses of chemotherapy. There less than 250/mL (Põ 0.01) (Fig. 3). Thirty-two percentwere 51 episodes of fever, but in only 41 episodes was of patients with ANC of less than 100/mL had a docu-the ANC less than 1000/mL, hence fulfilling the criteria mented infection during that course of chemotherapy.for chemotherapy-induced, neutropenia-associated Urinary tract and blood were the most commonfever. These 41 episodes occurred in 40 patients; 1 sites of documented infections, accounting for 15 epi-patient had 2 episodes of neutropenic fever. Hence, sodes each. Two patients had urinary tract infections23% of the patients had at least one episode of neutro- and bacteremia at the same time, but these conditionspenic fever during their courses of this salvage chemo- were caused by two different organisms. The organ-therapy. This constituted 9% of the chemotherapy isms cultured and the sources of culture are shown incourses. The incidence of neutropenic fever did not Table 2. Gram-positive (n Å 7) and gram-negative (nincrease until the ANC was less than 500/mL and then Å 7) organisms were equally responsible for the bac-had a linear relationship with decreasing ANC (linear teremia. The most common organisms cultured fromtrend, P õ 0.01). This correlation is shown in Figure the urine were Escherichia coli (nÅ 8), Klebsiella pneu-1. The incidence of neutropenic fever was 55% among moniae (n Å 3), and Pseudomonas aeruginosa (n Å 2).patients with ANCs of less than 100/mL. Two patients had radiologically documented pneumo-
nia, and one of them also had blood cultures that werepositive for Propionibacterium acnes. This latter pa-Documented Infections
A source of infection was documented in 24 of 41 epi- tient died of overwhelming infection. The organismcausing pneumonia in the second patient could notsodes of chemotherapy-induced neutropenic fever
(59%). Thirty-two episodes of documented infection be determined.
/ 7b50$$0950 02-24-97 16:16:12 cana W: Cancer
Neutropenic Fever in Breast Carcinoma Patients/Rahman et al. 1153
TABLE 2Organisms Cultured and the Sources of Culture during 32 Episodes ofDocumented Infections in 30 Patients
Sites of infection/organisms No. of casesa
Urinary tract 15Escherichia coli 8Klebsiella pneumoniae 3Pseudomonas aeruginosa 2Morganella morganii 1a-hemolytic streptococcus 1
Blood (bacteremia) 15Staphylococcus
epidermidis 3a-hemolytic streptococcus 3Klebsiella pneumoniae 2Escherichia coli 2Bacillus species 2Propionibacterium acnes 1Streptococcus pneumoniae 1Candida albicans 1
Skin 3Staphylococcus aureus 1Klebsiella pneumoniae 1Pseudomonas 1
Oropharynx 1FIGURE 2. The relationship between absolute neutrophil count (ANC) Candida albicans 1and infection after salvage chemotherapy is shown for patients with meta-
a Two patients had urinary tract infections and bacteremia at the same time from different organisms,static breast carcinoma. There is a significant increase in the incidence ofand two patients each had two episodes of documented infections.infection when the ANC decreases to less than 250/mL (P õ 0.01). *:
Number of courses with documented infection/number of courses withnadir ANC in the same range.
Course Number of ChemotherapyThe frequency of fever and infection was highest dur-ing the initial three courses of chemotherapy. Therewere 19 episodes of chemotherapy-induced, neutro-penia-associated fever during the first course, 12 dur-ing the second, and 5 during the third (Fig. 3)(Table3). With each course of chemotherapy, the percentageof patients who developed neutropenia decreasedslightly and median ANC increased slightly, while theincidence of fever and infection decreased dramati-cally more (Fig. 3). The total number of patients de-creased with each successive course; the patients withprogressive disease or unacceptable toxicity were re-moved from the study (Fig. 3).
DeathsFour patients (2%) died of documented infections. Allfour had an ANC of less than 100/mL and positiveblood cultures on admission. Two patients had multi-ple-organism septicemia documented by blood andcatheter tip cultures, one patient had septicemia andradiologically documented pneumonia, and the fourth
FIGURE 3. The relationship between the course number of chemother- patient had septicemia and a urinary tract infectionapy and the incidence of neutropenia, fever, and infection is shown for caused by two different organisms (Table 4). All pa-patients with metastatic breast carcinoma receiving salvage chemotherapy. tients had advanced disease with extensive visceral
/ 7b50$$0950 02-24-97 16:16:12 cana W: Cancer
1154 CANCER March 15, 1997 / Volume 79 / Number 6
TABLE 3Details of Myelosuppression and Associated Fever and Infection by Course Number of Chemotherapy
Course no.
1 2 3 4
No. of patients 143 107 62 46Median ANC/mL 792 783 909 972No. (%) of patients with neutropenia 85 (60) 62 (58) 36 (58) 24 (53)No. (%) of neutropenic patients with:
fever 19 (22) 12 (19) 5 (14) 1 (4)Documented infection 13 (15) 7 (11) 3 (8) 1 (4)
ANC: absolute neutrophil count.
TABLE 4Course Number of Chemotherapy, Bone Marrow Metastasis, Site of Infection, and Organisms Cultured for the Four Patients with MetastaticBreast Carcinoma Who Died during Chemotherapy
Patient Course Bone marrowno. no. metastasis Type of infection Organisms cultured
1 1 No Septicemia Staphylococcus aureus, Bacillus species2 1 No Septicemia Propionibacterium acnes
Pneumonia3 2 Yes Septicemia Escherichia coli, Staphylococcus epidermidis4 4 Yes Septicemia Candida albicans
Urinary tract infection Escherichia coli
TABLE 5metastases and had previously been treated with threeAssociation among Performance Status, Neutropenic Fever, andto six chemotherapy regimens for metastatic disease.Documented InfectionTwo patients had bone marrow involvement with met-
astatic disease. Two patients died during the first che- Performance statusa
motherapy course, one died during the second course,0 or 1 2 or 3and one died during the fourth course.
No. of patients 80 94Performance StatusNo. of cycles 247 208
There was a statistically significant association be- Neutropenic fever 11 (13.8%)b 30 (31.9)b
tween poor performance status and both episodes of With infection 5 (6.2%)c 19 (20.2%)c
Without infection 6 (7.5%) 11 (11.7%)chemotherapy-induced neutropenic fever and docu-mented infections (P õ 0.008 and P õ 0.014, respec-
a Performance status was measured on Zubrod’s scale.tively) (Table 5). The rates of chemotherapy-induced, b P õ 0.008.neutropenia-associated fever and documented infec- c P õ 0.014.tion were approximately 14% and 6%, respectively,among the 80 patients with good performance status(0 or 1 on Zubrod’s scale) and approximately 32% and20%, respectively, among the 94 patients with poor tases received 77 courses of chemotherapy and had
11 episodes of neutropenic fever and 7 episodes ofperformance status (2 or 3 on Zubrod’s scale).documented infection. Two of the patients withknown bone marrow metastases and documented in-Bone Marrow Involvement
Thirty patients had documented bone marrow fections died. There was an increased frequency ofneutropenic fever, infection, and septic death in pa-involvement with metastatic breast carcinoma, and
the other 144 patients did not have bone marrow eval- tients with known bone marrow metastases, comparedwith patients whose bone marrow status was unknownuation. The patients with known bone marrow metas-
/ 7b50$$0950 02-24-97 16:16:12 cana W: Cancer

Neutropenic Fever in Breast Carcinoma Patients/Rahman et al. 1155
TABLE 6Association between Age and Neutropenic Fever with and without Infection
Neutropenic feverNo. of
Age group patients Without infection With infection Total no. (%)
õ50 yrs 71 6 11 17 (24%)50–65 yrs 80 10 12 22 (27.5%)ú65 yrs 23 2 1 3 (13%)
(fever, 37% vs. 21%; infection, 24% vs. 12%; septic ANC level, the frequency of infection was higher inpatients with active acute leukemia than in patientsdeath, 7% vs. 1%). These differences were not statisti-
cally significant. The patients with bone marrow me- in remission. A much smaller number of neutrophilsin breast carcinoma patients than in patients with leu-tastases also had a higher probability of developing
neutropenia and lower median ANCs than patients kemia seems to protect patients against spontaneousinfections. The total number of neutrophils is im-with unknown bone marrow status; these differences
also were not statistically significant. portant in preventing spontaneous infections, but it isapparent that some other factor or factors, yet unde-termined, also play an important role in preventingAge
There was no association between age and chemother- these infections. Whether it is abnormal intrinsic neu-trophil function in patients with leukemia or alteredapy-induced, neutropenia-associated fever and infec-
tion. The incidence of chemotherapy-induced, neutro- cytokine production needs to be determined. Pizzoet al. reported a large prospective series of pediatricpenia-associated fever was 24% in the 71 patients
younger than 50 years, approximately 27% in the 80 patients with cancer who presented with fever.19 Therewas no difference in the patients with hematologicpatients age 50–65 years, and 13% in the 23 patients
older than 65 years. The number of documented infec- malignancies or solid tumors with respect to the typesof infection or the percentage of patients who weretions is shown in Table 6. These numbers were too
small for definitive conclusions to be drawn. neutropenic on presentation.19 The authors did notevaluate whether the relationships between ANC andinfections in these two groups of patients were similarDISCUSSION
This is the first report to evaluate chemotherapy-in- or not.In this study, a source of infection was docu-duced neutropenia and its associated fever and infec-
tion in patients with metastatic breast carcinoma re- mented in 59% of the chemotherapy-induced, neutro-penia-associated fever episodes. The most commonceiving chemotherapy. Patients with metastatic breast
carcinoma routinely receive multiple regimens of pal- types of infection identified were septicemia and uri-nary tract infection. Nobbenhuis and Cleton reportedliative chemotherapy, and there is cumulative myelo-
suppression with each subsequent chemotherapy regi- on 90 patients with solid tumors who received chemo-therapy on European Organization for Research andmen. A substantial proportion of patients become
neutropenic and are exposed to increased risk of fever, Treatment of Cancer protocols.10 A source of infectionwas documented in a similar proportion of chemo-infection, and death.
Among the patients with metastatic breast carci- therapy-induced, neutropenia-associated fever epi-sodes (33 of 51). The common sites of documentednoma in this study, there was an inverse relationship
between ANC and fever with and without infection, infection were also the blood and the urinary tract.Pizzo et al also reported a similar percentage (52%) ofas previously shown by Bodey et al., in patients with
leukemia.2 The incidence of fever seems to have a documentation of the source of infection in patientswith neutropenic fever.19 Curtin et al. reported 56 epi-threshold and did not increase until the ANC de-
creased to less than 500/mL (Fig. 1). The incidence of sodes of chemotherapy-induced, neutropenia-associ-ated fever in 43 patients with ovarian carcinoma whoinfection did not significantly increase until the ANC
decreased to less than 250/mL (Fig. 2). This is different received platinum-based chemotherapy.9 In 12 of the56 episodes (21%), septicemia was documented byfrom the observation in patients with leukemia, in
whom the risk of infection increases significantly when positive blood cultures. The exact incidence of infec-tion at other sites was not reported.the ANC decreases to less than 1000/mL.2 Bodey et al.,
in their original article, also reported that for any given It has been an anecdotal clinical experience that
/ 7b50$$0950 02-24-97 16:16:12 cana W: Cancer

1156 CANCER March 15, 1997 / Volume 79 / Number 6
the risk of neutropenic fever and infection is highest also been shown to result in lower response ratesand survival.20 Patients with bone marrow involve-during the initial courses of chemotherapy. This
study is the first documentation of this clinical ob- ment should be treated with full doses in those cen-ters where aggressive supportive measures are easilyservation. The most noteworthy finding was that this
risk did not correlate with the percentage of the pa- available, or doses should be reduced in the initialcourses (when the rate of fever and infection is high-tients developing neutropenia or with the median
ANC (Fig. 3). The patients who developed neutro- est) and then rapidly escalated to full doses.In a study of more than 5000 patients enteredpenic fever or infection had dose reduction in the
next cycle, but that did not change the myelosup- into the Veterans Administration Lung Group proto-cols, performance status at the start of therapy waspression profile of the entire population at risk, and
very similar percentages of patients in each cycle shown to be the most important prognostic factorfor survival.21 Poor performance status has been as-developed neutropenia (Fig. 3). This could be due
to cumulative myelotoxicity in the entire group com- sociated with increased risk of complications andpoor survival in a number of other tumor types.22–24pensating for any reduced myelosuppression
achieved by the dose reduction in some patients. In this study, poor performance status was also associ-ated with increased risk of neutropenic fever and in-Why more patients develop neutropenic fever dur-
ing the first course of chemotherapy is not known. fection (Table 5).The older patients had the same risk of chemo-One possible explanation is that some patients are
intrinsically at higher risk for developing neutro- therapy-induced neutropenia, fever, and infection asthe younger patients (Table 6). Ibrahim et al. reportedpenic fever and infection. When they declare them-
selves during the initial courses of chemotherapy, in on the relationship between age and efficacy and tox-icity of doxorubicin-based chemotherapy in patientsthe subsequent courses either the drug doses are
reduced or colony-stimulating factors are adminis- with metastatic breast carcinoma and found that theincidence of neutropenia, infection, response rate,tered to reduce the risk of neutropenic fever and
infection. Another possibility is that some patients time to progression, and survival were similar for pa-tients older than 65 years and patients age 50–65already have a subclinical infection that becomes
evident as a fever or a documented infection with the years.25
With the increasing awareness that patientsonset of neutropenia. When these patients receiveantibiotics, the subclinical infection is eradicated in with solid tumors are not as immunocompromised
as patients with hematologic malignancies, andsome of them. The patients who had progressive dis-ease or excessive toxicity were removed from this with changing medical economics, a large number
of centers are managing ‘‘low risk’’ solid tumor pa-study, and only patients with responding diseasewho tolerated chemotherapy well remained. This se- tients with neutropenic fever in outpatient settings
or discharging them early to continue antibiotics atlection bias is shown by the decrease in the numberof patients with each successive course and might home.6,26 – 30 In these patients, ANC of less than 250/
mL, poor performance status, initial courses of che-also explain increased incidence of fever and infec-tion during initial courses of chemotherapy (Table motherapy, and bone marrow involvement by the
malignancy also signifies increased risk of infection3). The mortality rate was also higher during theinitial courses of chemotherapy. and death and should be taken into account when
decisions are made about outpatient management.Bone marrow involvement by metastatic breastcarcinoma has been reported to be associated withan increased risk of infectious complications.20 In REFERENCESa prior report from the University of Texas M. D. 1. Wingo P, Tong T, Bolden S. Cancer Statistics, 1995. CA Can-
cer J Clin 1995;45:8–30.Anderson Cancer Center, patients with bone marrow2. Bodey GP, Buckley M, Sathe YS, Freireich EJ. Quantitativeinvolvement by metastatic breast carcinoma had a
relationships between circulating leukocytes and infectionhigher incidence of neutropenia and infectious com-in patients with acute leukemia. Ann Intern Med 1966;
plications than did patients without bone marrow 64:328–39.involvement.20 In this report, we also found a higher 3. Pizzo PA. Management of fever in patients with cancer and
treatment-induced neutropenia [review]. N Engl J Medincidence of neutropenia and its associated fever,1993;328:1323–32.infection, and death in patients with bone marrow
4. Smith GM, Leyland MJ, Farrell ID, Geddes AM. A clinical,metastases, although these differences were not sta-microbiological and pharmacokinetic study of ciprofloxacin
tistically significant, probably because of the sample plus vancomycin as initial therapy of febrile episodes insize. Dose reduction in women with bone marrow neutropenic patients. J Antimicrob Chemother 1988;21:647–
55.involvement by metastatic breast carcinoma has
/ 7b50$$0950 02-24-97 16:16:12 cana W: Cancer
Neutropenic Fever in Breast Carcinoma Patients/Rahman et al. 1157
5. Klastersky J. Febrile neutropenia [review]. Curr Opin Oncol mopentin in the prevention of febrile episodes in cancerpatients undergoing highly cytotoxic chemotherapy. Anti-1993;5:625–32.
6. Rubenstein EB, Rolston KV. Outpatient treatment of febrile neu- cancer Res 1994;14:731–4.18. Zubrod CG, Schneiderman M, Frei I, Emil, et al. Appraisaltropenic patients with cancer. Eur J Cancer 1995;31A:2–4.
7. Kojima A, Shinkai T, Soejima Y, et al. A randomized prospec- of methods for the study of chemotherapy of cancer in man:comparative therapeutic trial of nitrogen mustard and tri-tive study of imipenem-cilastatin with or without amikacin
as an empirical antibiotic treatment for febrile neutropenic ethylene thiophosphoramide. Cancer 1960;11:7–33.19. Pizzo PA, Robichaud KJ, Wesley R, Commers JR. Fever inpatients. Am J Clin Oncol 1994;17:400–4.
8. Carlson JW, Fowler JM, Saltzman AK, et al. Chemoprophy- the pediatric and young adult patient with cancer. Medicine1982;61:153–65.laxis with oral ciprofloxacin in ovarian cancer patients re-
ceiving taxol. Gynecol Oncol 1994;55 (Pt 1):415–20. 20. Rodriguez-Kraul R, Hortobagyi GN, Buzdar AU, Blumensch-ein GR. Combination chemotherapy for breast cancer meta-9. Curtin JP, Hoskins WJ, Rubin SC, et al. Chemotherapy-in-
duced neutropenia and fever in patients receiving cisplatin- static to bone marrow. Cancer 1981;48:227–32.21. Stanley KE. Prognostic factors for survival in patients withbased chemotherapy for ovarian malignancy. Gynecol Oncol
1991;40:17–20. inoperable lung cancer. J Natl Cancer Inst 1980;25–32.22. Swenerton KD, Legha SS, Smith T, et al. Prognostic factors10. Nobbenhuis M, Cleton FJ. Febrile neutropenic events in
cancer patients: treatment for fever and neutropenia in in metastatic breast cancer treated with combination che-motherapy. Cancer Res 1979;39:1552–62.young adult patients during intensive chemotherapy for
solid tumours. J Cancer Res Clin Oncol 1992;118:395–9. 23. Blijham G, Wagener T, Wils J, et al. Modulation of high-doseinfusional fluorouracil by low-dose methotrexate in patients11. Engervall PA, Stiernstedt GT, Gunther GC, Bjorkholm MJ.
Trimethoprim-sulfamethoxazole plus amikacin as first-line with advanced or metastatic colorectal cancer: final results ofa randomized European Organization for Research and Treat-therapy and imipenem/cilastatin as second empirical ther-
apy in febrile neutropenic patients with hematological disor- ment of Cancer Study. J Clin Oncol 1996;96;14:2266–73.24. Ringdal GI, Gotestam KG, Kaasa S, Kvinnsland S, Ringdal K.ders. J Chemother 1992;4:99–106.
12. Gruppo Italiano Malattie Ematologiche. Prevention of bacte- Prognostic factors and survival in a heterogeneous sampleof cancer patients. Br J Cancer 1996;96;73:1594–9.rial infection in neutropenic patients with hematologic ma-
lignancies. A randomized, multicenter trial comparing nor- 25. Ibrahim N, Buzdar A, Frye D, Hortobagyi G. Should age bea determinant factor in treating breast cancer patients withfloxacin with ciprofloxacin. The GIMEMA Infection Pro-
gram. Ann Intern Med 1991;115:7–12. combination chemotherapy? [meeting abstract] Proc Am SocClin Oncol 1993;12:A74.13. Balducci L, Halbrook JC, Chapman SW, Vance RB, Thigpen
JT, Morrison FS. Acute leukemia and infections: perspectives 26. Talcott JA, Siegel RD, Finberg R, Goldman L. Risk assessmentin cancer patients with fever and neutropenia: a prospective,from a general hospital. Am J Hematol 1983;15:57–63.
14. Lohner D, Debusscher L, Prevost JM, Klastersky J. Compara- two-center validation of a prediction rule. J Clin Oncol1992;10:316–22.tive randomized study of protected environment plus oral
antibiotics versus oral antibiotics alone in neutropenic pa- 27. Malik IA, Khan WA, Karim M, Aziz Z, Khan MA. Feasibilityof outpatient management of fever in cancer patients withtients. Cancer Treat Rep 1979;63:363–8.
15. Gebbia V, Testa A, Valenza R, et al. A prospective evaluation low-risk neutropenia: results of a prospective randomizedtrial. Am J Med 1995;98:224–31.of the activity of human granulocyte-colony stimulating fac-
tor on the prevention of chemotherapy-related neutropenia 28. Talcott JA, Whalen A, Clark J, Rieker PP, Finberg R. Homeantibiotic therapy for low-risk cancer patients with fever andin patients with advanced carcinoma. J Chemother 1993;
5:186–90. neutropenia: a pilot study of 30 patients based on a validatedprediction rule. J Clin Oncol 1994;12:107–14.16. Mayordomo JI, Rivera F, Diaz-Puente MT, et al. Improving
treatment of chemotherapy-induced neutropenic fever by 29. Rubenstein EB, Rolston K, Benjamin RS, et al. Outpatienttreatment of febrile episodes in low-risk neutropenic pa-administration of colony-stimulating factors. J Natl Cancer
Inst 1995; 87:803–8. tients with cancer. Cancer 1993;71:3640–6.30. Rubenstein EB, Rolston K. Outpatient management of fe-17. Gebbia V, Valenza R, Testa A, Cannata G, Borsellino N, Geb-
bia N. A prospective randomized trial of thymopentin versus brile episodes in neutropenic cancer patients [review]. Sup-port Care Cancer 1994;2:369–73.granulocyte-colony stimulating factor with or without thy-
/ 7b50$$0950 02-24-97 16:16:12 cana W: Cancer






![(filgrastim) - accessdata.fda.gov · severe neutropenia (absolute neutrophil count [ANC] < 500/mm; 3) following chemotherapy were all significantly reduced. The incidence of severe](https://img.pdfslide.us/doc/110x75/5d358ca888c99341768bddf1/filgrastim-severe-neutropenia-absolute-neutrophil-count-anc-500mm.jpg)