Embed Size (px)
Citation preview

:
Chemotherapy and targeted therapies of NSCLC
Rolf Stahel
Comprehensive Cancer Center Zürich
1 |
Berlin, March 23, 2019
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
Disclosures
Consultant or Advisory Role in the last two years
I have received honoraria as a consultant at advisory boards from Abbvie,
AstraZeneca, Boehringer Ingelheim, MSD, Pfizer, Roche and Takeda.
Speaker Honoraria in the last two years
I have received honoraria as a speaker from Astra Zeneca, Boehringer
Ingelheim, Lilly, MSD and Roche.
DMC in the last two years
Roche and Takeda
Financial Support of ETOP trials (president and scientific chair)
AstraZeneca, BMS, Boehringer Ingelheim, Genentech, MSD, Roche, and
Pfizer.
2 |
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
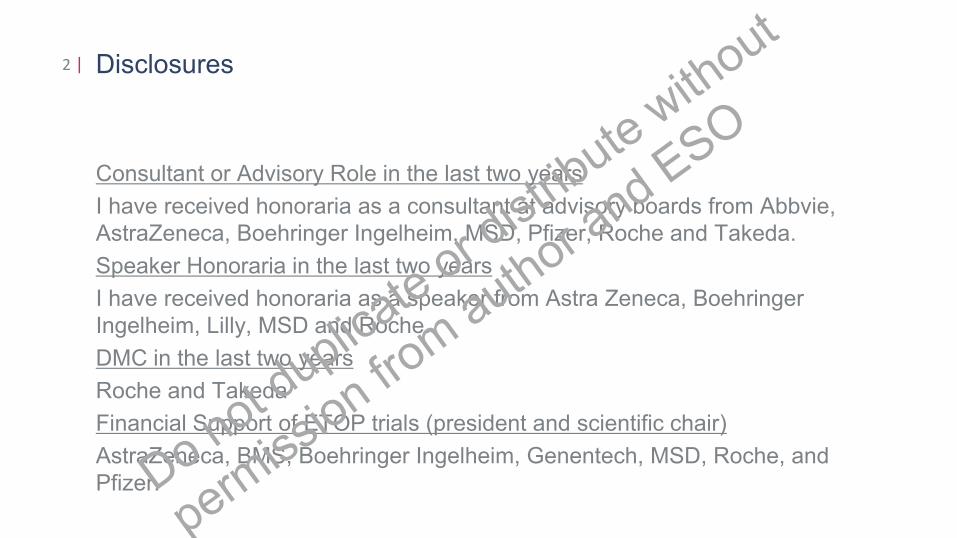
Lynch, Surgery, 27: 268-285, 1950
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
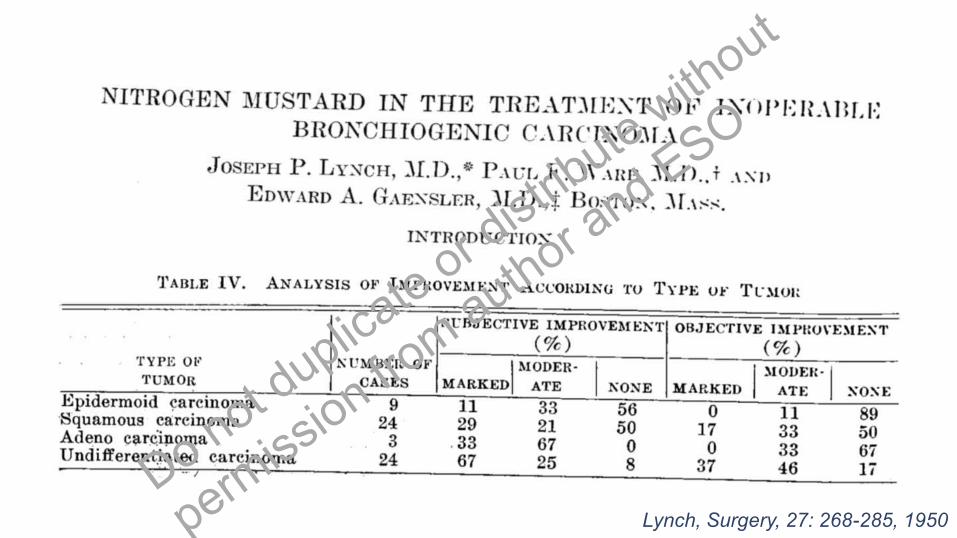
Chemotherapy of NSCLC: a meta-analysis using updated data on
individual patients from 52 randomized trials
4 |
Non-small cell lung cancer collaborative group, BMJ 1995
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
Dabate on the use of chemotherapy in advanced NSCLC5 |
BMJ 1994
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
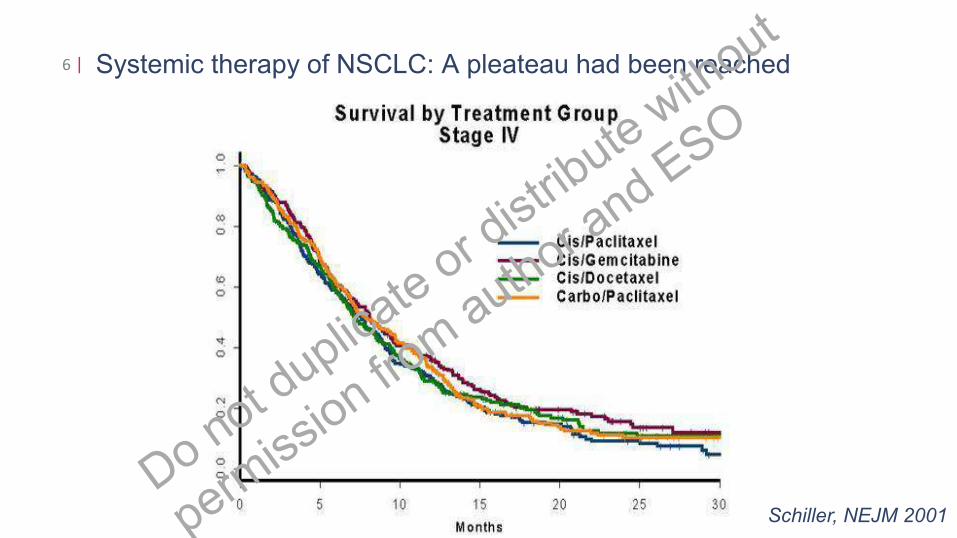
Systemic therapy of NSCLC: A pleateau had been reached6 |
Schiller, NEJM 2001
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
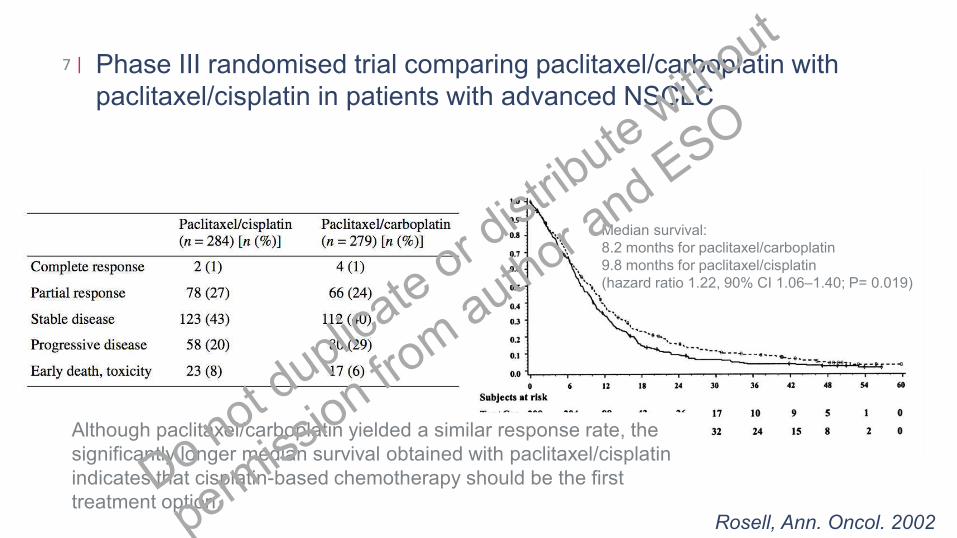
Phase III randomised trial comparing paclitaxel/carboplatin with
paclitaxel/cisplatin in patients with advanced NSCLC
7 |
Rosell, Ann. Oncol. 2002
Although paclitaxel/carboplatin yielded a similar response rate, the
significantly longer median survival obtained with paclitaxel/cisplatin
indicates that cisplatin-based chemotherapy should be the first
treatment option.
Median survival:
8.2 months for paclitaxel/carboplatin
9.8 months for paclitaxel/cisplatin
(hazard ratio 1.22, 90% CI 1.06–1.40; P= 0.019)
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
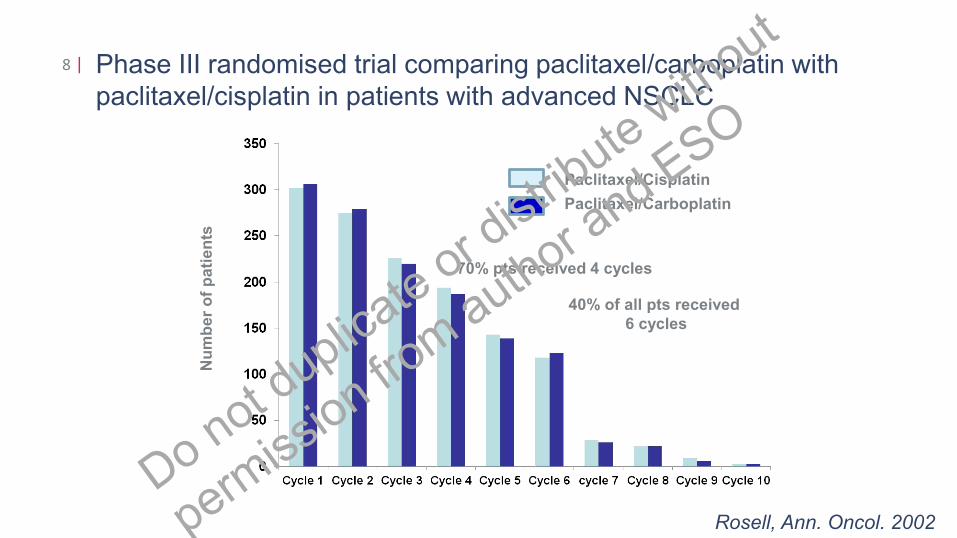
Phase III randomised trial comparing paclitaxel/carboplatin with
paclitaxel/cisplatin in patients with advanced NSCLC
8 |
Rosell, Ann. Oncol. 2002
Paclitaxel/Cisplatin
Paclitaxel/CarboplatinN
um
be
r o
f p
ati
en
ts
40% of all pts received
6 cycles
70% pts received 4 cycles
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
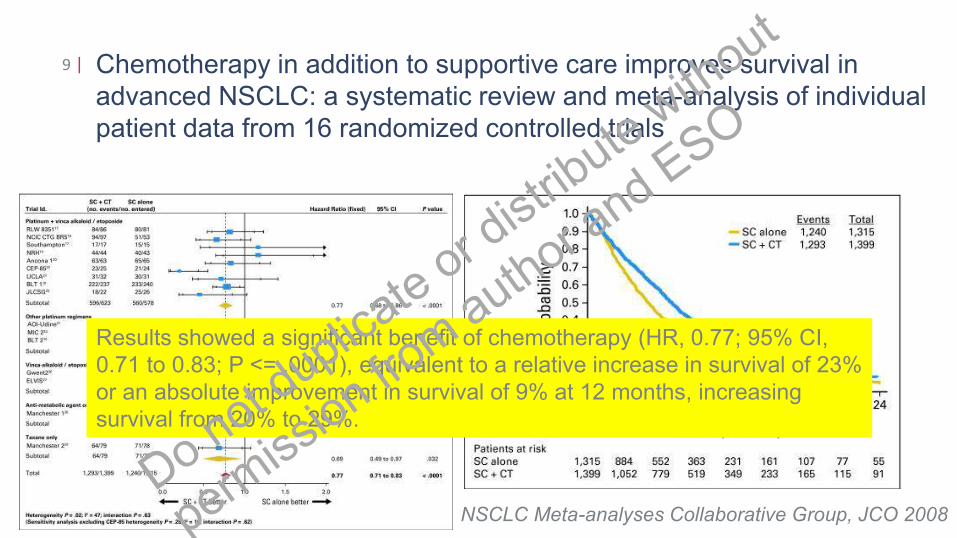
Chemotherapy in addition to supportive care improves survival in
advanced NSCLC: a systematic review and meta-analysis of individual
patient data from 16 randomized controlled trials
9 |
NSCLC Meta-analyses Collaborative Group, JCO 2008
Results showed a significant benefit of chemotherapy (HR, 0.77; 95% CI,
0.71 to 0.83; P <= .0001), equivalent to a relative increase in survival of 23%
or an absolute improvement in survival of 9% at 12 months, increasing
survival from 20% to 29%.
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
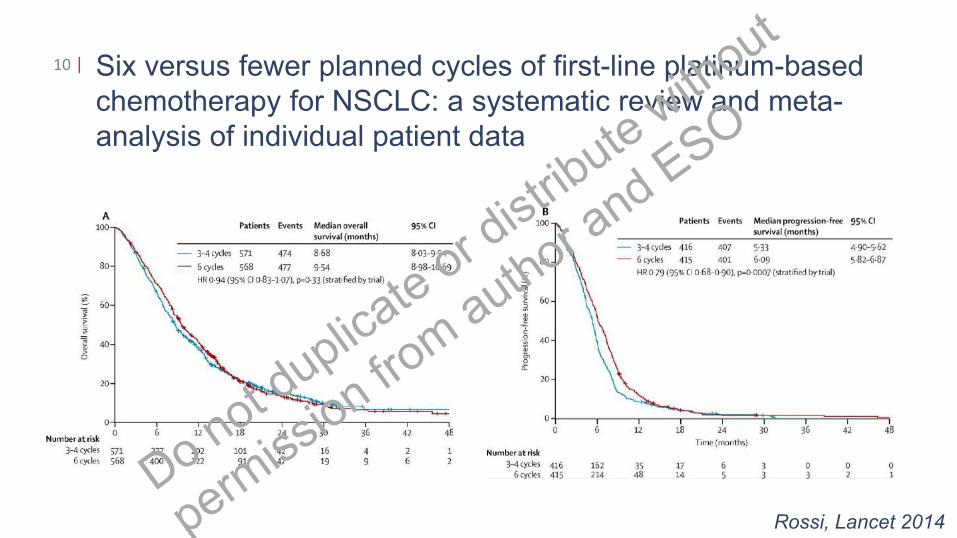
Six versus fewer planned cycles of first-line platinum-based
chemotherapy for NSCLC: a systematic review and meta-
analysis of individual patient data
10 |
Rossi, Lancet 2014
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
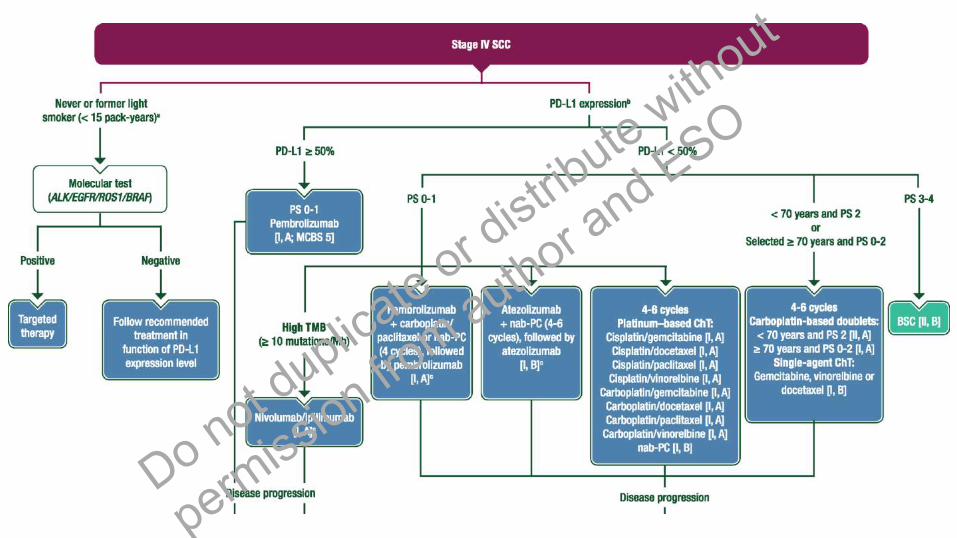
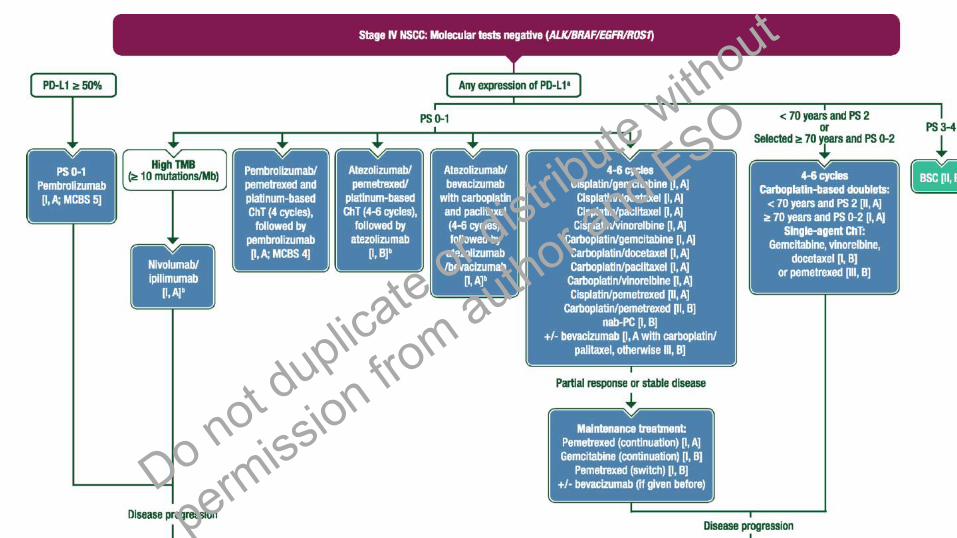
What can we conclude for the first line therapy of advanced
NSCLC without oncogenic driver mutation
• There is no single platinum-based doublet standard chemotherapy, however
pemetrexed combinations are favoured in non-squamous cell NSCLC
• If platinum-based chemotherapy is indicated, a combination with
bevacizumab is a treatment option in eligible patients with non-squamous
NSCLC. In this case, carboplatin/paclitaxel is the preferred combination
• Pemetrexed maintenance therapy is an option for patients with non-
squamous NSCLC without progression after first line therapy
• Immune checkpoint inhibition with pembrolizumab is becoming a standard for
patients with tumors with strong PD-L1 expression
• For patients with NSCLC with absent or week PD-L1 expression the
emerging treatments include chemotherapy/IO or IO/IO combinations
11 |
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
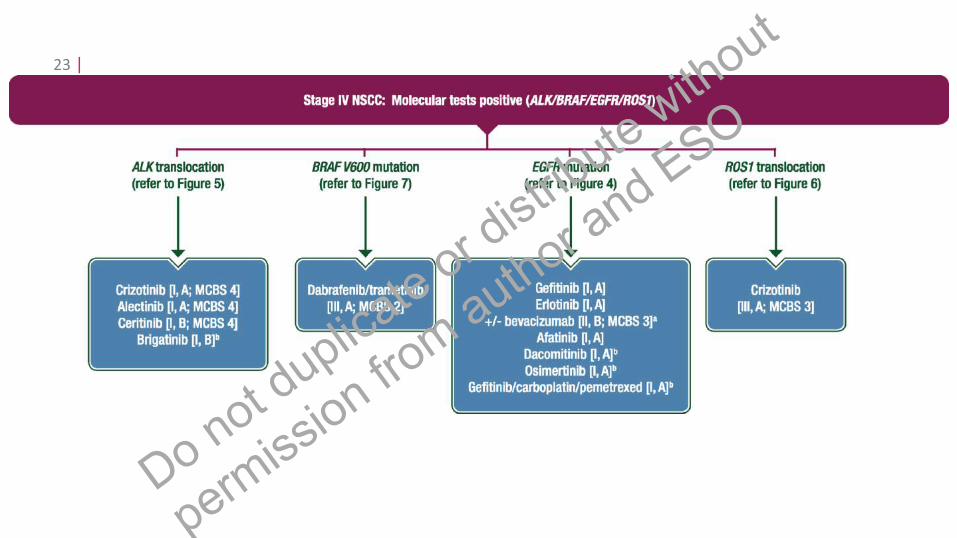
SO
Histological classification is necessary for decision making in
advanced NSCLC
• A diagnosis of “non-small cell lung cancer” is no longer acceptable as sufficient basis for treatment decisions:
• Cisplatin superior to carboplatin in adenocarcinomaArdizzoni, JNCI 2007
• Benefit of bevacizumab added to first line chemotherapy in non-
squamous cell carcinomaSandler, JCO 2006; Reck; JCO 2009; Zhou, JCO 2015
• Differential effect of pemetrexed in non-squamous vs squamous cell
carcinoma and use of pemetrexed maintenanceScagliotti, JCO 2008; Paz-Ares, JCO 2013
12 |
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
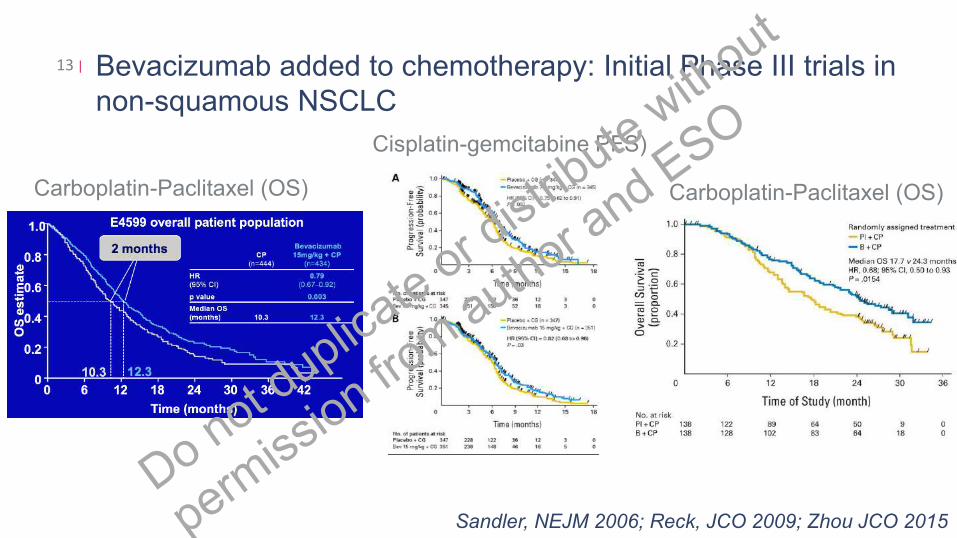
Bevacizumab added to chemotherapy: Initial Phase III trials in
non-squamous NSCLC
13 |
Sandler, NEJM 2006; Reck, JCO 2009; Zhou JCO 2015
Carboplatin-Paclitaxel (OS) Carboplatin-Paclitaxel (OS)
Cisplatin-gemcitabine PFS)
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
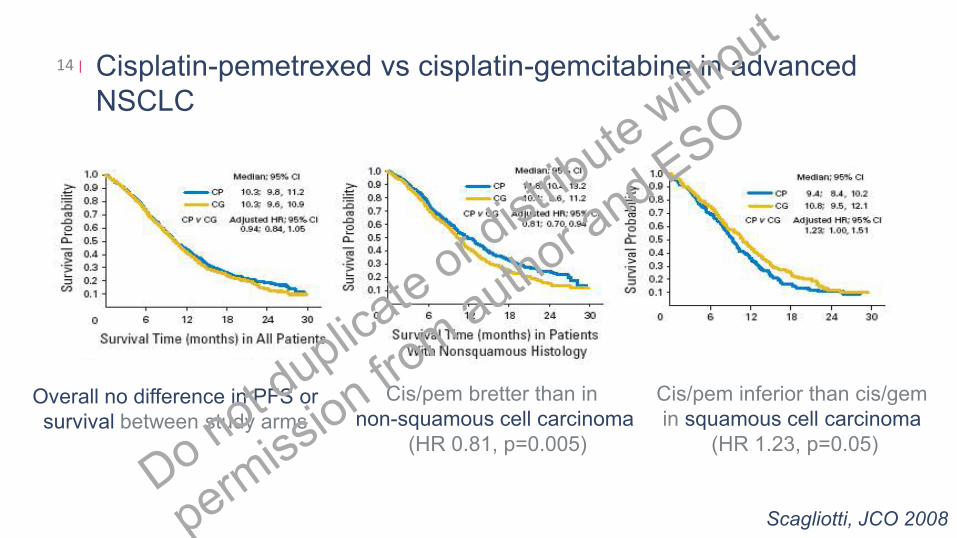
Cisplatin-pemetrexed vs cisplatin-gemcitabine in advanced
NSCLC
14 |
Overall no difference in PFS or
survival between study arms
Cis/pem bretter than in
non-squamous cell carcinoma
(HR 0.81, p=0.005)
Cis/pem inferior than cis/gem
in squamous cell carcinoma
(HR 1.23, p=0.05)
Scagliotti, JCO 2008
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
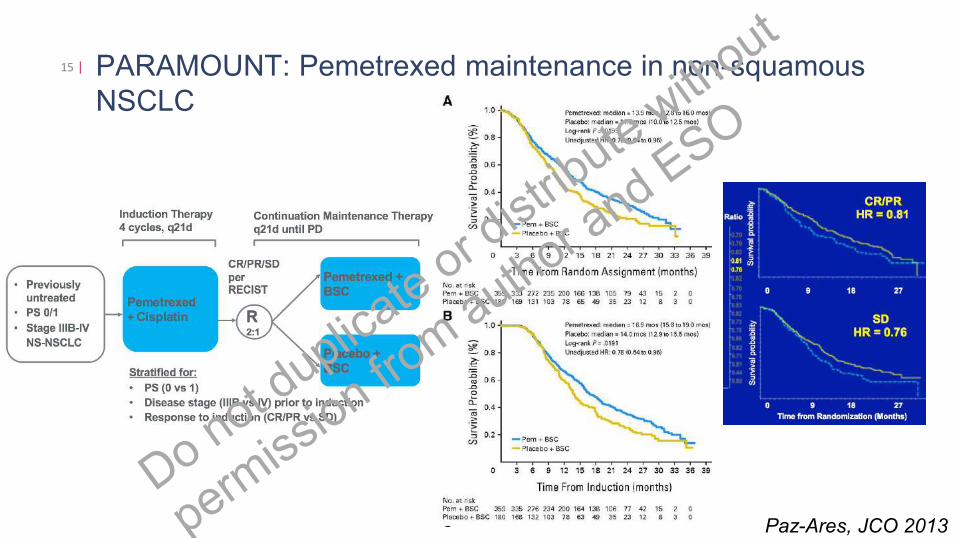
PARAMOUNT: Pemetrexed maintenance in non-squamous
NSCLC
15 |
Paz-Ares, JCO 2013
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
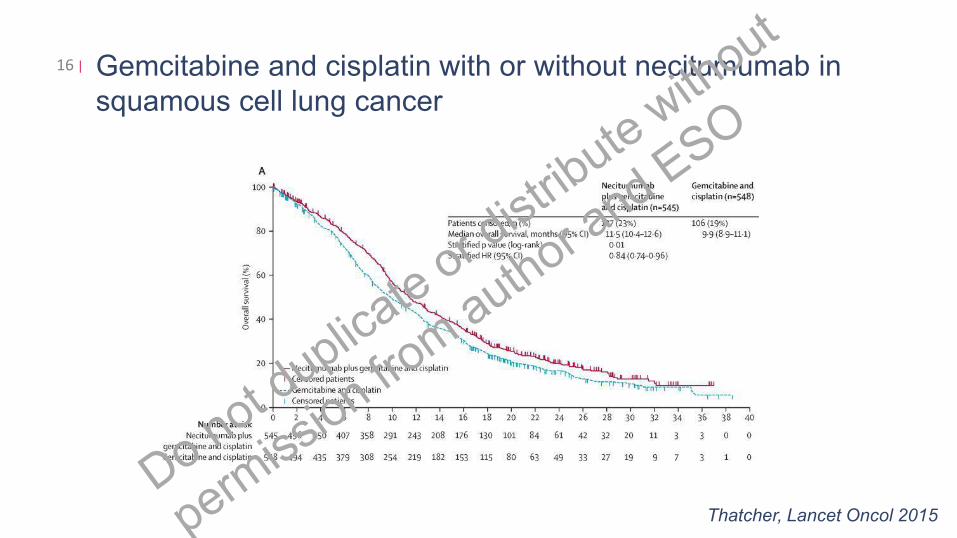
Gemcitabine and cisplatin with or without necitumumab in
squamous cell lung cancer
16 |
Thatcher, Lancet Oncol 2015
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
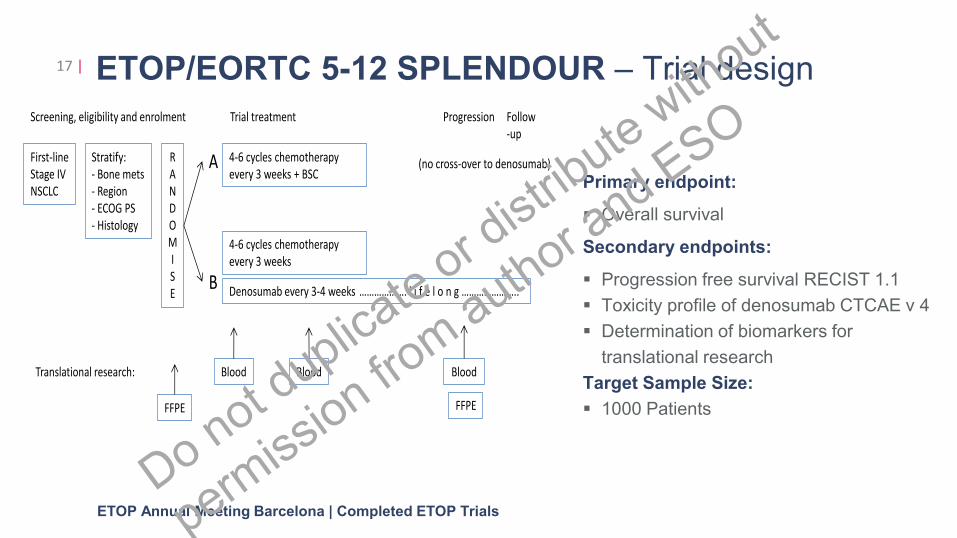
First-line
Stage IV
NSCLC
Stratify:
- Bone mets
- Region
- ECOG PS
- Histology
R
A
N
D
O
M
I
S
E
4-6 cycles chemotherapy
every 3 weeks + BSC
4-6 cycles chemotherapy
every 3 weeks
Denosumab every 3-4 weeks ………………. l i f e l o n g …………………..
A
B
Blood Blood Blood
Progression
Translational research:
Trial treatmentScreening, eligibility and enrolment Follow
-up
FFPE FFPE
(no cross-over to denosumab)
ETOP/EORTC 5-12 SPLENDOUR – Trial design
Primary endpoint:
▪ Overall survival
Secondary endpoints:
▪ Progression free survival RECIST 1.1
▪ Toxicity profile of denosumab CTCAE v 4
▪ Determination of biomarkers for
translational research
Target Sample Size:
▪ 1000 Patients
17 |
ETOP Annual Meeting Barcelona | Completed ETOP Trials
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
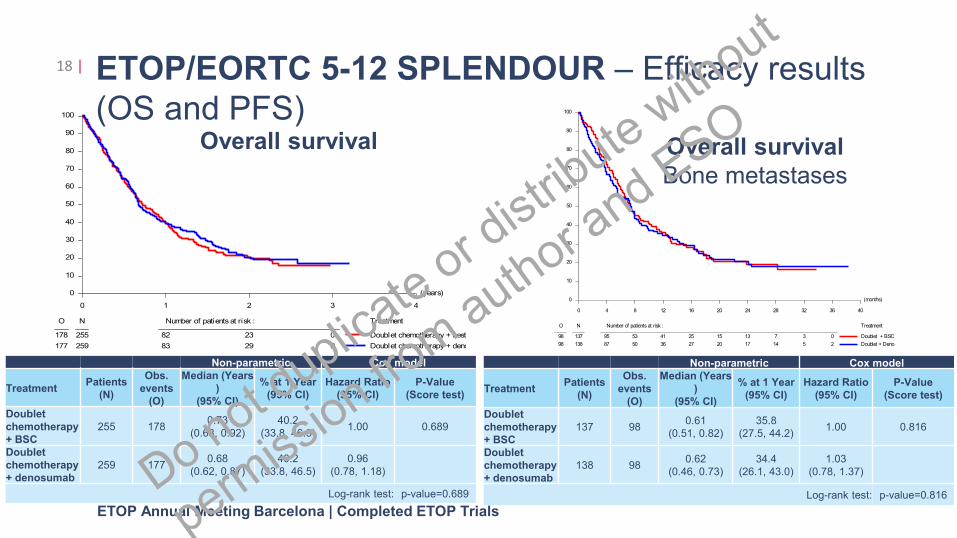
ETOP/EORTC 5-12 SPLENDOUR – Efficacy results
(OS and PFS)
18 |
ETOP Annual Meeting Barcelona | Completed ETOP Trials
(years)
0 1 2 3 4
0
10
20
30
40
50
60
70
80
90
100
O N Number of patients at risk : Treatment
178 255 82 23 0
177 259 83 29 2
Doublet chemotherapy + best su
Doublet chemotherapy + denos
Overall Score test: p=0.689
Non-parametric Cox model
TreatmentPatients
(N)
Obs.
events
(O)
Median (Years
)
(95% CI)
% at 1 Year
(95% CI)
Hazard Ratio
(95% CI)
P-Value
(Score test)
Doublet
chemotherapy
+ BSC
255 1780.73
(0.63, 0.92)
40.2
(33.8, 46.5) 1.00 0.689
Doublet
chemotherapy
+ denosumab
259 1770.68
(0.62, 0.87)
40.2
(33.8, 46.5)
0.96
(0.78, 1.18)
Log-rank test: p-value=0.689
Overall survival
(months)
0 4 8 12 16 20 24 28 32 36 40
0
10
20
30
40
50
60
70
80
90
100
O N Number of patients at risk : Treatment
98 137 95 53 41 25 15 13 7 3 0
98 138 87 50 36 27 20 17 14 5 2
Doublet + BSC
Doublet + Deno
Bone Metastasis
Overall Score test: p=0.816
Overall survival
Bone metastases
Non-parametric Cox model
TreatmentPatients
(N)
Obs.
events
(O)
Median (Years
)
(95% CI)
% at 1 Year
(95% CI)
Hazard Ratio
(95% CI)
P-Value
(Score test)
Doublet
chemotherapy
+ BSC
137 980.61
(0.51, 0.82)
35.8
(27.5, 44.2) 1.00 0.816
Doublet
chemotherapy
+ denosumab
138 980.62
(0.46, 0.73)
34.4
(26.1, 43.0)
1.03
(0.78, 1.37)
Log-rank test: p-value=0.816 Do n
ot duplic
ate o
r dist
ribute
with
out
permiss
ion from
auth
or and E
SO
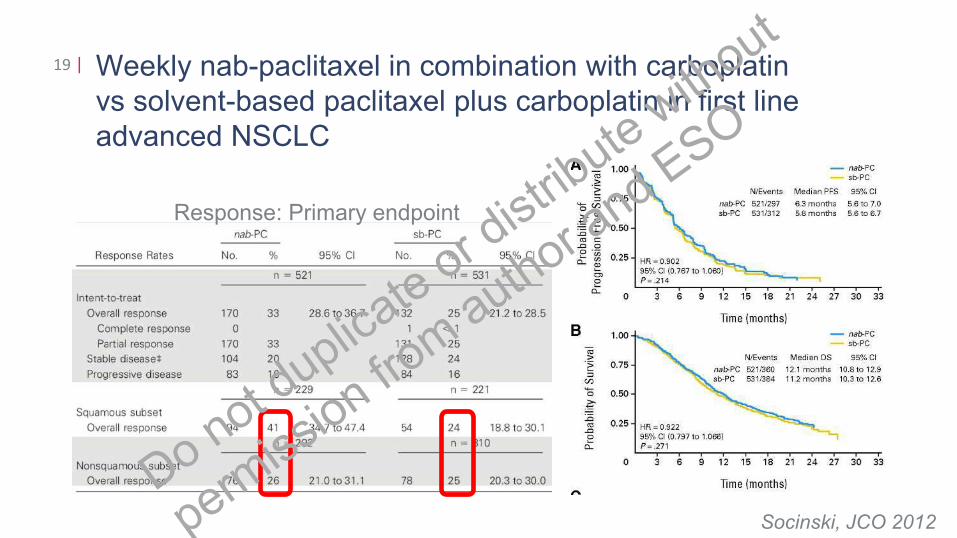
Weekly nab-paclitaxel in combination with carboplatin
vs solvent-based paclitaxel plus carboplatin in first line
advanced NSCLC
19 |
Socinski, JCO 2012
Response: Primary endpoint
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
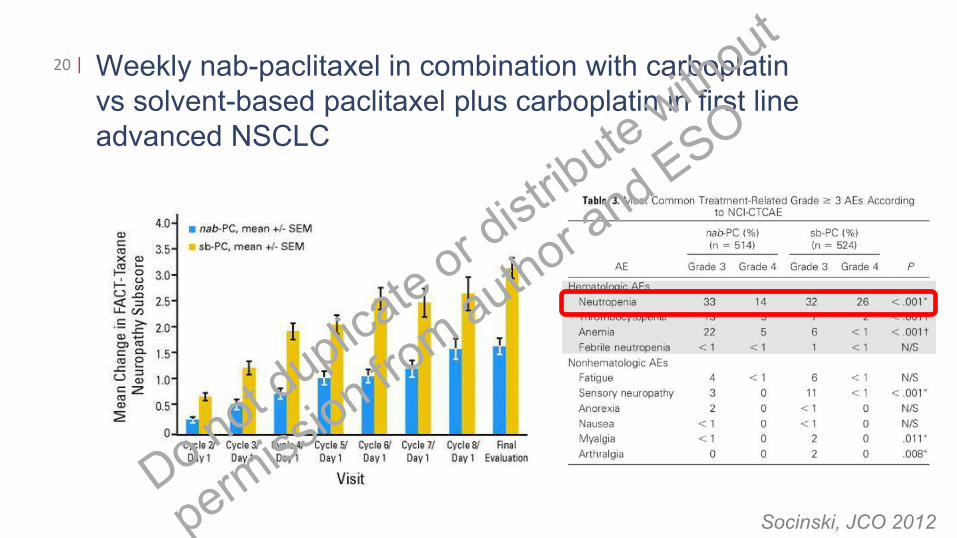
Weekly nab-paclitaxel in combination with carboplatin
vs solvent-based paclitaxel plus carboplatin in first line
advanced NSCLC
20 |
Socinski, JCO 2012
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
21 |
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
22 |
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
23 |
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
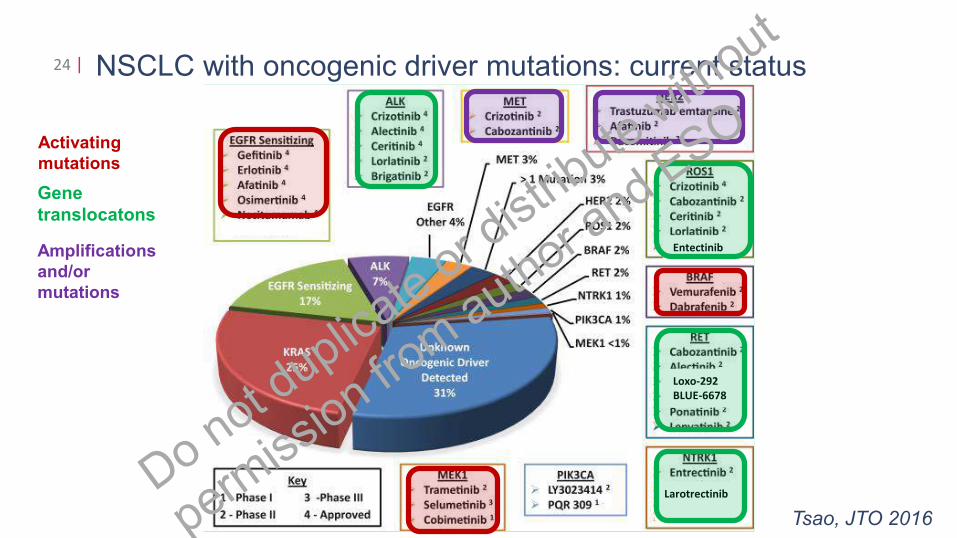
NSCLC with oncogenic driver mutations: current status24 |
Tsao, JTO 2016
Activating
mutations
Amplifications
and/or
mutations
Entectinib
Loxo-292
BLUE-6678
Larotrectinib
Gene
translocatons
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
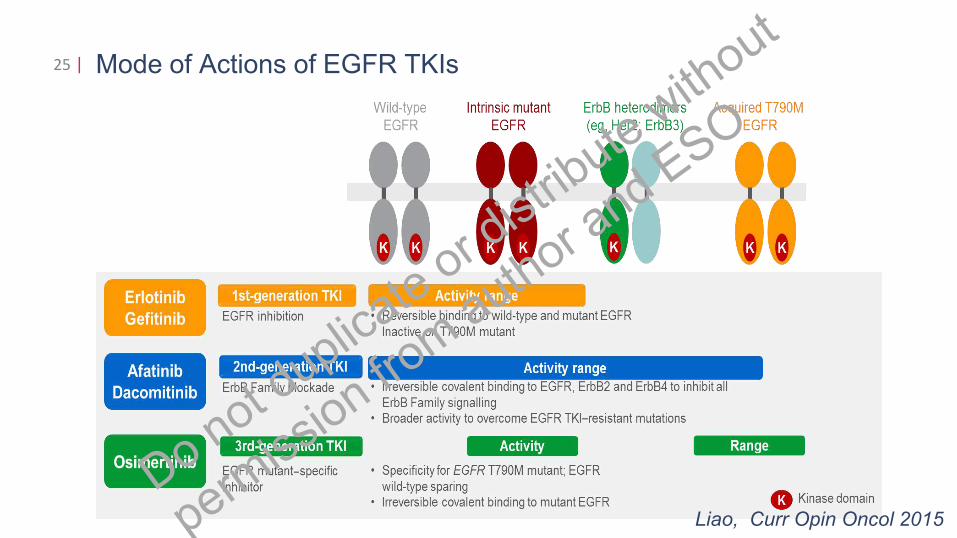
Mode of Actions of EGFR TKIs25 |
Liao, Curr Opin Oncol 2015
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
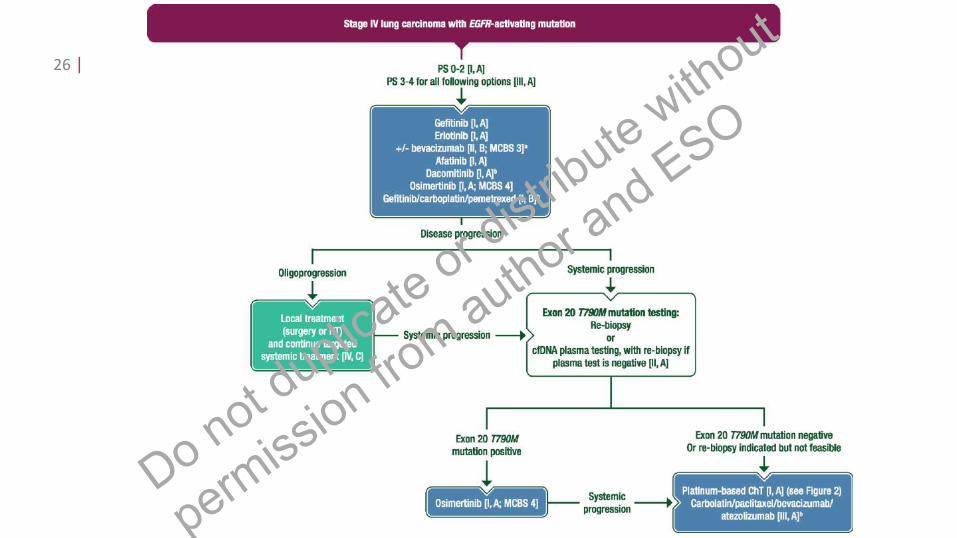
26 |
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
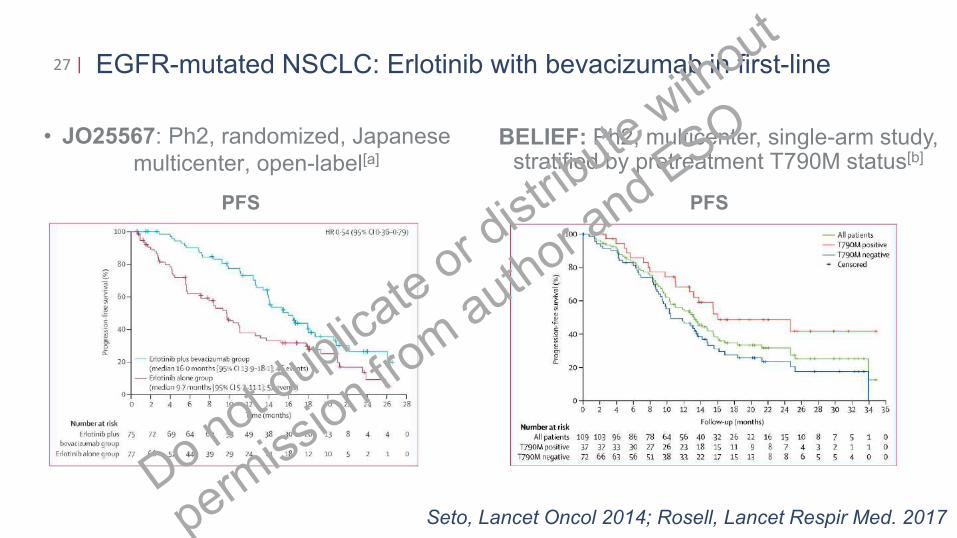
EGFR-mutated NSCLC: Erlotinib with bevacizumab in first-line27 |
• JO25567: Ph2, randomized, Japanese
multicenter, open-label[a]
Seto, Lancet Oncol 2014; Rosell, Lancet Respir Med. 2017
PFS
BELIEF: Ph2, multicenter, single-arm study, stratified by pretreatment T790M status[b]
PFS
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
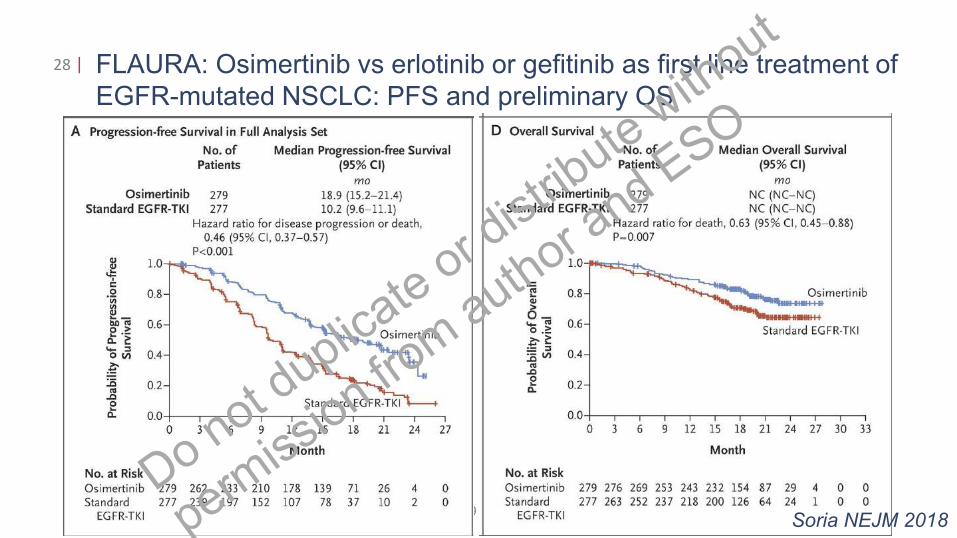
FLAURA: Osimertinib vs erlotinib or gefitinib as first line treatment of
EGFR-mutated NSCLC: PFS and preliminary OS
28 |
ETOP | Name Project | Title Presentation | Zurich, July 27, 2009Soria NEJM 2018
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
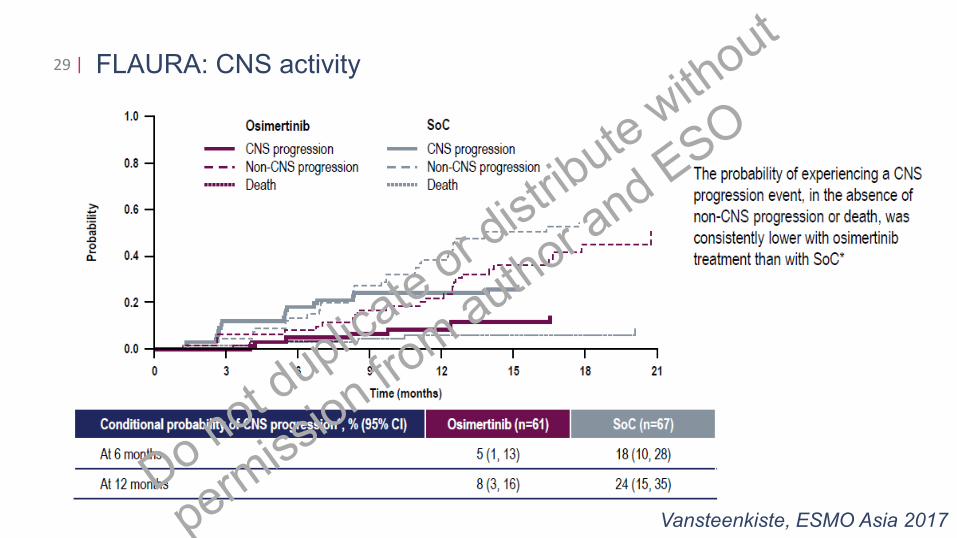
FLAURA: CNS activity29 |
Vansteenkiste, ESMO Asia 2017
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
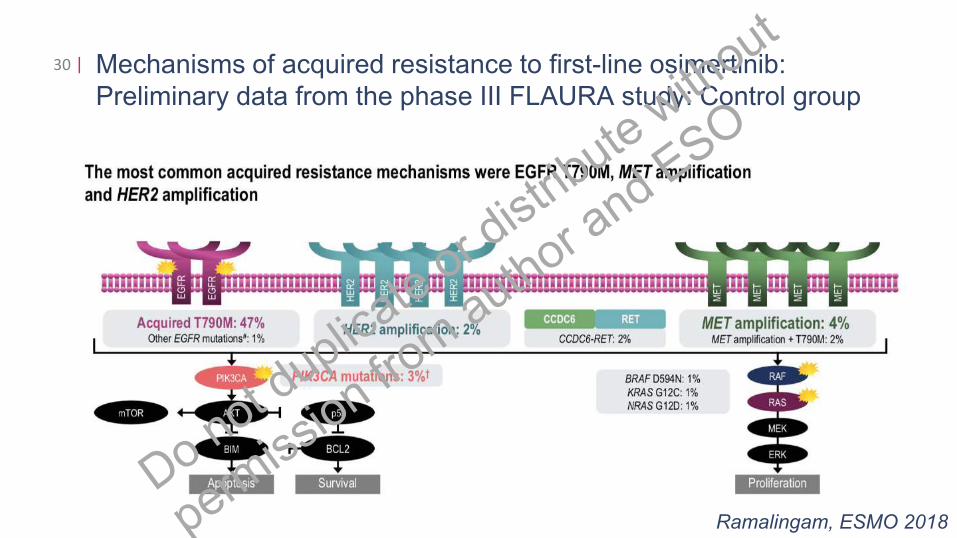
Mechanisms of acquired resistance to first-line osimertinib:
Preliminary data from the phase III FLAURA study: Control group
30 |
Ramalingam, ESMO 2018
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
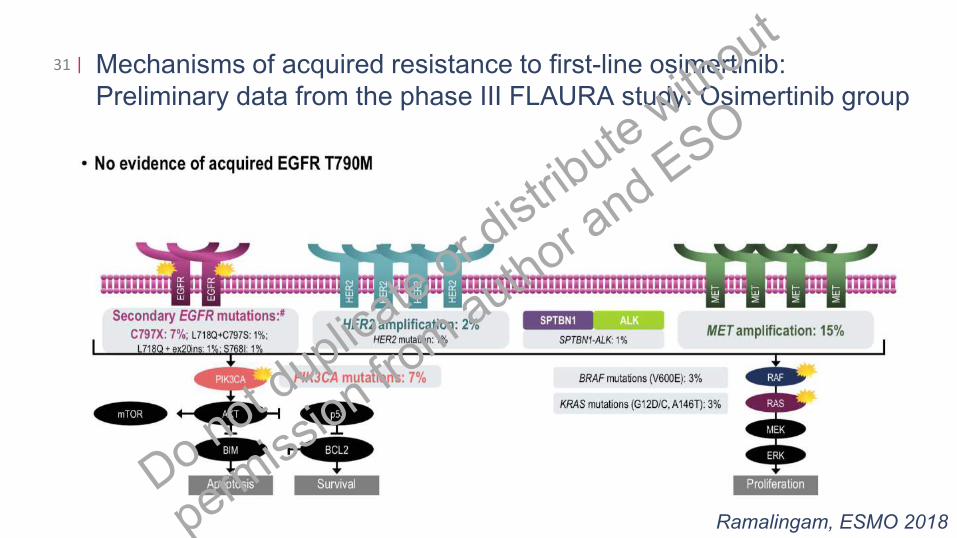
Mechanisms of acquired resistance to first-line osimertinib:
Preliminary data from the phase III FLAURA study: Osimertinib group
31 |
Ramalingam, ESMO 2018
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
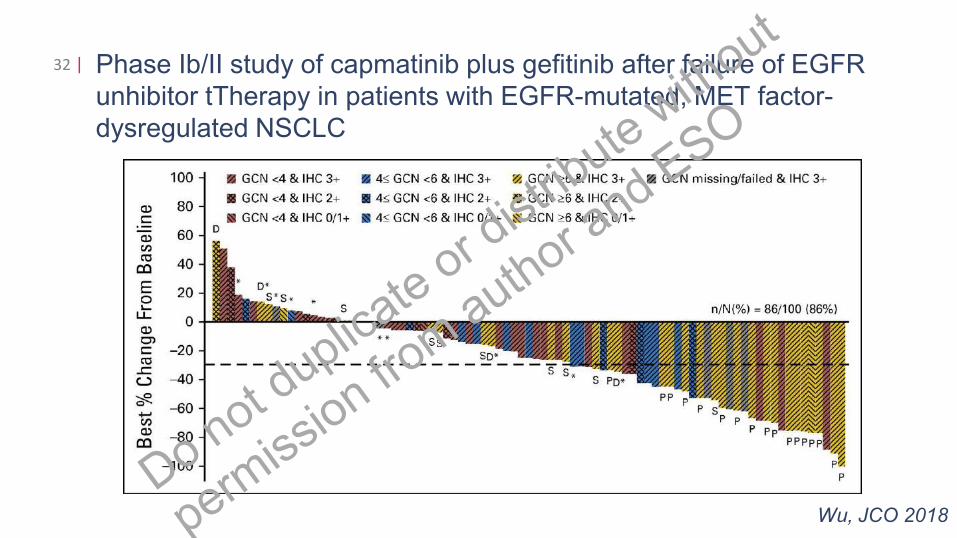
Phase Ib/II study of capmatinib plus gefitinib after failure of EGFR
unhibitor tTherapy in patients with EGFR-mutated, MET factor-
dysregulated NSCLC
32 |
Wu, JCO 2018
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
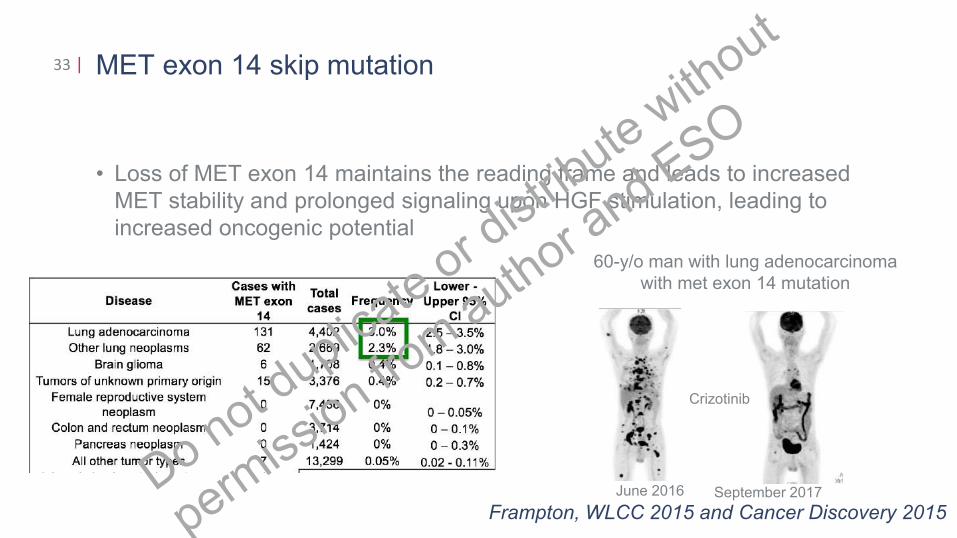
MET exon 14 skip mutation
• Loss of MET exon 14 maintains the reading frame and leads to increased
MET stability and prolonged signaling upon HGF stimulation, leading to
increased oncogenic potential
33 |
Frampton, WLCC 2015 and Cancer Discovery 2015
June 2016 September 2017
60-y/o man with lung adenocarcinoma
with met exon 14 mutation
Crizotinib
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
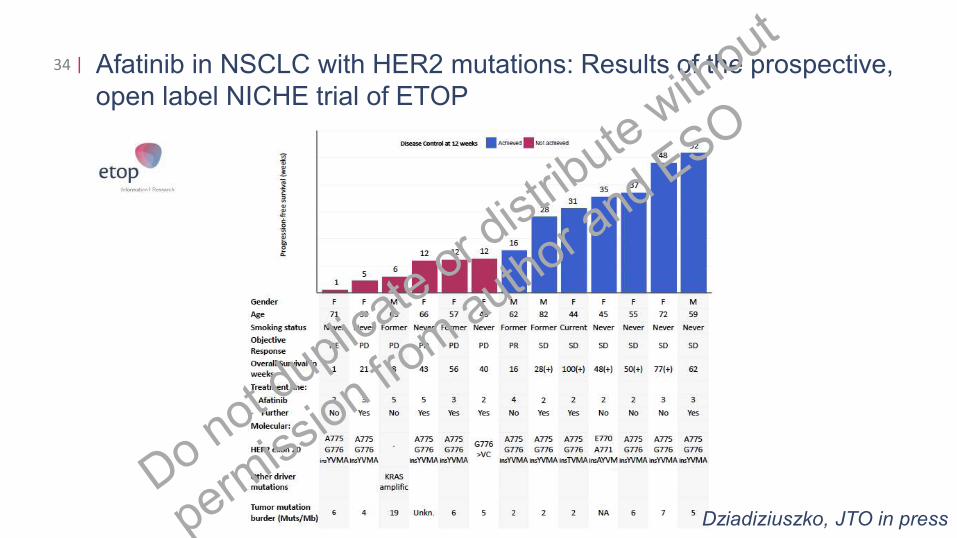
Afatinib in NSCLC with HER2 mutations: Results of the prospective,
open label NICHE trial of ETOP
34 |
Dziadiziuszko, JTO in press
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
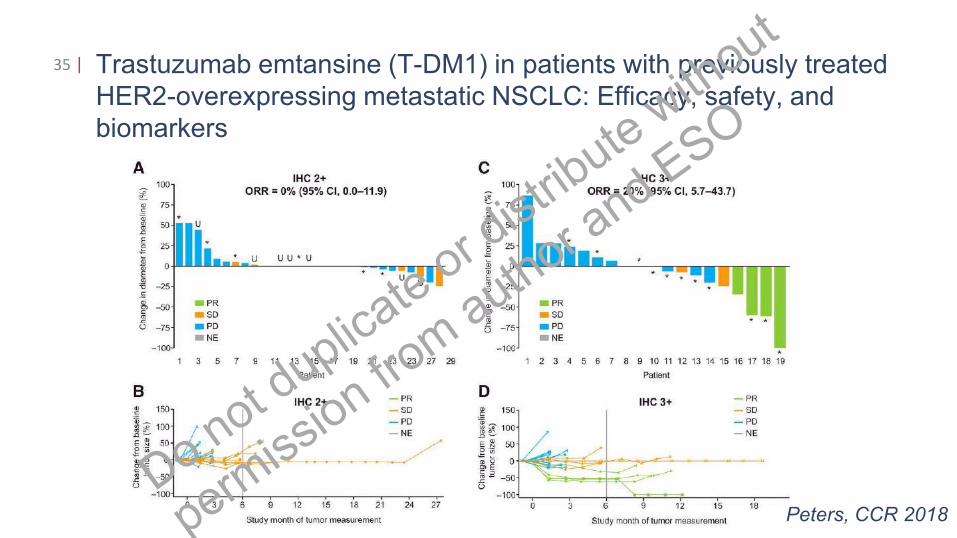
Trastuzumab emtansine (T-DM1) in patients with previously treated
HER2-overexpressing metastatic NSCLC: Efficacy, safety, and
biomarkers
35 |
Peters, CCR 2018
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
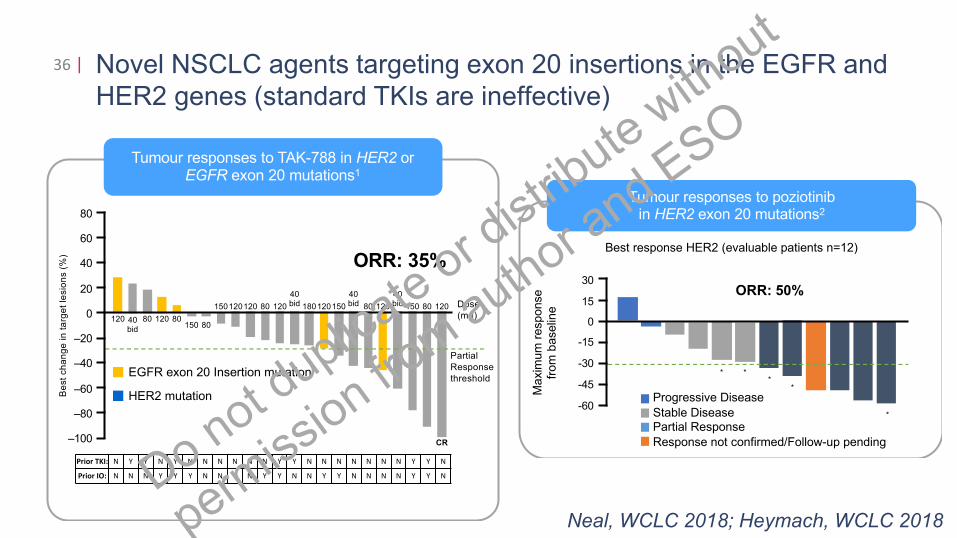
Novel NSCLC agents targeting exon 20 insertions in the EGFR and
HER2 genes (standard TKIs are ineffective)
36 |
Tumour responses to poziotinib in HER2 exon 20 mutations2
Best response HER2 (evaluable patients n=12)
Progressive Disease
Stable DiseasePartial Response
Response not confirmed/Follow-up pending
Ma
xim
um
resp
onse
from
baselin
e
ORR: 50%
* **
*
*
30
-60
-15
-45
15
0
-30
80
Tumour responses to TAK-788 in HER2 or EGFR exon 20 mutations1
ORR: 35%
120 40bid
80 120150 80
150120120 80 120
40 bid 180120 120
CR
150 80
40 bid12080
40 bid150 Dose
(mg)
Partial
Response
threshold
Prior TKI: N Y Y N Y N N N N N N Y Y N N N N N N N Y Y N
Prior IO: N N N Y Y Y N N Y N Y Y N N Y Y N N N N Y Y N
80
–100
60
20
–20
–60
–80
40
0
–40
Be
st
ch
an
ge
in
ta
rge
t le
sio
ns (
%)
EGFR exon 20 Insertion mutation
HER2 mutation
Neal, WCLC 2018; Heymach, WCLC 2018
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
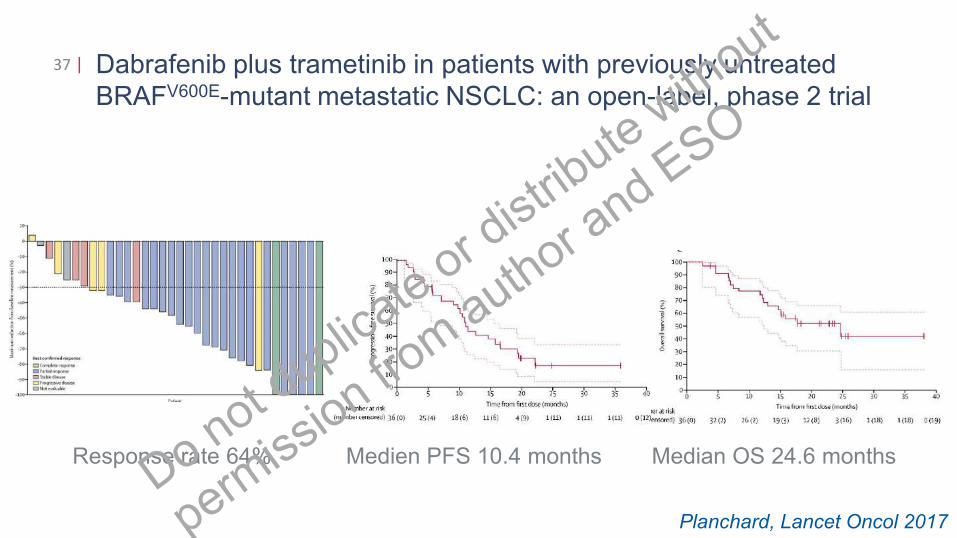
Dabrafenib plus trametinib in patients with previously untreated
BRAFV600E-mutant metastatic NSCLC: an open-label, phase 2 trial
37 |
Planchard, Lancet Oncol 2017
Response rate 64% Medien PFS 10.4 months Median OS 24.6 months
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
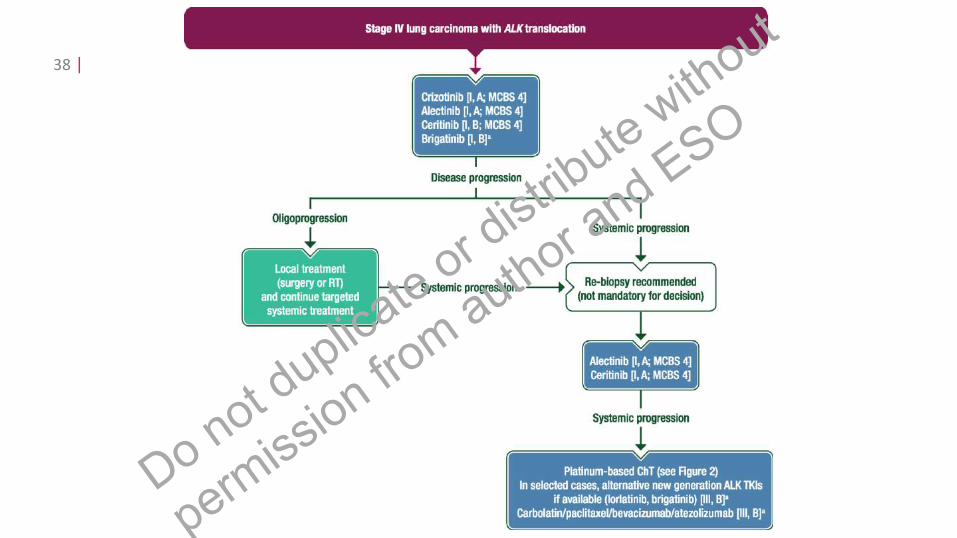
38 |
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
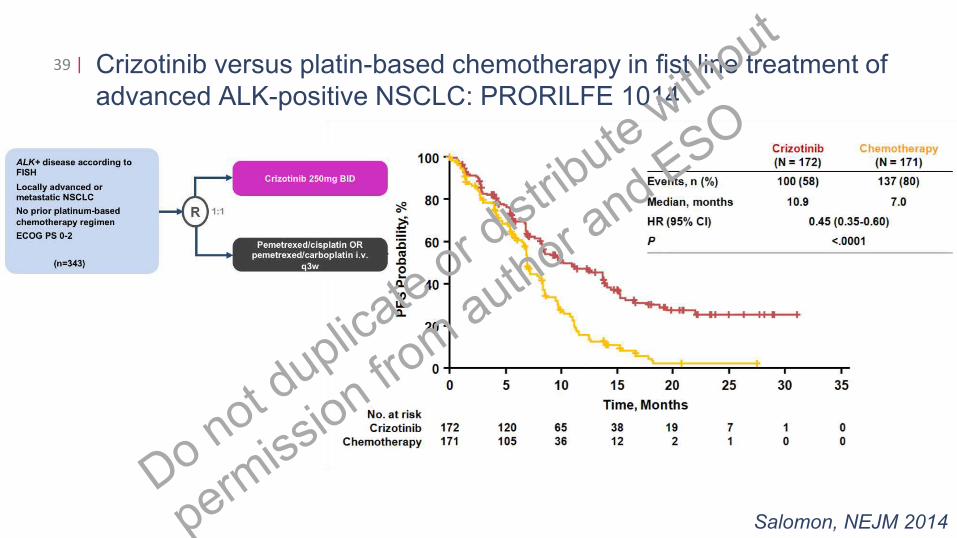
Crizotinib versus platin-based chemotherapy in fist line treatment of
advanced ALK-positive NSCLC: PRORILFE 1014
39 |
Salomon, NEJM 2014
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
Case 1: 52-y/o man
• July 2012:
• Presentation to pneumologists with
cough and dyspnea
• Bronchoscopy demonstrated occlusion of
R main bronchus
• Biopsy: Adenocarcinoma
• PET/CT: right central tumor with contralateral
mediastinal and supraclavicular lymph node
metastases
• Molecular pathology: Neg for EGFR mutation,
40 |
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
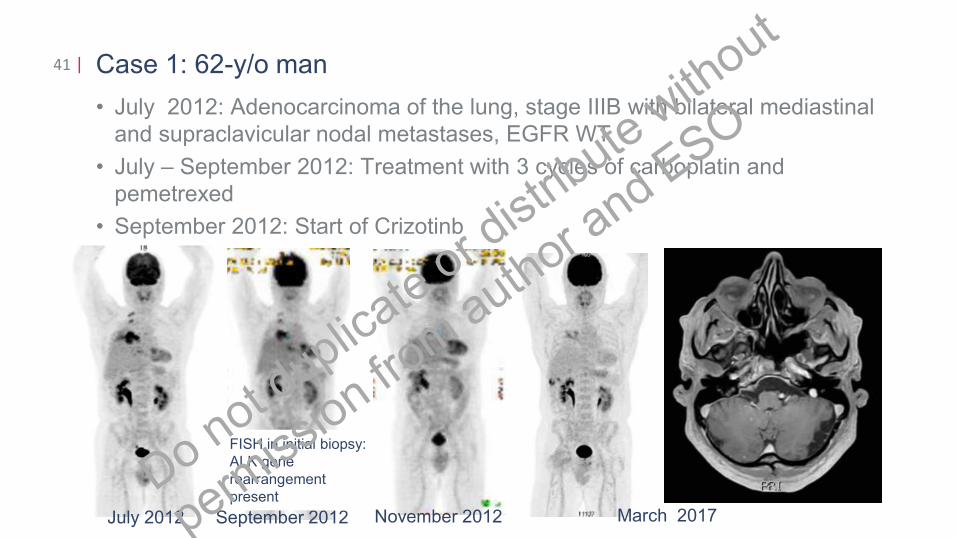
Case 1: 62-y/o man
• July 2012: Adenocarcinoma of the lung, stage IIIB with bilateral mediastinal
and supraclavicular nodal metastases, EGFR WT
• July – September 2012: Treatment with 3 cycles of carboplatin and
pemetrexed
• September 2012: Start of Crizotinb
41 |
July 2012 September 2012
FISH in initial biopsy:
ALK gene
rearrangement
present
November 2012 March 2017
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
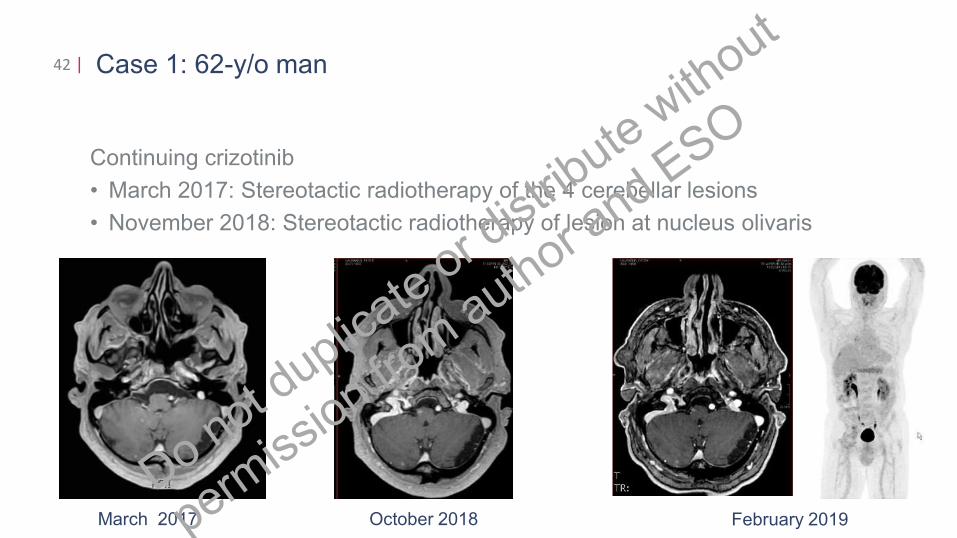
Case 1: 62-y/o man
Continuing crizotinib
• March 2017: Stereotactic radiotherapy of the 4 cerebellar lesions
• November 2018: Stereotactic radiotherapy of lesion at nucleus olivaris
42 |
March 2017 October 2018 February 2019
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
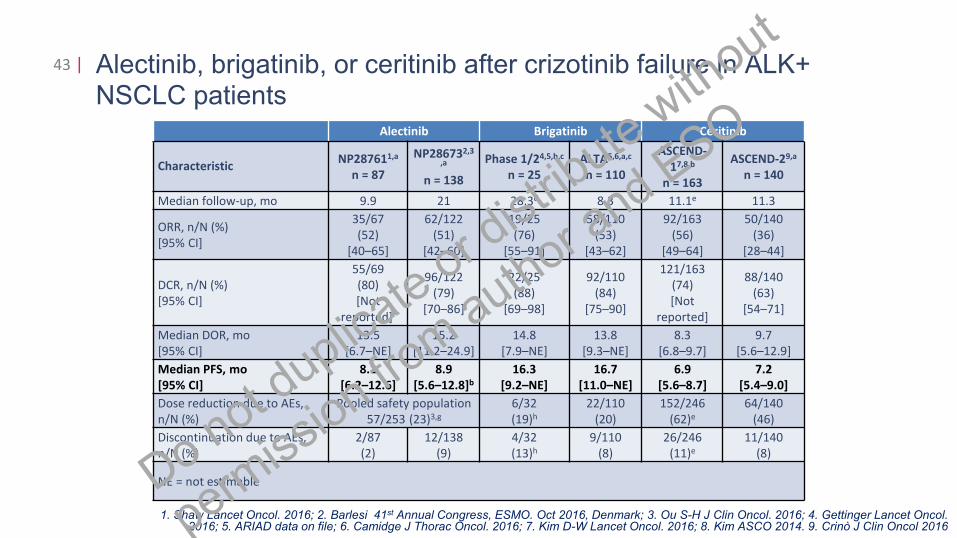
Alectinib, brigatinib, or ceritinib after crizotinib failure in ALK+ NSCLC patients
43 |
Alectinib Brigatinib Ceritinib
CharacteristicNP287611,a
n = 87
NP286732,3
,a
n = 138
Phase 1/24,5,b,c
n = 25
ALTA5,6,a,c
n = 110
ASCEND-
17,8,b
n = 163
ASCEND-29,a
n = 140
Median follow-up, mo 9.9 21 28.3d 8.3 11.1e 11.3
ORR, n/N (%)
[95% CI]
35/67
(52)
[40–65]
62/122
(51)
[42–60]
19/25
(76)
[55–91]
58/110
(53)
[43–62]
92/163
(56)
[49–64]
50/140
(36)
[28–44]
DCR, n/N (%)
[95% CI]
55/69
(80)
[Not
reported]f
96/122
(79)
[70–86]
22/25
(88)
[69–98]
92/110
(84)
[75–90]
121/163
(74)
[Not
reported]
88/140
(63)
[54–71]
Median DOR, mo
[95% CI]
13.5
[6.7–NE]
15.2
[11.2–24.9]
14.8
[7.9–NE]
13.8
[9.3–NE]
8.3
[6.8–9.7]
9.7
[5.6–12.9]
Median PFS, mo
[95% CI]
8.1
[6.2–12.6]
8.9
[5.6–12.8]b
16.3
[9.2–NE]
16.7
[11.0–NE]
6.9
[5.6–8.7]
7.2
[5.4–9.0]
Dose reduction due to AEs,
n/N (%)
Pooled safety population
57/253 (23)3,g
6/32
(19)h
22/110
(20)
152/246
(62)e
64/140
(46)
Discontinuation due to AEs,
n/N (%)
2/87
(2)
12/138
(9)
4/32
(13)h
9/110
(8)
26/246
(11)e
11/140
(8)
NE = not estimable
1. Shaw Lancet Oncol. 2016; 2. Barlesi 41st Annual Congress, ESMO. Oct 2016, Denmark; 3. Ou S-H J Clin Oncol. 2016; 4. Gettinger Lancet Oncol. 2016; 5. ARIAD data on file; 6. Camidge J Thorac Oncol. 2016; 7. Kim D-W Lancet Oncol. 2016; 8. Kim ASCO 2014. 9. Crinò J Clin Oncol 2016
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
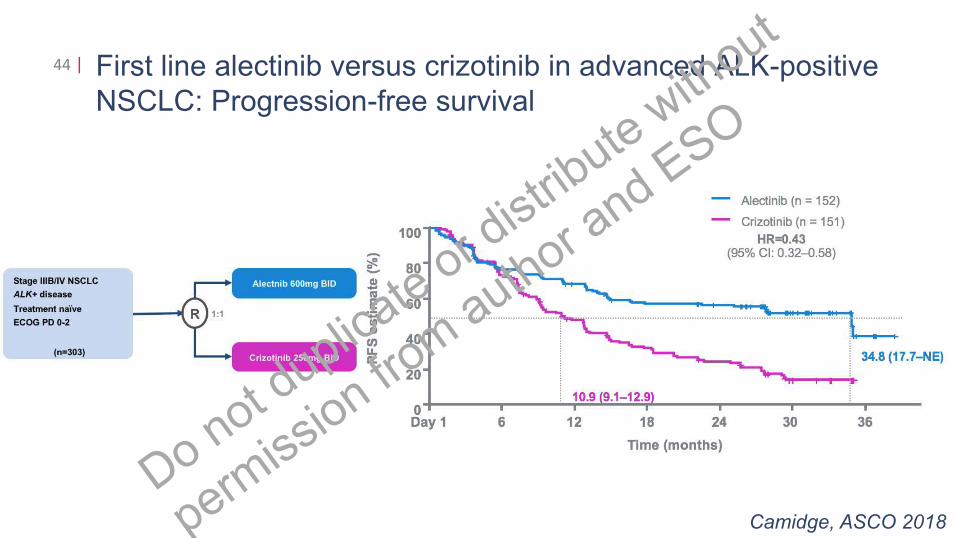
First line alectinib versus crizotinib in advanced ALK-positive
NSCLC: Progression-free survival
44 |
Camidge, ASCO 2018
ICB
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
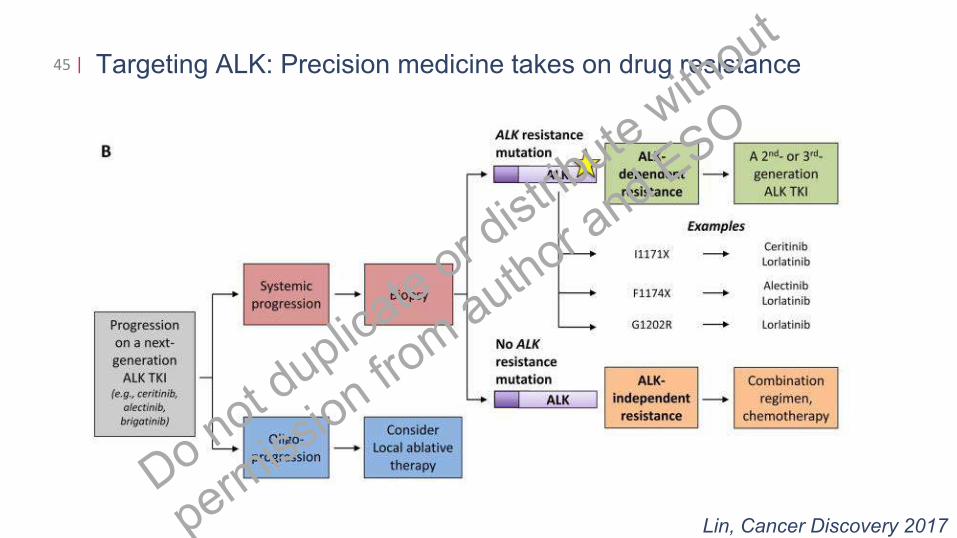
Targeting ALK: Precision medicine takes on drug resistance45 |
Lin, Cancer Discovery 2017
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
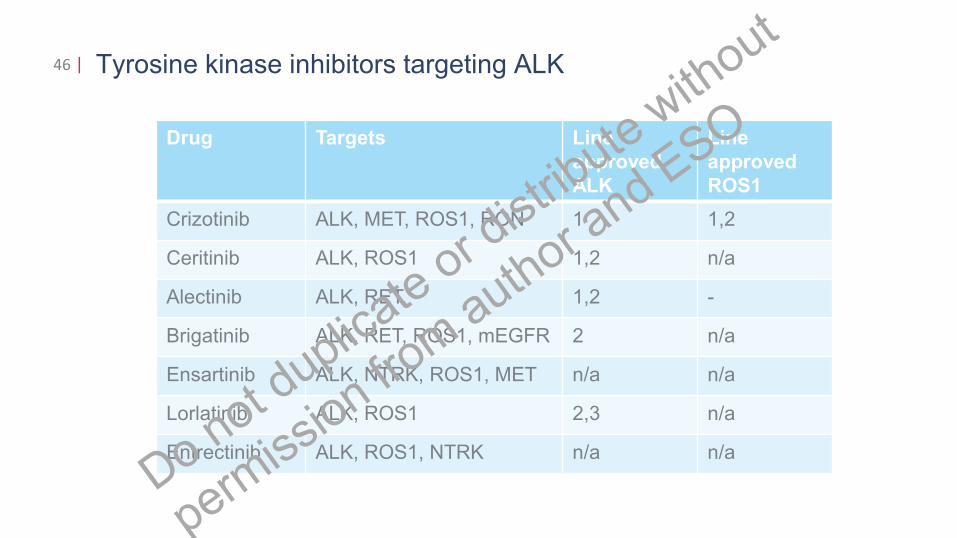
Tyrosine kinase inhibitors targeting ALK
Drug Targets Line
approved
ALK
Line
approved
ROS1
Crizotinib ALK, MET, ROS1, RON 1 1,2
Ceritinib ALK, ROS1 1,2 n/a
Alectinib ALK, RET, 1,2 -
Brigatinib ALK, RET, ROS1, mEGFR 2 n/a
Ensartinib ALK, NTRK, ROS1, MET n/a n/a
Lorlatinib ALK, ROS1 2,3 n/a
Entrectinib ALK, ROS1, NTRK n/a n/a
46 |
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
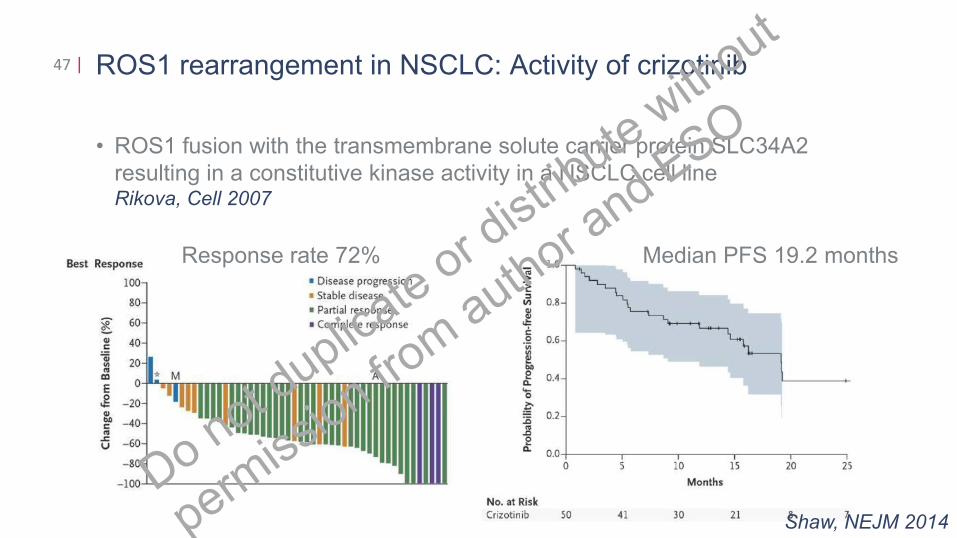
ROS1 rearrangement in NSCLC: Activity of crizotinib
• ROS1 fusion with the transmembrane solute carrier protein SLC34A2
resulting in a constitutive kinase activity in a NSCLC cell lineRikova, Cell 2007
47 |
Shaw, NEJM 2014
Response rate 72% Median PFS 19.2 months
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
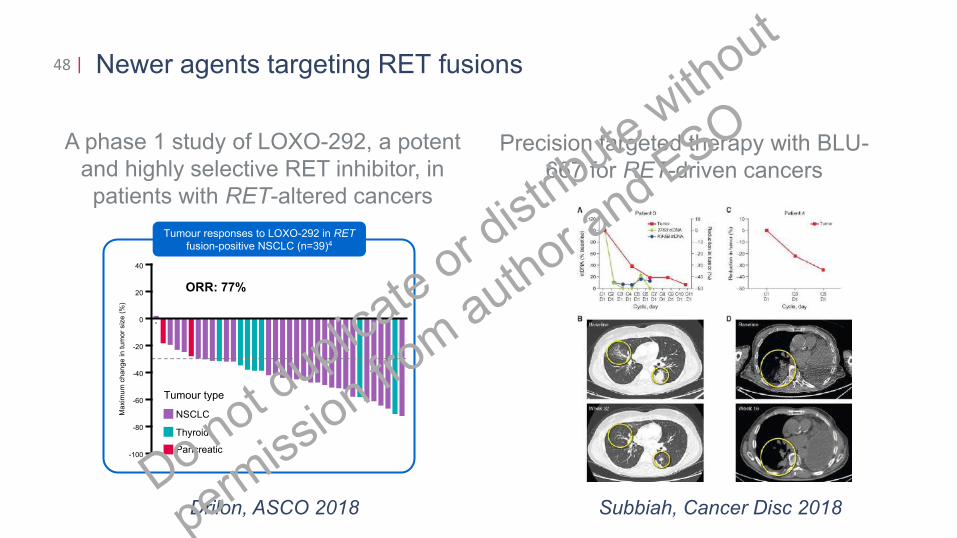
Newer agents targeting RET fusions48 |
Drilon, ASCO 2018
–
ORR: 77%
40
-100
0
-20
-60
-80
20
-40
Ma
xim
um
ch
an
ge
in
tu
mo
r siz
e (
%)
*
NSCLC
Thyroid
Pancreatic
Tumour type
Tumour responses to LOXO-292 in RET
fusion-positive NSCLC (n=39)4
A phase 1 study of LOXO-292, a potent
and highly selective RET inhibitor, in
patients with RET-altered cancers
Precision targeted therapy with BLU-
667 for RET-driven cancers
Subbiah, Cancer Disc 2018Do n
ot duplic
ate o
r dist
ribute
with
out
permiss
ion from
auth
or and E
SO
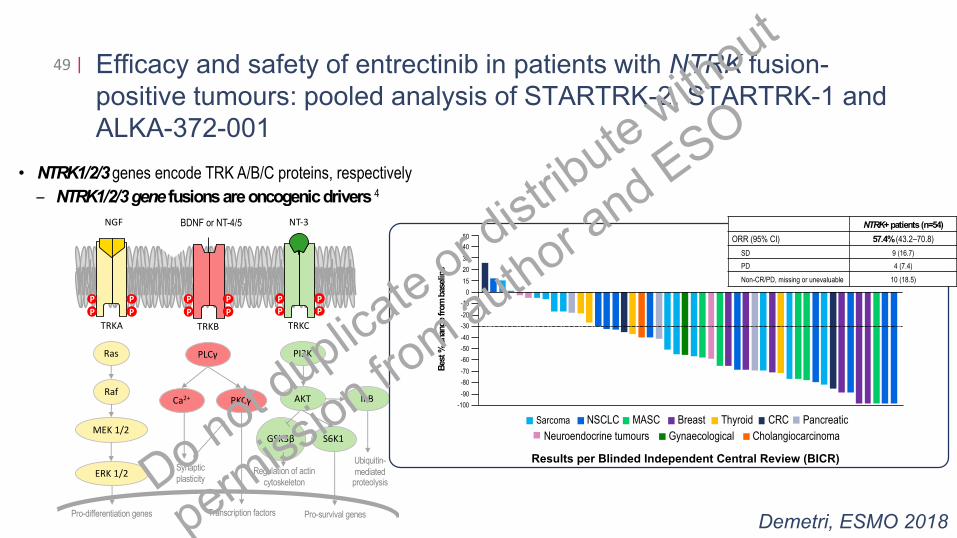
Efficacy and safety of entrectinib in patients with NTRK fusion-
positive tumours: pooled analysis of STARTRK-2, STARTRK-1 and
ALKA-372-001
49 |
Demetri, ESMO 2018Pro-survival genes
TRKA
NGF
Ras
Raf
MEK 1/2
ERK 1/2
PLCγ
Ca2+ PKCγ
PI3K
AKT
P
P
P
P
TRKB
BDNF or NT-4/5
P
P
P
P
TRKC
NT-3
P
P
P
P
GSK3β S6K1
IκB
Pro-differentiation genes
Synaptic
plasticity
Transcription factors
Regulation of actin
cytoskeleton
Ubiquitin-
mediated proteolysis
• NTRK1/2/3 genes encode TRK A/B/C proteins, respectively
– NTRK1/2/3 gene fusions are oncogenic drivers 4
0
-30
-50
-90
Bes
t %
chan
ge
from
bas
elin
e
15
-80
-70
-60
-40
-20
-10
20
30
40
-100
50
CRCNSCLCSarcoma
Neuroendocrine tumours
PancreaticThyroidMASC Breast
CholangiocarcinomaGynaecological
NTRK+patients (n=54)
ORR (95% CI) 57.4% (43.2–70.8)
SD 9 (16.7)
PD 4 (7.4)
Non-CR/PD, missing or unevaluable 10 (18.5)
Results per Blinded Independent Central Review (BICR)
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
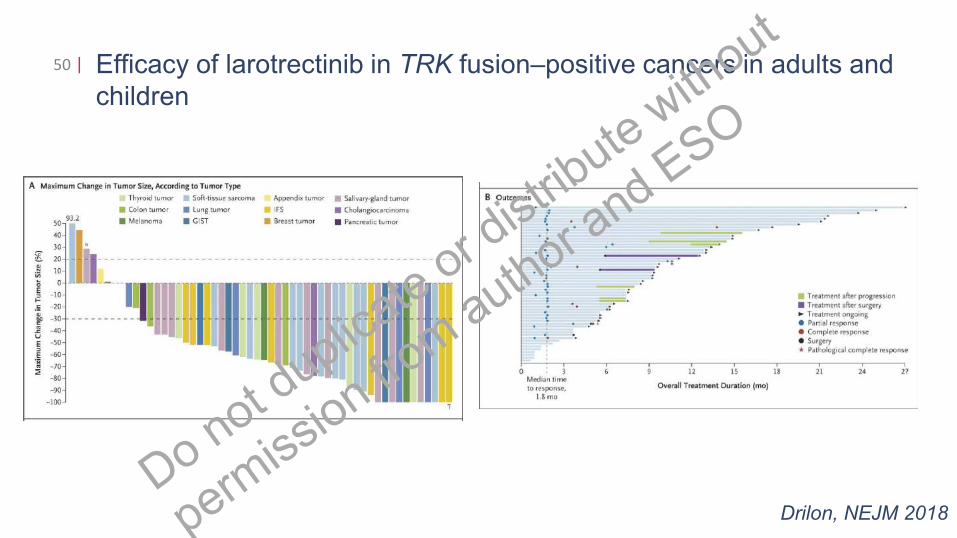
Efficacy of larotrectinib in TRK fusion–positive cancers in adults and
children
50 |
Drilon, NEJM 2018
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
Thomas Hart Benton
America Today
Thomas Hart Benton:
“America Today”Do n
ot duplic
ate o
r dist
ribute
with
out
permiss
ion from
auth
or and E
SO