Embed Size (px)
DESCRIPTION
Chemotherapy
Citation preview
CHEMOTHERAPY
Presented By: Dr. Joseph John K. PothanikatOMFS
he abnormal mass of tissue the growth of which exceeds and
is uncoordinated with that of normal tissue and persists in
the same excessive manner after cessation of the stimuli
which evoked the change
(Rupert Willis)
Neoplasia – Greek word – ‘new growth’
T
Chemotherapy• The treatment of malignancies and other diseases
with chemical agents; use of cytotoxic chemicals to destroy rapidly dividing cancer cells throughout the body; including normal, rapidly dividing cells in the bone marrow and gastrointestinal tract
• The treatment of disease by chemicals especially by killing micro-organisms or cancerous cells.

INTRODUCTION
• Cancer of the oral cavity -most prevalent tumor of the upper aero-digestive tract (UADT).
• Accounts for 3% of all cancers .
• In India 80,000 new cases/year
HISTORIC PERCEPTIVE

Mustard Gas (Bis 2 chloro-ethyl sulfide)
World War I – mustard gas –studied during WW-II – low WBC –damage rapidly growing WBC –effect on cancer
Louis S Goodman and AlfredGilmen(1942) – recruited by US Deptof defense – to investigate potentialtherapeutic applications of chemicalwarfare agents – autopsy of peopleexposed to mustard gas – lymphoidand myeloid suppression

ANTIFOLATES
• Farber , Harriett Kilte – used folate analogues- first Aminopterin and then Amethopterin (now methotrexate)
• In 1948 – first drug – induce remission – childrenALL – children died in peace
• National cancer institute – Roy Hertz and Min ChiuLi – choriocarcinoma (1958) – first solid tumorcured by chemotherapy
• James Holland, Freireich and Frei (1965) –simultaneously methotrexate, vincristine, mercaptopurine and prednisone – POMP regimen – long term remission in children –ALL
Combination Chemotherapy

Cancer Models

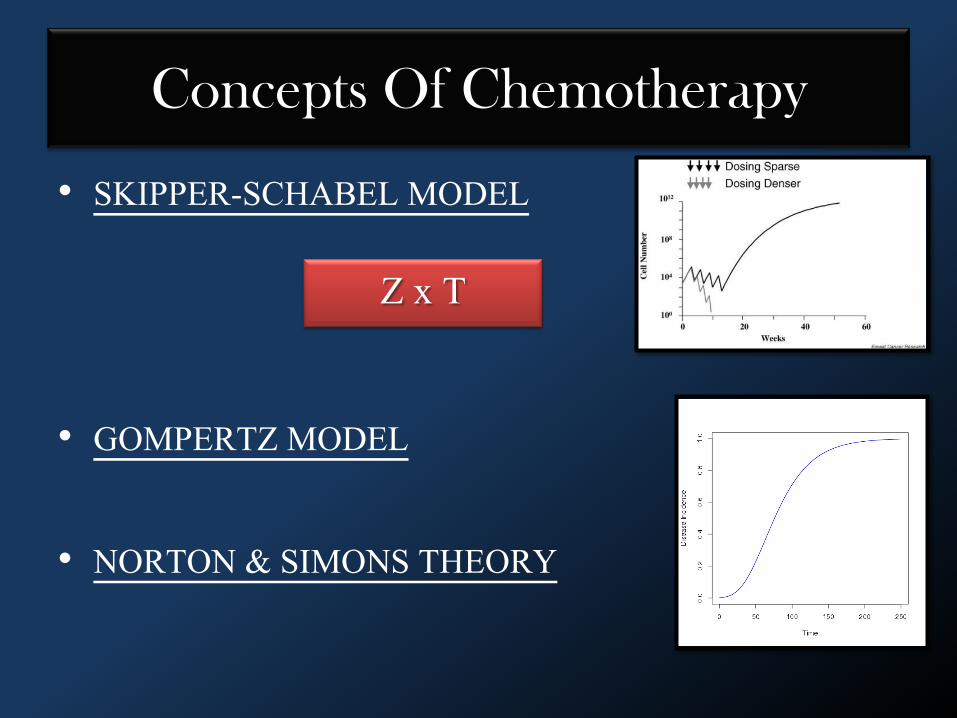
Concepts Of Chemotherapy
• SKIPPER-SCHABEL MODEL
• GOMPERTZ MODEL
• NORTON & SIMONS THEORY
Z x T
Concepts Of Chemotherapy
• SKIPPER-SCHABEL MODEL
• GOMPERTZ MODEL
• NORTON & SIMONS THEORY
Z x T
Gompertz’s Model; Implications
1. The initial growth of tumor is rapid and of first order, later growth being much slower.
2. Small tumors grow slowly but large % of dividing cells.
3. Medium tumors grow more quickly but small no of growth fraction.
4. Large tumor has small growth rate & growth fraction.
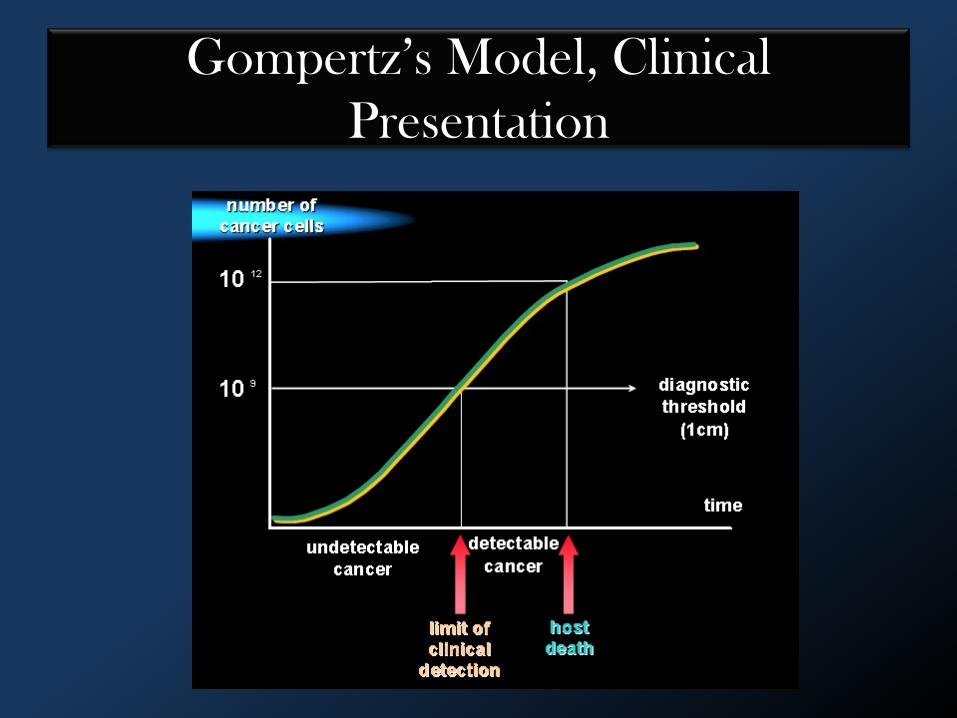
Gompertz’s Model, Clinical
Presentation
Limitations of Gompertz’s Model
• Discrepancy exist between the predicted values and the in vivo results.
NEED FOR A NEW CONCEPT !
• MOLECULAR BEAM EXITAXY (MBE) UNIVERSALITY CLASS
MOLECULAR BEAM EXITAXY (MBE) UNIVERSALITY CLASS
Clinical Implications
• All tumors exhibit similar growth dynamics.• Cell diffusion on the border is balanced with the
random duplication.• Movement of cells away from the tumor does
not influence the growth.• The outer cells divide about 30 times more than
the cells in the centre.• The most malignant cells are located at the
border and the degree of malignancy progress along the radius of the tumor..
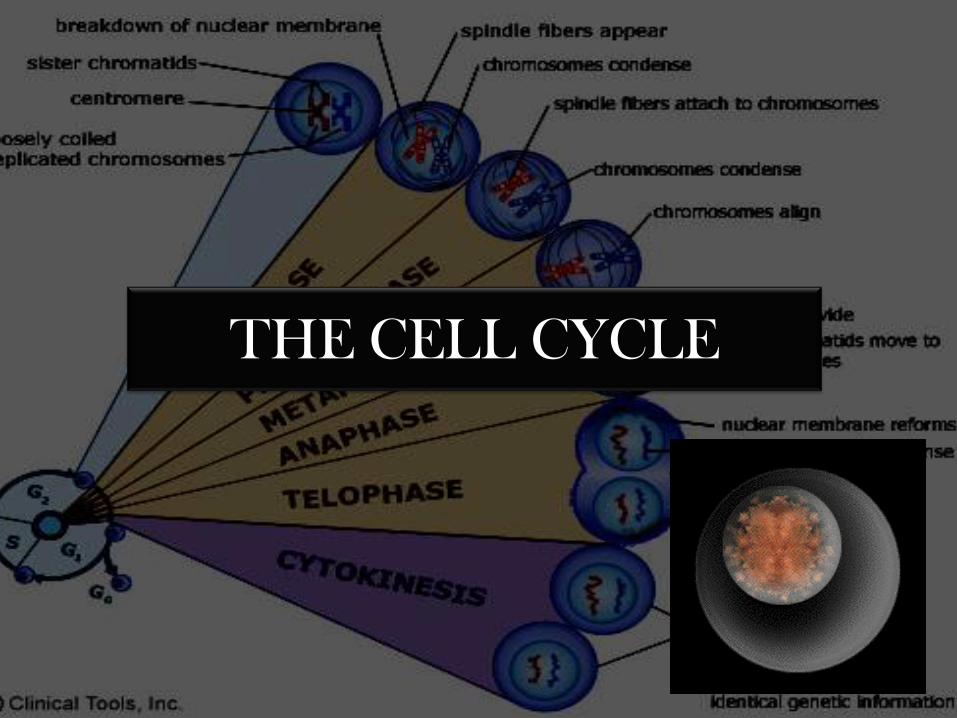
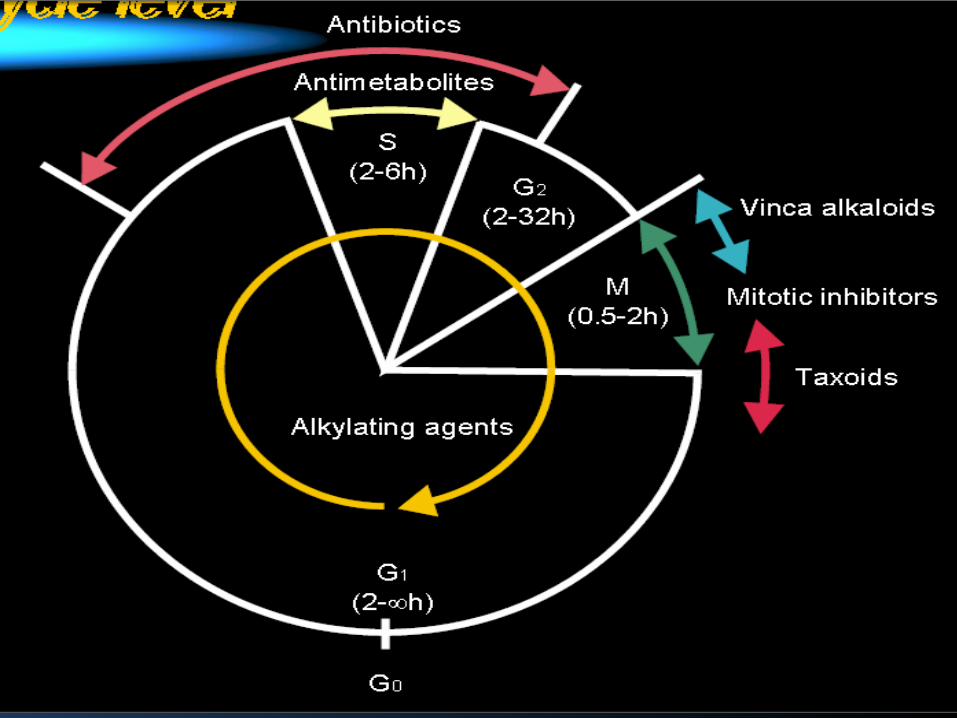
THE CELL CYCLE
Clinical Trials
Principles of Clinical Trials
• Evaluate efficacy of chemotherapy or combined modalities
• Parameters to be evaluated:– Object survival– disease free survival– duration of response– toxicity
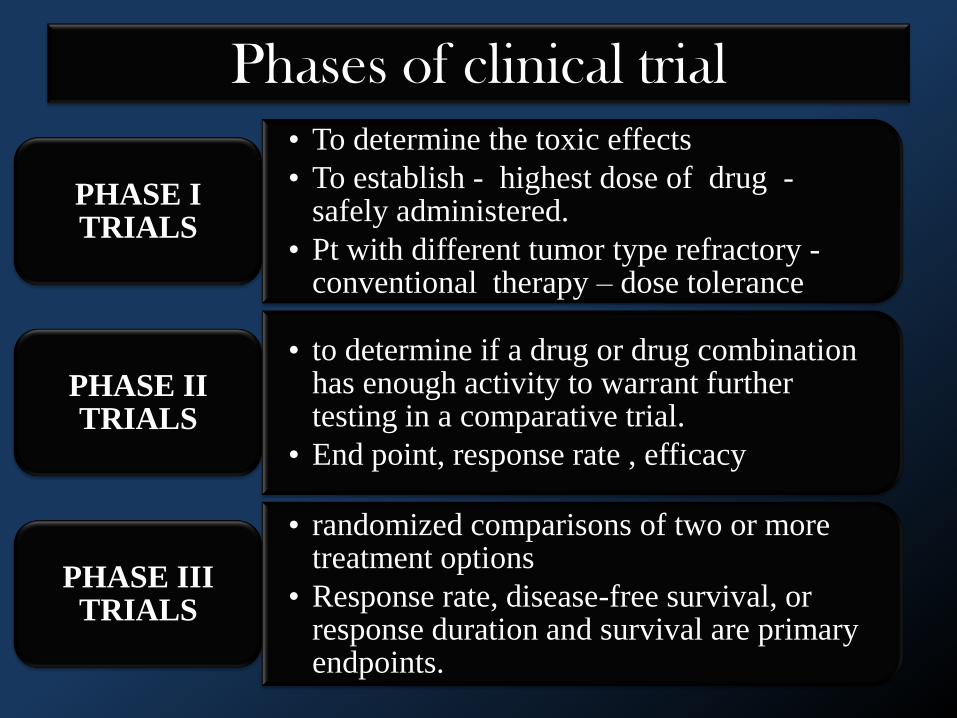
Phases of clinical trial
• To determine the toxic effects
• To establish - highest dose of drug -safely administered.
• Pt with different tumor type refractory -conventional therapy – dose tolerance
PHASE I TRIALS
• to determine if a drug or drug combination has enough activity to warrant further testing in a comparative trial.
• End point, response rate , efficacy
PHASE II TRIALS
• randomized comparisons of two or more treatment options
• Response rate, disease-free survival, or response duration and survival are primary endpoints.
PHASE III TRIALS
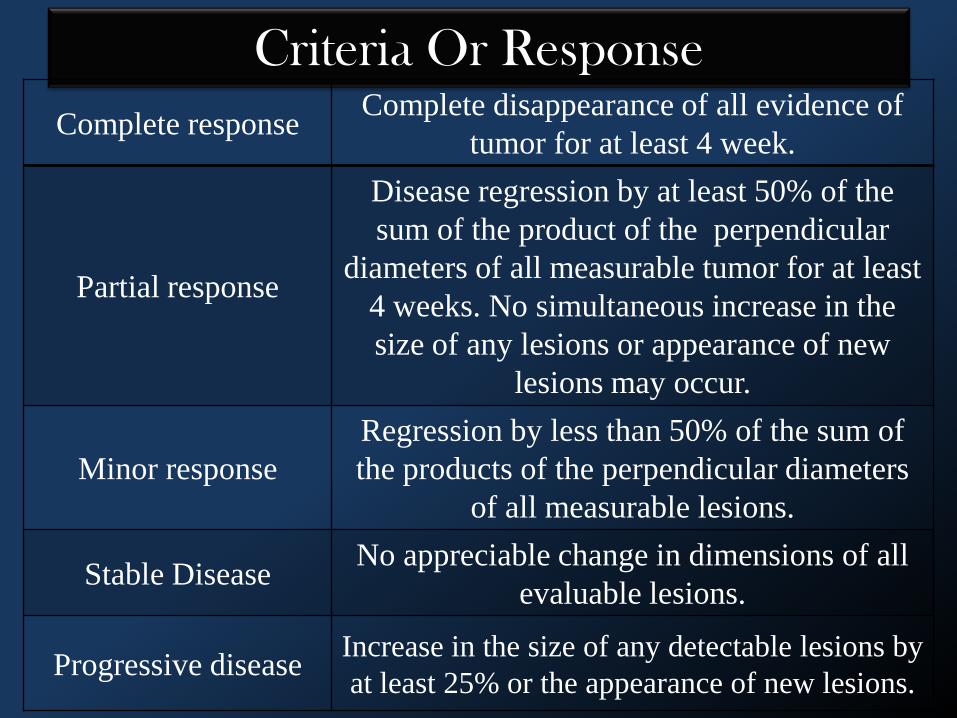
Criteria Or Response
Complete responseComplete disappearance of all evidence of
tumor for at least 4 week.
Partial response
Disease regression by at least 50% of the
sum of the product of the perpendicular
diameters of all measurable tumor for at least
4 weeks. No simultaneous increase in the
size of any lesions or appearance of new
lesions may occur.
Minor response
Regression by less than 50% of the sum of
the products of the perpendicular diameters
of all measurable lesions.
Stable Disease No appreciable change in dimensions of all
evaluable lesions.
Progressive diseaseIncrease in the size of any detectable lesions by
at least 25% or the appearance of new lesions.
Performance scales
• Zubrid Scale
• Kamofsky Performance Status
• Used today :Zubrid scale
Performance Scale

PROGNOSTIC FACTORS IN
PLANNING CHEMOTHERAPY
Prognostic factors in planning
chemotherapy
• Bulky primary tumors/extensive LN spread /advanced stage IV /with widespread visceral metastases
• Prior radiation
• Prior treatment status
• Prior chemotherapy
Prognostic factors in planning
chemotherapy
• Bulky primary tumors/extensive LN spread /advanced stage IV /with widespread visceral metastases
• Prior radiation
• Prior treatment status
• Prior chemotherapy
• Functional status of - kidneys, liver, bone marrow,heart, and lungs.
• Motivation and compliance of the patient.
• Performance status and nutritional state
• Degree of tumor differentiation
Prognostic factors in planning
chemotherapy

PRINCIPLES OF CHEMOTHERAPY
1. A single cancer cell can multiply and eventually kill the host
2. Survival and ability to respond to chemotherapy are inversely related to the numbers of viable tumor cells
3. Generally a direct relationship exists between the dose of a drug and its ability to kill tumor cells
4. A given dose of drug will kill a constant fraction of tumor cells regardless of the number present prior to therapy.

INDICATIONS
• Metastatic or locally advanced disease not amenable to curative therapy – surgery/radiation
• Patient undergone surgery and radiotherapy• Advanced laryngeal carcinoma – primary curative
treatment – voice preservation• Experimental protocols as primary therapy or combined
with radiotherapy for patients with a high risk of relapse
CONTRAINDICATIONS
• First Trimester Pregnancy
• Thrombocytopenia
• Liver or Kidney Impairment
• Recent Surgery

CLASSIFICATION
OF
CHEMOTHERAPEUTIC AGENTS
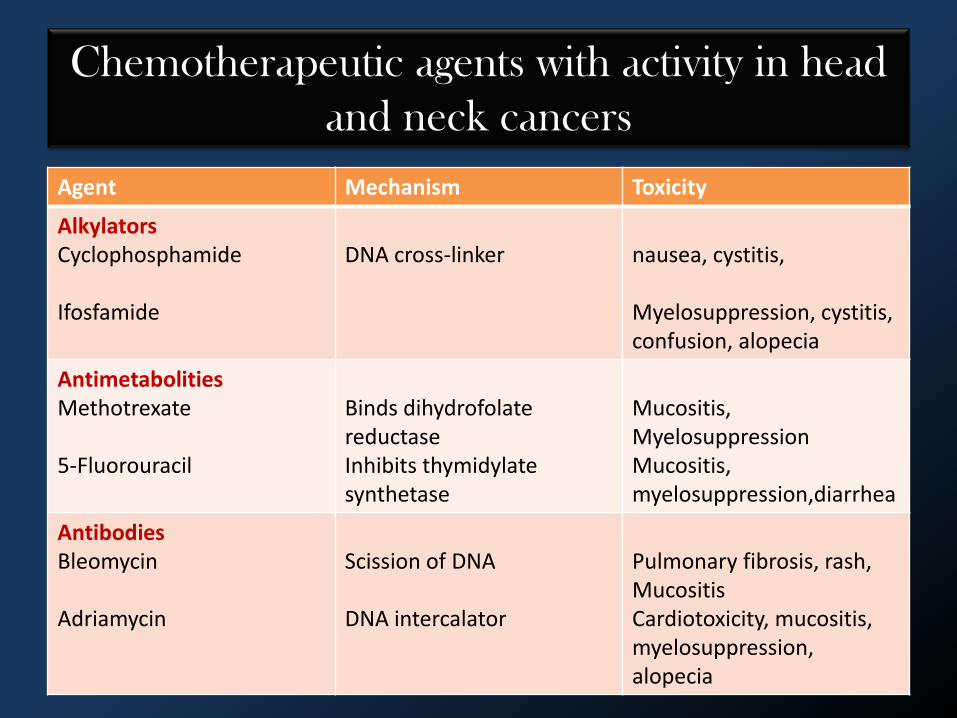
Agent Mechanism Toxicity
AlkylatorsCyclophosphamide
Ifosfamide
DNA cross-linker nausea, cystitis,
Myelosuppression, cystitis, confusion, alopecia
Antimetabolities Methotrexate
5-Fluorouracil
Binds dihydrofolate reductaseInhibits thymidylate synthetase
Mucositis, MyelosuppressionMucositis, myelosuppression,diarrhea
AntibodiesBleomycin
Adriamycin
Scission of DNA
DNA intercalator
Pulmonary fibrosis, rash, MucositisCardiotoxicity, mucositis, myelosuppression, alopecia
Chemotherapeutic agents with activity in head
and neck cancers
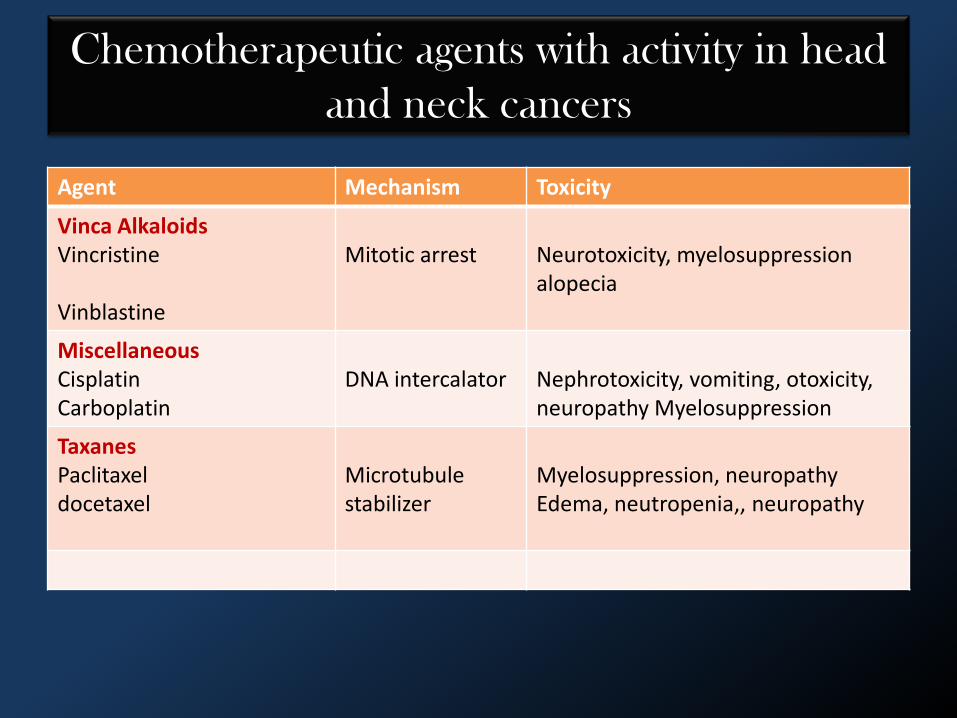
Agent Mechanism Toxicity
Vinca AlkaloidsVincristine
Vinblastine
Mitotic arrest Neurotoxicity, myelosuppression alopecia
MiscellaneousCisplatinCarboplatin
DNA intercalator Nephrotoxicity, vomiting, otoxicity, neuropathy Myelosuppression
TaxanesPaclitaxeldocetaxel
Microtubule stabilizer
Myelosuppression, neuropathyEdema, neutropenia,, neuropathy
Chemotherapeutic agents with activity in head
and neck cancers
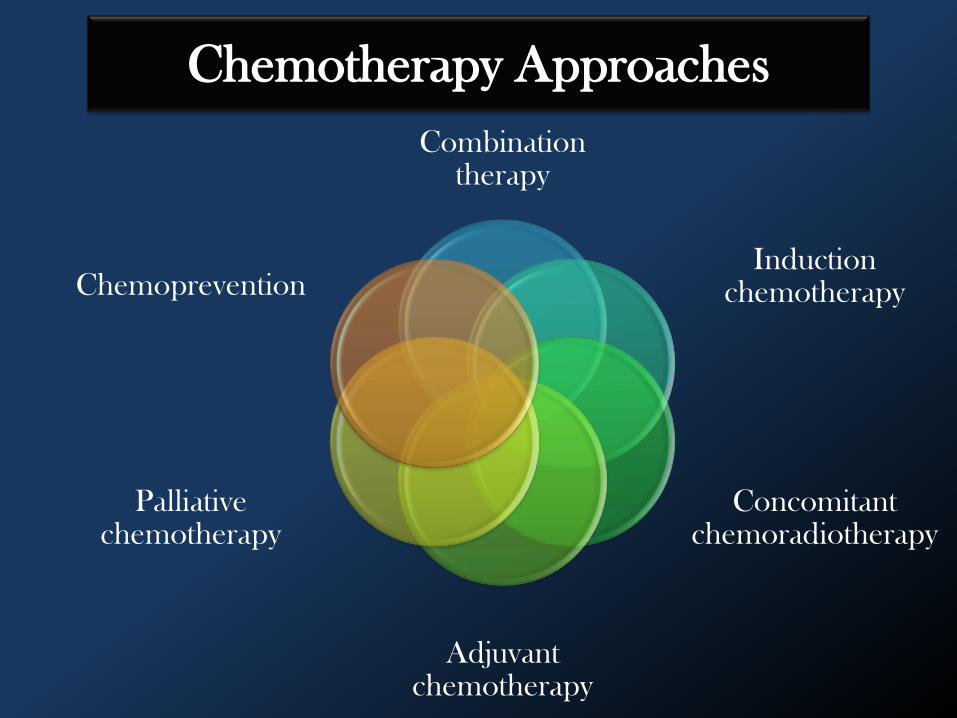
Chemotherapy Approaches
Combination therapy
Induction chemotherapy
Concomitant chemoradiotherapy
Adjuvant chemotherapy
Palliative chemotherapy
Chemoprevention

CHEMOPREVENTION
• The term was given by Michael BSporn in 1976
• More than 2000 agents from more than 20 chemical classes –chemopreventive activity – important ones are:– Retinoids– β carotene– α tocopherol
Molecular mechanism of retinoids
• Nuclear retinoid receptors – ligand activated DNA binding protein – modulate gene transcription.
• Upto 30-40% premalignant lesion regress spontaneously.
Palliative Chemotherapy
• Primary goal - improve quality of life. • Accomplished by
– relieving pain, – preserving or improving organ function, – preventing obstruction of the airway or esophagus.
Single Agent Methotrexate Therapy
• The standard palliative therapy for head and neckcancer.
• Well tolerated, convenient, and inexpensive.• Response rates range from 15% to 30%, with a
median duration that has generally been less than 6months

METHOTREXATE
• It is one of the oldest and highly efficacious antineoplastic drugs;
• Relatively nontoxic, inexpensive, and convenient.
MECHANISM OF ACTION
Folic acid analog that is S-phase specific.
Binding to the enzyme dihydrofolate
reductase,
Blocks the reduction of dihydrofolate to
tetrahydrofolic acid.
Tetrahydrofolic acid is necessary for the
synthesis of thymidineand purine synthesis.
Interrupts the synthesis of DNA, RNA, and
protein.
• Methotrexate is absorbed orally, 50% plasma protein boundlittle metabolized and largely excreted unchanged in urine.
• Methotrexate can be administered by intramuscular injectionor subcutaneous, intravenous oral routes.-- 2.5mg tabs,5 15,50 mg/vial inj..
• Aspirin and sulfonamides decrease its renal tubular secretion.These drugs enhance the toxicity of Mtx.
• Mechanisms for resistance to methotrexate include ,decreased transport of methotrexate into cells and increaseddihydrofolate reductase activity.
Toxicity
• Moderate dose– Mild stomatitis. – Exfoliate maculo-papular rash
• Renal dysfunction -because of precipitation of the drug, especially in acid urine.
• Hydration and alkalinization of the urine before and after methotrexate administration can reduce risk.

CISPLATIN
• inorganic metal coordination complexwith major anti-tumor activity in anumber of diseases.
• behaves as a bi-functional alkylatingagent binding to DNA to cause inter-strand and intra-strand cross-linking.
• also binds to nuclear and cytoplasmicproteins.
• Resistance is believed to develop through increased metabolic inactivation.
• Cisplatin is administered by the intravenous route and requires hydration and diuresis to prevent renal tubular damage.
• The major toxic reaction is renal dysfunction,
• Nausea and vomiting are almost universal. Ototoxicity can occur. Hematologic toxicity, including neutropenia and thrombocytopenia, is mild ,bone marrow suppression
CISPLATIN
• Resistance is believed to develop through increased metabolic inactivation.
• Cisplatin is administered by the intravenous route and requires hydration and diuresis to prevent renal tubular damage.
• The major toxic reaction is renal dysfunction,
• Nausea and vomiting are almost universal. Ototoxicity can occur. Hematologic toxicity, including neutropenia and thrombocytopenia, is mild ,bone marrow suppression
CISPLATIN

Taxanes
• New class of compounds
• include paclitaxel (taxol) and docetaxel (taxotere).
• active against a variety of solid tumors
• prolonged infusions - more effective.
• response rates of approximately 30% to 40%.

Mechanism Of Action
Binding to the B-subunit of tubulin,
Stabilizing microtubules
Inhibiting microtubule de-polymerization,
Cell cycle arrest at G.
Dosage
• Paclitaxel - 135 to 250 mg/m2 given over 3 or 24 hours.
• Docetaxel - 60 to 100 mg/m2 by bolus injection every 3 weeks.
IFOSFAMIDE
• Congener of cyclophosphamide.
• DNA interstrand and intrastrandcross-linking that disrupts DNA replication.
• its metabolites are excreted in the urine.
Dosage
• Total doses of 7 to 10 g/m2 usually is administered as a 5-day continuous infusion or over 3 to 5 days in equally divided doses.
• Need to be well hydrated before drug administration.
BLEOMYCIN
• Anti-neoplastic antibiotic which is a
mixture of closely relatedglycopeptides.
• Chelates copper or iron - producessuperoxide ions - intercalates betweenDNA strands - Causes chain scissionand inhibits repair

Mechanism Of Action
• Binds to DNA and produces DNA strand breaks by generating oxygen free-radicals.
• 10 to 20 units/m2 or twice weekly IM/IV
• continuous 24-hour infusion over 5 or 7 days at a dose of 10 units/m2 each 24 hours.
DOSAGE

5-FLUOROURACIL (5-FU)
PYRIMIDINE ANTAGONISTS
• Converted in the body to -corresponding nucleotide 5 ~ fluoro -2 -deoxyuridine monophosphate, -which inhibits thymidylatesynthetase.
• Fluorouracil itself gets incorporated into nucleicacids and this may contribute to its toxicity.
• Even resting cells are affected though rapidlymultiplying ones are more susceptible
• response rates of 15%,
• used in combination with other agents, particularly cisplatin.
5-FLUOROURACIL (5-FU)

Dose
• Conventional intravenous dose -10 to 15 mg/kg weekly
• Alternate method of delivery -loading dose of 400 to 500 mg/m.sq daily for 5 days, followed by a weekly intravenous dose of 400 to 500 mg/m.sq
NO MORE THAN 800 MG GIVEN AS A SINGLE BOLUS.
ALKYLATING AGENTS
• These compounds produce highly reactive carbonium ion.
• This results in cross linking/ abnormal base pairing/scissionof DNA strand.
• Alkylating agents have cytotoxic and radiomimetic(likeionizing radiation) actions

• It has prominent immunosuppressant property. Thusit is one of the most popular anti cancer drugs.
• Mechanism Of Action– cross-linking DNA strands, preventing further
division.• Can be given orally or intravenously.
• single dose of 500 to 1500 mg/m2 repeated every 3 or 4weeks.
Cyclophosphamide
Vinblastine and VincristineMECHANISM OF ACTION • These are mitotic inhibitors, bind to
microtubular protein tubulin , prevent itspolymerization and assembly of microtubules.
• Cause disruption of mitotic spindle andinterfere with cytoskeletal function .
• The chromosomes fail to move apart duringmitosis, metaphase arrest occurs.
Vinca Alkaloids
Dose
• Vinblastine (Velban) – given weekly at 5 mg/m2 or it may be given by
continuous infusion over several days.
• Vincristine (Oncovin) – 1.0 to 1.5 mg/m2 once or twice monthly.
– single dose not exceed 2 mg.

MECHANISM OF ACTION
Inhibits Ribonucleotide Reductase
Interfering with the conversion of ribonucleotide to deoxyribonucleotide
Causing inhibition of DNA synthesis.
Hydroxyurea
New Single Agents
New Single Agents
Topotecan Gemcitabine VinorelbineAnalogs of
methotrexate
• Median duration of response ranges from 2 to 6 months.
• ECOG study
• SWOG Study
COMBINATION THERAPY

ECOG Study
Cisplatin
Bleomycin & Methotrexate Methotrexate.
•Response to single agent therapy with methotrexate was 35%, and to the combination 48%.•Toxicity was greater-for the combination with no difference in survival time.

SWOG Study
Cisplatin and 5-FU Methotrexate.
•Cisplatin and 5-FU arm was associated with significantly more toxicity than methotrexate.•Carboplatin and 5-FU were intermediate in toxicity. • Median survival times were not different, varying between 4.7 and 6.6 months.
Carboplatin and 5-FU
Ways Of Combined Chemotherapy
Benefits
• Increased compliance • Better tolerance of therapy. • Reduce tumor burden • Resulting in the preservation of organ function
by obviating the need for surgery. • Reduce metastatic seeds • Eliminate problems with poor vascularity that
often occur after surgery or radiation, thus reducing a potential pharmacologic sanctuary.
Induction Chemotherapy
• First use of induction chemotherapy – methotrexate with leucovorin rescue given twice
before surgery. – 77% of patients had some tumor shrinkage,
• Other studies – methotrexate and bleomycin. – response rate was approximately 5%
Disadvantages
Delay in potentially curative surgery or radiotherapy, or both, in tumors with chemoresistant cells. -can result in selective proliferation of clones, which are less responsive to radiotherapy.
Patients may refuse potentially curative follow-up radiotherapy or surgery because of tumor response to initial chemotherapy.
Increased morbidity and costs of treatment.
Concomitant Chemoradiotherapy :
• Primarily in patients with unresectable disease to improve local and regional control.
• Theoretic rationale and mechanism for the interaction between cytotoxic drugs and radiation that results in additive or synergistic enhancement -mechanisms.
• Net effect - improve cellular cytotoxicity.
Adjuvant (Maintenance) Chemotherapy
• Subsequent to definitive locoregional therapy, adjuvant chemotherapy has been given to control microscopic residual disease and micrometastatic disease.
• Although there appears to be some reduction in the incidence of distant metastases, adjuvant therapy has not been demonstrated to improve survival.
• At this time, adjuvant chemotherapy has not been shown to have a role in management of carcinomas of the head and neck
Intra-arterial Chemotherapy
• Based on delivering an increased drug concentration to the tumor bed, with possible avoidance of systemic toxicity
• Intra-arterial cisplatin given before surgery or radiation has produced responses in the 70% to 80% range.
Intralesional Chemotherapy
• Intralesional injection of vinblastine, vincristine, or interferon has been shown to be effective in the local control of epidemic Kaposi’s sarcoma and can be used in combination with systemic chemotherapy or radiotherapy.
• If necessary, lesions are reinjected at 3-to-6-week intervals.
TOPICAL CHEMOTHERAPY
• Actinic keratotic lesions have been effectively treated with the application of 5% fluorouracil cream--applied twice daily until the area exhibits a significant inflammatory reaction (usually 3 to 4 weeks).
• Similar topical application of fluorouracil in selected cases of multiple superficial basal cell carcinomas, as may be seen in basal cell nevus syndrome, has been effective.
• Topical therapy, however, is not effective for invasive lesions and results in needless delay in definitive therapy

Chemotherapy Regimen
Concurrent chemoradiation for stage III, IVA and IVB cancer
• Cisplatin + RTCisplatin (CDDP) 100 mg/m2 iv d1, 22 and 43Concurrent radiotherapy 2 Gy/d to a total of 70 Gy
• 5-FU + Carboplatin + RTCarboplatin (Paraplatin) 70 mg/m2/d iv d1-4, 22-25 and 43-465-FU 600 mg/m2/d civi d1-4, 22-25 and 43-46Concurrent radiotherapy 2 Gy/d to a total of 70 Gy
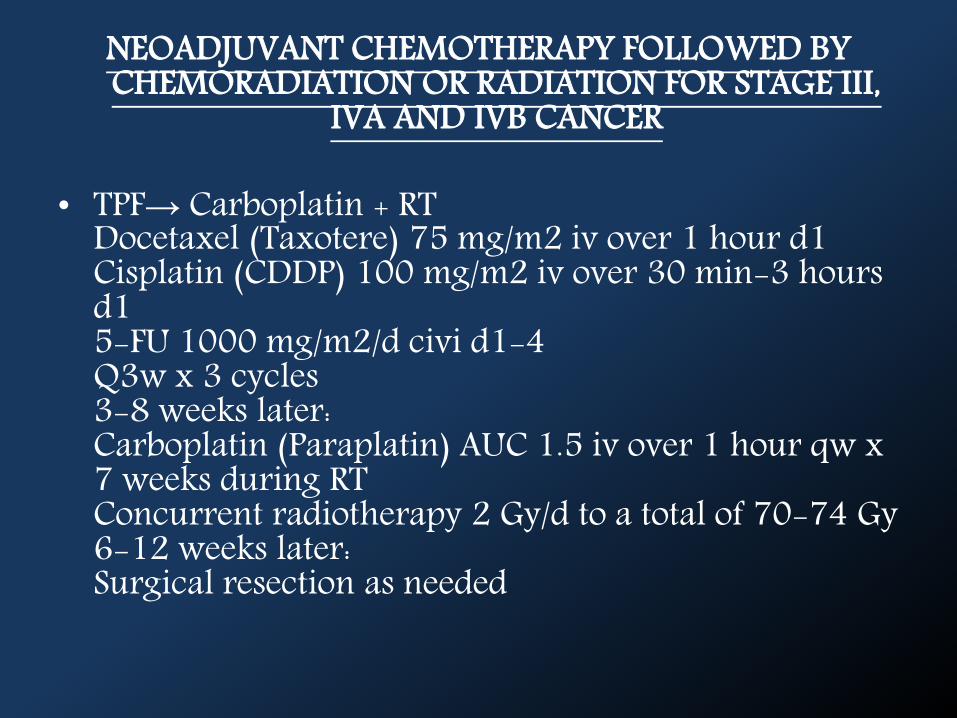
NEOADJUVANT CHEMOTHERAPY FOLLOWED BY CHEMORADIATION OR RADIATION FOR STAGE III,
IVA AND IVB CANCER
• TPF→ Carboplatin + RTDocetaxel (Taxotere) 75 mg/m2 iv over 1 hour d1Cisplatin (CDDP) 100 mg/m2 iv over 30 min-3 hours d15-FU 1000 mg/m2/d civi d1-4Q3w x 3 cycles3-8 weeks later:Carboplatin (Paraplatin) AUC 1.5 iv over 1 hour qw x 7 weeks during RTConcurrent radiotherapy 2 Gy/d to a total of 70-74 Gy6-12 weeks later:Surgical resection as needed
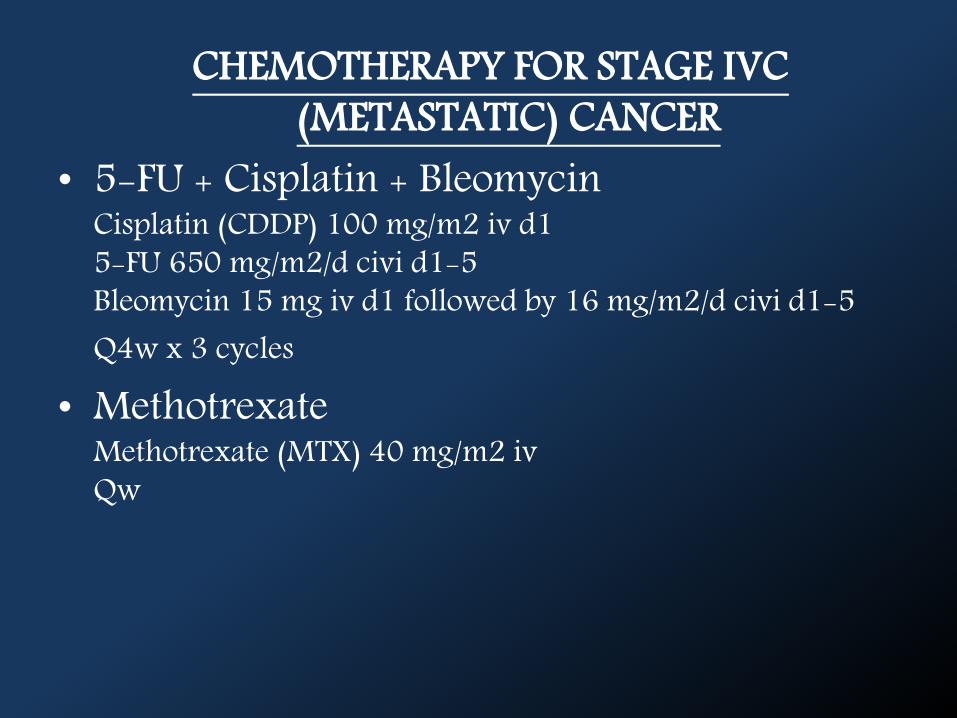
CHEMOTHERAPY FOR STAGE IVC (METASTATIC) CANCER
• 5-FU + Cisplatin + BleomycinCisplatin (CDDP) 100 mg/m2 iv d15-FU 650 mg/m2/d civi d1-5Bleomycin 15 mg iv d1 followed by 16 mg/m2/d civi d1-5Q4w x 3 cycles
• MethotrexateMethotrexate (MTX) 40 mg/m2 ivQw
CHEMO CYCLES
6 CYCLE SINGLE DOSE
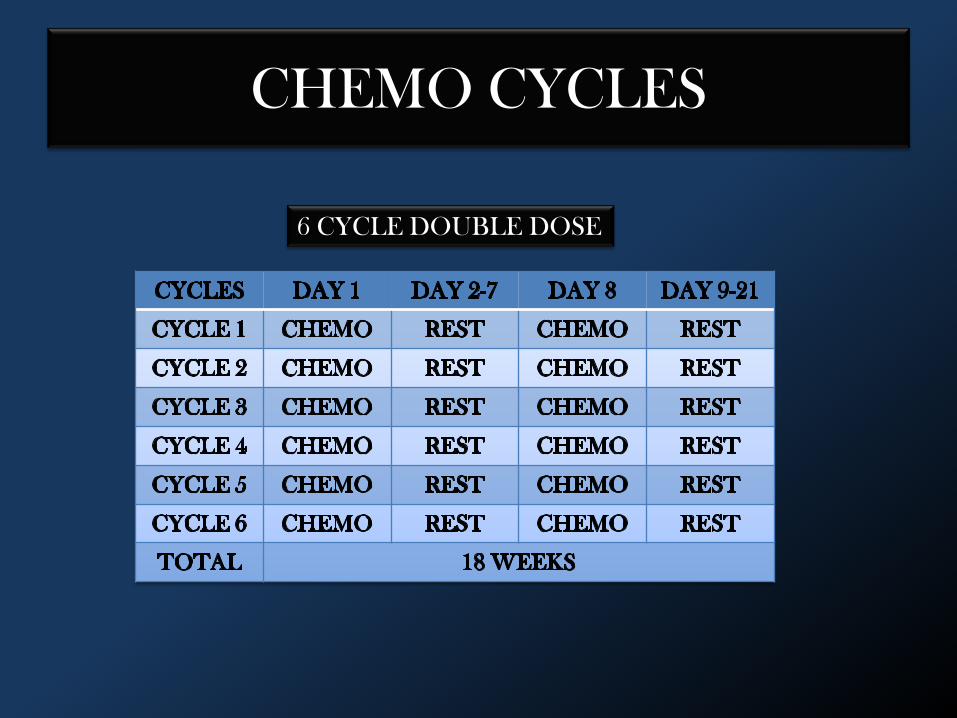
CHEMO CYCLES
6 CYCLE DOUBLE DOSE
BLOOD TEST AND CHEMOTHERAPY
• Leukopenia• Thrombocytopenia.• Anemia.
CHEMOTHERAPY REGIME• CBC should be done before and 7 days after starting
Chemo drugs as well as after any dose increase. Thereafter, the blood counts can be monitored every 2 to 4 weeks.
SIDE EFFECTS OF CHEMOTHERAPY
1. Sore Mouth2. Loss / Change Of Taste3. Nausea / Vomiting4. Loss Of Appetite5. Constipation6. Diarrhoea7. Lymphedema8. Hair Loss ( Alopecia)9. Infertility

Sore Mouth
Loss / Change Of Taste
Nausea / Vomiting
Loss Of Appetite

Constipation

Diarrhoea

Lymphedema

Hair Loss
Infertility
Dental treatment considerations in the
chemotherapy patient
1.Infections2.Neurological & Dental Alterations3.Dysgeusia4.Hyposialia & Xerostomia5.Bleeding Tendency6.The Development Of Osteonecrosis.
BEFORE CHEMOTHERAPY
DURING CHEMOTHERAPY
AFTER CHEMOTHERAPY
BEFORE CHEMOTHERAPY
• Exhaustive examination of the oral cavity• Denture fitting should be checked• Radiological study• General prophylactic measures• Teeth that are Non-viable or Poor prognosis:
– Minor surgery: al least two weeks before chemotherapy.
– Major surgery: 4-6 weeks before chemotherapy.
DURING CHEMOTHERAPY
• Treatment of the oral complications of chemotherapy.
• Continued patient reminder of the need to maintain strict dental hygiene
• No elective dental treatment should be carried out.
• ONLY emergency dental care.

AFTER CHEMOTHERAPY
• Insist on the need for routine systematic oral hygiene.– Use of chlorhexidine rinses and fluorization.
• Elective dental treatment.
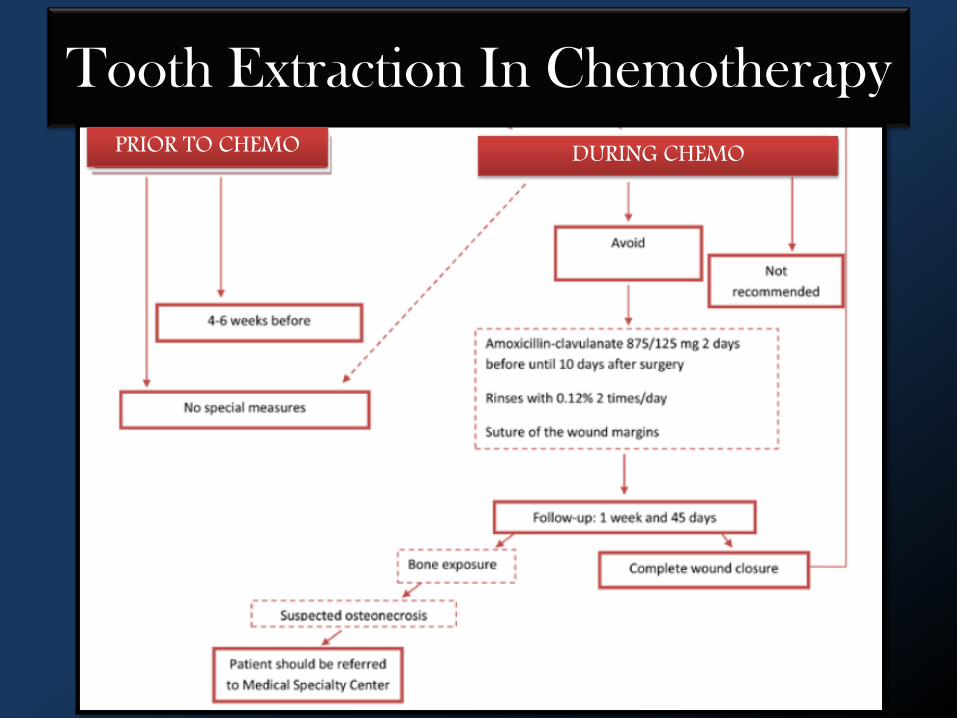
Tooth Extraction In Chemotherapy
PRIOR TO CHEMO DURING CHEMO
CHEMOTHERAPY SAFETY
• They can cause abnormal changes in DNA. (They are mutagenic.)
• They may be able to alter development of a fetus or embryo, leading to birth defects.
• They may be able to cause another type of cancer. • Some may cause skin irritation or damage.
• Wear double gloves, goggles, and gowns.• Proper ventilation systems to avoid spattering
and/or inhaling the droplets that can form while mixing.
• Special precautions when handle urine and stool.
• Use of separate plastic containers to dispose of sharp items, syringes, IV tubing & medicine bags.


Recent Advances InChemotherapy
• Bacterial treatments – clostridium novyi• HAMLET (human alpha-lactalbumin made
lethal to tumor cells)• Insulin potentiation therapy• Telomerase therapy – Inositol hexaphosphate• Electrochemotherapy
BIBLIOGRAPHY
1. CANCER-PRINCIPLE AND PRACTICE OF ONCOLOGY- DE-VITA, ROSENBERG2. HEAD AND NECK CANCER – J.P SHAH3. CANCER OF FACE AND MOUTH- IAN MC’GREGOR4. MEDICAL PHARMACOLOGY- K.D TRIPATHI5. MAXILLOFACIAL SURGERY- PETER WARD BOOTH6. HEAD AND NECK CANCER –EMERGING PERSPECTIVES-JOHN.F ENSLEY7. HEAD AND NECK CANCER- FEE, GOEFERT8. Myers, Suen ‘cancer of the head and neck’ 2003, 4th edition9. WWW.WIKIPEDIA.ORG10. WWW.CANCER.COM






























