Embed Size (px)
Citation preview

Hematol Oncol Stem Cell Ther (2016) 9, 71–75
Avai lab le a t www.sc ienced i rec t .com
ScienceDirect
journal homepage: www.elsev ier .com/ locate /hemonc
CASE REPORT
Chediak–Higashi syndrome presentingin accelerated phase: A case reportand literature review
http://dx.doi.org/10.1016/j.hemonc.2015.07.0021658-3876/� 2015 King Faisal Specialist Hospital & Research Centre. Published by Elsevier Ltd.This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
* Corresponding author at: Faculty of Medicine, Pediatric Depart-ment, Hedi Chaker Hospital, El Ain Street Km 0,5, 3029 Sfax, Tunisia
E-mail address: [email protected] (I. Maaloul).
I. Maaloul a,*, J. Talmoudi a, I. Chabchoub a, L. Ayadi b,a, T.H. Kamoun a,T. Boudawara b, C.H. Kallel c, M. Hachicha a
a Faculty of Medicine, Pediatric Department, Hedi Chaker Hospital, Sfax, Tunisiab Faculty of Medicine, Anatomical Pathology Laboratory, Habib Bourguiba Hospital, Sfax, Tunisiac Faculty of Medicine, Laboratory of Hematology, Habib Bourguiba Hospital, Sfax, Tunisia
Received 10 September 2014; accepted 15 July 2015Available online 1 August 2015
KEYWORDSAccelerated phase;Chediak–Higashi syndrome;Hematology;Treatment
Abstract
Chediak–Higashi syndrome (CHS) is a rare autosomal recessive lysosomal disorder characterizedby frequent infections, oculocutaneous albinism, bleeding diathesis, and progressive neurologicdeterioration. In 85% of cases, CHS patients develop the accelerated phase characterized bypancytopenia, high fever, and lymphohistiocytic infiltration of liver, spleen, and lymph nodes.Treatment of accelerated-phase CHS is difficult and the prognosis is poor. Here, we report a caseof CHS in a 2-year-old boy who presented in the accelerated phase of the disease. CHS diagnosiswas made on the basis of clinical characteristics, hair analysis, and identification ofpathognomonic giant azurophilic granules in peripheral blood and bone marrow.� 2015 King Faisal Specialist Hospital & Research Centre. Published by Elsevier Ltd. This is anopen access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Chediak Higashi syndrome (CHS) is a rare autosomalrecessive disorder with fewer than 500 cases publishedworldwide over the last 20 years [1]. The largest CHS studyto date included 15 patients [2]. In Tunisia, Bouatay et al.
(2014) [3] reported a single case of CHS. The clinicalfeatures of this syndrome include partial albinism, photo-sensitivity, severe recurrent bacterial infections, bleedingdiasthesis, and late onset neurological manifestations (cen-tral and peripheral neuropathies, sensory loss, muscleweakness, parkinsonism, cerebellar ataxia, and cognitiveimpairment) [4,5]. Approximately 85% of cases develop afatal accelerated phase characterized by pancytopenia,

72 I. Maaloul et al.
hemophagocytosis, and marked infiltration of organs bylymphocytes, leading to multi-organ dysfunction [6].
Owing to the rarity of the condition and the characteristicclinical and hematological findings, we report a case of Che-diak–Higashi syndrome, which presented as accelerated phase.
Case report
The patient is a 2-year-old male that presented with amonth-long history of fever, abdominal distension, and
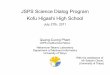
Figure 2 Bone marrow aspirate (A–C) and peripheral blood (D) smgranules.
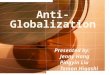
Figure 1 Face of the patient. Note skin hypopigmentationand blond hair.
cough. There was a prior history of repeated attacks oflow respiratory-tract infections and he developedosteomyelitis at 1 year of age. He is the third child from aconsanguineous marriage, displays normal psychomotordevelopment, and there is no family history of the disease.On examination, the patient was febrile, of average build,weighed 14 kg, and had blond hair and hypopigmentationof the skin (Figure 1). The child was anemic, with cervicaland axillary lymphadenopathy. Respiratory system examina-tion revealed moderate respiratory distress with bilateralcoarse crepitations. The patient had a protuberant abdo-men with massive hepatosplenomegaly. The cardiovascularand nervous systems were normal.
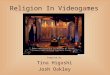
Laboratory investigations showed elevated C-reactiveprotein (132 mg/L), hyponatremia (124 mmol/L), high fer-ritin levels (2685 ng/mL), low fibrinogen levels (<1.5 g/L),and hypertriglyceridemia (3.57 mmol/L). The relevanthematological findings were hemoglobin 5.2 g/dL, leucope-nia at 3.56 � 109/L, and thrombocytopenia (Platelet count26 � 109/L). Peripheral blood smear showed several abnor-mal giant granules in most leukocytes. Bone marrow aspi-rate revealed prominent granules within the lymphocytesand myeloid cells (Figure 2). Phagocytosis of red blood cellsand red-blood-cell precursors hemophagocytosis was alsoobserved (Figure 3).
The patient fulfilled the diagnostic criteria forhemophagocytic lymphohistiocytosis (HLH), e.g., prolongedfever, splenomegaly pancytopenia, high ferritin levels, lowfibrinogen levels, hypertriglyceridemia, and hemophagocy-tosis. Thus, the diagnosis of accelerated phase of CHS was
ear showing myeloid precursor and lymphocytes with abnormal

Chediak–Higashi syndrome 73
made on the basis of clinical presentation (hypopigmenta-tion, blond hair) and hematological findings (giant azurophi-lic granules in leukocytes).
Figure 3 Bone marrow aspirate showing hemophagocytosis.
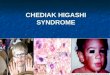
Figure 4 Microscopic examination of the hair shaft shows atypical pattern of evenly distributed, regular melanin granuleslarger than those seen in normal hairs (hematoxylin–eosin,original magnification �400).
Figure 5 Chest tomography showing
Blood and urine cultures were negative. Serologies ofEpstein–Barr virus, cytomegalovirus, and Aspergillus werenegative. Because of recurrent and severe infections, weinitiated immune-system investigation. The patient had nor-mal immunoglobulin levels and T and B cells (CD3, CD4,CD8, and CD19) were examined using flow cytometry, how-ever, chemotaxis of natural killer cells was not studied.Optical microscopy examination of the hair showed groupsof pigment scattered along the length of the hair shafts,contrasting with the normal pattern of fine, diffuse pigmen-tation (Figure 4). Chest X-ray showed opacities in interest-ing bilateral lower zones. Chest computed tomographyshowed two cavitary lesions of the middle right pulmonarylobe (Figure 5). Abdominal ultrasound revealed hep-atosplenomegaly with a normal echo pattern.
The child was treated with ceftazidime, Vancomycin,and fluconazole. He received high doses of intravenous gam-maglobulin (1 g/kg per day for 2 days). He also receivedmultiple transfusions, including platelets and packed redblood cells for anemia. He died 7 days after admissionbecause of status epilepticus and multi-organ failure.
Discussion
CHS was first described over 60 years ago by Beguez-Cesar(1943) [7] in three siblings bearing the main clinical featuresof neutropenia and abnormal granules in leukocytes. Che-diak, a Cuban hematologist, reported another case in 1952[8] and in 1954, Higashi, a Japanese pediatrician, describeda series of cases finding misdistribution of myeloperoxidasein the neutrophilic granules of affected patients [9]. CHS is arare disease (approximately 500 cases reported worldwide),the prevalence and incidence of which are unknown. In anationwide survey in Japan, 15 patients were diagnosed dur-ing a period of 11 years (2000–2010), indicating that one ortwo patients with CHS were diagnosed each year [2].
The mean age of onset is 5.85 years, however, mostpatients die before age 10. In patients that do survivebeyond childhood, neurological problems persist and/orincrease in magnitude [10].
cavitary lesions in the right lung.

74 I. Maaloul et al.
CHS is characterized by partial oculocutaneous albinism,repeated infections, and pathognomonic abnormal giantgranules in neutrophils, lymphocytes, monocytes, andplatelets. Patients develop recurrent infections that mostcommonly involve the skin and respiratory system.Staphylococcus aureus and beta-hemolytic Streptococcusare the predominant organisms. Viral and fungal infections,however, have also been described [11]. Increased suscepti-bility to recurrent infections is attributed to defects inT-cell cytotoxicity and natural killer function and defectsin granulocyte chemotaxis and bactericidal activity [12].
The accelerated phase is observed in 85% of individualsand can occur at any age, including shortly after birth orwithin several years. Clinical manifestations include fever,lymphadenopathy, hepatosplenomegaly, anemia, neutrope-nia, thrombocytopenia, and neurological abnormalities [10].Originally thought to be a malignancy resembling lymphoma,the accelerated phase is now known to be an HLH character-ized by multi-organ inflammation. The accelerated phaseand its complications are the most common cause of mortal-ity in individuals with CHS [11]. Prognosis associated with theaccelerated phase is poor. In an Indian study of five childrenwith CHS, accelerated phase was seen in three cases, with allthree resulting in fatal outcomes [13].
Clinical and laboratory findings by Farhoudi et al. (2003)[14] in six cases of CHS reported hypopigmentation of theskin, silvery hair, photophobia, and nystagmus observed inall patients, a history of recurrent infections in four patients,and accelerated-phase progression in three patients.
Roy et al. (2011) [13] studied the clinico-hematologicalprofile of five cases of CHS, reporting that all patients hadsilvery hair, partial albinism, photophobia, and recurrentskin and/or chest infection, with three of them (50%) pre-senting an accelerated phase.
Of the 15 patients enrolled in the Japanese study [2], 10(67%) had recurrent bacterial infections, five (33%) devel-oped life-threatening HLH, and one patient had complicatedmalignant lymphoma. Our patient had hypopigmented skin,blond hair, a history of recurrent low respiratory tract infec-tions, and had developed osteomyelitis 1 year ago.
The genetic hallmark of CHS is mutations in the CHS1/LYST gene located on chromosome 1q42–43 [15]. Mutationsof this gene result in a defect in granule morphogenesis inmultiple tissues [4]. The gene encodes a protein called thelysosomal trafficking regulator [16] which regulates thesynthesis, transport, and fusion of cytoplasmic vesicles.The abnormalities observed in these vesicles result in grosslyenlarged and nonfunctional lysosomes, which are identifiedduring cytology as giant coalesced azurophilic granulespresent mostly in granulocytes and monocytes, but alsofibroblasts, melanocytes, astrocytes, Schwann cells, andhematopoietic cells [16]. These granules are specific toCHS and their presence in granulocytes from peripheralblood and bone marrow is the basis of diagnosis [4].
Clinical CHS phenotypes correlate with molecular geno-types. CHS patients with deletions in the LYST gene usuallypresent with a fulminant accelerated phase early in life,whereas, those with missense mutations have a better prog-nosis, characterized by the absence of an accelerated phaseand no neurological involvement [17]. Our patient had arapidly fatal course, thus, genetic analysis has not beenundertaken.
The only treatment that cures the hematologic andimmunologic defects is allogenic hematopoietic stem celltransplantation (HSCT), but this therapy does not preventthe progressive neurological dysfunction frequentlyobserved during long-term follow up [1,11].
A conditioning regimen, described in detail by Haddadet al. (1995) [18], generally includes a combination of etopo-side, busulfan, and cyclophosphamide. The current standardof care is HSCT as soon as the diagnosis is confirmed and theaccelerated phase has either been ruled out or is in remis-sion. The most favorable outcome is achieved when HSCTis performed prior to development of the accelerated phase.
If signs of the accelerated phase are present,hemophagocytosis must be brought into clinical remissionbefore HSCT can be performed. Guidelines for treatmentof the accelerated phase, revised in 2004 [19], are the sameas those for familial hemophagocytic lymphocytic lympho-histiocytosis. Combination therapy consists of etoposide,dexamethasone, and cyclosporine A. Remission is achievedin 75% of individuals within 8 weeks [20] however, relapsesare common and response to treatment declines over time.Once remission occurs, prompt HSCT is recommended.
Conclusion
CHS is a rare disease with a varied spectrum of clinical pre-sentation and investigation findings. The prognosis of theaccelerated phase is poor. HSCT is the only curative treat-ment for hematological and immunological disorders. Weemphasize the need for early diagnosis on basis of charac-teristic clinical findings and diagnostic laboratory examina-tions, which leads to early transplantation beforedevelopment of the accelerated phase.
Conflicts of interest
The authors declare no conflicts of interest.
References
[1] Kaplan J, De Domenico I, Ward DM. Chediak–Higashi syn-drome. Curr Opin Hematol 2008;15(1):22–9, Review.
[2] Nagai K, Ochi F, Terui K, Maeda M, Ohga S, Kanegane H, et al.Clinical characteristics and outcomes of Chediak–Higashisyndrome: a nationwide survey of Japan. Pediatr Blood Cancer2013;60:1582–6.
[3] Bouatay A, Hizem S, Tej A, Moatamri W, Boughamoura L,Kortas M. Chediak–Higashi syndrome presented as acceleratedphase: case report and review of the literature. Indian JHematol Blood Transfus 2014;30(1):S223–6.
[4] De Azambuja AP, DoNascimento B, Comar SR, Loth G, RibeiroLL, Bonfim C, et al. Four cases of Chediak–Higashi syndrome.Rev Bras Hematol Hemoter 2011;33:315–22.
[5] Bhambhani V, Introne WJ, Lungu C, Cullinane A, Toro C.Chediak–Higashi syndrome presenting as young-onset levo-dopa-responsive parkinsonism. Mov Disord 2013;28:127–9.
[6] Bharti S, Bhatia P, Bansal D, Varma N. The accerated phase ofChediak–Higashi syndrome: the importance of hematologicalevaluation. Turk J Hematol 2013;30:85–7.
[7] Beguez-Cesar A. Neutropeneiacronicamaligna familiar congranulaciounesatipicas de los leucocitos. Bol Soc CubanaPediatr 1943;15:900–22.

Chediak–Higashi syndrome 75
[8] Chediak MM. New leukocyte anomaly of constitutional andfamilial character. Rev Hematol 1952;7:362–7.
[9] Higashi O. Congenital gigantism of peroxidase. Tohoku J ExpMed 1954;59:315–22.
[10] Usha HN, Prabhu PD, Sridevi M, Baindur K, Balakrishnan CM.Chediak–Higashi syndrome. Indian Pediatr 1994;34:1115–9.
[11] Dotta L, Parolini S, Prandini A, Tabellini A, Antolini M,Kurtzberg J, et al. Clinical, laboratory and molecular signs ofimmunodeficiency in patients with partial oculo-cutaneousalbinism. Orphanet J Rare Dis 2013;8:168.
[12] Pujani M, Agarwal K, Bansal S, Ahmad I, Puri V, Verma D, et al.Chediak–Higashi syndrome: a report of two cases with unusualhyperpigmentation of the face. Turk Patoloji Derg2011;27:246–8.
[13] Roy A, Kar R, Basu D, Srivani S, Badhe BA. Clinico-hematolog-ical profile of Chediak Higashi: experience from a tertiary carecenter in south India. Indian J Pathol Microbiol2011;54:547–51.
[14] Farhoudi A, Chavoshzadeh Z, Pourpak Z, Izadyar M, Gharago-zlou M, Movahedi M, et al. Report of six cases of Chediak–Higashi syndrome with regard to clinical and laboratoryfindings. Iran J Allergy Asthma Immunol 2003;2(4):189–92.
[15] Barrat FJ, Auloge L, Pastural E, Lagelouse RD, Vilmer E, CantAJ, et al. Genetic and physical mapping of the Chediak–Higashi syndrome on chromosome 1q42–43. Am J Hum Genet1996;59:625–32.
[16] Olkkonen VM, Ikonen E. Genetic defects of intracellular-membrane transport. N Engl J Med 2000;343:1095–104.
[17] Westbroek W, Adams D, Huizing M, Koshoffer A, Dorward H,Tinloy B, et al. The severity of cellular defects inChediak–Higashi syndrome correlate with the molecular geno-type and clinical phenotype. J Invest Dermatol 2007;127:2674–7.
[18] Haddad E, Le Deist F, Blanche S, Benkerrou M, Rohrlich P,Vilmer E, et al. Treatment of Chediak–Higashi syndrome byallogenic bone marrow transplantation: report of 10 cases.Blood 1995;85:3328–33.
[19] Henter JI, Horne A, Arico M, Egeler RM, Filipovich AH,Imashuku S, et al. HLH 2004: diagnostic and therapeuticguidelines for hemophagocytic lymphohistiocytosis. PediatrBlood Cancer 2007;48:124–31.
[20] Filipovich AH. Hemophagocytic lymphohistiocytosis andrelated disorders. Curr Opin Allergy Clin Immunol 2006;6:410–5.