Embed Size (px)
Citation preview

Supplementary appendixThis appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors.
Supplement to: Overman MJ, McDermott R, Leach JL, et al. Nivolumab in patients with metastatic DNA mismatch repair-deficient or microsatellite instability-high colorectal cancer (CheckMate 142): an open-label, multicentre, phase 2 study. Lancet Oncol 2017; published online July 19. http://dx.doi.org/10.1016/S1470-2045(17)30422-9.

1
Supplementary Appendix Contents
Supplementary methods 2
Table S1: Study sites and investigators 3
Table S2: Concordance between local and central assessments of dMMR/MSI-H status 4
Table S3: Summary of patients with discrepancies between local and central assessments of dMMR/MSI-H status 5
Table S4: Objective response rate, best overall response, and disease control rate in patients with non–MSI-H and microsatellite status not reported metastatic or recurrent colorectal cancer per central assessment of MSI-H status
6
Table S5: Summary of time to and duration of response per BICR assessment 7
Table S6: Best overall response per BICR assessment in biomarker-defined patient populations 8
Table S7: Completion rates for patient-reported outcome measures 9
Table S8: EORTC QLQ-C30: number (%) of patients with ≥10-point deterioration from baseline 10
Table S9: EQ-5D: Number (%) of patients reporting health problems 11
Table S10: Selected treatment-related adverse events reported in patients treated with nivolumab 12
Figure S1: Plots of change from baseline in target lesion size over time and PFS per BICR assessment in patients with metastatic or recurrent colorectal cancer locally assessed as dMMR/MSI-H
14
Figure S2: Event charts per BICR assessment for patients with metastatic or recurrent colorectal cancer locally assessed as dMMR/MSI-H who responded to treatment or with stable disease
16
Figure S3: Changes in CEA levels correlated with response per investigator assessment 17
Figure S4: Patient-reported changes per EORTC QLQ-C30 18
Figure S5: Patient-reported changes per EQ-5D VAS and Utility Index 20

2
Supplementary methods Criteria for treatment delay Criteria for treatment delay include any grade ≥2 non–skin- (except grade 2 fatigue or laboratory abnormalities) or grade 3 skin-related adverse event (AE); any grade 3 laboratory abnormality, except asymptomatic grade 3 amylase or lipase abnormalities, or grade ≥2 (if levels were normal at baseline) or ≥3 (if grade 1 at baseline) alanine aminotransferase (ALT) or aspartate aminotransferase (AST) or total bilirubin abnormalities; and any AE, laboratory abnormality, or intercurrent illness that was considered to warrant a delay by the investigator. Criteria for treatment discontinuation Criteria for treatment discontinuation include disease progression, any grade 2 treatment-related uveitis, eye pain, or blurred vision that does not respond to topical therapy and does not improve to grade 1 within the retreatment period or requires systemic treatment; any grade 3 non–skin treatment–related AE lasting >7 days (exceptions include grade 3 treatment-related uveitis, pneumonitis, bronchospasm, diarrhoea, colitis, neurological toxicity, hypersensitivity reaction, or infusion reaction of any duration that requires discontinuation; for grade 3 endocrinopathy AEs such as adrenal insufficiency, adrenocorticotropic hormone deficiency, hyperthyroidosis or hypothyroidosis, or glucose intolerance that resolve or are adequately controlled with physiological hormone replacement [steroids, thyroid hormones] or glucose-controlling agents do not require treatment discontinuation; grade 3 drug-related laboratory abnormalities do not require treatment discontinuation except for grade 3 treatment-related thrombocytopenia lasting >7 days [associated with bleeding requires discontinuation]; and any treatment-related liver function test abnormality that meets the criteria [AST or ALT >8 × upper limit of normal (ULN), total bilirubin >5 × ULN, or concurrent AST or ALT >3 × ULN and total bilirubin >2 × ULN require discontinuation]); any grade 4 treatment-related AE or laboratory abnormality, except asymptomatic grade 4 amylase or lipase abnormalities, isolated grade 4 electrolyte imbalances/abnormalities that are not associated with clinical sequelae and are corrected with supplementation/appropriate management within 72 hours of their onset; any dosing interruption lasting >6 weeks from the last dose except interruptions for prolonged steroid tapers to manage treatment-related AEs and interruptions >6 weeks from the last dose that occur for non–treatment-related reasons; and any AE, laboratory abnormality, or intercurrent illness that in the judgement of the investigator presents a substantial clinical risk to the patient receiving continued nivolumab.

3
Table S1: Study sites and investigators
Site—country
Site number
Investigator Site—institution Patients treated
(N=74)
USA 0002 Eunice L. Kwak, MD Massachusetts General Hospital, Boston, MA
2
USA 0003 Michael J. Overman, MD The University of Texas MD Anderson Cancer, Houston, TX
12
USA 0004 Heinz-Josef Lenz, MD USC Norris Comprehensive Cancer Center, Los Angeles, CA
1
USA 0006 Emily Chan, MD Vanderbilt-Ingram Cancer Center, Nashville, TN
3
USA 0008 Bassel El-Rayes, MD Emory University, Atlanta, GA 1
Spain 0010 Antonio Cubillo Gracian, MD
Hospital de Madrid, Norte Sanchinarro, Madrid
1
Spain 0012 Pilar Garcia, MD Hospital General Universitario Gregorio, Maranon
1
USA 0013 James J. Lee, MD UPMC Cancer Pavilion, Pittsburgh, PA 2 Canada 0016 Albiruni Razak, MBBCh Mount Sinai Hospital, Toronto, ON 1 Belgium 0018 Bart Neyns, MD Universitair Ziekenhuis Brussel, Jette 2 Belgium 0019 Alain Hendlisz, MD Institut Jules Bordet, Brussels 2
Belgium 0020 Eric Van Cutsem, MD Universitaire Ziekenhuizen Leuven, Gasthuisberg
2
Ireland 0022 Ray Mcdermott, MBBCh St Vincent’s University Hospital, Dublin
5
USA 0024 Michael Morse, MD Duke University Medical Center, Durham, NC
2
France 0025 Thierry André, MD Hopital Saint Antoine, Paris 13
USA 0028 Tomislav Dragovich, MD MD Anderson Cancer Center, Houston, TX
1
USA 0029 Franklin L. Chen, MD Novant Health Oncology Specialists, Winston-Salem, NC
3
Italy 0030 Massimo Aglietta, MD IRCC, Candiolo 5
Italy 0032 Vittorina Zagonel, MD Istituto Oncologico Veneto IRCCS, Padua
5
USA 0034 Joseph W. Leach, MD Allina Health, Virginia Piper Cancer Institute, Minneapolis, MN
2
Italy 0035 Gabriele Luppi, MD Azienda Ospedaliera Universitaria di Modena
9
USA 0036 Eunice L. Kwak, MD Massachusetts General Hospital, Boston, MD
1
Australia 0037 Jayesh Desai, MBBS Royal Melbourne Hospital, Parkville, VIC
1
Australia 0039 Andrew G. Hill, MD Tasman Oncology Research Pty Ltd, Southport, QLD
1
Australia 0040 Ka Yeung Mark Wong, MBBS
Westmead Hospital, Westmead, NSW 2

4
Table S2: Concordance between local and central assessments of dMMR/MSI-H status
Patients, n (%)
dMMR/MSI-H per local assessment
N=74 MSI per central assessment
MSI-H Non–MSI-H* No result
53 (72) 14 (19) 7 (9)
Reasons for missing central MSI assessment H&E processing
No tumour identified No viable tumour identified
PCR processing Tumour and control DNA low/no amplification Tumour DNA low/no amplification
1 (1) 1 (1)
3 (4) 2 (3)
Local method used for concordant patients IHC only PCR only IHC and PCR
n=53 27 (51) 17 (32) 9 (17)
Local method used for discordant patients IHC only PCR only IHC and PCR
n=14 10 (71) 2 (14) 2 (14)
dMMR/MSI-H=DNA mismatch repair deficient/microsatellite instability–high. H&E, hematoxylin and eosin. IHC=immunohistochemistry. PCR=polymerase chain reaction. *Includes patients with microsatellite stable and MSI-low tumours.

5
Table S3: Summary of patients with discrepancies between local and central assessments of dMMR/MSI-H status
Patient
Local laboratory Central
laboratory result
Clinical history of Lynch
syndrome* Method Result
1 IHC dMMR MSI-L† Unknown
2‡ IHC dMMR MSS No
3 IHC dMMR MSS Yes
4 IHC dMMR MSS Yes
5# IHC/ PCR
pMMR (IHC)/ MSI-H (PCR)
MSS No
6 IHC dMMR MSS Yes
7 IHC dMMR MSS No
8 PCR MSI-H MSS Yes
9 IHC/ PCR
dMMR (IHC)/ MSI-H (PCR)
MSS Yes
10 IHC dMMR MSS No
11 IHC dMMR MSS Unknown
12 PCR MSI-H MSS Unknown
13 IHC dMMR MSI-L† Unknown
14 IHC dMMR MSS Unknown
dMMR=DNA mismatch repair deficient. IHC=immunohistochemistry. MSI-H=microsatellite instability high. MSI-L=microsatellite instability low. MSS=microsatellite stable. PCR=polymerase chain reaction. pMMR=DNA mismatch repair proficient. *Lynch syndrome designation was based on the clinical records of the patients at sites in countries where this reporting was permitted (excluded Italy). †MSI-L, categorized as MSS. ‡Patient had two primary tumours, one of which was assessed as dMMR per local laboratory; a metastatic tumour from a lymph node was assessed as MSS per central laboratory. #Patient had 2 results from local testing: MSS by IHC and MSI-H by PCR; central test result is MSS, discordant from the local PCR test result.

6
Table S4: Objective response rate, best overall response, and disease control rate in patients with non–MSI-H and microsatellite status not reported metastatic or recurrent colorectal cancer per central assessment of MSI-H status
Patients, n (%)
Non–MSI-H per central assessment
(n=14)*
Microsatellite status not reported
per central assessment (n=7)
Investigator BICR Investigator BICR
Objective response rate
[95% CI] 3 (21) [5–51]
3 (21) [5–51]
1 (14) [0·4–58]
2 (29) [4–71]
Best overall response
Complete response Partial response Stable disease Progressive disease Not determined
0
3 (21) 5 (36) 5 (36) 1 (7)
0
3 (21) 3 (21) 7 (50) 1 (7)
0
1 (14) 3 (43) 3 (43)
0
1 (14) 1 (14) 3 (43) 2 (29)
Disease control for ≥12 weeks [95% CI]
8 (57) [29–82]
5 (36) [13–65]
4 (57) [18–90]
5 (71) [29–96]
BICR=blinded independent central review. MSI-H=microsatellite instability–high. *Includes patients with microsatellite stable and MSI-low tumours.

7
Table S5: Summary of time to and duration of response per BICR assessment
Parameter All treated patients
(N=74)
Median time to response (IQR), months 2.8 (1.5–8.1)
Median duration of response (range), months NE (1.4+, 26.5+)
Duration ≥12 months (95% CI), %* 95% (68–99)
The + indicates censored values. BICR=blinded independent central review. MSI-H=microsatellite instability–high. ORR=objective response rate. *Kaplan-Meier 12-month event rate.

8
Table S6: Best overall response per BICR assessment in biomarker-defined patient populations
dMMR/MSI-H metastatic colorectal cancer per local assessment
(N=74) Tumour cell
PD-L1 expression Immune cell
PD-L1 expression Mutation
status Clinical history of Lynch syndrome*
≥1% (n=21)
<1% (n=47)
Rare (n=24)
Intermediate (n=21)
Numerous (n=23)
BRAF mutant (n=12)
KRAS mutant (n=26)
BRAF and KRAS
wild type (n=29)
Yes (n=27)
No (n=28)
Objective response rate, n (%) [95%CI]
7 (33) [14–57]
13 (28) [16–43]
5 (21) [7–42]
5 (24) [8–47]
10 (44) [23–65]
4 (33) [10–65]
8 (31) [14–52]
9 (31) [15–51]
8 (30) [14–50]
10 (36) [19–56]
Disease control rate 11 (52.4) [30–74]
31 (66) [50–79]
13 (54) [33–74]
14 (67) [43–85]
15 (65) [42–84]
NA NA NA NA NA
dMMR/MSI-H=DNA mismatch repair deficient/microsatellite instability–high. NA, not available. PD-L1=programmed death 1 ligand 1. *Lynch syndrome designation was based on the clinical records of the patients at sites in countries where this reporting was permitted (excluded Italy).

9
Table S7: Completion rates for patient-reported outcome measures
EORTC=European Organisation for Research and Treatment of Cancer. n/N, number of patients who completed questionnaire/number of patients on study.
n/N (%) BaselineWeek
7 Week
13 Week
19 Week
25 Week
31 Week
37 Week
43 Week
49 Week
55 Week
61 Week
67 Week
73 Week
79 Week
85 Week
91 Week
97
EORTC QLQ-C30
70/74 (95)
59/64 (92)
50/53 (94)
43/48 (90)
42/46 (91)
38/43 (88)
35/41 (85)
28/41 (68)
26/32 (81)
20/24 (83)
13/17 (76)
14/16 (88)
14/16 (88)
15/16 (94)
13/16 (81)
12/15 (80)
13/13 (100)
EQ-5D 66/74 (89)
59/64 (92)
49/53 (92)
42/48 (88)
42/46 (91)
38/43 (88)
36/41 (88)
27/41 (66)
25/32 (78)
17/24 (71)
13/17 (76)
13/16 (81)
14/16 (88)
15/16 (94)
13/16 (81)
12/15 (80)
13/13 (100)

10
Table S8: EORTC QLQ-C30: patients with ≥10-point deterioration from baseline
Week 7 (n=57)
Week 13
(n=48)
Week 19
(n=42)
Week 25
(n=41)
Week 31
(n=37)
Week 37
(n=34)
Week 43
(n=28)
Week 49
(n=26)
Week 55
(n=19)
Week 61
(n=13)
Week 67
(n=14)
Week 73
(n=14)
Week 79
(n=15)
Week 85
(n=13)
Week 91
(n=12)
Week 97
(n=13)
Physical functioning
8 (14) 3 (6) 3 (7) 4 (10) 2 (5) 2 (6) 1 (4) 2 (8) 2 (11) NA 2 (14) 2 (14) 1 (7) 1 (8) 2 (17) 3 (23)
Role functioning
13 (23) 6 (13) 7 (17) 5 (12) 3 (8) 3 (9) 4 (14) 4 (15) 3 (16) 13(23) 5 (36) 3 (21) 3 (20) 3 (23) 4 (33) 3 (23)
Emotional functioning
7 (12) 2 (4) 3 (7) 3 (7) 4 (11) 2 (6) 1 (4) NA 1 (5) 1 (8) 2 (14) 2 (14) 2 (13) 1 (8) 2 (17) 2 (15)
Cognitive functioning
16 (28) 9 (19) 8 (19) 6 (15) 11 (30) 6 (18) 2 (7) 5 (19) 4 (21) 13 (23) 7 (50) 3 (21) 2 (13) 3 (23) 5 (42) 1 (8)
Social functioning
11 (19) 2 (4) 6 (14) 7 (17) 6 (16) 3 (9) 1 (4) 4 (15) 4 (21) 13 (23) 4 (29) 3 (21) 3 (20) 3 (23) 5 (42) 2 (15)
Fatigue 12 (21) 10 (21) 10 (24) 5 (12) 8 (22) 5 (15) 5 (18) 4 (15) 3 (16) 1 (8) 3 (21) 5 (36) 2 (13) 3 (23) 4 (33) 3 (23)
Nausea and vomiting
11 (19) 2 (4) 3 (7) 4 (10) 4 (11) 2 (6) 2 (7) 1 (4) 2 (11) NA NA NA 1 (7) 2 (15) 1 (8) 1 (8)
Pain 9 (16) 4 (8) 7 (17) 4 (10) 6 (16) 3 (9) 1 (4) 4 (15) 4 (21) 1 (8) 3 (21) 4 (29) 3 (20) 2 (15) 4 (33) 3 (23)
Dyspnea 7 (12) 3 (6) 4 (10) 3 (7) 2 (5) 4 (12) 3 (11) NA 2 (11) 1 (8) 3 (21) 2 (14) 1 (7) 2 (15) 1(8) 2 (15)
Insomnia 6 (11) 7 (15) 9 (21) 6 (15) 4 (11) 2 (6) 3 (11) 2 (8) 1 (5) NA 2 (14) 1 (7) NA 1 (8) 2 (17) NA
Appetite loss
10 (18) 4 (8) 3 (7) 2 (5) 1 (3) 2 (6) 2 (7) 3 (12) 2 (11) NA 1 (7) 3 (21) 1 (7) 2 (15) 3 (25) 1 (8)
Constipation 5 (9) 3 (6) 4 (10) 5 (12) 2 (5) NA 1 (4) 2 (8) 1 (5) NA 1 (7) 1 (7) 1 (7) 5 (38) 1 (8) NA
Diarrhea 13 (23) 10 (21) 4 (10) 7 (17) 5 (14) 6 (18) 2 (7) 1 (4) 3 (16) 1 (8) NA 4 (29) 1 (7) 3 (23) 1 (8) 2 (15)
Financial difficulties
11 (19) 6 (13) 7 (17) 6 (15) 7 (19) 5 (15) 3 (11) 3 (12) 2 (11) 2 (15) 3 (21) 3 (21) 3 (20) 2 (15) 2 (17) 3 (23)
Quality of life
11 (19) 2 (4) 6 (14) 4 (10) 5 (14) 4 (12) 3 (11) 3 (12) 4 (21) NA 3 (21) 2 (14) 4 (27) 3 (23) 4 (33) 2 (15)
Data are in n (%). EORTC=European Organisation for Research and Treatment of Cancer. NA, not available.

11
Table S9: EQ-5D: patients reporting health problems
Data are in n (%). *n=66 patients at baseline.
Baseline (n=67)
Week 7
(n=59)
Week 13
(n=49)
Week 19
(n=42)
Week 25
(n=42)
Week 31
(n=38)
Week 37
(n=36)
Week 43
(n=27)
Week 49
(n=25)
Week 55
(n=17)
Week 61
(n=13)
Week 67
(n=13)
Week 73
(n=14)
Week 79
(n=15)
Week 85
(n=13)
Week 91
(n=12)
Week 97
(n=13)
Mobility* 21
(32) 15
(25) 9
(18) 5
(12) 5
(12) 3
(8) 3
(8) 6
(22) 5
(20) 4
(23) 3
(23) 2
(15) 4
(27) 2
(13) 2
(15) 3
(25) 2
(15)
Self-care 8
(12) 7
(12) 3
(6) 1
(2) 2
(5) 3
(8) 1
(3) 3
(11) 2
(8) 2
(12) 2
(15) 2
(15) 2
(14) 2
(13) 2
(15) 2
(17) 2
(15)
Usual activities
24 (36)
18 (30)
13 (26)
6 (14)
10 (24)
8 (21)
9 (25)
6 (22)
5 (20)
4 (23)
3 (23)
4 (31)
5 (36)
7 (47)
5 (38)
3 (25)
4 (31)
Pain 38
(57) 26
(44) 15
(31) 12
(29) 11
(26) 12
(32) 8
(22) 8
(30) 9
(36) 4
(23) 4
(31) 4
(31) 5
(36) 5
(33) 2
(15) 5
(42) 4
(31)
Anxiety 29
(43) 25
(42) 15
(31) 11
(26) 11
(26) 16
(42) 9
(25) 8
(30) 6
(24) 4
(23) 2
(15) 2
(15) 5
(36) 4
(27) 3
(23) 1
(8) 3
(23)

12
Table S10: Selected treatment-related adverse events reported in patients treated with nivolumab
Selected adverse event category
dMMR/MSI-H
(N=74)
Any grade Grade 3 or 4
Skin
Pruritus 10 (13) 0
Rash 8 (11) 0
Maculopapular rash 5 (7) 1 (1)
Dry skin 4 (5) 0
Gastrointestinal
Diarrhoea 16 (22) 1 (1)
Nausea 7 (10) 0
Stomatitis 3 (4) 1 (1)
Abdominal pain 2 (3) 1 (1)
Colitis 1 (1) 1 (1)
Oesophagitis 1 (1) 1 (1)
Gastritis 1 (1) 1 (1)
Endocrine
Hyperthyroidism 3 (4) 0
Hypothyroidism 3(4) 0

13
Adrenal insufficiency 1 (1) 1 (1)
Hepatic
Lipase increase 9 (12) 6 (8)
Aspartate aminotransferase increase 5 (7) 0
Alanine aminotransferase increase 4 (5) 1 (1)
Amylase increase 4 (5) 2 (3)
Gamma-glutamyl transferase increase 1 (1) 1 (1)
Hypersensitivity/infusion
Hypersensitivity 2 (3) 0
Infusion-related reaction 1 (1) 0
Renal
Creatinine increase 2 (3) 1 (1)
Acute kidney injury 1 (1) 1 (1)
Data are in n (%). dMMR/MSI-H=DNA mismatch repair–deficient/microsatellite instability–high.

14
Figure S1: Plots of change from baseline in target lesion size over time and PFS per BICR assessment in patients with metastatic or recurrent colorectal cancer locally assessed as dMMR/MSI-H BICR=blinded independent central review. dMMR/MSI-H=DNA mismatch repair deficient/microsatellite instability–high. PFS=progression-free survival. Percentage change from baseline in the sum of tumour burden for target lesions over time per BICR for evaluable patients treated with nivolumab. Triangles indicate complete or partial response per Response Evaluation Criteria In Solid Tumors v1.1, plus signs indicate the first occurrence of a new lesion, and squares indicate percentage change truncated to 100%. (B) Kaplan-Meier curve for PFS per BICR in patients treated with nivolumab. Triangles indicate censored observations.
A.

15
B.

16
Figure S2: Event charts per BICR assessment for patients with metastatic or recurrent colorectal cancer locally assessed as dMMR/MSI-H who responded to treatment or with stable disease BICR=blinded independent central review. dMMR/MSI-H=DNA mismatch repair deficient/microsatellite instability–high. Characteristics of response (top panel) or stable disease (bottom panel) evaluated per BICR by Response Evaluation Criteria In Solid Tumors v1.1. Triangles indicate censored observations, plus signs indicate first responses, open circles indicate the last nivolumab doses, closed circles indicate the last nivolumab doses when off treatment, and hash signs indicate death.

17
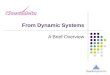
Figure S3: Changes in CEA levels correlated with response per investigator assessment CEA=carcinoembryonic antigen. CEA levels (September database lock) were measured at baseline and on day 1 of week 7 (day 43 [range 38–48]). (A) Percentage change from baseline in patients with complete responses or partial responses and patients with stable disease for ≥12 weeks. (B) Percentage change from baseline in patients with disease control for ≥12 weeks and patients with stable disease or progressive disease for <12 weeks; a significant difference in the percentage change in CEA levels was observed between these groups by Kruskal-Wallis test (p=0·038). Circles represent individual patients, plus sign indicates mean percentage change, and black lines indicate median percentage change.
A.
B.

18
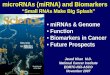
Figure S4: Patient-reported outcomes: EORTC QLQ-C30 Patient-reported outcomes were evaluated by the European Organisation for Research and Treatment of Cancer (EORTC) QLQ-C30 and the 3-level EQ-5D.15,16 The EORTC QLQ-C30 assesses functioning, symptoms, and quality of life on scales ranging from 0 to 100, with higher scores indicating better functioning, quality of life, or worsening symptoms, including fatigue, appetite loss, and pain.

19

20
Figure S5: Patient-reported outcomes: EQ-5D VAS and Utility Index Patient-reported outcomes were evaluated by the European Organisation for Research and Treatment of Cancer QLQ-C30 and the 3-level EQ-5D.15,16 The EQ-5D assesses the proportion of patients reporting health problems and consists of a visual analogue scale (VAS) evaluating self-reported health on a scale from 0 to 100, with higher scores indicating better health status.