Embed Size (px)
Citation preview

Checking Your Insurance Benefits IMPORTANT
Please check your insurance coverage prior to any Nutrition or Diabetes Education appointment. You will be responsible for any services that are not covered. Call the number on the back of your insurance card and give
them the following information:
1. You are being seen at Community Health and Life Center, PLLC.The dietitian NPI # is 1417431644.The office NPI # is 1609369172. The office TAX ID # is 83-0675758.
2. You will be billed as *OUTPATIENT CONSULTATION* NOT a physician visit. 3. The procedure codes are:
o Medical Nutrition Therapy with a Registered Dietitian:(Nutrition Diagnosis ONLY: Check the 2 procedure codes below.) 97802 (Initial Visit) 97803 (Follow Up Visit)
4. Tell them you need monthly visits to discuss your weight:One Per Calender Month, 30-days Apart, Consecutive - In Order, No Breaks
5. Be sure to ask for the representative’s first name and last initial and a reference number for the call. Document the date of the call for your files.
6. Additional questions to ask your insurance company:o Any limitations on visits and how many visits per calendar year are allowed? If visits are
limited, are there different limits for the Diabetes Nurse and the Registered Dietitian?o Are Referrals or Pre-Certification required? If a referral is needed, please call your doctors
office and bring it the day of your appointment. If you need a Pre-Certification please contact us.
o What is your responsibility: co-pay, co-insurance, or deductible?o Be sure to ask for the representative’s first name and last initial, a reference number for the
call and document the date of the call.
If your insurance informs you that our services are NOT a covered benefit please call our center so that we may discuss other options or have your insurance company representative contact our office at 346-616-0038.
**Medicare and Medicaid have other Billing Codes and different eligibility. Please contact our office for more information.
Thank you!

© 2019 Community Health and Life Center, PLLC. All right reserved worldwide. CHLC - Nutritional Services 1
Name: _______________________________ Age: ______ Birth Date: ____________
Bariatric Surgeon: ____________________________
Surgery Planned: Roux-en-Y Gastric Bypass
Sleeve Gastrectomy
Other: __________________
Cell Phone: ___________________ E-mail Address: ___________________________
Gender: Male Female Live with: Spouse Family Friend Alone
Employment: Full-time Part-time Retired Student Other__________ Occupation: ___________________________________ Work Hours: ______________
Have you seen a dietitian before? Yes No If yes, for what diet? _________________ When? ___________ Where? __________
Have you had any previous weight loss surgeries? Yes No If yes, what type(s)? When?
Height: _______ Present Weight: ________ BMI (if known):_______
Highest adult weight: ________ Date: _________________
Lowest adult weight: ________ Date: _________________
Recent weight change? Yes No How many pounds lost? ____ Gained? ____
What would you like to weigh? ______________
How much weight do you expect to lose as a result of weight loss surgery?
Less than 50 lbs. 50-100 lbs. 100-150 lbs. More than 150 lbs.
What age did you begin to gain excess weight? _______________________________
Looking back, what would you attribute the weight gain to at that time?________________________________________________________________
Dietitian to complete: % estimated weight loss/surgery type_________________
Weight loss expected: _______________ Goal weight range: _______________
Weight Loss Surgery Nutrition Screening Evaluation Form

2
Check any of the following problems you had previously or are now experiencing:
Hearing Problems Heart disease Asthma Memory/Concentration High Blood Pressure Kidney Disease
Blurred Vision Congestive Heart Failure Pre-Diabetes
Problems Reading Stroke Diabetes: Type 1___ Reflux/ Heartburn High Cholesterol Type 2 ___
Hiatal Hernia Anemia Thyroid disease Polycystic Ovary Syndrome Anxiety/Depression Excessive Thirst Constipation/ Diarrhea Mental Health Problems Frequent Urination Nausea/ Vomiting Liver Disease Sleep Apnea
Colon Surgery Back, Knee, Hip Problems Cancer
Loss of Feeling/ Tingling/ Pain in: __Feet __Legs __Hands __Arms
Please list any other medical problems or surgeries (not listed above). Also, include any medical procedures (such as balloon angioplasty): ___________________________________________
For women: Are you currently pregnant? Yes No Are you planning to become pregnant? Yes No Are you currently breastfeeding? Yes No Age at menopause: __________
Check all over-the-counter medications you take:
Multi-vitamins: brand:________________________________
Single vitamins (Vitamin C, E, etc.): type(s):____________________________________
Calcium: type: ______________________________amount:________________________
Herbs: type(s):_______________________________________________
Other over-the-counter medications:____________________________________________
Write down all the prescription medications you take.
1.________________________ 5.________________________
2.________________________ 6.________________________
3. ________________________ 7.________________________
4.________________________ 8. ________________________
© 2019 Community Health and Life Center, PLLC. All right reserved worldwide. CHLC - Nutritional Services
Weight Loss Surgery Nutrition Screening Evaluation Form

3
On a scale of 1 -5, circle the number that best describes you or your situation.
Stro
ngl
y D
isag
ree
Dis
agre
e
Nei
ther
A
gree
nor
D
isag
ree
Agr
ee
Stro
ngl
y A
gree
I have family and friends that will be a strong support system for me after surgery. 1 2 3 4 5
I have researched bariatric surgery and talked with people who have had weight loss surgery. 1 2 3 4 5
I will be involved with my follow-up care and attendance at bariatric support groups after surgery. 1 2 3 4 5
I am highly motivated. 1 2 3 4 5
I am quick to learn and can easily follow directions. 1 2 3 4 5
1. Have you ever been diagnosed with an eating disorder? Yes NoIf yes, what type? Binge Eating Anorexia Nervosa Bulimia
Other: _______________________ 2. Do you drink alcoholic beverages? Yes No If yes, how often? ________________
If yes, what do you drink? Beer (regular) Beer (light) Wine Mixed drinks Brandy Liquor (Gin, Rum, Vodka) Liqueur (Kahlua, Bailey’s, Crème de Menthe)
3. Do you use marijuana, cocaine, crack or other recreational drugs? Yes No
4. Do you smoke? Yes NoIf yes, how much do you smoke in 24 hours? _____________ If no, have you ever smoked? Yes No If yes, when did you quit? ____________
5. How many hours do you usually sleep (out of a 24 hour day)? ____________What time do you get up? _________ What time is your first meal? _______________
6. Do you have any food or medication allergies? Yes NoIf yes, please list: ________________________________________________________
7. Do you follow any religious or cultural rules that influence what or how you eat? Yes No If yes, please explain: _______________________________________
8. How do you learn best? Verbal (explanation/tapes/video) Demonstration Written (books/pamphlets/guidelines) Other (please explain):_____________
Weight Loss Surgery Nutrition Screening Evaluation Form
© 2019 Community Health and Life Center, PLLC. All right reserved worldwide. CHLC - Nutritional Services

4
Please check ( ) everything below that describes your diet and/or lifestyle behaviors:
1. I eat large portions, get seconds, or
overfill my plate.
11. I eat too quickly, chew foods poorlyor take too large of bites.
2. I skip meals or go for longer than fivehours between meals.
12. I am an emotional eater or I eatmore when I am stressed.
3. I dine out (includes carry-in) morethan three times a week.
13. I drink less than 64 ounces (8 cups)daily (all fluids count).
4. I frequently eat fried foods, fastfoods, and high fat foods.
14. I gulp (rather than sip) mybeverages or drink too quickly.
5. I frequently eat sweets and desserts(candy, cakes, cookies, pies).
15. I drink beverages with calories(juice, punch, soda, sweet tea, etc.).
6. I graze (snack on food all day long)while doing other things (reading,computer work, watching TV).
16. I usually drink more than twocarbonated drinks (soda pop,bubbly drinks) daily.
7. I eat high calorie snacks.17. I usually drink more than two cups
of coffee or caffeine drinks daily.
8. I wake up and eat during the middleof the night.
18. I usually drink two or more alcoholicbeverages daily.
9. I don’t eat enough protein (less than4-6 ounces of meat, fish or poultrydaily).
19. I lack sufficient exercise (less than30 minutes on most days of theweek).
10. I get less than three dairy servings(milk, yogurt, cheese) daily.
20. Other:
Dietitian to fill out: Pre-surgery goals selected: _________________________________
Weight Loss Surgery Nutrition Screening Evaluation Form
© 2019 Community Health and Life Center, PLLC. All right reserved worldwide. CHLC - Nutritional Services

5
Please check ( ) those statements below that apply to you. Identifying problem areas before surgery is the first step towards being successful after surgery.
I have a relative or friend who may try to hinder my weight loss efforts.
In the past I have not been good about taking vitamins and/or medications.
I rely on someone else to purchase and/or prepare my food.
English is not my first language. I have a language barrier.
I have problems with chewing and swallowing.
My calorie intake is already low (below 1000 calories per day).
I have a physical condition(s) that limits activity or exercise. I am a stress eater or emotional eater.
I have an eating disorder. I have problems with eyesight or hearing.
I have a difficult work schedule. I never feel full even when I have eaten a lot.
I may not be able to afford supplements. I am addicted to food.
I have difficulty making changes. I would have a difficult time reducing or giving up: __________________.
Other: Other:
Please complete the following sentences:
1. The main reason I have been unable to lose weight (or maintain lost weight) is because:______________________________________________________________________________________________________________________________________________________
2. I want to lose weight (or I have decided to have weight loss surgery) because______________________________________________________________________________________________________________________________________________________
3. Questions I would like to discuss with the dietitian are:_____________________________________________________________________________ _____________________________________________________________________________ _____________________________________________________________________________
Weight Loss Surgery Nutrition Screening Evaluation Form
© 2019 Community Health and Life Center, PLLC. All right reserved worldwide. CHLC - Nutritional Services

6
Sample Menu (Use as an example to fill out the menu below):
Time Meal Foods and Beverages Include Amounts and How Food is Prepared
8:00 a.m. Breakfast 1 cup coffee with 3 teaspoons sugar and one creamer
9:30 a.m. Snack Large toasted bagel with 2 tablespoons cream cheese 20 ounce soda pop
11:30 a.m. Lunch Wendy’s Chicken BLT Salad with 2 packets of honey mustard dressing and croutons 20 ounce lemonade + refill
2:00 p.m. Snack Pretzels, grab-it size 16 ounce bottle cranberry juice
7:30 p.m. Dinner
2 fried chicken breasts, extra crispy ½ c. green beans with ham 1 cup mashed potatoes with ¼ cup gravy 2 biscuits with 2 tablespoons butter 2 tablespoons honey 2 cans of beer
11:00 p.m. Snack 6 Oreo Cookies 12 ounces 2% milk
Describe your usual daily eating pattern:
Time Meal Foods and Beverages Include Amounts and How Food is Prepared
Breakfast
Snack
Lunch
Snack
Dinner
Snack
Weight Loss Surgery Nutrition Screening Evaluation Form
© 2019 Community Health and Life Center, PLLC. All right reserved worldwide. CHLC - Nutritional Services

7
Name: Height: _______ Weight: _______ Date: _____________
Insurance companies often require a list of diets followed within the past 5 years. The best you can remember, please complete the form below. Refer to the last page for a list of popular diets.
Name or Type of Diet
Year You Began
This Diet
Number of Months on
This Diet
Pounds Lost
Who Supervised This Diet? (Name of
Doctor/Facility)
EXAMPLE: Weight Watcher’s 2012 5-6 months 30
EXAMPLE: Diet Pills 2018 2 months 5-10
Dr. JudyMedical Center
TX
1.
2.
3.
4.
5.
6.
Weight Loss Surgery Nutrition Screening Evaluation Form
© 2019 Community Health and Life Center, PLLC. All right reserved worldwide. CHLC - Nutritional Services

8
Use the information below to help you remember diets followed in the past 5 years so you can more easily complete the “History of Weight Loss Method’s” form on the previous page.
Commercial Programs Popular Diets or Fad Diets Diet Center Blood Type Diet Diet Workshop Body for Life
Jenny Craig Cabbage Soup Diet
LA Weight Loss Calorie Counting
NutriSystems Carbohydrates Addicts Diet
Overeaters Anonymous (OA) Dr. Phil’s Ultimate Weight Loss
Physician’s Weight Loss Center Eat More, Weigh Less (Dr. Ornish)
Take Off Pounds Sensibly (TOPS) eDiets.com
Weight Watchers Glycemic Index
Grapefruit Prescription Diet Medications Hollywood
Amphetamines Low Carb (i.e. Atkins) Meridia (sibutramine) Low Fat
Mayo Clinic Diet Phentermine (Fastin/Adipex/Ionamin)
Protein Power Xenical (orlistat) Richard Simmons
South BeachLiquid Diets Sugar Buster’s
Carefast The ZoneFormula 3 Volumetrics HMR Medifast New Direction
Therapy and Other Programs/Diets
Optifast AcupunctureSlimfast Behavior Therapy
Diabetic DietExercise Programs Herbal and
Non-Prescription Remedies Fasting Alli Hypnosis Dexatrim Inpatient psychiatric programEphedra (ma huang) Previous weight loss surgery Hydroxcut Previous gastric stapling Laxatives PsychotherapyMetabolife Registered Dietitian
© 2019 Community Health and Life Center, PLLC. All right reserved worldwide. CHLC - Nutritional Services
Weight Loss Surgery Nutrition Screening Evaluation Form

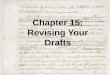
PATIENT HEALTH QUESTIONNAIRE (PHQ-9)DATE:NAME:Over the last 2 weeks, how often have you beenbothered by any of the following problems? Not at all Severaldays More thanhalf thedays Nearlyevery day(use "ⁿ" to indicate your answer) 0 1 2 3Little interest or pleasure in doing things1. 0 1 2 3Feeling down, depressed, or hopeless2. 0 1 2 3Trouble falling or staying asleep, or sleeping too much3. 0 1 2 3Feeling tired or having little energy4. 0 1 2 3Poor appetite or overeating5. 0 1 2 3Feeling bad about yourself or that you are a failure orhave let yourself or your family down6. 0 1 2 3Trouble concentrating on things, such as reading thenewspaper or watching television7. 0 1 2 3Moving or speaking so slowly that other people couldhave noticed. Or the opposite being so figety orrestless that you have been moving around a lot morethan usual8. 0 1 2 3Thoughts that you would be better off dead, or ofhurting yourself9. add columns + +TOTAL:(Healthcare professional: For interpretation of TOTAL,please refer to accompanying scoring card). Not difficult at allIf you checked off any problems, how difficulthave these problems made it for you to doyour work, take care of things at home, or getalong with other people?10. Somewhat difficultVery difficultExtremely difficultCopyright © 1999 Pfizer Inc. All rights reserved. Reproduced with permission. PRIME-MD© is a trademark of Pfizer Inc.A2663B 10-04-2005

Patient Waiver for Non-Covered Services
This waiver is to inform you that you will have an appointment with a registered
dietitian today in our office. This appointment will be coded and billed as
"medical nutrition therapy" only. It will be your responsibility to verify that your
insurance covers this type of service. It is important to know that the coding of
this service will not be altered once performed.
Please be aware that insurance may not pay for all of your healthcare costs.
Some items and services are considered “non-covered benefits” under your
health insurance plan and, your insurance may not pay for these services. By
signing below you acknowledge that every billing effort will be made to your
insurer for the reimbursement of medical nutrition therapy. In the event that your
insurance does not pay, then you agree to be responsible for the balance.
I acknowledge that I have been informed in advance of receiving these
services, and that these services may not be covered by my health insurance
plan. I have chosen to receive these services and understand that I will be
financially responsible for the charges and any remaining balance, in the event
my insurance company does not make payment.
Print Patient Name: ________________________________________________________________________________________________________
________________________________________________________________________________________ __________________________
Patient Signature Date