Embed Size (px)
Citation preview

Seeking Higher Value in Medicaid: A National Scan of State Purchasers
Funded through Kaiser Permanente Community Benefit and the Robert Wood Johnson Foundation.
www.chcs.org
Center for Health Care Strategies, Inc.CHCS
By Melanie Bella, Claudia Williams, Lindsay Palmer, Stephen A. Somers
November 2006

About the Center for Health Care Strategies
The Center for Health Care Strategies (CHCS) works to improve the value of publicly
financed care for people with chronic illnesses and disabilities, the elderly, and
racially and ethnically diverse populations. We work with the federal government,
state Medicaid agencies, health plans, providers, and consumers to design and test
strategies for delivering care that is effective, equitable, and efficient.
About the Authors
Melanie Bella is a senior vice president at CHCS; Claudia Williams is a principal with
AZA Consulting; Lindsay Palmer is a program associate at CHCS; and Stephen A.
Somers, PhD, is the president of CHCS.
© 2006 Center for Health Care Strategies
M. Bella, C. Williams, L. Palmer, S.A. Somers, “Seeking Higher Value in Medicaid: A National Scan of State Purchasers.” Center for Health Care Strategies, Inc.,November 2006.

Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3Characteristics of States Interviewed . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4
Study Findings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5 Theme 1: States are generally happy with and continue to pursue full-risk managed care and are also using managed care alternatives as a way to provide accountable medical homes and expand care management. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5
Theme 2: States want to expand and extend mechanisms for accountable medical homes and care management into new areas (rural) and new populations (aged, blind, and disabled and dual eligibles). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .8
Theme 3: States now realize that they can do much more with their purchasing power than merely secure financial predictability, and they are acting accordingly. Increasing quality, efficiency, and accountability are all important goals. . . . . . . . . . . . . . .15
Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .21
AppendicesAppendix 1: Medicaid Overview in Scan States . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .22
Appendix 2: Medicaid Managed Care Programs Overview in Scan States . . . . . . . . . . . . .23
1
Table of Contents
Seeking Higher Value in Medicaid: A National Scan of State Purchasers

Seeking Higher Value in Medicaid: A National Scan of State Purchasers
2
AcknowledgementsWe are grateful for generous support from Kaiser Permanente Community Benefit, and the addi-tional funding from the Robert Wood Johnson Foundation that made this scan of Medicaidmanaged care possible. The authors would also like to thank the Medicaid officials in the 14states that participated in the purchaser scan for sharing their experiences and perspectives onthe current state of Medicaid managed care, and for reviewing a formative draft to ensure we“got it right.” By sharing their insights, other states can learn from these laboratories of innova-tion to adapt and adopt managed care best practices to improve health services for Medicaidbeneficiaries. Special thanks also go to John Barth of CHCS for his valuable assistance withstate interviews and overall feedback, and to Lorie Martin of CHCS for her contributions andeditorial expertise.

Seeking Higher Value in Medicaid: A National Scan of State Purchasers
Introductionedicaid managed care has come a longway since it took its first baby steps in
many states in the mid-1990s. From whatwas often a harried scramble to implementquickly crafted procurements, states nowhave deliberate and well-tested strategies forembarking on managed care expansions —derived both from their own experiences andother states’ examples. In approaching theseexpansions, states clearly recognize that allhealth care — like politics — is local, andvariations in managed care approaches, espe-cially in rural areas and for more complexpopulations, must be made to accommodatestate-specific conditions. States also recog-nize that there is more to do to assure thathealth plan and primary care case management (PCCM) arrangements provideaccountable medical homes, access to needed specialty services, care management,consumer engagement, and incentives forimproving performance.
This report presents key findings from inter-views with Medicaid directors and staff in 14states to provide a nationwide scan of thecurrent state of Medicaid managed care.1
The states — California, Colorado, Florida,Georgia, Hawaii, Kentucky, Maryland,Michigan, Ohio, Oregon, Pennsylvania,Texas, Washington, and Wisconsin — represent a variety of purchasing strategies,geographies, and managed care experiencespast and present. Because this scan reflectsonly a subset of state purchasers and wasdesigned to limit focus to a number of keyareas, there is a risk that it may only scratchthe surface of issues critical to other states;
M however, we feel that the perspectives ofthe states interviewed provide a rich snap-shot of Medicaid managed care today.
During our interviews, Medicaid purchasersshared perspectives about managed care andits potential to address the most significantchallenges facing Medicaid: providing valuethrough improved quality, controllingexpenditures, and developing effective andefficient approaches to care for those withmultiple chronic conditions and the highestcosts. Our interviews particularly focusedon state plans for managed care expansions,trends in the Medicaid managed care mar-ketplace, and promising state practices forimproving quality.2 Three cross-cuttingthemes emerged:
1. States are generally happy with andcontinue to pursue full-risk managedcare, and are also using managedcare alternatives as a way to provideaccountable medical homes andexpand care management.
2. States want to expand and extendmechanisms for accountable medicalhomes and managed care into newareas (rural) and populations (aged,blind, and disabled and dual eligibles).
3. States now realize that they can domuch more with their purchasingpower than merely secure financialpredictability, and they are actingaccordingly. Increasing quality, effi-ciency, and accountability are allimportant goals.
3
1 For the purposes of this report, “managed care” includes full-risk (capitated) managed care as well as primary care case management programs (PCCM), enhancedPCCM programs, and disease and/or care management programs.
2 While we did not specifically focus on the states’ ability to achieve cost savings through managed care, it is important to note that a number of states, several of which are included in this scan, have sought independent evaluation of these savings. Examples include: Medicaid Capitation Expansion’s Potential Cost Savings.The Lewin Group. April 2006; Comparative Evaluation of Pennsylvania’s HealthChoices Program and Fee-For-Service Program. The Lewin Group. May 2005; and Michigan Medicaid: Relative Cost Effectiveness of Alternative Service Delivery Systems. Center for Health Program Development and Management, University of Maryland Baltimore County. April 2005.

Seeking Higher Value in Medicaid: A National Scan of State Purchasers
These three themes form the backbone ofthis report. Overall, we found that states areexpanding the boundaries of traditional full-risk managed care and are using innovativemodels, including enhanced primary carecase management and comprehensive caremanagement, to find the best value in deliv-ering care to Medicaid beneficiaries. Thefindings within this report outline future priorities, barriers, and opportunities formanaged care expansion or enhancements,in the eyes of leading state purchasers. Wehope that the lessons herein offer valuableinsights and direction to help all Medicaidstakeholders — not only state purchasers, butalso managed care organizations, consumerorganizations, providers, and legislators —pursue innovative strategies for improvingthe lives of the 55 million Americans receiv-ing publicly financed care under Medicaidand related State Children’s Health InsurancePrograms.
Characteristics of States Interviewed
The 14 states interviewed for this reportwere chosen to represent the variation inMedicaid delivery across the country. TheMedicaid programs included in the scanrange in size from small (e.g., Hawaii, withapproximately 200,000 total enrollees) tovery large (e.g., California, with more thansix million enrollees). Children account forthe majority of Medicaid enrollees in 10 ofthe 14 states, while the aged, blind and dis-abled (ABD) population makes up between19% and 40% of Medicaid enrollees depend-
ing on the state. Each of the 14 states oper-ates full-risk Medicaid managed care pro-grams and more than half administer a pri-mary care case management program(PCCM). The states vary in whether thesemanaged care programs operate statewide oron a more limited, geographic basis. As aresult, the level of Medicaid managed carealso varies from state to state, with theoverall Medicaid managed care penetrationrate (including PCCM and full-risk) rang-ing from 30% to 85%. All 14 states includethe Temporary Assistance for NeedyFamilies and related populations in theirMedicaid managed care programs and themajority of states serve or plan to serve theABD population as well (although theMedicaid managed care penetration rate forthis group is much lower on average). Dualeligibles (those eligible for both Medicareand Medicaid), on the other hand, areincluded in less than half of the Medicaidmanaged care programs, although this couldchange in the near future as states becomemore familiar with the potential for con-tracting with Medicare Special Needs Plans(SNPs) to integrate their care. Additionalinformation on the characteristics of thestate Medicaid programs that were surveyedcan be found in the Appendices.
4

Seeking Higher Value in Medicaid: A National Scan of State Purchasers
n many states the growth and develop-ment of large, multi-state, for-profit
health plans, especially those focusing exclusively on Medicaid, has made managedcare more feasible by increasing access andparticipation. Publicly traded firms areexerting increasing influence on Medicaidmanaged care with four firms (Amerigroup,Centene, Molina, and Wellcare) now operat-ing 30 plans with 3.8 million members in 18states. Another five publicly traded managedcare companies (United Healthcare,Wellpoint, Coventry, HealthNet, Humana)have separate Medicaid lines of business withfour million Medicaid members in 30 plansin more than 16 states.3 The so-calledMedicaid “pure plays,” which only operate aMedicaid line of business, have experiencedsome financial “right-sizing” of late, but con-tinue to expand market position.
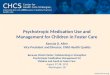
In order to better understand the currentdynamics of Medicaid managed care, thisscan incudes states actively pursuing a vari-ety of Medicaid managed care models. Notonly are all of the states using traditionalfull-risk managed care, but the penetrationrate for both full-risk and PCCM models is atleast one-half (and in some cases as much astwo-thirds) in the majority of states weselected (Figure 1). Regardless of this highmanaged care penetration rate, all of thestates interviewed recognize that full-riskcapitation is not the only vehicle for man-aged care expansion.
5
Study Findings
The prospect of more extensive enrollmentof the ABD population offers potentialappeal to many of the pure play plans, whichalready have invested in a data and caremanagement infrastructure that is wellequipped to serve these members. Somestates, however, continue to be cautiousabout these plans — either because of stake-holder resistance or because these plans maynot be willing and/or able to develop themore tailored approaches that states are seek-ing. Moreover, in some rural and frontierareas there simply are not enough potentialmembers or interested providers to make full-risk managed care work.
Figure 1: Medicaid Managed Care in Scan States
Full-RiskManaged
CareProgram(s)
PCCM/EPCCM
Program(s)
At Least One-Half ofMedicaid
Enrollees inManaged
Care
Two-Thirdsof MedicaidEnrollees inManaged
Care
14
12
10
8
6
4
2
0
Source: State interviews and websites, Kaiser State Health Facts. Note:Figures are not unduplicated counts.
I
Num
ber
of S
tate
s (n
=14
)
3 R. Hurley. Understanding the Influence of Publicly Traded Health Plans on Medicaid Managed Care. Center for Health Care Strategies, Inc. November 2006.
Theme 1: States are generally happy with and continue to pursuefull-risk managed care and are also using managed care alternativesas a way to provide accountable medical homes and expand caremanagement.

Seeking Higher Value in Medicaid: A National Scan of State Purchasers
6
When capitated managed care is not feasi-ble, states are experimenting with alterna-tives to introduce medical homes and caremanagement to more Medicaid consumers.Enhanced primary care case management(EPCCM), disease management, and com-prehensive care management are seen aspotential strategies to manage the care ofpopulations not historically enrolled in full-risk managed care (Figure 2).
Pennsylvania, for example, is piloting anEPCCM program in rural areas that do notyet have Medicaid managed care. The statemay also introduce this approach in urbanareas as an alternative to capitated man-aged care, thereby creating opportunities totest how the models can function in thesame region. The program, called ACCESSPLUS, was implemented in 2005 and offersdisease management for asthma, diabetes,chronic obstructive pulmonary disease,
coronary artery disease, and congestiveheart failure. ACCESS PLUS links mem-bers with these conditions with a primarycare physician (PCP) who provides or coor-dinates the members’ care. IntroducingEPCCM is a departure from Pennsylvania’sformer plan of deliberate progressiontoward statewide full-risk managed care.Two issues drove this change: the challengeof developing plan networks in rural areasand questions about whether the tightercapitation rates being imposed by thestate’s fiscal realities might be underminingthe plans’ incentives to improve care man-agement. ACCESS PLUS will rely on thestate Medicaid agency’s capacity and infra-structure for managing care developed overyears of running managed care programs.For example, the state has created a fee-for-service special needs unit to work withmedically complex ACCESS PLUS con-sumers that is modeled after Medicaidplans’ special needs units. In addition,pharmacy management for the program isbased on a managed care best-practicesreport prepared by the state’s actuarial con-sultants.
Pennsylvania is also taking a proactiveapproach to chronic care management bydeveloping health initiatives for smokingand obesity that aim to prevent the onsetof disease. To increase the low numbers ofconsumers using smoking cessation bene-fits, the state is reaching out to providers toshare information about the positive returnon investment for smoking cessation and toencourage more patient referrals to smok-ing cessation programs. In addition, thestate is developing a childhood obesity ben-efit and a program for kids at risk for obesi-ty that includes nutritional counseling. Apositive return on investment is predictedfor the childhood obesity program, withinitial analysis indicating that it will payfor itself in two years. The state is consider-
Figure 2: State Alternatives to Full-Risk ManagedCare
Model Description
Enhanced Primary EPCCM programs use primary medical Care Case providers to coordinate primary careManagement and approve specialty referrals for(EPCCM) Medicaid beneficiaries, and also
incorporate features originally developed for capitated managed care programs, such as care coordination and quality improvement efforts.
Disease Disease management is a strategy ofManagement delivering health care services to
improve the health outcomes of patients with specific diseases. It often uses telephone interventions, interdisciplinary clinical teams, and patient self-management education.
Comprehensive Comprehensive care management isCare Management designed to ensure continuity and
accessibility of services to overcome rigidity, fragmented services, and the misutilization of facilities and resources. It also attempts to match the appropriate intensity of services with the patient’s changing needs over time.

ing requiring the adoption of these benefitsby plans in the 2007-2008 contracts.
Like Pennsylvania, several other states areexperimenting with care and disease man-agement programs as alternatives to full-risk managed care. Much of the impetus forthese experiments comes from trying toovercome political resistance to capitatedmanaged care for populations with chronicconditions and disabilities. In addition,some states are beginning to question thewisdom of paying for three or four caremanagement infrastructures in three or fourhealth plans, when the state can potential-ly develop one program on its own or witha single contractor acting as its administra-tor. Washington recently issued a newrequest for proposals for care managementof its high-risk Medicaid population thattakes “a consumer rather than a disease-focused approach.” The new approach willinclude predictive modeling to identify at-risk populations and contracts with region-al community-based organizations (in addi-tion to a statewide entity) that will workwith consumers and PCPs to managechronic care needs. The local care manage-ment entity will not only provide the tradi-tional care management activities of assess-ment and disease-specific education andsupport, but will also ensure that the clienthas a medical home by entering into con-tractual relationships with providers whoagree to serve aged, blind and disabled
clients. In areas of the state without a localcare management entity, a statewide caremanagement contractor will provide caremanagement that takes a holistic view ofclient needs, as opposed to a single-diseasefocus. Another state is developing a diseasemanagement program that would contractwith a single entity to manage the care ofthe state’s highest-risk, highest-cost mem-bers. The program, still in the early concep-tual stage and tentatively set for a 2008launch, would link medical services withbehavioral health and social supports.
Georgia, building on its existing care man-agement infrastructure, is launching a newdisease management program as a wrap-around to its EPCCM for the ABD popula-tion. All EPCCM enrollees except dual eli-gibles will be automatically enrolled in thedisease management initiative with an opt-out option. The disease management vendorwill be responsible for analyzing data to pro-duce provider profiles and will be at risk forperformance, but all care management activ-ities will be the responsibility of the primarycare provider. A similar program will beimplemented for dual-eligible beneficiariesusing an administrative services organiza-tion, rather than a risk-based contract.
Seeking Higher Value in Medicaid: A National Scan of State Purchasers
7

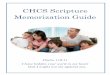
disease or care management programs. Asindicated in Figure 3, a number of statesare interested in increasing access to med-ical homes by extending some type of managed care delivery system to includeadditional populations (ABD), benefits(long-term care), and regions of the state(rural areas). Furthermore, while statesacknowledge the benefits of mandatoryenrollment (higher enrollee participation,ability to reward high-performing planswith default enrollment, and less potentialfor adverse selection), they recognize thatmandatory enrollment may not always befeasible, at least not initially, due to thelack of plan capacity in rural areas, as wellas resistance from state legislators, providers,and ABD beneficiaries. In those circum-stances, state leaders are also consideringmechanisms to increase participation involuntary programs.
As noted earlier, states are exploring a vari-ety of managed care delivery models toachieve their expansions, including tradi-tional full-risk managed care; alternative
Seeking Higher Value in Medicaid: A National Scan of State Purchasers
States are striving to create “medicalhomes” for all Medicaid beneficiaries.Although there is not a universally accept-ed definition of “medical home,” the termgenerally represents an ongoing connec-tion between a beneficiary and the healthcare system that results in the coordinationand management of that person’s totalhealth care needs. In practice, a medicalhome often refers to a primary careprovider who directly or through caremanagers coordinates and facilitates anindividual’s health care needs by makingreferrals, conducting home assessments,providing care management, and helpingthe consumer navigate the health care sys-tem. The American Academy of Pediatricsdescribes the medical home as being“accessible, continuous, comprehensive,family-centered, coordinated and culturallyeffective.”4 This definition does notrestrict medical home to a particular typeof provider, location, or payment structure;rather, it defines the concept broadly aslong as it “provides the services that con-stitute comprehensive care.” A medicalhome ideally replaces the traditionallyfragmented, uncoordinated care receivedunder the fee-for-service system that tendsto be more costly and less effective, partic-ularly for people with complex or chronicconditions. Challenges to establishingmedical homes range from the morestraightforward issues of provider availabil-ity and access in rural areas to selectingfrom among multiple providers for benefi-ciaries with more complex conditions.
By definition, managed care organizationsshould provide members with a medicalhome, as should EPCCM and specialty
8
Theme 2: States want to expand and extend mechanisms foraccountable medical homes and managed care into new areas (rural)and new populations (aged, blind, and disabled and dual eligibles).
Figure 3: Managed Care Expansions in Scan States
Expansions intoABD Population
Long-Term CareExpansions
Rural Expansions
14
12
10
8
6
4
2
0
Source: State interviews. Note: Figures are not unduplicated counts.
Num
ber
of S
tate
s (n
=14
)
4 The National Center for Medical Home Initiatives for Children with Special Health Care Needs. The American Academy of Pediatrics. Available at: http://www.medicalhomeinfo.org/ Accessed July 11, 2006.

methods such as EPCCM, disease/caremanagement; and contractual relationshipswith Medicare Advantage SNPs to coordi-nate care for dual-eligible beneficiaries(Figure 4).
Managed care choices are more limited in rural areas.
States with large rural populations facecommon challenges getting plans to partic-ipate and building provider networks inthese areas. Believing rural populationscould be better served by some form ofmanaged care, a number of states are inter-vening to build rural managed care capaci-ty or experimenting with alternative man-aged care models such as EPCCM. As dis-cussed previously, Pennsylvania hopes itsnew EPCCM program will be an effectiveand efficient way to extend care manage-ment resources to rural areas. Maryland,meanwhile, anticipates that planned physi-cian fee increases will increase provideraccess in rural areas.
States are considering a variety of models for introducing medical homes and expanding managed care to the aged, blind, and disabled population.
After years of experience implementingmanaged care for relatively healthy families,states are increasingly realizing that theyneed to obtain the same level of increasedaccess, quality, and financial predictabilityfor their most complex and costly popula-tions — ABD beneficiaries. These adultswith specialized needs constitute roughly25% of members yet account for nearly 70%of Medicaid costs nationally.5 As a result, several states are interested in implementingprograms that better manage the care of theABD population. The ABD population itselfis quite diverse and includes not only theelderly but also persons with physical disabil-ities and the developmentally disabled, manyof whom may also be dually-eligible forMedicare and Medicaid and all of whommay require a range of medical and support-ive/social services from multiple providersand in a variety of settings. The complexcare needs of many ABD beneficiaries oftenrequire additional services that may not typi-cally be included in traditional managed careprograms. For example, adults with chronicconditions are also more likely to report poormental health; however, behavioral healthservices are often carved out of full-risk man-aged care programs. Although a number ofstates expressed interest in programs thatcombine behavioral and physical health, fewhad concrete plans for integrating these serv-ices in the near future. In part, this may bebecause, in many states, behavioral healthservices are provided through other state orcommunity programs and agencies that areoften reluctant to cede those services to aMedicaid agency or managed care plan, mak-ing behavioral and physical health integra-tion difficult. Instead, most states seemed to
Seeking Higher Value in Medicaid: A National Scan of State Purchasers
9
Figure 4: Type of Managed Care Delivery SystemTargeted for Expansions in Scan States
Full-RiskManaged
Care
SpecialNeeds Plans
(SNPs)
PCCM/EPCCM
Programs
DiseaseManagement/
CareManagement
Programs
14
12
10
8
6
4
2
0
Source: State interviews. Note: Figures are not unduplicated counts.
Num
ber
of S
tate
s (n
=14
)
5 Medicaid Program at a Glance. Kaiser Family Foundation. May 2006. http://www.kff.org/medicaid/upload/7235.pdf

focus more on achieving better coordina-tion between current acute care and behav-ioral health programs and/or other carve-outs. States developing managed care pro-grams for ABD beneficiaries must alsodetermine whether to include the entireABD population or to design programs thataddress the needs of individual subsets ofthe population (e.g., a program for the eld-erly and a separate program for personswith developmental disabilities).
Ohio is developing a full-risk managed careprogram for select ABD beneficiaries to morecost-effectively manage health care services.In designing its ABD program, Ohio madecritical departures from its current managedcare program for families and children.Specifically, the care management require-ments for the ABD health plans will beincreased to focus not only on a single condi-tion but also on the complexities of multiplecomorbid conditions. Further, the state’s per-formance measurement set was expanded tobetter represent the unique needs of the pop-ulation. The state will also use plan-specificenrollment data to risk adjust the healthplan capitation rates to ensure an equitablepayment structure for plans serving benefici-aries with more complex needs.
In Colorado, while many stakeholders stilloppose major managed care expansions forthe ABD population due to an unsatisfac-tory experience with an earlier mandatorymanaged care enrollment initiative, thelegislature recently approved a small pilotmanaged care program for people with spe-cial needs. It is fashioned after theMassachusetts Commonwealth CareAlliance program. In keeping with thestate’s preference for local and nonprofitsolutions, the authorizing legislation stipu-lates that the program be developed by alocal nonprofit organization with experi-ence in the disability arena.
Creating medical homes is also the intentof Washington, which plans to transitionthe ABD population into managed careover the next three to five years. The statedefines managed care to include PCCMand aggressive chronic care managementmodels. The focus of the effort will be toestablish medical homes, actively managethe care of this population, and increaseconsumer engagement. There is consider-able interest from current Medicaid plans aswell as several new plans entering the mar-ket. Implementation challenges anticipatedby the state include: building adequate net-works (particularly for specialty care); riskadjustment; and incorporating structuredcase management into PCCM.
Wisconsin operates a mandatory Medicaidmanaged care program for ABD recipients.The program is currently operational in fivecounties, but the state plans to expand theprogram into 37 additional counties overthe next year and a half. Wisconsin attrib-utes the success of its ABD Medicaid man-aged care initiative to:
• Integrated care teams, which provideholistic, patient-centered and high-qualitycare;
• An automatic enrollment approach (discussed later in this document); and
• The requirement that plans assess mem-bers and develop a care plan in the first60 days of enrollment.
However, not all states have been as suc-cessful in implementing managed carestrategies for the ABD population. For thelast two years, California has attempted toimplement mandatory enrollment of theABD population in Medi-Cal managedcare, including a scaled-down pilot pro-gram, but the state was not able to securelegislative approval or the support of keyadvocacy organizations. The state is cur-rently seeking other options to enroll ABDbeneficiaries in managed care (page 14).
Seeking Higher Value in Medicaid: A National Scan of State Purchasers
10

There is considerable state interest inmanaged long-term care, but a num-ber of barriers are slowing the rate ofadoption.
While the pursuit of managed care for all orpart of the ABD population, including dualeligibles, is in full swing in a number ofstates, the “tipping point” for capitatingMedicaid long-term care (LTC) services forany of these beneficiaries is still far off onthe horizon. Aside from Arizona, with itslong-established Arizona Long Term CareSystem (ALTCS) program of capitated long-term care, and now Wisconsin, Texas, andNew York, few states are aggressively movingforward with the implementation ofstatewide programs.
Texas, in particular, is poised for growth inits managed long-term care efforts, extend-ing integrated managed acute and long-termcare into several new areas of the state. Aspart of this effort the state is expanding itscurrent mandatory capitated program,STAR+PLUS, to four new metropolitanareas and will extend its non-capitatedIntegrated Care Management program toone new area. Managed care plans areresponsible for the first four months of nurs-ing home care, but after that the memberreceives services through the fee-for-servicesystem. This approach (modeled after theMinnesota Senior Health Options program)is designed to encourage home- and commu-nity-based alternatives. Texas is just oneexample of a state that is experimentingwith payments and incentives that promotecare in the community and decrease institu-tional placements, a major challenge forstates pursuing managed LTC programs.
Wisconsin offers several innovative pro-grams that provide managed long-term carefor ABD beneficiaries, including dual eligi-bles. The four sites in the WisconsinPartnership Program integrate care acrossthe full spectrum of Medicaid and Medicare
services, including long-term care. Thestate’s Family Care program provides capitat-ed Medicaid long-term care services to10,000 Medicaid beneficiaries through coun-ty-based managed care organizations. Thestate is preparing to launch a statewideexpansion of Family Care to encourage thedevelopment of multi-county consortia andpublic-private partnerships. While FamilyCare is a voluntary program, the state mayimplement an “automatic enrollment withopt-out” option paralleling the enrollmentdesign for its ABD managed care program.By contrast, expansion of the WisconsinPartnership Program is stymied by a highdegree of stakeholder skepticism aboutMedicare managed care.
A number of other states are also interestedin developing managed care programs thatintegrate the full range of services for theABD population, including dual eligibles.Florida recently received waiver approvalfrom the Centers for Medicare and MedicaidServices (CMS) to create an integrated,managed long-term care delivery system forMedicaid beneficiaries age 60 and older. Theproposed program, Florida Senior Care, willprovide all Medicaid services, includinglong-term care, using managed care organiza-tions to build integrated service deliverymodels under fixed payment financing. Thestate believes that the coordination of allMedicaid services under one organizationwill establish accountability for the deliveryof high-quality comprehensive health andlong-term care services to its seniors.
Hawaii is also planning a substantial man-aged care expansion for its ABD population(including dual-eligible beneficiaries) thatwill include long-term care, carving in nurs-ing facility and home- and community-basedservices. The state will begin a phased-inimplementation in 2008, beginning with theelderly and persons with physical disabilitiesand ending with enrollment of the
Seeking Higher Value in Medicaid: A National Scan of State Purchasers
11

developmentally disabled/ mentally retard-ed population.
As in Florida, Maryland’s proposedCommunityChoice program will cover pri-mary, acute, and long-term care services.The program will be mandatory for dual-eligible members, adult Medicaid-only consumers who meet a nursing facility levelof care, and any other Medicaid consumersage 65 and over. Under CommunityChoice,the state will make capitation payments toCommunity Care Organizations (CCOs)that will be responsible for providing pri-mary, acute, and long-term care services,including many of the services that are cur-rently available only through a 1915(c)waiver. Behavioral health services will becarved out. In addition, participating CCOsmust be licensed as Medicare Advantageplans to facilitate the integration ofMedicare services and funding for the dualeligibles. These organizations will berequired to provide care coordination andoffer a consumer-directed model for thedelivery of personal care services. Byincluding primary, acute, and long-termcare services under one capitation payment,Maryland believes that it will create anenvironment for integrated care andimproved outcomes.
Meanwhile, Georgia is expandingSOURCE, a modified Program of AllInclusive Care for the Elderly (PACE).SOURCE uses case managers to integrateMedicare acute care and Medicaid home-and community-based services for frail eld-erly and persons with disabilities. The pro-gram, which was recently approved to oper-ate statewide, is expected to expand fromserving 7,000 to approximately 10,000 vol-untary enrollees.
In some states Medicare AdvantageSpecial Needs Plans are generatingconsiderable interest from plans and Medicaid; other states are notyet prepared to partner.
The Medicare Modernization Act’s SpecialNeeds Plan provision, which creates anopportunity for integration of Medicaidand Medicare services for dual eligiblesincluding long-term care, is creating sub-stantial interest in some states. IntegratingMedicare and Medicaid via SNPs providesstates with an opportunity to improve thequality, coordination, and cost-effectivenessof care for the duals. Some states also viewSNPs as a way to gain access to informa-tion on prescription drug utilization by dualeligibles that was lost with the creation ofMedicare Part D.
In Oregon, about 60% of duals are alreadyenrolled in Medicaid managed care. Ten ofthe state’s 13 Medicaid plans serving dualshave Medicare SNP status, which greatlyfacilitated the Part D transition process.State officials noted that dual-eligible ben-eficiaries in these plans had a much easiertransition than those in other plans. Theyalso discussed the possibility of developinga pilot program that would combineMedicare, Medicaid acute and long-termcare, and mental and dental health fundinginto one program. Furthermore, the statealso believes that a number of the 10Medicaid plans with SNP status are inter-ested in and capable of managing long-term care services. Oregon will be develop-ing potential mechanisms for contractingwith these plans in the near future.
Despite the significant administrative andoperational challenges to integratingMedicare and Medicaid, several states areactively pursuing capitated contracts withSNPs. Although there is no specificrequirement for Florida Senior Care con-
Seeking Higher Value in Medicaid: A National Scan of State Purchasers
12

tractors to be SNPs, the state anticipatesthat some SNPs will apply, and is open tocontracting with them. In addition, Floridarecently approved a policy shift that willallow dual-eligible beneficiaries to enroll inMedicaid managed care. This shift was madeto facilitate a state strategy to contract withSNPs to integrate care for the duals. Floridaanticipates implementing the program inthe next year. Washington currently con-tracts with two SNPs that provide managed,integrated acute and long-term care fordual-eligible members and Medicaid-onlyconsumers in two areas of the state. To bettersupport these plans in meeting consumerneeds, the state is working to set rates thatmore accurately reflect the cost of long-termcare, particularly home- and community-based services.
In Texas, there are nine SNPs, includingtwo that were approved by CMS to auto-matically enroll dual eligibles who were planmembers prior to receiving SNP approval(called passive enrollment). In addition tothe current nine, at least two of the plansparticipating in the STAR+PLUS programare planning to establish SNPs, and willthen jointly manage the full spectrum ofMedicare and Medicaid services (exceptMedicaid inpatient care, which is currentlycarved out). Outside of the STAR+PLUSprogram, the state has not pursued payingSNPs or other Medicare Advantage plans acapitated rate for long-term care, as officialsare unsure how Medicaid will share in anysavings resulting from better care manage-ment. Initial savings, most likely throughreduced hospital utilization, will accrue onlyto Medicare. Unless Medicaid can share inMedicare savings, the fiscal advantages tothe state of integrating Medicaid andMedicare through SNPs are potentiallymodest. This concern is shared by all statesinterested in integrating Medicare andMedicaid for duals.
In Michigan, two Medicaid plans, includingone of the largest in the state, have receivedapproval to operate as Medicare SNPs. Thestate is considering developing managedlong-term care pilots with these plans.However, state implementation efforts wouldbe hampered by the state’s enrollment system,which currently excludes all dual eligiblesfrom enrollment in managed care plans.
Several other states are in a “watchful wait-ing” mode vis-à-vis SNPs. Colorado,California, Georgia, Hawaii, Ohio,Pennsylvania, and Kentucky are potentiallyinterested in partnering with SNPs, but arenot yet ready to do so. Colorado faces severalbarriers, including a state law that, inessence, prohibits Medicaid managed long-term care except through a PACE program.Several of these other states, although inter-ested in working with SNPs, are in the midstof multiple Medicaid reforms and feel thatthe time is not right for entering into newarrangements with additional plans.
States are making concerted efforts to build support for ABD managedcare models from advocates and legislators.
The emergence and growth of alternativemanaged care models for the ABD popula-tion is driven by several factors, includingconcerns from stakeholder groups regardingprovider networks, access to services, andconsumer choice. State Medicaid leadershave invested considerable time and effort inbuilding the case for managed care with leg-islatures and forging partnerships with inter-ested stakeholders.
Wisconsin cites the involvement of con-sumers in contract development as one keyto the success of its managed care initiativefor the ABD population. Medicaid con-sumers were included in the negotiationteams for each of the ABD managed carecontracts. This helped strengthen consumer
Seeking Higher Value in Medicaid: A National Scan of State Purchasers
13

buy-in, and led to the negotiation of sever-al important contract requirements toassure quality, including the in-depth evaluation of a plan’s provider network as a condition of certification. Having con-sumers at the table enabled the state toproceed with its “automatic enrollment”approach, in which all beneficiaries areenrolled in managed care but have theability to opt out under certain circum-stances.
The support or opposition of legislatorsoften determines how states proceed withmanaged care plans for the ABD popula-tion. In Ohio, for example, legislative support tempered opposition from somegroups, and state officials are now workingcollaboratively with stakeholders to ensurea smooth transition. Provider opposition,which has been limited and mainlyemanates from hospitals, is based on solvency and reimbursement issues.
Michigan is one of a number of stateswhere term limits have required a renewedeffort to educate legislators on the poten-tial benefits of managed care every four tosix years. In some states, such as Colorado,the legislature has strongly influenced thedirection of Medicaid managed care. InPennsylvania and Georgia, by contrast, leg-islative pressure is not as significantbecause less of the Medicaid program iscontained in statute in these states, givingthe Medicaid agency more flexibility.
Seeking Higher Value in Medicaid: A National Scan of State Purchasers
14
As in Colorado, the California legislaturehas played a major role in determining thefuture of managed care. Although the gov-ernor’s office has strongly backed managedcare expansions, the California legislaturehas been reluctant to approve all proposals.The legislature recently approved a geo-graphic expansion of full-risk managed carein 13 of 58 counties (in addition to the 22counties already in managed care), but itwould not approve mandatory enrollmentof the ABD population in all managed carecounties. (California currently enrollsABD beneficiaries on a mandatory basis inits county organized health systems[COHS] in eight counties.) The legislaturehas encouraged increased efforts to volun-tarily enroll the ABD population in non-COHS counties and has approved fundingfor the development of performance stan-dards and a state-financed consumer educa-tion effort encouraging people with disabil-ities to explore the benefits of full-riskmanaged care.

Seeking Higher Value in Medicaid: A National Scan of State Purchasers
15
Generally, there has been growing continu-ity and stability among the plans participat-ing in Medicaid managed care. Mergers havebecome less disruptive because they oftenpair an existing local plan with a largernational entity. The overall stability has pro-duced many positive effects, includingimproved state-plan communication andcollaboration and continuity of enrollmentfor consumers. But some state Medicaidleaders wonder if the stability could have acost. Will stable markets translate into lessaggressive or innovative efforts by plans toimprove quality and increase efficiencies?
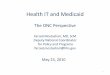
While states agree on the need to increasequality and efficiency in Medicaid managedcare, opinions vary about how to do this.Some states have focused primarily on devel-oping and strengthening quality partnershipswith a stable group of at-risk plans. Otherstates, seeing healthy competition amongplans as key to higher performance, areencouraging new market entrants. Still oth-ers hope that new managed care models,including EPCCM and care management,might increase innovation and competitionbetween divergent models, if not amongplans. Regardless of the method, most statesagree that they want more from managedcare, and they are using their purchasingpower to ensure that medical homes areaccountable in terms of both quality andcost. To that end, states are employing anumber of tools — including improved datainfrastructure, pay for performance programs,health information technology (HIT), con-sumer engagement, and chronic care man-agement — to get more from managed careprograms (Figure 5).
States are strengthening data-related infrastructure both to maximize their purchasing power and to support care management initiatives.
States are becoming increasingly sophisti-cated in their use of data to improve pur-chasing strategies. Whether expandingcapitated managed programs or developingnew care management approaches, statesrealize they need better data from theirplans and providers, a more advanced datainfrastructure, and stronger in-house expert-ise than was required in the past. Newstate tasks may include: using claims data toidentify and stratify target populations fordisease management; analyzing claims toexamine disease prevalence, predict recur-rences, and design interventions; acquiringand validating encounter data to measureand reward quality; and developing per-formance measurement approaches (e.g.,HEDIS-like measures) for EPCCM and care
Theme 3: States now realize that they can do much more withtheir purchasing power than merely secure financial predictability,and they are acting accordingly. Increasing quality, efficiency, andaccountability are all important goals.
Figure 5: Tools Scan States Are Pursuing toEnhance Managed Care
Pay forPerformance
Initiative
EnhancedData
Collection/Infrastructure
ConsumerEngagement
Other (CareManagement,
Standardization,etc.)
14
12
10
8
6
4
2
0
Source: State interviews. Note: Figures are not unduplicated counts.
Num
ber
of S
tate
s (n
=14
)

Seeking Higher Value in Medicaid: A National Scan of State Purchasers
management programs. States increasinglyview data and systems improvements as keyto achieving quality and efficiency gains, astance that is bolstered by broad support forhealth information technology comingfrom national, political, and health careleadership.
To support better chronic care and caremanagement, two states have implementedor are considering initiatives to provideconsumer-level data to plans and providers.Recently, Michigan offered plans 12months of historical encounter data fortheir new members, although so far just twoplans have requested the data. Similarly,Pennsylvania is considering reinstating itsformer practice of providing historical uti-lization data to plans for their new members.
States are also harnessing the power ofencounter data submitted by health plans.States can use encounter data to monitorhealth plan performance and patient uti-lization patterns, implement provider profil-ing, and identify high-risk beneficiaries forcare management. With less access to fee-for-service utilization data in states transi-tioning to managed care, perhaps the mostimportant use of health plan encounterdata for states is in rate setting and riskadjustment for plan payments. Florida,which historically has not focused onencounter data collection, used its recentmanaged care reform initiative to requireencounter data submission. Florida willbegin to use the data immediately to riskadjust and set appropriate plan-specific cap-itation rates. Florida plans to use encounterdata to better monitor quality measuresfrom its health plans and report that infor-mation publicly on an ongoing basis.
More advanced data analysis examining thesize of primary care provider practices andtheir performance on chronic care measures
has given Michigan new insights intowhere beneficiaries receive care. In a studyof Wayne County (Detroit), Michiganfound that approximately half of theMedicaid beneficiaries receive primary carefrom small one- and two-physician prac-tices. This will require the state to workwith its health plans to determine how toimprove quality in smaller practices thatoften lack the infrastructure found in largerentities.
States are looking for ways to alignpayment and quality. The leadingstrategy is pay for performance.
Incentive programs are emerging inMedicaid as a way to improve health careservices and outcomes. Whereas reimburse-ment in health care has traditionallyfocused on volume — the more patients aphysician sees, the more he or she gets paid— pay-for-performance (P4P) programsattempt to better align payment and qualitywith the goal of improving the efficiency,timeliness, and quality of care.6 Not surpris-ingly, many states are using P4P to pursuequality improvement and performancegoals. These efforts are increasingly special-ized and tailored to the states’ needs,whether that is improving quality, promot-ing prevention, strengthening care manage-ment, or increasing managed care participa-tion in quality improvement activities.
Ohio has invested considerable resources inP4P initiatives, holding 1% of the premiumat risk for graduated performance-basedpayments. Tiered incentives are paid basedon plan performance. The highest pay-ments go to plans achieving SuperiorPerformance (for satisfactory performanceon 21 measures) while somewhat lowerpayments are made to plans achievingExcellent Performance (for satisfactory per-formance on three measures). Although
16
6 N. Highsmith and J. Reller Rothstein. Rewarding Performance in Medicaid Managed Care. Center for Health Care Strategies, Inc. March 2006. http://www.chcs.org/usr_doc/MedicaidP4PBrief.pdf

Seeking Higher Value in Medicaid: A National Scan of State Purchasers
17
strategies may vary by health plan and /orgeographic area, many plans also provideincentives at the physician level to secureprovider panels, improve quality of care,and enhance consumer access to preventivecare outside regular office hours. Someplans partner with providers on profit/risksharing to help address systems issues suchas e-billing. Incentives to promote healthcare compliance at the consumer level arealso quite common. Leveraging the successof its P4P effort with managed care plans,Ohio would like to extend performance-based payment to its fee-for-service program.
Likewise, Michigan has established a with-hold pool to fund for its P4P initiative. The$3 million P4P capitation bonus pool isused to pay managed care organizationsbased on their performance on five clustersof measures. Some Michigan plans haveincorporated these performance-based pay-ments into capitated provider contracts.Others have reverted to fee-for-serviceprovider payment as a way to more easilygenerate the encounter data needed todemonstrate performance for the state P4Pinitiative. Both Hawaii and Wisconsin arealso developing P4P efforts. Wisconsin’sP4P initiative will focus on dental care,lead testing, birth outcomes and tobaccouse cessation. Future efforts will focus onchronic care. Washington has incentivesfor EPSDT screening and childhood immu-nizations and would also like to adopt an“outcomes focus” to encourage care man-agement. Under pressure from providers togive more generous rate increases (abovethe usual 2 to 4% increases), Washington isconsidering increasing rates through pay-for-performance initiatives rather thanacross the board.
Maryland has initiated sanctions, but notrewards, for plan performance on 11 meas-ures, including HEDIS and locally devel-oped indicators, such as lead screening for
children. The state is planning to instituteperformance awards in addition to penaltiesin 2007.
Pennsylvania is focusing its P4P efforts onencouraging better chronic care manage-ment. As part of ACCESS PLUS, the statecontracts with a disease management ven-dor to coordinate care for several chronicdiseases, including asthma, diabetes, chron-ic heart failure, chronic obstructive pul-monary disorder and coronary artery dis-ease. The program’s vendor has 5% of itsper member per month fee for the PCCMportion of its contract tied to incentives/penalties based on five measures related tobetter screening and prevention. In addi-tion, ACCESS PLUS operates a P4P pro-gram to encourage primary care physiciansto participate and play an active, collabora-tive role with the disease management pro-gram. Pennsylvania is also developing aquality measurement and performance sys-tem for the EPCCM program, which wouldpotentially produce HEDIS-like measuresfrom fee-for-service data, as well as institut-ing P4P programs within its full-risk managedcare program, HealthChoices. The managedcare plans can earn bonuses of up to half apercent of premium, based on improvementon 10 HEDIS measures. Pennsylvania alsoencourages managed care plans to reduceunnecessary emergency room visits andinpatient stays by building incentivesdirectly into the rate-setting process.
Other states (Colorado, Florida, Georgia,and Oregon) are interested in developingP4P efforts, but face barriers including con-cerns about the sources of funding for P4Pinitiatives and lack of plan and data capaci-ty to make it work. Oregon is interested indeveloping P4P efforts, although it wouldlike to do so with new money, instead ofwithholds from current plan payments.While interested in P4P, Colorado feelsthat this strategy would not be effective

Seeking Higher Value in Medicaid: A National Scan of State Purchasers
18
without more robust competition amongplans — the state has voluntary enrollmentand a very limited number of full-risk plans(two at the time of the interviews, sincethen reduced to one). Florida is similarlyinterested in P4P initiatives, but needs tostrengthen its encounter-data system to cre-ate the baseline and measure progress.
Another form of incentives for health plansis default enrollment, or auto-assignment ofnew members to those plans with the high-est performance. California has implement-ed an auto-assignment algorithm in 14counties that rewards higher quality planswith more default assignments of memberswho do not actively choose a plan forthemselves. California bases the algorithmon five HEDIS measures and two measuresof plan participation with safety-netproviders. The state believes this will helpmotivate the plans to improve their per-formance, resulting in higher quality carefor the approximately 2.7 million managedcare enrollees that reside in the participat-ing counties.
To increase participation in its managedcare programs, Wisconsin recently imple-mented automatic Medicaid managed careenrollment with an opt-out provision forthe Milwaukee ABD population, resultingin a 92% retention rate. Yet plan-imposedenrollment caps and a lack of provider net-works in rural areas of the state still limitstatewide participation. The state is consid-ering establishing incentives — dubbed“enrollment P4P” — to reward plans forincreasing enrollment by expanding their
service areas or relaxing their enrollmentcaps.
Beyond P4P, states are trying new approaches to hold plansaccountable.
Pay-for-performance approaches are not theonly strategies states are using to improveperformance and care management. Oregonhas required all plans to have exceptional-needs coordinators, and feels that this is agood model for helping consumers navigateboth medical and social services. Havingseen positive results from its disease man-agement programs serving the fee-for-serv-ice population, the state is also consideringincluding specific disease managementrequirements in its managed care contracts.
Several states are grappling with how tocreate more standardization across plans forquality improvement. Georgia joins a num-ber of other states in having standard quali-ty improvement requirements, and has alsoimplemented uniform disease measurementrequirements across plans. Ohio is interest-ed in standardizing performance measuresacross plans and measuring performance atthe provider level, rather than just at theplan level. The state is researching optionsthat will enhance its current P4P structuresand will be viable in its expanded full-riskmanaged care environment. Through itsnew Medicaid Management InformationSystem (MMIS) procurement, the stateplans to give providers patient registriesand daily access to patient health status.The state’s commitment to value-based

Seeking Higher Value in Medicaid: A National Scan of State Purchasers
purchasing can also be seen in the scoringsystem used for its recent procurement ofplans to serve the ABD population (Figure6). Of the 1,000 available points, over halfwere allocated for quality improvementtools that plans could use to improvepatient outcomes and cost-effectivenesssuch as performance improvement/clinicalmanagement systems, information systems,and a robust provider panel.7
Some states are implementingreforms that vary benefits by eligibil-ity group and ask consumers tochoose among coverage options.
Both Florida and Kentucky have proposednew reform initiatives that will vary benefitpackages by eligibility group and offer con-sumers a choice of coverage options, includ-ing a health savings account-like option.Enrollees in Florida may earn credits towardtheir “Enhanced Benefits Accounts” if theypursue identified healthy behaviors. Whilea great deal of policy debate has focused onthe potential benefits and risks of thisapproach, its significance in the short termis not clear. The consumer-direction ele-ments will only be implemented in twoFlorida counties, and will allow healthplans to create customized benefit packagestailored to a target population. As ofOctober 2006, Florida had contracted with14 plans. The plans have offered creativepackages by targeting co-payments, limiting
select services, and offering additional serv-ices. Examples of additional servicesinclude preventive adult dental services,home-delivered meals post-surgical care,respite care, and acupuncture services. Thestate is implementing “choice counselors”to help consumers select among plans, andis also grappling with how best to providequality data on available plans andproviders to Medicaid consumers.Developing better approaches to monitor-ing plan quality remains an issue. AlthoughFlorida is joined by a number of other states— most notably South Carolina, WestVirginia, and Kentucky — in exploringways of enhancing the consumer role inchoosing care and health healthy behaviors,the concepts are too new and untested inMedicaid to say much more than “staytuned” and wait for results from early evalu-ations of these experiments.
Reimbursement rates continue to be a key issue for states.
Whether attempting to increase reimburse-ment rates to build provider or plan partici-pation, or managing the effects of stagnantrates, states remain concerned with reim-bursement issues. In an effort to enhanceprovider participation, especially in ruralareas, Maryland hopes to increase providerrates until they are at least comparable toMedicare rates. After a gubernatorally-initiated review of all Medicaid plans,California obtained rate increases from thelegislature for several plans. Meanwhile, thestate has engaged a consulting firm to makerecommendations on its rate methodologythat will allow development of rates thatare more predictive of plan costs.
In states with low or declining rates, plancomplaints, as opposed to outright with-drawal from the market, have been thenorm. Having experienced a 12% ratedecrease in the last year, some Oregon plans
Figure 6: Ohio ABD Procurement Scoring System
Mandatory Application Requirements Review Pass/Fail
Experience & Compliance History 200
Delegation 100
Performance Improvement and Clinical Management 250
Information Systems 100
HIPAA 50
Provider Panel (region-specific) 300
Total 1,000
7 “Industry Overview: MOH, CNC, & WLP Win Big on OH Awards.” Lehman Brothers Equity Research. October 9, 2006. p.5.
19

may now be operating in the red, but so farnone have dropped Medicaid. In a depar-ture from this trend, Colorado’s largestplan, and one of only two full-risk entities,announced it would withdraw fromMedicaid managed care in response to thestate’s announcement of a significant ratedecrease that resulted from a legislativelymandated rate methodology. Even beforethe plan left the market, Medicaid officialsin Colorado were interested in attractingnew plans, and had been approached bytwo national Medicaid managed care enti-ties. State officials are not optimistic, how-ever, about their success in contractingwith these plans, given that the state legis-lature has typically resisted entry by out-of-state plans. In Georgia, state officials haveattempted to avoid plan complaints intheir new full-risk managed care programby requiring the plans to bid their rates aspart of the proposal, rather than having thestate set rates in the more traditional man-ner. While this method may not eliminateplan dissatisfaction with rates altogether,
the state hopes it will reduce the number ofcomplaints in the short term, since theplans bid their own rates.
Because of the burden of annual rate nego-tiations, Medicaid leaders in Pennsylvaniasay it is difficult to establish a meaningful,ongoing quality partnership with plans.Medicaid officials are exploring adopting atwo-year rate period, which might allowmore breathing room for state-plan collab-oration on quality and other issues beyondrates.
The actuarial soundness of rates may pres-ent an additional challenge to states.While the states included in this scan didnot have much to say about the issues theyare facing regarding actuarial soundnessrequirements overall, it seems likely that asthey go forward with managed care expan-sions, actuarial soundness may particularlyimpact their ability to include non-tradi-tional, supplemental support services aspart of their managed care programs.
Seeking Higher Value in Medicaid: A National Scan of State Purchasers
20

Seeking Higher Value in Medicaid: A National Scan of State Purchasers
21
edicaid and managed care have comea long way together, proving that
they indeed have a lasting relationship.8
Together they have successfully evolved,adapting to continuing changes in the man-aged care marketplace and responding tostate budget priorities. Today’s definition ofMedicaid managed care goes far beyond thetraditional full-risk model. States are using avariety of innovative mechanisms, includingenhanced primary care case management,disease management, and comprehensive caremanagement to effectively manage high-quality and cost-effective care for Medicaidbeneficiaries.
Satisfied with the opportunities for increasedquality and efficiency that Medicaid managedcare, in all its forms, is able to provide, manystates are now looking to it to developaccountable medical homes not only for chil-dren and families, but for adults with chronicconditions and seniors as well. Elderly adultsand those with complex health needs repre-sent only one-quarter of the 55 million peo-ple served by Medicaid, yet they consumenearly 70% of the program’s resources.9 Byshifting the focus from managing the costs tomanaging the care of this population, statessee an opportunity to reap long-term value inimproved health outcomes and reduced costs.
Overall, the subset of states interviewed forthis scan have become more sophisticatedpurchasers both in reaction to external budg-et pressures and due to internal recognitionthat they can use their purchasing leverage toobtain better value. States are adopting newtools to achieve quality and efficiencyimprovements, including new approaches formanaging care; incentives for improving
performance; standardized process and out-come measures; consumer engagement strate-gies; and methods to systematically collectencounter data. Indeed, a recent 50-state sur-vey by the Kaiser Commission on Medicaidand the Uninsured confirmed that progres-sively more states are focusing on qualityimprovement and disease management tocurb long-term costs and improve quality,particularly for high-cost beneficiaries.10
Medicaid managed care’s first 20 years haveshown that as the program continues toevolve, states will expect managed care toevolve with it. This is already being tested assome states try out the flexibility provided bythe Deficit Reduction Act of 2005 (DRA).While some of the states included in the scanhave used or are considering using DRAauthority to implement new cost sharing orexpand home-and community-based services,others appear to be taking more of a wait andsee approach when it comes to integratingthe DRA into their Medicaid managed carestrategies in the near term.
Medicaid is challenged to provide health careservices for a rapidly expanding and vastlydiverse group of Americans, including adultswith complex chronic conditions and disabil-ities, the low-income elderly, and a dispropor-tionate number of consumers in racial andethnic minority populations. Throughincreasingly sophisticated and varied models,state purchasers are demanding more valuefor public expenditures and are effectively tar-geting investments to deliver high-qualityhealth care services and, ultimately,improved health outcomes, for Medicaidbeneficiaries.
Conclusion
8 R. Hurley and S. Somers. “Medicaid and Managed Care: A Lasting Relationship?” Health Affairs 22.1 (2003): 77-88.
9 Medicaid Program at a Glance, op. cit. 10 V. Smith, et al. Low Medicaid Spending Growth Amid Bounding State Revenues: Results from a 50 State Medicaid Budget Survey State Fiscal Years 2006 and
2007. Kaiser Family Foundation. October 2006. http://www.kff.org/medicaid/upload/7569.pdf
M

Seeking Higher Value in Medicaid: A National Scan of State Purchasers
State Total Distribution of Medicaid % of Medicaid Overall % Aged, Blind &Medicaid Enrollment Population by Eligibility Population with Dual Managed Care Disabled in
(June 2005) Group Eligibility Status Penetration Managed Care
California 6,552,553 Children, 50% 15% 50% 19%Adults, 27%Elderly, 12%
Blind and Disabled, 11%Colorado 410,445 Children, 59% 14% 30% 19%
Adults, 17%Elderly, 10%
Blind and Disabled, 12%Florida 2,247,559 Children, 53% 17% 67% 11%
Adults, 7%Elderly, 17%
Blind and Disabled, 13%Georgia 1,377,746 Children, 60% 9% 57% 0%
Adults, 17%Elderly, 9%
Blind and Disabled, 14%Hawaii12 200,534 Children, 47% 10% 80% 0%
Adults, 32%Elderly, 10%
Blind and Disabled, 11%Kentucky 692,053 Children, 51% 17% 69% 36%
Adults, 13%Elderly, 12%
Blind and Disabled, 24%Maryland 701,601 Children, 60% 12% 70% 0%
Adults, 14%Elderly, 7%
Blind and Disabled, 18%Michigan 1,435,236 Children, 55% 14% 66% 41%
Adults, 19%Elderly, 9%
Blind and Disabled, 17%Ohio 1,711,152 Children, 55% 11% 57% 0%13
Adults, 21%Elderly, 8%
Blind and Disabled, 16%
Oregon 411,478 Children, 41% 13% 80% 65%Adults, 41%Elderly, 7%
Blind and Disabled, 11%Pennsylvania 1,697,693 Children, 48% 17% 62% 55%
Adults, 17%Elderly, 23%
Blind and Disabled, 12%Texas 2,767,261 Children, 59% 24% 71% 20%
Adults, 17%Elderly, 12%
Blind and Disabled, 12%Washington 963,057 Children, 56% 10% 49% 3%
Adults, 24%Elderly, 13%
Blind and Disabled, 7%Wisconsin 862,426 Children, 40% 19% 54% 35%
Adults, 27%Elderly, 16%
Blind and Disabled, 17%
11 Information presented in both Appendix 1 and Appendix 2 was taken from each state’s Medicaid website, the CMS website, and Kaiser State Health Facts and validated by the states.
12 Data presented for Hawaii have not been validated by the state.13 The ABD population is currently excluded from Ohio Medicaid managed care; however, the state will begin enrolling approximately 125,000 SSI consumers in
December 2006.
APPENDIX 1: MEDICAID OVERVIEW IN SCAN STATES11
22

23
14D
ata
pres
ente
d fo
r H
awai
i hav
e no
t be
en v
alid
ated
by
the
stat
e.
AP
PE
ND
IX 2
: M
ED
ICA
ID M
AN
AG
ED
CA
RE
PR
OG
RA
MS
OV
ER
VIE
W I
N S
CA
N S
TATE
S
Popu
lati
ons
Serv
ed
Type
of
Rela
tion
ship
wit
h by
Med
icai
d M
anag
edM
anag
ed C
are
Bene
fits
Incl
uded
in M
CO
Sp
ecia
l Nee
ds P
lans
ST
ATE
Car
e Pr
ogra
ms
Del
iver
y Sy
stem
Geo
grap
hyEn
rollm
ent
or P
CC
M P
rogr
am(S
NPs
) Inte
rest
St
ate-
Cur
rent
lyin
TAN
FA
BDD
uals
PCC
MM
CO
Lim
ited
wid
eM
anda
tory
Volu
ntar
yA
cute
LTC
BHC
ontr
act
Con
trac
t
Cal
ifo
rnia
Co
lora
do
Flo
rid
a
Geo
rgia
Haw
aii14
Ken
tuck
y
Mar
ylan
d
✓ ✓ ✓ ✓ ✓ ✓ ✓
✓ ✓ ✓ ✓ ✓ ✓ ✓
In c
erta
inco
untie
s
✓ ✓ ✓ ✓ ✓
In c
erta
inco
untie
s
Cur
rent
lyin
clud
ed
in H
CBS
man
aged
care
wai
ver
prog
ram
and
will
be
incl
uded
infu
ture
LTC
prog
ram
✓
✓ ✓ ✓ ✓
✓ ✓ ✓ ✓ ✓ ✓ ✓
✓ ✓
Refo
rm in
two
pilo
tco
untie
s
✓ ✓
✓ ✓ ✓ (Not
Pa
sspo
rtH
ealth
Pla
n
✓
For c
erta
in
aid
code
s in
al
l cou
ntie
s;
for a
ll ai
d co
des
in
CO
HS
✓C
urre
ntly
choi
ce
betw
een
PCC
M a
ndM
CO
s ex
clud
ing
refo
rm
coun
ties
(Exc
ept
SOU
RCE)
✓
✓(E
xcep
tPa
sspo
rt H
ealth
Pla
n)
✓
For c
erta
in
aid
code
s in
non-
CO
HS
coun
ties
✓
Refo
rm
initi
ativ
e w
ill
be v
olun
tary
fo
r cer
tain
popu
latio
ns
✓ ✓ ✓
✓ ✓ ✓ ✓ ✓ ✓ ✓
Lim
ited
cove
rage
in
cer
tain
plan
s an
d fu
lly
cove
red
in 4
pla
ns
in 7
CO
HS
coun
ties
Will
be
incl
uded
in
Flo
rida
Seni
or
Car
e on
ly
In S
OU
RCE
only
✓
✓(E
xcep
tPa
sspo
rt H
ealth
Pla
n)
Plan
s to
incl
ude
in fu
ture
prog
ram
✓ ✓
✓(E
xcep
tPa
sspo
rt H
ealth
Pla
n)
✓
✓

24
AP
PE
ND
IX 2
: M
ED
ICA
ID M
AN
AG
ED
CA
RE
PR
OG
RA
MS
OV
ER
VIE
W I
N S
CA
N S
TATE
S
Popu
lati
ons
Serv
ed
Type
of
Rela
tion
ship
wit
h by
Med
icai
d M
anag
edM
anag
ed C
are
Bene
fits
Incl
uded
in M
CO
Sp
ecia
l Nee
ds P
lans
ST
ATE
Car
e Pr
ogra
ms
Del
iver
y Sy
stem
Geo
grap
hyEn
rollm
ent
or P
CC
M P
rogr
am(S
NPs
) Inte
rest
St
ate-
Cur
rent
lyin
TAN
FA
BDD
uals
PCC
MM
CO
Lim
ited
wid
eM
anda
tory
Volu
ntar
yA
cute
LTC
BHC
ontr
act
Con
trac
t
Mic
hig
an
Ohi
o
Ore
go
n
Penn
sylv
ania
Texa
s
Was
hing
ton
Wis
cons
in
✓
✓ ✓ ✓ ✓ ✓ ✓
✓ ✓ ✓ ✓ ✓
✓
A po
rtion
will
bein
clude
d in
expa
nsio
n
✓ ✓ ✓ Pilo
t in
tegr
ated
prog
ram
s
✓
✓ ✓ Pilo
t in
tegr
ated
prog
ram
s
✓
✓ ✓ ✓ ✓
✓
✓ ✓ ✓ ✓ ✓ ✓
✓
✓ ✓ ✓ ✓
✓
Will
be
stat
ewid
eby
12/
06
✓ ✓
✓
In c
erta
in
coun
ties
by12
/06
In c
erta
in
coun
ties
In c
erta
in
coun
ties
For T
AN
F po
pula
tions
inST
AR
HM
Os;
A
BD in
ST
AR
+PLU
S; fo
rTA
NF
and
ABD
in P
CC
M
✓ (E
xcep
t for
th
e tw
o pi
lot
inte
grat
ed
prog
ram
s)
For T
AN
F po
pula
tions
whe
re 2
+H
MO
s; d
uals
✓
In c
erta
in
coun
ties
In c
erta
in
coun
ties
In c
erta
in
coun
ties
For A
BD
in S
TAR
HM
Os
ABD
may
op
t-out
✓
✓ ✓ ✓ ✓ ✓
✓N
ot in
Fam
ily
Car
e
✓
Lim
ited
toPA
CE
and
20 d
ays
SNF
✓
In S
TAR
+PLU
S se
rvic
ear
eas
In p
ilot
inte
grat
edpr
ogra
ms
Onl
y in
Fam
ily
Car
e an
dPa
rtner
ship
Prog
ram
✓(N
ot
subs
tanc
eab
use)
✓ ✓ ✓
✓C
arve
d ou
t of
Nor
th-
STA
R(D
alla
s ar
ea)
In p
ilot
inte
grat
edpr
ogra
ms
✓
✓ ✓ ✓

Center for Health Care Strategies, Inc.CHCS200 American Metro Blvd., Suite 119Hamilton, NJ 08619 Phone: (609) 528-8400Fax: (609) 586-3679
www.chcs.org