Embed Size (px)
DESCRIPTION
Evidence for the Duration of Antibiotic Therapy. Charles Feldman Professor of Pulmonology Charlotte Maxeke Johannesburg Academic Hospital University of the Witwatersrand. Potential COI to Declare. Abbott , Aspen-GSK,Jansen , MSD, Pfızer , Sanofi. Introduction to the Talk. - PowerPoint PPT Presentation
Citation preview
Charles FeldmanProfessor of Pulmonology
Charlotte Maxeke Johannesburg Academic Hospital University of the Witwatersrand
Abbott, Aspen-GSK,Jansen, MSD, Pfızer, Sanofi
Potential COI to Declare
CAP is one of the leading causes of morbidity and mortality throughout the world – 5.6 million cases diagnosed annually
Little consensus on most appropriate duration of antibiotic therapy and recent recognition that prolonged therapy may be related to development of resistance
A range of recommendations are found encompassing courses of between 5 – 14 days
Introduction to the Talk
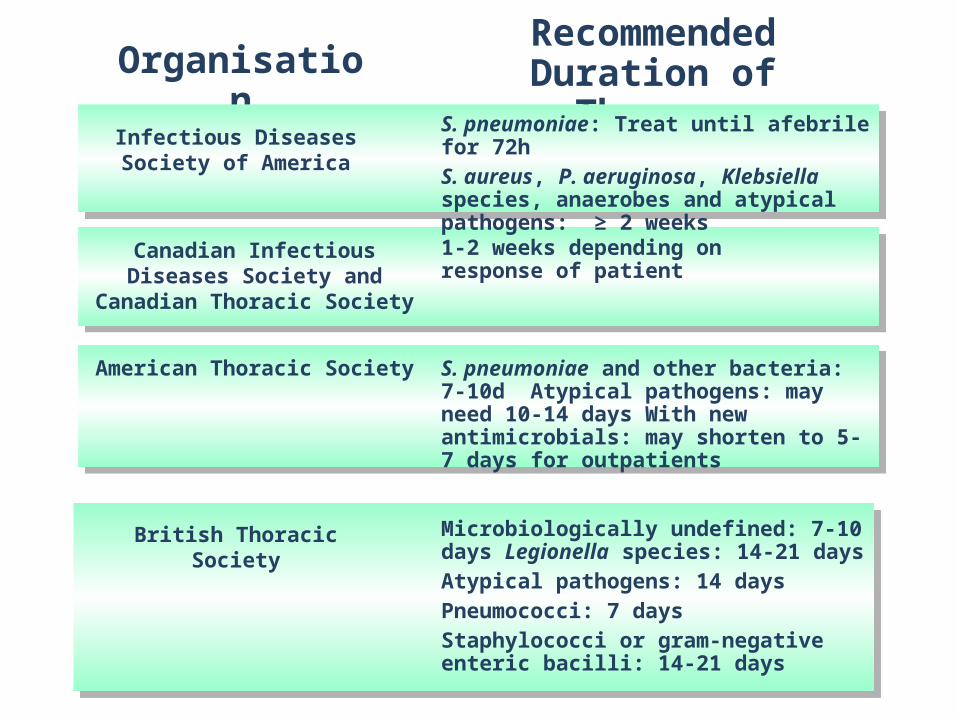
1-2 weeks depending on response of patient
Canadian Infectious Diseases Society and Canadian Thoracic
Society
S. pneumoniae and other bacteria: 7-10d Atypical pathogens: may need 10-14 days With new antimicrobials: may shorten to 5-7 days for outpatients
American Thoracic Society
Microbiologically undefined: 7-10 days Legionella species: 14-21 daysAtypical pathogens: 14 daysPneumococci: 7 daysStaphylococci or gram-negative enteric bacilli: 14-21 days
British Thoracic Society
OrganisationRecommended
Duration of TherapyS. pneumoniae: Treat until afebrile for 72hS. aureus, P. aeruginosa, Klebsiella species, anaerobes and atypical pathogens: ≥ 2 weeks
Infectious Diseases Society of America
Short course regimens (< 7 days) theoretically useful in reducing antimicrobial resistance and favouring improved patient compliance
Prolonged treatment especially with low-dose antibiotics was associated with increased carriage of PRSP in nasopharynx (3.5 x and 6 x respectively)
Patient compliance decreases after 5 days of treatment and with resolution of symptoms
Rationale for Short-Course Therapy
Scalera NM et al. Curr Opin Infect Dis 2007; 20: 177-181
Study recruited 2000 children aged 2 – 59 months with non-severe pneumonia (WHO criteria)
Patients randomly assigned to 3 days or 5 days treatment with oral amoxicillin
Primary outcome was treatment failure and analyses were intention to treat
Short Course Therapy - Beta-Lactams
MASCOT Pneumonia Study Group Lancet 2002; 360: 835-841
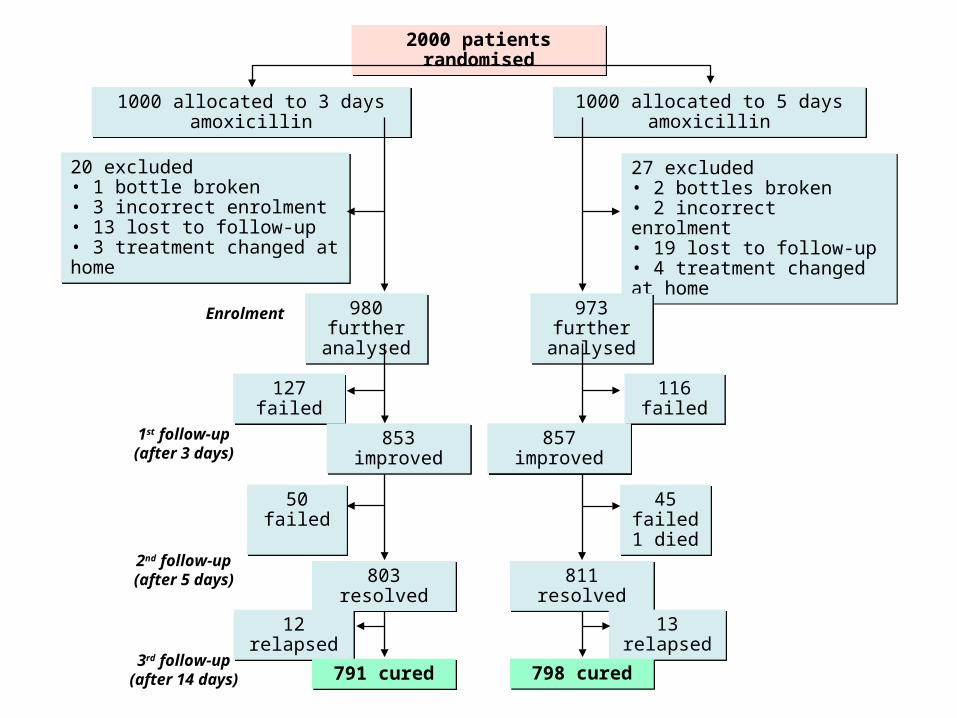
2000 patients randomised2000 patients randomised
20 excluded• 1 bottle broken• 3 incorrect enrolment• 13 lost to follow-up• 3 treatment changed at home
20 excluded• 1 bottle broken• 3 incorrect enrolment• 13 lost to follow-up• 3 treatment changed at home
27 excluded• 2 bottles broken• 2 incorrect enrolment• 19 lost to follow-up• 4 treatment changed at home
27 excluded• 2 bottles broken• 2 incorrect enrolment• 19 lost to follow-up• 4 treatment changed at home
980 further analysed
980 further analysed
973 further analysed
973 further analysed
127 failed127 failed 116 failed116 failed
853 improved853 improved 857 improved857 improved
45 failed1 died
45 failed1 died
50 failed50 failed
803 resolved803 resolved 811 resolved811 resolved
12 relapsed12 relapsed 13 relapsed13 relapsed
791 cured791 cured 798 cured798 cured
1000 allocated to 5 days amoxicillin
1000 allocated to 5 days amoxicillin
1000 allocated to 3 days amoxicillin1000 allocated to 3 days amoxicillin
Enrolment
1st follow-up (after 3 days)
2nd follow-up (after 5 days)
3rd follow-up (after 14 days)
Treatment failed in 209 (21%) patients in 3-day group and 202 (20%) patients in 5-day group
Overall 12 (1%) children in 3-day group and 13 (1%) children in 5-day group relapsed
Non-adherence was associated with failure of treatment in 5-day group (p<0.0001)
Treatment of Childhood Pneumonia
MASCOT Pneumonia Study Group Lancet 2002; 360: 835-841
Overall failure was most likely in children
that did not adhere to treatment (p<0.0001),
less than 12 months (p<0.0001),
whose illness lasted > 3 days (p=0.004),
whose RR was >10 breaths/min above the age specific cut-off (p=0.004),
with vomiting (p=0.009)
Treatment of Childhood Pneumonia
MASCOT Pneumonia Study Group Lancet 2002; 360: 835-841

Randomised, double-blind, multicentre study in children 2 – 59 months of age with non-severe pneumonia showed oral amoxicillin for three days to be as effective as five days
Cochrane database systematic review confirmed the evidence that short course therapy (3 days) was as effective as longer treatment (5 days) in children < 5 years with non-severe CAP
Treatment of Childhood Pneumonia
Agarwal G et al (ISCAP). BMJ 2004; 328: 791Haider BA et al. Cochrane Database Syst Rev 2008; Apr 16; (2): CD005976
Prospective study of hospitalised CAP following the implementation of early switch to oral antibiotics and early hospital discharge showed no difference in safety and patient satisfaction compared to historical controls
Prospective, randomised, parallel group study of non-severe CAP which indicated that abbreviated (2-day) course of i.v. antibiotics with rapid oral switch had similar clinical course and cure rates and lower costs
Treatment of Adult Pneumonia
Lee RW et al. Respirology 2007; 12: 111-116Siegel RE et al. Chest 1996; 110: 965-971
Multicentre, randomised, double-blind study comparing levofloxacin 750mg daily for 5 days versus 500mg daily for 10 days in mild-severe pneumonia
Clinical success rate was 92.4% versus 91.1% and microbiological eradication 93.2% versus 92.4%
Subgroup analysis confirmed benefit in elderly > 65 years
Short Course Therapy - Fluoroquinolones
Dunbar LW et al. Clin Infect Dis 2003; 37: 752-760Shorr AF et al. Clin Ther 2005; 27: 1251-1259
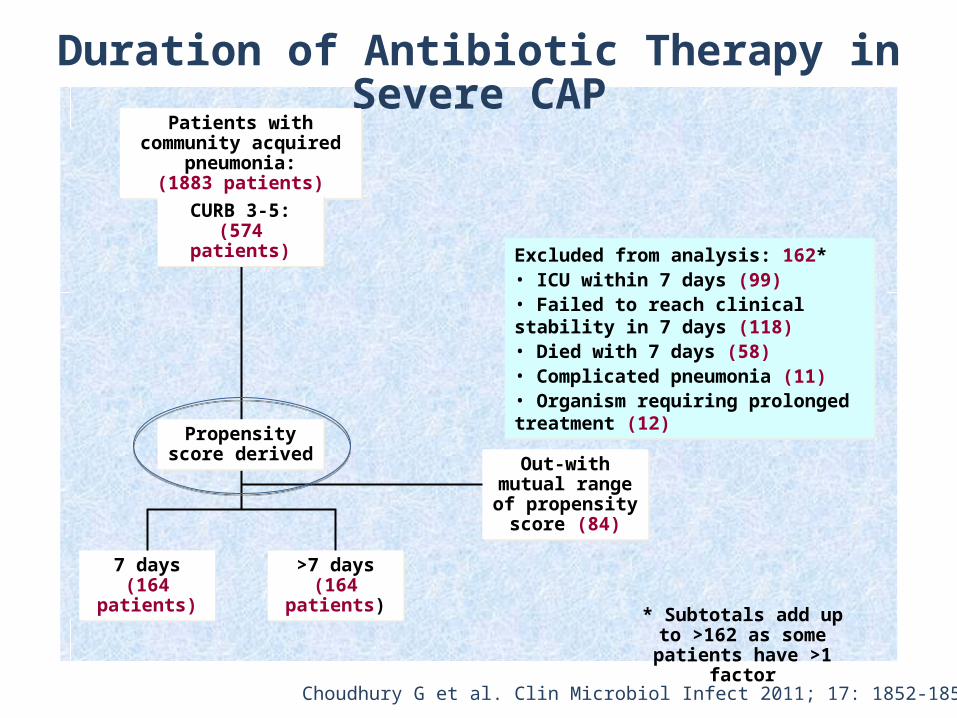
Duration of Antibiotic Therapy in Severe CAP
Patients with community acquired pneumonia:
(1883 patients)
Patients with community acquired pneumonia:
(1883 patients)
CURB 3-5:(574 patients)
CURB 3-5:(574 patients)
Excluded from analysis: 162*• ICU within 7 days (99)• Failed to reach clinical stability in 7 days (118)• Died with 7 days (58)• Complicated pneumonia (11)• Organism requiring prolonged treatment (12)
Excluded from analysis: 162*• ICU within 7 days (99)• Failed to reach clinical stability in 7 days (118)• Died with 7 days (58)• Complicated pneumonia (11)• Organism requiring prolonged treatment (12)
Propensity score derived
Propensity score derived
7 days(164
patients)
7 days(164
patients)
>7 days(164
patients)
>7 days(164
patients)
Out-with mutual range of
propensity score (84)
Out-with mutual range of
propensity score (84)
* Subtotals add up to >162 as some patients
have >1 factor
Choudhury G et al. Clin Microbiol Infect 2011; 17: 1852-1858
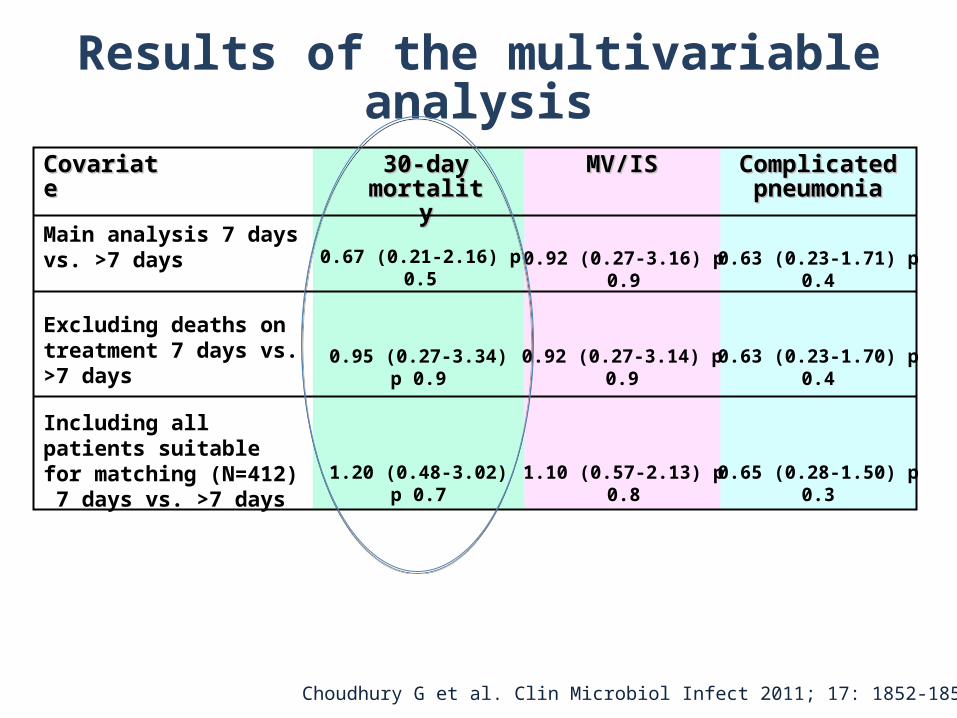
Results of the multivariable analysis
CovariateCovariate
Main analysis 7 days vs. >7 days 0.67 (0.21-2.16) p 0.5
Including all patients suitable for matching (N=412) 7 days vs. >7 days
Excluding deaths on treatment 7 days vs. >7 days
0.95 (0.27-3.34) p 0.9
1.20 (0.48-3.02) p 0.7
30-day 30-day mortalitymortality
MV/ISMV/IS Complicated Complicated pneumoniapneumonia
0.92 (0.27-3.16) p 0.9
0.92 (0.27-3.14) p 0.9
1.10 (0.57-2.13) p 0.8
0.63 (0.23-1.71) p 0.4
0.63 (0.23-1.70) p 0.4
0.65 (0.28-1.50) p 0.3
Choudhury G et al. Clin Microbiol Infect 2011; 17: 1852-1858
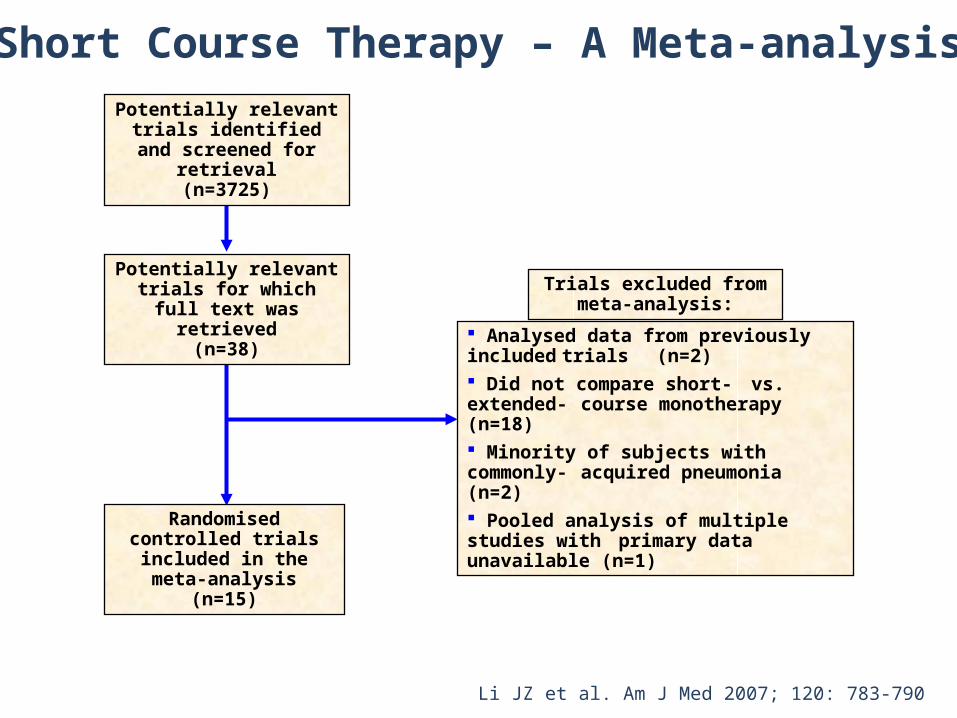
Potentially relevant trials identified and screened for
retrieval(n=3725)
Potentially relevant trials for which full text was retrieved
(n=38)
Randomised controlled trials included in the meta-
analysis(n=15)
Trials excluded from meta-analysis:
Analysed data from previously includedtrials (n=2)
Did not compare short- vs. extended- course monotherapy (n=18) Minority of subjects with commonly-acquired pneumonia (n=2) Pooled analysis of multiple studies with primary data unavailable (n=1)
Li JZ et al. Am J Med 2007; 120: 783-790
Short Course Therapy – A Meta-analysis
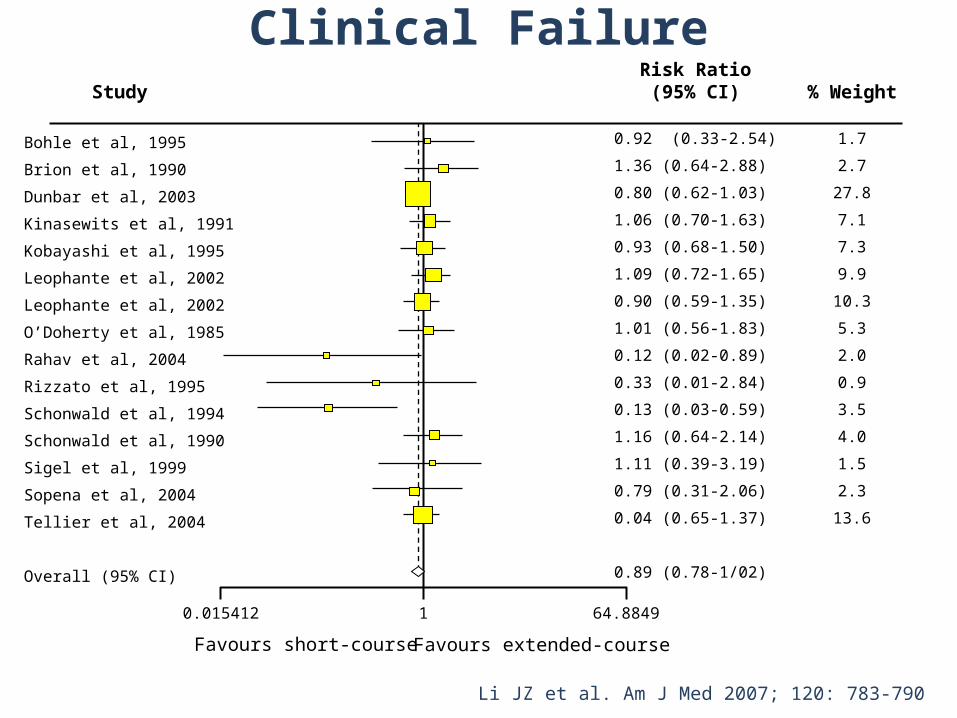
Bohle et al, 1995
Brion et al, 1990
Dunbar et al, 2003
Kinasewits et al, 1991
Kobayashi et al, 1995
Leophante et al, 2002
Leophante et al, 2002
O’Doherty et al, 1985
Rahav et al, 2004
Rizzato et al, 1995
Schonwald et al, 1994
Schonwald et al, 1990
Sigel et al, 1999
Sopena et al, 2004
Tellier et al, 2004
Overall (95% CI)
0.015412 64.88491
0.92 (0.33-2.54)
1.36 (0.64-2.88)
0.80 (0.62-1.03)
1.06 (0.70-1.63)
0.93 (0.68-1.50)
1.09 (0.72-1.65)
0.90 (0.59-1.35)
1.01 (0.56-1.83)
0.12 (0.02-0.89)
0.33 (0.01-2.84)
0.13 (0.03-0.59)
1.16 (0.64-2.14)
1.11 (0.39-3.19)
0.79 (0.31-2.06)
0.04 (0.65-1.37)
0.89 (0.78-1/02)
Favours short-course Favours extended-course
1.7
2.7
27.8
7.1
7.3
9.9
10.3
5.3
2.0
0.9
3.5
4.0
1.5
2.3
13.6
Risk Ratio(95% CI) % WeightStudy
Li JZ et al. Am J Med 2007; 120: 783-790
Clinical Failure
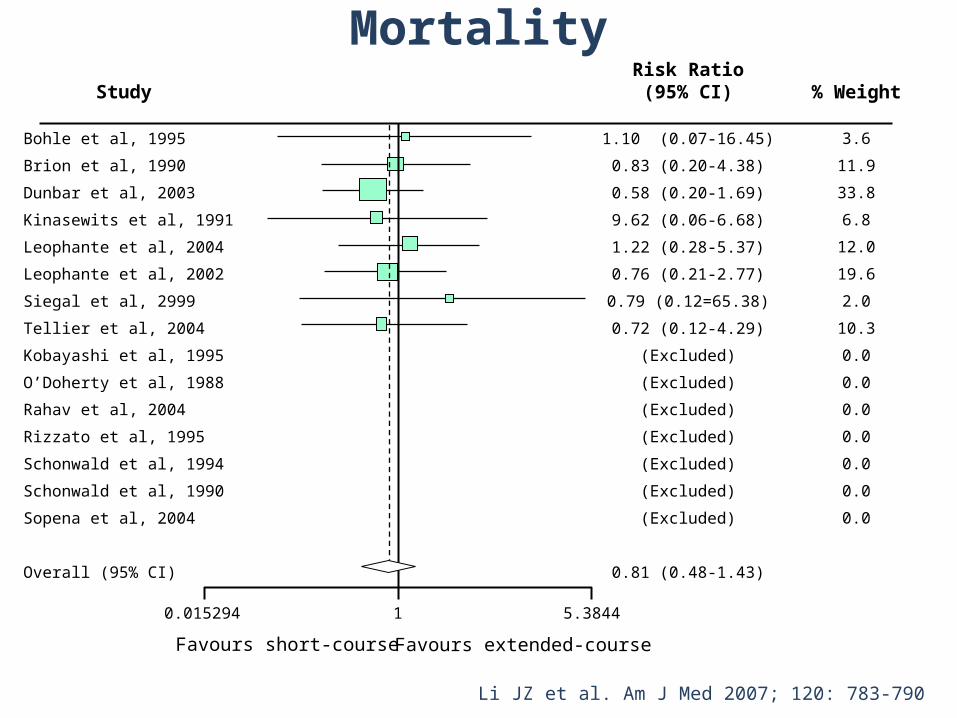
Bohle et al, 1995
Brion et al, 1990
Dunbar et al, 2003
Kinasewits et al, 1991
Leophante et al, 2004
Leophante et al, 2002
Siegal et al, 2999
Tellier et al, 2004
Kobayashi et al, 1995
O’Doherty et al, 1988
Rahav et al, 2004
Rizzato et al, 1995
Schonwald et al, 1994
Schonwald et al, 1990
Sopena et al, 2004
Overall (95% CI)
3.6
11.9
33.8
6.8
12.0
19.6
2.0
10.3
0.0
0.0
0.0
0.0
0.0
0.0
0.0
Risk Ratio(95% CI) % WeightStudy
1.10 (0.07-16.45)
0.83 (0.20-4.38)
0.58 (0.20-1.69)
9.62 (0.06-6.68)
1.22 (0.28-5.37)
0.76 (0.21-2.77)
0.79 (0.12=65.38)
0.72 (0.12-4.29)
(Excluded)
(Excluded)
(Excluded)
(Excluded)
(Excluded)
(Excluded)
(Excluded)
0.81 (0.48-1.43)
0.015294 5.38441
Favours short-course Favours extended-course
Li JZ et al. Am J Med 2007; 120: 783-790
Mortality
Clinical Implications of The Study
Adults with mild-moderate community-acquired pneumonia can be effectively treated with an antibiotic
regimen of 7 days or less
This result is consistent among the 4 antibiotic classes studies (macrolide, fluoroquinolone, beta-lactam, and ketolide)
There is a trend toward decreased adverse events with antibiotic regimens of 7 days or less
Li JZ et al. Am J Med 2007; 120: 783-790
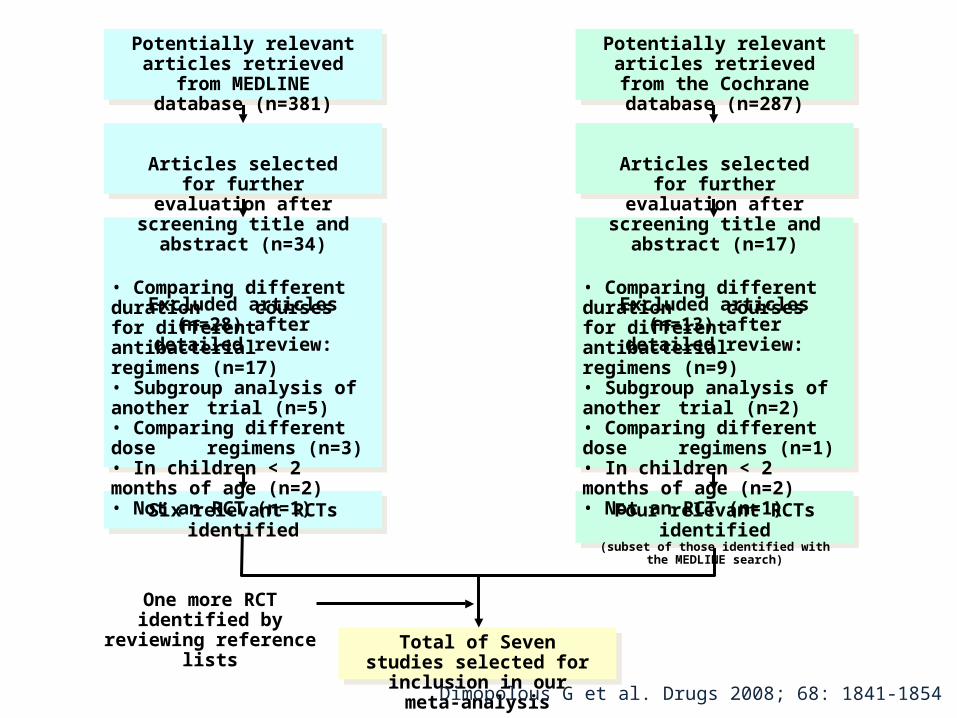
• Comparing different duration courses for different antibacterial
regimens (n=17)• Subgroup analysis of another trial (n=5)• Comparing different dose regimens (n=3)• In children < 2 months of age (n=2)• Not an RCT (n=1)
Six relevant RCTs identified
One more RCT identified by reviewing reference lists
Potentially relevant articles retrieved from the Cochrane
database (n=287)
Articles selected for further evaluation after screening title
and abstract (n=17)
Excluded articles (n=13) after detailed review:
• Comparing different duration courses for different antibacterial
regimens (n=9)• Subgroup analysis of another trial (n=2)• Comparing different dose regimens (n=1)• In children < 2 months of age (n=2)• Not an RCT (n=1)
Four relevant RCTs identified(subset of those identified with the MEDLINE search)
Total of Seven studies selected for inclusion in our meta-analysis
Potentially relevant articles retrieved from MEDLINE
database (n=381)
Articles selected for further evaluation after screening title
and abstract (n=34)
Excluded articles (n=28) after detailed review:
Dimopolous G et al. Drugs 2008; 68: 1841-1854
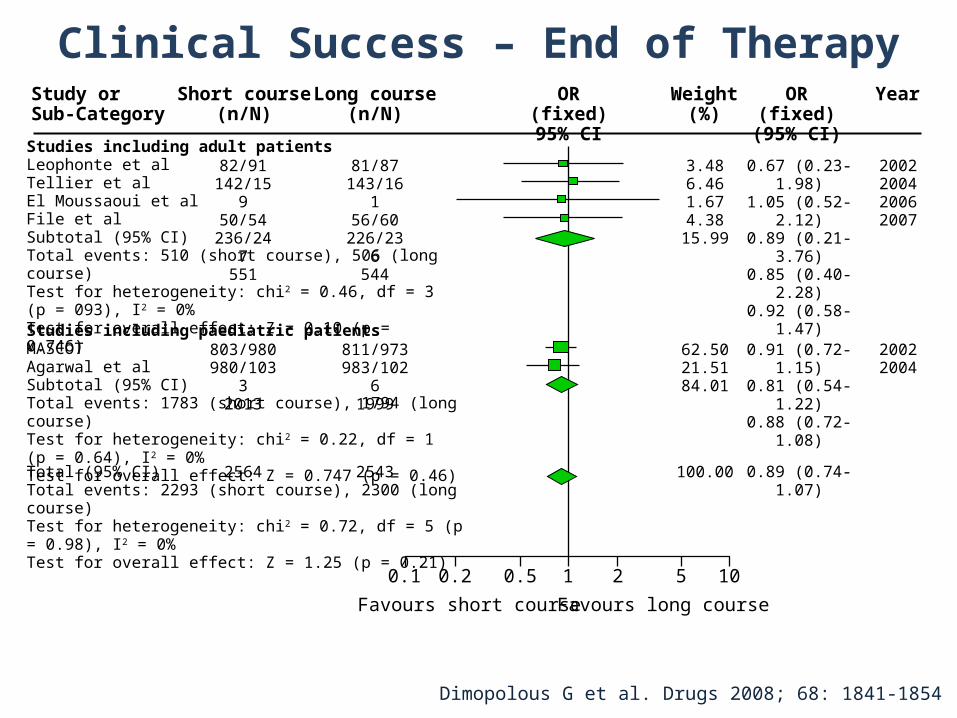
0.1 0.2 0.5 1 2 5 10
Favours short course Favours long course
Study orSub-Category
Short course(n/N)
Long course(n/N)
OR (fixed)95% CI
Weight(%)
OR (fixed)(95% CI)
Year
2002200420062007
20022004
Studies including adult patientsLeophonte et alTellier et alEl Moussaoui et alFile et alSubtotal (95% CI)Total events: 510 (short course), 506 (long course)Test for heterogeneity: chi2 = 0.46, df = 3 (p = 093), I2 = 0%Test for overall effect: Z = 0.10 (p = 0.746)
81/87143/16
156/60
226/236
544
82/91142/15
950/54
236/247
551
Studies including paediatric patientsMASCOTAgarwal et alSubtotal (95% CI) Total events: 1783 (short course), 1794 (long course)Test for heterogeneity: chi2 = 0.22, df = 1 (p = 0.64), I2 = 0%Test for overall effect: Z = 0.747 (p = 0.46)
Total (95% CI)Total events: 2293 (short course), 2300 (long course)Test for heterogeneity: chi2 = 0.72, df = 5 (p = 0.98), I2 = 0%Test for overall effect: Z = 1.25 (p = 0.21)
2564 2543
811/973983/1026
1999
803/980980/1033
2013
3.486.461.674.38
15.99
62.5021.5184.01
100.00 0.89 (0.74-1.07)
0.67 (0.23-1.98)1.05 (0.52-2.12)0.89 (0.21-3.76)0.85 (0.40-2.28)0.92 (0.58-1.47)
0.91 (0.72-1.15)0.81 (0.54-1.22)0.88 (0.72-1.08)
Dimopolous G et al. Drugs 2008; 68: 1841-1854
Clinical Success – End of Therapy
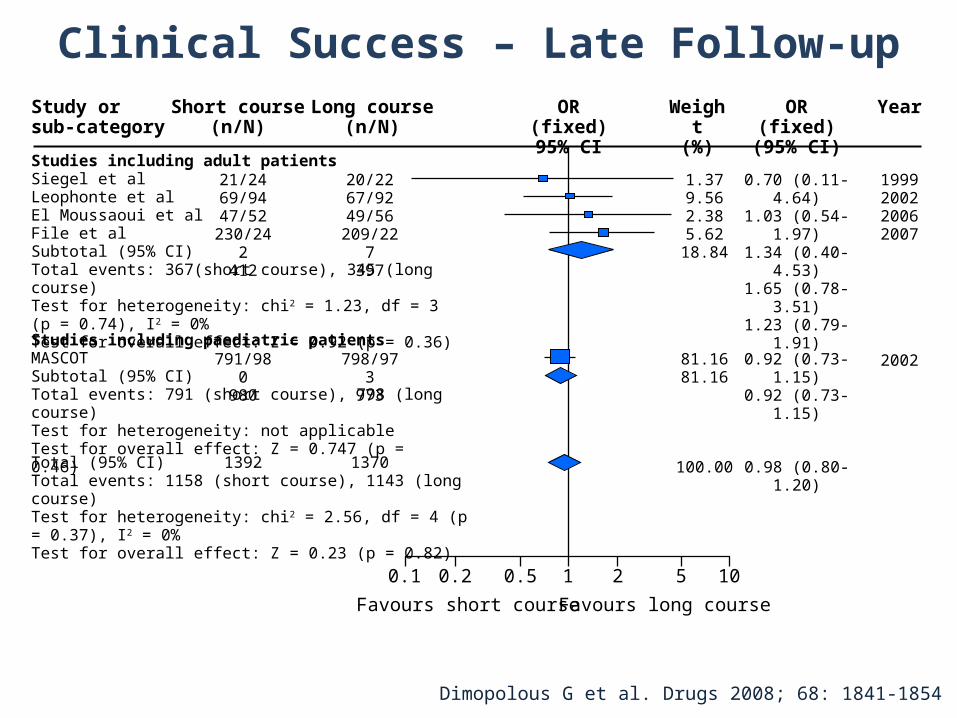
0.1 0.2 0.5 1 2 5 10
Favours short course Favours long course
Studies including adult patientsSiegel et alLeophonte et alEl Moussaoui et alFile et alSubtotal (95% CI)Total events: 367(short course), 345 (long course)Test for heterogeneity: chi2 = 1.23, df = 3 (p = 0.74), I2 = 0%Test for overall effect: Z = 0.92 (p = 0.36)
20/2267/9249/56
209/227
397
Study orsub-category
Short course(n/N)
Long course(n/N)
1.379.562.385.62
18.84
81.1681.16
100.00
OR (fixed)95% CI
Weight(%)
OR (fixed)(95% CI)
Year
21/2469/9447/52
230/242
412
Studies including paediatric patientsMASCOTSubtotal (95% CI) Total events: 791 (short course), 798 (long course)Test for heterogeneity: not applicableTest for overall effect: Z = 0.747 (p = 0.46)
1392
798/973
973
1370
791/980
980
Total (95% CI)Total events: 1158 (short course), 1143 (long course)Test for heterogeneity: chi2 = 2.56, df = 4 (p = 0.37), I2 = 0%Test for overall effect: Z = 0.23 (p = 0.82)
0.98 (0.80-1.20)
0.70 (0.11-4.64)1.03 (0.54-1.97)1.34 (0.40-4.53)1.65 (0.78-3.51)1.23 (0.79-1.91)
0.92 (0.73-1.15)0.92 (0.73-1.15)
1999200220062007
2002
Dimopolous G et al. Drugs 2008; 68: 1841-1854
Clinical Success – Late Follow-up
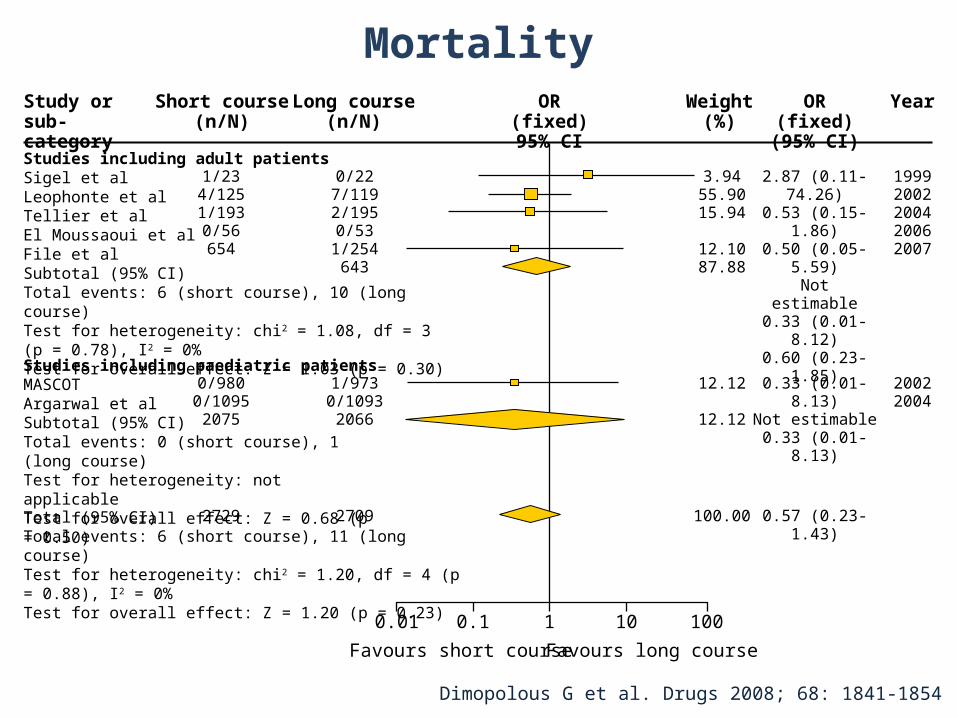
0.01 0.1 1 10 100
Favours short course Favours long course
0/227/1192/1950/53
1/254643
1/9730/10932066
2709
Study orsub-category
Short course(n/N)
Long course(n/N)
3.9455.9015.94
12.1087.88
12.12
12.12
100.00
2.87 (0.11-74.26)
0.53 (0.15-1.86)0.50 (0.05-5.59)Not estimable
0.33 (0.01-8.12)0.60 (0.23-1.85)
0.33 (0.01-8.13)Not estimable
0.33 (0.01-8.13)
0.57 (0.23-1.43)
19992002200420062007
20022004
OR (fixed)95% CI
Weight(%)
OR (fixed)(95% CI)
Year
Studies including adult patientsSigel et alLeophonte et alTellier et alEl Moussaoui et alFile et alSubtotal (95% CI)Total events: 6 (short course), 10 (long course)Test for heterogeneity: chi2 = 1.08, df = 3 (p = 0.78), I2 = 0%Test for overall effect: Z = 1.03 (p = 0.30)
Studies including paediatric patientsMASCOTArgarwal et alSubtotal (95% CI) Total events: 0 (short course), 1 (long course)Test for heterogeneity: not applicableTest for overall effect: Z = 0.68 (p = 0.50)
Total (95% CI)Total events: 6 (short course), 11 (long course)Test for heterogeneity: chi2 = 1.20, df = 4 (p = 0.88), I2 = 0%Test for overall effect: Z = 1.20 (p = 0.23)
1/234/1251/1930/56654
2729
0/9800/10952075
Dimopolous G et al. Drugs 2008; 68: 1841-1854
Mortality
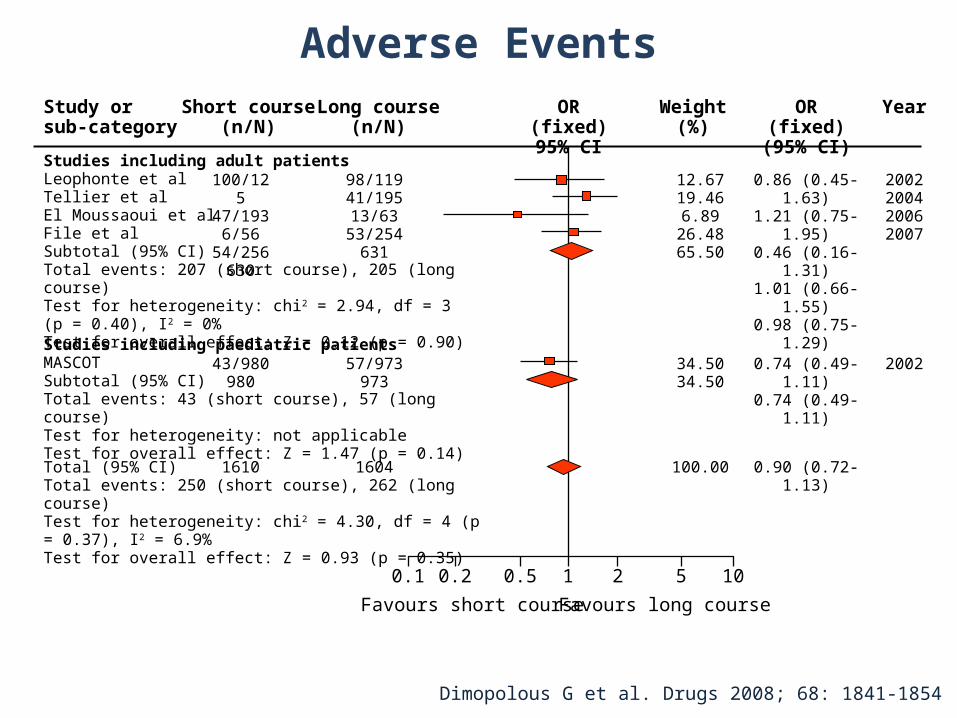
0.1 0.2 0.5 1 2 5 10
Favours short course Favours long course
Studies including adult patientsLeophonte et alTellier et alEl Moussaoui et alFile et alSubtotal (95% CI)Total events: 207 (short course), 205 (long course)Test for heterogeneity: chi2 = 2.94, df = 3 (p = 0.40), I2 = 0%Test for overall effect: Z = 0.12 (p = 0.90)
Studies including paediatric patientsMASCOTSubtotal (95% CI) Total events: 43 (short course), 57 (long course)Test for heterogeneity: not applicableTest for overall effect: Z = 1.47 (p = 0.14)
Total (95% CI)Total events: 250 (short course), 262 (long course)Test for heterogeneity: chi2 = 4.30, df = 4 (p = 0.37), I2 = 6.9%Test for overall effect: Z = 0.93 (p = 0.35)
100/125
47/1936/56
54/256630
43/980980
1610
98/11941/19513/63
53/254631
57/973973
1604
Study orsub-category
Short course(n/N)
Long course(n/N)
12.6719.466.89
26.4865.50
34.5034.50
100.00
0.86 (0.45-1.63)1.21 (0.75-1.95)0.46 (0.16-1.31)1.01 (0.66-1.55)0.98 (0.75-1.29)
0.74 (0.49-1.11)0.74 (0.49-1.11)
0.90 (0.72-1.13)
2002200420062007
2002
OR (fixed)95% CI
Weight(%)
OR (fixed)(95% CI)
Year
Dimopolous G et al. Drugs 2008; 68: 1841-1854
Adverse Events
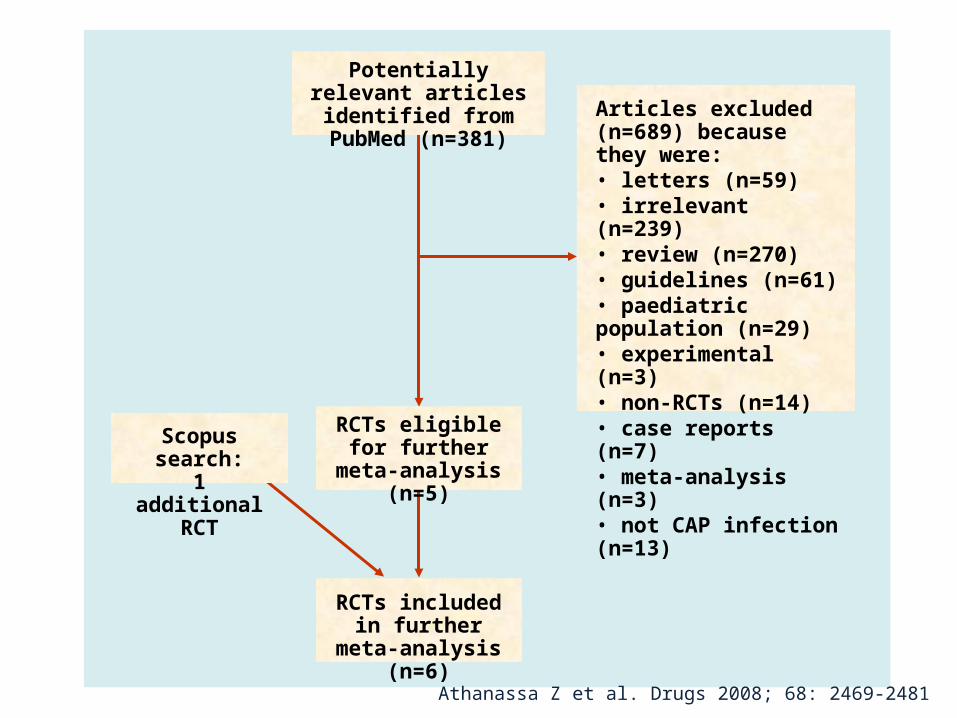
Articles excluded (n=689) because they were:• letters (n=59)• irrelevant (n=239)• review (n=270)• guidelines (n=61)• paediatric population (n=29)• experimental (n=3)• non-RCTs (n=14)• case reports (n=7)• meta-analysis (n=3)• not CAP infection (n=13)
RCTs included in further meta-analysis
(n=6)
Scopus search:1 additional RCT
Potentially relevant articles identified from PubMed
(n=381)
RCTs eligible for further meta-analysis
(n=5)
Athanassa Z et al. Drugs 2008; 68: 2469-2481
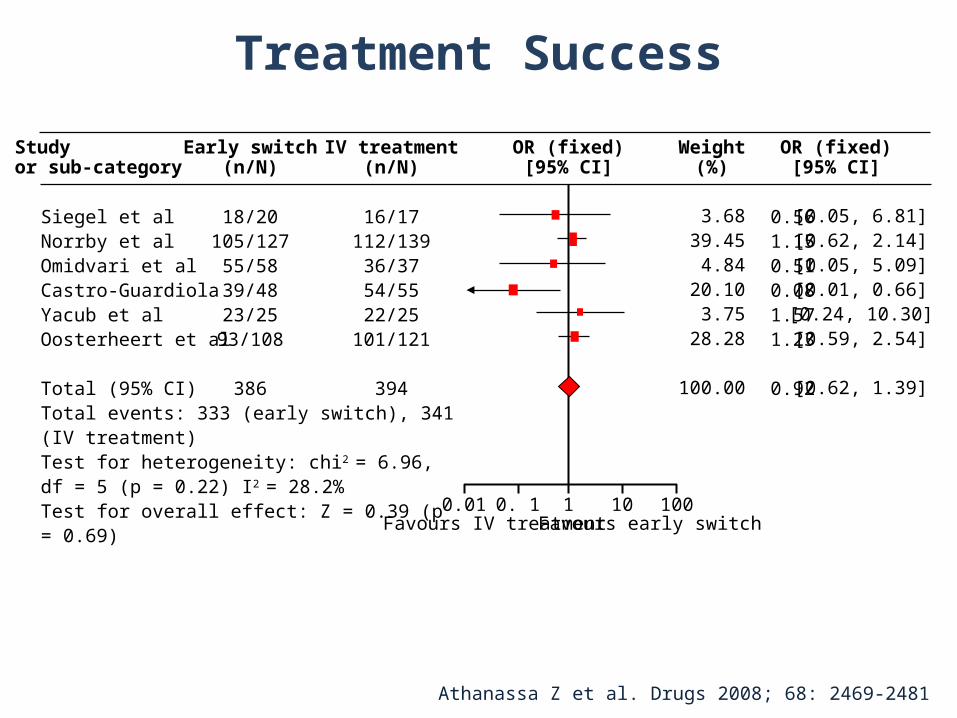
0.01 0. 1 1 10 100Favours IV treatment Favours early switch
Siegel et alNorrby et alOmidvari et alCastro-GuardiolaYacub et alOosterheert et al
Total (95% CI)Total events: 333 (early switch), 341 (IV treatment)Test for heterogeneity: chi2 = 6.96, df = 5 (p = 0.22) I2 = 28.2%Test for overall effect: Z = 0.39 (p = 0.69)
18/20105/12755/5839/4823/2593/108
386
16/17112/13936/3754/5522/25
101/121
394
3.6839.454.84
20.103.75
28.28
100.00
0.561.150.510.081.571.23
0.92
[0.05, 6.81][0.62, 2.14][0.05, 5.09][0.01, 0.66][0.24, 10.30][0.59, 2.54]
[0.62, 1.39]
Studyor sub-category
Early switch(n/N)
IV treatment(n/N)
OR (fixed)[95% CI]
Weight(%)
OR (fixed)[95% CI]
Athanassa Z et al. Drugs 2008; 68: 2469-2481
Treatment Success
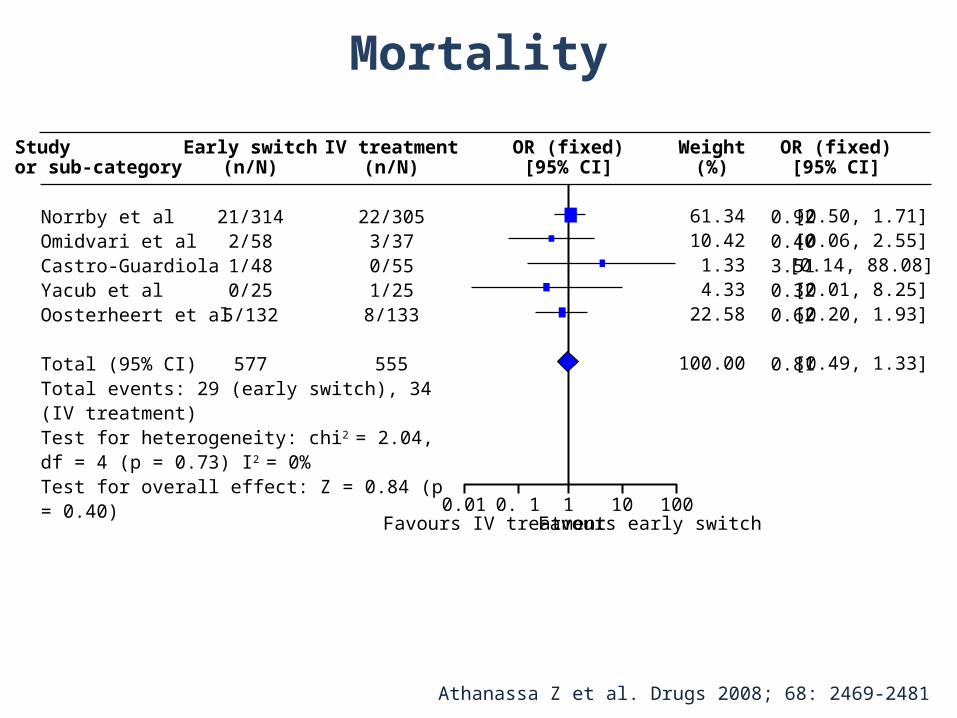
0.01 0. 1 1 10 100Favours IV treatment Favours early switch
Norrby et alOmidvari et alCastro-GuardiolaYacub et alOosterheert et al
Total (95% CI)Total events: 29 (early switch), 34 (IV treatment)Test for heterogeneity: chi2 = 2.04, df = 4 (p = 0.73) I2 = 0%Test for overall effect: Z = 0.84 (p = 0.40)
21/3142/581/480/25
5/132
577
22/3053/370/551/25
8/133
555
61.3410.421.334.33
22.58
100.00
0.920.403.510.320.62
0.81
[0.50, 1.71][0.06, 2.55][0.14, 88.08][0.01, 8.25][0.20, 1.93]
[0.49, 1.33]
Studyor sub-category
Early switch(n/N)
IV treatment(n/N)
OR (fixed)[95% CI]
Weight(%)
OR (fixed)[95% CI]
Athanassa Z et al. Drugs 2008; 68: 2469-2481
Mortality
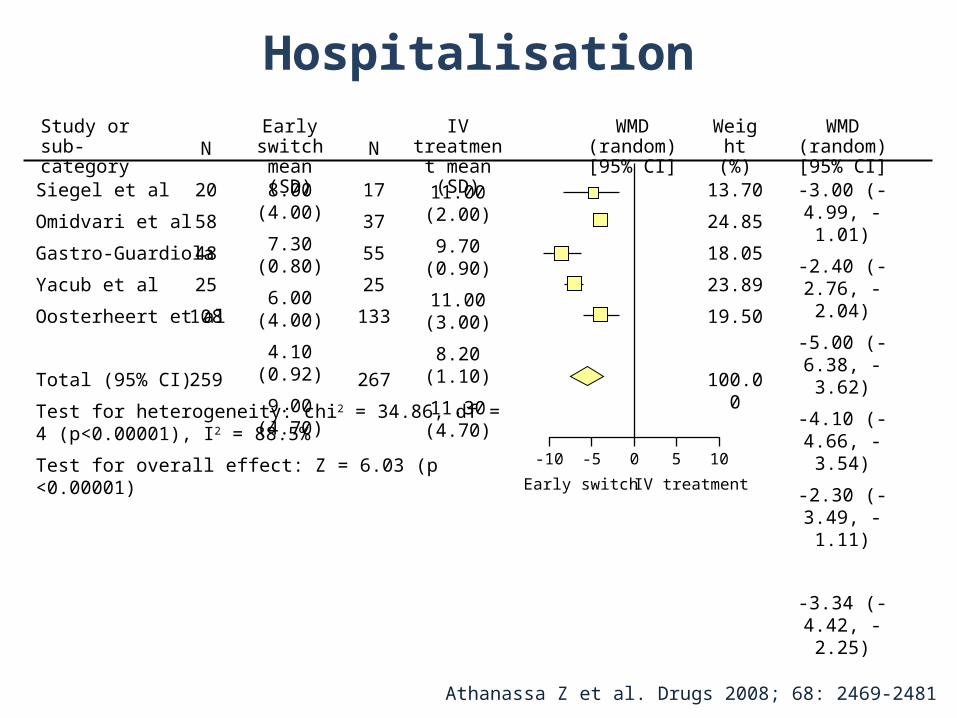
Siegel et al
Omidvari et al
Gastro-Guardiola
Yacub et al
Oosterheert et al
Total (95% CI)
Test for heterogeneity: chi2 = 34.86, df = 4 (p<0.00001), I2 = 88.5%
Test for overall effect: Z = 6.03 (p <0.00001)-10
Study orsub-category N
Early switch mean (SD)
13.70
24.85
18.05
23.89
19.50
100.00
Weight(%)
20
58
48
25
108
259
8.00 (4.00)
7.30 (0.80)
6.00 (4.00)
4.10 (0.92)
9.00 (4.70)
N
17
37
55
25
133
267
IV treatment mean (SD)
11.00 (2.00)
9.70 (0.90)
11.00 (3.00)
8.20 (1.10)
11.30 (4.70)
WMD (random) [95% CI]
WMD (random) [95% CI]
-3.00 (-4.99, -1.01)
-2.40 (-2.76, -2.04)
-5.00 (-6.38, -3.62)
-4.10 (-4.66, -3.54)
-2.30 (-3.49, -1.11)
-3.34 (-4.42, -2.25)
-5 0 5 10
Early switch IV treatment
Athanassa Z et al. Drugs 2008; 68: 2469-2481
Hospitalisation
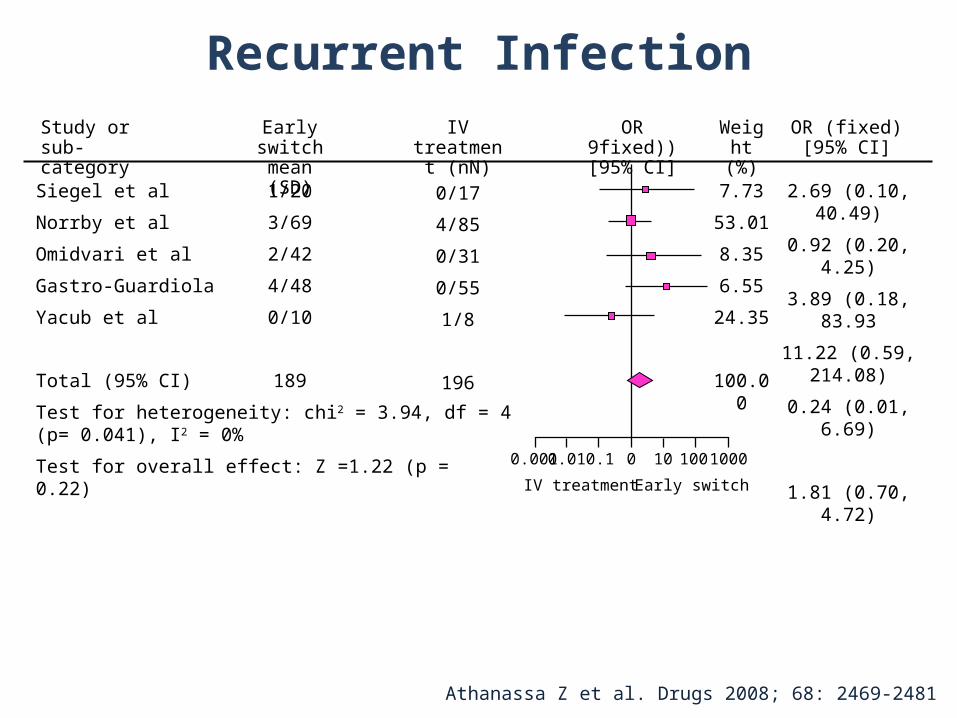
Siegel et al
Norrby et al
Omidvari et al
Gastro-Guardiola
Yacub et al
Total (95% CI)
Test for heterogeneity: chi2 = 3.94, df = 4 (p= 0.041), I2 = 0%
Test for overall effect: Z =1.22 (p = 0.22)0.001
Study orsub-category
Early switch mean (SD)
7.73
53.01
8.35
6.55
24.35
100.00
Weight(%)
1/20
3/69
2/42
4/48
0/10
189
IV treatment (nN)
0/17
4/85
0/31
0/55
1/8
196
OR 9fixed)) [95% CI]
OR (fixed) [95% CI]
2.69 (0.10, 40.49)
0.92 (0.20, 4.25)
3.89 (0.18, 83.93
11.22 (0.59, 214.08)
0.24 (0.01, 6.69)
1.81 (0.70, 4.72)
0.01 0 10 1000
IV treatment Early switch
0.1 100
Athanassa Z et al. Drugs 2008; 68: 2469-2481
Recurrent Infection
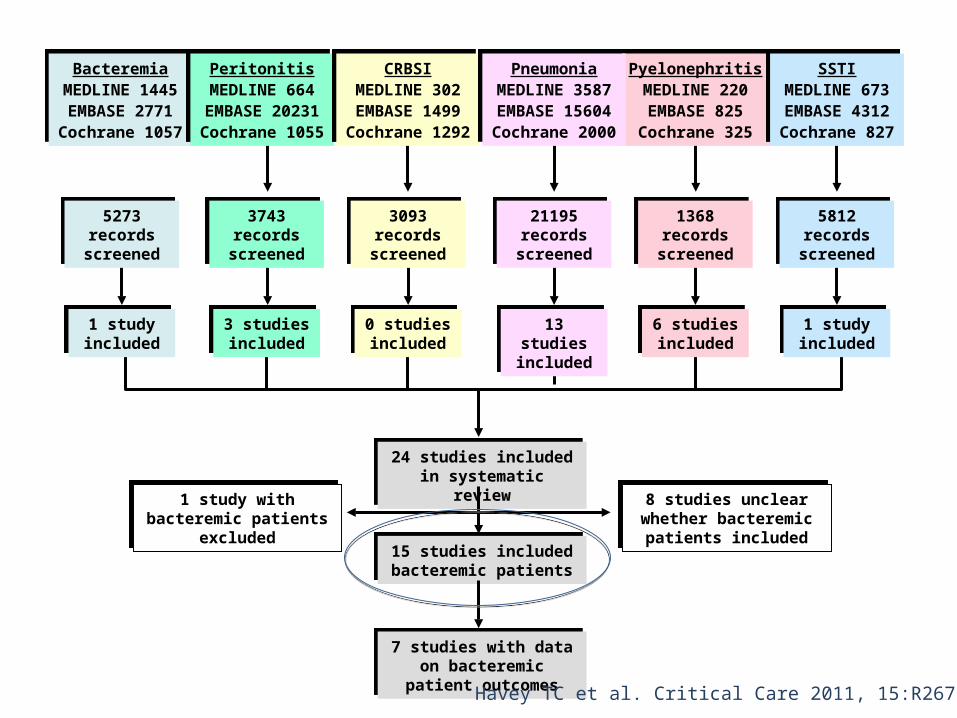
24 studies included in systematic review
24 studies included in systematic review
1 study with bacteremic patients excluded
1 study with bacteremic patients excluded
8 studies unclear whether bacteremic patients included
8 studies unclear whether bacteremic patients included
15 studies included bacteremic patients15 studies included bacteremic patients
7 studies with data on bacteremic patient outcomes
7 studies with data on bacteremic patient outcomes
BacteremiaMEDLINE 1445EMBASE 2771Cochrane 1057
BacteremiaMEDLINE 1445EMBASE 2771Cochrane 1057
PeritonitisMEDLINE 664
EMBASE 20231Cochrane 1055
PeritonitisMEDLINE 664
EMBASE 20231Cochrane 1055
CRBSIMEDLINE 302EMBASE 1499Cochrane 1292
CRBSIMEDLINE 302EMBASE 1499Cochrane 1292
PyelonephritisMEDLINE 220EMBASE 825Cochrane 325
PyelonephritisMEDLINE 220EMBASE 825Cochrane 325
PneumoniaMEDLINE 3587EMBASE 15604Cochrane 2000
PneumoniaMEDLINE 3587EMBASE 15604Cochrane 2000
SSTIMEDLINE 673EMBASE 4312Cochrane 827
SSTIMEDLINE 673EMBASE 4312Cochrane 827
21195 records screened
21195 records screened
3743 records screened
3743 records screened
3093 records screened
3093 records screened
5273 records screened
5273 records screened
1368 records screened
1368 records screened
5812 records screened
5812 records screened
1 study included
1 study included
3 studies included3 studies included
0 studies included0 studies included
13 studies included13 studies included
6 studies included6 studies included
1 study included
1 study included
Havey TC et al. Critical Care 2011, 15:R267
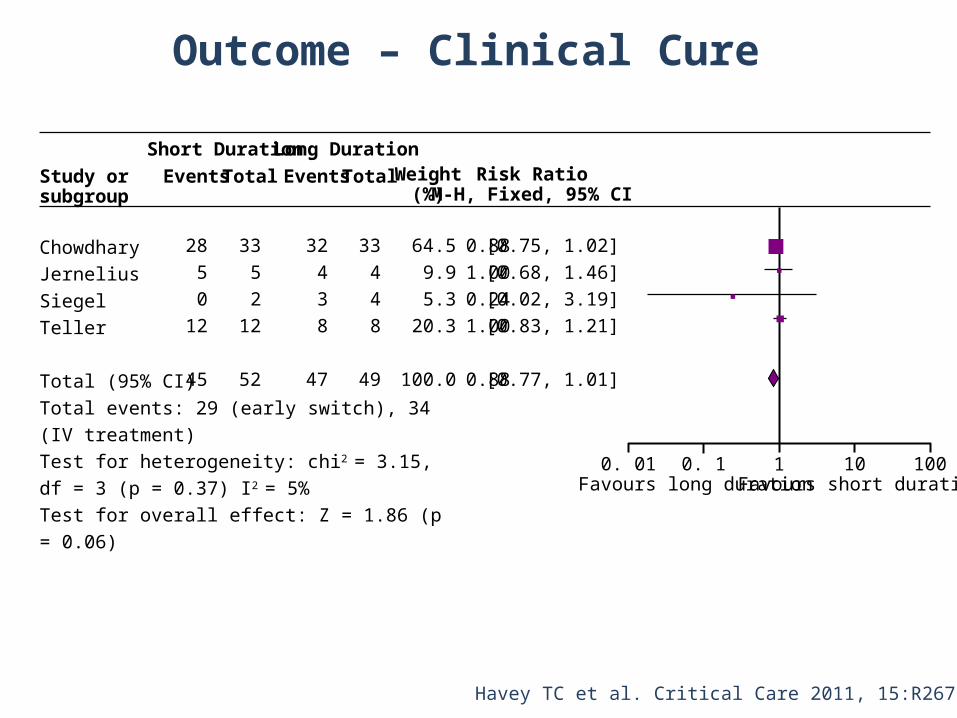
ChowdharyJerneliusSiegelTeller
Total (95% CI)Total events: 29 (early switch), 34 (IV treatment)Test for heterogeneity: chi2 = 3.15, df = 3 (p = 0.37) I2 = 5%Test for overall effect: Z = 1.86 (p = 0.06)
2850
12
45
Study or subgroup
Events
Short Duration
Total
3352
12
52
32438
47
Events
Long Duration
Total
33448
49
Weight(%)
64.59.95.3
20.3
100.0
Risk RatioM-H, Fixed, 95% CI
0.881.000.241.00
0.88
[0.75, 1.02][0.68, 1.46][0.02, 3.19][0.83, 1.21]
[0.77, 1.01]
0. 1 10 100Favours long duration Favours short duration
10. 01
Havey TC et al. Critical Care 2011, 15:R267
Outcome – Clinical Cure
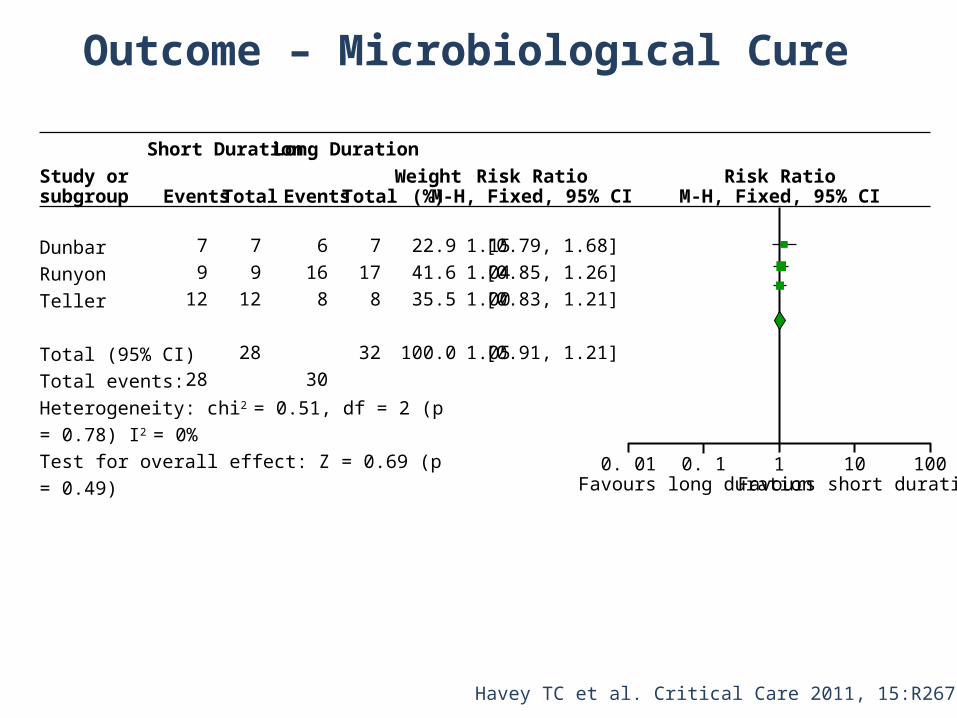
DunbarRunyonTeller
Total (95% CI)Total events:Heterogeneity: chi2 = 0.51, df = 2 (p = 0.78) I2 = 0%Test for overall effect: Z = 0.69 (p = 0.49)
79
12
28
Study or subgroup Events
Short Duration
Total
79
12
28
6168
30
Events
Long Duration
Total
7178
32
Weight(%)
22.941.635.5
100.0
Risk RatioM-H, Fixed, 95% CI
1.151.041.00
1.05
[0.79, 1.68][0.85, 1.26][0.83, 1.21]
[0.91, 1.21]
0. 1 10 100Favours long duration Favours short duration
10. 01
Risk RatioM-H, Fixed, 95% CI
Havey TC et al. Critical Care 2011, 15:R267
Outcome – Microbiologıcal Cure
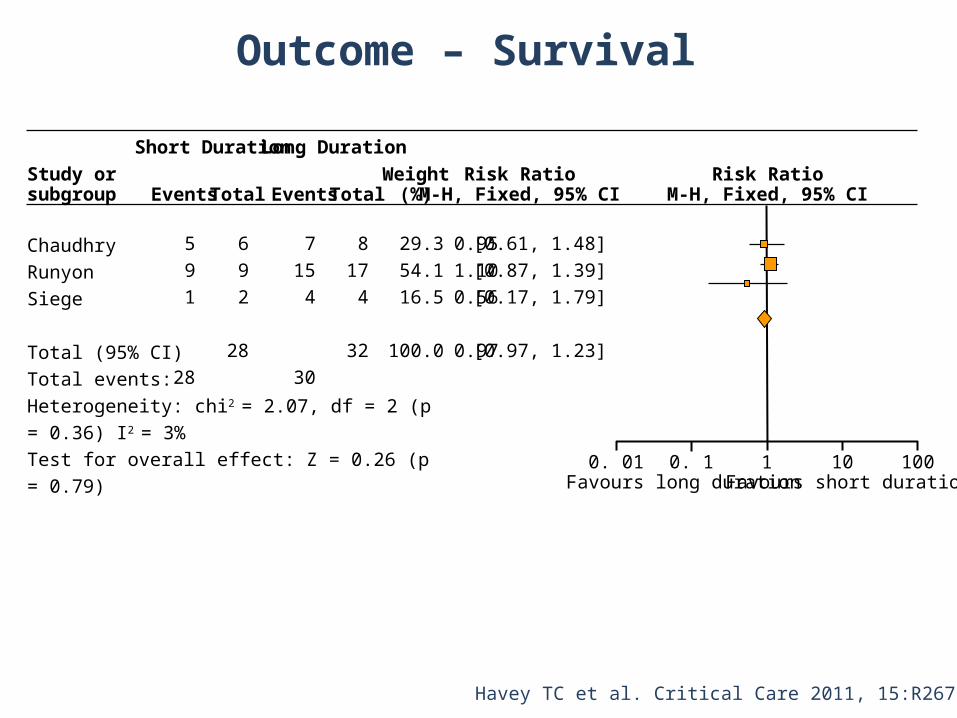
ChaudhryRunyonSiege
Total (95% CI)Total events:Heterogeneity: chi2 = 2.07, df = 2 (p = 0.36) I2 = 3%Test for overall effect: Z = 0.26 (p = 0.79)
591
28
Study or subgroup Events
Short Duration
Total
692
28
7154
30
Events
Long Duration
Total
8174
32
Weight(%)
29.354.116.5
100.0
Risk RatioM-H, Fixed, 95% CI
0.951.100.56
0.97
[0.61, 1.48][0.87, 1.39][0.17, 1.79]
[0.97, 1.23]
0. 1 10 100Favours long duration Favours short duration
10. 01
Risk RatioM-H, Fixed, 95% CI
Havey TC et al. Critical Care 2011, 15:R267
Outcome – Survival
Bacterial etiology very unlikely
Bacterial etiology very unlikely
Bacterial etiology unlikely
Bacterial etiology unlikely
Bacterial etiology likely
Bacterial etiology likely
Bacterial etiology very likely
Bacterial etiology very likely
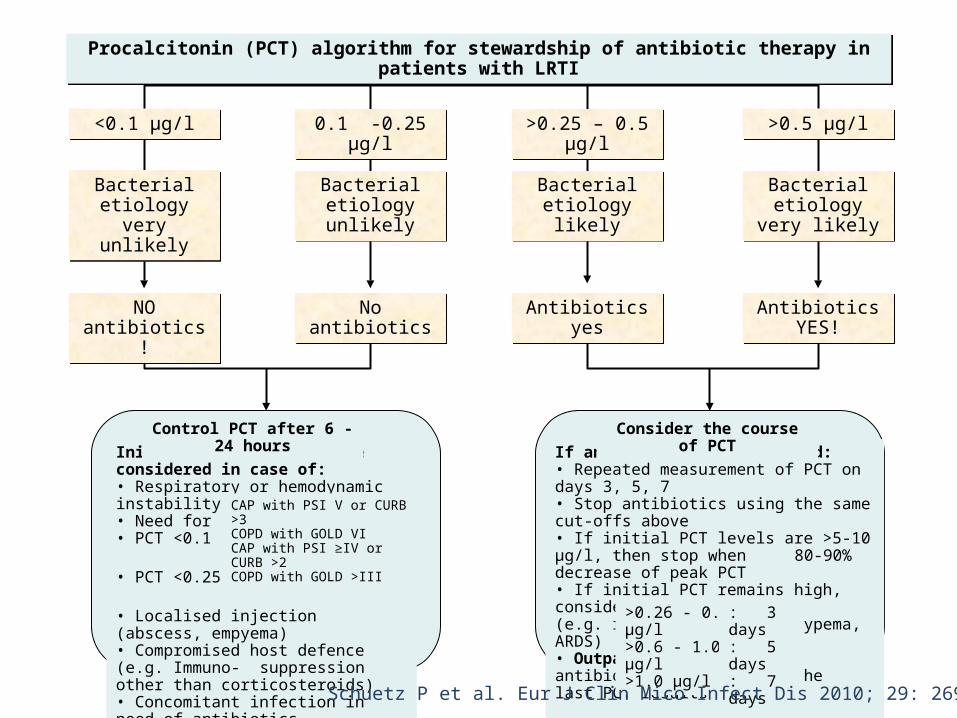
Initial antibiotics can be considered in case of:• Respiratory or hemodynamic instability• Need for ICU admission• PCT <0.1 µg/l
• PCT <0.25 µg/l
• Localised injection (abscess, empyema)• Compromised host defence (e.g. Immuno-suppression other than corticosteroids)• Concomitant infection in need of antibiotics
CAP with PSI V or CURB >3COPD with GOLD VICAP with PSI ≥IV or CURB >2COPD with GOLD >III
Control PCT after 6 - 24 hours
If antibiotics are initiated:• Repeated measurement of PCT on days 3, 5, 7• Stop antibiotics using the same cut-offs above • If initial PCT levels are >5-10 µg/l, then stop when
80-90% decrease of peak PCT• If initial PCT remains high, consider treatment failure
(e.g. resistant strain, emypema, ARDS)• Outpatients: duration of antibiotics according to the
last PCT results>0.26 - 0.6 µg/l>0.6 - 1.0 µg/l>1.0 µg/l
Consider the course of PCT
: 3 days: 5 days: 7 days
Procalcitonin (PCT) algorithm for stewardship of antibiotic therapy in patients with LRTIProcalcitonin (PCT) algorithm for stewardship of antibiotic therapy in patients with LRTI
<0.1 µg/l<0.1 µg/l 0.1 -0.25 µg/l0.1 -0.25 µg/l >0.25 – 0.5 µg/l>0.25 – 0.5 µg/l >0.5 µg/l>0.5 µg/l
NO antibiotics!NO antibiotics! No antibioticsNo antibiotics Antibiotics yesAntibiotics yes Antibiotics YES!Antibiotics YES!
Schuetz P et al. Eur J Clin Mico Infect Dis 2010; 29: 269-277
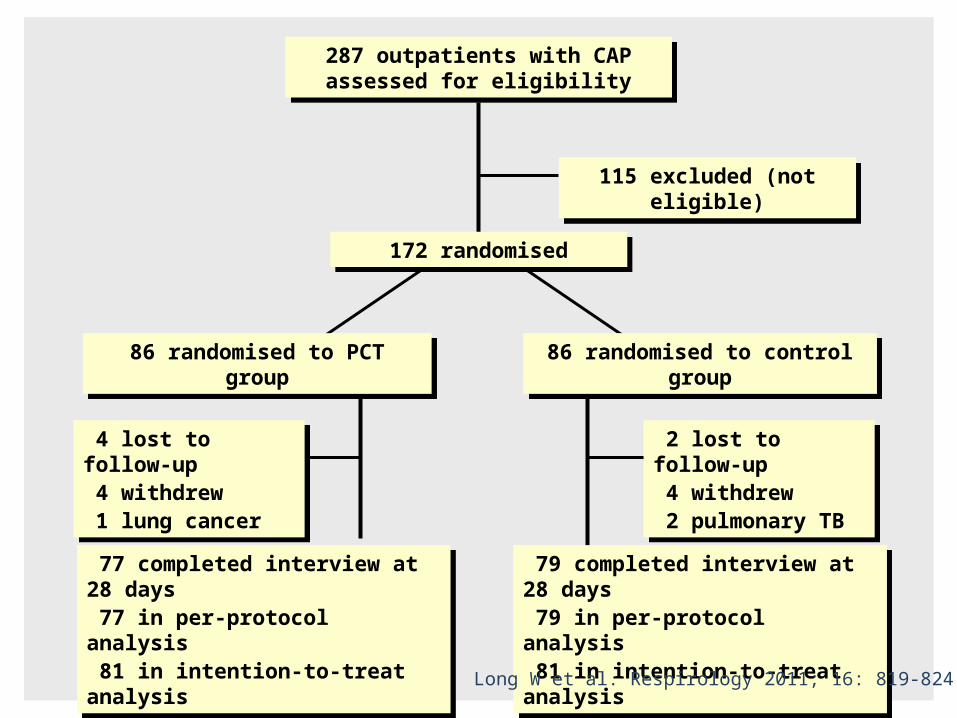
287 outpatients with CAP assessed for eligibility
287 outpatients with CAP assessed for eligibility
115 excluded (not eligible)115 excluded (not eligible)
172 randomised172 randomised
86 randomised to PCT group86 randomised to PCT group 86 randomised to control group86 randomised to control group
4 lost to follow-up 4 withdrew 1 lung cancer
4 lost to follow-up 4 withdrew 1 lung cancer
2 lost to follow-up 4 withdrew 2 pulmonary TB
2 lost to follow-up 4 withdrew 2 pulmonary TB
77 completed interview at 28 days 77 in per-protocol analysis 81 in intention-to-treat analysis
77 completed interview at 28 days 77 in per-protocol analysis 81 in intention-to-treat analysis
79 completed interview at 28 days 79 in per-protocol analysis 81 in intention-to-treat analysis
79 completed interview at 28 days 79 in per-protocol analysis 81 in intention-to-treat analysis
Long W et al. Respirology 2011; 16: 819-824
Patients with CAP should be treated for a minimum of 5 days, should be afebrile for 48 – 72h and should have no more than one CAP-associated sign of clinical instability
Longer duration for certain infections such as S. aureus pneumonia because of risk of endocarditis and deep-seated infections, Pseudomonas aeruginosa infections and atypical pathogens
Common Recommendations
Siegel RE et al. Am J Therapeutics 1999; 6: 217-222
It is reasonable to treat patients with CAP for 5-7 days, if the patient has been afebrile for > 48 hours, has no more than one of CAP-associated signs of clinical instability, and complications of CAP are absent
Concluding Comments
Lim WS et al – BTS Guideline. Thorax 2009Mandell LA et al – IDSA/ATS Guideline. Clin Infect Dis 2007
Hoffken G et al. Pneumologie 2010









![[Medstudy] MedStudy Internal Medicine Pulmonology,(BookFi.org)](https://img.pdfslide.us/doc/110x75/577cc6c01a28aba7119f0e58/medstudy-medstudy-internal-medicine-pulmonologybookfiorg.jpg)