Embed Size (px)
Citation preview

JOURNAL OF VIROLOGY, June 2008, p. 5548–5561 Vol. 82, No. 110022-538X/08/$08.00�0 doi:10.1128/JVI.00124-08Copyright © 2008, American Society for Microbiology. All Rights Reserved.
Characterization of the Follicular Dendritic Cell Reservoir of HumanImmunodeficiency Virus Type 1�†
Brandon F. Keele,1‡ Loubna Tazi,2 Suzanne Gartner,3 Yiling Liu,3 Trever B. Burgon,1§Jacob D. Estes,1¶ Tyler C. Thacker,1� Keith A. Crandall,2
Justin C. McArthur,3 and Gregory F. Burton1*Department of Chemistry and Biochemistry1 and Department of Biology,2 Brigham Young University, Provo, Utah 84602, and
Department of Neurology, Johns Hopkins University, Baltimore, Maryland 212873
Received 17 January 2008/Accepted 24 March 2008
Throughout the natural course of human immunodeficiency virus (HIV) infection, follicular dendritic cells(FDCs) trap and retain large quantities of particle-associated HIV RNA in the follicles of secondary lymphoidtissue. We have previously found that murine FDCs in vivo could maintain trapped virus particles in aninfectious state for at least 9 months. Here we sought to determine whether human FDCs serve as an HIVreservoir, based on the criteria that virus therein must be replication competent, genetically diverse, andarchival in nature. We tested our hypothesis using postmortem cells and tissues obtained from three HIV-infected subjects and antemortem blood samples obtained from one of these subjects. Replication competencewas determined using coculture, while genetic diversity and the archival nature of virus were established usingphylogenetic and population genetics methods. We found that FDC-trapped virus was replication competentand demonstrated greater genetic diversity than that of virus found in most other tissues and cells. Antiret-rovirus-resistant variants that were not present elsewhere were also detected on FDCs. Furthermore, geneticsimilarity was observed between FDC-trapped HIV and viral species recovered from peripheral blood mono-nuclear cells obtained 21 and 22 months antemortem, but was not present in samples obtained 4 and 18 monthsprior to the patient’s death, indicating that FDCs can archive HIV. These data indicate that FDCs representa significant reservoir of infectious and diverse HIV, thereby providing a mechanism for viral persistence formonths to years.
A major obstacle in the treatment of human immunodefi-ciency virus (HIV) disease is the establishment of viral reser-voirs that provide a continuing source of infectious virus (3, 6,14, 25, 39, 40, 49). HIV reservoirs not only maintain viralinfectivity but also harbor drug-resistant and immune-escapequasispecies that may contribute to ongoing viral evolutionunder drug- or immune-selective pressures. Much attentionhas been focused on the latently infected CD4� T-cell reser-voir (7, 15, 62) and, to a lesser extent, the macrophage reser-voir (9, 32, 51); however, little information exists regardingfollicular dendritic cells (FDCs) as an HIV reservoir (16, 29).
HIV reservoirs have been characterized as cells or tissuesthat restrict virus replication and preserve replication-compe-tent HIV for long periods of time (35). Reservoirs will containinfectious virus, having a greater stability (i.e., a longer half-
life) than virus in cells where active viral expression is ongoing(3). Because of this stability, virus accumulates over time, thuscreating an “archive” possessing higher overall genetic diver-sity than that of the non-reservoir-associated virus (5, 34, 35).Because viral reservoirs present major obstacles to the successof antiretroviral (ARV) therapy, we sought to characterize theFDC HIV reservoir.
FDCs are localized in the follicles of all secondary lymphoidtissues, where they help establish and maintain potent, long-term immunoglobulin G (IgG) and IgE humoral immunity (22,26, 31). FDCs trap and retain antigens on the surfaces of theirdendritic processes, including intact HIV virions. Thesetrapped antigens and virus particles exist in the form of im-mune complexes (4, 24, 52). FDC-trapped antigens and virusparticles have a half-life of approximately 2 months and aremaintained in their native nondegraded state (52, 59). BecauseHIV is held on the surface of the FDC, it does not activelyreplicate or further evolve, despite retaining the ability to in-fect nearby trafficking cells (52). Importantly, although FDCsthemselves remain uninfected, they reside immediately adja-cent to activated T and B cells in the germinal center and thelong dendritic processes of FDCs interact directly with theseadjacent lymphocytes.
During primary HIV infection, massive quantities of virusare trapped on FDCs (1, 2, 45, 58). In fact, FDCs likely rep-resent the largest repository of HIV, with a viral burden esti-mated to contain 1.5 � 108 copies of viral RNA per gram oflymphoid tissue (19, 20). FDC-associated virus remainsthroughout the course of disease until the ultimate demise of
* Corresponding author. Mailing address: Rm. C211A BNSN, De-partment of Chemistry and Biochemistry, Brigham Young University,Provo, UT 84602. Phone: (801) 422-4917. Fax: (801) 422-0153. E-mail:[email protected].
† Supplemental material for this article may be found at http://jvi.asm.org/.
‡ Present address: Department of Medicine, University of Alabamaat Birmingham, Birmingham, AL 35294-0024.
§ Present address: Department Microbiology and Immunology,Stanford University, Stanford, CA 94305.
¶ Present address: AIDS Vaccine Program, NCI-Frederick, FortDetrick Campus, Frederick, MD 21702.
� Present address: Tuberculosis Research Unit, USDA AgriculturalResearch Service, Ames, IA 50201.
� Published ahead of print on 2 April 2008.
5548
at BR
IGH
AM
YO
UN
G U
NIV
on February 5, 2009
jvi.asm.org
Dow
nloaded from

the FDCs. Furthermore, throughout the natural course of in-fection, active viral replication in T cells can be observed sur-rounding germinal centers where the FDC resides. In a non-permissive murine model, FDC-trapped virus possessed an invivo half-life of 8 weeks and infectious virus could be rescuedfrom FDCs for at least 9 months after a single injection of virus(52). Importantly, the maintenance of infectivity of FDC-trapped HIV did not require either infection of the FDC orreplication of the virus. Studies using human FDCs in vitroindicate that HIV is preserved in a replication-competent statefor about 1 month (52, 53). In contrast to the case for otherdendritic cells, FDCs do not express CD209 (dendritic cell-specific, ICAM-3-grabbing nonintegrin [DC-SIGN]) for themaintenance of infectivity and trapped virus particles are notinternalized (36). FDC maintenance of viral infectivity re-quires Fc and/or complement receptors on the FDC and thepresence of a specific antibody that reacts with the virion (24,53, 54).
Although FDCs have been suggested as a possible HIVreservoir because of their ability to retain virus in a replication-competent form for many months in a murine model (52),direct testing of FDCs isolated from infected human subjectshas not been performed. Here we tested the hypothesis thatFDCs are a reservoir of HIV in humans. We found that FDC-trapped virus was replication competent and possessed greatergenetic diversity than that of virus found in most other cellsand tissues tested, suggesting the accumulation of genetic vari-ants over time. Consistent with the archival nature of virusreservoirs, HIV on FDCs had genotypes similar to those ofviral variants detected from peripheral blood mononuclearcells (PBMCs) obtained at 21 and 22 months, but not 4 and18 months, prior to the patient’s death. Thus, we report herethat FDCs do indeed fulfill the criteria of an HIV reservoirin humans and have the ability to contribute to persistingdisease. A greater understanding of the nature of the FDCreservoir should provide the foundation needed to devisemore successful strategies to target this important source ofinfectious HIV.
MATERIALS AND METHODS
Patient population. Lymph nodes (LN) and spleen sections were obtained atautopsy from three HIV-infected subjects (JHU559, -614, and -621) at JohnsHopkins Hospital, Baltimore, MD (Table 1). The LN (and in one instance, i.e.,
for subject JHU614, splenic fragments) from each patient were collected andused for the isolation and culture of specific cell types. In some instances (i.e., forsubjects JHU559 and -614) mid-frontal gyrus, deep white matter, meninges, andbone marrow (for subject JHU614 only) were also obtained for direct viral DNAisolation. This research has complied with all relevant federal guidelines andinstitutional policies.
FDC and CD4� T-cell isolation from secondary lymphoid tissues. FDC andCD4� T-cell populations were isolated from LN or splenic fragments. Briefly,tissue was cut into small cubes (�2 mm3) and digested in RPMI 1640 (Hy-Clone, Logan, UT) containing DNase I (150 IU; Sigma, St. Louis, MO),collagenase D (20 mg; Roche Applied Science, Indianapolis, IN), and gen-tamicin (50 �g/ml; Invitrogen, Carlsbad, CA). Tissues were then incubated at37°C for 45 min, with periodic mixing. The freed cells were removed andtransferred to medium supplemented with antibiotics and heat-inactivatedfetal bovine serum (FBS) (33%, vol/vol) (HyClone, Logan, UT). The remain-ing undigested tissue sections were again incubated in fresh medium contain-ing the above enzyme cocktail, and newly released cells were collected asbefore. After the second digestion, any remaining tissue was gently passed inand out of a sterile pipette to further disassociate any remaining cells. Allcollected cells were pooled, washed in fresh medium to remove enzymes, andresuspended in fresh medium.
FDCs were isolated using positive selection. Cells were incubated on ice (withgentle agitation) with the primary antibody HJ2 (mouse IgM monoclonal anti-body that binds human FDCs [kindly provided by Moon Nahm, University ofAlabama at Birmingham]), after which they were washed in fresh medium andlabeled for 30 min with a secondary antibody (rat anti-mouse IgM) conjugated tomagnetic beads (Dynabeads; Invitrogen, Carlsbad, CA). Cells were isolated bymagnet separation and washed thoroughly to remove residual contaminatingcells. In some instances, FDCs were isolated via fluorescence-activated cellsorting using a FACSVantage SE system with FACSDiva software (BD Bio-sciences, San Jose, CA) with HJ2 as the primary antibody, followed by a goatF(ab�)2 anti-murine IgM-fluorescein isothiocyanate-labeled secondary antibody(Jackson ImmunoResearch Laboratories, West Grove, PA). In all cases, thepreparations of FDCs were subjected to 3,000 rad of � irradiation before use toblock the proliferation of any possible contaminating lymphocytes that couldotherwise be activated to support viral replication. Even though we failed todetect the presence of HIV DNA in our irradiated FDC preparations, thepossibility that a rare contaminating HIV-infected T cell was present cannot beunambiguously ruled out. The lymphoid tissue cells remaining after FDC en-richment were subjected to the depletion of B cells, macrophages, NK cells, andCD8� T cells, followed by collection of the remaining CD4� T cells by usingnegative selection (Miltenyi Biotec, Auburn, CA). The isolated CD4� T cellswere not mitogen activated or otherwise stimulated before use. Our enrichmentprocedures typically yielded cell purities of 75 to 95%. To ensure that FDC-trapped HIV was replication competent, whenever insufficient tissue was avail-able for both coculture and direct virus sequencing (i.e., in the cases of theJHU559 and JHU621 samples), we prioritized the use of isolated FDCs forcoculture and virus rescue. In the case of subject JHU614, we obtained sufficienttissue to isolate FDCs for both virus rescue coculture and direct virus sequencingwithout culture.
CD4� T-cell isolation from the peripheral blood of an HIV-infected sub-ject. Antemortem peripheral blood samples were collected from HIV-in-fected subject JHU614. These cells were subjected to density gradient sepa-ration using Ficoll-Paque Plus (GE Healthcare, Piscataway, NJ) according tothe manufacturer’s directions. The cells were then subjected to DNA lysis asdescribed below.
CD4� T-cell isolation from the peripheral blood of healthy donors. CD4� Tcells were obtained from healthy donors after informed consent. These cells weresubjected to density gradient separation as described above, after which theywere depleted of macrophages, NK cells, B lymphocytes, and CD8 T cells and theremaining CD4� T cells were collected using a CD4 negative selection kit asdescribed above. These cells were activated for 3 days using phytohemagglutinin(5 �g/ml), after which the cells were washed to remove the mitogen and thenresuspended and maintained throughout culture in complete RPMI (containingRPMI, interleukin-2 [20 U/ml; Roche Applied Science, Indianapolis, IN], 20%fetal bovine serum, gentamicin [50 �g/ml], nonessential amino acids, HEPES [10ml/500 ml RPMI], and glutamine).
Detection of infectious HIV from FDCs and CD4� T cells from HIV-positive(HIV�) subjects. Rescue bioassays were performed to determine the infectiousnature of virus on FDCs or in CD4� T cells from HIV� subject JHU559.Immunoselected FDCs or identical numbers of CD4� T cells were obtained fromthe same LN collected at autopsy. These cells were cultured without in vitroactivation with allogeneic, mitogen-activated CD4� T cells obtained from the
TABLE 1. HIV-infected subjects involved in this study
Patient ARVa CD4countb
PBMC sampleobtained FDC sequence type
JHU559 Yesc 2 No ccd onlyJHU614 Yese 246 Yesf cc and unculturedJHU621 No 3 No cc only
a Indicates whether ARV therapy was received.b Data are expressed per mm2 and were the most recent available. Samples
were obtained 4 months, 18.5 months, and 2 weeks prior to death for subjectsJHU559, JHU614, and JHU621, respectively.
c Subject received undefined ARV treatment that was discontinued approxi-mately 2 months prior to death.
d cc, coculture.e Subject began treatment with azidothymidine, lamivudine, and efavirenz
approximately 2 years before death. Treatment was discontinued 13 months priorto death, reinstated 2 months later, and finally stopped 7 months before death.
f PBMCs were obtained 4, 18, 21, and 22 months prior to death.
VOL. 82, 2008 FDC RESERVOIR OF HIV 5549
at BR
IGH
AM
YO
UN
G U
NIV
on February 5, 2009
jvi.asm.org
Dow
nloaded from

peripheral blood of a healthy donor. The cocultures were maintained for 18 days,during which culture fluid was removed and the production of p24 was measuredusing an antigen capture enzyme-linked immunosorbent assay (BeckmanCoulter, Fullerton, CA) to detect productive infection. The cells from thesecocultures were also harvested, and their DNA was isolated and subjected tonested PCR amplification as described below. Furthermore, immunoselectedFDCs and CD4� T cells (both isolated from the same LN or piece of splenictissue) were obtained from HIV� subjects JHU621 and JHU614 and coculturedfor at least 6 days in the same manner as that described above, after which thecellular DNA was also isolated and subjected to nested PCR amplification. TheHIV amplicons obtained from these cells were subjected to DNA sequencing andphylogenetic analysis as described below.
Proviral DNA and viral RNA isolation. Cells were lysed using 50 �l DNA lysisbuffer (0.01% sodium dodecyl sulfate, 0.001% Triton X-100, 0.42 �g/ml protein-ase K in TE [10 mM Tris and 1 mM EDTA]). Cell lysis and protein digestionwere performed at 56°C overnight, after which the DNA was aliquoted andstored at �80°C. RNA was isolated by adding 160 �l of chloroform-800 �l RNASTAT-60 (Tel-Test, Inc., Friendswood, TX) and the solution was vortexed andthen centrifuged at 13,000 � g for 15 min at 4°C. Equal volumes of the aqueousphase from each sample were transferred to a fresh tube containing an equalvolume of isopropanol. This tube was vortexed and incubated at �20°C for 30min and then centrifuged at 4°C for 30 min at 13,000 � g. The RNA pellet waswashed once in 75% ethanol (1.0 ml), air dried, and resuspended in an equalvolume of RNase-free water. Pretreatment of RNA with DNase I (Invitrogen,Carlsbad, CA) was performed to exclude DNA contamination. Equal volumes ofRNA were then reverse transcribed using the GeneAmp RNA PCR kit (AppliedBiosystems, Foster City, CA) according to the manufacturer’s instructions. Equalvolumes of cDNA were PCR amplified under the same conditions as those usedfor the isolated DNA.
PCR amplification of HIV env and pol genes. Using nested-set PCR technol-ogy, we examined the entire env gene and/or a portion of the pol genecontaining all of the protease (Pro) and the first 248 amino acids of thereverse transcriptase (RT) genes. Genomic DNA or cDNA was used atempirically determined optimal concentrations for the first round of PCRamplification. Multiple first-round amplifications (three or more) werepooled to guard against selection bias. For the second-round PCR, 1 or 2 �lof the pooled first-round reaction mixture was added as the template. Allreactions were performed in 50-�l volumes and included 50 �M deoxynucleo-side triphosphates, 0.40 �M of each primer, 3 mM MgCl2, PCR buffer II, and2.5 U Expand HiFi Long-Taq polymerase (Roche Applied Science, Indianap-olis, IN), having an error rate of 6.1 � 10�6. The PCR cycling conditions forboth rounds of amplification consisted of an initial denaturation at 94°C for2 min, followed by 10 cycles of 94°C for 11 s, 55°C for 31 s, and 68°C for 4 min.This denaturation was followed by an additional 24 cycles, with 20 s added tothe extension of each cycle, followed by a final extension at 72°C for 12 min.All PCRs were performed with precautionary procedures to safeguard againstcontamination. All reagents were aliquoted in a DNA-free hood, and allamplicons were physically separated from nonamplified DNA. Replicate con-trol PCRs were performed without template to demonstrate no carryovercontamination. The outer primers for the complete env gene were 160out3(5�-GTTCTGCCAATCAGGGAAGTAGCCTTGTGTGTGG-3�) and 160out5 (5�-CCTATGGCAGGAAGAAGCGGAGACAGCGACGAA-3�) and the inner prim-ers were nJL69 (5�-TAATAGAAAGAGCAGAAGACAGT-3�) and JL71 (5�-TTTTGACCACTTGCCACCCAT-3�), which produced an approximately 2.6-kbamplicon (HXB2, nucleotides 6225 to 8795) (30). For the examination of HIVprotease-RT sequences, an approximately 1-kb fragment (HXB2, nucleotides2253 to 3278) was PCR amplified. The outer primers were Polout5 (5�-CAGAGCCAACAGCCCCACAAGAG-3�) and Polout3 (5�-TTGCCCAATTCAATTTTCCCACTAACTT-3�). The inner primers were Polin5 (5�-CCTCTCAGAAGCAGGAGCCGATAGA-3�) and Polin3 (5�-TCAATTTTCCCACTAACTTCTGTATGTCATT-3�).
Cloning and sequencing HIV genes. PCR-amplified products were T/A clonedinto the vector pCR3.1 (Invitrogen, Carlsbad, CA) by directly ligating the vectorwith fresh PCR product at 15°C overnight. STBL2 bacteria (Invitrogen, Carls-bad, CA) were then transformed via heat shock (25 s at 42°C) and plated on LBplates with 100 �g/ml ampicillin. Individual colonies were selected and screenedfor correctly sized inserts via a modified toothpick boiling method. Briefly,bacteria were incubated in a 96-well, V-bottom plate at 30°C overnight. Cellswere then centrifuged and lysed, and genomic DNA and proteins were precip-itated and removed by centrifugation. The plasmid DNA in the supernatant wasthen subjected to electrophoresis, and plasmids with inserts were identified byrelative size. Insert-positive clones were then cultured in 5 ml LB broth at 30°C,with shaking at 225 rpm. Clean, sequence-ready, plasmid DNA was purified using
the QIAprep spin column (Qiagen, Valencia, CA). Clones for each gene wererandomly selected and sequenced using the BigDye (version 3.1) terminatormethod (Applied Biosystems, Foster City, CA), with a battery of previouslydeveloped primers. After the sequencing reaction, the samples were purifiedusing the DyeEx terminator removal kit (Qiagen, Valencia, CA). Sequences werethen analyzed on an ABI-3730XL DNA analyzer at Brigham Young University’score facility. Both strands of each viral insert were sequenced, with all geneshaving at least two overlapping independent sequences per site. All contigs weretrimmed, and a consensus sequence was made with Sequencher (Gene Codes,Ann Arbor, MI).
Phylogenetic analysis of HIV from FDCs and other cells/sites. We alignedsequences by using the default settings in ClustalX 1.81 (61). The sequences werethen manually adjusted and checked for insertions and deletions (indels) topreserve codon structure using MacClade 4 (Sinauer Associates, Sunderland,MA). Phylogenies were estimated using maximum likelihood (13), with nodalsupport assessed via bootstrapping (1,000 pseudoreplicates) (12) as implementedin PHYML (18). We also estimated phylogenies by using Bayesian methods (23)coupled with the Markov Chain Monte Carlo inference as implemented inMrBayes, version 3.1.2 (48). Model selection for these analyses followed theprocedure outlined previously by Posada and Buckley (41), as implemented inModelTest, version 3.6 (43). For the techniques using Bayesian methods (23)coupled with the Markov chain Monte Carlo method, two independent analyseswere run, with each consisting of four chains. Each Markov chain started from arandom tree and ran for 2.0 � 107 cycles, with sampling every 1,000th generation.In order to confirm that our Bayesian analyses converged and mixed well, wemonitored the fluctuating value of likelihood and compared means and variancesof all likelihood parameters and likelihood scores from the independent runsusing the program Tracer, version 1.4 (http://beast.bio.ed.ac.uk/tracer). Thesephylogenetic analyses were performed on the supercomputing cluster of theCollege of Life Sciences at Brigham Young University.
The genetic diversity of FDC-trapped HIV and virus obtained from othertissues and cells was determined using a phylogenetic approach to estimatenucleotide diversity implemented in LAMARC, version 2.0.2 (27). This programprovided a maximum likelihood estimate of theta (� 2Ne�), where Ne is theinbreeding effective population size and � is the per site mutation rate.
Genotype network reconstruction and genetic diversity estimates. To compareFDC and PBMC RT genetic sequences in subject JHU614 within a 95% parsi-mony limit, a haplotype network was constructed using the program TCS, version1.21 (8). The networks are constructed so that colored squares (putative out-groups) and circles represent actual cloned sequences, the sizes of which areproportional to the number of clones with the same sequence. Each open circlerepresents a putative quasispecies in the evolutionary pathway. Solid lines con-necting a network suggest that two quasispecies can be connected with at least a
TABLE 2. FDC-trapped HIV is replication competenta
HIV�
subject
FDCculture
condition
Amt (pg/ml) of p24 fromcocultureb HIV pol or env
amplified fromcoculturesc
Day 9 Day 12 Day 18
JHU559 Alone ND ND 62 NDWith allo T 59,000 48,000 65,000 �
JHU614 With allo T ND ND ND �JHU621 With allo T ND ND ND �
a FDCs or CD4� T cells were immunoselected from a single LN obtained fromsubjects JHU559, JHU614, and JHU621. To inhibit the potential for any con-taminating T cells to support virus replication, the FDCs were subjected to 3,000rad � irradiation prior to the inception of culture. Cocultures were performedusing the immunoselected cells without activation and mitogen-stimulated, allo-geneic CD4� T (allo T) cells from an uninfected, normal blood donor. At thespecified time interval or at the end of the coculture, DNA was obtained from thetarget cells and HIV pol or env genes were amplified using nested PCR. ND, notdetermined.
b A total of 2 � 104 irradiated FDCs and 2 � 105 activated, allogeneicperipheral blood lymphocytes were cultured together for the indicated numberof days, after which the amount of p24 per milliliter culture fluid was determinedusing antigen capture enzyme-linked immunosorbent assay. Input virus presentin the FDC preparations was determined by culturing the irradiated cells aloneand measuring the amount of p24 present at the end of culture.
c At the end of culture, DNA was obtained and subjected to PCR amplifica-tion, cloning, and sequencing. PCR amplification of DNA from the FDCs of allsubjects was negative, indicating that these cells are not themselves infected.
5550 KEELE ET AL. J. VIROL.
at BR
IGH
AM
YO
UN
G U
NIV
on February 5, 2009
jvi.asm.org
Dow
nloaded from

95% degree of confidence. Broken lines in a network represent a more tenuousconnection.
Analyses of sequence data for recombination. It is well known that HIV-1undergoes recombination (46, 47, 57) and that this can potentially impact estimatesof both population genetic parameters (50) and phylogeny estimation (44). Theimpact of recombination on phylogeny estimation seems to be more severe when the
recombination event involves roughly equal divisions across the gene (44). Other-wise, the tree estimated is the history of the majority of the gene sequence after therecombination event. To test the robustness of our phylogenetic conclusions torecombination, we used a network approach (TCS) that allows for recombination(42) and has an associated test for it (10). While there is no doubt that recombinationis occurring, there are no identifiable recombinants in these data by using this
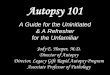
FIG. 1. Phylogenetic analysis of HIV Pro-RT obtained from FDC and CD4 T-cell cocultures from subject JHU559. FDCs and CD4 T cells (2 �104 cells per well) were immunopurified and cocultured with mitogen-activated, allogeneic T-cell blasts. Following 9 days of culture, cells wereharvested, and their DNA was collected. HIV pol was amplified by nested PCR, cloned, and sequenced as described in the text. Phylogeneticanalysis was performed using both maximum likelihood (ML) and Bayesian methods, which generated identical topologies. Statistical analysis isprovided for both analyses and is displayed as bootstrap values in the numerator and posterior probability (by using the Bayesian Markov MonteCarlo method) in the denominator. Statistical support of 50% or greater is shown. Each sequence was identified by the cell type from which theviral gene was cloned, followed by “cc” (to indicate that it was derived from coculture) and the clone designation (e.g., FDC_cc458). Thecorresponding sequence deposited with GenBank is prefaced by the identifier for the infected subject (e.g., JHU559_FDC_cc458). BMCMC,Bayesian methods coupled with the Markov chain Monte Carlo method.
VOL. 82, 2008 FDC RESERVOIR OF HIV 5551
at BR
IGH
AM
YO
UN
G U
NIV
on February 5, 2009
jvi.asm.org
Dow
nloaded from

approach. The sequences were very closely related (there was typically only a singlenucleotide difference among sequence variants), and those few that were moredistantly related were not connected to disparate places in the network (a telltalesign of recombination). Thus, our analyses indicate that recombination does notsignificantly impact our conclusions.
Nucleotide sequence accession numbers. GenBank accession numbers forthe sequences determined in this study are EF440689 to EF441210,EU009131 to EU009140, and EU330488 to EU330524. Each sequence isidentified by using the subject name, the tissue and cell type, and the clonedesignation (e.g., JHU559_CFDC_3D6). When a sequence was derived from
FIG. 2. Phylogenetic analysis of HIV Pro-RT obtained from FDC and CD4 T-cell cocultures using cells obtained from subject JHU621 (asdescribed for Fig. 1). Phylogenetic analysis was performed using both maximum likelihood (ML) and Bayesian methods, which generated identicaltopologies. Statistical analysis is provided for both analyses and is displayed as bootstrap values in the numerator and posterior probability (by usingthe Bayesian Markov Monte Carlo method) in the denominator. Each sequence was identified by the cell type from which the viral gene wascloned, followed by “cc” (to indicate that it was derived from coculture) and the clone designation (e.g., FDC_cc42B). The corresponding sequencedeposited with GenBank is prefaced by the identifier for the infected subject (e.g., JHU621_FDC_cc42B). BMCMC, Bayesian methods coupledwith the Markov chain Monte Carlo method.
5552 KEELE ET AL. J. VIROL.
at BR
IGH
AM
YO
UN
G U
NIV
on February 5, 2009
jvi.asm.org
Dow
nloaded from

a coculture, we added “cc” immediately before the clone identification (e.g.,JHU559_CFDC_cc3D9).
RESULTS
FDCs retain infectious HIV. Because the most essentialaspect of an HIV reservoir is the harboring of infectiousvirus, we first sought to determine whether FDC-trappedvirus was replication competent. We reasoned that if FDC-
trapped HIV was infectious, we could transfer the infectionto susceptible CD4 T cells and detect viral protein produc-tion and/or viral DNA. We therefore immunoselected FDCsfrom a postmortem LN obtained from HIV-infected subjectJHU559 and used these as the only source of input virus ina rescue bioassay (Table 2). The FDCs used in each culturewell (i.e., 10,000 cells) contained 62 pg of HIV p24 permilliliter of cell culture fluid. When this input virus on FDCs
FIG. 3. Phylogenetic analysis of HIV RT obtained from FDC and CD4 T-cell cocultures from subject JHU614 (as described for Fig. 1).Phylogenetic analysis was performed using both maximum likelihood (ML) and Bayesian methods, which generated identical topologies. Statisticalanalysis is provided for both analyses and is displayed as bootstrap values in the numerator and posterior probability (by using the Bayesian MarkovMonte Carlo method) in the denominator. Each sequence was identified by the tissue and cell type from which the viral gene was cloned, followedby “cc” (to indicate that it was derived from coculture), and the clone designation (e.g., CFDC_cc3B8). The corresponding sequence deposited withGenBank is prefaced by the identifier for the infected subject (e.g., JHU614_CFDC_cc3B8). Tissue identifiers are A (axillary LN), C (cervical LN),and S (spleen). BMCMC, Bayesian methods coupled with the Markov chain Monte Carlo method.
VOL. 82, 2008 FDC RESERVOIR OF HIV 5553
at BR
IGH
AM
YO
UN
G U
NIV
on February 5, 2009
jvi.asm.org
Dow
nloaded from

FIG. 4. Phylogenetic analysis of uncultured (bone marrow, brain [meninges and mid-frontal gyrus], and an unfractionated LN) and cocultured(FDCs and T cells) HIV gp160 sequences derived from multiple sites in subject JHU559. Phylogenetic analysis was performed using both maximumlikelihood (ML) and Bayesian methods, which generated identical topologies. Statistical analysis is provided for both analyses and is displayed asbootstrap values in the numerator and posterior probability (by using the Bayesian Markov Monte Carlo method) in the denominator. Eachsequence was identified by the tissue and cell type from which the viral gene was cloned and the clone designation (e.g., BM_C5). Thecorresponding sequence deposited with GenBank is prefaced by the identifier for the infected subject (e.g., JHU559_BM_C5). When FDC and
5554 KEELE ET AL. J. VIROL.
at BR
IGH
AM
YO
UN
G U
NIV
on February 5, 2009
jvi.asm.org
Dow
nloaded from

was cultured with activated allogeneic CD4� T-cell targets,we detected the production of significant quantities of HIVp24 (59,000 and 65,000 pg/ml at 9 and 18 days of culture,respectively). To confirm that FDC-trapped HIV was infec-tious, we performed additional cocultures with FDCs ob-tained postmortem from two additional subjects, JHU614and JHU621 (Table 2). To detect the transmission of infec-tion in these assays, we harvested the target cells from thecocultures and examined them for the presence of HIVDNA (Table 2). While HIV DNA could not be amplifiedfrom FDCs themselves (which bear only HIV RNA), it wasamplified from all of the FDC cocultures, confirming itsinfectious nature.
FDC-trapped HIV is genetically diverse. We first analyzedthe pol gene from virus obtained by coculture of FDCs and Tcells obtained from subjects JHU559 (Fig. 1), JHU621 (Fig. 2),and JHU614 (Fig. 3). In samples from subjects JHU559 andJHU621, FDC HIV and virus from T cells formed distinctclades in the phylogenetic tree, demonstrating the compart-mentalization of virus populations. In the third subject(JHU614), however, virus from the FDCs and T cells wassubstantially more intermixed. We also noted a relationshipbetween viruses in spatially separated secondary lymphoid tis-sues; FDC viruses from the spleen clustered not only withsplenic T cells but also with T-cell-derived viruses from theaxillary LN (i.e., SFDC_cc3F6 and SFDC_cc3H8 were relatedto ST_ccC3C9, ST_ccC3C9b, ST_ccC3E9, A1T_ccC11,A1T_ccB1E5, and A1T_ccT1C3). In all but one of these in-stances (i.e., ST_ccC3E9 was identical to SFDC_cc3F6), theT-cell-derived HIV differed from the FDC virus by a single,nonsynonymous nucleotide change in the RT gene, resulting inthe following amino acid alterations: T128A for ST_ccC3C9and ST_C3C9b, E203G for A1T_ccC11, and E224G forA1T_ccT1C3, where the first amino acid listed at a given po-sition was present in FDCs and the second was present in theT cells. No known drug resistance was associated with thesechanges.
We also assessed the genetic relatedness of gp160 sequencesfrom subject JHU559. In this analysis, we examined both FDCand T-cell viral sequences derived from coculture and directlycloned sequences obtained from uncultured HIV DNA fromthe bone marrow, the brain (the meninges and mid-frontalgyrus), and from a second LN where immunoselection andculture of cells were not performed prior to sequencing (Fig.4). FDC-associated virus formed a monophyletic group (a dis-tinct evolutionary lineage containing all the descendants froma common ancestor). Furthermore, virus on FDCs was genet-ically heterogeneous, as evidenced by the presence of multiplebranches within the monophyletic group and the long branchlengths of the FDC-derived sequences. In contrast to HIVobtained from LN FDCs, virus from the unfractionated LNwas not monophyletic but clustered with a number of differentsites, including the brain and the bone marrow; however, virusfrom this tissue still contained substantial genetic diversity, as
indicated by the relatively long branch lengths compared tothose for virus from other tissues.
We next examined RT sequences of uncultured and cocul-tured virus from multiple sites in subject JHU614, who wastreated only with RT inhibitors (Fig. 5). FDC-trapped viruswas found distributed throughout the phylogenetic tree. How-ever, we also noted examples of completely segregated virusthat could be found in both the FDC and T-cell compartments,regardless of whether the samples originated from unculturedor cocultured material.
Because HIV in a presumed reservoir is predicted to have ahigh degree of genetic diversity due to the accumulation ofmultiple quasispecies over time, we measured the genetic di-versity of FDC-trapped HIV and compared diversity levelswith those of virus from other cell and tissue types. We selectedsubjects JHU559 and JHU614 for study because we couldcompare the diversity of sequences obtained from multiplecells and tissues. Genetic diversity was estimated by theta (� 2Ne�); Ne is the effective population size, and � is the mutationrate per site per generation (Table 3). Theta estimates forsubject JHU559 indicated that the FDC-derived sequenceswere more diverse (i.e., higher theta value) than all othersequences examined, with the exception of those derived fromthe unfractionated LN. An analysis of JHU614 sequences in-dicated that LN FDCs possessed quasispecies having a greaterdiversity than virus from all other tissue-derived cells. We alsonoted a difference in the overall diversity between FDC se-quences derived from the LNs and the spleen, where the LNFDC quasispecies demonstrated a threefold increase over thesplenic quasispecies. The effect of coculture on the geneticdiversity of FDC-trapped HIV appeared to be minimal, asevidenced by the similar theta estimates from sequences de-rived from either cultured or uncultured samples.
FDC-trapped HIV contains archived viral variants. Becauselong-term reservoirs contain archival virus, we comparedJHU614 viral sequences trapped on FDCs obtained postmor-tem with those from antemortem PBMCs to obtain evidence ofquasispecies that were extant at earlier times. We reasonedthat if FDC-trapped HIV included archived variants, we wouldobserve FDC isolates having genotypes identical or very closelyrelated to those present in the PBMC samples obtained manymonths prior to the patient’s death. We therefore constructeda genotype network comprised of FDC and PBMC-derivedviral RT sequences from JHU614 (Fig. 6). This network showsthe number of nucleotide changes existing between differentgenotypes (comprised of various numbers of identical se-quences). It was readily apparent that the FDC genotypes weredistributed throughout the network of PBMC-derived se-quences, consistent with the presence of multiple quasispeciesextant at different time intervals during the course of disease(Fig. 6). FDC samples also contained genotypes with few (e.g.,H39 and H40) as well as multiple nucleotide changes (e.g., H91and H92) separating the genotypes, consistent with virus trap-ping throughout the disease course. Most importantly, the
T-cell-derived sequences were obtained from coculture, “cc” prefaced the clone designation (e.g., FDC_cc34). Cocultured FDCs and T cells wereobtained from the same LN used for Fig. 1. Tissue sites are bone marrow (BM), meninges (MEN), mid-frontal gyrus (MFG), and unfractionatedlymph node (LN). BMCMC, Bayesian methods coupled with the Markov chain Monte Carlo method.
VOL. 82, 2008 FDC RESERVOIR OF HIV 5555
at BR
IGH
AM
YO
UN
G U
NIV
on February 5, 2009
jvi.asm.org
Dow
nloaded from

FDC genotypes were closely related to those of many previ-ously collected PBMC samples. Notably, the H26 genotypeconsisted of six identical sequences: five derived from FDCsand one from a PBMC sample collected 22 months prior to thepatient’s death. Furthermore, eight PBMC genotypes, H27,H30, H37, H47, H29, H36, H46, and H48, differed from theH26 genotype (largely derived from FDCs) by only a singlenucleotide and the PBMC sequences were all obtained fromsamples collected more than 20 months prior to the patient’sdeath (Fig. 6). Five of the single-nucleotide changes for theabove genotypes (i.e., V75A for H46, M184R for H47, D17Gfor H48, T139A for H29, and V241E for H36) were nonsyn-onymous, but none conferred drug resistance by itself. We alsonoted a difference in the overall number of nucleotide changespresent in samples obtained over 20 months prior to the pa-tient’s death compared to samples obtained 4 and 18 months
before death (Fig. 6). In general, the genotypes derived fromthe oldest two PBMC samples showed fewer nucleotidechanges than those obtained closer to death, as evidenced bythe numerous small circles connecting the genotypes in Fig. 6,where each small circle represents a putative ancestor with asingle nucleotide alteration.
We also examined drug resistance mutations from FDC- andPBMC-derived virus to determine whether the same resistantquasispecies were represented (Table 4). The K103N mutation(nonnucleoside RT inhibitor [NNRTI] resistance) was foundin 47 of 85 (55%) FDC and 14 of 70 (20%) PBMC-derivedsequences. Of the latter 14 PBMC resistance quasispecies, allwere found in samples obtained over 20 months prior to thepatient’s death. We observed five additional drug resistancemutations on the FDCs: K103S, V108I, Y188C, Y188H, andT215Y. All of these mutations confer resistance to NNRTIsexcept T215Y, which provides resistance to azidothymidine.Lastly, we discovered a resistance mutation, Y181C (NNRTIresistance), which could be detected only in a single PBMCclone obtained 18 months prior to the patient’s death. Thus, allbut one of the seven drug resistance genotypes found in subjectJHU614 were present on the FDCs. Collectively, these dataindicated the existence of archival virus on FDCs, therebysatisfying this criterion of a reservoir.
DISCUSSION
Viral reservoirs present major obstacles to the successfultreatment of HIV infection (3, 6). In the present study, weexamined human FDCs isolated from secondary lymphoid tis-sues obtained postmortem from infected subjects and foundthat FDC-trapped HIV was indeed a reservoir. This virus wasinfectious, genetically diverse, and included archived isolateswith drug resistance mutations that were not seen in other cellsor tissue sites. Furthermore, in contrast to other HIV reser-voirs, where each infected cell harbors on average one virus, asingle FDC may trap and retain multiple, genetically diverse,replication-competent virus particles. Thus, FDC-trapped HIVhas the potential to contribute to virus transmission, persis-tence, and diversification.
The replication-competent nature of FDC-trapped HIV wasdetermined in two different ways: a sensitive virus rescue bio-assay and cloning of virus quasispecies from uninfected T-celltargets that were cocultured with virus-bearing FDCs. Whenthe production of p24 was assessed in a coculture of FDCsobtained from subject JHU559, we noted the transmission of asignificant spreading infection, as evidenced by increasing p24production over the period of culture. In fact, less than 100 pgof HIV p24 present on the input FDCs led to the productionof over 65 ng of p24 in just 18 days, a more than 650-foldincrease. The establishment of a productive infection indicatesthat FDCs trapped intact virus particles as opposed to just viralproteins. It is also important to note that the FDCs themselves
FIG. 5. Phylogenetic analysis of uncultured and cocultured HIV RT sequences obtained from multiple sites in subject JHU614 (as describedfor Fig. 1). Phylogenetic analysis was performed using a Bayesian method. Statistical analysis is displayed as the posterior probability (by using theBayesian Markov Monte Carlo method). For sequence identification of the displayed data, see Fig. S1 in the supplemental material; theidentification utilizes the nomenclature explained for Fig. 1 to 4.
TABLE 3. Theta estimates of viral diversitya
Cell type/tissue forpatient � 95% CI
No. ofsequencesexamined
JHU559BM env 0.0193 0.0120–0.0326 22FDC env 0.0379 0.0246–0.0611 23T-cell env 0.0116 0.0068–0.0202 22MEN env 0.0289 0.0176–0.0504 18MFG env 0.0157 0.0081–0.0342 10LN (bulk) env 0.0896 0.0561–0.1546 17FDCb pol 0.0769 0.0565–0.1078 56T-cellb pol 0.018 0.0097–0.0345 17
JHU614BM pol 0.038 0.021–0.073 15DWM pol 0.067 0.034–0.152 9MEN pol 0.041 0.020–0.094 9FDC-LNc pol 0.123 0.095–0.162 75FDC-Splc pol 0.034 0.017–0.075 10LN pol 0.029 0.016–0.055 18T-cell-LNd pol 0.097 0.072–0.134 59T-cell-Spld pol 0.087 0.067–0.117 73PBMC 4-2000 pol 0.018 0.008–0.044 9PBMC 5-2000 pol 0.029 0.015–0.063 11PBMC 8-2000 pol 0.141 0.093–0.222 26PBMC 10-2001 pol 0.106 0.069–0.17 24
a The genetic diversity of HIV env and pol genes obtained from cells andtissues was determined using a phylogenetic approach to estimate nucleotidediversity implemented in LAMARC, version 2.0.2 (27). This program provided amaximum likelihood estimate of theta (� 2Ne�) where Ne is the inbreedingeffective population size and � is the per site mutation rate. BM, bone marrow;CI, confidence interval; DWM, deep white matter; MEN, meninges; MFG,mid-frontal gyrus.
b JHU559 FDC and T-cell sequences were derived from cocultured samples.c JHU614 FDC sequences were derived from both uncultured and cocultured
samples. Theta estimates for LN FDCs, excluding coculture (53 sequences), were0.102 with a 95% CI of 0.074 to 0.142.
d JHU614 T cell sequences were derived from both uncultured and coculturedsamples. Theta estimates for LN T cells, excluding coculture (24 sequences),were 0.043 (95% CI of 0.026 to 0.073) and for splenic T cells, excluding coculture(36 sequences), were 0.082 (95% CI of 0.056 to 0.123).
VOL. 82, 2008 FDC RESERVOIR OF HIV 5557
at BR
IGH
AM
YO
UN
G U
NIV
on February 5, 2009
jvi.asm.org
Dow
nloaded from

did not require an activation step to transmit infection, aswould be the case with a latent T-cell reservoir. The amount ofp24 generated in our cocultures in this study is consistent withour previous observations examining FDC transfer of virus,where a few picograms of HIV on FDCs produced 12 ngp24/ml after culture (52). These data from human FDCs arealso consistent with previous observations based on using xe-nogeneic cocultures of virus-bearing murine FDCs and humanCD4 T-cell targets, where we found that 40 pg of p24 trappedon murine FDCs in vivo resulted in the production of nano-gram levels of p24 in vitro (52). Thus, these data in both humanand murine systems confirm that FDC-trapped HIV is readilytransmissible.
Virus trapping and retention on FDCs are mediated primar-ily by specific antibodies and/or complement proteins coupledwith immune complex receptors on FDCs (21, 24, 53). Theantibodies involved in virus trapping would likely consist ofboth neutralizing and nonneutralizing forms, although the an-tibodies involved may have differing affinities, which in turn
could affect the stability of the virus over time. We postulatethat the FDC network of HIV may actually favor the mainte-nance of infectious virus particles. This preference could occuras a consequence of trapping virus with bound antibody, whichfrom in vitro studies maintains infectivity, a part of which ismediated by inhibiting gp120 shedding (53). A number ofother features of FDCs may also protect virus from degrada-tion, including the presence of high levels of thiol groups onFDC surfaces that create a reducing microenvironment (60),the envelopment of virions in the FDCs’ dendritic processesthat are known to sequester conventional protein antigensfrom the surrounding cells (55, 56), and the presence of com-plement regulatory proteins, such as CD55 (decay acceleratingfactor) (28).
Genetic analysis of FDC-trapped HIV indicated the pres-ence of a diverse repertoire of viral quasispecies. We foundinstances where FDC-trapped virus was genetically distinctfrom virus present in other cells; however, we also detectedexamples where FDC HIV was found associated with virus
FIG. 6. Genotype network analysis of HIV RT sequences obtained from postmortem FDCs and antemortem PBMCs from JHU614. Each solidline represents one mutational step and connects two quasispecies with at least a 95% confidence level. Small circles between genotype connectionsindicate a requirement for an additional mutational step per circle encountered between the genotypes. Broken lines indicate a more tenuousconnection, requiring 10 or more mutational steps connecting genotypes. The sizes of the solid squares and circles are proportional to the genotypefrequency, with the smallest size representing only one sequence. In the key, numbers following PBMC indicate the month and last two digits ofthe year in which the sample was collected.
5558 KEELE ET AL. J. VIROL.
at BR
IGH
AM
YO
UN
G U
NIV
on February 5, 2009
jvi.asm.org
Dow
nloaded from

from other cells and tissues. Our interpretation is that some ofthis “virus mixing” between FDCs and T-cell sequences reflectsthe mobile nature of T cells as they traffic throughout thesecondary lymphoid tissues. The presence of similar virus qua-sispecies on FDCs and T cells could arise in different ways. TheT cells could acquire virus from FDCs as they entered thegerminal center microenvironment, or alternatively, they couldenter the lymphoid tissue and produce virus that becametrapped on FDCs. A third alternative could occur where apreviously infected, virus-expressing cell releases progeny virusthat is in turn transported into secondary lymphoid tissues,where it both infects susceptible lymphocytes and becomestrapped on FDCs. These alternatives are not mutually exclu-sive, and we envision that within this dynamic tissue compart-ment, all three scenarios could occur simultaneously.
We do not yet understand whether virus trapped on FDCs atdifferent times during the disease course has different associ-ation/dissociation kinetics. However, if FDCs trap HIVthroughout the disease course, we expect multiple virus quasi-species to accumulate, thereby increasing the overall diversityof HIV in this site. When we analyzed the genetic diversity(i.e., theta) of virus from multiple cells and tissues in twoindependent infected subjects, we found that viral sequencestrapped on FDCs demonstrated greater diversity than didthose on most other cells and tissues. Because theta estimatesare derived from a linear function, one can directly analyze thevalues between different sites to compare the overall differ-ences in diversity from one site to another. In general, FDC-associated virus was about twofold more diverse than se-quences obtained from other tissue sites, regardless of whetherenv or pol genes were compared. Exceptions to this observationwere the unfractionated LN cells obtained from JHU559 and
the PBMC sample from JHU614 collected 18 months prior tothe patient’s death. In the latter instance, the sample showsdiversity similar to that of virus obtained from the LN FDCs. Itwas also apparent that PBMC samples segregated into twopopulations having theta values that differ by fivefold (i.e.,�0.02 for samples collected 21 and 22 months prior to thepatient’s death or 0.1 in samples collected at 4 or 18 monthsbefore death). This segregation based on diversity is furthersupported by the genotype network analysis of virus fromPBMCs, where the two older samples show a low number ofnucleotide changes between genotypes and the more recentones demonstrate a greater number of changes.
We also noted a difference in sequence diversity of virussamples from FDCs in the LN versus those from the spleen,with a threefold decrease in diversity noted in the splenicsamples. The different theta values in the two types of lym-phoid tissue were paralleled in JHU614 samples by the distinctgenetic differences observed between HIV on FDCs in the LNand those in the spleen. At this time, we do not know whetherthese observations represent a fundamental difference in viruslocalization in different types of secondary lymphoid tissues orare simply limited to a single specific patient. In the presentstudy, we were unable to address this question because of thelack of splenic tissue samples from more than one infectedsubject. Differences in virus localization in different secondarylymphoid tissues support the concept that at least in somesubjects, similar tissues may harbor unique virus isolates, eachof which could contribute to persisting infection. Further stud-ies with additional blood and tissue samples will undoubtedlyhelp resolve a number of these questions.
HIV reservoirs possess archived virus that is acquiredthroughout the course of disease. We looked for evidence of
TABLE 4. ARV resistance mutations from post- and antemortem samples from JHU614a
Cell type K103Nb K103S V108I Y188C Y188H T215Y Y181C
LN FDCs (cc) 6/22 0/22 0/22 0/22 0/22 0/22 0/22Ax 0/12 0/12 0/12 0/12 0/12 0/12 0/12Cx 6/10 0/10 0/10 0/10 0/10 0/10 0/10
LN FDCs (unc) 41/53 1/53 1/53 1/53 1/53 0/53 0/53Ax1 26/31 0/31 1/31 1/31 1/31 0/31 0/31Ax2 11/13 1/13 0/13 0/13 0/13 0/13 0/13Cx 4/9 0/9 0/9 0/9 0/9 0/9 0/9
Spl FDCs (cc) 0/10 0/10 0/10 0/10 0/10 2/10 0/10
Total cc FDCs 6/32 0/32 0/32 0/32 0/32 2/32 0/32
Total unc FDCs 41/53 1/53 1/53 1/53 1/53 0/53 0/53
Total FDCs 47/85 1/85 1/85 1/85 1/85 2/85 0/85PBMC (22 mo) 6/9 0/9 0/9 0/9 0/9 0/9 0/9PBMC (21 mo) 8/11 0/11 0/11 0/11 1/11 0/11 0/11PBMC (18 mo) 0/26 0/26 0/26 0/26 0/26 0/26 1/26PBMC (4 mo) 0/24 0/24 0/24 0/24 0/24 0/24 0/24
Total PBMC 14/70 0/70 0/70 0/70 1/70 0/70 1/70
Total mutations 61/155 1/155 1/155 1/155 2/155 2/155 1/155
a FDCs were immunoselected from postmortem tissue samples, and subgenomic pol was cloned and sequenced as described in the text. PBMCs were obtained fromantemortem blood samples and cloned and sequenced without culture. Results are shown as no. of samples/total number of samples. Abbreviations: Ax, axillary lymphnode; Cx, cervical lymph node; Ax1, the first axillary lymph node when more than one lymph node was obtained; Ax2, the second axillary lymph node when more thanone lymph node was obtained; Spl, spleen; For PBMCs, the number of months prior to the patient’s death is shown in parentheses. cc, cocultured; unc, uncultured.
b Numbering based on subgenomic sequencing of the first 248 amino acids of the reverse transcriptase gene.
VOL. 82, 2008 FDC RESERVOIR OF HIV 5559
at BR
IGH
AM
YO
UN
G U
NIV
on February 5, 2009
jvi.asm.org
Dow
nloaded from

archival virus by examining drug resistance mutations fromFDCs and comparing them to resistance mutations present inPBMC samples collected several months prior to the patient’sdeath. We found mutations on FDCs that were present in ourearliest samples of blood but that then disappeared in bloodsamples obtained closer to death. We reason that as subjectJHU614 discontinued and then reinstituted ARV therapy,there were periods of time when drug concentrations would below enough to allow the virus to mutate, while at the same timebe present in a high enough concentration to provide selectivepressure for the establishment of resistance mutations. Wepresume that in the absence of drug treatment, these muta-tions possessed no selective advantage and were lost from thecirculating virus pool but remained trapped on FDCs. It shouldbe noted that the FDC-derived sequences with this mutationwere detected in both uncultured and cultured FDCs, indicat-ing the infectious nature of these virus variants. Another strongargument for the archival nature of FDC HIV is the genotypicanalysis of virus derived from FDC and PBMC samples. Thesegenotypes indicate a very close relationship (i.e., one or twonucleotide changes) and, in one case, an identical one betweenthe FDC and a majority of the PBMC genotypes collected at 21and 22 months antemortem. Taken together, these datastrongly support the archival nature of FDC-trapped HIV.
Since the first identification of HIV on FDCs, it has beendifficult to directly measure virus in this compartment (11, 37).To help understand this important site, investigators have im-plemented mathematical modeling to estimate viral dynamicswithin lymphoid tissue. These dynamics include the originalestimates of viral reservoirs, with a biphasic decay rate duringantiretroviral treatment (38). These models accurately esti-mated the rapid reduction of the lymphoid tissue compart-ment, but could not directly estimate virus trapped on FDCs(33). A more recent mathematical model, which directly esti-mates on/off rates for virus trapped on FDCs, concludes thatthese cells can be reservoirs of infectious virus, thus offeringadditional support to the data reported here (17). Further-more, this model predicts that a patient with a rapid dissocia-tion of virus on FDCs may have a better clinical outcome withsuccessful therapy. Those subjects with slow dissociation kinet-ics of FDC virus may have worsening clinical prognoses withmore frequent drug failures. As we gain greater understandingof the contributions of FDC-trapped HIV in pathogenesis, weshould be able to directly test the above estimates.
Here we report the genetic characterization of HIV trappedon human FDCs. This study illustrates the infectious and di-verse nature of virus in this reservoir. Moreover, the presenceof archival forms coupled with the ability of FDCs to preservevirus infectivity over time suggests the continued presence ofdiverse virus that could reignite and perpetuate infectionthroughout the disease course. A better understanding of thislarge and diverse repository of infectious virus may be criticalin the goal of controlling HIV and understanding how to de-feat the virus in this reservoir.
ACKNOWLEDGMENTS
This research complied with all relevant federal and institutionalpolicies. The authors acknowledge that they have no financial or otherrelationships that would pose a conflict of interest relating to theresearch presented in this study.
This work was supported by grants from the National Institutes ofHealth, National Institute of Allergy and Infectious Disease (AI39963and AI57007), National Institutes of Health, National Institute ofGeneral Medicine (GM66276), and the American Foundation forAIDS Research (106365-33-RGRL).
REFERENCES
1. Armstrong, J. A. 1991. Ultrastructure and significance of the lymphoid tissuelesions in HIV infection, p. 69–82. In P. Racz, C. D. Dijkstra, and J. C.Gluckman (ed.), Accessory cells in HIV and other retroviral infections.Karger, Basel, Switzerland.
2. Biberfeld, P., A. Porwit, G. Biberfield, M. Harper, A. Bodner, and R. Gallo.1988. Lymphadenopathy in HIV (HTLV-III LAV) infected subjects: the roleof virus and follicular dendritic cells. Cancer Detect. Prev. 12:217–224.
3. Blankson, J. N., D. Persaud, and R. F. Siliciano. 2002. The challenge of viralreservoirs in HIV-1 infection. Annu. Rev. Med. 53:557–593.
4. Burton, G. F., A. Masuda, S. L. Heath, B. A. Smith, J. G. Tew, and A. K.Szakal. 1997. Follicular dendritic cells (FDC) in retroviral infection: host/pathogen perspectives. Immunol. Rev. 156:185–197.
5. Chun, T. W., L. Carruth, D. Finzi, X. Shen, J. A. DiGiuseppe, H. Taylor, M.Hermankova, K. Chadwick, J. Margolick, T. C. Quinn, Y. H. Kuo, R. Brook-meyer, M. A. Zeiger, P. Barditch-Crovo, and R. F. Siliciano. 1997. Quanti-fication of latent tissue reservoirs and total body viral load in HIV-1 infec-tion. Nature 387:183–188.
6. Chun, T. W., and A. S. Fauci. 1999. Latent reservoirs of HIV: obstacles to theeradication of virus. Proc. Natl. Acad. Sci. USA 96:10958–10961.
7. Chun, T. W., L. Stuyver, S. B. Mizell, L. A. Ehler, J. A. Mican, M. Baseler,A. L. Lloyd, M. A. Nowak, and A. S. Fauci. 1997. Presence of an inducibleHIV-1 latent reservoir during highly active antiretroviral therapy. Proc. Natl.Acad. Sci. USA 94:13193–13197.
8. Clement, M., D. Posada, and K. A. Crandall. 2000. TCS: a computer pro-gram to estimate gene genealogies. Mol. Ecol. 9:1657–1659.
9. Collman, R. G., C. F. Perno, S. M. Crowe, M. Stevenson, and L. J. Montaner.2003. HIV and cells of macrophage/dendritic lineage and other non-T cellreservoirs: new answers yield new questions. J. Leukoc. Biol. 74:631–634.
10. Crandall, K. A., and A. R. Templeton. 1999. Statistical approaches to de-tecting recombination, p. 153–176. In K. A. Crandall (ed.), The evolution ofHIV. The Johns Hopkins University Press, Baltimore, MD.
11. Dumaurier, M. J., S. Gratton, S. Wain-Hobson, and R. Cheynier. 2005. Themajority of human immunodeficiency virus type 1 particles present withinsplenic germinal centres are produced locally. J. Gen. Virol. 86:3369–3373.
12. Felsenstein, J. 1985. Confidence limits on phylogenies: an approach usingthe bootstrap. Evolution 39:783–791.
13. Felsenstein, J. 1981. Evolutionary trees from DNA sequences: a maximumlikelihood approach. J. Mol. Evol. 17:368–376.
14. Finzi, D., J. Blankson, J. D. Siliciano, J. B. Margolick, K. Chadwick, T.Pierson, K. Smith, J. Lisziewicz, F. Lori, C. Flexner, T. C. Quinn, R. E.Chaisson, E. Rosenberg, B. Walker, S. Gange, J. Gallant, and R. F. Siliciano.1999. Latent infection of CD4� T cells provides a mechanism for lifelongpersistence of HIV-1, even in patients on effective combination therapy. Nat.Med. 5:512–517.
15. Finzi, D., M. Hermankova, T. Pierson, L. M. Carruth, C. Buck, R. E.Chaisson, T. C. Quinn, K. Chadwick, J. Margolick, R. Brookmeyer, J. Gal-lant, M. Markowitz, D. D. Ho, D. D. Richman, and R. F. Siliciano. 1997.Identification of a reservoir for HIV-1 in patients on highly active antiret-roviral therapy. Science 278:1295–1300.
16. Fox, C. H., K. Tenner-Racz, P. Racz, A. Firpo, P. A. Rizzo, and A. S. Fauci.1991. Lymphoid germinal centers are reservoirs of human immunodeficiencyvirus type 1 RNA. J. Infect. Dis. 164:1051–1057.
17. Garcıa, J. A., L. E. Soto-Ramirez, G. Cocho, T. Govezensky, and M. V. Jose.2006. HIV-1 dynamics at different time scales under antiretroviral therapy. J.Theor. Biol. 238:220–229.
18. Guindon, S., and O. Gascuel. 2003. A simple, fast, and accurate algorithm toestimate large phylogenies by maximum likelihood. Syst. Biol. 52:696–704.
19. Haase, A. T. 1999. Population biology of HIV-1 infection: viral and CD4� Tcell demographics and dynamics in lymphatic tissues. Annu. Rev. Immunol.17:625–656.
20. Haase, A. T., K. Henry, M. Zupancic, G. Sedgewick, R. A. Faust, H. Melroe,W. Cavert, K. Gebhard, K. Staskus, Z.-Q. Zhang, P. Dailey, H. H. Balfour,Jr., A. Erice, and A. S. Perelson. 1996. Quantitative image analysis of HIV-1infection in lymphoid tissue. Science 274:985–989.
21. Heath, S. L., J. G. Tew, J. G. Tew, A. K. Szakal, and G. F. Burton. 1995.Follicular dendritic cells and human immunodeficiency virus infectivity. Na-ture 377:740–744.
22. Helm, S. L., G. F. Burton, A. K. Szakal, and J. G. Tew. 1995. Folliculardendritic cells and the maintenance of IgE responses. Eur. J. Immunol.25:2362–2369.
23. Huelsenbeck, J. P., B. Larget, R. E. Miller, and F. Ronquist. 2002. Potentialapplications and pitfalls of Bayesian inference of phylogeny. Syst. Biol. 51:673–688.
24. Kacani, L., W. M. Prodinger, G. M. Sprinzl, M. G. Schwendinger, M.
5560 KEELE ET AL. J. VIROL.
at BR
IGH
AM
YO
UN
G U
NIV
on February 5, 2009
jvi.asm.org
Dow
nloaded from

Spruth, H. Stoiber, S. Dopper, S. Steinhuber, F. Steindl, and M. P. Dierich.2000. Detachment of human immunodeficiency virus type 1 from germinalcenters by blocking complement receptor type 2. J. Virol. 74:7997–8002.
25. Kay, M. S. 2003. Silent, but deadly—eliminating reservoirs of latent HIV.Trends Biotechnol. 21:420–423.
26. Klaus, G. G. B., J. H. Humphrey, A. Kunkl, and D. W. Dongworth. 1980. Thefollicular dendritic cell: its role in antigen presentation in the generation ofimmunological memory. Immunol. Rev. 53:3–28.
27. Kuhner, M. K. 2006. LAMARC 2.0: maximum likelihood and Bayesianestimation of population parameters. Bioinformatics 22:768–770.
28. Lampert, I. A., J. B. Schofield, P. Amlot, and S. Van Noorden. 1993. Pro-tection of germinal centres from complement attack: decay-accelerating fac-tor (DAF) is a constitutive protein on follicular dendritic cells. A study inreactive and neoplastic follicles. J. Pathol. 170:115–120.
29. Laurence, J. 1993. Reservoirs of HIV infection or carriage: monocytic, den-dritic, follicular dendritic, and B cells. Ann. N. Y. Acad. Sci. 693:52–64.
30. Liu, Y., X. P. Tang, J. C. McArthur, J. Scott, and S. Gartner. 2000. Analysisof human immunodeficiency virus type 1 gp160 sequences from a patientwith HIV dementia: evidence for monocyte trafficking into brain. J. Neuro-virol. 6(Suppl. 1):S70–S81.
31. Mandel, T. E., R. P. Phipps, A. Abbot, and J. G. Tew. 1980. The folliculardendritic cell: long term antigen retention during immunity. Immunol. Rev.53:29–59.
32. Meltzer, M. S., M. Nakamura, B. D. Hansen, J. A. Turpin, D. C. Kalter, andH. E. Gendelman. 1990. Macrophages as susceptible targets for HIV infec-tion, persistent viral reservoirs in tissue, and key immunoregulatory cells thatcontrol levels of virus replication and extent of disease. AIDS Res. Hum.Retrovir. 6:967–971.
33. Muller, V., A. F. Maree, and R. J. De Boer. 2001. Release of virus fromlymphoid tissue affects human immunodeficiency virus type 1 and hepatitis Cvirus kinetics in the blood. J. Virol. 75:2597–2603.
34. Nickle, D. C., M. A. Jensen, D. Shriner, S. J. Brodie, L. M. Frenkel, J. E.Mittler, and J. I. Mullins. 2003. Evolutionary indicators of human immuno-deficiency virus type 1 reservoirs and compartments. J. Virol. 77:5540–5546.
35. Nickle, D. C., D. Shriner, J. E. Mittler, L. M. Frenkel, and J. I. Mullins.2003. Importance and detection of virus reservoirs and compartments ofHIV infection. Curr. Opin. Microbiol. 6:410–416.
36. Orenstein, J. M., C. Fox, K. Tenner-Racz, and P. Racz. 1997. Is HIV foundin the cytoplasm of dendritic cells? Am. J. Pathol. 151:1173–1176.
37. Pantaleo, G., O. J. Cohen, T. Schacker, M. Vaccarezza, C. Graziosi, G. P.Rizzardi, J. Kahn, C. H. Fox, S. M. Schnittman, D. H. Schwartz, L. Corey,and A. S. Fauci. 1998. Evolutionary pattern of human immunodeficiencyvirus (HIV) replication and distribution in lymph nodes following primaryinfection: implications for antiviral therapy. Nat. Med. 4:341–345.
38. Perelson, A. S., P. Essunger, Y. Cao, M. Vesanen, A. Hurley, K. Saksela, M.Markowitz, and D. D. Ho. 1997. Decay characteristics of HIV-1-infectedcompartments during combination therapy. Nature 387:188–191.
39. Pierson, T., J. McArthur, and R. F. Siliciano. 2000. Reservoirs for HIV-1:mechanisms for viral persistence in the presence of antiviral immune re-sponses and antiretroviral therapy. Annu. Rev. Immunol. 18:665–708.
40. Pomerantz, R. J. 2003. Reservoirs, sanctuaries, and residual disease: thehiding spots of HIV-1. HIV Clin. Trials 4:137–143.
41. Posada, D., and T. R. Buckley. 2004. Model selection and model averagingin phylogenetics: advantages of Akaike information criterion and Bayesianapproaches over likelihood ratio tests. Syst. Biol. 53:793–808.
42. Posada, D., and K. A. Crandall. 2001. Intraspecific gene genealogies: treesgrafting into networks. Trends Ecol. Evol. 16:37–45.
43. Posada, D., and K. A. Crandall. 1998. MODELTEST: testing the model ofDNA substitution. Bioinformatics 14:817–818.
44. Posada, D., and K. A. Crandall. 2002. The effect of recombination on theaccuracy of phylogeny estimation. J. Mol. Evol. 54:396–402.
45. Racz, P., K. Tenner-Racz, and H. Schmidt. 1989. Follicular dendritic cells inHIV-induced lymphadenopathy and AIDS. APMIS Suppl. 8:16–23.
46. Robertson, D. L., B. H. Hahn, and P. M. Sharp. 1995. Recombination inAIDS viruses. J. Mol. Evol. 40:249–259.
47. Robertson, D. L., P. M. Sharp, F. E. McCutchan, and B. H. Hahn. 1995.Recombination in HIV-1. Nature 374:124–126.
48. Ronquist, F., and J. P. Huelsenbeck. 2003. MrBayes 3: Bayesian phylogeneticinference under mixed models. Bioinformatics 19:1572–1574.
49. Saksena, N. K., and S. J. Potter. 2003. Reservoirs of HIV-1 in vivo: impli-cations for antiretroviral therapy. AIDS Rev. 5:3–18.
50. Schierup, M. H., and J. Hein. 2000. Consequences of recombination ontraditional phylogenetic analysis. Genetics 156:879–891.
51. Siliciano, R. F. 1999. Latency and reservoirs for HIV-1. AIDS 13(Suppl.A):S49–S58.
52. Smith, B. A., S. Gartner, Y. Liu, A. S. Perelson, N. I. Stilianakis, B. F. Keele,T. M. Kerkering, A. Ferreira-Gonzalez, A. K. Szakal, J. G. Tew, and G. F.Burton. 2001. Persistence of infectious HIV on follicular dendritic cells.J. Immunol. 166:690–696.
53. Smith-Franklin, B. A., B. F. Keele, J. G. Tew, S. Gartner, A. K. Szakal, J. D.Estes, T. C. Thacker, and G. F. Burton. 2002. Follicular dendritic cells andthe persistence of HIV infectivity: the role of antibodies and Fc� receptors.J. Immunol. 168:2408–2414.
54. Stoiber, H., A. Clivio, and M. P. Dierich. 1997. Role of complement in HIVinfection. Annu. Rev. Immunol. 15:649–674.
55. Szakal, A. K., and M. G. Hanna, Jr. 1968. The ultrastructure of antigenlocalization and virus-like particles in mouse spleen germinal centers. Exp.Mol. Pathol. 8:75–89.
56. Szakal, A. K., M. H. Kosco, and J. G. Tew. 1989. Microanatomy of lymphoidtissue during the induction and maintenance of humoral immune responses:structure function relationships. Annu. Rev. Immunol. 7:91–109.
57. Temin, H. M. 1991. Sex and recombination in retroviruses. Trends Genet.7:71–74.
58. Tenner-Racz, K., and P. Racz. 1995. Follicular dendritic cells initiate andmaintain infection of the germinal centers by human immunodeficiencyvirus. Curr. Top. Microbiol. Immunol. 201:141–159:141-159.
59. Tew, J. G., and T. E. Mandel. 1979. Prolonged antigen half-life in thelymphoid follicles of specifically immunized mice. Immunology 37:69–76.
60. Tew, J. G., J. Wu, D. Qin, S. Helm, G. F. Burton, and A. K. Szakal. 1997.Follicular dendritic cells and presentation of antigen and costimulatory sig-nals to B cells. Immunol. Rev. 156:39–52.
61. Thompson, J. D., T. J. Gibson, F. Plewniak, F. Jeanmougin, and D. G.Higgins. 1997. The CLUSTAL_X windows interface: flexible strategies formultiple sequence alignment aided by quality analysis tools. Nucleic AcidsRes. 25:4876–4882.
62. Wong, J. K., M. Hezareh, H. F. Gunthard, D. V. Havlir, C. C. Ignacio, C. A.Spina, and D. D. Richman. 1997. Recovery of replication-competent HIV,despite prolonged suppression of plasma viremia. Science 278:1291–1295.
VOL. 82, 2008 FDC RESERVOIR OF HIV 5561
at BR
IGH
AM
YO
UN
G U
NIV
on February 5, 2009
jvi.asm.org
Dow
nloaded from