Embed Size (px)
Citation preview

Chapter01.3.indd 30 10/02/14 11:17 AM

CHAPTER 1.3THE CURRENT STATUS OF TB IN
THE WORLD: THE INFLUENCE OF POVERTY, PRISONS, HIV,
IMMIGRATION AND CONTROL PROGRAMMES
Joan-Pau Millet, Angels Orcau, Patricia García de Olalla, Vicente Martín, Antonio Moreno, Laia Fina, Lucia del Baño,
Pere Simón, Eva Masdeu, Joan A. Caylà.
‘Compared to the diseases that generate misery, compared to sadness, the anguish and the social misfortune of the people, the
microbes, as causes of disease, are minor causes.’
Ramon Carrillo
‘…there is a killer on the road.’
Riders on the stormThe doors
From the series Local WarmingRoberto FabeloOil on canvas; 175 3 205 cm
Chapter01.3.indd 31 10/02/14 11:17 AM

Chapter01.3.indd 32 10/02/14 11:17 AM

INTRODUCTION According to the last WHO Tuberculosis Annual Report (1), in 2011, there were 8.7 million new cases of TB. Similarly, in 2010 there were 8.8 million (range, 8.5–9.2 million) incident cases, 1.1 million (range, 0.9–1.2 million) deaths from TB among HIV-negative people and an additional 0.35 million (range, 0.32–0.39 million) deaths from HIV-associated TB (2).
Although the burden of the disease lies largely in low income countries, high income countries have also seen the highest rates of TB mortality in past centuries. Historically, studies have also shown that these rates can vary greatly according to occupation or social class (3). Among men from London in 1930, lawyers, bankers, physicians, and surgeons had very low risk of death from TB, while servants, waiters, factory and construction labourers had the highest mortality rates (4). Historical data in Spain from the last century reveal that over 2 million of its inhabitants died from TB between 1900 and 1950, more deaths than those in the Spanish Civil War. Before the introduction of effective drugs against Mycobacterium tuberculosis (MTB) in the 1950s, mortality had decreased considerably in high income countries due to improving economic and social conditions.
The objective of this chapter is to describe the current epidemiology of TB worldwide — particularly in Europe (5), with Spain, and Barcelona as specific examples — by analysing the role of poverty, prisons, HIV infection, immigration, and TB control programmes. The epidemiological data from Spain in general, and Barcelona in particular are from the official registries.
TB INCIDENCE AND MORTALITY BY WHO REGIONS To address TB as a global problem, the WHO defines six world regions: the African Region (AFR), the American Region (AMR), the Eastern Mediterranean Region (EMR), the European Region (EUR), the South-East Asian Region (SEAR), and the Western Pacific Region (WPR). The number of cases as well as the rates of prevalence, incidence, and mortality associated with TB fluctuates by year and region.
CHAPTER 1.3THE CURRENT STATUS OF TB IN THE WORLD: THE INFLUENCE OF POVERTY, PRISONS, HIV, IMMIGRATION AND CONTROL
PROGRAMMES
Chapter01.3.indd 33 10/02/14 11:17 AM

34 SECTION 1 THE PRoblEm
The global TB incidence in the world has appeared to be slowly decreasing by 1.3% per year since 2002. According to WHO estimates, 8.8 million cases existed in 2010 (range 8.5–9.2 million), equivalent to 128 cases per 100,000 globally. However, great variation existed by country and region (Figure 1.3.2): 276 per 100,000 population in AFR, 29 per 100,000 in AMR, 109 per 100,000 in EMR, 47 per 100,000 in EUR, 193 per 100,000 in SEAR and 93 per 100,000 population in WPR. Incidence rates are declining in all of WHO’s six regions. The rate of decline ranges from less than 1% per year in the EMR, to 1.8% in the AFR and 3.7% per year in the AMR (2). If this trend is sustained, the Millennium Development Goals (MDG) Target 6.c will be achieved by 2015.
The absolute number of incidence cases has started to fall slowly since 2006. Most of the 8.8 million estimated number of cases in 2010 occurred in Asia (59%) and Africa (26%) with smaller proportions in the EMR, EUR and AMR of 7%, 5% and 3% respectively. The 22 High Burden Countries (HBC) have been the highest priority at the global level, since the year 2000 have accounted for the 81% of all estimated cases worldwide. The five countries with the largest number of incident cases in 2010 were India (2.0–2.5 million), China (0.89–1.2 million), South Africa (0.4–0.59 million), Indonesia (0.37–0.54 million) and Pakistan (0.33–0.48 million). India and China accounted for an estimated of 38% of the total TB cases (2).
Regarding an estimated 12.0 million prevalent cases (range, 11–14 million) of TB in 2010, current forecasts suggest that the Stop TB Partnership’s target of halving TB prevalence by 2015 will not be achieved. However, regional prevalence is falling globally in all six WHO regions. In fact, the Stop TB partnership target has already been met in the AMR, and in the WPR the target has been close to achieve. Since the year 2000, prevalence in the EMR, EUR and SEAR have experienced significant reductions, but the 2015 target will not be reached. As for the African Region, prevalence rates by 2015 seem unlikely to reach the target (2).
As the 2011 WHO report shows, TB mortality rates have also fallen by more than one-third since 1990 and the target of the Stop TB Partnership of a 50% reduction by 2015 compared to 1990 will be met if the current trend is sustained. It could also be achieved in all WHO regions with the exception of the American Region. However, in 2010, approximately 1.4 million (1.2–1.5 million) were still reportedly died of TB in 2010 (20 deaths per 100,000 population). An estimated of 1.1 million deaths (ranging from 0.9–1.2 million) occurred among HIV-negative cases of TB, an equivalent of 15 deaths per 100,000 population. An estimated of 0.35 million deaths (range, 0.32–0.39 million) were among incident HIV-infected TB cases (2). In the EUR more than 60,000 deaths were estimated as being due to TB (6.7 cases per 100,000 population) (4).
Chapter01.3.indd 34 10/02/14 11:17 AM

35 CHAPTER 1.3THE CURRENT STATUS OF TB IN THE WORLD: THE INFLUENCE OF POVERTY, PRISONS, HIV, IMMIGRATION AND CONTROL
PROGRAMMES
Regarding HIV, of the 8.8 million incident cases in 2010, 1.0 million to 1.2 million (12–14%) were among people living with HIV, with the best estimate of 1.1 million (13%). The proportion of TB cases co-infected with HIV is the highest in countries in the African Region, and accounted for 82% of TB cases among people living with HIV. In relation to TB cases co-infected with HIV globally, since 2002 the incidence rate has dropped at around 1.3% a year, peaking in 2004 and the absolute number of incident cases has started to fall since 2006. In the European region, 3.9% of TB incidence is found in HIV-infected individuals (2).
The latest ECDC/WHO surveillance report 2012 (5), describes the situation in the EUR as a mixed epidemiological picture, with a high percentage of TB cases of foreign origin (Figure 1.3.1).
Source: ECDC report 2009.
Figure 1.3.1 Percentage of notified TB cases of foreign origin in Europe, 2009
According to WHO (2), the incidence rate for the EUR countries ranges from less than 5 to over 200 cases per 100,000 population with a regional average of 34 cases per 100,000 population. The TB incidence in the European Union/European Economic Area countries remains low, with TB notification rates in Central and Eastern Europe are much higher than the rates in the West. The majority of the new
Chapter01.3.indd 35 10/02/14 11:17 AM

36 SECTION 1 THE PRoblEm
episodes of TB in 2010 and deaths from TB in the EUR were from the 18 HPC (High Priority Countries) within the region, where notifications of newly detected and relapse TB cases (68.5 per 100,000 population) remained almost 8 times higher than those reported in the rest of the region (8.4 per 100,000 population) (6).
The incidence of TB in Spain was estimated at 38.5 per 100,000 population in 1995 and 1996 with significant regional differences. The notified rate of pulmonary TB was 11.6 per 100,000 population in 2010 and ranged between 7.1 and 28.5 per 100,000 population according to region. In 2010, the WHO and ECDC estimated a TB incidence of 16 per 100,000 population in Spain and almost double for the TB incidence in Portugal (29 cases per 100,000 population) (2).
THE INFLUENCE OF POVERTY AND ECONOMIC CRISISTB incidence can vary by country from 10 to over 300 cases per 100,000 population (Figure 1.3.2) and also mirrors the country’s Gross Domestic Product (GDP) (Figure 1.3. 3).
Source: WHO report 2011.
Figure 1.3.2 Estimated TB incidence rates per 100,000 inhabitants in the world by country in 2011
Chapter01.3.indd 36 10/02/14 11:17 AM

37 CHAPTER 1.3THE CURRENT STATUS OF TB IN THE WORLD: THE INFLUENCE OF POVERTY, PRISONS, HIV, IMMIGRATION AND CONTROL
PROGRAMMES
Source: International Monetary Fund, 2010.
Figure 1.3.3 GDP per capita in the world by country in 2010
However, it is noteworthy that some low income countries, such as Peru or Cuba, have given TB control a political priority and achieved better results than high income countries.
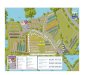
The trend observed within most countries is that poorer areas tend to have higher TB incidences. The relationship between the socio-economic level and TB is most apparent in large cities. Metropolitan areas also have higher incidences than their country’s overall, and when the TB incidence is analysed by district or neighbourhood, the most disadvantaged areas have the higher incidences, as shown in Paris, London or Barcelona. For example, the Ciutat Vella neighbourhood in Barcelona has an incidence 5-6 times higher than that of the entire city. This trend is due to pockets of poverty (especially in the inner city) that exist within large cities. The TB risk factors in these areas include being a recently-arrived immigrant from a low income country with high TB incidence and precarious living conditions. In Barcelona, 80 per cent of the TB cases in poor neighbourhoods are manifested in immigrants (Figure 1.3.4).
Chapter01.3.indd 37 10/02/14 11:17 AM

38 SECTION 1 THE PRoblEm
Figure 1.3.4 Geographical distribution of TB cases in South Raval, Barcelona in 2011
To put in other words, the important economic and financial crisis that the world is facing and the increase of poverty caused by it, will have an impact on TB epidemiology.
THE INFLUENCE OF PRISONS An estimated 10 million people are incarcerated in the world and the number continues to grow. It could be multiplied by four to six if the number of people admitted per year is included. The prison population is normally comprised of young men of low socio-economic status and belonging to an ethnic, political, or religious minority. Prisons tend to have problems with overcrowding, poor hygiene, violence, and few health care resources. The characteristics of the prisoners and the conditions of a prison both favour disease transmission and complicate disease control. TB can be seen as a paradigm of this phenomenon (6).
Chapter01.3.indd 38 10/02/14 11:17 AM

39 CHAPTER 1.3THE CURRENT STATUS OF TB IN THE WORLD: THE INFLUENCE OF POVERTY, PRISONS, HIV, IMMIGRATION AND CONTROL
PROGRAMMES
In spite of the fact that the highest TB incidences in prisons have never been published, the incidences that are published frequently exceed the country’s global rate by 100 times. TB prevalence in Russian and Georgian prisons is 4,560 and 5,995 cases per 100,000 population, respectively. It is estimated that TB prevalence in prisons in Europe — 393 per 100,000 — is 84 times higher compared to the non-incarcerated population. Similarly, TB incidence in prisons in Latin America and the Caribbean are an estimated 22 times higher (1,000 per 100,000) than those of the general population (7). The highest rates in prison populations are found in Africa, where published studies reveal rates of 3,500 to 5,800 cases per 100,000 prisoners. Published data on TB in prisons in Asia is sparse; the estimated incidence in Taiwan is 25.9 cases per 100,000 prisoners and the prevalence in Pakistan is 3,900 cases per 100,000 prisoners (8).
Lack of effective prevention and control programmes in prisons have given rise to the high prevalence of multidrug-resistant TB (MDR-TB) and extensively drug-resistant TB (XDR-TB), especially in countries where anti-TB drugs are available but not monitored. For example, in Russia and other republics of the former Soviet Union, between 12 and 55 per cent of MDR-TB patients have previously been treated. A study from Thailand also reports that 19 per cent of the TB cases are MDR (2, 5).
HIV and MTB co-infection is also an important concern in prison populations, notably in countries where co-infection prevalence is high. For example, studies estimate that between 26 per cent and 73 per cent of TB patients in Africa are co-infected with HIV. Intravenous drug users (IDU) also have an elevated risk of co-infection. In Spain, an estimated 10 per cent of TB patients in prisons are infected with HIV (9) and 42.8 per cent of HIV patients are IDU (9). An incidence of more than 2,000 per 100,000 prisoners was calculated by molecular epidemiology: 51 per cent were in clusters and one smear-positive patient had transmitted TB to 20 HIV-infected prisoners (11).
THE INFLUENCE OF HIV INFECTION HIV-induced immunosupression is the most important risk of progression to active TB disease. People with HIV co-infection are about 21–34 times more likely to develop TB disease compared with those who are HIV-negative (2, 12). Although antiretroviral treatment is available and TB is curable, 1.8 million people still die of AIDS-related causes and 1.45 million from TB, 24% of whom die from HIV-associated TB (2).
Chapter01.3.indd 39 10/02/14 11:17 AM

40 SECTION 1 THE PRoblEm
One-third of people infected with HIV are also infected with MTB. TB is the most common opportunistic infection and a major cause of mortality among HIV-infected persons. In addition, TB is the first manifestation of AIDS in more than 50% of cases in low income countries, and the second indicative disease in Europe (18%) (5, 7, 13). Globally, 30% of HIV-infected persons are estimated to have infection with MTB; this percentage varies from 14% in Europe to 46% in Southeast Asia (14). This dual epidemic mainly occurs in low income countries, particularly in the African Region, which accounts for 82% of the new TB co-infected with HIV cases in 2010. It is estimated that 39% of the 2.3 million people who developed TB in 2010 were HIV-infected (2).
The global epidemiology of drug-resistant TB in HIV-infected persons is not well known due to the lack of information. In a systematic review including 32 studies from 15 countries, it does not demonstrate any association between MDR-TB and HIV infection (15). However, outbreaks of drug-resistant TB primarily affect HIV-infected persons and are associated with a significantly higher mortality rate and short survival period (16, 17).
Diagnosis of active TB disease in HIV-infected persons is difficult, since patients with HIV-associated TB have fewer bacilli in their sputum than HIV-negative patients with pulmonary TB (18). Also, it has been observed that the presence of a cough for 13 weeks is not by itself sensitive enough for the diagnosis of TB in HIV-infected persons (19). In addition, the chest X-ray can be normal in up to 14% of HIV-infected persons who have culture-confirmed pulmonary TB (20). On the other hand, morbidity and mortality of patients co-infected with TB and HIV have been improved due to the introduction of highly active antiretroviral therapy (HAART). According to the WHO, only 42% of the world population that needs the treatment, have access to the HAART. This treatment must be extended around the world, particularly in low income countries where more people are affected with this lethal co-infection (21, 22).
In conclusion, these two diseases represent a deadly combination, since they are more destructive together than either of them alone. TB is harder to diagnose in HIV-infected people, progresses faster and is almost certain to be fatal if undiagnosed or left untreated. The dual HIV-TB epidemic poses one of the greatest diagnostic and therapeutic challenges for public health. Early identification of persons with TB, provision of TB prevention and treatment in a safe environment with no risk of TB transmission, and the appropriate treatment of the HIV-infected patients will increase patient’s survival and reduce the risk of developing TB, HIV resistances and TB recurrences worldwide.
Chapter01.3.indd 40 10/02/14 11:17 AM

41 CHAPTER 1.3THE CURRENT STATUS OF TB IN THE WORLD: THE INFLUENCE OF POVERTY, PRISONS, HIV, IMMIGRATION AND CONTROL
PROGRAMMES
THE INFLUENCE OF IMMIGRATION The migratory movements play an important role in the TB profile worldwide. Germany, France, and the United Kingdom have experienced stable immigration from former colonies since the 1950s. In Spain, immigration for economic reasons did not experience a significant increase until the last decades of the 20th century and early 21st century, taking over from the increase due to AIDS. This relationship has modulated the map of TB in our country.
In 2010, more than 5,700,000 (12%) people living in Spain were from other countries. In recent years, Romania, Morocco, United Kingdom, Ecuador, Colombia and Bolivia are the most common countries of origin. However, the distribution is not homogeneous in our regions. According to the 2009 census, in Madrid and Catalonia, Latin Americans and Africans represent two thirds of the immigrants, while 75.5% of all Pakistani immigrants are in Catalonia. The majority of British immigrants living in Spain are in Alicante and Málaga, and almost half of the Romanians, are living in Madrid or Castellon. This complex picture is reflected in the TB distribution in our country (23).
In 2010, from all the cases detected in Barcelona, 233 (54.3%) were foreign-born. Ciutat Vella, the neighbourhood with the lowest socio-economic level had an incidence of more than 166 cases per 100,000 population and 80% of the TB cases identified in this neighbourhood were diagnosed in immigrants. By areas, people coming from the Asiatic continent represent 43% of the total number of cases, with the majority from Pakistan. Out of the total immigrant population, 37 % were from Latin America and 13% from Africa (24). Moreover, a population-based cohort study in Barcelona shows that immigrants also have three times more risk of TB recurrence, as well as the fact of being male and IDU (25).
More than 60% of immigrant cases had developed TB during their first five years living in Spain (16% during the first year), suggesting that the disease was imported. Pulmonary forms were diagnosed in 55.4% of the cases and 33% were exclusively extrapulmonary. The incidence of Pulmonary TB was higher in the Spaniards and lymphatic forms higher in immigrants (24).
Chapter01.3.indd 41 10/02/14 11:17 AM

42 SECTION 1 THE PRoblEm
THE INFLUENCE OF TB PROGRAMMES An effective TB control programme in a medium and high TB-burden countries should be accompanied by an annual decline in incidence, of 5–10 per cent or more, assuming stable circumstances. External factors such as the HIV epidemic or massive immigration can increase TB infection by up to 20 individuals and TB disease by two individuals annually for each smear-positive TB case.
Political commitment is fundamental towards developing effective TB control programmes and incorporating novel strategies such as Directly Observed Therapy (DOT). For example, when TB was considered to be controlled in New York in the 1980s, TB programme resources decreased and TB and MDR-TB incidence rose at the time of HIV/AIDS epidemic. The programmes were then reinforced by additional human and financial resources (around US$40 million) and TB incidence started to decline from 3,811 cases in 1992 (51.1 per 100,000 population) to less than 1,000 cases in 2005, 2006, and 2007 (only 11.7 per 100,000 inhabitants in the last year) (26).
The Barcelona TB Programme began in 1987 because TB was the most frequently reported disease and was still significantly under-notified (Figure 1.3.5). Many preventive and control interventions were implemented and strengthened by additional research. Epidemiological surveillance for TB and AIDS is based on notification by physicians, control of microbiological results, hospital records, and TB, AIDS and mortality registries. The TB programme has incorporated public health nurses who perform active surveillance of TB in large hospitals, as well as follow-up of patients and contact tracing (24).
When we study the predictors of the non-compliance to TB treatment, we have found that the homeless, prisoners, and IDU are the least compliant. It is, therefore, important to pursue social interventions to improve adherence to treatment. For example, we provide a residence hall for the homeless to stay for several months in order to receive medication. IDU, including those released from prison, are enrolled in methadone programmes to achieve better treatment compliance. Coordination between methadone programmes and penitentiaries has also been beneficial. In infected patients, or MDR patients who refuse treatment and DOT services, the compulsory therapeutic hospitalisation is available. After a resolution of the public health authority, the patient is forced to enter a long-stay facility and follow the treatment. Because of the incorporation of these activities, treatment completion rate (cured divided by cured plus lost to follow-up) has exceeded 95 per cent since 1995 (24).
Chapter01.3.indd 42 10/02/14 11:17 AM

43 CHAPTER 1.3THE CURRENT STATUS OF TB IN THE WORLD: THE INFLUENCE OF POVERTY, PRISONS, HIV, IMMIGRATION AND CONTROL
PROGRAMMES
When TB is diagnosed, we screen the patient’s close contacts, who have more than six hours of daily interactions. Based on this information, we sometimes investigate additional contacts with less frequent interactions with the patient. Between 2003 and 2010, more than 24,000 Tuberculin Skin Tests (TST) were administered as part of the contact investigations, 35% reacted positively and the prevalence of TB found was 1.3%. To improve contact tracing among immigrants, we incorporated community health workers (CHW) in our programme who act as cultural mediators and translators (26). Public health nurses can also try to accommodate appointment difficulties due to a patient’s work obligations. To strengthen the coordination, we conduct regular meetings with public health nurses, doctors, CHW, and persons responsible in administering DOT.
In the last few years, health care services have been reorganized. All large hospitals in the city have clinical TB units which carry out the diagnosis, treatment and monitoring of the patient and the contact tracing in the family. The case manager nurse is the key professional in this new reorganization. The public health nurse and the case manager nurse with the help of the CHW, work together to bring the
80
70
60
50
40
30
20
10
0
85 86 87 88 89 90 91 92 93 94 95 96 97 98 9920
0020
0120
0220
0320
0420
0520
0620
0720
0820
0920
1020
1120
12
Lower incidenceLess IDU among prison
inmates.HIV/infection treated with
HAARTIncrease in immigration
Higher incidenceHIV-IDU association
Prison inmates
TBProgramme
founded
27
36
46
5859
67 6762 62
5854
4944
38 373533 32
2630
2731
272426 25
21
cases/100,000 inhab.
Source: TB Programme of Barcelona.
Figure 1.3.5 The evolution of TB in Barcelona, 1986–2011
Chapter01.3.indd 43 10/02/14 11:17 AM

44 SECTION 1 THE PRoblEm
patient back to health and take care of their environment (family, job, etc.). They offer their support throughout the treatment period and make the access to the health system easier (28).
In high income countries, the improvement of TB control could be related to the management of the resources. A ratio of one nurse per 40 notifications is an effective method to reduce the high incidence observed in some big cities and to maintain the decline in cities of lower incidence (29).
THINkING ABOUT THE FUTURE
The influence of resistancesThe use of antimicrobials not adapted to the susceptibility of the causal agents, low adherence and completion of treatments, poor TB control programmes and lack of access to drugs or TB fix dose combinations, have been appointed as associated factors in the increase of resistances (30). In 2010, more than 650,000 cases amongst 12 million TB cases (5.4%) in the world had reportedly met the MDR-TB criteria. Recent data confirm the high rates of TB caused by resistant strains in Eastern Europe and Central Asia. However, only 60% of countries have available notification data. The prevalence of MDR-TB among new TB cases in the EUR amounted to 13.7% in 2010, showing an increase as compared to how the statistics fared in 2009 (12%). Amongst European countries, Moldova and Belarus have the highest rates (65% and 60%, respectively). Up to 19.4% of the strains in Moldova, 15.4% in Estonia and 14.2% in Kazakhstan present a primary MDR profile. There has been an increase in the number of TB patients diagnosed with MDR-TB in the last five years. However, only 16% of the MDR-TB cases were enrolled on an adequate MDR-TB treatment in 2010 (2).
Every year, there are estimatedly 25,000 new cases of XDR-TB (Strains resistant to isoniazid, rifampin, quinolones and to, at least, one second line injectable drug for TB treatment). XDR-TB represents an important and increasing health problem and a global threat. While the MDR-TB notifications have been stable in the EU/EEA over the past 5 years, the proportion of XDR-TB among this group rose from 8.2% in 2009 to 13.2% in 2010. However, data on XDR-TB are not yet representative of the current situation (5).
Chapter01.3.indd 44 10/02/14 11:17 AM

45 CHAPTER 1.3THE CURRENT STATUS OF TB IN THE WORLD: THE INFLUENCE OF POVERTY, PRISONS, HIV, IMMIGRATION AND CONTROL
PROGRAMMES
In Barcelona, during 2010, 43 of the 301 (14.3%) culture positive patients presented some sort of resistance. Primary resistance to isoniazid was 8.7%, with 3.1% being Spanish born and 13.6% immigrants. Rifampicin resistance was found in only 1.8% samples (1.5% and 2.0% were Spanish-born and immigrants, respectively). Only 3 (1.0%) of cases presented MDR criteria, with all 3 born abroad. In 2009, no XDR cases were identified (24).
In the last few years, public networks working together with the pharmaceutical industry and private partners, had joined efforts to achieve better and simpler early diagnosis methods, new drugs and drug combinations for the efficacious treatment of these patients (31, 32). The use of already known drugs for new indications (such as linezolid, thioridazine and fluoroquinolones) associated with new research antimicrobials (new rifampicin derivatives, azoles, nitroimidazoles, or diarylquinolones) could offer new therapeutical possibilities in the next few years (33, 34, 35).
In conclusion, despite the decrease in TB incidence, drug-resistant TB is becoming a major concern. According to the WHO and ECDC, there is an urgent need to address the causes of transmission and emergence of drug resistant TB. An early TB diagnose (susceptible or drug resistant) and a correct TB treatment in various strengthened national health systems are the key to fight TB resistance worldwide (2, 5). In this sense, an Action Plan to Prevent and Combat MDR and XDR-TB has been created in the European Region and includes a set of activities to be implemented by countries during 2011–2015 (5).
The influence of diabetes mellitusDiabetes mellitus (DM) increases by three-fold the risk of a person to develop active TB; different studies have shown prevalences from 5 to 30% (36). In the last years, low income countries with higher TB burden and mortality, like China and India, are experiencing an epidemic increase in the prevalence of DM. This increase could be influencing TB incidences in some settings and could increase serious clinical forms and complicate treatments in countries with limited access to anti-TB drugs and in big cities, where immigration is concentrated in areas with low social-economic level. In this sense, the Collaborative Framework for Care and Control of Tuberculosis and Diabetes, published by WHO in 2011 (37), attempts to establish guidelines and coordinated actions between the different actors to achieve an effective control of both diseases.
Chapter01.3.indd 45 10/02/14 11:17 AM

46 SECTION 1 THE PRoblEm
In Barcelona, from 2,000 to 2010, 5146 TB cases were notified to the TB Control Programme and 287 (5.6%) had DM. Sixty nine percent were males, where 81.5% were born in Spain, 2.4% being HIV-infected, 4.5% being IDU and 24% being alcohol abusers. The median age was 63 years and the most frequent clinical form was the pulmonary TB (74%). In the city, the prevalence of DM among TB patients has remained stable during the last few years, in contrast to that shown in low income countries. In our environment, Diabetic TB patients are elderly people, born in Spain, drug abusers and have more treatment side effects (11.5%) compared to non-DM patients (38).
The influence of tobaccoIn a review published in 2007, WHO and International Union Against Tuberculosis and Lung Diseases concluded that both active and passive smoking were significantly associated with TB infection and disease. These associations were independent of alcohol use, socioeconomic status and other potential confounders. Significant independent associations were also found between active smoking and recurrent TB and TB mortality (39). Similar conclusions were drawn from further reviews (40, 41, 42, 43).
It is estimated that 30% of the adult world population (approximately 1.250 million people) smoke, and from this, 45% of men and 12% of women (44). According to WHO (2009), smoking causes 5 million deaths per year, and 70% of smokers live in low or intermediate income countries (45). By 2030, the yearly deaths from tobacco could be 8 million, 80% of which had died in such settings (46). It is worth noting that in high income countries, most smokers are from low socio-economic status (47). Regarding TB, in 2010, 38% of TB patients in Barcelona smoked (24), while in the general population the percentage was 24% (2006 data) (48).
Public health actions against tobacco, especially in high income countries, have made marketing strategies in low and middle income countries the focal point in the industry, with higher population growth rates. This will increase the burden of diseases and deaths caused by tobacco in populations with weaker health systems and access to health, and will probably have an impact on the TB dynamics in such settings where the two epidemics collide, increasing the number of infections, cases, relapses and deaths from TB (47).
WHO has published recommendations to tackle the tobacco and TB epidemics in a joint manner which include enforcing smoke-free policies, linking the TB and tobacco control programmes, integrating tobacco interventions in TB program activities and offering TB patients counselling for smoking cessation, among others (46, 49).
Chapter01.3.indd 46 10/02/14 11:17 AM

47 CHAPTER 1.3THE CURRENT STATUS OF TB IN THE WORLD: THE INFLUENCE OF POVERTY, PRISONS, HIV, IMMIGRATION AND CONTROL
PROGRAMMES
Goals and strategies for the control of TBThe MDGs describe the following goals to control the global TB incidence:
- to halt and reverse the trend of TB incidence by 2015;
- to diagnose at least 70 per cent of the sputum smear-positive and cure at least 85 per cent of diagnosed cases by 2005;
- to reduce the prevalence and mortality of TB per capita by 50 per cent relative to rates in 1990, and
- to eliminate TB as a public health problem by 2050, by reducing incidence to less than one case per 1 million people per year (1).
The strategy illustrates six measures to implement for TB control:
1 to pursue high-quality DOTs expansion and enhancement;
2 to address TB/HIV coinfection, MDR-TB and other special challenges;
3 to contribute to health system consolidation;
4 to engage all healthcare providers;
5 to empower TB patients and their communities, and
6 to enable and promote further research.
The strategy has been underway for 10 years and is described in the Global Plan to Stop TB 2006-2015 (1).
Advancement towards the goalsGlobal TB incidence slowly started to decline after its obvious peak in 2002. If an annual decrease by 1.3 per cent is maintained, the MDG on incidence reduction should be reached before 2015 in all WHO regions. Regarding TB prevalence, in spite of its reduction in all six WHO regions, the MDG target will not be achieved in 2015 for the EMR, EUR, SEAR and AFR. However, if the reduction of the mortality continues, the target of the Stop TB partnership of a 50% reduction by 2015 compared to that in 1990 will be met in all WHO regions with the exception of the AFR (2).
Chapter01.3.indd 47 10/02/14 11:17 AM

48 SECTION 1 THE PRoblEm
The best available data on treatment outcomes are for sputum smear positive cases of pulmonary TB, i.e the most infectious cases. The rate of treatment success for the 2.6 million new cases of sputum smear positive pulmonary TB treated during 2009 was 87%. This was the third consecutive year that the target 85% was exceeded globally (2). Among the WHO regions, EMR, SEAR and the WPR exceeded the 85%, set for the first time by World Health Assembly in 1991. The main effort to improve treatment success should be done in the European, the Americas and the African Regions, which currently have 66%, 76% and 81% of treatment success (defined as cured divided by all TB patients) (2). In the EUR treatment success among new and previously treated TB cases, the rate has decreased from 72.5% and 50% in 2005 to 68.7% and 47.6% in 2010, indicating a high MDR TB rate, and therefore a low efficiency of the current TB regiments. It underlines the importance of an early drug resistance test and the need to scale up the first line of drug susceptibility testing in the 18 HPC (5).
It is historically clear that TB and poverty are directly related, as shown by the complementary tendency between TB incidence and the socio-economic level of each country and region. Economically disadvantaged populations throughout all areas in the world are more affected by TB.
There has been relevant progress in TB diagnosis and treatment research in recent years. New challenges for future treatments imply establishing international networks with the participation of different actors. Public and private entities must work together to achieve shorter treatments, with less side effects and easier adherence (2). The TB Alliance or the Tuberculosis Trials Consortium (TBTC), for instance, is made available in different countries worldwide. In this sense, new drugs and combinations have recently shortened the treatment of latent TB infection from 9 to 3 months. Moreover, there are 10 vaccine candidates in Phase I or II that could enter the Phase III trial in the next 2-3 years, and 10 TB drugs in clinical trials that have the potential to shorten the TB and MDR-TB treatments (2).
CONCLUSION TB is still not well-controlled and continues to be a significant problem in many countries, especially in low income countries and even in large cities in high income countries. The ongoing cooperation between high and low TB-burden countries is helpful for both parties.
Chapter01.3.indd 48 10/02/14 11:17 AM

49 CHAPTER 1.3THE CURRENT STATUS OF TB IN THE WORLD: THE INFLUENCE OF POVERTY, PRISONS, HIV, IMMIGRATION AND CONTROL
PROGRAMMES
TB epidemiology is negatively influenced by factors such as poverty, imprisonment, HIV, immigration, resistances, diabetes, tobacco, etc. Fortunately, we can identify some positive factors like improvements in social determinants and health conditions, multicenter and multidisciplinary TB research, the strengthening of TB control programmes and their coordination with other health programmes that may have an impact on TB epidemiology.
In the next few years, TB control will still be based on classic control programmes. If a new vaccine is to be introduced in 5 to 10 years (due to the fact that it is not likely to happen previously), the impact on TB incidence could therefore only be witnessed in 15 to 25 years. We need effective TB control programmes focused on the surveillance of real incidence, avoiding diagnosis delay and treatment abandonment and improving contact tracing. These programmes with annual evaluations should reach acceptable limits of TB levels.
REFERENCES 1. WHo Report 2012. Global Tuberculosis Control 2012. Geneva: WHo, 2011.
Available at: http://www.who.int/tb/publications/global_report/en/index.html
2. WHo Report 2011. Global Tuberculosis Control 2011. Geneva: WHo, 2011. Available at: http://www.who.int/tb/publications/global_report/2011/gtbr11_full.pdf.
3. Hinman AR, Judd Jm, Kolnik JP, and Daitch Pb. Changing risks in tuberculosis. Am J Epidemiol, 1976; 103(5): 486–97.
4. brahdy l. Tuberculosis in hospital personnel. JAmA, 1940; 114: 102–5.
5. European Center for Disease Prevention and Control (ECDC) and WHo. Tuberculosis Surveillance and monitoring in Europe, 2012. Available at: http://ecdc.europa.eu/en/publications/Publications/1203-Annual-Tb-Report.pdf.
6. organización mundial de la Salud y Comité Internacional de la Cruz Roja. El control de la Tuberculosis en prisiones: manual para directores de programas. Available at: http://www.sesp.es/sesp/pdf/libroTbC.pdf.
7. organización Panamericana de la Salud. Guía para el control de la tuberculosis en poblaciones privadas de libertad de América latina y el Caribe. Washington DC: oPS, 2008.
Chapter01.3.indd 49 10/02/14 11:17 AM

50 SECTION 1 THE PRoblEm
8. WHo. literature Review on Tb Control in Prisons. Available at: http://www.who.int/tb/challenges/prisons/tb_in_prisons_lit_review_10feb08.pdf.
9. martín V, González P, Caylà JA, mirabent J, Cañellas J, Pina Jm, et al. Case-finding of pulmonary tuberculosis on admission to a penitentiary centre. Tuber Lung Dis, 1994; 75(1): 49–53.
10. martín V, Guerra Jm, Caylà JA, Rodríguez JC, blanco mD, and Alcoba m. Incidence of tuberculosis and treatment of latent tuberculosis infection in a Spanish prison population. Int J Tuberc lung Dis, 2001; 5(10): 926–32.
11. Coll P, Guerrero RA, busquets E, Caylà JA, and Prats G. Predictors of tuberculosis transmission in prisons: an analysis using conventional and molecular methods. AIDS, 2000; 14(5): 525–35.
12. Selwyn PA, Hartel D, lewis VA, Schoenbaum EE, Vermund SH, Klein RS, et al. A prospective study of the risk of tuberculosis among intravenous drug users with human immunodeficiency virus infection. N Engl J med, 1989; 320(9): 545–50.
13. UNAIDS. 2010 Epidemic update. UNAIDS report on the global AIDS epidemic 2010. Available at: http://www.unaids.org/documents/ 20101123_GlobalReport_Chap2_em.pdf.
14. Corbett El, Watt CJ, Walker N, maher D, Williams bG, Raviglione mC, et al. The growing burden of tuberculosis. The growing burden of tuberculosis: global trends and interactions with the HIV epidemic. Arch Intern med, 2003; 163(9): 1009–21.
15. Suchindran S, brouwer ES, and Van Rie A. Is HIV infection a risk factor for multi-drug resistant tuberculosis? A systematic review. PloS oNE, 2009; 4(5): e5561.
16. Wells CD, Cegielski JP, Nelson lJ, laserson KF, Holtz TH, Finlay A, et al. HIV infection and multidrugresistant tuberculosis: the perfect storm. J Infect Dis, 2007; 196 Suppl: S86–S107.
17. Gandhi NR, moll A, Sturm AW, Pawinski R, Govender T, lalloo U, et al. Extensively drug-resistant tuberculosis as a cause of death in patients co-infected with tuberculosis and HIV in a rural area of South Africa. lancet, 2006; 368(9547): 1575–80.
Chapter01.3.indd 50 10/02/14 11:17 AM

51 CHAPTER 1.3THE CURRENT STATUS OF TB IN THE WORLD: THE INFLUENCE OF POVERTY, PRISONS, HIV, IMMIGRATION AND CONTROL
PROGRAMMES
18. brindle RJ, Nunn PP, batchelor bI, Gathua SN, Kimari JN, Newnham RS, et al. Infection and morbidity in patients with tuberculosis in Nairobi, Kenya. AIDS, 1993; 7(11): 1469–74.
19. Reid mJ and Shah NS. Approaches to tuberculosis screening and diagnosis HIV Infection–Associated Tb in people with HIV in resource-limited settings. lancet Infect Dis, 2009; 9: 173–84.
20. Getahun H, Harrington m, o’brien R, and Nunn P. Diagnosis of smearnegative pulmonary tuberculosis in people with HIV infection or AIDS in resource-constrained settings: informing urgent policy changes. lancet, 2007; 369: 2042–9.
21. WHo. Towards universal access: scaling up priority HIV/AIDS interventions in the health sector. World Health organization, Geneva, Switzerland, 2008. Available at: http://www.who.int/hiv/pub/tuapr 2009 en.pdf.
22. Getahun H, Gunneberg C, Granich R, and Nunn P. HIV infection-associated tuberculosis: the epidemiology and the response. Clin Infect Dis, 2010; 50: S201–7.
23. Instituto Nacional de Estadistica. Avance del pardon municipal a 1 de enero de 2011. Available at: http://www.ine.es/prensa/np648.pdf.
24. Agencia de Salud Pública de barcelona. la tuberculosi a barcelona. Informe 2010.Available at: http://www.aspb.es/quefem/docs/Tuberculosi_2010.pdf.
25. millet JP, orcau A, de olalla PG, Casals m, Rius C, and Caylà JA. Tuberculosis Recurrence and its associated risk factors among successfully treated patients. J Epidemiol Community Health, 2009; 63(10): 799–804.
26. Tb Annual Summary: 2007. New York: New York City Department of Health and mental Hygiene, 2008.
27. ospina JE, orcau A, millet JP, Sánchez F, Casals m, Rius C, et al. Improving contact tracing in tuberculosis effectiveness of community health workers in a city with massive recent immigration. bmC Public Health, 2012; 12: 158.
28. Caylà JA and orcau A. Control of tuberculosis in large cities in developed countries: an organizational problem. bmC med, 2011; 9: 127. Available at: http://www.biomedcentral.com/1471-2458/11/896.
Chapter01.3.indd 51 10/02/14 11:17 AM

52 SECTION 1 THE PRoblEm
29. bothamley GH, Kruijshaar mE, Kunst H, Woltmann G, Cotton m, Saralaya D, et al. Tuberculosis in UK cities: workload and effectiveness of tuberculosis control programmes. bmC Public Health, 2011; 11: 896. Available at: http://www.biomedcentral.com/1741-7015/9/127.
30. Sharma SK and mohan A. multidrug-Resistant tuberculosis: a menace that threatens to destabilize tuberculosis control. Chest, 2006; 130: 162–272.
31. Chan ED and Iseman mD. multidrug-resistant and extensively drug-resistant tuberculosis: a review. Curr opin Infect Dis, 2008;21(6): 587–95.
32. Ruiz-manzano J, blanquer R, Calpe Jl, Caminero JA, Caylà J, Domínguez JA, et al. Diagnóstico y tratamiento de la tuberculosis. Normativa SEPAR. Arch bronconeumol, 2008; 44: 551–66.
33. Sarkar S and Suresh mR. An overview of tuberculosis chemotherapy – Aliterature review. J Pharm Pharmaceut Sci, 2011; 14: 148–61.
34. Singla R, Caminero JA, Jaswal A, Singla N, Gupta S, bali RK, et al. linezolid, an effective, safe and cheap drug in mDR-Tb treatment failure in India. Eur Respir J, 2011; Sep 29. [Epub ahead of print]
35. Amaral l, boeree mJ, Gillespie SH, Udwadia ZF, and van Soonlingen D. Thioridazine cures extensively drug-resistant tuberculosis (XDR-Tb) and the need for global trials is now! Int J Antimicrobiol Agents, 2010; 35: 524–6.
36. Ruslami R, Aarnoutse RE, Alisjahbana b, van der Ven AJAm, and van Crevel R. Implications of the global increase of diabetes for tuberculosis control and patient care. Trop med Int Health, 2010; 15: 1289–99.
37. Collaborative Framework for Care and Control of Tuberculosis and Diabetes, WHo 2011. Available: http://whqlibdoc.who.int/publications/2011/9789241502252_eng.pdf.
38. moreno A, millet JP, orcau A, Fina l, del baño l, Simon P, et al. Factors associated with diabetes mellitus among tuberculosis patients in a western european city. Communication 22nd ECCmID, london 2012.
39. WHo. The Union Against Tuberculosis and lung Diseases. A WHo / The Union monograph on Tb and tobacco control: joining efforts to control two relatedglobal epidemics. 2007; WHo/HTm/Tb/2007.390:21-23.
Chapter01.3.indd 52 10/02/14 11:17 AM

53 CHAPTER 1.3THE CURRENT STATUS OF TB IN THE WORLD: THE INFLUENCE OF POVERTY, PRISONS, HIV, IMMIGRATION AND CONTROL
PROGRAMMES
40. Slama K, Chiang CY, Enarson DA, Hassmiller, Fanning A, Gupta P, et al. Tobacco and tuberculosis: a qualitative systematic review and meta-analysis. Int J Tuberc lung Dis, 2007; 11(10): 1049–61.
41. lin HH, Ezzati m, and murray m. Tobacco smoke, indoor air pollution and tuberculosis: a systematic review and meta-analysis. PloS med, 2007; 4(1): e20.
42. bates mN, Khalakdina A, Pai m, Chang l, lessa F, and Smith KR. Risk of tuberculosis from exposure to tobacco smoke. A systematic review and meta-analysis. Arch Intern med, 2007; 167: 335–42.
43. moreno A, millet JP, orcau A, Fina l, del baño l, Villegas S, et al. Tabaco y tuberculosis, una asociación evidente. Prev tabaquismo, 2011;13Suppl 1. Available at: http://issuu.com/separ/docs/revista_prevenci_n_del_tabaquismo_diciembre_2011.
44. Shafey o, Eriksen m, Ross H, and mackay J. El atlas del tabaco. Sociedad Americana del Cáncer 2009; 3ª Ed:18-21.
45. WHo. Factsheet on Tuberculosis and Tobacco, 2009. Available at: http://www.who.int/tobacco/resources/publications/factsheet_tub_tob.pdf.
46. WHo report on the global tobacco epidemic, 2009: implementing smoke-free environments.
47. leung Cm, leung KC, Hon KE, and Kong AY. Fighting Tobacco Smoking – a difficult but not impossible battle. Int J Environ Res Public Health, 2009; 6(1): 69–83.
48. Agencia de Salud Publica de barcelona. Enquesta de salut de barcelona 2006. Available at: http://www.aspb.es/quefem/docs/Enquesta%20Salut%20barcelona%202006.pdf.
49. WHo Report on the global tobacco epidemic, 2011.Available at: http://whqlibdoc.who.int/publications/2011/9789240687813_eng.pdf.
Chapter01.3.indd 53 10/02/14 11:17 AM





![HOME []...1Safety 4 InstallationandmaintenanceinstructionsHOME0020224338_00 1.3.4 Riskofdeathfromescapingflue gas Ifyouoperatetheproductwithanemptycon-densatesiphon](https://img.pdfslide.us/doc/110x75/5ed15649a1ede55bf9720898/home-1safety-4-installationandmaintenanceinstructionshome002022433800-134.jpg)